Contents
What is basal cell carcinoma
Basal cell carcinoma (BCC), also known as basal cell epithelioma, is the most common form of skin cancer. There are several sub-types of basal cell carcinoma including nodular basal cell carcinoma, infiltrating basal cell carcinoma and superficial basal cell carcinoma. All types of basal cell carcinoma usually occur on sun-damaged skin but can occur anywhere on the body (except the palms and soles). More than 99% of people with basal cell carcinoma are white, and 95% are between the ages of 40 and 80.
Basal cell carcinoma is the most common type of cancer in Europe, Australia and the US, and is caused primarily by chronic sun exposure. Luckily, it rarely metastasizes, but may be locally destructive.
- In a study of Canadians, the lifetime incidence in Caucasians ranged from 15-28% in women and 17-39% in men 1. A recent study however of the Medicare beneficiaries in the US found equal incidence of basal cell carcinoma and squamous cell carcinoma 2.
- The single best predictor of the likelihood of future development of basal cell carcinoma is the number of basal cell carcinomas in the past 5 years 3.
- Other important risk factors are UV exposure (e.g., cumulative exposure, sunburns over 20 years prior, sunbed use) and genetics (e.g., red hair, blue or green eyes, family history of skin cancer, type I skin, tendency to freckle, and Irish, Scottish, Scandinavian or German heritage).
- Basal cell carcinoma occurs most commonly in older adults on the head, neck, and back but may occur in children.
- When a basal cell carcinoma occurs in a child, it may be associated with radiation therapy, a genetic defect (e.g., basal cell nevus syndrome, xeroderma pigmentosum), a nevus sebaceous, or just significant sun exposure.
- Any basal cell carcinoma occurring before age 19 should prompt consideration of basal cell nevus syndrome.
- For some unknown reason, basal cell carcinomas rarely occur on the back of the hands.
There are several histologic subtypes that influence morphology. The most common are:
- Nodular basal cell carcinoma
- Superficial basal cell carcinoma
- Morpheaform basal cell carcinoma
Various clinical types include:
- Recurrent basal cell carcinoma
- Large or Ulcerative
- Cystic basal cell carcinoma
- Pigmented basal cell carcinoma
- Linear basal cell carcinoma
The basal cell carcinoma can take on many appearances. A pearly papule with telangiectasias on the face of an older person is classic (see Figure 1). Other potential presentations include a blue papule (cystic basal cell carcinoma), a rodent ulcer, a waxy telangiectatic plaque and a red, scaly area (superficial basal cell carcinoma). The superficial basal cell carcinoma appears as a fixed, blanchable, ham-red lesion surrounded by sun-damaged skin.
Figure 1. Basal cell skin carcinoma

Note: The basal cell carcinoma can take on many forms. A pearly telangiectatic papule is the most classic.
Figure 2. Basal cell carcinoma on face

Figure 3. Basal cell carcinoma face

Figure 4. Basal cell carcinoma eyelid
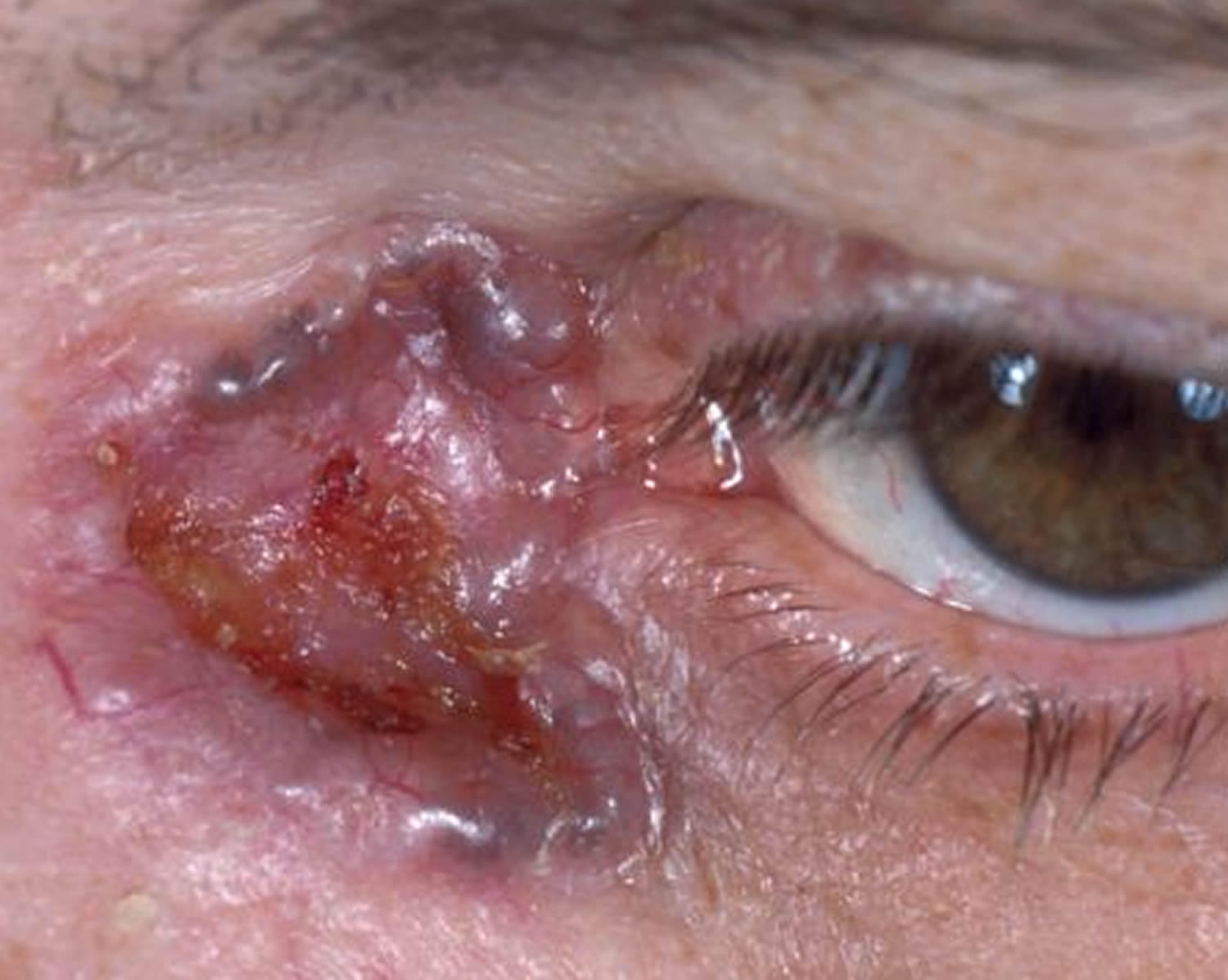
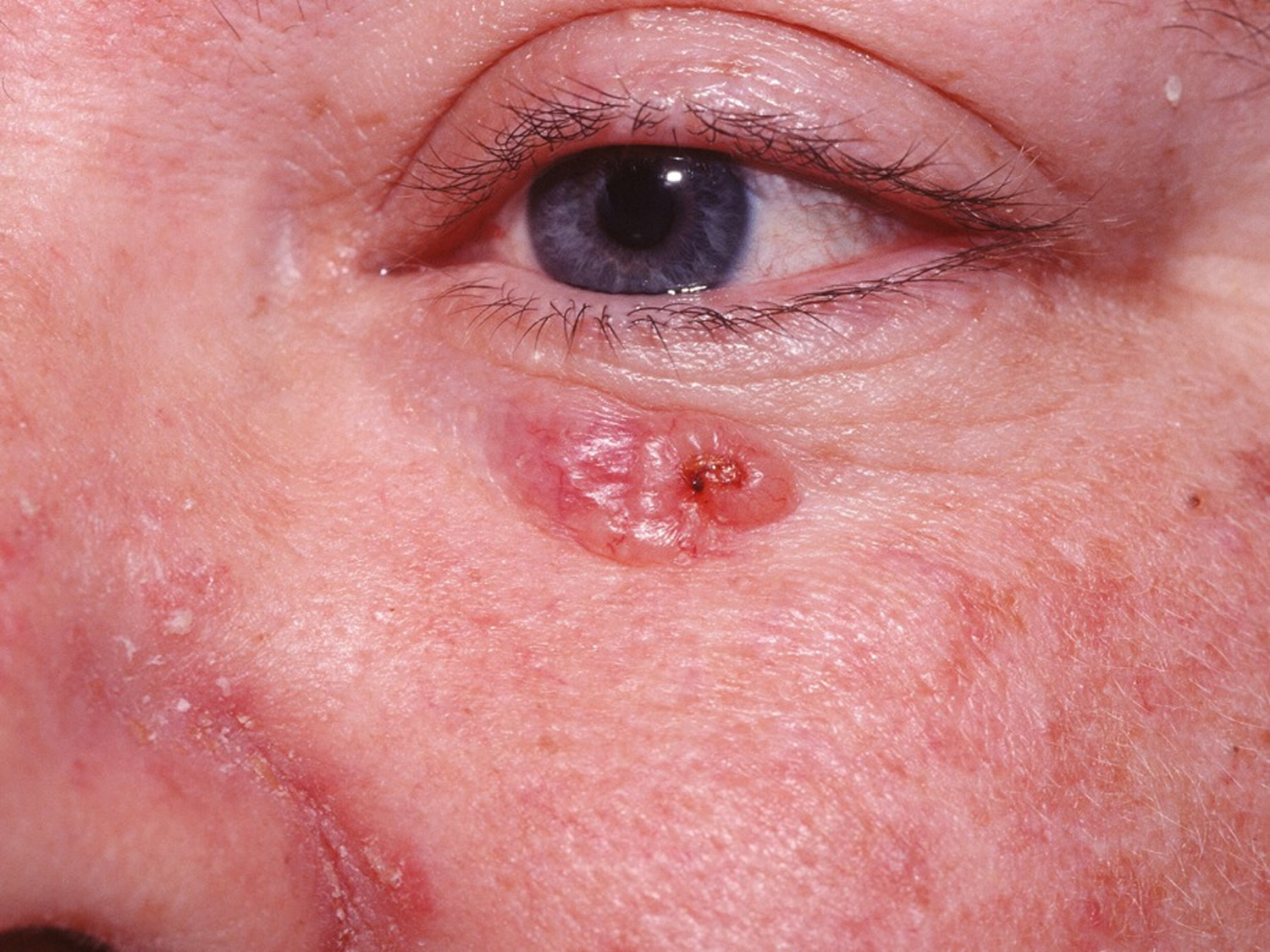
Figure 5. Basal cell carcinoma nose (pigmented)

Note: The basal cell carcinoma may be completely pigmented or have specks of pigment embedded in a pink to red background. This change is more common in darker-skinned individuals, e.g., Hispanics, Filipinos.


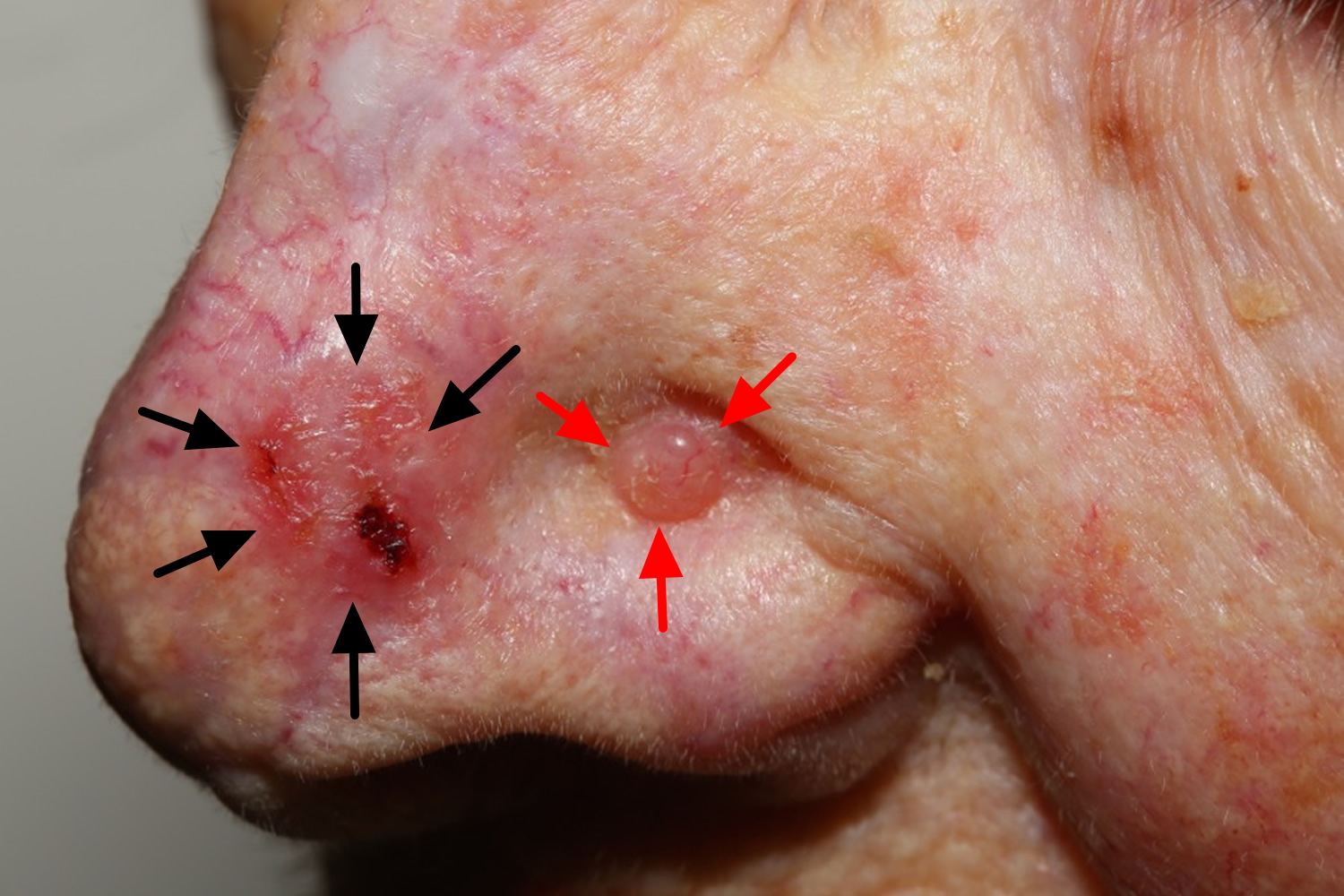
Note: Two basal cell carcinomas here. The crusty, red plaque on the left and the pearly telangiectatic papule to the right.
Figure 6. Basal cell carcinoma on scalp


Types of basal cell carcinoma
There are several distinct clinical types of basal cell carcinoma, and over 20 histological growth patterns of basal cell carcinoma.
Superficial basal cell carcinoma
A superficial basal cell carcinoma is a basal cell carcinoma which histologically shows a superficial proliferation of neoplastic basal cells.
The superficial basal cell carcinoma usually appears as a red, scaly area in a sea of brown, photodamaged skin. This is the thinnest of basal cell carcinomas and thus usually the easiest to treat.
- Most common type in younger adults
- Most common type on upper trunk and shoulders
- Slightly scaly, irregular plaque
- Thin, translucent rolled border
- Multiple microerosions
A shave biopsy is needed for diagnosis. Often, a curettage and electrodessication may be done at the same time. See treatment of basal cell carcinoma below. A comparison of imiquimod, fluorouricil and photodynamic therapy found imiquimod treatment superior 4. 5-FU 5% twice daily x 4 weeks is quoted as having a 70-80% clearance rate of small superficial basal cell carcinomas of the trunk.
Imiquimod is approved for the treatment of superficial basal cell carcinomas. The patient must be an immunocompetent adult, with a basal cell carcinoma no greater than 2 cm in diameter and should not be on the face, head, anogenital area, hands, or feet. Imiquimod is applied 5 days a week for 6 weeks and left on for 8 hours each application. The cure rate has ranged in studies from 69 to 79%.
Figure 7. Superficial basal cell carcinoma

Nodular basal cell carcinoma
A nodular basal cell carcinoma is a general term which refers to the classic basal cell carcinoma. It typically presents clinically as a papule or nodule.
Nodular basal cell carcinoma
- Most common type of facial basal cell carcinoma
- Shiny or pearly nodule with a smooth surface
- May have central depression or ulceration, so its edges appear rolled
- Blood vessels cross its surface
- Cystic variant is soft, with jelly-like contents
- Micronodular, microcystic and infiltrative types are potentially aggressive subtypes.
Off-label use of imiquimod for nodular basal cell carcinoma has been studied. Cure rates for the regimen of daily x 6 weeks may be as high as 70-80%. It is not recommended for recurrent basal cell carcinoma. Elderly patients reluctant to undergo surgery might be good candidates.
Figure 8. Nodular basal cell carcinoma

Figure 9. Cystic basal cell carcinoma


Morphoeiform basal cell carcinoma
A morpheaform basal cell carcinoma or sclerosing basal cell carcinoma is a basal cell carcinoma which histologically has a fibrotic or scar-like component. It is often more aggressive than the nodular basal cell carcinoma. The prior use of fluorouracil has been shown to predispose to the development of morpheaform basal cell carcinoma in elderly men 5. Also patients whose first basal cell carcinoma was morpheaform and that developed a second basal cell carcinoma, the second basal cell carcinoma was 12 times more likely to be morpheaform compared with patients whose first basal cell carcinoma was not morpheaform.
Morpheaform basal cell carcinoma:
- Usually found in mid-facial sites
- Waxy, scar-like plaque with indistinct borders
- Wide and deep subclinical extension
- May infiltrate cutaneous nerves (perineural spread)
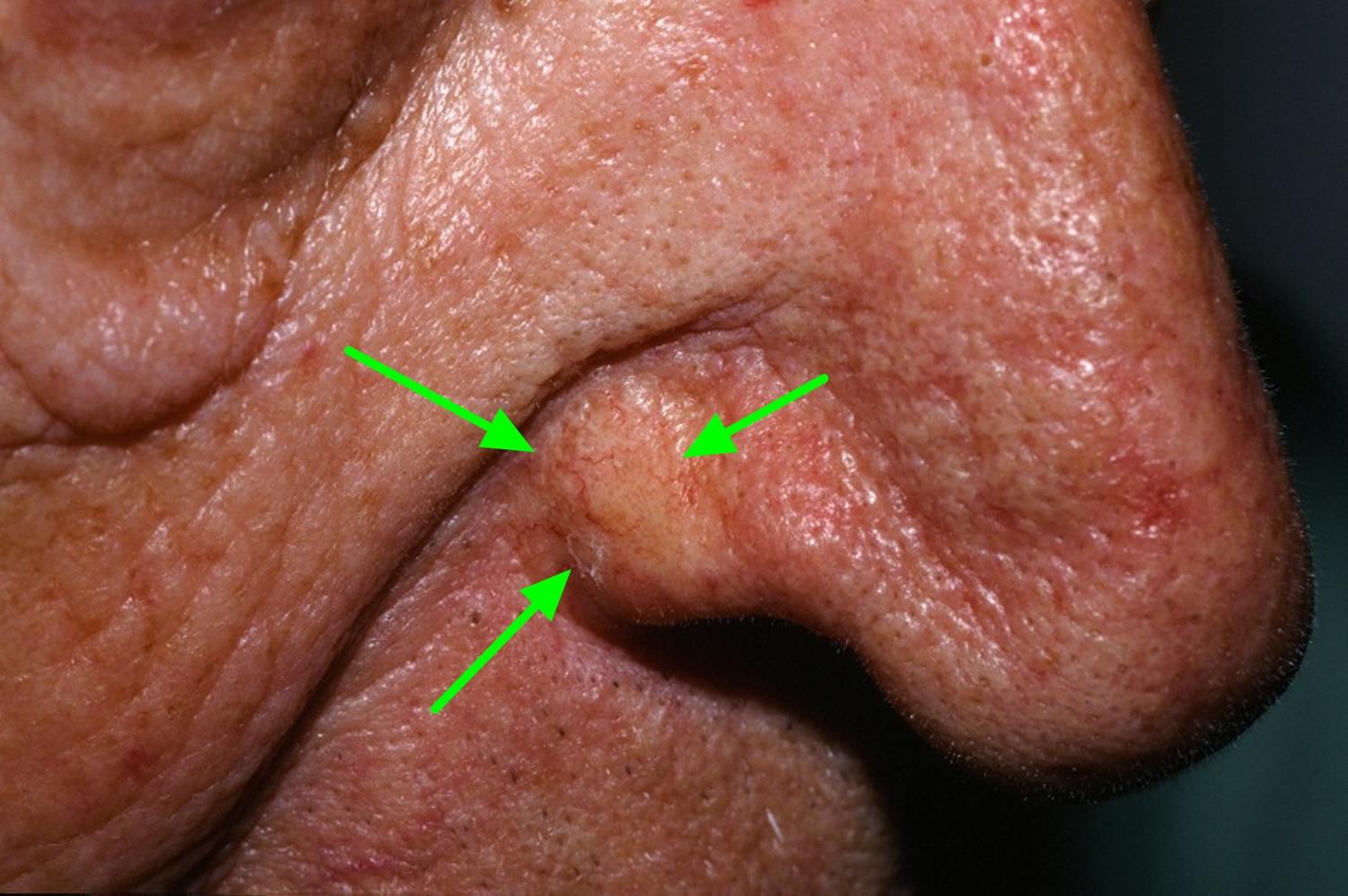
The morpheaform basal cell carcinoma resembles the more common nodular basal cell carcinoma in many ways, although it may have a slightly more yellowish tinge.
Surgical excision is the indicated treatment. Mohs surgery is appropriate for lesions on the face. Therapies used for other histologic types of basal cell carcinoma, e.g. photodynamic therapy are not sufficiently effective for morpheaform basal cell carcinoma.
Figure 10. Morpheaform basal cell carcinoma

Basal cell carcinoma causes
The cause of basal cell carcinoma is multifactorial.
- Most often, there are DNA mutations in the patched (PTCH) tumour suppressor gene, part of hedgehog signalling pathway
- These may be triggered by exposure to ultraviolet radiation
- Various spontaneous and inherited gene defects predispose to basal cell carcinoma
Risk factors for basal cell carcinoma
Risk factors for basal cell carcinoma include:
- Age and gender: basal cell carcinomas are particularly prevalent in elderly males. However, they also affect females and younger adults
- Previous basal cell carcinoma or other form of skin cancer (squamous cell carcinoma, melanoma)
- Sun damage (photoageing, actinic keratoses)
- Repeated prior episodes of sunburn
- Fair skin, blue eyes and blond or red hair—note; basal cell carcinoma can also affect darker skin types
- Previous cutaneous injury, thermal burn, disease (eg cutaneous lupus, sebaceous naevus)
- Inherited syndromes: basal cell carcinoma is a particular problem for families with basal cell naevus syndrome (Gorlin syndrome), Bazex-Dupré-Christol syndrome, Rombo syndrome, Oley syndrome and xeroderma pigmentosum
- Other risk factors include ionizing radiation, exposure to arsenic, and immune suppression due to disease or medicines.
Basal cell carcinoma prevention
- Stay indoors or under the shade in the middle of the day
- Wear covering clothing, hat and sunglasses
- Use broadspectrum sunscreens SPF 50+ generously to exposed skin if outdoors and sun avoidance
- Avoid indoor tanning (sun beds, solaria)
- Nicotinamide (vitamin B3) in a dose of 500 mg twice daily may reduce the number and severity of basal cell carcinomas.
A recent placebo-controlled study of 386 patients who had been diagnosed with at least two skin cancers – such as basal cell carcinoma and squamous cell carcinoma – in the past five years, showed that taking 500 milligrams twice daily of nicotinamide (not nicotinic acid) reduced the subsequent risk of non-melanoma skin cancers by 23%. When patients stopped taking the supplements, their risk of getting skin cancer rose again about six months later.
A prospective, randomized, double-blind, placebo-controlled study of acitretin 25 mg/day 5 days a week over 2 years did not show any reduction in the development of basal cell carcinoma in patients with a history of multiple basal cell carcinomas 6.
Topical tretinoin and tazarotene have been shown to not be effective in preventing basal cell carcinoma 7.
Basal cell carcinoma complications
Recurrent basal cell carcinoma
Recurrence of basal cell carcinoma after initial treatment is not uncommon. Characteristics of recurrent basal cell carcinoma often include:
- Incomplete excision or narrow margins at primary excision
- Morphoeic, micronodular, and infiltrative subtypes
- Location on head and neck
Advanced basal cell carcinoma
Advanced basal cell carcinomas are large, often neglected tumours.
- They may be several centimetres in diameter
- They may be deeply infiltrating into tissues below the skin
- They are difficult or impossible to treat surgically
Metastatic basal cell carcinoma
- Very rare
- Primary tumor is often large, neglected or recurrent, located on head and neck, with aggressive subtype
- May have had multiple prior treatments
- May arise in site exposed to ionizing radiation
- Can be fatal
Basal cell carcinoma symptoms
Basal cell carcinoma is a locally invasive skin tumor. The main characteristics are:
- Slowly growing plaque or nodule
- Skin colored, pink or pigmented
- Varies in size from a few millimetres to several centimetres in diameter
- Spontaneous bleeding or ulceration
Basal cell carcinoma is very rarely a threat to life. A tiny proportion of basal cell carcinomas grow rapidly, invade deeply, and/or metastasise to local lymph nodes.
If left for years, a basal cell carcinoma (basal cell carcinoma) may become quite large (see Figure 10 below). Metastasis is still relatively uncommon, but may occur. The term “locally advanced basal cell carcinoma” has been used for these large basal cell carcinomas that present a treatment challenge and may potentially metastasize. It has been estimated several thousand people die each year in the US from basal cell carcinoma. Unfortunately, patients with these neglected skin carcinomas commonly have been seen by multiple physicians and received a long list of topical medications before reaching the right diagnosis 8.
Figure 11. Basal cell carcinoma (untreated)


Basal cell carcinoma prognosis
Most basal cell carcinomas are cured by treatment. Cure is most likely if treatment is undertaken when the lesion is small.
About 50% of people with basal cell carcinoma develop a second one within 3 years of the first. They are also at increased risk of other skin cancers, especially melanoma. Regular self-skin examinations and long-term annual skin checks by an experienced health professional are recommended.
Basal cell carcinoma diagnosis
Basal cell carcinoma is diagnosed clinically by the presence of a slowly enlarging skin lesion with typical appearance. The diagnosis and histological subtype is usually confirmed pathologically by a diagnostic biopsy or following excision.
Some typical superficial basal cell carcinomas on trunk and limbs are clinically diagnosed and have non-surgical treatment without histology.
Basal cell carcinoma treatment
Several types of treatment can be used to remove or destroy basal cell skin cancers. The options depend on factors such as the tumor size and location, and a person’s age, general health, and preferences. These cancers very rarely spread to other parts of the body, although they can grow into nearby tissues if not treated.
All of the treatments listed here can be effective. The chance of the cancer coming back (recurring) ranges from less than 5% after Mohs surgery to up to 15% or higher after some of the others, but this depends on the size of the tumor. Small tumors are less likely to recur than larger ones. Even if a tumor does recur, it can often still be treated effectively.
Radiation therapy
Radiation therapy is often a good option for treating patients who aren’t able to have surgery and for treating tumors on the eyelids, nose, or ears – areas that can be hard to treat surgically – especially in older patients where cure may not be as important as control over the long term. Virtually any basal cell carcinoma of the face is a reasonable candidate and certain sites are excellent for radiation therapy, e.g., the nasal ala. Radiation therapy is also sometimes used after surgery if it’s not clear that all of the cancer has been removed.
Radiation is also useful when combined with other treatments. For example, radiation can be used after surgery as an adjuvant (additional) treatment to kill any small areas of remaining cancer cells that may not have been visible during surgery. This lowers the risk of cancer coming back after surgery. Radiation may also be used to help treat skin cancer that has spread to lymph nodes or other organs.
Radiation therapy is a good alternative in certain situations. Large basal cell carcinomas on the trunk are also reasonable candidates if surgery would be difficult.
Cure rates for most basal cell carcinomas are around 95% 9. For recurrent basal cell carcinomas it drops down to 90%.
Radiated skin after 20 years may not be as appealing cosmetically, so most patients treated with radiation therapy are usually over 60 years of age but some radiation therapists treat patients as young as 45. Morpheaform histology is usually a contraindication. Potential side effects include hypopigmentation, e.g., in 10% and less likely atrophy. Multiple treatment sessions are usually done over 3-6 weeks.
In one study of 141 basal cell carcinomas in 117 frail elderly patients, weekly radiation therapy for 6 weeks gave a relapse-free survival after 5 years of 95% 10.
When radiation therapy is used to treat skin cancers, the radiation is focused from outside the body onto the tumor. This is often done with a type of radiation called electron beam radiation. It uses a beam of electrons that don’t go any deeper than the skin. This helps limit the side effects to other organs and body tissues.
Getting radiation treatment is much like getting an x-ray, but the radiation is stronger and aimed more precisely at the cancer. The procedure itself is painless. Each treatment lasts only a few minutes, although the setup time – getting you into place for treatment – takes longer.
Possible side effects of radiation
Side effects of radiation are usually limited to the area getting radiation, and can include:
- Skin irritation, ranging from redness to blistering and peeling
- Changes in skin color
- Hair loss in the area being treated
- Damage to saliva-making glands and teeth when treating cancers near these structures
With longer treatment, these side effects may get worse.
After many years, new skin cancers sometimes develop in areas previously treated by radiation. For this reason, radiation usually is not used to treat skin cancer in young people. Radiation is also not recommended for people with certain inherited conditions (such as basal cell nevus syndrome or xeroderma pigmentosum), who may be at higher risk for new cancers, or for people with connective tissue diseases (such as lupus or scleroderma), which radiation might make worse.
Immune response modifiers, photodynamic therapy, or topical chemotherapy
These treatments are sometimes options for treating very superficial tumors (tumors that have not grown too deeply into the skin). Close follow-up is needed because these treatments do not destroy any cancer cells that have grown deep below the surface.
- Topical chemotherapy
Chemotherapy uses drugs that kill cancer cells. Topical chemotherapy means that an anti-cancer medicine is put directly on the skin (usually in a cream or ointment) rather than being given by mouth or injected into a vein.
5-fluorouracil (5-FU): The drug most often used in topical treatment of actinic keratoses, as well as some basal and squamous cell skin cancers, is 5-FU (with brand names such as Efudex, Carac, and Fluoroplex). It is typically applied to the skin once or twice a day for several weeks.
When put directly on the skin, 5-FU kills tumor cells on or near the skin’s surface, but it can’t reach cancer cells deeper in the skin or those that have spread to other organs. For this reason, 5-FU is generally used only for pre-cancerous conditions such as actinic keratosis and for some very superficial skin cancers.
Because the drug is only applied to the skin, it doesn’t spread throughout the body, so it doesn’t cause the same side effects as systemic chemotherapy (treatment that affects the whole body). But it does make the treated skin red and very sensitive for a few weeks. Other topical medicines can be used to help relieve this, if needed. 5-FU can also make the skin more sensitive to sunlight, so treated areas must be protected from the sun to prevent sunburn for a few weeks after use of this cream.
A very small portion of people have a condition called DPD deficiency, which makes it hard for their bodies to break down and get rid of 5-FU. This can result in serious or even life-threatening side effects. If you are applying 5-FU and have any reactions beyond those you were told to expect on your skin, call your doctor or nurse right away.
Systemic Chemotherapy for Basal Cell Carcinoma
Systemic chemotherapy (chemo) uses anti-cancer drugs that are injected into a vein or given by mouth. These drugs travel through the bloodstream to all parts of the body. Unlike topical chemotherapy, which is applied to the skin, systemic chemotherapy can attack cancer cells that have spread to lymph nodes and other organs.
Basal cell carcinoma very rarely reaches an advanced stage, so systemic chemotherapy is not typically used to treat these cancers. Advanced basal cell cancers are more likely to be treated with targeted therapy.
If basal cell carcinoma has spread, chemo drugs such as cisplatin, doxorubicin, 5-fluorouracil (5-FU), capecitabine, topotecan, and etoposide might be used. These drugs are given into a vein (intravenously, or IV), usually once every few weeks. They can often slow the spread of these cancers and relieve some symptoms. In some cases, they might shrink tumors enough so that other treatments such as surgery or radiation therapy can be used.
Possible side effects of chemotherapy
Chemo drugs can cause side effects. These depend on the type and dose of drugs given and how long they are used. The side effects of chemo can include:
- Hair loss
- Mouth sores
- Loss of appetite
- Nausea and vomiting
- Diarrhea or constipation
- Increased risk of infection (from having too few white blood cells)
- Easy bruising or bleeding (from having too few blood platelets)
- Fatigue (from having too few red blood cells)
These side effects usually go away once treatment is finished. Some drugs can have specific effects that are not listed above, so be sure to talk with your cancer care team about what you might expect.
There are often ways to lessen these side effects. For example, drugs can help prevent or reduce nausea and vomiting. Tell your medical team about any side effects or changes you notice while getting chemo so that they can be treated promptly.
- Immune response modifiers
Certain drugs can boost the body’s immune response against the cancer, causing it to shrink and go away.
Imiquimod (Zyclara) is a cream that can be applied to actinic keratoses and some very early basal cell cancers. It causes the immune system to react to the skin lesion and destroy it. It’s typically applied at least a few times a week for several weeks, although schedules can vary. Like other topical gels, it can cause severe skin reactions in some people. It can also cause flu-like symptoms.
Interferon is a man-made version of an immune system protein. It can be injected directly into the tumor to boost the immune response against it. It might be an option when surgery isn’t possible, but it may not be as effective as other treatments.
- Photodynamic therapy
Photodynamic therapy can be used to treat actinic keratoses. But its exact role in treating basal and squamous cell skin cancers, if any, still needs to be determined.
This treatment uses a special liquid drug that is applied to the skin. The drug collects in the tumor cells over several hours or days, where it is converted to a different chemical that makes the cells very sensitive to certain types of light. A special light source is then focused on the tumor(s), which kills the cells.
Photodynamic therapy can cause redness and swelling on the skin where it is used. Another possible side effect of photodynamic therapy is that it can make a person’s skin very sensitive to sunlight for some time, so precautions may be needed to avoid severe burns.
Cure rates as high as 87% have been reported for photodynamic therapy treatment of superficial basal cell carcinomas. Cosmesis is a selling point and can be excellent. It is not recommended for recurrent lesions and is usually not used for other histologic subtypes. A cure rate of 76% (5 year followup) was found for methyl aminolevulinate photodynamic therapy treatment of nodular basal cell carcinoma 11.
Cryotherapy
For this treatment, the doctor applies liquid nitrogen to the tumor to freeze and kill the cells. This is often repeated a couple of times in the same office visit. After the dead area of skin thaws, it will swell, blister and crust over.
Cryotherapy (cryosurgery) can be used for some small basal cell carcinomas, but it’s not usually recommended for larger tumors or those on certain parts of the nose, ears, eyelids, scalp, or legs.
Cryotherapy can also be used to treat large tumors in one treatment session to relieve symptoms from the cancer.
The wound may have fluid draining from it for a while and take a month or two to heal. It will leave a scar, and the treated area may have less color after treatment.
Targeted therapy for advanced basal cell cancers
In rare cases where basal cell cancer spreads to other parts of the body or can’t be cured with surgery or radiation therapy, a targeted drug (Hedgehog pathway inhibitors) such as vismodegib (Erivedge) or sonidegib (Odomzo) can often shrink or slow some advanced or recurrent basal cell skin cancers. Odomzo and Erivedge are FDA-approved for metastatic or locally advanced basal cell carcinomas that may not be surgically amenable. Side effects are significant.
These drugs target parts of skin cancer cells that make them different from normal skin cells. Targeted drugs work differently from standard chemotherapy drugs. They may work sometimes when chemotherapy drugs don’t. They may also have less severe side effects. Doctors are still learning the best way to use these drugs to treat skin cancers.
It’s very rare for basal cell cancers to reach an advanced stage, but if they do, these cancers can be hard to treat. Most basal cell cancers have mutations (changes) in genes that are part of a cell signaling pathway called hedgehog. The hedgehog pathway is crucial for the development of the embryo and fetus and is important in some adult cells, but it can be overactive in basal cell cancer cells. These drugs target a protein in this pathway.
These drugs are capsules taken once a day. For basal cell cancers that have spread or come back after surgery or other local treatments, these drugs have been shown to help shrink tumors in some people, although it’s not yet clear if they help people live longer.
Side effects can include muscle spasms, joint pain, hair loss, fatigue, problems with taste, poor appetite and weight loss, nausea and vomiting, itchy skin, diarrhea, and constipation. These drugs can also cause women to stop having their periods.
Because the hedgehog pathway affects fetal development, these drugs should not be taken by women who are pregnant or could become pregnant. It is not known if they could harm the fetus if taken by a male partner. Anyone taking these drugs should use reliable birth control during and for some time after treatment.
Basal cell carcinoma removal
Surgery
Many factors impact the choice of therapy for a basal cell carcinoma (basal cell carcinoma). Size, location, and histologic pattern are most important. The patient’s cosmetic sensibility also plays a role. For example, Mohs surgery is appropriate for ill-defined tumors on the face, recurrent lesions, large tumors, and those with morpheaform histology. Curettage and electrodessication is appropriate for small nodular or superficial basal cell carcinomas on the trunk. Surgical excision leaves a straight line scar and is very appropriate for most nodular basal cell carcinomas that are not candidates for Mohs surgery.
Classic surgical excision with 3-4 mm margins is one of the first-line therapies for basal cell carcinoma. Given clear margins, the cure rate is estimated at 98%. It is usually employed for uncomplicated basal cell carcinomas at a distance from important anatomic structures. Certain features are associated with a further extension beyond clinical margins or the need for tissue sparing. In these cases, Mohs surgery is typically used. They include proximity to the nose, eyes, or ears, larger lesions, recurrent lesions, and morpheaform histology.
Different types of surgery can be used to treat basal cell cancers.
- Curettage and electrodesiccation: This is a common treatment for small, uncomplicated basal cell carcinomas. Curettage and electrodessication might need to be repeated to help make sure all of the cancer has been removed. In this treatment, the doctor removes the cancer by scraping it with a long, thin instrument with a sharp looped edge on one end (called a curette). The area is then treated with an electric needle (electrode) to destroy any remaining cancer cells. This process is often repeated once or twice during the same office visit. Curettage and electrodesiccation is a good treatment for superficial (confined to the top layer of skin) basal cell and squamous cell cancers. It will leave a scar.Curettage and electrodessication cure rate is high (>95%) 12. However, the resulting scar is on average less pleasing to the patient than those resulting from surgery 13. Curettage and electrodessication is very appropriate for lesions 1 cm or less and non-facial lesions. The H zone (nasolabial fold, nasal alae, orbital area and auricular area) in some studies has been associated with a higher rate of recurrence following curettage and electrodessication.The experienced dermatologist will evaluate a lesion prior to biopsy as to 1) the likelihood that it is a basal cell carcinoma and 2) the appropriate treatment if the biopsy is positive. If the lesion is very likely a basal cell carcinoma and it is amenable to curettage and electrodessication, both biopsy and treatment may be done at that same visit 14.
- Curettage AloneBarlow et al achieved a 5-year cure rate of 96% using curettage alone followed by 20% aluminum chloride application for hemostasis 15. Quoting from the methods section of the article: “Thorough curettage was performed in at least 3 directions to treat the base and a 2-5 mm peripheral margin until only normal dermis remained…A normal base was characterized by a uniform appearance and the texture of firm collagen without residual irregularity.” The supposed benefits of curettage without electrodessication include simplicity, lack of equipment requirements, avoidance of potentially hazardous viral smoke plumes, and reduced risk of hyperpigmentation and scarring.
- Excision: Excision (cutting the tumor out) is often used to remove basal cell carcinomas, along with a margin of normal skin. For this procedure, the skin is first numbed with a local anesthetic. The tumor is then cut out with a surgical knife, along with some surrounding normal skin. The remaining skin is carefully stitched back together, which will leave a scar.
- Mohs surgery: Mohs micrographic surgery is also called microscopically controlled surgery. Mohs surgery is the gold standard for the treatment of basal cell carcinoma with a recurrence rate of only 1-2%. Cost limits its use however. For example Mohs surgery is not appropriate for a 4 mm nodular basal cell carcinoma on the back. Mohs surgery should be considered first option for larger lesions (e.g., > 2 cm), recurrent lesions, morpheaform histology, and facial lesions, especially those near the ears, nose, or eyes. It’s used to remove certain skin cancers by shaving off one very thin layer at a time. After each layer is removed, the doctor looks at the tissue with a microscope to check for cancer cells. This procedure is repeated until all the cells in a layer look normal. This is a slow process, often taking several hours, but it means that more normal skin near the tumor can be saved. This can help the area look better after surgery. Mohs surgery is used when the extent of the cancer is not known or when as much healthy tissue as possible needs to be saved, such as when treating skin cancers near the eye. Mohs surgery has the best cure rate for basal cell carcinoma. It’s especially useful in treating large tumors, tumors where the edges are not well-defined, tumors in certain locations (such as on or near the nose, eyes, ears, forehead, scalp, fingers, and genital area), and those that have come back after other treatments. However, it’s also usually more complex and time-consuming than other methods. In recent years, skin cancer experts have developed guidelines for when it’s best to use this technique based on the type and size of skin cancer, where it is on the body, and other important features.
Skin grafting and reconstructive surgery
After surgery to remove a large basal (or squamous) cell skin cancer, it may not be possible to stretch the nearby skin enough to stitch the edges of the wound together. In these cases, healthy skin can be taken from another part of the body and grafted over the wound to help it heal and to restore the appearance of the affected area. Other reconstructive surgical procedures can also be helpful in some cases.
Treatment for advanced or metastatic basal cell carcinoma
Locally advanced primary, recurrent or metastatic basal cell carcinoma requires multidisciplinary consultation. Often a combination of treatments is used.
- Surgery
- Radiotherapy
- Targeted therapy
Targeted therapy refers to the hedgehog signalling pathway inhibitors, vismodegib and sonidegib. These drugs have some important risks and side effects.
- BJD 2010;163;146[↩]
- JAMA Derm 2015;151;1081[↩]
- JID 2012;132:2544[↩]
- J Eur Acad Dermatol Venereol 2011; 25:565–9[↩]
- JAMADerm 2014;150;332[↩]
- Cancer. 2012;118:2128[↩]
- JID 2012;132:1583[↩]
- JEADV 2016;30;367[↩]
- JAAD 2012;67;1235[↩]
- JAAD 2015;73;166[↩]
- Arch Dermatol. 2007;143:1131-6[↩]
- JID 2013:123:1188-96[↩]
- JAAD 2014:71:1026-7[↩]
- JAMA Dermatol 2013;149:980-1[↩]
- JAAD 2006;54;1039[↩]





{kind=link}