Contents
- What is knee replacement
- When a knee replacement is needed
- How your new knee is different
- Knee replacement surgery risks
- How long will a replacement knee last?
- Deciding to Have Knee Replacement Surgery
- The Knee Joint
- Types of knee replacement surgery
- Preparing for knee replacement surgery
- How knee replacement surgery is performed
- After knee replacement surgery
- Knee replacement recovery
- Recovery at Home
What is knee replacement
Knee replacement surgery is also called knee arthroplasty, is a routine operation that involves replacing a damaged, worn or diseased knee with an artificial joint made of metal and plastic parts. Adults of any age can be considered for a knee replacement, although most are carried out on people between the ages of 60 and 80. More people are now receiving this operation at a younger age.
Most people leave hospital 1-4 days after a knee replacement surgery. How quickly you get back to normal depends on many factors, including your age and general health and fitness.
You will probably need a cane, crutches or walking frame in the first few weeks and an exercise and physiotherapy program to help you recover.
Knee replacement surgery was first performed in 1968. Since then, improvements in surgical materials and techniques have greatly increased its effectiveness. Total knee replacements are one of the most successful procedures in all of medicine. According to the Agency for Healthcare Research and Quality, more than 600,000 knee replacements are performed each year in the United States.
There are four basic steps to a knee replacement procedure:
- Prepare the bone. The damaged cartilage surfaces at the ends of the femur and tibia are removed along with a small amount of underlying bone.
- Position the metal implants. The removed cartilage and bone is replaced with metal components that recreate the surface of the joint. These metal parts may be cemented or “press-fit” into the bone.
- Resurface the patella. The undersurface of the patella (kneecap) is cut and resurfaced with a plastic button. Some surgeons do not resurface the patella, depending upon the case.
- Insert a spacer. A medical-grade plastic spacer is inserted between the metal components to create a smooth gliding surface.
The decision to have total knee replacement surgery should be a cooperative one between you, your family, your family physician, and your orthopedic surgeon. Your physician may refer you to an orthopedic surgeon for a thorough evaluation to determine if you might benefit from this surgery.
When a knee replacement is needed
Knee replacement surgery is usually necessary when the knee joint is worn or damaged to the extent that your mobility is reduced and you experience pain even while resting.
If your knee is severely damaged by arthritis or injury, it may be hard for you to perform simple activities, such as walking or climbing stairs. You may even begin to feel pain while you are sitting or lying down.
If nonsurgical treatments like medications and using walking supports are no longer helpful, you may want to consider total knee replacement surgery. Knee joint replacement surgery is a safe and effective procedure to relieve pain, correct leg deformity, and help you resume normal activities.
The most common cause of chronic knee pain and disability is arthritis. Although there are many types of arthritis, most knee pain is caused by just three types: osteoarthritis, rheumatoid arthritis, and post-traumatic arthritis.
- Osteoarthritis. This is an age-related “wear and tear” type of arthritis. It usually occurs in people 50 years of age and older, but may occur in younger people, too. The cartilage that cushions the bones of the knee softens and wears away. The bones then rub against one another, causing knee pain and stiffness.
- Rheumatoid arthritis. This is a disease in which the synovial membrane that surrounds the joint becomes inflamed and thickened. This chronic inflammation can damage the cartilage and eventually cause cartilage loss, pain, and stiffness. Rheumatoid arthritis is the most common form of a group of disorders termed “inflammatory arthritis.”
- Post-traumatic arthritis. This can follow a serious knee injury. Fractures of the bones surrounding the knee or tears of the knee ligaments may damage the articular cartilage over time, causing knee pain and limiting knee function.
The most common reason for knee replacement surgery is osteoarthritis. Other conditions that cause knee damage include:
- Rheumatoid arthritis
- Hemophilia
- Gout
- Disorders that cause unusual bone growth (bone dysplasias)
- Death of bone in the knee joint following blood supply problems (avascular necrosis)
- Knee injury
- Knee deformity with pain and loss of cartilage
Who is offered knee replacement surgery
A knee replacement is major surgery, so is normally only recommended if other treatments, such as physiotherapy or steroid injections, haven’t helped reduce pain or improve mobility.
You may be offered knee replacement surgery if:
- You have severe knee pain, swelling and stiffness in your knee joint that limits your everyday activities, including walking, climbing stairs, and getting in and out of chairs. You may find it hard to walk more than a few blocks without significant pain and you may need to use a cane or walker
- Your knee pain is so severe that it interferes with your quality of life and sleep
- Moderate or severe knee pain while resting, either day or night
- Everyday tasks, such as shopping or getting out of the bath, are difficult or impossible
- You’re feeling depressed because of the pain and lack of mobility
- You can’t work or have a normal social life
- Chronic knee inflammation and swelling that does not improve with rest or medications
- Knee deformity — a bowing in or out of your knee
- Failure to substantially improve with other treatments such as anti-inflammatory medications, cortisone injections, lubricating injections, physical therapy, or other surgeries
You’ll also need to be well enough to cope with both a major operation and the rehabilitation afterwards.
Candidates for knee replacement surgery
There are no absolute age or weight restrictions for total knee replacement surgery.
Recommendations for knee replacement surgery are based on a patient’s pain and disability, not age. Most patients who undergo total knee replacement are age 50 to 80, but orthopedic surgeons evaluate patients individually. Total knee replacements have been performed successfully at all ages, from the young teenager with juvenile arthritis to the elderly patient with degenerative arthritis.
How your new knee is different
Improvement of knee motion is a goal of total knee replacement, but restoration of full motion is uncommon. The motion of your knee replacement after surgery can be predicted by the range of motion you have in your knee before surgery. Most patients can expect to be able to almost fully straighten the replaced knee and to bend the knee sufficiently to climb stairs and get in and out of a car. Kneeling is sometimes uncomfortable, but it is not harmful.
Most people feel some numbness in the skin around your incision. You also may feel some stiffness, particularly with excessive bending activities.
Most people also feel or hear some clicking of the metal and plastic with knee bending or walking. This is a normal. These differences often diminish with time and most patients find them to be tolerable when compared with the pain and limited function they experienced prior to surgery.
Your new knee may activate metal detectors required for security in airports and some buildings. Tell the security agent about your knee replacement if the alarm is activated.
Knee replacement surgery risks
Knee replacement surgery is a common operation and most people don’t experience complications. However, as with any operation, knee replacement surgery has risks as well as benefits.
Possible complications of knee replacement surgery are rare but can include:
Complications occur in about one in 20 cases, but most are minor and can be successfully treated. Possible complications include:
- infection of the wound – this is usually treated with antibiotics, but occasionally the wound can become deeply infected and require further surgery; in rare cases it may require replacement of the artificial knee joint.
- stiffness of the knee
- deep infection of the joint replacement, needing further surgery
- unexpected bleeding into the knee joint
- ligament, artery or nerve damage in the area around the knee joint
- blood clots or deep vein thrombosis (DVT) – clots may form in the leg veins as a result of reduced movement in the leg during the first few weeks after surgery. They can be prevented by using special support stockings, starting to walk or exercise soon after surgery, and by using anticoagulant medicines
- fracture in the bone around the artificial joint during or after surgery – treatment will depend on the location and extent of the fracture
- excess bone forming around the artificial knee joint and restricting movement of the knee – further surgery may be able to remove this and restore movement
- excess scar tissue forming and restricting movement of the knee – further surgery may be able to remove this and restore movement
- the kneecap becoming dislocated – surgery can usually repair this
- numbness in the area around the wound scar
- allergic reaction – you may have an allergic reaction to the bone cement if this is used in your procedure
- persistent pain the in the knee
- fracture – a break in the bone around the knee replacement during or after the operation
In some cases, the new knee joint may not be completely stable and further surgery may be needed to correct it.
The complication rate following total knee replacement is low. Serious complications, such as a knee joint infection, occur in fewer than 2% of patients. Major medical complications such as heart attack or stroke occur even less frequently. Chronic illnesses may increase the potential for complications. Although uncommon, when these complications occur, they can prolong or limit full recovery.
Discuss your concerns thoroughly with your orthopedic surgeon prior to surgery.
Infection. Infection may occur in the wound or deep around the prosthesis. It may happen while in the hospital or after you go home. It may even occur years later. Minor infections in the wound area are generally treated with antibiotics. Major or deep infections may require more surgery and removal of the prosthesis. Any infection in your body can spread to your joint replacement.
Blood clots. Blood clots in the leg veins are one of the most common complications of knee replacement surgery. These clots can be life-threatening if they break free and travel to your lungs. Your orthopedic surgeon will outline a prevention program, which may include periodic elevation of your legs, lower leg exercises to increase circulation, support stockings, and medication to thin your blood.
Implant problems. Although implant designs and materials, as well as surgical techniques, continue to advance, implant surfaces may wear down and the components may loosen. Additionally, although an average of 115° of motion is generally anticipated after surgery, scarring of the knee can occasionally occur, and motion may be more limited, particularly in patients with limited motion before surgery.
Continued pain. A small number of patients continue to have pain after a knee replacement. This complication is rare, however, and the vast majority of patients experience excellent pain relief following knee replacement.
Neurovascular injury. While rare, injury to the nerves or blood vessels around the knee can occur during surgery.
In some cases, the new knee joint may not be completely stable and further surgery may be needed to correct it.
Anesthesia
Anesthetics are extremely safe, but carry a risk of minor side effects such as sickness and confusion (usually temporary). There is also a slight risk of serious complications.
The risk of death in a healthy person having routine surgery is very small. Death occurs in around one in every 100,000 general anesthetics given.
The risk is higher if you’re older or have other health conditions, such as heart or lung disease.
Your anesthetist and surgeon can answer questions you may have about your personal risks from anesthetic or the surgery itself.
How long will a replacement knee last?
Wear and tear through everyday use means your replacement knee won’t always last forever. Some people will need further surgery.
According to the National Joint Registry, around 5% of patients who have a knee replacement (1 in 20) will need further surgery after 12 years. However, this varies depending on the type of replacement. Total knee replacements tend to last longer than partial knee replacements.
Extending the life of your knee implant
Currently, more than 90% of modern total knee replacements are still functioning well 15 years after the surgery. Following your orthopaedic surgeon’s instructions after surgery and taking care to protect your knee replacement and your general health are important ways you can contribute to the final success of your surgery.
Protecting your knee replacement
After knee replacement surgery, make sure you also do the following:
- Participate in regular light exercise programs to maintain proper strength and mobility of your new knee.
- Take special precautions to avoid falls and injuries. If you break a bone in your leg, you may require more surgery.
- Make sure your dentist knows that you have a knee replacement. Talk with your orthopedic surgeon about whether you need to take antibiotics prior to dental procedures.
- See your orthopedic surgeon periodically for a routine follow-up examination and x-rays, usually once a year.
Deciding to Have Knee Replacement Surgery
An important factor in deciding whether to have total knee replacement surgery is understanding what the procedure can and cannot do.
More than 90% of people who have total knee replacement surgery experience a dramatic reduction of knee pain and a significant improvement in the ability to perform common activities of daily living. But total knee replacement will not allow you to do more than you could before you developed arthritis.
With normal use and activity, every knee replacement implant begins to wear in its plastic spacer. Excessive activity or weight may speed up this normal wear and may cause the knee replacement to loosen and become painful. Therefore, most surgeons advise against high-impact activities such as running, jogging, jumping, or other high-impact sports for the rest of your life after surgery.
Realistic activities following total knee replacement include unlimited walking, swimming, golf, driving, light hiking, biking, ballroom dancing, and other low-impact sports.
With appropriate activity modification, knee replacements can last for many years.
The Knee Joint
The knee joint (tibiofemoral joint) is the largest and most complex joint of the body (Figures 1) and having healthy knees is required to perform most everyday activities. The knee joint (tibiofemoral joint) is a modified hinge joint (because its primary movement is a uniaxial hinge movement) that consists of three joints within a single synovial cavity:
- Laterally is a tibiofemoral joint, between the lateral condyle of the femur, lateral meniscus, and lateral condyle of the tibia, which is the weight-bearing bone of the leg.
- Medially is another tibiofemoral joint, between the medial condyle of the femur, medial meniscus, and medial condyle of the tibia.
- An intermediate patellofemoral joint is between the patella and the patellar surface of the femur.
The knee is made up of the lower end of the thighbone (femur), the upper end of the shinbone (tibia), and the kneecap (patella). The ends of these three bones where they touch are covered with articular cartilage, a smooth substance that protects the bones and enables them to move easily.
The menisci are located between the femur and tibia. These C-shaped wedges act as “shock absorbers” that cushion the joint.
Large ligaments hold the femur and tibia together and provide stability. The long thigh muscles give the knee strength.
All remaining surfaces of the knee are covered by a thin lining called the synovial membrane. This membrane releases a fluid that lubricates the cartilage, reducing friction to nearly zero in a healthy knee.
Normally, all of these components work in harmony. But disease or injury can disrupt this harmony, resulting in pain, muscle weakness, and reduced function.
Figure 1. Anatomy of the knee
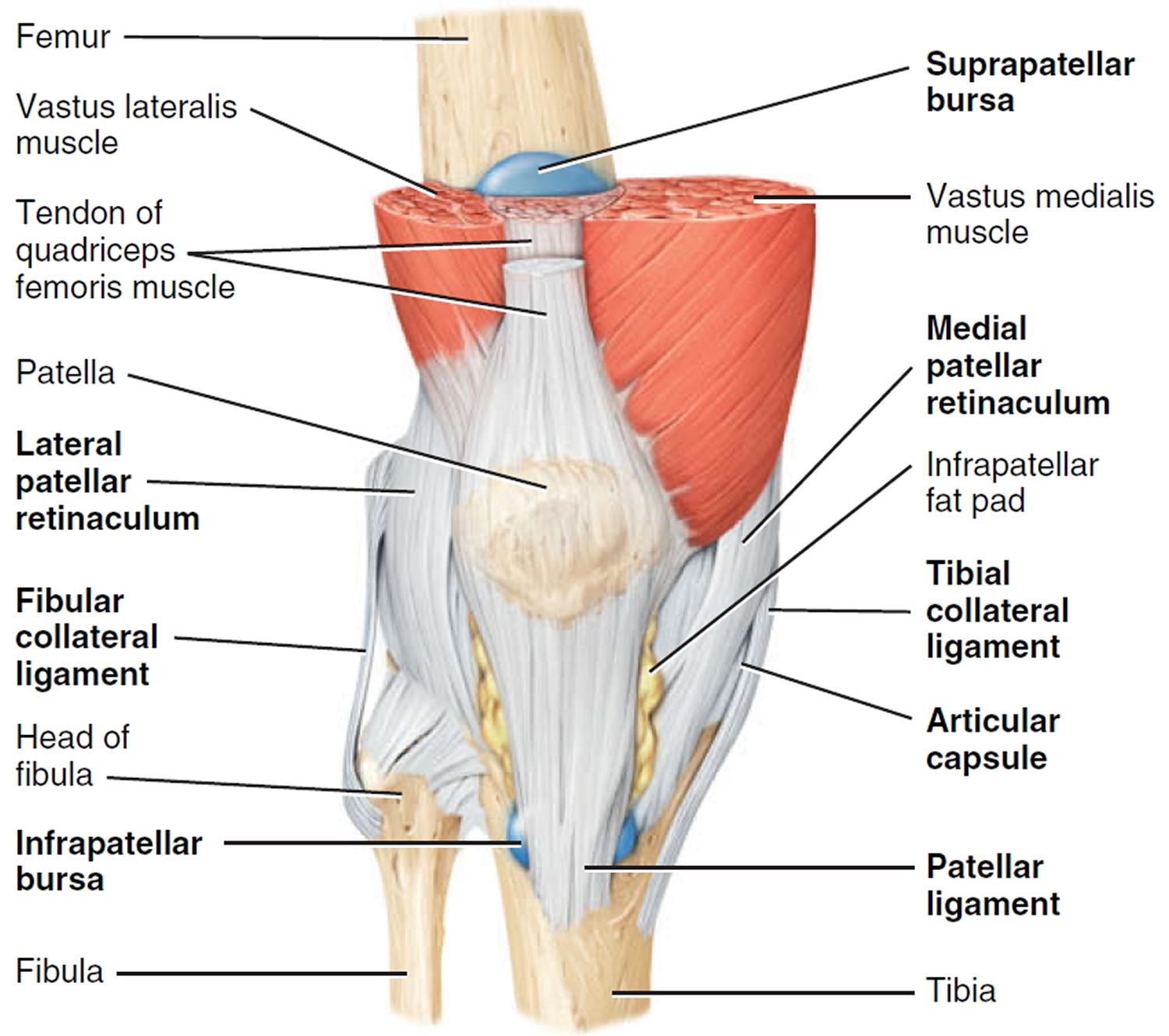
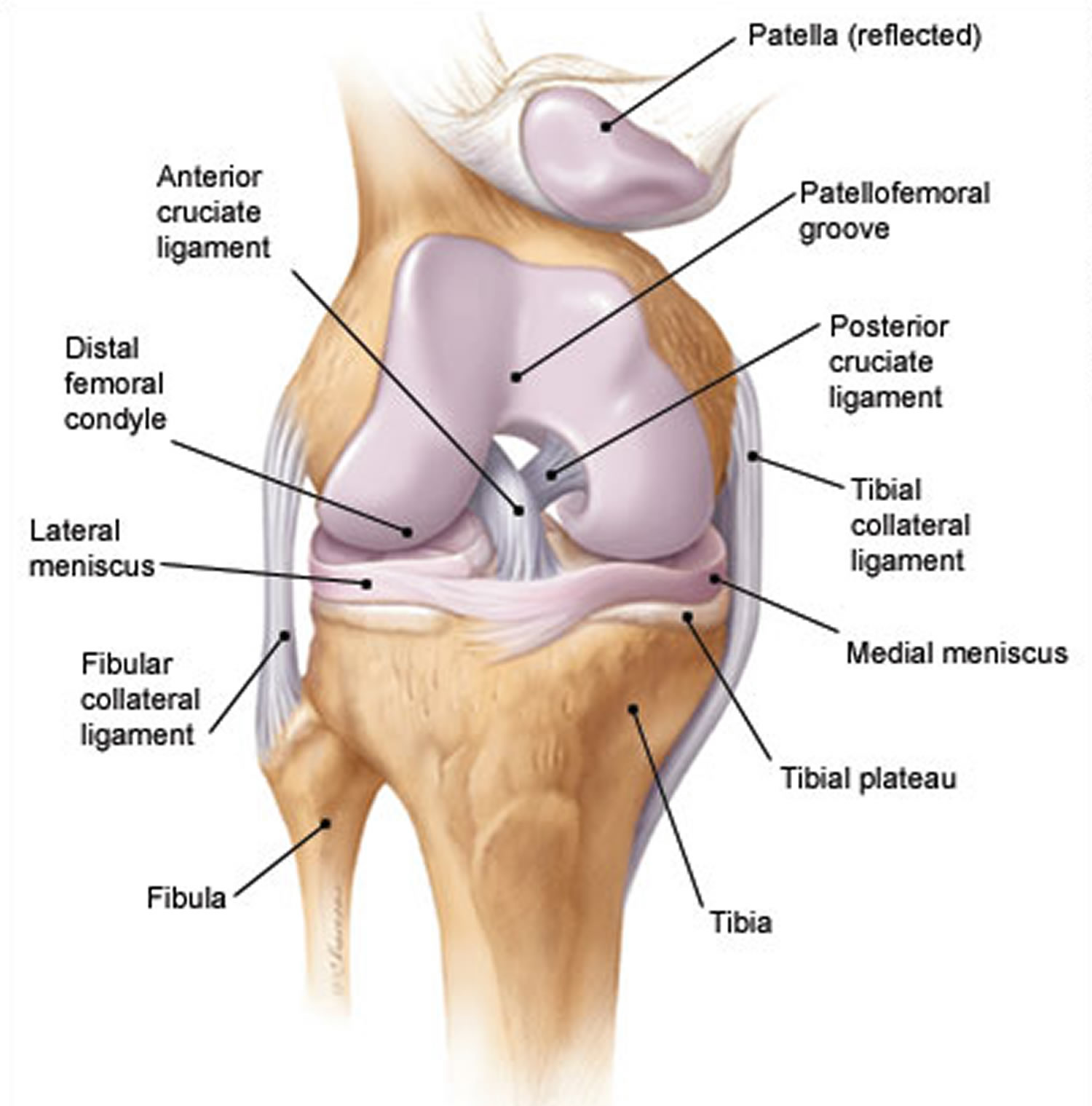
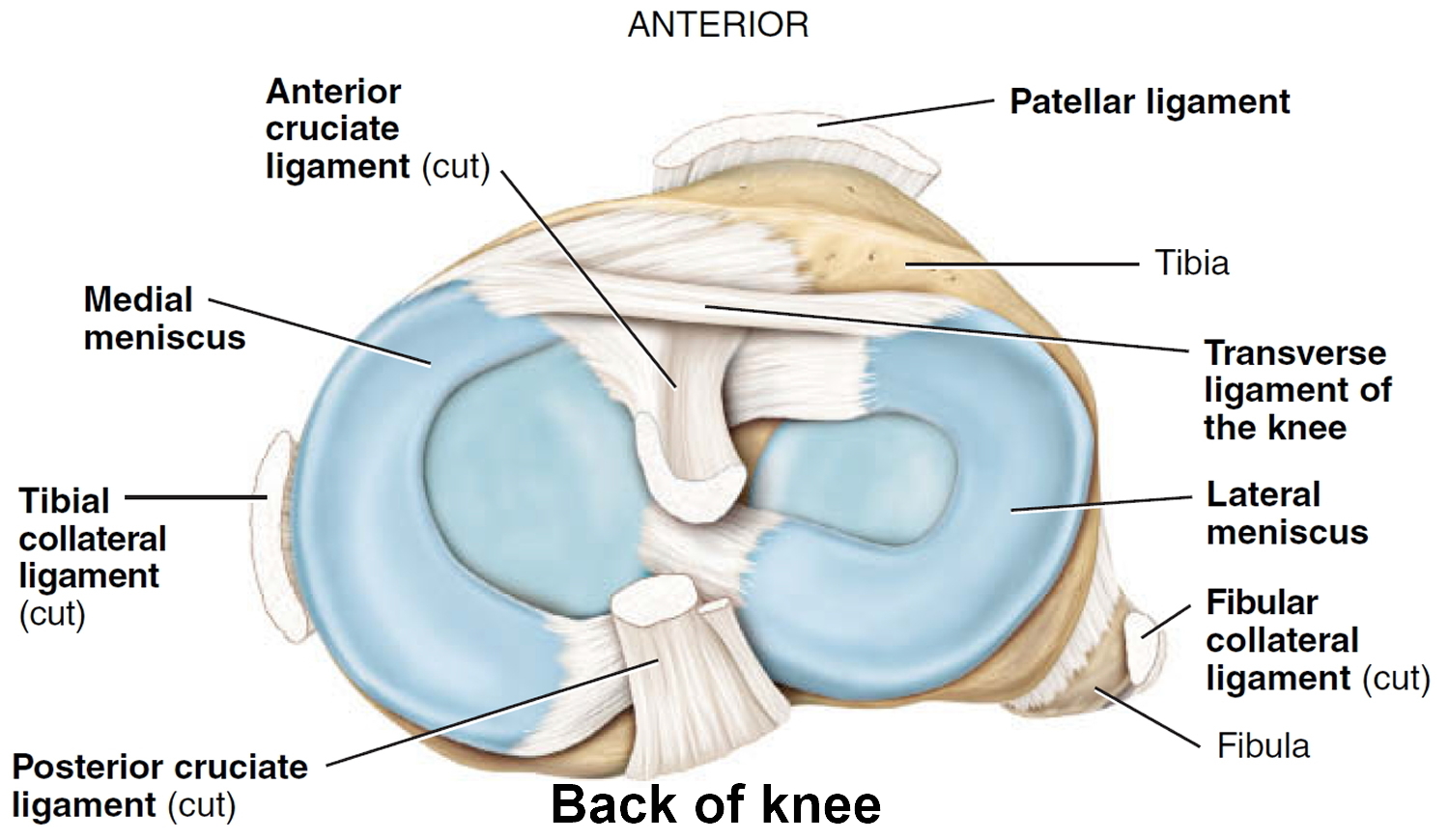
Figure 2. Knee joint anatomy posterior view
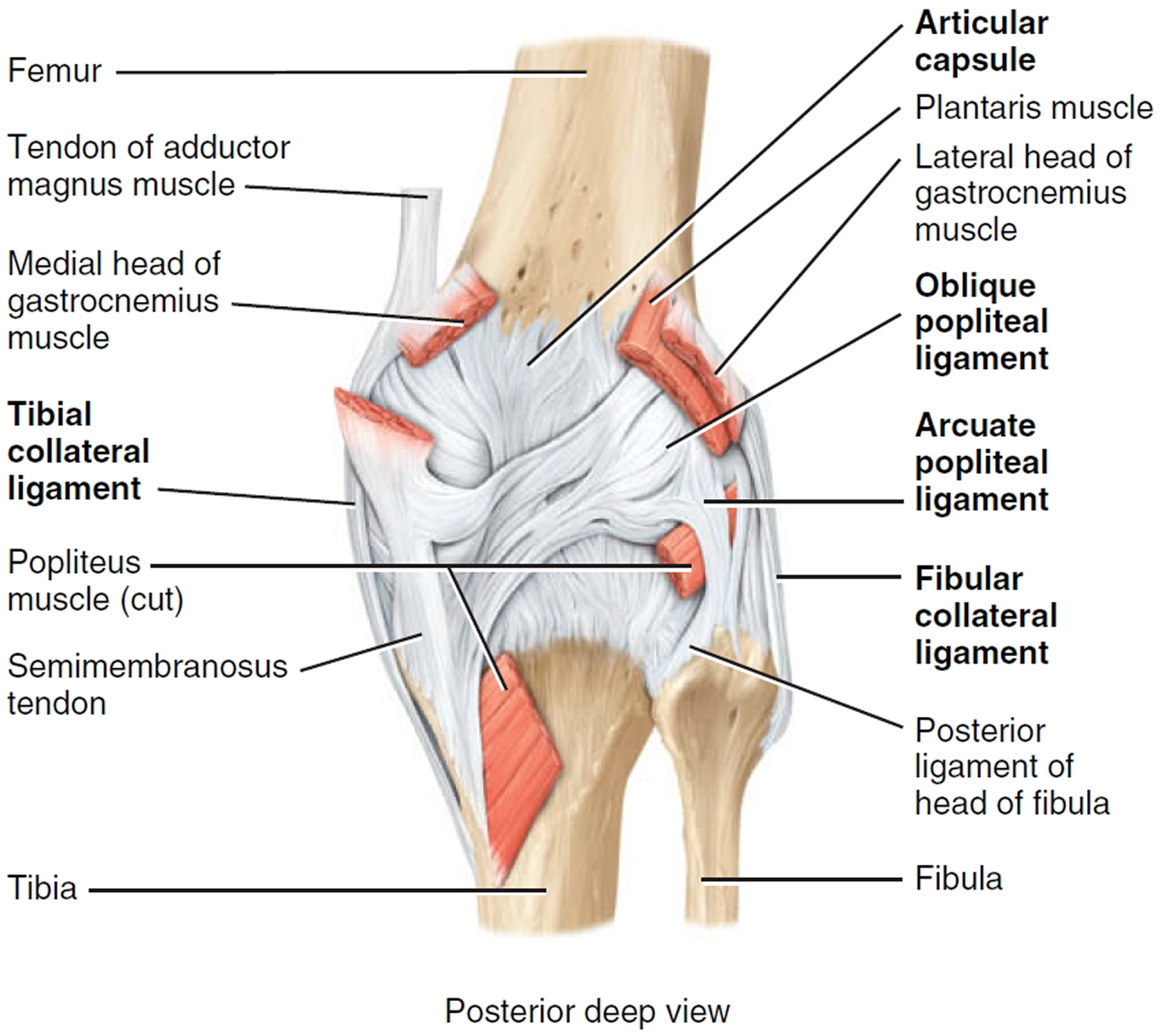
Figure 3. Knee joint anatomy sagittal view
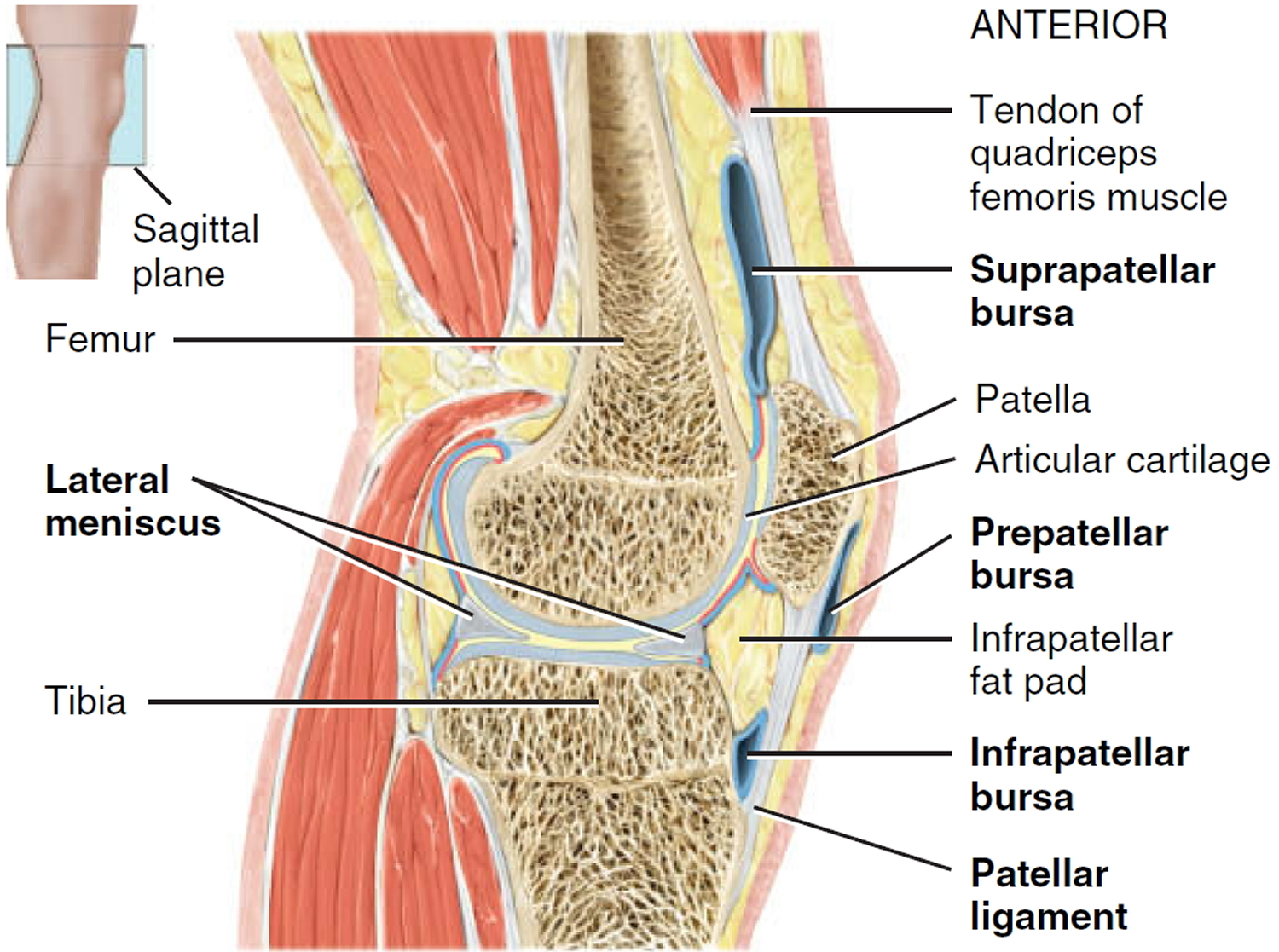
Figure 4. Different types of knee implants that are used in knee replacement to meet each patient’s individual needs.

Figure 5. Knee replacement
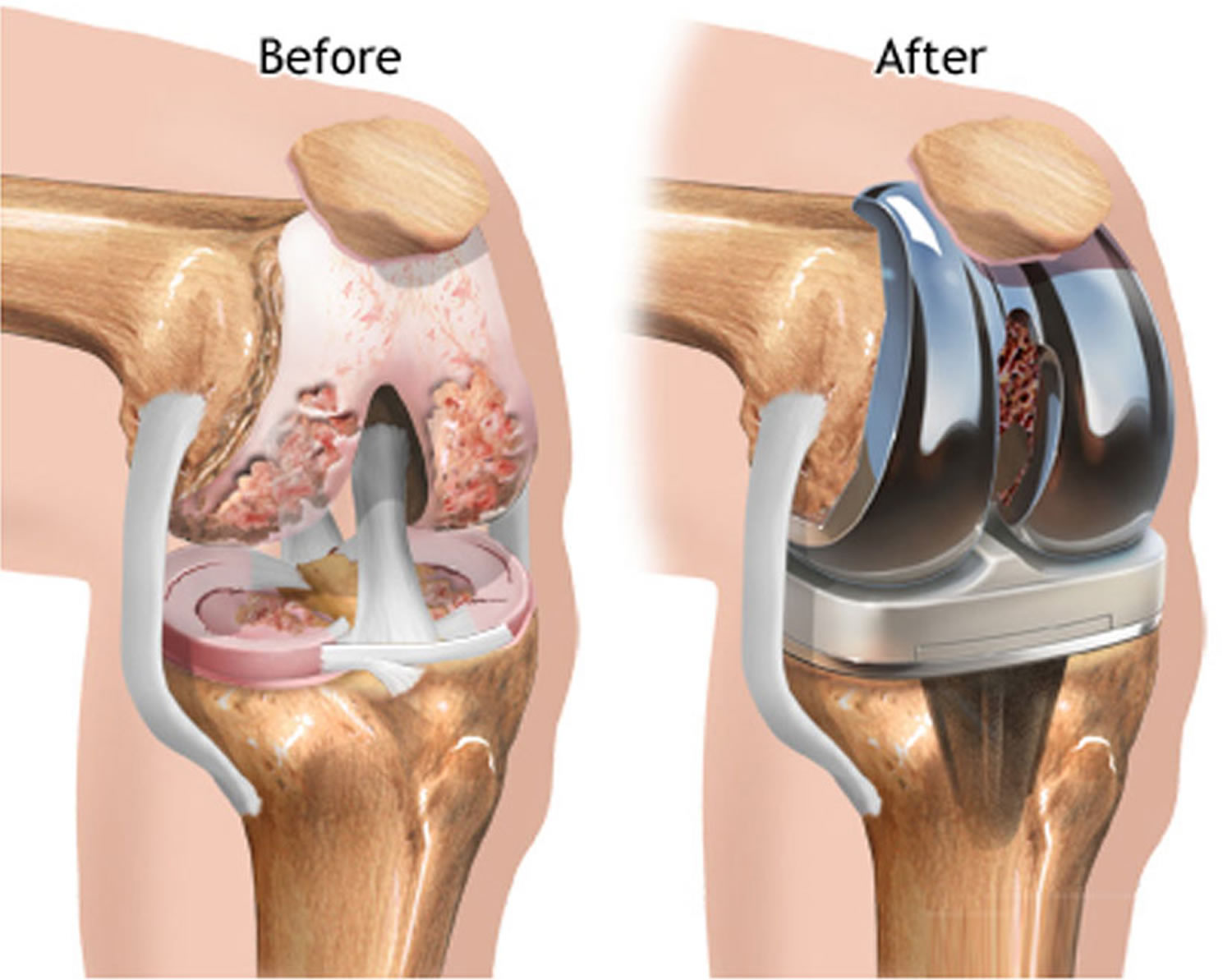
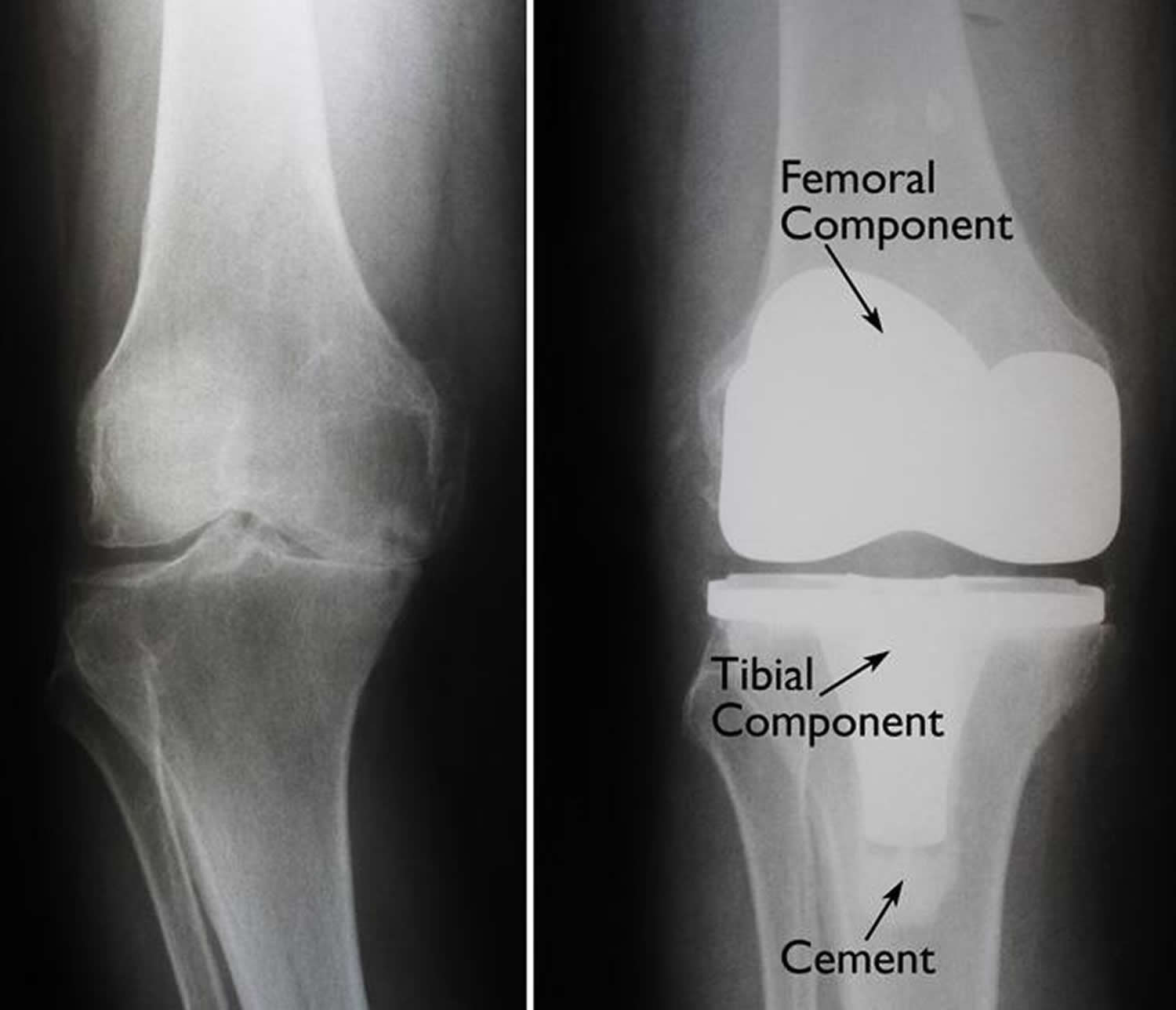
Figure 6. Knee replacement surgery before and after (X-rays) – (Left) An x-ray of a severely arthritic knee. (Right) The x-ray appearance of a total knee replacement. Note that the plastic spacer inserted between the components does not show up in an x-ray.
Types of knee replacement surgery
There are two main types of surgery, depending on the condition of the knee:
- Total knee replacement (TKR) – both sides of your knee joint are replaced
- Partial (half) knee replacement (PKR) – only one side of your joint is replaced in a smaller operation with a shorter hospital stay and recovery period
Knee replacement surgery alternatives
There are alternative surgeries to knee replacement, but results are often not as good in the long term. Your doctor will discuss the best treatment option with you. Alternatives may include:
- Arthroscopic washout and debridement – an arthroscope (tiny telescope) is inserted into the knee, which is then washed out with saline to clear out any bits of bone or cartilage
- Osteotomy – during an open operation, the surgeon cuts the shin bone and realigns it so that weight is no longer focused on the damaged part of the knee
- Mosaicplasty – a keyhole operation that involves transferring plugs of hard cartilage, together with some underlying bone from another part of your knee, to repair the damaged surface
Preparing for knee replacement surgery
Before you go into hospital, find out as much as you can about what’s involved in your operation. Your surgeon and hospital should provide written information or videos.
Stay as active as you can. Strengthening the muscles around your knee will aid your recovery. If you can, continue to take gentle exercise, such as walking and swimming, in the weeks and months before your operation. You can be referred to a physiotherapist, who will give you helpful exercises.
Orthopedic Evaluation
An evaluation with an orthopedic surgeon consists of several components:
- A medical history. Your orthopedic surgeon will gather information about your general health and ask you about the extent of your knee pain and your ability to function.
- A physical examination. This will assess knee motion, stability, strength, and overall leg alignment.
- X-rays. These images help to determine the extent of damage and deformity in your knee.
- Other tests. Occasionally blood tests, or advanced imaging such as a magnetic resonance imaging (MRI) scan, may be needed to determine the condition of the bone and soft tissues of your knee.
Medical Evaluation
If you decide to have total knee replacement surgery, your orthopaedic surgeon may ask you to schedule a complete physical examination with your family physician several weeks before the operation. This is needed to make sure you are healthy enough to have the surgery and complete the recovery process. Many patients with chronic medical conditions, like heart disease, may also be evaluated by a specialist, such as a cardiologist, before the surgery.
Tests
Several tests, such as blood and urine samples, and an electrocardiogram, may be needed to help your orthopaedic surgeon plan your surgery.
Medications
Tell your orthopaedic surgeon about the medications you are taking. He or she will tell you which medications you should stop taking and which you should continue to take before surgery.
Dental Evaluation
Although the incidence of infection after knee replacement is very low, an infection can occur if bacteria enter your bloodstream. To reduce the risk of infection, major dental procedures (such as tooth extractions and periodontal work) should be completed before your total knee replacement surgery.
Urinary Evaluations
People with a history of recent or frequent urinary infections should have a urological evaluation before surgery. Older men with prostate disease should consider completing required treatment before undertaking knee replacement surgery.
Your orthopedic surgeon will review the results of your evaluation with you and discuss whether total knee replacement is the best method to relieve your pain and improve your function. Other treatment options — including medications, injections, physical therapy, or other types of surgery — will also be considered and discussed.
In addition, your orthopedic surgeon will explain the potential risks and complications of total knee replacement, including those related to the surgery itself and those that can occur over time after your surgery.
Social Planning
Although you will be able to walk on crutches or a walker soon after surgery, you will need help for several weeks with such tasks as cooking, shopping, bathing, and doing laundry.
If you live alone, your orthopaedic surgeon’s office, a social worker, or a discharge planner at the hospital can help you make advance arrangements to have someone assist you at home. They also can help you arrange for a short stay in an extended care facility during your recovery, if this option works best for you.
Home Planning
Several modifications can make your home easier to navigate during your recovery. The following items may help with daily activities:
- Safety bars or a secure handrail in your shower or bath
- Secure handrails along your stairways
- A stable chair for your early recovery with a firm seat cushion (and a height of 18 to 20 inches), a firm back, two arms, and a footstool for intermittent leg elevation
- A toilet seat riser with arms, if you have a low toilet
- A stable shower bench or chair for bathing
- Removing all loose carpets and cords
- A temporary living space on the same floor because walking up or down stairs will be more difficult during your early recovery
How knee replacement surgery is performed
You’ll usually be admitted to hospital on the day of your knee replacement surgery. The surgeon and anesthetist will usually come and see you to discuss what will happen and answer any questions you have.
Most people would have seen their surgeon at a pre-assessment clinic and had the chance to discuss any relevant details of the knee replacement surgery.
How the knee replacement surgery is carried out
Anesthesia
The most common types of anesthesia are general anesthesia (you are put to sleep) or spinal, epidural, or regional nerve block anesthesia (you are awake but your body is numb from the waist down). The anesthesia team, with your input, will determine which type of anesthesia will be best for you. There’s no need to be anxious about having a general anesthetic: the anesthetist will be by your side the whole time you’re asleep, carefully monitoring you, and will be there when you wake up.
Knee replacement surgery is usually performed either under general anesthetic (you’re asleep throughout the procedure) or under spinal or epidural anesthetic (you’re awake but have no feeling from the waist down).
Knee replacement procedure
The knee replacement procedure itself takes approximately 1 to 3 hours. Your orthopedic surgeon will remove the damaged cartilage and bone in your knee joint, and then position the new metal and plastic implants (a prosthesis), which have been measured to fit, to restore the alignment and function of your knee.
You may have either a total or a half-knee replacement. This will depend on how damaged your knee is. Total knee replacements are the most common.
Total knee replacement
In a total knee replacement (TKR), both sides of your knee joint are replaced. The total knee replacement procedure takes one to three hours:
- Your surgeon makes a cut down the front of your knee to expose your kneecap. This is then moved to the side so the surgeon can get to the knee joint behind it.
- The damaged ends of your thigh bone (femur) and shin bone (tibia) are carefully cut away. The ends are precisely measured and shaped to fit the appropriately sized prosthetic replacement. A dummy joint is positioned to test that the joint is working properly. Adjustments are made, the bone ends are cleaned, and the final prosthesis is fitted.
- The end of your femur is replaced by a curved piece of metal, and the end of your tibia is replaced by a flat metal plate. These are fixed using special bone ‘cement’, or are treated to encourage your bone to fuse with the replacement parts. A plastic spacer is placed between the pieces of metal. This acts like cartilage, reducing friction as your joint moves.
- The back of the knee cap may also be replaced, depending on the reasons for replacement.
- The wound is closed with either stitches or clips and a dressing is applied to the wound. In rare cases a splint is used to keep your leg immobile, but you’re usually encouraged to move your knee as early as possible.
Total knee replacement is a common procedure but you’re still likely to have some difficulty moving, especially bending your knee, and kneeling may be difficult because of the scar.
Partial (half) knee replacement
If only one side of your knee is damaged, you may be able to have a partial (half) knee replacement (PKR). Partial (half) knee replacement is a smaller operation, which uses a smaller incision, and involves less bone being removed. It’s suitable for around one in four people with osteoarthritis.
There are advantages to partial (half) knee replacement including a shorter hospital stay and recovery period. Blood transfusions are also rarely needed. Partial (half) knee replacement often results in more natural movement in the knee and you may be able to be more active than after a total knee replacement.
Talk to your surgeon about the type of surgery they intend to use and why they think it’s the best choice for you.
Other procedures
In some cases, there may be other types of procedure used, including:
Kneecap replacement
If only your kneecap is damaged, an operation called a patellofemoral replacement or patellofemoral joint arthroplasty can be performed. This involves a smaller surgery with a faster recovery time. However, the long-term results are still unclear and it’s not suitable for most people with osteoarthritis.
Mini-incision total knee replacement surgery
This new technique has been recommended by the National Institute for Health and Care Excellence. It can be used for either total or half knee replacements, but is currently more commonly used for partial knee replacements.
The surgeon makes a smaller cut (an incision 10 to 12 cm long over the knee) than in standard total knee replacement surgery which requires an incision 20 to 30 cm long. Specialized instruments are then used to maneuver around the tissue, rather than cutting through it. The same prostheses (knee replacement implants) are inserted using specially designed instruments. This should lead to a quicker recovery.
Image-guided knee replacement surgery
The surgeon performs this operation using computerized images, which are generated by attaching infrared beacons to parts of your leg and to the operating tools. These are tracked on infrared cameras in the operating theater. Results so far suggest that this may enable the new knee joint to be positioned more accurately.
Most hospitals don’t yet have the equipment to do this and only around 1% of knee replacements are performed in this way.
Patient-specific knee replacement
This is a more recent advance in knee replacement surgery. A guide is created using magnetic resonance imaging (MRI) scans. This helps to create the best fitting implant for each patient.
The potential advantage of this procedure is that the implant may last longer, as the most accurate fitting is used. However, as this is a new technique, the results and long-term effects aren’t fully known yet.
After knee replacement surgery
After surgery, you’ll be moved back to the ward (after local anesthetic) or a recovery room (after general anesthetic or epidural), where you’ll be told how the operation went.
You may feel hazy or groggy as you come round from the general anesthetic. A nurse may give you oxygen (through tubes in your nose or a mask) to help you feel better.
In the surgical ward, you may be given a switch that enables you to self-administer painkillers at a safe rate. You may also be given oxygen through a mask or tubes. If necessary, you’ll be given a blood transfusion.
It’s common to feel sick or vomit after you’ve been given general anesthesia. Your nurse may offer you medicine to help with sickness. You may also have a sore throat and dry mouth.
Your blood pressure will be taken regularly. This will either be done by a nurse or by using an automatic cuff that squeezes tightly at regular times. Your temperature will also be taken.
You’ll have a large dressing on your knee to protect your wound. Various drains will syphon off blood from the operation site to prevent it collecting inside the wound.
Your wound dressing will be changed regularly until it’s healed over.
Research shows the earlier you get out of bed and start walking, eating and drinking after your operation, the better.
Your hospital may offer an enhanced recovery programme if you have had major surgery. This rehabilitation programme aims to get you back to full health quickly.
Pain Management
After surgery, you will always feel some pain. This is a natural part of the healing process. Your doctor and nurses will work to reduce your pain, which can help you recover from surgery faster. Tell your nurse as soon as you start to feel any pain so they can give you painkilling medication as soon as possible.
Medications are often prescribed for short-term pain relief after surgery. Many types of medicines are available to help manage pain, including opioids, non-steroidal anti-inflammatory drugs (NSAIDs), and local anesthetics. Your doctor may use a combination of these medications to improve pain relief, as well as minimize the need for opioids.
Be aware that although opioids help relieve pain after surgery, they are a narcotic and can be addictive. Opioid dependency and overdose has become a critical public health issue in the U.S. It is important to use opioids only as directed by your doctor. As soon as your pain begins to improve, stop taking opioids. Talk to your doctor if your pain has not begun to improve within a few days of your surgery.
Blood Clot Prevention
Your orthopedic surgeon may prescribe one or more measures to prevent blood clots and decrease leg swelling. You may be given special support stockings to wear after surgery to help your blood circulation. Your nurse or doctor will explain how you should use these.
Some people are given an injection to thin the blood slightly to help reduce the risk of clots.
Foot and ankle movement also is encouraged immediately following surgery to increase blood flow in your leg muscles to help prevent leg swelling and blood clots. These may be as simple as flexing your knees or ankles and rotating your feet.
The sooner you start to move around, the better. Lying in bed for too long can cause some of your blood to pool in your legs. This puts you at risk of a blood clot.
Physical Therapy
Most patients begin exercising their knee the day after surgery. In some cases, patients begin moving their knee on the actual day of surgery. A physical therapist will teach you specific exercises to strengthen your leg and restore knee movement to allow walking and other normal daily activities soon after your surgery.
To restore movement in your knee and leg, your surgeon may use a knee support that slowly moves your knee while you are in bed. The device is called a continuous passive motion (CPM) exercise machine. Some surgeons believe that a continuous passive motion machine decreases leg swelling by elevating your leg and improves your blood circulation by moving the muscles of your leg.
Figure 7. Continuous passive motion exercise machine

Preventing Pneumonia
It is common for patients to have shallow breathing in the early postoperative period. This is usually due to the effects of anesthesia, pain medications, and increased time spent in bed. This shallow breathing can lead to a partial collapse of the lungs (termed “atelectasis”) which can make patients susceptible to pneumonia. To help prevent this, it is important to take frequent deep breaths. Your nurse may provide a simple breathing apparatus called a spirometer to encourage you to take deep breaths.
How soon will you be up and about?
The nursing staff will help you to get up and walk about as quickly as possible. If you’ve had minimally invasive knee replacement surgery or are on an enhanced recovery programme, you may be able to walk on the same day as your operation. Generally, you’ll be helped to stand within 12-24 hours after your knee replacement operation.
Walking with a frame or crutches is encouraged. Most people are able to walk independently with sticks after about a week but this can vary depending on the individual.
During your stay in hospital, a physiotherapist will teach you exercises to help strengthen your knee. You can usually begin these the day after your operation. It’s important to follow the physiotherapist’s advice to avoid complications or dislocation of your new joint.
It’s normal to experience initial discomfort while walking and exercising, and your legs and feet may be swollen.
You may be put on a passive motion machine to restore movement in your knee and leg. This support will slowly move your knee while you are in bed. It helps to decrease swelling by keeping your leg raised and helps improve your circulation.
Going home
You’ll usually be in hospital for three to five days, depending on what progress you make and what type of knee replacement you have. Patients who have a half knee replacement usually have a shorter hospital stay.
If you’re generally fit and well, the surgeon may suggest an enhanced recovery programme where you start walking on the day of the operation and are discharged within one to three days.
Before you leave hospital, you may (depending on the type of operation you had) have an appointment with a physiotherapist. They’ll be able to advise you about any exercises you need to carry out.
You’ll also be given advice about how to care for your wound, any equipment you may require, such as dressings, bandages, crutches and splints, and maybe a dose of painkillers.
Each hospital will have its own policy and arrangements for discharging patients.
Your discharge will be affected by:
- how quickly your health improves while you’re in hospital
- what support you’ll need after you return home
You may want to ask some questions before you leave hospital, such as:
- Who should I call if I have any concerns once I’m home?
- What should I be trying to do on my own – for example, going to the bathroom and getting out of bed?
- Is there anything I should avoid doing?
- When can I go back to work?
- How much pain, bruising or swelling should I expect when I get home?
- When and where will any stitches be removed?
- Do I need to return to hospital or my doctor for follow-up? If so, when will this be?
The outcome of your operation
It’s important to find out how your operation went.
Here are some questions you may want to ask:
- Was the operation as successful as expected?
- What effect has the operation had on my condition?
- How will I expect to feel when I get home?
- How long will it be before I’m back to normal?
Transport home
You won’t usually be able to drive yourself home after surgery. Instead, you could ask someone to pick you up or take you home in a taxi.
It’s a good idea to have an adult available to help you for at least 24 hours after leaving the hospital.
Knee replacement recovery
Recovery times can vary depending on the individual and type of surgery carried out. It’s important to follow the advice the hospital gives you on looking after your knee.
You’ll usually be in hospital for three to five days, but recovery times can vary depending on the individual and type of surgery being carried out.
Once you’re able to be discharged, your hospital will give you advice about looking after your knee at home. You’ll need to use a frame or crutches at first and a physiotherapist will teach you exercises to help strengthen your knee.
Most people can stop using walking aids around six weeks after surgery, and start driving after about eight to 12 weeks.
Three to six weeks after surgery, you generally can resume most daily activities, such as shopping and light housekeeping. Driving is also possible at around three weeks if you can bend your knee far enough to sit in a car, if you have enough muscle control to operate the brakes and accelerator, and if you’re not still taking narcotic pain medications.
After recovery, you can engage in various low-impact activities, such as walking, swimming, golfing or biking. But you should avoid higher impact activities — such as jogging, skiing, tennis and sports that involve contact or jumping. Talk to your doctor about your limitations.
Full recovery can take up to two years as scar tissue heals and your muscles are restored by exercise. A very small amount of people will continue to experience some pain after two years.
After having a knee replacement surgery, contact your doctor if:
- you develop hot, reddened, hard or painful areas in your legs in the first few weeks after your operation – although this may just be bruising from the surgery, it could mean a blood clot has developed
- you experience chest pains or breathlessness – although it’s very rare, you could have a clot on your lung (pulmonary embolism) which needs urgent treatment
Recovery at Home
The success of your knee replacement surgery will depend largely on how well you follow your orthopedic surgeon’s instructions at home during the first few weeks after surgery.
Don’t be surprised if you feel extremely tired at first. You’ve had a major operation and muscles and tissues surrounding your new knee will take time to heal. Follow the advice of the surgical team and call your doctor if you have any particular worries or queries.
You may be eligible for home help and there may be aids that can help you. You may also want to arrange for someone to help you out for a week or so.
The exercises your physiotherapist gives you are an important part of your recovery. It’s essential you continue with them once you’re at home. Your rehabilitation will be monitored by a physiotherapist.
Wound Care
You will have stitches or staples running along your wound or a suture beneath your skin on the front of your knee. The stitches or staples will be removed several weeks after surgery. A suture beneath your skin will not require removal.
Avoid soaking the wound in water until it has thoroughly sealed and dried. You may continue to bandage the wound to prevent irritation from clothing or support stockings.
Blood Clot Prevention
Follow your orthopedic surgeon’s instructions carefully to reduce the risk of blood clots developing during the first several weeks of your recovery. He or she may recommend that you continue taking the blood thinning medication you started in the hospital. Notify your doctor immediately if you develop any of the following warning signs.
Warning signs of blood clots. The warning signs of possible blood clots in your leg include:
- Increasing pain in your calf
- Tenderness or redness above or below your knee
- New or increasing swelling in your calf, ankle, and foot
Warning signs of pulmonary embolism. The warning signs that a blood clot has traveled to your lung include:
- Sudden shortness of breath
- Sudden onset of chest pain
- Localized chest pain with coughing
Preventing Infection
A common cause of infection following total knee replacement surgery is from bacteria that enter the bloodstream during dental procedures, urinary tract infections, or skin infections. These bacteria can lodge around your knee replacement and cause an infection.
After knee replacement, patients with certain risk factors may need to take antibiotics prior to dental work, including dental cleanings, or before any surgical procedure that could allow bacteria to enter the bloodstream. Your orthopedic surgeon will discuss with you whether taking preventive antibiotics before dental procedures is needed in your situation.
Warning signs of infection. Notify your doctor immediately if you develop any of the following signs of a possible knee replacement infection:
- Persistent fever (higher than 100 °F or 37.8 °C orally)
- Shaking chills
- Increasing redness, tenderness, or swelling of the knee wound
- Drainage from the knee wound
- Increasing knee pain with both activity and rest
An infected knee replacement usually requires surgery to remove the artificial parts and antibiotics to kill the bacteria. After the infection is cleared, another surgery is performed to install a new knee.
Avoiding Falls
A fall during the first few weeks after surgery can damage your new knee and may result in a need for further surgery. Stairs are a particular hazard until your knee is strong and mobile. You should use a cane, crutches, a walker, hand rails, or have someone to help you until you have improved your balance, flexibility, and strength.
Your surgeon and physical therapist will help you decide what assistive aides will be required following surgery and when those aides can safely be discontinued.
Diet
Some loss of appetite is common for several weeks after surgery. A balanced diet, often with an iron supplement, is important to help your wound heal and to restore muscle strength.
Activity
Exercise is a critical component of home care, particularly during the first few weeks after surgery. You should be able to resume most normal activities of daily living within 3 to 6 weeks following surgery. Some pain with activity and at night is common for several weeks after surgery.
Your activity program should include:
- A graduated walking program to slowly increase your mobility, initially in your home and later outside
- Resuming other normal household activities, such as sitting, standing, and climbing stairs
- Specific exercises several times a day to restore movement and strengthen your knee. You probably will be able to perform the exercises without help, but you may have a physical therapist help you at home or in a therapy center the first few weeks after surgery.
You will most likely be able to resume driving when your knee bends enough that you can enter and sit comfortably in your car, and when your muscle control provides adequate reaction time for braking and acceleration. Most people resume driving approximately 4 to 6 weeks after surgery.
Looking after your new knee
- Continue to take any prescribed painkillers or anti-inflammatories to help manage any pain and swelling
- Use your walking aids but aim to gradually decrease the amount you rely on them as your leg feels stronger
- Keep up your exercises to help prevent stiffness and do not force your knee
- Do not sit with your legs crossed for six weeks after your operation
- Do not put a pillow underneath your knee when sleeping as this can result in a permanently bent knee
- Avoid twisting at your knee
- Wear supportive outdoor shoes
- Do not kneel on your operated knee until your surgeon says you can
- Raise your leg when sitting and use ice packs to help with any swelling
How long will it be before I feel normal?
You should be able to stop using your crutches or walking frame and resume normal leisure activities six weeks after surgery. However, it may take up to three months for pain and swelling to settle down. It can take up to a year for any leg swelling to disappear.
Your new knee will continue to recover up to two years after your operation. During this time, scar tissue will heal and muscles will be restored by exercise.
Even after you have recovered, it’s best to avoid extreme movements or sports where there’s a risk of falling, such as skiing or mountain biking. Your doctor or a physiotherapist can advise you.
When can I drive again?
You can resume driving when you can bend your knee enough to get in and out of a car and control the car properly.
This is usually around four to six weeks after your surgery, but check with your physiotherapist or doctor whether it’s safe for you to drive.
When can I go back to work?
This depends on your job, but you can usually return to work six to 12 weeks after your operation.
When can I do housework?
For the first three months, you should be able to manage light chores, such as dusting and washing up.
Avoid heavy household tasks such as vacuuming and changing the beds. Do not stand for long periods as this may cause ankle swelling and avoid stretching up or bending down for the first six weeks.
How will knee replacement affect my sex life?
You may find that having the operation gives your sex life a boost. Your surgeon can advise when you can have sex again. As long as you’re careful, it should be fine after six to eight weeks. Avoid vigorous sex and kneeling positions.
Will I have to go back to the hospital?
You’ll be given an outpatient appointment to check on your progress, usually six to 12 weeks after your knee replacement.
Will I need another new knee?
The knee can be replaced as often as necessary, although results tend to be slightly less effective each time. Recovery may take longer, but once you’ve recovered, results are usually good.





{kind=link}