
Contents
What is ascariasis
Ascariasis is a type of roundworm infection. Ascariasis infection begins when you swallow roundworm eggs. Ascariasis is the most common human worm infection in people worldwide, it is estimated that there are 4 million cases in the United States at any time. Most recorded cases of ascariasis disease in the US are in rural areas of the southeastern United States. An estimated 807 million–1.2 billion people in the world are infected with Ascaris lumbricoides (sometimes called just Ascaris or ascariasis). Infections commonly occur in tropical and sub-tropical areas of the world, including in sub-Saharan Africa, the Americas, China and east Asia. Ascariasis eggs can be present in food or drink, or in the soil in which food has grown. Eating food grown in contaminated soil can expose you to infection. You may also become infected if you touch contaminated soil with your hands and then eat without first washing them. Contaminated soil or stools can also contaminate the water, making it possible to develop a roundworm infection by drinking contaminated water.
Most infected people have mild cases with no symptoms. But heavy ascariasis infestation can lead to serious symptoms and complications. Ascariasis, hookworm, and whipworm are parasitic worms known as soil-transmitted helminths. It’s estimated that about a quarter (24%) of the world’s population currently has a soil-transmitted worm infection.
The larvae and adult ascariasis worms live in the small intestine and can cause intestinal disease.These worms are parasites that use your body as a host to mature from larvae or eggs to adult worms (see ascariasis lifecycle in Figure 7 below). Adult ascariasis worms, which reproduce, can be more than a foot (30 centimeters) long.
Ascariasis occurs most often in children in tropical and subtropical regions of the world — especially in areas with poor sanitation and hygiene.
Ascariasis infection is more common in warm climates. Eggs are passed in the stool of infected animals or human and contaminate the soil. Ingestion of contaminated soil then leads to ascariasis infection.
- Ascariasis (Ascaris lumbricoides) infection is one of the most common intestinal worm infections. It is found in association with poor personal hygiene, poor sanitation, and in places where human feces are used as fertilizer. The geographic distributions of Ascaris lumbricoides are worldwide in areas with warm, moist climates and are widely overlapping. Infection occurs worldwide and is most common in tropical and subtropical areas where sanitation and hygiene are poor.
- Ascariasis caused by pig ascariasis (Ascaris suum) is found in association with pigs. People who raise pigs or use raw pig manure as fertilizer may be at risk for infection with Ascaris suum. Contact with pigs should be investigated as a potential cause upon diagnosis of ascariasis.
Ascaris parasites live in the lumen of the small intestine and Ascaris eggs are passed in the feces (poop) of infected people. If an infected person defecates outside (for example, near bushes, in a garden, or in a field), or if the feces of an infected person are used as fertilizer, eggs are deposited on soil. The eggs can then mature into a form of the parasite that is infective. Ascariasis is caused by ingesting eggs. This can happen when hands or fingers that have contaminated dirt on them are put in the mouth, or by consuming vegetables or fruits that have not been carefully cooked, washed, or peeled.
People infected with ascariasis often show no symptoms. If symptoms do occur they can be light and include abdominal discomfort. Heavy worm infections can cause intestinal blockage and impair growth in children. Migrating adult worms may cause symptomatic occlusion of the biliary tract (biliary ascariasis) or oral expulsion. Other symptoms such as cough are due to migration of the worms through the body. During the lung phase of larval migration, pulmonary symptoms can occur (cough, dyspnea [shortness of breath], hemoptysis [coughing up blood], eosinophilic pneumonitis – Loeffler’s syndrome).
Humans can also be infected by pig roundworm (Ascaris suum). Ascaris lumbricoides (human roundworm) and Ascaris suum (pig roundworm) are indistinguishable. It is unknown how many people worldwide are infected with Ascaris suum. Ascariasis caused by Ascaris suum is found in association with pigs. People who raise pigs or use raw pig manure as fertilizer may be at risk for infection with Ascaris suum. Many infected pigs do not have any symptoms at all and people may not be aware that their pigs are infected. Contact with pigs should be investigated as a potential cause of ascariasis upon diagnosis in humans.
The standard method for diagnosing ascariasis is by identifying Ascaris eggs in a stool sample using a microscope. Because eggs may be difficult to find in light infections, a concentration procedure is recommended.
Ascariasis is treatable with medication prescribed by your health care provider.
Ascariasis disease
People infected with Ascaris often show no symptoms, regardless of the species of worm. If symptoms do occur they can be light and include abdominal discomfort. Heavy infections can cause intestinal blockage and impair growth in children. Other symptoms such as cough are due to migration of the worms through the body. Ascariasis is treatable with medication prescribed by your health care provider.
How can I prevent ascariasis infection?
- Avoid contact with soil that may be contaminated with human feces, including with human fecal matter (“night soil”) used to fertilize crops.
- Wash your hands with soap and warm water before handling food.
- Teach children the importance of washing hands to prevent infection.
- Wash, peel, or cook all raw vegetables and fruits before eating, particularly those that have been grown in soil that has been fertilized with manure.
Transmission of ascariasis infection to others can be prevented by:
- not defecating outdoors, and by
- effective sewage disposal systems.
Figure 1. Ascaris egg

Figure 2. Ascaris larva

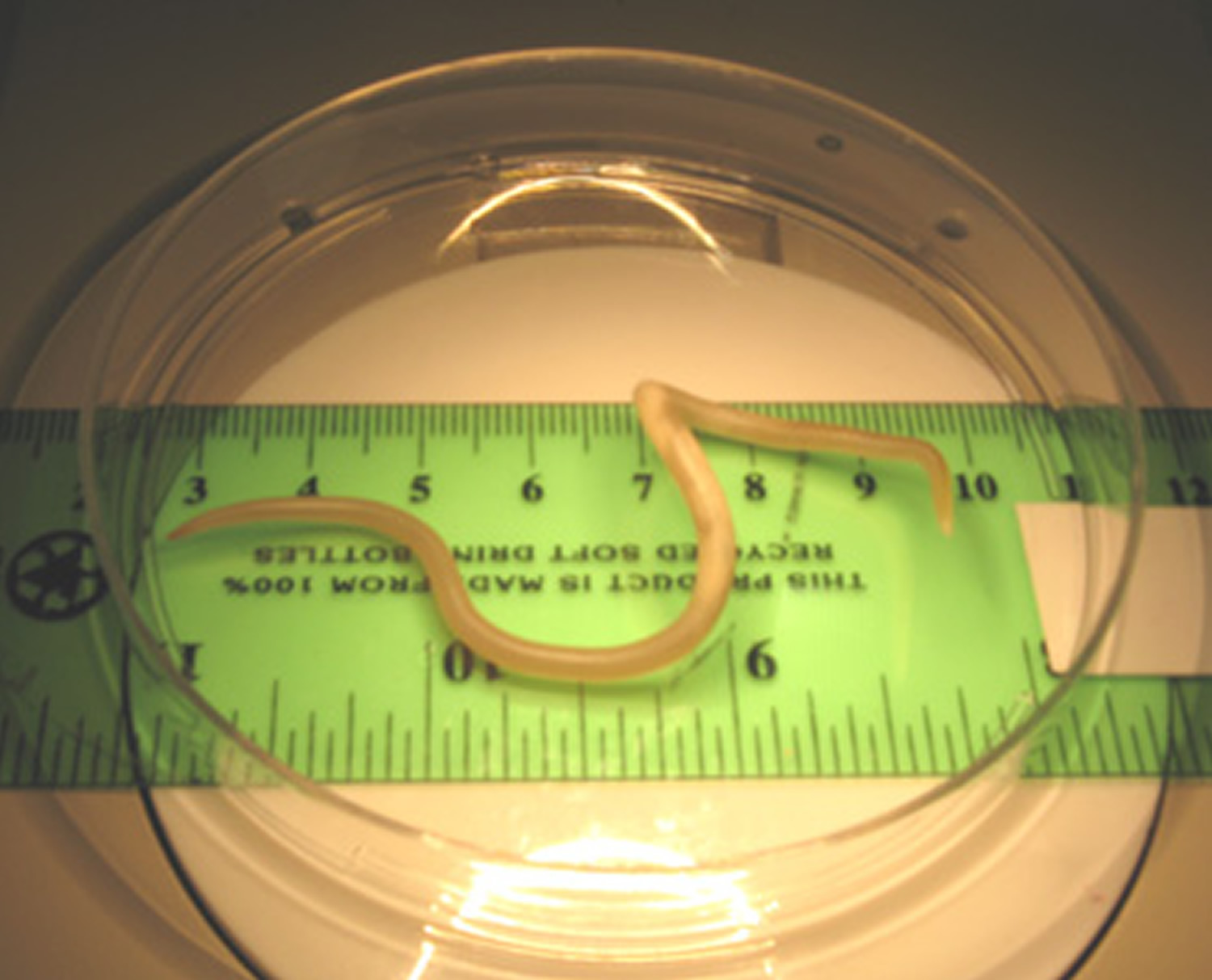
Figure 3. Ascaris adult worm (adult females: 20 to 35 cm; adult male: 15 to 30 cm.)
How is ascariasis spread or transmitted to humans?
Ascariasis isn’t spread directly from person to person. Instead, a person has to come into contact with soil mixed with human or animal feces that contain ascariasis eggs or infected water. Ascariasis is caused by ingesting infective eggs. This can happen when hands or fingers that have contaminated dirt on them are put in the mouth or by consuming vegetables or fruits that have not been carefully cooked, washed or peeled.
Ascaris lives in the small intestine and Ascaris eggs are passed in the feces of infected persons. If the infected person defecates outside (near bushes, in a garden, or field), or if the feces of an infected person are used as fertilizer, then eggs are deposited on the soil. In many developing countries, human feces are used for fertilizer, or poor sanitary facilities allow human waste to mix with soil in yards, ditches and fields.
Small children often play in dirt, and infection can occur if they put their dirty fingers in their mouths. Unwashed fruits or vegetables grown in contaminated soil also can transmit the ascariasis eggs.
Life cycle of a ascariasis worm
- Ingestion. The microscopic ascariasis eggs can’t become infective without coming into contact with soil. People can accidentally ingest contaminated soil through hand-to-mouth contact or by eating uncooked fruits or vegetables that have been grown in contaminated soil.
- Migration. Larvae hatch from the eggs in your small intestine and then penetrate the intestinal wall to travel to your lungs via your bloodstream or lymphatic system. After maturing for about a week in your lungs, the larvae break into your airway and travel up your throat, where they’re coughed up and swallowed.
- Maturation. Once back in the intestines, the parasites grow into male or female worms. Female worms can be more than 15 inches (40 centimeters) long and a little less than a quarter inch (6 millimeters) in diameter. Male worms are generally smaller.
- Reproduction. Male and female worms mate in the small intestine. Female worms can produce 200,000 eggs a day, which leave your body in your feces. The fertilized eggs must be in soil for at least 18 days before they become infective.
The whole process — from egg ingestion to egg deposits — takes about two or three months. Ascariasis worms can live inside you for a year or two.
Risk factors for ascariasis
Risk factors for ascariasis include:
- Age. Most people who have ascariasis are 10 years old or younger. Children in this age group may be at higher risk because they’re more likely to play in dirt.
- Warm climate. In the United States, ascariasis is more common in the Southeast, but it’s more prevalent in developing countries with warm temperatures year-round.
- Poor sanitation. Ascariasis is widespread in developing countries where human feces are allowed to mix with local soil.
Ascariasis from pigs
Ascaris suum (pig ascariasis) is an intestinal parasite of pigs that can also infect people.
How is pig ascariasis spread to humans?
The adult Ascaris suum worm lives in the pig’s intestines and produces eggs that are passed in the pigs’ feces (manure). These eggs are deposited into the soil wherever the pig defecates. The eggs require days to weeks in the environment to become infective. Ascaris suum infection is caused by ingesting these infective eggs. This happens when:
- People don’t wash their hands thoroughly after handling pigs, cleaning pig pens, or handling pig manure; and
- People consume fruits or vegetables grown in gardens fertilized with pig manure or in soil where pigs have previously been kept and that have not been carefully cooked, washed, or peeled.
Pig ascariasis (ascaris suum) is not transmitted to people by eating pork or pork products because the worm eggs are not found in the meat.
How do I know if my pigs are infected with pig ascariasis?
Many infected pigs do not show any symptoms. Heavily infected pigs may have symptoms including the following:
- Difficulty breathing, sometimes called “thumps”
- Weight loss
- Unthrifty (not strong or healthy)
- Slow weight gain
- Possibly passing whole worms in manure
A veterinarian can take a fecal sample from your pig(s) and look for evidence of roundworm infection. A veterinarian can also prescribe deworming medications for your pigs if they are infected.
Who is at risk for infection with pig ascariasis?
People who raise pigs or use raw pig manure as fertilizer may be at risk for infection with Ascaris suum.
How can I prevent infection with pig ascariasis?
- Avoid contact with soil that may be contaminated with pig feces, including soil where pig manure has been used to fertilize crops.
- Wash your hands with soap and water after handling pigs, cleaning pig pens, or handling pig manure, and always before handling food.
- Teach children the importance of washing hands to prevent infection. Supervise children around pigs, ensuring that they do not put unwashed hands or other potentially contaminated objects in their mouths.
- Wash, peel, or cook all raw vegetables and fruits before eating, particularly those that have been grown in soil that has been fertilized with pig manure.
Consult a veterinarian for recommendations on preventing and controlling Ascaris suum in your pigs.
Biliary and hepatic ascariasis
Hepato-biliary ascariasis (hepatic and biliary ascariasis) one type of human ascariasis and seen more commonly now in the endemic zones due to the frequent usage of ultrasonograms and endoscopic diagnostic procedures in the clinical practice 1). Even then, the magnitude of the problem was probably underestimated because the worms move in and out of the bile ducts actively from the duodenum and therefore many would have been absent from the biliary tree at the time of surgery 2). Ascaris lumbricoides has a natural inclination to migrate and seek small orifices 3). Heavy worm infestation or other intestinal infections of viral, bacterial or parasitic origin (leading to altered gut motility) are the usual pre-requisites to reach the duodenum from their natural habitat-the jejunum. However, host reaction to an adult worm can by itself alter the vasomotor reflexes and secretory responses which in turn affect the intestinal tone and motility 4). From the duodenum, it can enter the ampulla of Vater to lodge: (a) In the ampulla itself (b) the common bile duct or (c) the hepatic ducts or anywhere in the biliary tree. It can also enter the orifice of the cystic duct and block it while traversing the common bile duct, but relatively rarely enters the gall-bladder or the pancreatic duct.
There are a variety of manifestations in hepatic and biliary ascariasis and diagnosis depends on a high index of suspicion in endemic areas coupled with subsequent confirmation by sonographic or endoscopic demonstration of the worm. Most of them present with acute abdomen and jaundice caused by common bile duct obstruction and stricture 5). Oriental or recurrent pyogenic cholangiopathy is possibly the result of hepatic and biliary ascariasis, commonly encountered in South-East Asian countries. In Indian studies from Kashmir, at highly endemic area, ascariasis was found to be the cause in 36.7% cases of 109 patients with proven biliary and pancreatic disorders 6). Hepatic and biliary ascariasis is quite frequently seen in children in South Africa while in Philippines, 20% of all biliary diseases are reported to be due to dead or live worms 7). However in one series from Middle-East, there were only two cases of biliary ascariasis found in 668 Jordanian patients evaluated by endoscopic retrograde cholangiopancreatography (ERCP) for biliary/pancreatic disease and unexplained upper abdominal pain 8).
There is a female preponderance (F:M ratio of 3:1) in hepatic and biliary ascariasis as studies have shown higher prevalence of roundworm infestation in females 9). Hepatic and biliary ascariasis is commonly seen in the mid-thirties with a range of 4-70 years 10). Hepato-biliary ascariasis is less common in children because they tend to present more with intestinal rather than biliary obstruction. This may partly be due to very small caliber of the biliary system in children 11). Persons who may be at a greater risk of developing hepatic and biliary ascariasis include:
- a) Those who had prior biliary surgery (cholecystectomy, choledocholithotomy, sphincteroplasty, endoscopic sphincterotomy 12).
- b) Pregnant when compared with non-pregnant women 13) probably owing to hormonal effects on the ampula during the pregnancy.
- c) Disturbance of the environment around the worm e.g., fever, anesthetics and tetrachlorethylene 14).
Figure 4. Gallbladder location
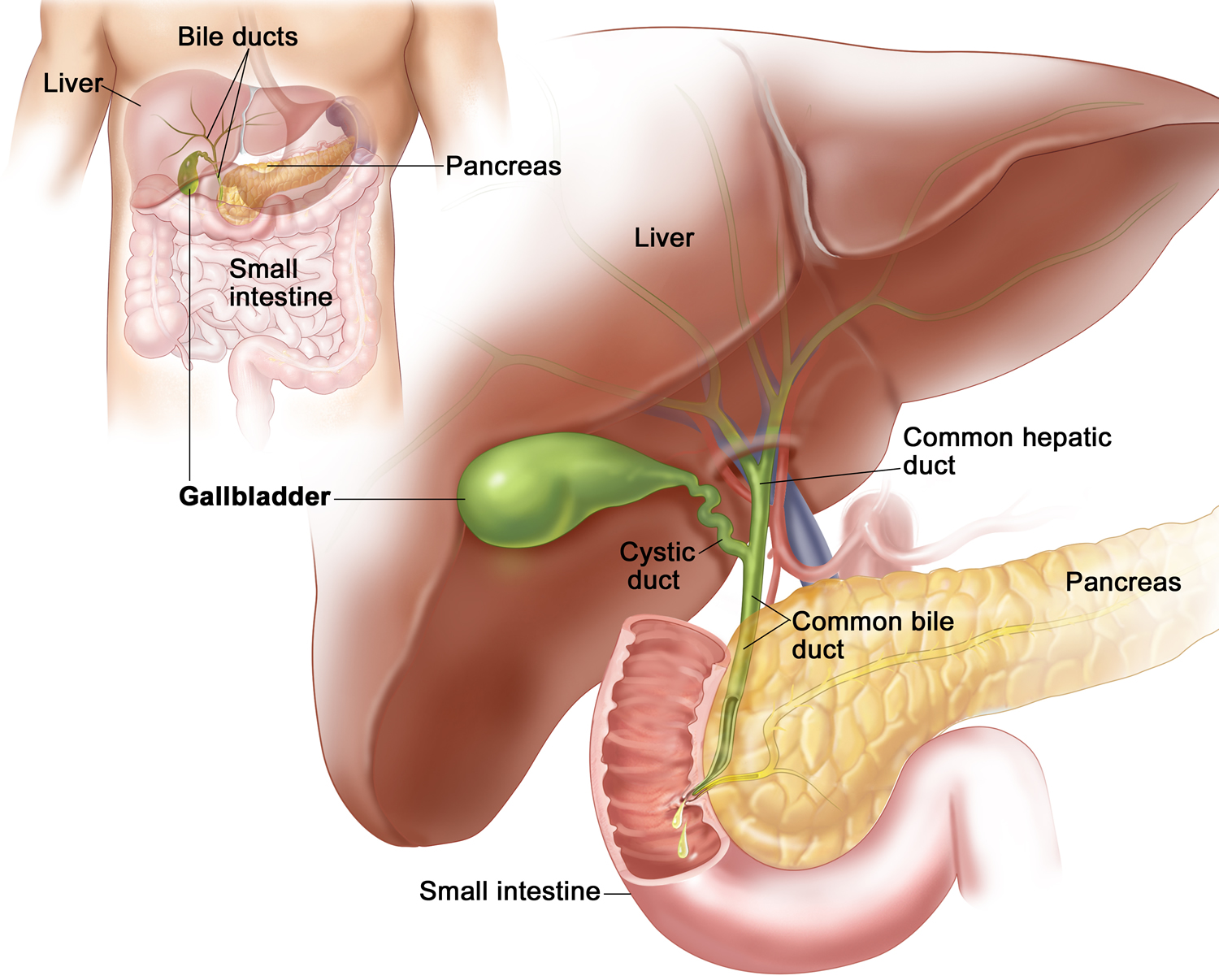
Figure 5. Bile duct anatomy
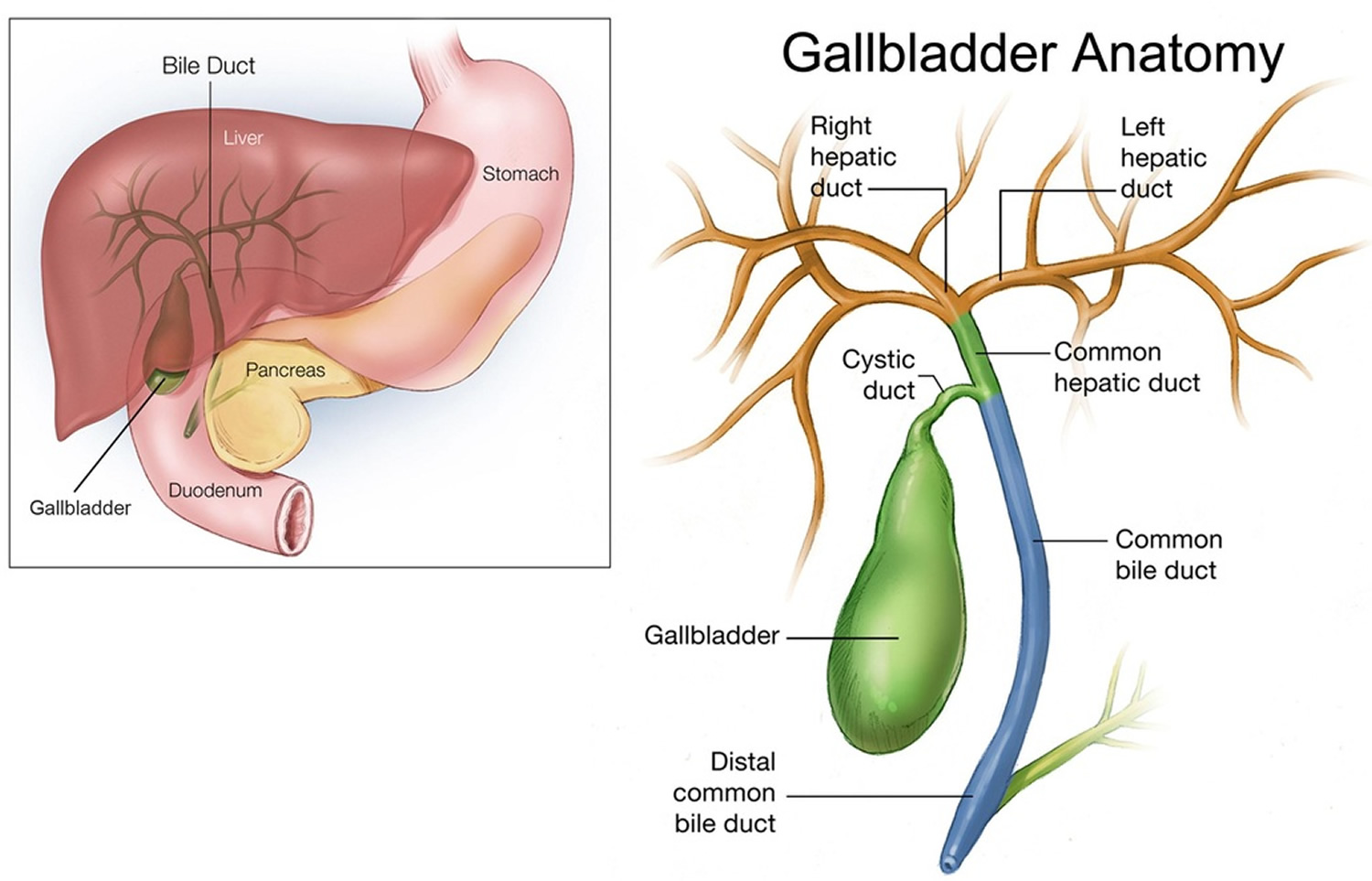
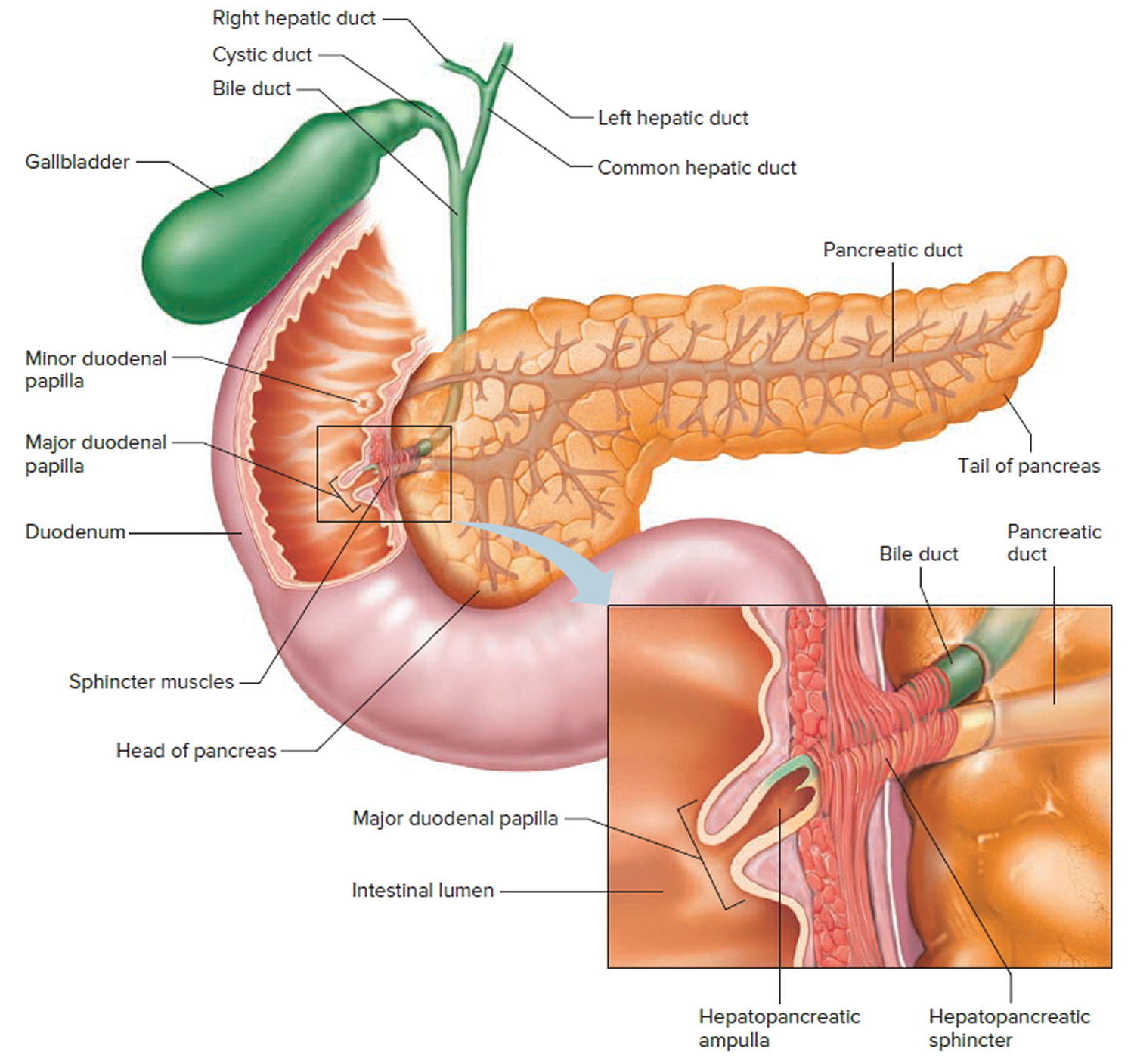
Figure 6. The common bile duct is closely associated with the pancreatic duct and the duodenum
Hepatic and biliary ascariasis signs and symptoms
- Biliary colic in hepatic and biliary ascariasis presents as acute onset right hypochondrial pain which may be recurrent or continuous lasting a few days. It occurs due to entry of the worm into the ampullary orifice from the duodenum. Cholangitic features such as shaking chills, fever and mild jaundice are seen only occasionally.
- Acute cholangitis in hepatic and biliary ascariasis is an emergency 15), presenting with high grade fever, chill, icterus and upper abdominal pain. On examination, there is hypotension, tender hepatomegaly, leucocytosis, raised bilirubin (mostly conjugated) and raised liver enzymes – especially serum alanine aminotransferase and alkaline phosphatase. Those going on to develop pyogenic cholangitis, pus forms, which may be seen at the ampullary orifice or can be aspirated by ERCP.
- Acute cholecystitis is suspected by right hypochondrial pain and guarding, vomiting and fever. The pain may be referred to the interscapular area or the tip of the right shoulder. Tenderness and a palpable mass in the right hypochondrium may be present. The temperature is usually of low grade and there is no shock. The gall-bladder reveals thickened wall with distension and biliary sludge is usually found 16).
- Hepatic abscess may be solitary or multiple and contains pus. There is tender hepatomegaly, high fever, intercostal tenderness and edema along with right hypochondrial pain. These abscesses may result from dead ova released by female worms migrating up the common bile duct, producing a granulomatous inflammatory reaction with subsequent breakdown with eosinophil infiltration. It may be commoner in children 17).
- Recurrent pyogenic cholangitis. This condition was first described in 1954 in Hong Kong and is also called “Asiatic or Oriental cholangio-hepatitis” and is seen commonly in Hong Kong, Taiwan, South China, Korea and South East Asia 18). It is also increasingly being seen in the west, and is probably a result of the migration of Oriental Nationals to these countries 19). It is characterized by biliary sludge, intrahepatic bile duct stones and chronic secondary bacterial infection. The subjects are thin, young and occasionally malnourished. Recurrent upper abdominal pain, cholestatic jaundice and fever with chill are characteristic and the frequency of such recurrent attacks increase over time. Cholangiograms will demonstrate both the intra and extra hepatic biliary tree to be filled with soft “biliary mud”. The biliary radicles are dilated with excessive branching and single or multiple biliary strictures of variable length 20). In many patients with severe distortion of biliary ducts, recurrent episodes of cholangitis appear to be self-perpetuating in absence of active ascariasis. In longstanding cases, hepatic abscess and scarring may result 21). This is exacerbated by recurrent biliary sepsis as a result of papillitis and sphincter of Oddi motor dysfunction which is probably related to the mechanical injury of the papilla caused by the worm invading the orifice 22). In addition, there is a breakdown of normal defense mechanisms and the enteric bacterial flora may reach the intrahepatic bile tree via the portal system 23). recurrent pyogenic cholangitis and ascariasis shows similar geographical distribution 24) and over 5% of hepatic and biliary ascariasis develop recurrent pyogenic cholangitis after 2 or more years. Stones are common in recurrent pyogenic cholangitis (90% cases) and 50% occur in CBD or common hepatic ducts whereas 15% of them have stones in the gall-bladder 25). Conversely 10% of recurrent pyogenic cholangitis have a definite evidence of ascariasis 26).The stones in recurrent pyogenic cholangitis are pigment stones with layers of bilirubinates deposited on top of a nidus. More importantly, the nidus of biliary stones in 72% of recurrent pyogenic cholangitis is formed by part or whole of Ascaris worm which confirms the significant role of this helminth in cholelithiasis 27). All these strongly imply that hepatic duct stones found in recurrent pyogenic cholangitis may be an aftermath of biliary damage by biliary ascariasis especially recurrent, frequent in endemic zones.
Hemobilia can very rarely occur as a result of biliary ascariasis 28).
Hepatic and biliary ascariasis diagnosis
The diagnosis depends upon demonstrating the worm in the biliary tree in a clinical set-up compatible with the conditions described above, especially in an endemic zone. This is not always easy because frequently most of the worms move in and out of the ducts within 7 days 29). Ultrasonography is a highly sensitive and specific in visualizing a worm in the biliary system, as well as monitoring its mobility to and from the ducts over time. Ascariasis worm, which has not changed its position after 10 days in the duct system, is usually a dead and macerated one. The drawback of ultrasonography is in not being able to detect worms in the duodenum or the ampullary orifice and thereby has been reported to miss up to 50% cases of hepatic and biliary ascariasis 30). ERCP (Endoscopic Retrograde Cholangio-Pancreatography) is helpful in these situations both for diagnostic and therapeutic aspects 31). ERCP is a procedure that enables your physician to examine the pancreatic and bile ducts. A bendable, lighted tube (endoscope) about the thickness of your index finger is placed through your mouth and into your stomach and first part of the small intestine (duodenum). Ascariasis worms appear commonly as linear, smooth filling defects with or without characteristic movements but without distal acoustic shadowing, and may also be seen as parallel filling defects “Railway tract” sign 32), curved defects or transverse loops across the ducts 33). Worms in the gall-bladder appear as long tubular coiled echogenic structure which may be rapidly mobile and is easier to diagnose than biliary ductal ascariasis 34). Computed tomography (CT) will reveal the worms as cylindrical structures 35). Sometimes CT may be used for better visualization of the dilated ductal system 36).
Stool examination may show Ascaris eggs in stool. Many a times the patient passes an adult worm with vomitus or with stool.
Peripheral eosinophilia, due to larval invasion of the blood, is very common 37). Aspiration of the pus from hepatic abscesses may reveal Ascaris ova 38) because larval stages or the ovas are more likely to produce inflammation leading to granulomatous necrosis than adult worms 39).
Although antibodies against ascariasis develop in infected persons, they are not of much help in the immuno-diagnosis, owing to extensive cross-reactivity with other helminthic antigen 40).
Hepatic and biliary ascariasis treatment
The patients with hepatic and biliary ascariasis are to be hospitalized without delay because in them the worm load is usually high. In addition, co-existing mechanical intestinal obstruction are common (especially in young children) but may also follow deworming during or after institution of treatment. It must be remembered that excretion products of the worms can cause marked bowel contraction 41). Similarly, associated acute pancreatitis may complicate the clinical course and there is a definite mortality risk in those with hemorrhagic pancreatitis 42).
Pure biliary ascariasis have a negligible mortality <2% 43). The principles of treatment of biliary ascariasis are 44):
- Treatment of cholangitis or cholecystitis by conservative means.
- Oral administration of anthelminthics, which allows the paralyzed worms to be expelled by normal intestinal activity.
- Endoscopic and Surgical treatment.
Coexistent obstructive jaundice and intestinal obstruction in documented cases of hepatic and biliary ascariasis is usually an indication for surgery 45).
Conservative treatment includes broad-spectrum antibiotics, analgesics, intravenous fluid and electrolytes and most of the acute acalculous cholecystitis patients recover without any complications 46). However in acute pyogenic cholangitis, more specific antibiotics are indicated depending on the biliary pus culture and sensitivity results. The pus is obtained by duodenoscopy or ERCP from the pus points in the papillary orifice or bile aspiration respectively. Other common therapeutic measures to treat endotoxic shock are also to be instituted including correction of metabolic acidosis. However most of them require some form of interventional treatment to improve morbidity and mortality.
Chemotherapy: An ideal antihelminth should be 47):
- Safe at high therapeutic dosage,
- Inexpensive, easily available and easy to administer orally,
- Stable and effective for a long time in different climatic conditions.
Oral anthelminths act by paralyzing the adult worm but none can affect the larval stage. They are administered only if the patient has passed flatus or feces. The worm clearance is usually completed by 3 days in most cases depending on the gut transit time, pre-existing diarrhea and worm load 48). Preferably a soluble preparation is given 49). Direct instillation of anthelminthic e.g., piperazine citrate in the biliary tree surgico-endoscopically is not helpful and is not recommended 50). Treatment failure may occasionally occur and persistent eosinophilia should alert one to this possibility 51). The names, dosage and important contraindications are mentioned in Table 1 52).
Table 1. Efficacy of anti-ascarial drugs with their mode of action
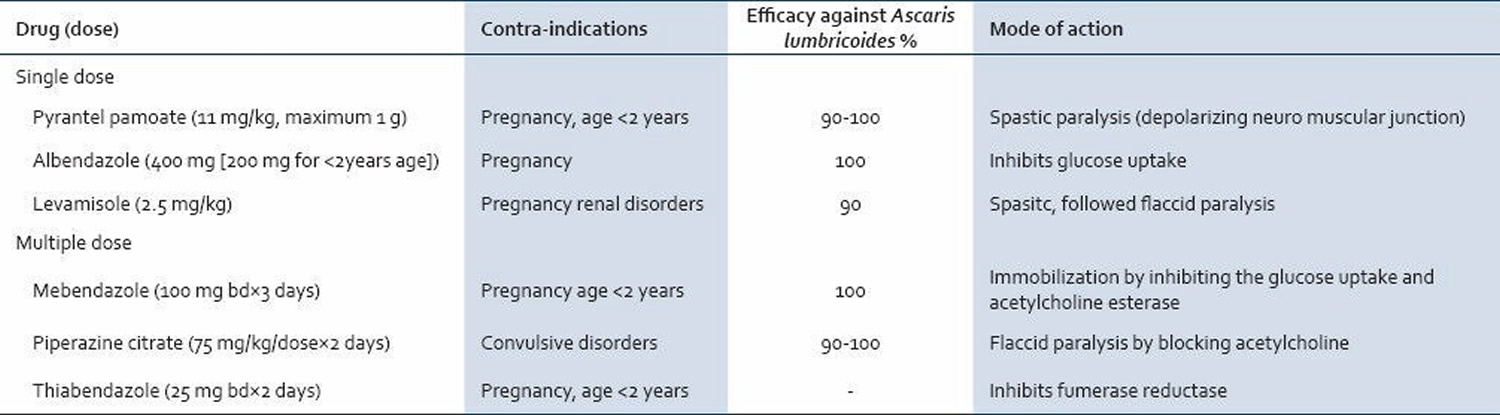
Endoscopic and surgical interventions are indicated when patients do not respond to energetic conservative treatment within few days after hospitalization or when the worm is not expelled from the biliary tree after 3 weeks despite vermifuge 53). Acute pyogenic cholangitis needs biliary decompression or drainage in most cases 54). According to some, cholangitis with biliary strictures or with worms in the gall-bladder are also indications for surgery 55). Endoscopic worm extraction from ampullary orifice rapidly relieves the symptoms in biliary colic 56). This may also be necessary in acute pyogenic cholangitis as an urgent measure. In almost 100% cases, endoscopic worm extraction from the ampulla is successful and from the bile ducts in 90% cases by using the endoscopic basket. The complications of endoscopic procedures in such cases are low (6%) consisting mainly of hypotension and cholangitis 57). Therefore endoscopic extraction of the worms by snares, dormia basket or biopsy forceps is becoming the treatment of choice in biliary ascariasis 58).
Percutaneous needle drainage under ultrasound guidance or rarely surgically is necessary in hepatic abscesses which are large.
Gall-bladder ascariasis usually requires cholecystectomy; but as a whole it is encountered less frequently than bile duct ascariasis 59). Laparotomy is indicated if ERCP is not available for worm extraction in the patients who deteriorate during hospitalization. It must be remembered that acute pancreatitis, intestinal obstruction with complications (like volvulus, gangrene or perforation) may be present alongwith HBA which can be identified on hospitalization by ultrasonographic and biochemical studies.
In recurrent pyogenic cholangitis, recurrent cholangitis with obstructing stones may be managed by placing a Roux-en-Y jejunal conduit for biliary access 60).
Ascariasis lifecycle
Ascaris lumbricoides is the largest roundworm (nematode) parasitizing the human intestine.
- Adult worms, live in the lumen of the small intestine. A female may produce approximately 200,000 eggs per day, which are passed with the feces.
- Unfertilized eggs may be ingested but are not infective. Fertile eggs embryonate and become infective after 18 days to several weeks.
- Depending on the environmental conditions (optimum: moist, warm, shaded soil).
- After infective eggs are swallowed.
- After one to two weeks, the eggs will hatch into larvae. The larvae invade the intestinal mucosa into your bloodstream and are carried via the portal, then systemic circulation to the lungs.
- The larvae mature further in the lungs (10 to 14 days), penetrate the alveolar walls, ascend the bronchial tree to the throat where they’re swallowed.
- Upon reaching the small intestine, they develop into adult worms. Between 2 and 3 months are required from ingestion of the infective eggs to oviposition by the adult female (it takes 60 to 70 days from the initial ingestion of eggs to the production of new ones). Adult worms can live 1 to 2 years.
Figure 7. Ascariasis lifecycle
Ascariasis prevention
The best defense against ascariasis is good hygiene and common sense. Follow these tips to avoid infection:
- Practice good hygiene. Before handling food, always wash your hands with soap and water. Wash fresh fruits and vegetables thoroughly.
- Use care when traveling. Use only bottled water, and avoid raw vegetables unless you can peel and wash them yourself. As a rule, eat only foods that are cooked and hot.
Transmission of ascariasis infection to others can be prevented by:
- not defecating outdoors, and by
- effective sewage disposal systems.
Preventive treatment
In developing countries, groups at higher risk for soil-transmitted helminth infections (hookworm, ascariasis, and whipworm) are often treated without a prior stool examination. Treating in this way is called preventive treatment (or “preventive chemotherapy”). The high-risk groups identified by the World Health Organization are preschool and school-age children, women of childbearing age (including pregnant women in the 2nd and 3rd trimesters and lactating women) and adults in occupations where there is a high risk of heavy infections. School-age children are often treated through school-health programs and preschool children and pregnant women at visits to health clinics.
What is mass drug administration?
The soil-transmitted helminths (hookworm, Ascaris, and whipworm) and four other “neglected tropical diseases” (river blindness, lymphatic filariasis, schistosomiasis and trachoma) are sometimes treated through mass drug administrations. Since the drugs used are safe and inexpensive or donated, entire risk groups are offered preventive treatment. Mass drug administrations are conducted periodically (often annually), commonly with drug distributors who go door-to-door. Multiple neglected tropical diseases are often treated simultaneously using mass drug administrations.
Ascariasis symptoms
Ascariasis symptoms in humans
Most people infected with ascariasis have no symptoms. Moderate to heavy infestations cause various symptoms, depending on which part of your body is affected.
Ascariasis in the lungs
After you ingest the microscopic ascariasis eggs, they hatch in your small intestine and the larvae migrate through your bloodstream or lymphatic system into your lungs. Symptoms usually begin 4-16 days after swallowing the eggs and last up to three weeks. At this stage, you may experience signs and symptoms similar to asthma or pneumonia, including:
- Fever (high temperature) of 38 °C (100.4 °F) or above
- Persistent cough
- Shortness of breath
- Wheezing
It’s unclear why some people develop these symptoms while others don’t.
After spending six to 10 days in the lungs, the larvae travel to your throat, where you cough them up and then swallow them.
Ascariasis in the intestines
The larvae mature into adult worms in your small intestine, and the adult worms typically live in the intestines until they die.
In mild or moderate ascariasis, the intestinal infestation can cause:
- Vague abdominal pain
- Nausea and vomiting
- Diarrhea or bloody stools
If you have a large number of ascariasis worms in your intestine, you might have:
- Severe abdominal pain
- Fatigue
- Vomiting
- Weight loss or malnutrition
- A worm in your vomit or stool
These symptoms are caused by adult worms living in the intestine. The worms can’t reproduce inside you. There will only be as many worms as the eggs you first ingested (see the life cycle of ascariasis).
However, most people have no symptoms.
If your intestines are blocked due to a large number of worms, you will probably experience vomiting and severe abdominal pain.
Ascariasis complications
Mild cases of ascariasis usually don’t cause complications. If you have a heavy infestation, potentially dangerous complications may include:
- Slowed growth. Loss of appetite and poor absorption of digested foods put children with ascariasis at risk of not getting enough nutrition, which can slow growth.
- Intestinal blockage and perforation. In heavy ascariasis infestation, a mass of worms can block a portion of your intestine, causing severe abdominal cramping and vomiting. The blockage can even perforate the intestinal wall or appendix, causing internal bleeding (hemorrhage) or appendicitis.
- Duct blockages. In some cases, worms may block the narrow ducts of your liver (bile duct obstruction) or pancreas, causing severe pain.
Ascariasis diagnosis
In heavy infestations, it’s possible to find worms after you cough or vomit, and the worms can come out of other body openings, such as your mouth or nostrils. If this happens to you, take the worm to your doctor to identify it and prescribe the proper treatment.
Health care providers can diagnose ascariasis by taking a stool sample and using a microscope to look for the presence of eggs.
Stool tests
Mature female ascariasis worms in your intestine begin laying eggs. These eggs travel through your digestive system and eventually can be found in your stool.
To diagnose ascariasis, your doctor will examine your stool for the microscopic eggs and larvae. But eggs won’t appear in stool until at least 40 days after you’re infected. And if you’re infected with only male worms, you won’t have eggs.
Microscopic identification of eggs in the stool is the most common method for diagnosing intestinal ascariasis. The recommended procedure is as follows:
- Collect a stool specimen.
- Fix the specimen in 10% formalin.
- Concentrate using the formalin–ethyl acetate sedimentation technique
- Examine a wet mount of the sediment.
Where concentration procedures are not available, a direct wet mount examination of the specimen is adequate for detecting moderate to heavy infections. For quantitative assessments of infection, various methods such as the Kato-Katz can be used. Larvae can be identified in sputum or gastric aspirate during the pulmonary migration phase (examine formalin-fixed organisms for morphology). Adult worms are occasionally passed in the stool or through the mouth or nose and are recognizable by their macroscopic characteristics.
Blood tests
Your blood can be tested for the presence of an increased number of a certain type of white blood cell, called eosinophils. Ascariasis can elevate your eosinophils, but so can other types of health problems.
Imaging tests
- X-rays. If you’re infested with worms, the mass of worms may be visible in an X-ray of your abdomen. In some cases, a chest X-ray can reveal the larvae in your lungs.
- Ultrasound. An ultrasound may show worms in your pancreas or liver. This technology uses sound waves to create images of internal organs.
- CT scans or MRIs. Both types of tests create detailed images of your internal structures, which can help your doctor detect worms that are blocking ducts in your liver or pancreas. CT scans combine X-ray images taken from many angles; MRI uses radio waves and a strong magnetic field.
Treatment of ascariasis in humans
Typically, only infections that cause symptoms need to be treated. In some cases, ascariasis will resolve on its own.
Ascariasis is treated with anti-parasite medications – albendazole, mebendazole, or ivermectin. Dosage is the same for children as for adults. Albendazole should be taken with food. Ivermectin should be taken on an empty stomach with water. Albendazole is not FDA-approved for treating ascariasis, and the safety of ivermectin for treating children who weigh less than 15 kg has not been established. These medications, taken for one to three days, kill the adult worms. Side effects include mild abdominal pain or diarrhea.
| Drug | Dosage |
|---|---|
| Albendazole | 400 mg orally once |
| Mebendazole | 100 mg orally twice daily for 3 days or 500 mg orally once |
| Ivermectin | 150-200 mcg/kg orally once |
* Oral albendazole is available for human use in the United States.
* Mebendazole is available in the United States only through compounding pharmacies.
* Oral ivermectin is available for human use in the United States.
Albendazole
Treatment in Pregnancy
Albendazole is pregnancy category C. Data on the use of albendazole in pregnant women are limited, though the available evidence suggests no difference in congenital abnormalities in the children of women who were accidentally treated with albendazole during mass prevention campaigns compared with those who were not. In mass prevention campaigns for which the World Health Organization (WHO) has determined that the benefit of treatment outweighs the risk, WHO allows use of albendazole in the 2nd and 3rd trimesters of pregnancy. However, the risk of treatment in pregnant women who are known to have an infection needs to be balanced with the risk of disease progression in the absence of treatment.
Pregnancy Category C: Either studies in animals have revealed adverse effects on the fetus (teratogenic or embryocidal, or other) and there are no controlled studies in women or studies in women and animals are not available. Drugs should be given only if the potential benefit justifies the potential risk to the fetus.
Treatment During Lactation
It is not known whether albendazole is excreted in human milk. Albendazole should be used with caution in breastfeeding women.
Treatment in Children
The safety of albendazole in children less than 6 years old is not certain. Studies of the use of albendazole in children as young as one year old suggest that its use is safe. According to WHO guidelines for mass prevention campaigns, albendazole can be used in children as young as 1 year old. Many children less than 6 years old have been treated in these campaigns with albendazole, albeit at a reduced dose.
Mebendazole
Treatment in Pregnancy
Mebendazole is in pregnancy category C. Data on the use of mebendazole in pregnant women are limited. The available evidence suggests no difference in congenital anomalies in the children of women who were treated with mebendazole during mass treatment programs compared with those who were not. In mass treatment programs for which the World Health Organization (WHO) has determined that the benefit of treatment outweighs the risk, WHO allows use of mebendazole in the 2nd and 3rd trimesters of pregnancy. The risk of treatment in pregnant women who are known to have an infection needs to be balanced with the risk of disease progression in the absence of treatment.
Pregnancy Category C: Either studies in animals have revealed adverse effects on the fetus (teratogenic or embryocidal, or other) and there are no controlled studies in women or studies in women and animals are not available. Drugs should be given only if the potential benefit justifies the potential risk to the fetus.
Treatment During Lactation
It is not known whether mebendazole is excreted in breast milk. The WHO classifies mebendazole as compatible with breastfeeding and allows the use of mebendazole in lactating women.
Treatment in children
The safety of mebendazole in children has not been established. There is limited data in children age 2 years and younger. Mebendazole is listed as an intestinal antihelminthic medicine on the WHO Model List of Essential Medicines for Children, intended for the use of children up to 12 years of age.
Ivermectin
Treatment in Pregnancy
Ivermectin is pregnancy category C. Data on the use of ivermectin in pregnant women are limited, though the available evidence suggests no difference in congenital abnormalities in the children of women who were accidentally treated during mass prevention campaigns with ivermectin compared with those who were not. The World Health Organization (WHO) excludes pregnant women from mass prevention campaigns that use ivermectin. However, the risk of treatment in pregnant women who are known to have an infection needs to be balanced with the risk of disease progression in the absence of treatment.
Pregnancy Category C: Either studies in animals have revealed adverse effects on the fetus (teratogenic or embryocidal, or other) and there are no controlled studies in women or studies in women and animals are not available. Drugs should be given only if the potential benefit justifies the potential risk to the fetus.
Treatment During Lactation
Ivermectin is excreted in low concentrations in human milk. Ivermectin should be used in breast-feeding women only when the risk to the infant is outweighed by the risk of disease progress in the mother in the absence of treatment.
Treatment in Children
The safety of ivermectin in children who weigh less than 15kg has not been demonstrated. According to the WHO guidelines for mass prevention campaigns, children who are at least 90 cm tall can be treated safely with ivermectin. The WHO growth standard curves show that this height is reached by 50% of boys by the time they are 28 months old and by 50% of girls by the time they are 30 months old, many children less than 3 years old been safely treated with ivermectin in mass prevention campaigns, albeit at a reduced dose.
Surgery
In cases of heavy infestation, surgery may be necessary to remove worms and repair damage they’ve caused. Intestinal obstruction or perforation, bile duct obstruction, and appendicitis are complications that may require surgery.
References [ + ]





{kind=link}