
Contents
- What you need to know about breastfeeding
- When can I start breastfeeding?
- Is breastfeeding good for babies with special needs?
- Is any amount of breastfeeding good?
- How do you know when your baby’s ready to eat?
- How often do you breastfeed?
- How long does each feeding last?
- How do you know if your baby is getting enough milk?
- Is breastfeeding good for the mother?
- Can breastfeeding help me lose weight?
- Is breastfeeding safe for all moms and babies?
- How long should a mother breastfeed?
- What can happen if someone else’s breast milk is given to another child?
- Should mothers who smoke breastfeed?
- When should a baby start eating solid foods such as cereals, vegetables, and fruits?
- How to stop breastfeeding?
- Does your baby need vitamin supplements if you breastfeed?
- How does breastfeeding help in an emergency?
- Do you need special clothes to breastfeed?
- Breastfeeding vs Formula
- Breastfeeding while pregnant
- Breastfeeding diet
- Breastfeeding tips
- Problems and discomforts when breastfeeding
- What can you do if you’re sore after having a c-section?
- What to do if you have strong let-down reflex?
- What is breast engorgement?
- What to do when you have oversupply of breast milk?
- What to do if you think you have low milk supply?
- What can you do about nipple pain?
- What can you do if your breasts leak?
- What are plugged ducts?
- What is mastitis?
- What is fungal infection?
- What is nipple confusion?
- What are inverted, flat, or very large nipples?
- What is nursing strike?
- Benefits of breastfeeding
- Contraindications to Breastfeeding
- Alcohol and breastfeeding
What you need to know about breastfeeding
Doctors agree that breastfeeding is best for babies. But many mothers can find breastfeeding challenging. Decades of research has proved the benefits of breastfeeding. Your early breast milk, known as colostrum, provides an important source of antibodies to protect your baby against diseases. Other benefits include lowering the risk of allergies and infections in your baby, as well as helping you recover faster from birth. The American Academy of Pediatrics recommends exclusive breastfeeding for approximately the first 6 months of life and continued breastfeeding with complementary foods through at least the first 12 months 1) or longer as mutually desired by mother and infant, a recommendation concurred to by the World Health Organization 2) and the Institute of Medicine 3). Support for this recommendation of exclusive breastfeeding is found in the differences in health outcomes of infants breastfed exclusively for 4 vs 6 months, for gastrointestinal disease, otitis media, respiratory illnesses, and atopic disease, as well as differences in maternal outcomes of delayed menses and postpartum weight loss 4).
Exclusive breastfeeding for six months (versus three to four months, with continued mixed breastfeeding thereafter) reduces gastrointestinal infection and helps the mother lose weight after birth and prevent pregnancy but has no long-term impact on allergic disease, growth, obesity, dental caries, cognitive ability, or behavior problems 5). The results of two controlled trials and 21 other studies suggest that exclusive breastfeeding (no solids or liquids besides human milk, other than vitamins and medications) for six months has several advantages over exclusive breastfeeding for three to four months followed by mixed breastfeeding 6).
Compared with infants who never breastfed, infants who were exclusively breastfed for 4 months had significantly greater incidence of lower respiratory tract illnesses, otitis media, and diarrheal disease than infants exclusively breastfed for 6 months or longer 7). When compared with infants who exclusively breastfed for longer than 6 months, those exclusively breastfed for 4 to 6 months had a fourfold increase in the risk of pneumonia 8). Furthermore, exclusively breastfeeding for 6 months extends the period of lactational amenorrhea and thus improves child spacing, which reduces the risk of birth of a preterm infant 9).
Why breastfeeding is good for your baby
- Breast milk has hormones and the right amount of protein, sugar, fat and most vitamins to help your baby grow and develop. Breast milk has antibodies that help protect your baby from many illnesses. Antibodies are cells in the body that fight off infection. Breastfed babies have fewer health problems than babies who aren’t breastfed. Breastfed babies don’t have as many ear, lung or urinary tract infections. And they’re less likely to have asthma, certain cancers and diabetes (having too much sugar in your blood) later in life. They’re also less likely to be overweight.
- Breast milk has fatty acids, like DHA (docosahexaenoic acid), that may help your baby’s brain and eyes develop. It may lower the chances of sudden infant death syndrome (SIDS). SIDS is the unexplained death of a baby younger than 1 year old.
- Breast milk is easy to digest. A breastfed baby may have less gas and belly pain than a baby who is fed formula. Formula is a man-made product that you buy and feed your baby.
- Breast milk changes as your baby grows so he gets exactly what he needs at the right time. For example, for the first few days after giving birth, your breasts make a thick, yellowish form of breast milk called colostrum. Colostrum has nutrients and antibodies that your baby needs in the first few days of life. It changes to breast milk in 3 to 4 days. Breast milk is always ready when your baby wants to eat. The more you breastfeed, the more milk you make. Most breastfeeding moms make as much breast milk as their babies need.
In the United States, most new moms (about 4 in 5 or 80 percent) breastfeed their babies. About half of these moms breastfeed their babies for at least 6 months.
Breastfeeding benefits for infants
Infants who are breastfed have reduced risks of 10):
- Asthma
- Obesity (during childhood)
- Type 2 diabetes
- Ear and respiratory infections
- Sudden infant death syndrome (SIDS)
- Leukemia (during childhood)
- Ear infections
- Eczema (atopic dermatitis)
- Diarrhea and vomiting
- Lower respiratory infections
- Necrotizing enterocolitis, a disease that affects the gastrointestinal tract in premature babies, or babies born before 37 weeks of pregnancy
Your breastmilk helps your baby grow healthy and strong from day one.
Your first milk is liquid gold. Called liquid gold for its deep yellow color, colostrum is the thick first milk that you make during pregnancy and just after birth. This milk is very rich in nutrients and includes antibodies to protect your baby from infections.
- Colostrum also helps your newborn’s digestive system to grow and function. Your baby gets only a small amount of colostrum at each feeding, because the stomach of a newborn infant is tiny and can hold only a small amount. (Read How do I know if my baby is getting enough breastmilk? to see just how small your newborn’s tummy is!)
- Your milk changes as your baby grows. Colostrum changes into mature milk by the third to fifth day after birth. This mature milk has just the right amount of fat, sugar, water, and protein to help your baby continue to grow. It looks thinner than colostrum, but it has the nutrients and antibodies your baby needs for healthy growth.
Breastfeeding benefits for mothers
Breastfeeding helps a mother’s health and healing following childbirth. Breastfeeding leads to a lower risk of these health problems in mothers 11):
- Heart disease
- Type 2 diabetes
- Ovarian cancer
- Breast cancer
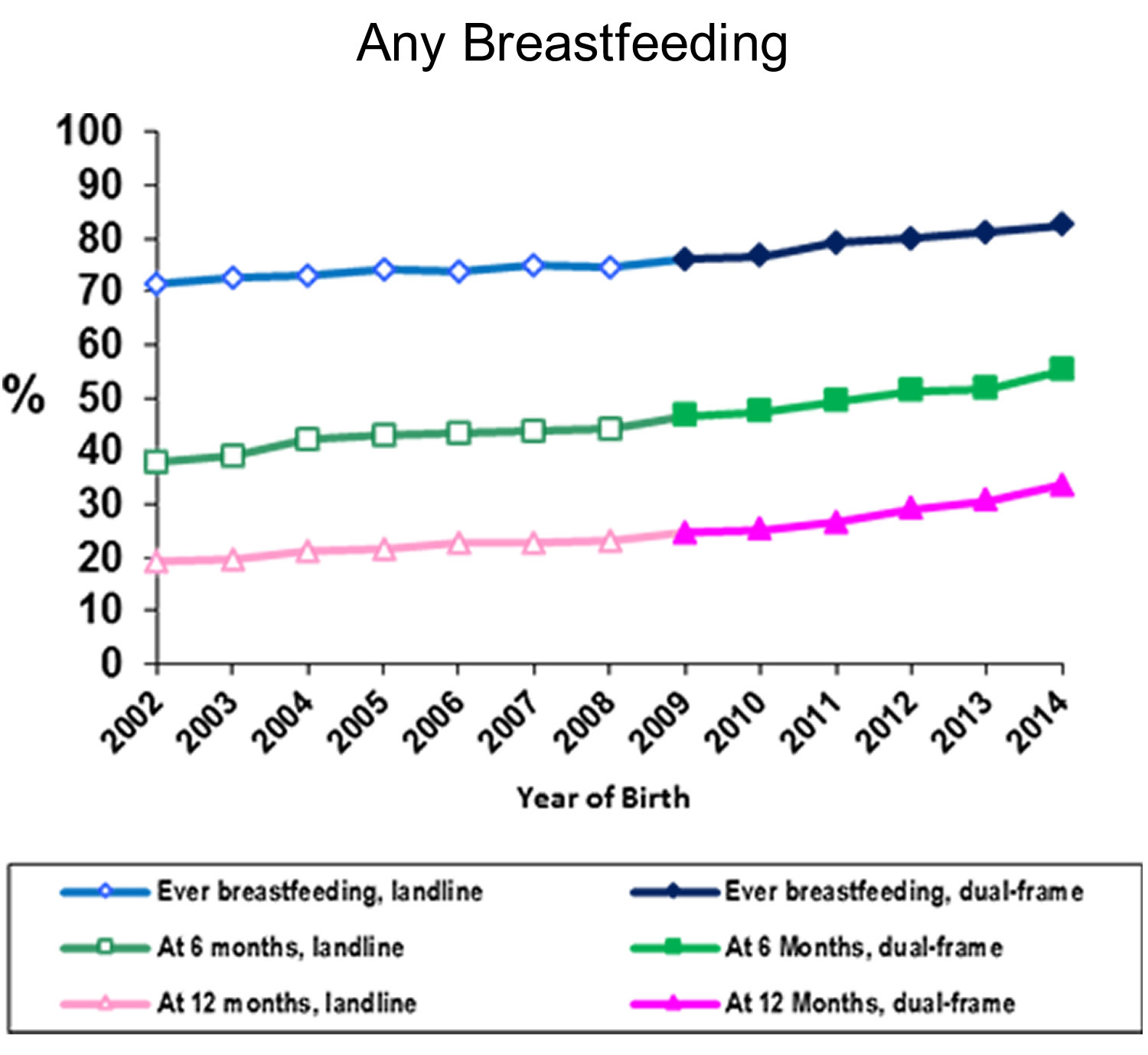
According to a report by the Centers for Disease Control and Prevention 12), the proportion of mothers who breastfed their infants rose from 70.3 percent to 83 percent between 2004 and 2014. Babies are also breastfeeding for longer; 55% of U.S. babies born in 2014 were being breastfed at 6 months, up from 42% in 2004. Despite these overall increases, racial disparities between black and white infants persist 13).
A recent Centers for Disease Control and Prevention study, published in the Morbidity and Mortality Weekly Report 14), describes how breastfeeding rates continue to differ between African American and white infants within states.
- Among infants born during 2010–2013, 64.3% of African American infants started breastfeeding, compared to 81.5% of non-Hispanic white infants, a gap of 17.2 percentage points.
- Most of the 34 states included in the study reported lower rates of breastfeeding initiation rates among African American infants than among non-Hispanic white infants. Among low-income mothers (participants in the Special Supplemental Nutrition Program for Women, Infants, and Children [WIC]), the breastfeeding initiation rate was 67.5%, but in those with a higher income ineligible for Women, Infants, and Children, it was 84.6% 15). Breastfeeding initiation rate was 37% for low-income African American mothers 16). Similar disparities are age-related; mothers younger than 20 years initiated breastfeeding at a rate of 59.7% compared with the rate of 79.3% in mothers older than 30 years. The lowest rates of initiation were seen among African American mothers younger than 20 years, in whom the breastfeeding initiation rate was 30%
- 17).
- In 14 states (primarily in the South and Midwest) the percentage of African American infants who ever breastfed was at least 15 percentage points lower than among non-Hispanic white infants.
- African American infants also had significantly lower rates than non-Hispanic white infants of exclusive breastfeeding at 6 months and breastfeeding for 12 months.
Many factors influence a woman’s decision to start and continue breastfeeding. Some barriers disproportionately affect African American women, such as:
- Returning earlier to work.
- Not receiving enough information about breastfeeding from providers.
- Lack of access to professional breastfeeding support.
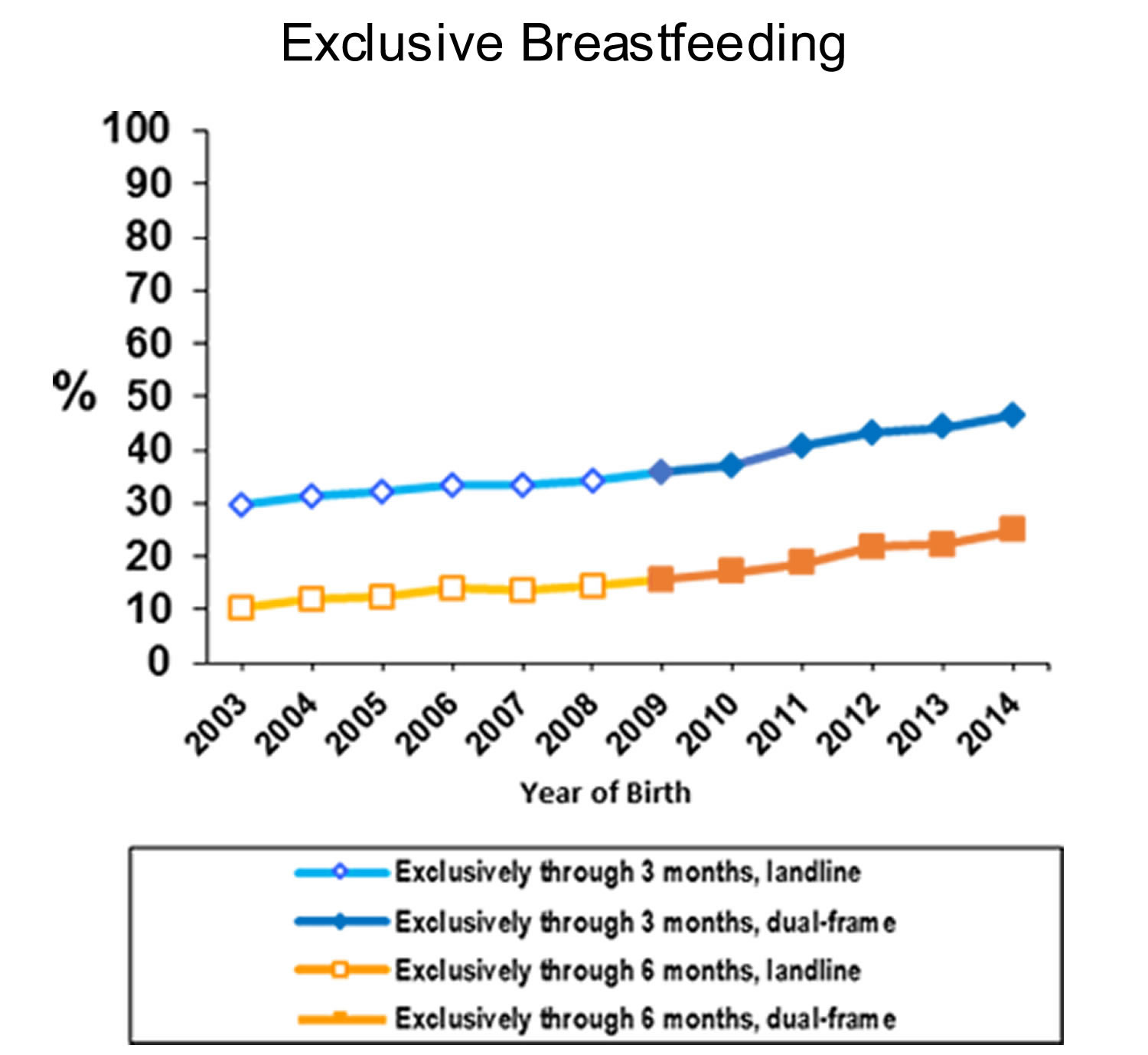
Figure 1. Breastfeeding Among U.S. Children Born 2002–2014
When can I start breastfeeding?
Most women can start breastfeeding within 1 hour after their baby is born. A nurse or lactation consultant can help you get started:
- Tell the nurses that you want to breastfeed.
- Ask to have your baby stay in the room with you so you can breastfeed him when he needs to eat.
- Ask your nurses, the lactation consultant and your baby’s provider to help make sure breastfeeding is going well before you leave the hospital.
Is breastfeeding good for babies with special needs?
Yes. Some babies are born premature (before 37 weeks of pregnancy) or with birth defects or other medical conditions. Breastfeeding a baby with special needs like these can help her grow and protect her from illness. But you may need help to make breastfeeding work for you and your baby.
Talk to your health care provider or lactation consultant about breastfeeding your baby with special needs. A lactation consultant is a person with special training in helping women breastfeed.
Is any amount of breastfeeding good?
Yes. It’s best to feed your baby only breast milk for at least 6 months. This means no water, formula, other liquids or solid food—just breast milk. But any amount of breastfeeding is good for your baby’s health and development. Even breastfeeding for a short time is good for your baby.
How do you know when your baby’s ready to eat?
Look for her feeding cues. Feeding cues are ways that your baby tells you that she’s hungry. Examples are:
- Rooting (turning her head toward anything that strokes her cheek or mouth)
- Sucking movements or sounds
- Putting her hand to her mouth
- Crying — This is a late feeding cue. Try to breastfeed your baby before she starts to cry.
How often do you breastfeed?
Feed your baby when she’s hungry. This is called on-demand feeding. Most newborns eat about eight to 12 times over 24 hours, which is about once every 2 to 3 hours. But each baby is different. Your baby may want to feed more often or less often. As your baby grows, her feeding patterns may change, and she may go longer between feedings.
To make nighttime feedings easier, put the baby’s crib in your room. Just don’t sleep with the baby in your bed.
How long does each feeding last?
Let your baby feed as long as she wants at one breast. This is called feeding unlimited at the breast. This usually takes about 15 to 30 minutes. Your baby may take more or less time. When she is finished with one breast, burp her. Then switch her to feed from the other breast. It’s OK if she only wants to nurse from one breast. Just be sure to start her on the other breast at the next feeding. Let your baby end breastfeeding on her own.
How do you know if your baby is getting enough milk?
Lots of new moms ask this question. Your body is pretty amazing. As you breastfeed, your body learns when your baby needs more milk. Your body makes exactly the right amount for your baby. But what if you’re still not sure he’s eating enough? Your baby is probably getting enough milk if he:
- Is gaining weight
- Is making six to eight wet diapers a day by the time he’s 5 to 7 days old
Is breastfeeding good for the mother?
Yes. Breastfeeding your baby helps you because:
- It increases the amount of a hormone in your body called oxytocin. This helps your uterus (womb) go back to the size it was before you got pregnant. It also helps stop bleeding that you have after giving birth.
- It burns extra calories. This helps you get back to your pre-pregnancy weight (your weight before pregnancy).
- It may help lower your risk for diabetes, breast cancer and ovarian cancer.
- It can help you bond with your baby.
Breastfeeding also delays the return of your period. But this can make it hard to know when your body can get pregnant again. Use birth control when you start having sex again. Talk to your provider about birth control that’s safe to use when you’re breastfeeding.
Can breastfeeding help me lose weight?
Besides giving your baby nourishment and helping to keep your baby from becoming sick, breastfeeding may help you lose weight. Many women who breastfed their babies said it helped them get back to their pre-pregnancy weight more quickly, but experts are still looking at the effects of breastfeeding on weight loss.
Is breastfeeding safe for all moms and babies?
No. Breastfeeding may not be safe for your baby if you have certain medical conditions, take certain medicines or have other problems, like using street drugs or abusing prescription drugs. You can pass some infections, medicines and drugs to your baby through breast milk. Some can be very harmful to your baby. Talk to your provider if you think you have a condition that may make breastfeeding unsafe for your baby.
How long should a mother breastfeed?
The American Academy of Pediatrics recommends that breastfeeding continue for at least 12 months, and thereafter for as long as mother and baby desire. The World Health Organization recommends continued breastfeeding up to 2 years of age or beyond.
What can happen if someone else’s breast milk is given to another child?
HIV and other serious infectious diseases can be transmitted through breast milk. However, the risk of infection from a single bottle of breast milk, even if the mother is HIV positive, is extremely small. For women who do not have HIV or other serious infectious diseases, there is little risk to the child who receives her breast milk.
Should mothers who smoke breastfeed?
Mothers who smoke are encouraged to quit, however, breast milk remains the ideal food for a baby even if the mother smokes. Although nicotine may be present in breast milk, adverse effects on the infant during breastfeeding have not been reported. American Academy of Pediatrics recognizes pregnancy and lactation as two ideal times to promote smoking cessation, but does not indicate that mothers who smoke should not breastfeed.
When should a baby start eating solid foods such as cereals, vegetables, and fruits?
Breast milk alone is sufficient to support optimal growth and development for approximately the first 6 months after birth. For these very young infants, the American Academy of Pediatrics 18) states that water, juice, and other foods are generally unnecessary. Even when babies enjoy discovering new tastes and textures, solid foods should not replace breastfeeding, but merely complement breast milk as the infant’s main source of nutrients throughout the first year. Beyond one year, as the variety and volume of solid foods gradually increase, breast milk remains an ideal addition to the child’s diet.
How to stop breastfeeding?
You can breastfeed your baby for as long as you want. When you stop breastfeeding, it’s called weaning your baby. Some babies begin weaning on their own between 6 and 12 months as they start eating solid food and become more active. Weaning is a slow process that doesn’t happen in a few days. Taking your time can make weaning easier for you and your baby.
If you wean your baby off breast milk before she’s 12 months old, feed her formula. She can stay on formula until she’s ready to drink regular milk after she turns 1.
Does your baby need vitamin supplements if you breastfeed?
Yes. A supplement is a product you take to make up for certain nutrients that you don’t get enough of in the foods you eat.
Breast milk doesn’t have enough vitamin D for your baby. Vitamin D helps make bones and teeth strong and helps prevent a bone disease called rickets. Give your baby vitamin D drops starting in the first few days of life. Talk to your baby’s provider about vitamin D drops for your baby.
If you’re a vegan or if you’ve had gastric bypass surgery, you need extra vitamin B12. A vegan is someone who doesn’t eat meat or anything made with animal products, like eggs or milk. Gastric bypass is surgery on the stomach and intestines to help a person lose weight. Ask your provider about taking a vitamin B12 supplement to make sure you and your baby get the right amount.
How does breastfeeding help in an emergency?
During an emergency, such as a natural disaster, breastfeeding can save your baby’s life:
- Breastfeeding protects your baby from the risks of an unclean water supply.
- Breastfeeding can help protect your baby against respiratory illnesses and diarrhea.
- Your breast milk is always at the right temperature for your baby. It helps to keep your baby’s body temperature from dropping too low.
- Your breast milk is always available without needing other supplies.
Do you need special clothes to breastfeed?
No, but nursing bras have flaps that make breastfeeding easier than if you’re wearing your regular bra. You may want to get one or two while you’re pregnant so you have them when your baby is born. Get a nursing bra that is one size larger than your regular bra size so it will fit when your breasts get larger when your breast milk comes in.
You may find it easier to breastfeed in shirts that pull up, rather than shirts that button. Sometimes it’s hard to get buttons undone quickly when you’ve got a hungry baby wanting to eat.
Breastfeeding vs Formula
How does breastfeeding compare to formula feeding?
- Formula can be harder for your baby to digest. For most babies, especially premature babies (babies born before 37 weeks of pregnancy), breastmilk substitutes like formula are harder to digest than breastmilk. Formula is made from cow’s milk, and it often takes time for babies’ stomachs to adjust to digesting it.
- Your breastmilk changes to meet your baby’s needs. As your baby gets older, your breastmilk adjusts to meet your baby’s changing needs. Researchers think that a baby’s saliva transfers chemicals to a mother’s body through breastfeeding. These chemicals help a mother’s body create breastmilk that meets the baby’s changing needs.
- Life can be easier for you when you breastfeed. Breastfeeding may seem like it takes a little more effort than formula feeding at first. But breastfeeding can make your life easier once you and your baby settle into a good routine. When you breastfeed, there are no bottles and nipples to sterilize. You do not have to buy, measure, and mix formula. And there are no bottles to warm in the middle of the night! When you breastfeed, you can satisfy your baby’s hunger right away.
- Not breastfeeding costs money. Formula and feeding supplies can cost well over $1,500 each year. As your baby gets older he or she will eat more formula. But breastmilk changes with the baby’s needs, and babies usually need the same amount of breastmilk as they get older. Breastfed babies may also be sick less often, which can help keep your baby’s health costs lower.
- Breastfeeding keeps mother and baby close. Physical contact is important to newborns. It helps them feel more secure, warm, and comforted. Mothers also benefit from this closeness. The skin-to-skin contact boosts your oxytocin (OKS-ee-TOH-suhn) levels. Oxytocin is a hormone that helps breastmilk flow and can calm the mother.
Sometimes, formula feeding can save lives:
- Very rarely, babies are born unable to tolerate milk of any kind. These babies must have an infant formula that is hypoallergenic, dairy free, or lactose free. A wide selection of specialist baby formulas now on the market include soy formula, hydrolyzed formula, lactose-free formula, and hypoallergenic formula.
- Your baby may need formula if you have a health problem that won’t allow you to breastfeed and you do not have access to donor breastmilk.
Talk to your doctor before feeding your baby anything besides your breastmilk.
Breastfeeding while pregnant
You can breastfeed while pregnant; some mothers go on to nurse both their new baby and their older child after the birth. This is known as ‘tandem nursing’.
Family, friends and healthcare professionals may express concern if you are breastfeeding while pregnant. Their concerns might include perceived risk to the health of your unborn baby, and they may also worry about your well being. There is no evidence that breastfeeding during low risk pregnancy leads to increased chance of harm to mother or baby.
Breastfeeding during pregnancy is a personal decision. Many mothers chose to continue breastfeeding to best meet the needs of their older child. You may also chose to wean your child now, or later in your pregnancy.
A concern you may have is the health of your unborn baby. It may be reassuring to know that in a normal pregnancy there is no evidence that continuing to breastfeed will deprive your unborn child of necessary nutrients. Another typical concern is that hormone oxytocin, released by nipple stimulation while breastfeeding, could trigger early labor. However, there is no reason to suggest a connection between miscarriage and breastfeeding in a normal pregnancy. According to Hilary Flowers 19), the uterus is “deaf” to oxytocin throughout pregnancy, and its sensitivity to this hormone only increases around the onset of labor.
Madarshahian and Hassanabadi 20), compared rates of success in reaching full-term delivery and newborn birth weights between two groups of pregnant women with more than one child: those who breastfed during pregnancy and those who did not. Results of this study found no significant difference in babies born at full-term or non-full-term between the two groups; birth weight was also unaffected. The researchers concluding that breastfeeding during normal pregnancy is safe, and “does not increase chance of untoward maternal and newborn outcomes. Overlap breastfeeding is a personal decision for mothers” 21). This research purposely excluded high-risk pregnancies. If you are expecting multiples, or considered to be at risk for miscarriage/early deliver, discuss your options with the health professionals supporting you.
Changes during pregnancy
Some mothers develop tender nipples during pregnancy. Careful attention to your child’s position can help. Breathing techniques from childbirth classes can help you cope with the increased sensitivity. The breathing techniques may also help if you become restless while your toddler breastfeeds. If your child is old enough, you can ask him or her to nurse more gently or for shorter periods of time. This will help with both your tender nipples and your feelings of restlessness.
Needing extra rest is normal in pregnancy. Breastfeeding during your pregnancy may help you get extra rest if you breastfeed your toddler while lying down. Completely childproofing one room with a mattress or pallet on the floor would allow you to continue to rest if your toddler goes off to play.
Milk supply and colostrum
Women who breastfeed while pregnant often find their milk supply decreases around the fourth or fifth month (sometimes earlier than that). The composition of your milk will also change slightly. These changes are associated with normal hormonal changes during pregnancy, and nursing more frequently or pumping won’t increase production in the same way it would do if you were not pregnant. If your breastfeeding baby is less than a year old, watch his weight gain to be sure he is getting enough to eat. It’s also not uncommon for the flavor of your milk to change. These changes may prompt some older toddlers to nurse less often or to wean entirely.
No matter how often or long he breastfeeds, colostrum will still be available after birth for the newborn. The hormones that maintain a pregnancy are found in breastmilk, but these are not harmful to the breastfeeding child.
Some mothers express concern that their toddler may be taking milk meant to nourish their baby. These mothers may take comfort in the fact that breasts are marvellous things that can adjust their production to meet the demands placed upon them–if they are asked to produce enough milk for two, they usually can! Also, most toddlers breastfeed considerably less frequently than an infant, and get most of their nutrition from other foods.
Breastfeeding diet
Well-nourished lactating mothers have an increased daily energy need of 450 to 500 kcal/day (approximately 2,300 to 2,500 kcal per day for breastfeeding women verses 1,800 to 2,000 kcal per day for moderately active, non-pregnant women who are not breastfeeding) that can be met by a modest increase in a normally balanced varied diet 22). The number of additional calories needed for an individual breastfeeding woman is also affected by her age, body mass index, activity level, and extent of breastfeeding (exclusively breastfeeding verses breastfeeding and formula feeding).
- Refer to guidance from the U.S. Department of Agriculture (USDA) My Plate Daily Checklist for more information on vitamins, minerals, and calories needed while breastfeeding at the Choose My Plate website (https://www.choosemyplate.gov/moms-breastfeeding-nutritional-needs).
- Calculate daily calories needed for pregnant and breastfeeding women using the My Plate Calculator (https://www.choosemyplate.gov/MyPlatePlan).
Although dietary reference intakes for breastfeeding mothers are similar to or greater than those during pregnancy, there is no routine recommendation for maternal supplements during lactation 23). Many clinicians recommend the continued use of prenatal vitamin supplements during lactation 24).
The mother’s diet should include an average daily intake of 200 to 300 mg of the omega-3 long-chain polyunsaturated fatty acids (docosahexaenoic acid [DHA]) to guarantee a sufficient concentration of preformed DHA in the milk 25). Consumption of 1 to 2 portions of fish (eg, herring, canned light tuna, salmon) per week will meet this need. The concern regarding the possible risk from intake of excessive mercury or other contaminants is offset by the neurobehavioral benefits of an adequate DHA intake and can be minimized by avoiding the intake of predatory fish (eg, pike, marlin, mackerel, tile fish, swordfish) 26). Poorly nourished mothers or those on selective vegan diets may require a supplement of DHA as well as multivitamins.
Foods to avoid while breastfeeding
Generally, women do not need to limit or avoid specific foods while breastfeeding. Mothers should be encouraged to eat a healthy and diverse diet. However, certain types of seafood should be consumed in a limited amount and some mothers may wish to restrict caffeine while breastfeeding.
Seafood
Although fish remains an excellent source of protein and contains essential vitamins and minerals for breastfeeding women, some care must be taken in deciding on the amount and types of seafood to consume. Most fish contain some amount of mercury, which accumulates in fish flesh and can pass from mother to infant through breast milk. This can have adverse effects on the brain and nervous system of the breastfed infant.
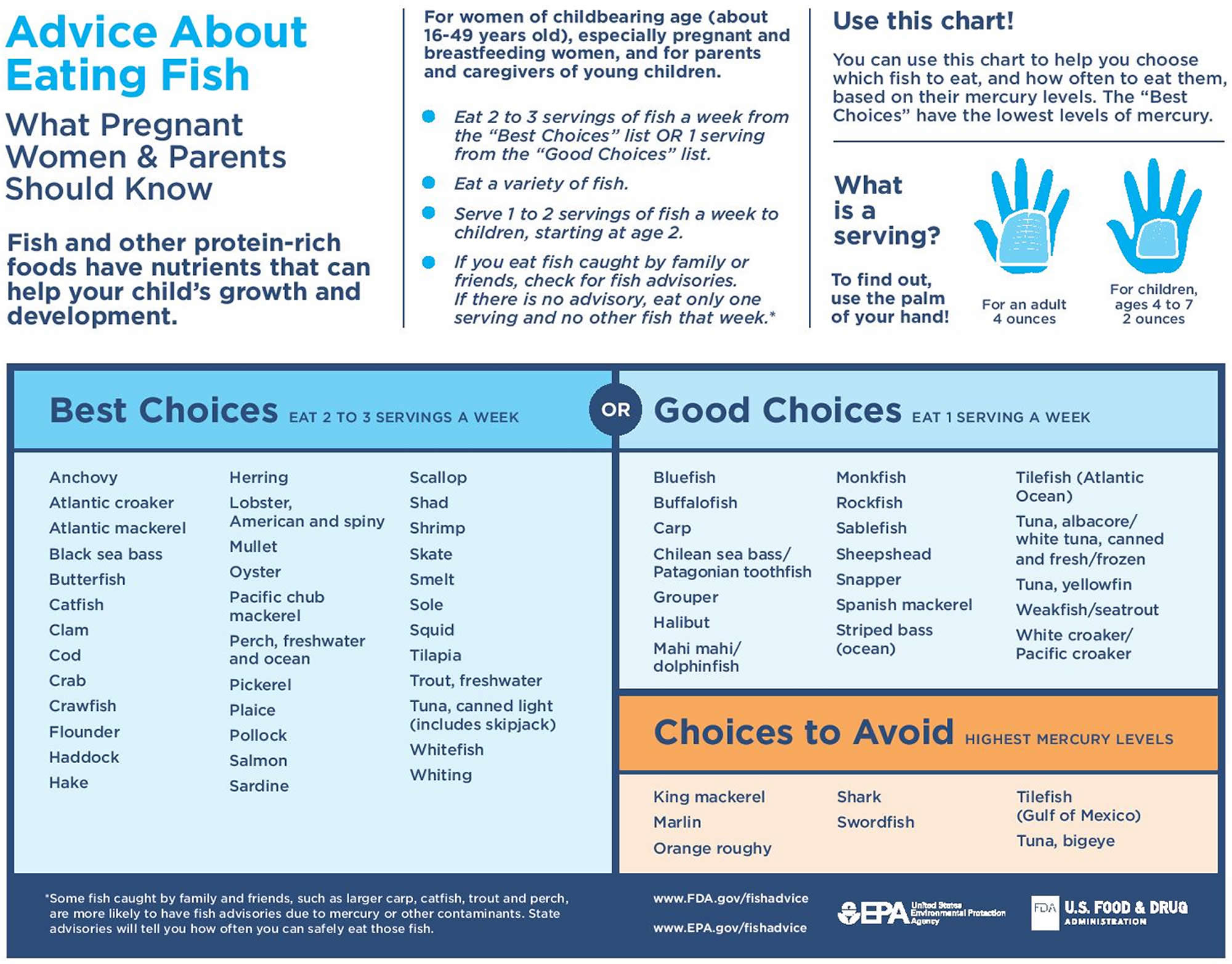
Breastfeeding women (as well as pregnant women, women of childbearing age, and parents and caregivers of young children) should follow the US Food and Drug Administration’s (FDA) advice about eating fish:
- Eat 2 to 3 servings of fish a week from the “Best Choices” list OR 1 serving from the “Good Choices” list from the FDA/EPA Advice on What Pregnant Women and Parents Should Know about Eating Fish.
- Eat a variety of fish.
- For fish caught by family or friends, check for fish advisories. If there is no advisory, eat only one serving and no other fish that week.
- Serve 1 to 2 servings of fish a week to children, starting at age 2.
Mercury can be harmful to the brain and nervous system of any person exposed to too much of it over time. Thus, lower mercury fish are a good choice for everyone.
Figure 2. Seafood and breastfeeding recommendation
Caffeine
Caffeine passes from the mother to infant in small amounts through breast milk, but usually does not adversely affect the infant when the mother consumes low to moderate amounts (about 300 milligrams or less per day, which is about 2 to 3 cups of coffee). Irritability, poor sleeping patterns, fussiness, and jitteriness have been reported in infants of mothers with very high intakes of caffeine, about 10 cups of coffee or more per day.
If an infant appears to be more fussy or irritable after the mother consumes high amounts of caffeine, she should consider decreasing her intake. Preterm and younger newborn infants break down caffeine more slowly, so mothers of these infants might consider consuming even less caffeine.
Common dietary sources of caffeine include the following:
- Coffee.
- Sodas.
- Energy drinks.
- Tea.
- Chocolate.
Should mothers take a multivitamin while breastfeeding?
Maybe. Some people, such as those with restrictive diets (for example, diets that limit the number of calories per day and vegetarian diets), may not get adequate nutrients through their diet alone and may be at greater risk for nutritional deficiencies. In addition, the recommended dietary allowances (RDAs) (the average amount of a vitamin or mineral that meets the daily nutrient needs of nearly all healthy people) for some nutrients (such as iodine) increase while breastfeeding; therefore, it is possible that diet alone may not be sufficient to ensure adequate nutrition for women who are breastfeeding. In these cases, breastfeeding mothers may benefit from taking a multivitamin supplement.
Are there any special diet recommendations for mothers who eat a vegan or vegetarian diet while breastfeeding?
Yes. Breastfed infants of women who do not consume any animal products may have very limited amounts of vitamin B12 in their bodies. These low amounts of vitamin B12 can put their infants at risk of vitamin B12 deficiency, which can result in neurological damage. Therefore, the American Dietetic Association recommends vitamin B12 supplementation during pregnancy and while breastfeeding for mothers who eat vegan or lacto-ovo vegetarian diets.
Maternal Medications
Recommendations regarding breastfeeding in situations in which the mother is undergoing either diagnostic procedures or pharmacologic therapy must balance the benefits to the infant and the mother against the potential risk of drug exposure to the infant. There are only a limited number of agents that are contraindicated, and an appropriate substitute usually can be found. The most comprehensive, up-to-date source of information regarding the safety of maternal medications when the mother is breastfeeding is LactMed (https://toxnet.nlm.nih.gov/newtoxnet/lactmed.htm), an Internet-accessed source published by the National Library of Medicine/National Institutes of Health. In general, breastfeeding is not recommended when mothers are receiving medication from the following classes of drugs: amphetamines, chemotherapy agents, ergotamines, and statins.
There are a wide variety of maternally administered psychotropic agents for which there are inadequate pharmacologic data with regard to human milk and/or nursing infant’s blood concentrations. In addition, data regarding the long-term neurobehavioral effects from exposure to these agents during the critical developmental period of early infancy are lacking. A recent comprehensive review noted that of the 96 psychotropic drugs available, pharmacologic and clinical information was only available for 62 (65%) of the drugs 27). In only 19 was there adequate information to allow for defining a safety protocol and thus qualifying to be compatible for use by lactating mothers. Among the agents considered to be least problematic were the tricyclic antidepressants amitriptyline and clomipramine and the selective serotonin-reuptake inhibitors paroxetine and sertraline.
Detailed guidelines regarding the necessity for and duration of temporary cessation of breastfeeding after maternal exposure to diagnostic radioactive compounds are provided by the US Nuclear Regulatory Commission and in medical reviews 28). Special precaution should be followed in the situation of breastfeeding infants with glucose-6-phosphate-dehydrogenase deficiency. Fava beans, nitrofurantoin, primaquine, and phenazopyridine should be avoided by the mother to minimize the risk of hemolysis in the infant 29).
Breastfeeding tips
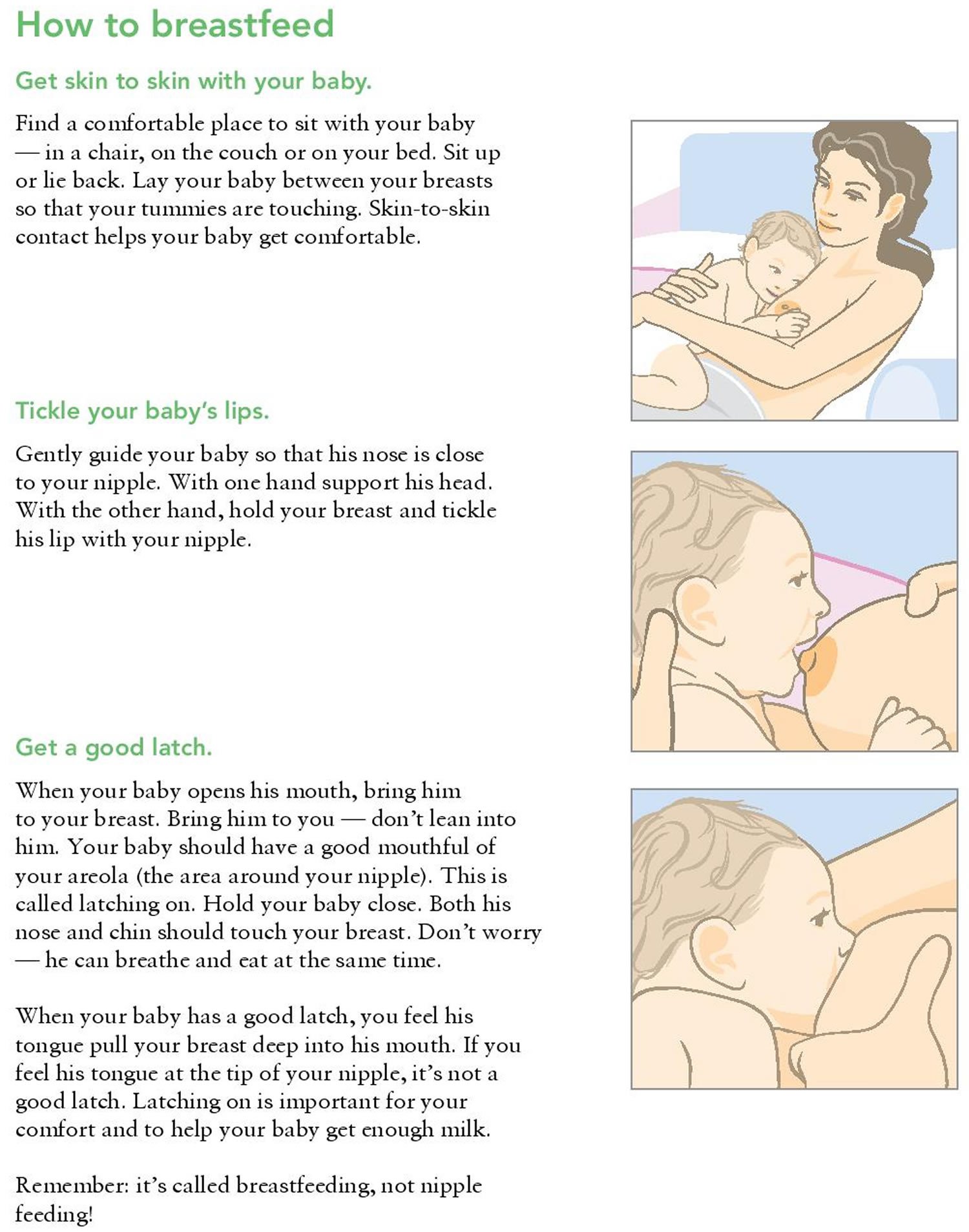
You may have heard people say that breastfeeding is the most natural thing in the world. The truth is that breastfeeding isn’t always easy. Breastfeeding feels a bit awkward at first, but don’t worry. Breastfeeding is a skill that you and your baby learn together, and it can take time and practice to get used to. Be patient and give yourself and your baby time to get comfortable with breastfeeding.
Most women can start breastfeeding within 1 hour after their baby is born. A nurse or lactation consultant can help you get started. A lactation consultant is a person with special training in helping women breastfeed.
In the first few days, you and your baby will be getting to know each other. It may take time for both of you to get the hang of breastfeeding.
This happens more quickly for some women than others. But nearly all women produce enough milk for their baby.
Having skin-to-skin contact with your baby straight after the birth will help to keep them warm and calm, and steady their breathing.
Skin to skin means holding your baby naked or dressed only in a nappy against your skin, usually under your top or under a blanket.
Skin-to-skin time can be a bonding experience for you and your baby. It’s also a great time to have your first breastfeed. If you need any help, your midwife will support you with positioning and attachment.
Skin-to-skin contact is good at any time. It will help to comfort you and your baby over the first few days and weeks as you get to know each other. It also helps your baby attach to your breast using their natural crawling and latching on reflexes.
If skin-to-skin contact is delayed for some reason – for example, if your baby needs to spend some time in special care – it doesn’t mean you won’t be able to bond with or breastfeed your baby.
If necessary, your midwife will show you how to express your breast milk until your baby is ready to breastfeed. They will also help you have skin-to-skin contact with your baby as soon as it’s possible.
There are lots of different positions you can use to breastfeed. You just need to check the following points:
- Are you comfortable? It’s worth getting comfortable before a feed. Use pillows or cushions if necessary. Your shoulders and arms should be relaxed.
- Are your baby’s head and body in a straight line? (It’s hard for your baby to swallow if their head and neck are twisted.)
- Are you holding your baby close to you, facing your breast? Supporting their neck, shoulders and back should allow them to tilt their head back and swallow easily.
- Always bring your baby to the breast rather than leaning forward to ‘post’ your breast into your baby’s mouth, as this can lead to poor attachment.
- Your baby needs to get a big mouthful of breast. Placing your baby with their nose level with your nipple will encourage them to open their mouth wide and attach to the breast well.
- Avoid holding the back of your baby’s head, so that they can tip their head back. This way your nipple goes past the hard roof of their mouth and ends up at the back of their mouth against the soft palate.
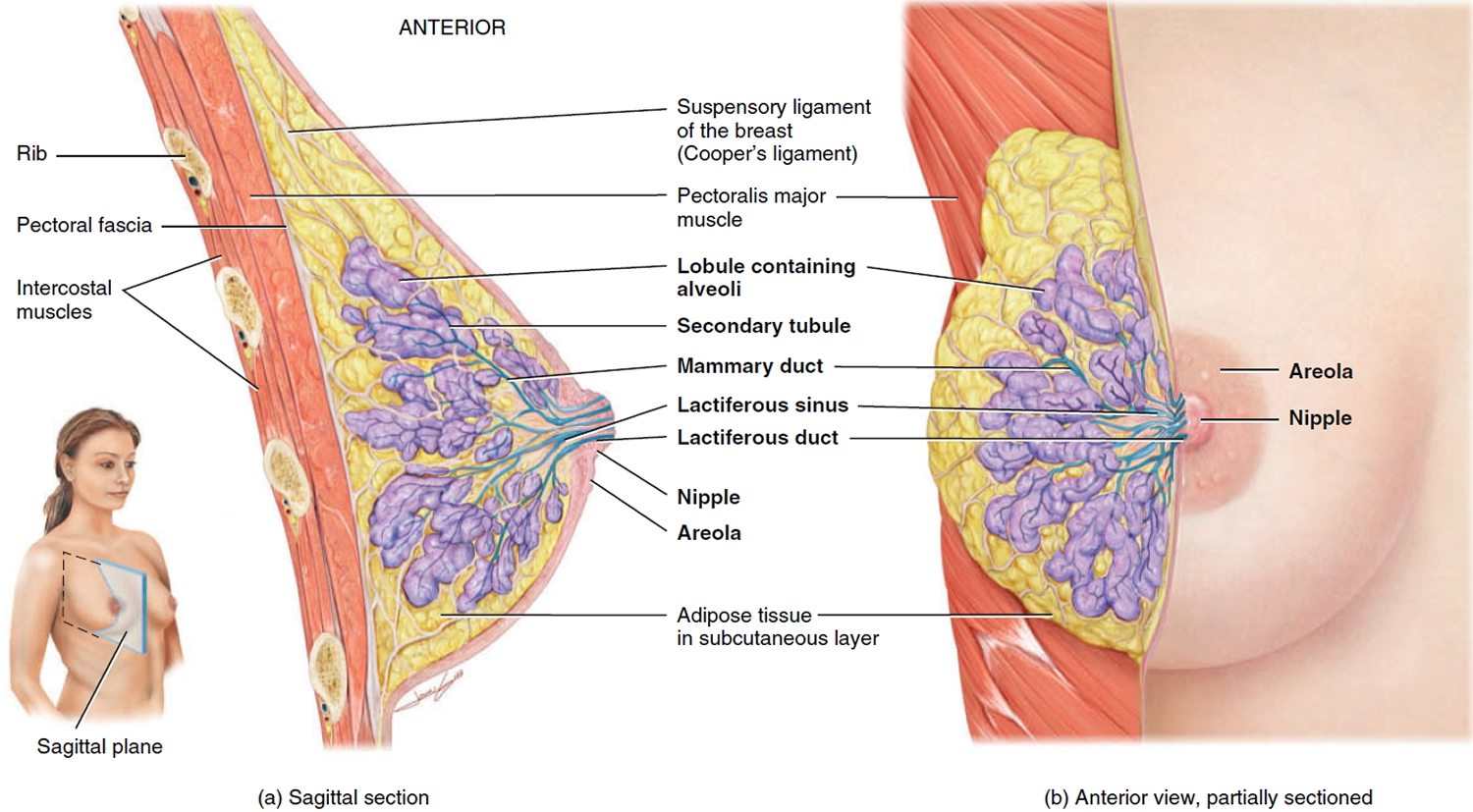
Figure 3. Normal breast (female)
Colostrum: your first milk
The fluid your breasts produce in the first few days after birth is called colostrum. It’s usually a golden yellow color. It’s a very concentrated food, so your baby will only need about a teaspoonful at each feed.
Your baby may want to feed quite often, perhaps every hour to begin with. They’ll begin to have fewer, longer feeds once your breasts start to produce more “mature” milk after a few days.
The more you breastfeed, the more your baby’s sucking will stimulate your supply and the more milk you’ll make.
Your let-down reflex
Your baby’s sucking causes milk stored in your breasts to be squeezed down ducts towards your nipples. This is called the let-down reflex.
Some women get a tingling feeling, which can be quite strong. Others feel nothing at all.
You’ll see your baby respond when your milk lets down. Their quick sucks will change to deep rhythmic swallows as the milk begins to flow. Babies often pause after the initial quick sucks while they wait for more milk to be delivered.
Occasionally this let-down reflex can be so strong that your baby coughs and splutters. Your midwife, health visitor or breastfeeding supporter can help with this, or see some tips for when you have too much breast milk.
If your baby seems to be falling asleep before the deep swallowing stage of feeds, they may not be properly attached to the breast. Ask your midwife, health visitor or breastfeeding supporter to check your baby’s positioning and attachment.
Sometimes you’ll notice your milk letting down in response to your baby crying or when you have a warm bath or shower. This is normal.
Building up your milk supply
Around two to four days after birth you may notice that your breasts become fuller and warmer. This is often referred to as your milk “coming in”.
Your milk will vary according to your baby’s needs. Each time your baby feeds, your body knows to make more milk for the next feed. The amount of milk you make will increase or decrease depending on how often your baby feeds.
In the early weeks, “topping up” with formula milk or giving your baby a dummy can lower your milk supply.
Feed your baby as often as they want and for as long as they want. This is called responsive feeding. In other words, responding to your baby’s needs. It’s also known as on-demand or baby-led feeding.
In the beginning, it can feel like you’re doing nothing but feeding. But gradually you and your baby will get into a pattern, and the amount of milk you produce will settle down.
It’s important to breastfeed at night because this is when you produce more hormones (prolactin) to build up your milk supply.
Ways to boost your breast milk supply
- Ask your midwife, health visitor or breastfeeding specialist to watch your baby feeding. They can offer guidance and support to help you properly position and attach your baby to the breast.
- Avoid giving your baby bottles of formula or a dummy until breastfeeding is well established. This usually takes a few weeks.
- Feed your baby as often as you and they want to.
- Expressing some breast milk after feeds once breastfeeding is established will help build up your supply.
- Offer both breasts at each feed and alternate which breast you start with.
- Keep your baby close to you and hold them skin to skin. This will help you spot signs your baby is ready to feed early on, before they start crying.
In rare cases, women may need to take a drug to help them produce more milk, but this isn’t usually necessary.
Breastfeeding positions
Some moms find that the following positions are helpful ways to get comfortable and support their babies while breastfeeding. You can also use pillows under your arms, elbows, neck, or back to give you added comfort and support. Keep trying different positions until you are comfortable. What works for one feeding may not work for the next feeding.
Clutch or “football” hold: useful if you had a C-section, or if you have large breasts, flat or inverted nipples, or a strong let-down reflex. This hold is also helpful for babies who like to be in a more upright position when they feed. Hold your baby at your side with the baby lying on his or her back and with his or her head at the level of your nipple. Support your baby’s head by placing the palm of your hand at the base of his or her head.
Cross-cradle or transitional hold: useful for premature babies or babies with a weak suck because this hold gives extra head support and may help the baby stay latched. Hold your baby along the area opposite from the breast you are using. Support your baby’s head at the base of his or her neck with the palm of your hand.
Cradle hold: an easy, common hold that is comfortable for most mothers and babies. Hold your baby with his or her head on your forearm and his or her body facing yours.
Laid-back hold (straddle hold): a more relaxed, baby-led approach. Lie back on a pillow. Lay your baby against your body with your baby’s head just above and between your breasts. Gravity and an instinct to nurse will guide your baby to your breast. As your baby searches for your breast, support your baby’s head and shoulders but don’t force the latch.
Side-lying position: useful if you had a C-section, but also allows you to rest while the baby breastfeeds. Lie on your side with your baby facing you. Pull your baby close so your baby faces your body.
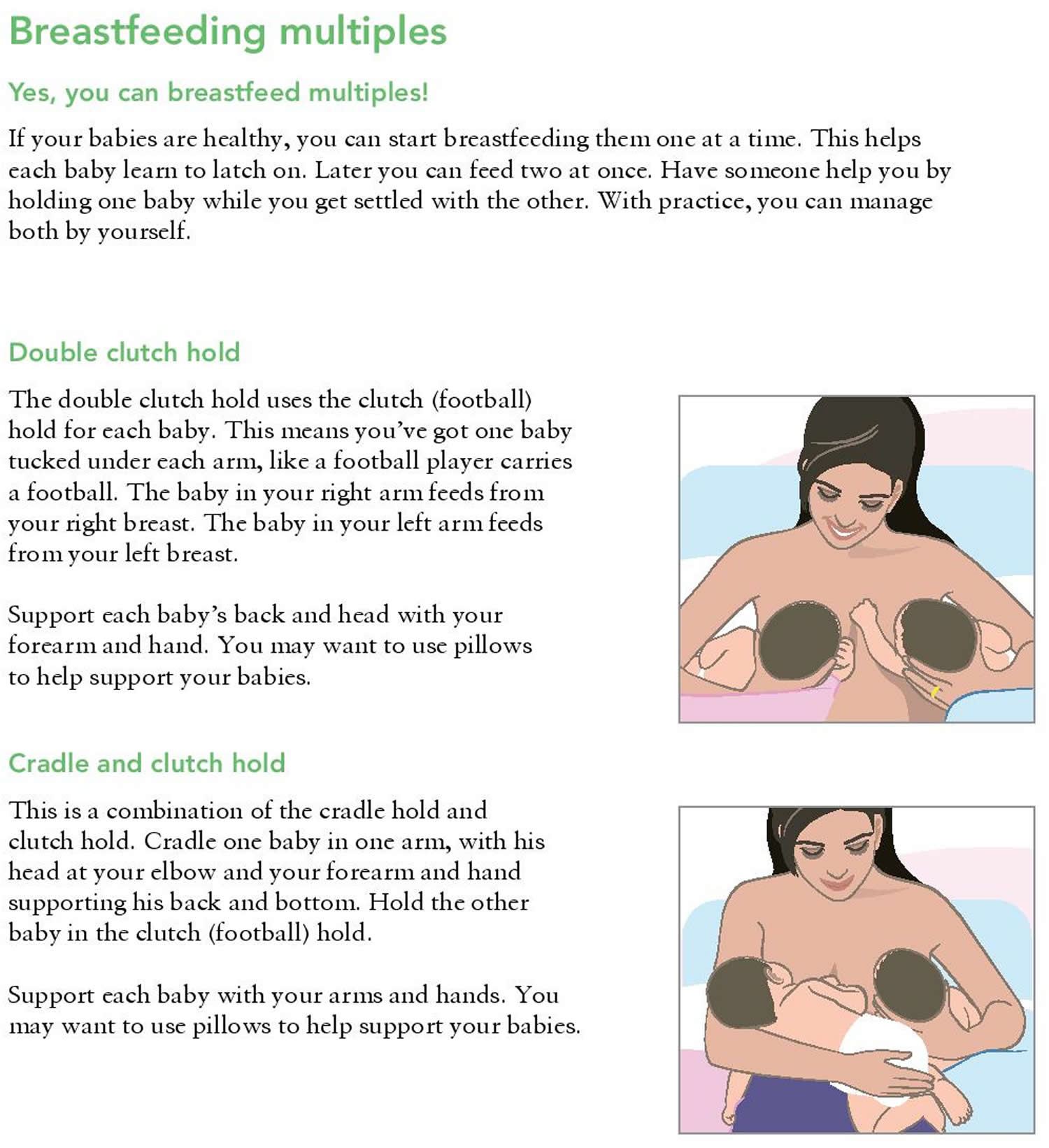
How to breastfeed twins, triplets or more
 Getting a good latch
Getting a good latch
Getting your baby to “latch on” properly can take some practice. You can try different breastfeeding holds to help your baby get a good latch.
The steps below can help your newborn latch on to the breast to start sucking when he or she is ready. Letting your baby begin the process of searching for the breast may take some of the pressure off you and keeps the baby calm and relaxed. This approach to learning to breastfeeding is a more relaxed, baby-led latch. Sometimes called biological nurturing, laid-back breastfeeding, or baby-led breastfeeding, this style of breastfeeding allows your baby to lead and follow his or her instincts to suck.
Keep in mind that there is no one way to start breastfeeding. As long as the baby is latched on well, how you get there is up to you.
- Create a calm environment first. Recline on pillows or other comfortable area. Be in a place where you can be relaxed and calm.
- Hold your baby skin-to-skin. Hold your baby, wearing only a diaper, against your bare chest. Hold the baby upright between your breasts and just enjoy your baby for a while with no thoughts of breastfeeding yet.
- Let your baby lead. If your baby is not hungry, she will stay curled up against your chest. If your baby is hungry, she will bob her head against you, try to make eye contact, and squirm around. Learn how to read your baby’s hunger signs.
- Support your baby, but don’t force the latch. Support her head and shoulders as she searches for your breast. Avoid the temptation to help her latch on.
- Allow your breast to hang naturally. When your baby’s chin hits your breast, the firm pressure makes her open her mouth wide and reach up and over the nipple. As she presses her chin into the breast and opens her mouth, she should get a deep latch. Keep in mind that your baby can breathe at the breast. The nostrils flare to allow air in.
If you have tried the “baby-led” approach and your baby is still having problems latching on, try these tips:
- Tickle the baby’s lips with your nipple to encourage him or her to open wide.
- Pull your baby close so that the baby’s chin and lower jaw moves in to your breast.
- Watch the baby’s lower lip and aim it as far from the base of the nipple as possible so that the baby takes a large mouthful of breast.
How to latch your baby on to your breast
- Hold your baby close to you with their nose level with the nipple.
- Wait until your baby opens their mouth really wide with their tongue down. You can encourage them to do this by gently stroking their top lip.
- Bring your baby on to your breast.
- Your baby will tilt their head back and come to your breast chin first. Remember to support your baby’s neck but not hold the back of their head. They should then be able to take a large mouthful of breast. Your nipple should go towards the roof of their mouth.
Step by Step Guide in Getting your baby into position
Breastfeeding – Step 1. Hold your baby’s whole body close with their nose level with your nipple.

Breastfeeding – Step 2. Let your baby’s head tip back a little so that their top lip can brush against your nipple. This should help your baby to make a wide open mouth.

Breastfeeding – Step 3. When your baby’s mouth opens wide, their chin should be able to touch your breast first, with their head tipped back so that their tongue can reach as much breast as possible.

Breastfeeding – Step 4. With your baby’s chin firmly touching your breast and their nose clear, their mouth should be wide open. You should see much more of the darker nipple skin above your baby’s top lip than below their bottom lip. Your baby’s cheeks will look full and rounded as they feed.

What are signs of a good latch?
Signs your baby is well attached to your breast
- The latch feels comfortable to you and does not hurt or pinch.
- Your baby’s chest rests against your body. Your baby does not have to turn his or her head while drinking.
- Your baby has a wide mouth and a large mouthful of breast.
- The baby’s tongue is cupped under the breast, so you might not see the baby’s tongue.
- You hear or see your baby swallow. Some babies swallow so quietly that a pause in their breathing may be the only sign of swallowing.
- You see the baby’s ears “wiggle” slightly.
- Your baby’s lips turn outward like fish lips, not inward. You may not even be able to see the baby’s bottom lip.
- Your baby’s chin is touching your breast, their lower lip is rolled down (you can’t always see this) and their nose isn’t squashed against your breast.
- You don’t feel any pain in your breasts or nipples when your baby is feeding, although the first few sucks may feel strong.
- You can see more of the dark skin around your nipple (areola) above your baby’s top lip than below their bottom lip, depending on the size of your areola and the size of your baby’s mouth.
What are some common breastfeeding latch problems?
Below are some common latch problems and how to deal with them.
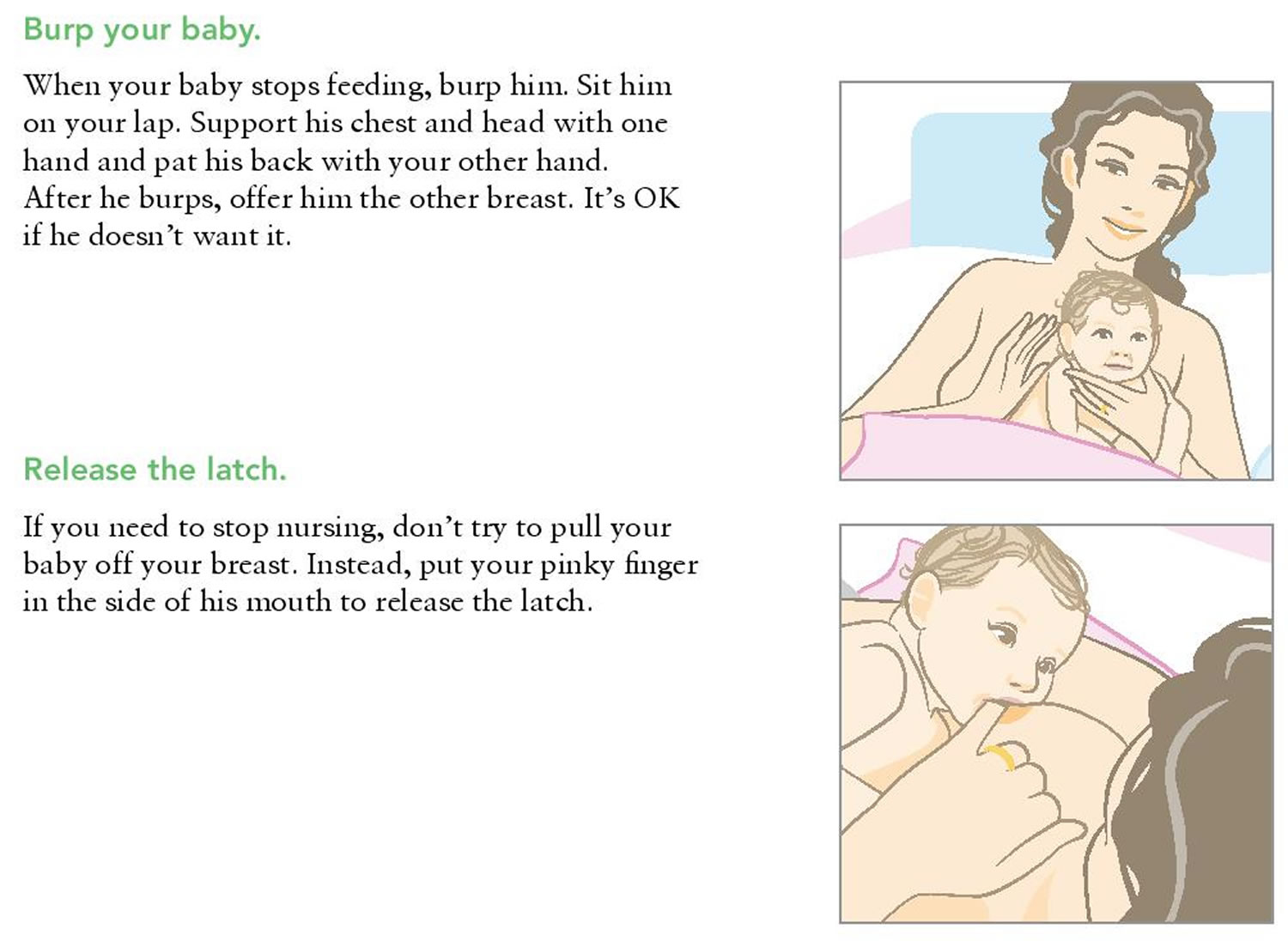
- You’re in pain. Many moms say their breasts feel tender when they first start breastfeeding. A mother and her baby need time to find comfortable breastfeeding positions and a good latch. If breastfeeding hurts, your baby may be sucking on only the nipple, and not also on the areola (the darker skin around the nipple). Gently break your baby’s suction to your breast by placing a clean finger in the corner of your baby’s mouth. Then try again to get your baby to latch on. To find out if your baby is sucking only on your nipple, check what your nipple looks like when it comes out of your baby’s mouth. Your nipple should not look flat or compressed. It should look round and long or the same shape as it was before the feeding.
- You or your baby feels frustrated. Take a short break and hold your baby in an upright position. Try holding your baby between your breasts with your skin touching his or her skin (called skin-to-skin). Talk or sing to your baby, or give your baby one of your fingers to suck on for comfort. Try to breastfeed again in a little while.
- Your baby has a weak suck or makes tiny sucking movements. Your baby may not have a deep enough latch to suck the milk from your breast. Gently break your baby’s suction to your breast by placing a clean finger in the corner of your baby’s mouth. Then try to get your baby to latch on again. Talk with a lactation consultant or pediatrician if you are not sure if your baby is getting enough milk. But don’t worry. A weak suck is rarely caused by a health problem.
- Your baby may be tongue-tied. Babies with a tight or short lingual frenulum (the piece of tissue attaching the tongue to the floor of the mouth) are described as “tongue-tied.” The medical term is ankyloglossia. These babies often find it hard to nurse. They may be unable to extend their tongue past their lower gum line or properly cup the breast during a feed. This can cause slow weight gain in the baby and nipple pain in the mother. If you think your baby may be tongue-tied, talk to your doctor.
How to tell if your baby is getting enough milk
- Your baby will appear content and satisfied after most feeds.
- They should be healthy and gaining weight (although it’s normal for babies to lose a little weight in the first days after birth). Talk to your midwife or health visitor if you are concerned your baby is not gaining weight and is unsettled during or after breast feeds.
- After the first few days, your baby should have at least six wet nappies a day.
- After the first few days, they should also pass at least two soft yellow poos (stools) every day.
How often you should feed your baby
How often babies feed varies. As a very rough guide, your baby should feed at least eight times or more every 24 hours during the first few weeks.
It’s fine to feed your baby whenever they are hungry, when your breasts feel full or if you just want to have a cuddle.
It’s not possible to overfeed a breastfed baby.
When your baby is hungry they may:
- get restless
- suck their fist or fingers
- make murmuring sounds
- turn their head and open their mouth (rooting)
It’s best to try and feed your baby during these early feeding cues as a crying baby is difficult to feed.
How to tell if your baby is getting enough milk
When you first start breastfeeding, you may be concerned your baby is not getting enough milk. You can’t always tell how much a breastfed baby is drinking.
It’s very rare that women don’t make enough breast milk for their babies, but it may take a little while before you feel confident your baby is getting what they need.
Your baby will generally let you know, but wet and dirty nappies are a good indication, as well as hearing your baby swallow.
If you need some reassurance your baby is getting enough milk, it’s a good idea to get a midwife, health visitor or breastfeeding specialist to watch your baby feed.
Try to carry on breastfeeding if you can. Introducing bottles of formula milk can fill up your baby’s stomach so they no longer want to breastfeed as frequently. This then reduces the stimulation for you to make more milk.
Signs your baby is getting enough milk
- Your baby starts feeds with a few rapid sucks followed by long, rhythmic sucks and swallows with occasional pauses.
- You can hear and see your baby swallowing.
- Your baby’s cheeks stay rounded, not hollow, during sucking.
- They seem calm and relaxed during feeds.
- Your baby comes off the breast on their own at the end of feeds.
- Their mouth looks moist after feeds.
- Your baby appears content and satisfied after most feeds.
- Your breasts feel softer after feeds.
- Your nipple looks more or less the same after feeds – not flattened, pinched or white.
- You may feel sleepy and relaxed after feeds.
Other signs your baby is feeding well
- Your baby gains weight steadily after the first two weeks – it’s normal for babies to lose some of their birth weight in the first two weeks.
- They appear healthy and alert when they’re awake.
- From the fourth day, they should do at least two soft, yellow poos (stools) every day for the first few weeks.
- From day five onwards, wet nappies should start to become more frequent, with at least six heavy, wet nappies every 24 hours. In the first 48 hours, your baby is likely to have only two or three wet nappies.
It can be hard to tell if disposable nappies are wet. To get an idea, take a nappy and add two to four tablespoons of water. This will give you an idea of what to look and feel for.
Things that can affect your milk supply
- Poor attachment and positioning.
- Not feeding your baby often enough.
- Drinking alcohol and smoking while breastfeeding – these can both interfere with your milk production.
- Previous breast surgery, particularly if your nipples have been moved.
- Having to spend time away from your baby after the birth – for example, because they were premature: Frequent gentle hand expression will help.
- Illness in you or your baby.
- Giving your baby bottles of formula or a dummy before breastfeeding is well established.
- Using nipple shields – although this may be the only way to feed your baby with damaged nipples and is preferable to stopping feeding.
- Some medications, including dopamine, ergotamine and pyridoxine.
- Anxiety, stress or depression.
- Your baby having a tongue tie that restricts the movement of their tongue.
With skilled help, lots of these problems can be sorted out. If you have concerns about how much milk your baby is getting, it’s important to ask for help early. Speak to your midwife, health visitor or a breastfeeding specialist. They can also tell you where you can get further support.
Dealing with leaking breasts
Sometimes, breast milk may leak unexpectedly from your nipples. Press the heel of your hand gently but firmly on your breast when this happens.
Wearing breast pads will stop your clothes becoming wet with breast milk. Remember to change them frequently to prevent any infection.
Expressing some milk may also help. Only express enough to feel comfortable as you don’t want to overstimulate your supply.
If your baby hasn’t fed recently you could offer them a feed as breastfeeding is also about you being comfortable.
Breastfeeding your premature baby
Your breast milk is important to your baby at any age. Research shows that giving your premature baby your breast milk benefits their health as well as yours.
Among other things, your breast milk:
- helps protect your baby from infections, particularly of their gut (premature babies are more prone to these)
- contains hormones, nutrients and growth factors that help your baby to grow and develop
- is easier for your baby to digest than formula milk, because it’s human milk specially designed by your body for your baby
If your baby is too small or sick to breastfeed, you’ll need to start regularly expressing your breast milk soon after they’re born to get your milk supply going. Then you can start breastfeeding once you and your baby are ready.
Even if you weren’t planning to breastfeed, you could express your breast milk for a while and see how it goes.
Spending lots of time close together can help boost your breast milk supply and establish breastfeeding.
As soon as possible, you’ll be encouraged to spend time holding your baby against your skin. This is sometimes called kangaroo care.
Your baby will be dressed just in a nappy and then placed inside your top or under a blanket so they can be held securely against your skin.
This skin-to-skin contact helps you feel close to your baby. Your partner can enjoy this kind of contact as well.
For your premature baby, skin-to-skin contact:
- reduces stress and/or pain
- promotes healthy weight gain
- helps to establish breastfeeding
- helps them adapt to their environment
- helps to regulate and support their heart rate and breathing
For mums, skin-to-skin contact:
- helps prevent postnatal depression
- increases your confidence as a new parent
- supports the hormones that help with breast milk production and supply
For dads, holding your baby skin to skin:
- helps you bond with your baby – babies can hear both parents’ voices in the womb and will be calmed by the sound of your voice as well as their mum’s
- helps you feel more confident as a parent
Expressing milk if your baby is premature
Always ask for help early if you have any worries or questions.
It’s recommended you express eight to 10 times a day to begin with, including at least once at night, to keep your milk supply up.
In the early days, it’s often easier to express your milk by hand. Your midwife or a breastfeeding supporter can show you how.
You’ll probably only express a few drops to begin with but, if you hand express often, this will increase.
In the early days you can collect your breast milk in a small, sterile cup and store it in a syringe. Every drop is beneficial for your baby.
Once you are producing more milk, you could try using a breast pump. If your baby is in a neonatal unit, the hospital will usually be able to lend you an electric breast pump for expressing your milk. If they can’t lend you one, you can hire one.
Problems and discomforts when breastfeeding
You want breastfeeding to be a calm, quiet time for you and your baby. But you may have some problems or discomforts when breastfeeding. Don’t let them get you down! They’re common for breastfeeding moms. And there are things you can do to help you feel better and make breastfeeding more comfortable.
If you have questions or need help with breastfeeding, tell your health care provider or a lactation consultant. A lactation consultant is a person with special training and education in helping women breastfeed.
What can you do if you’re sore after having a c-section?
A c-section (also called cesarean birth) is surgery in which your baby is born through a cut that your doctor makes in your belly and uterus (womb). You may be sore and tired after a c-section, but you can still breastfeed. Here’s what you can do:
- Use the side-lying and football holds for your baby when you breastfeed. Check out our breastfeeding feature to learn about ways to hold your baby during breastfeeding.
- Keep your baby with you in your hospital room so you don’t have to move around a lot to get her.
- Only take pain medicine that your health care provider gives you. She can make sure it’s safe for your baby during breastfeeding.
What to do if you have strong let-down reflex?
Some women have a strong milk ejection reflex or let-down. This can happen along with an oversupply of milk.
What you can do:
- Hold your nipple between your first and middle fingers or with the side of your hand. Lightly press on milk ducts to reduce the force of the milk ejection.
- If your baby chokes or sputters when breastfeeding, unlatch him or her and let the extra milk spray into a towel or cloth.
- Allow your baby to latch and unlatch from the breast whenever he or she wants to.
- Try positions that reduce the force of gravity, which can make milk spray worse. These positions include the side-lying position and the football hold. (See the Breastfeeding holds section for illustrations of these positions.)
What is breast engorgement?
This is when your breasts become swollen and full of milk. They may feel tender and sore. It is normal for your breasts to become larger, heavier, and a little tender when they begin making milk. Sometimes, this fullness may turn into engorgement, when your breasts feel very hard and painful. Engorgement is the result of the milk building up. It usually happens during the third to fifth day after giving birth. But it can happen at any time, especially if you have an oversupply of milk or are not feeding your baby or expressing your milk often.
Engorgement can also cause:
- Breast swelling
- Breast tenderness
- Warmth
- Redness
- Throbbing
- Flattening of the nipple
- Low-grade fever
Engorgement can lead to plugged ducts or a breast infection, so it is important to try to prevent it before this happens.
Most of the time the discomfort goes away once you start breastfeeding regularly. Here are some ways to help with engorgement:
- Try not to miss or go a long time between feedings. Don’t skip night feedings.
- Express a small amount of milk with a breast pump or by hand before breastfeeding.
- Take a warm shower or put warm towels on your breasts. If your engorgement is really painful, put cold packs on your breasts.
- Tell your provider if your breasts stay swollen.
What to do when you have oversupply of breast milk?
An overfull breast can make breastfeeding stressful and uncomfortable for you and your baby.
What you can do:
- Breastfeed on one side for each feeding. Continue to offer that same breast for at least two hours until the next full feeding, gradually increasing the length of time per feeding.
- If the other breast feels unbearably full before you are ready to breastfeed on it, hand express for a few moments to relieve some of the pressure. You can also use a cold compress or washcloth to reduce discomfort and swelling.
- Feed your baby before he or she becomes overly hungry to prevent aggressive sucking.
- Burp your baby often if he or she is gassy so there is more room in baby’s tummy for milk.
What to do if you think you have low milk supply?
Most mothers make plenty of milk for their babies. But many mothers worry about having enough milk. This video suggests that checking your baby’s weight and growth is the best way to make sure he or she gets enough milk. Let your baby’s doctor know if you are concerned.
For more ways to tell if your baby is getting enough milk, visit the How do I know if my baby is getting enough breastmilk? section.
There may be times when you think your supply is low, but it is actually just fine:
- When your baby is around 6 weeks to 2 months old, your breasts may no longer feel full. This is normal. At the same time, your baby may nurse for only five minutes at a time. This can mean that you and your baby are just getting used to breastfeeding — and getting good at it.
- Growth spurts can make your baby nurse longer and more often. These growth spurts often happen around 2 to 3 weeks, 6 weeks, and 3 months of age.
- Growth spurts can also happen at any time. Don’t be worried that your supply is too low to satisfy your baby. Follow your baby’s lead. Nursing more and more often will help increase your milk supply. Once your supply increases, you will probably be back to your usual routine.
What you can do:
- Make sure your baby is latched on and positioned well.
- Breastfeed often and let your baby decide when to end the feeding.
- Offer both breasts at each feeding. Have your baby stay at the first breast as long as he or she is still sucking and swallowing. Offer the second breast when the baby slows down or stops.
- Avoid giving your baby formula or cereal in addition to your breastmilk, especially in the first 6 months of life. Your baby may lose interest in your breastmilk, and your milk supply will decrease. If you need to supplement your baby’s feedings with more milk, try using a spoon, cup, or a dropper filled with pumped breastmilk.
Check with your doctor for health issues, such as hormonal issues or primary breast insufficiency, if the above steps don’t help.
What can you do about nipple pain?
Many women feel nipple pain when they first start breastfeeding. If your nipples are cracked and sore, you may need to change the position you use to breastfeed. If you have nipple pain:
- Make sure your baby is fully latched on. This means your baby’s mouth is securely attached to the area around your nipple for breastfeeding. If she’s not latched on, remove her from your breast and try again.
- After feeding, put some fresh breast milk on your nipples. Just like breast milk is good for your baby, it can help you, too. Or some creams can help. Ask your provider which kind to use.
- Help cracked nipples stay moist so you can continue breastfeeding. Try one or all of these tips:
- After breastfeeding, express a few drops of milk and gently rub the milk on your nipples with clean hands. Human milk has natural healing properties and contains oils that soothe.
- Use purified lanolin cream or ointment that is especially made for breastfeeding.
- Let your nipples air dry after feeding, or wear a soft cotton shirt.
- Talk to your provider or lactation consultant if the pain doesn’t go away.
What can you do if your breasts leak?
Your breasts may leak milk, especially right after birth. This is common and doesn’t hurt you or your baby. Here’s how to handle leaking breasts:
- Try not to miss feedings or go a long time between feedings. Don’t skip night feedings.
- Apply pressure to your breasts by crossing your arms over your chest.
- Use manual expression to remove milk from your breasts. Manual expression is when you massage your breasts with your hands to release breast milk. Ask your lactation consultant to show you how to manually express your breast milk.
- Put nursing pads in your bra to soak up leaked milk. Sleep in a nursing bra in case you have leakage at night.
What are plugged ducts?
Breast milk can get blocked in your breast ducts. Your breast may feel sore or look red. You may feel a hard spot in your breast. You may feel that your breast doesn’t empty when breastfeeding. Here’s what you can do to help with plugged ducts:
- Take a warm shower or put warm towels on your breast.
- Start each feeding on the sore breast. This may be uncomfortable, but it’s important to keep using the breast to unclog the duct.
- Massage the hard spot while your baby breastfeeds.
- Try manual expression to release milk from your breasts.
- Drink plenty of fluid.
- Don’t wear a bra that fits too tight or that has an underwire.
- Tell your provider if you develop a fever, chills, aches or pains. These could be signs of a breast infection.
What is mastitis?
Mastitis is a breast infection. It can happen when you have a plugged duct, you miss or delay breastfeedings or if your breasts become engorged. You may feel a tender or painful hard spot in your breast that’s warm to the touch. The area may be red. You may have a fever, chills, aches or pain. Here’s what you can to if you have a breast infection:
- Don’t stop nursing your baby even if your breast is sore. The infection doesn’t harm the baby. Breastfeeding more often can help clear the infection.
- Take a warm shower or put warm towels on your breast.
- Call your provider. You may need an antibiotic. This is medicine used to treat an infection.
- Drink plenty of fluid.
- Don’t wear a bra that fits too tight or a bra with an underwire.
What is fungal infection?
A fungal infection, also called a yeast infection or thrush, can form on your nipples or in your breast. This type of infection thrives on milk and is an overgrowth of the Candida organism. Candida lives in our bodies and is kept healthy and at the correct levels by the natural bacteria in our bodies. When the natural balance of bacteria is upset, Candida can overgrow, causing an infection.
A key sign of a fungal infection is sore nipples that last more than a few days, even after your baby has a good latch. Or you may suddenly get sore nipples after several weeks of pain-free breastfeeding. Other signs are pink, flaky, shiny, itchy, or cracked nipples or deep pink and blistered nipples. You could also have achy breasts or shooting pains deep in the breast during or after feedings.
Causes of fungal infection include:
- Thrush in your baby’s mouth, which can pass to you
- Nipples that are sore or cracked
- Receiving or taking antibiotics or steroids (often given to mothers during labor)
- A chronic illness like HIV, diabetes, or anemia
What you can do:
Fungal infections are treated with a medicine you rub on your breasts several times a day for about a week. It may take several weeks to clear up, so it is important to follow these tips to avoid spreading the infection:
- Change disposable nursing pads often.
- Wash any towels or clothing that comes in contact with the yeast in very hot water (above 122°F).
- Wear a clean bra every day.
- Wash your hands often.
- Wash your baby’s hands often, especially if he or she sucks on his or her fingers.
- Boil every day all pacifiers, bottle nipples, or toys your baby puts in his or her mouth. (To boil them, place them in a pot of water and heat the water to a rolling boil. Boil the items for about 10 minutes.)
- After one week of treatment, throw away all pacifiers and nipples and buy new ones.
- Every day, boil all breast pump parts that touch your milk.
- Make sure other family members do not have thrush or other fungal infections. If they have symptoms, do not let them care for you or your baby until they get treated.
What is nipple confusion?
Nipple confusion can happen if you give your baby a bottle or pacifier in the first few weeks of breastfeeding. He may forget how to latch on to your breast. Or he may not want to breastfeed at all. If this happens, you baby may not get all the breast milk he needs. And your breasts may become engorged. To help prevent nipple confusion:
- Only breastfeed your baby in the first few weeks after birth. Don’t use bottles or pacifiers until your baby’s breastfeeding well. The American Academy of Pediatrics recommends that if you’re breastfeeding, wait until your baby is 1 month old before using a pacifier.
- Tell your provider or lactation consultant if you think your baby has nipple confusion.
What are inverted, flat, or very large nipples?
Some women have nipples that turn inward instead of pointing outward or are flat and do not protrude. Nipples can also sometimes flatten for a short time because of engorgement or swelling from breastfeeding. Inverted or flat nipples can sometimes make it harder to breastfeed. For breastfeeding to work your baby must latch on to both the nipple and the breast, so even inverted nipples can work just fine. Often, flat and inverted nipples will protrude more over time as the baby sucks more.
Very large nipples can make it hard for the baby to get enough of the areola into his or her mouth to compress the milk ducts and get enough milk.
What you can do:
- Talk to your doctor or a lactation consultant if you are concerned about your nipples.
- You can use your fingers to try to pull your nipples out. You can also talk to your doctor or nurse about using a device that gently suctions or pulls out inverted or temporarily flattened nipples.
- The latch for babies of mothers with very large nipples will improve with time as the baby grows. It might take several weeks to get the baby to latch well. But if you have a good milk supply, your baby will get enough milk even with a latch that isn’t perfect.
What is nursing strike?
A nursing “strike” is when your baby has been breastfeeding well for months and then suddenly begins to refuse the breast. A nursing strike can mean that your baby is trying to let you know that something is wrong. This usually does not mean that the baby is ready to wean (stop breastfeeding totally).
Not all babies will react the same way to the different things that can cause a nursing strike. Some babies will continue to breastfeed without a problem. Other babies may just become fussy at the breast. And other babies will refuse the breast entirely.
Some of the major causes of a nursing strike include:
- Having mouth pain from teething, a fungal infection like thrush, or a cold sore
- Having an ear infection, which causes pain while sucking or pressure while lying on one side
- Feeling pain from a certain breastfeeding position, perhaps from an injury on the baby’s body or from soreness from an immunization
- Being upset about a long separation from the mother or a major change in routine
- Being distracted while breastfeeding, such as becoming interested in other things going on around the baby
- Having a cold or stuffy nose that makes breathing while breastfeeding difficult
- Getting less milk from the mother after supplementing breastmilk with bottles or overuse of a pacifier
- Responding to the mother’s strong reaction if the baby has bitten her while breastfeeding
- Being upset by hearing arguing or people talking in a harsh voice while breastfeeding
- Reacting to stress, overstimulation, or having been repeatedly put off when wanting to breastfeed
If your baby is on a nursing strike, it is normal to feel frustrated and upset, especially if your baby is unhappy. Be patient with your baby and keep trying to offer your breasts. You may also want to pump your breastmilk to offer during the strike and to make sure you do not get engorged.
What you can do:
- Try to hand express or pump your milk as often as the baby used to breastfeed, to prevent engorgement and plugged ducts.
- Try another feeding method temporarily to give your baby your breastmilk, such as using a cup, dropper, or spoon.
- Keep track of your baby’s wet and dirty diapers to make sure he or she is getting enough milk.
- Keep offering your breast to your baby. If your baby is frustrated, stop and try again later. You can also try offering your breast when your baby is very sleepy or is sleeping.
- Try breastfeeding positions where your bare skin is pressed next to your baby’s bare skin.
- Focus on your baby, and comfort him or her with extra touching and cuddling.
- Try breastfeeding while rocking your baby in a quiet room without distractions.
Benefits of breastfeeding
Breastfeeding results in improved infant and maternal health outcomes in both the industrialized and developing world.
To date, the most comprehensive publication that reviews and analyzes the published scientific literature that compares breastfeeding and commercial infant formula feeding as to health outcomes is the report prepared by the Evidence-based Practice Centers of the Agency for Healthcare Research and Quality (AHRQ) of the US Department of Health Human Services titled Breastfeeding and Maternal and Infant Health Outcomes in Developed Countries.13 The following sections summarize and update the AHRQ meta-analyses and provide an expanded analysis regarding health outcomes. Table 2 summarizes the dose-response relationship between the duration of breastfeeding and its protective effect.
Table 1. Dose-Response Benefits of Breastfeeding
| Condition | % Lower Risk (b) | Breastfeeding | Comments |
| Otitis media 30) | 23 | Any | — |
| Otitis media 31) | 50 | ≥3 or 6 months | Exclusive breastfeeding |
| Recurrent otitis media 32) | 77 | Exclusive breastfeeding ≥6 months (d) | Compared with breastfeeding 4 to <6 months (d) |
| Upper respiratory tract infection 33) | 63 | >6 months | Exclusive breastfeeding |
| Lower respiratory tract infection 34) | 72 | ≥4 months | Exclusive breastfeeding |
| Lower respiratory tract infection 35) | 77 | Exclusive breastfeeding ≥6 months (d) | Compared with BF 4 to <6 months (d) |
| Asthma 36) | 40 | ≥3 months | Atopic family history |
| Asthma 37) | 26 | ≥3 months | No atopic family history |
| RSV bronchiolitis 38) | 74 | >4 months | — |
| Necrotizing enterocolitis 39) | 77 | Neonatal intensive care unit (NICU) stay | Preterm infants Exclusive human milk |
| Atopic dermatitis 40) | 27 | >3 months | Exclusive breastfeeding negative family history |
| Atopic dermatitis 41) | 42 | >3 months | Exclusive breastfeeding positive family history |
| Gastroenteritis 42) | 64 | Any | — |
| Inflammatory bowel disease 32 | 31 | Any | — |
| Obesity 43) | 24 | Any | — |
| Celiac disease 44) | 52 | >2 months | Gluten exposure when breastfeeding |
| Type 1 diabetes 45) | 30 | >3 months | Exclusive breastfeeding |
| Type 2 diabetes 46) | 40 | Any | — |
| Leukemia (ALL) 47) | 20 | >6 months | — |
| Leukemia (AML) 48) | 15 | >6 months | — |
| Sudden infant death syndrome (SIDS) 49) | 36 | Any >1 months | — |
Footnotes:
Abbreviations: ALL, acute lymphocytic leukemia; AML, acute myelogenous leukemia; BF, breastfeeding; HM, human milk; RSV, respiratory syncytial virus.
a Pooled data.
b % lower risk refers to lower risk while breastfeeding compared with feeding commercial infant formula or referent group specified.
c Odds ratio expressed as increase risk for commercial formula feeding.
d Referent group is exclusive breastfeeding ≥6 months.
[Source 50)]Infant Outcomes
Respiratory Tract Infections and Otitis Media
The risk of hospitalization for lower respiratory tract infections in the first year is reduced 72% if infants breastfed exclusively for more than 4 months 51). Infants who exclusively breastfed for 4 to 6 months had a fourfold increase in the risk of pneumonia compared with infants who exclusively breastfed for more than 6 months 52). The severity (duration of hospitalization and oxygen requirements) of respiratory syncytial virus bronchiolitis is reduced by 74% in infants who breastfed exclusively for 4 months compared with infants who never or only partially breastfed 53).
Any breastfeeding compared with exclusive commercial infant formula feeding will reduce the incidence of otitis media by 23% 54). Exclusive breastfeeding for more than 3 months reduces the risk of otitis media by 50%. Serious colds and ear and throat infections were reduced by 63% in infants who exclusively breastfed for 6 months 55).
Gastrointestinal Tract Infections
Any breastfeeding is associated with a 64% reduction in the incidence of nonspecific gastrointestinal tract infections, and this effect lasts for 2 months after cessation of breastfeeding 56).
Necrotizing Enterocolitis
Meta-analyses of 4 randomized clinical trials performed over the period 1983 to 2005 support the conclusion that feeding preterm infants human milk is associated with a significant reduction (58%) in the incidence of necrotizing enterocolitis 57). A more recent study of preterm infants fed an exclusive human milk diet compared with those fed human milk supplemented with cow-milk-based infant formula products noted a 77% reduction in necrotizing enterocolitis 58). One case of necrotizing enterocolitis could be prevented if 10 infants received an exclusive human milk diet, and 1 case of necrotizing enterocolitis requiring surgery or resulting in death could be prevented if 8 infants received an exclusive human milk diet 59).
Sudden Infant Death Syndrome and Infant Mortality
Meta-analyses with a clear definition of degree of breastfeeding and adjusted for confounders and other known risks for sudden infant death syndrome (SIDS) note that breastfeeding is associated with a 36% reduced risk of SIDS 60). Latest data comparing any versus exclusive breastfeeding reveal that for any breastfeeding, the multivariate odds ratio (OR) is 0.55. When computed for exclusive breastfeeding, the OR is 0.27 61). A proportion (21%) of the US infant mortality has been attributed, in part, to the increased rate of SIDS in infants who were never breastfed 62). That the positive effect of breastfeeding on SIDS rates is independent of sleep position was confirmed in a large case-control study of supine-sleeping infants 63).
It has been calculated that more than 900 infant lives per year may be saved in the United States if 90% of mothers exclusively breastfed for 6 months 64). In the 42 developing countries in which 90% of the world’s childhood deaths occur, exclusive breastfeeding for 6 months and weaning after 1 year is the most effective intervention, with the potential of preventing more than 1 million infant deaths per year, equal to preventing 13% of the world’s childhood mortality 65).
Allergic Disease
There is a protective effect of exclusive breastfeeding for 3 to 4 months in reducing the incidence of clinical asthma, atopic dermatitis, and eczema by 27% in a low-risk population and up to 42% in infants with positive family history 66). There are conflicting studies that examine the timing of adding complementary foods after 4 months and the risk of allergy, including food allergies, atopic dermatitis, and asthma, in either the allergy-prone or nonatopic individual 67). Similarly, there are no convincing data that delaying introduction of potentially allergenic foods after 6 months has any protective effect 68). One problem in analyzing this research is the low prevalence of exclusive breastfeeding at 6 months in the study populations. Thus, research outcomes in studies that examine the development of atopy and the timing of introducing solid foods in partially breastfed infants may not be applicable to exclusively breastfed infants.
Celiac Disease
There is a reduction of 52% in the risk of developing celiac disease in infants who were breastfed at the time of gluten exposure 69). Overall, there is an association between increased duration of breastfeeding and reduced risk of celiac disease when measured as the presence of celiac antibodies. The critical protective factor appears to be not the timing of the gluten exposure but the overlap of breastfeeding at the time of the initial gluten ingestion. Thus, gluten-containing foods should be introduced while the infant is receiving only breast milk and not infant formula or other bovine milk products.
Inflammatory Bowel Disease
Breastfeeding is associated with a 31% reduction in the risk of childhood inflammatory bowel disease 70). The protective effect is hypothesized to result from the interaction of the immunomodulating effect of human milk and the underlying genetic susceptibility of the infant. Different patterns of intestinal colonization in breastfed versus commercial infant formula–fed infants may add to the preventive effect of human milk 71).
Obesity
Because rates of obesity are significantly lower in breastfed infants, national campaigns to prevent obesity begin with breastfeeding support 72). Although complex factors confound studies of obesity, there is a 15% to 30% reduction in adolescent and adult obesity rates if any breastfeeding occurred in infancy compared with no breastfeeding 73). The Framingham Offspring study noted a relationship of breastfeeding and a lower body mass index (BMI) and higher high-density lipoprotein concentration in adults 74). A sibling difference model study noted that the breastfed sibling weighed 14 pounds less than the sibling fed commercial infant formula and was less likely to reach BMI obesity threshold 75). The duration of breastfeeding also is inversely related to the risk of overweight; each month of breastfeeding being associated with a 4% reduction in risk 76).
The interpretation of these data is confounded by the lack of a definition in many studies of whether human milk was given by breastfeeding or by bottle. This is of particular importance, because breastfed infants self-regulate intake volume irrespective of maneuvers that increase available milk volume, and the early programming of self-regulation, in turn, affects adult weight gain 77). This concept is further supported by the observations that infants who are fed by bottle, formula, or expressed breast milk will have increased bottle emptying, poorer self-regulation, and excessive weight gain in late infancy (older than 6 months) compared with infants who only nurse from the breast 78).
Diabetes
Up to a 30% reduction in the incidence of type 1 diabetes mellitus is reported for infants who exclusively breastfed for at least 3 months, thus avoiding exposure to cow milk protein 79). It has been postulated that the putative mechanism in the development of type 1 diabetes mellitus is the infant’s exposure to cow milk β-lactoglobulin, which stimulates an immune-mediated process cross-reacting with pancreatic β cells. A reduction of 40% in the incidence of type 2 diabetes mellitus is reported, possibly reflecting the long-term positive effect of breastfeeding on weight control and feeding self-regulation 80).
Childhood Leukemia and Lymphoma
There is a reduction in leukemia that is correlated with the duration of breastfeeding 81). A reduction of 20% in the risk of acute lymphocytic leukemia and 15% in the risk of acute myeloid leukemia in infants breastfed for 6 months or longer 82). Breastfeeding for less than 6 months is protective but of less magnitude (approximately 12% and 10%, respectively). The question of whether the protective effect of breastfeeding is a direct mechanism of human milk on malignancies or secondarily mediated by its reduction of early childhood infections has yet to be answered.
Neurodevelopmental Outcomes
Consistent differences in neurodevelopmental outcome between breastfed and commercial infant formula–fed infants have been reported, but the outcomes are confounded by differences in parental education, intelligence, home environment, and socioeconomic status 83). The large, randomized Promotion of Breastfeeding Intervention Trial provided evidence that adjusted outcomes of intelligence scores and teacher’s ratings are significantly greater in breastfed infants 84). In addition, higher intelligence scores are noted in infants who exclusively breastfed for 3 months or longer, and higher teacher ratings were observed if exclusive breastfeeding was practiced for 3 months or longer. Significantly positive effects of human milk feeding on long-term neurodevelopment are observed in preterm infants, the population more at risk for these adverse neurodevelopmental outcomes 85).
Preterm Infants
There are several significant short- and long-term beneficial effects of feeding preterm infants human milk. Lower rates of sepsis and necrotizing enterocolitis indicate that human milk contributes to the development of the preterm infant’s immature host defense 86). The benefits of feeding human milk to preterm infants are realized not only in the neonatal intensive care unit (NICU) but also in the fewer hospital readmissions for illness in the year after neonatal intensive care unit (NICU) discharge 87). Furthermore, the implications for a reduction in incidence of necrotizing enterocolitis include not only lower mortality rates but also lower long-term growth failure and neurodevelopmental disabilities.60,61 Clinical feeding tolerance is improved, and the attainment of full enteral feeding is hastened by a diet of human milk 88).
Neurodevelopmental outcomes are improved by the feeding of human milk. Long-term studies at 8 years of age through adolescence suggest that intelligence test results and white matter and total brain volumes are greater in subjects who had received human milk as infants in the neonatal intensive care unit (NICU) 89). Extremely preterm infants receiving the greatest proportion of human milk in the neonatal intensive care unit (NICU) had significantly greater scores for mental, motor, and behavior ratings at ages 18 months and 30 months 90). These data remain significant after adjustment for confounding factors, such as maternal age, education, marital status, race, and infant morbidities. These neurodevelopmental outcomes are associated with predominant and not necessarily exclusive human milk feeding. Human milk feeding in the neonatal intensive care unit (NICU) also is associated with lower rates of severe retinopathy of prematurity 91). Long-term studies of preterm infants also suggest that human milk feeding is associated with lower rates of metabolic syndrome, and in adolescents, it is associated with lower blood pressures and low-density lipoprotein concentrations and improved leptin and insulin metabolism 92).
The potent benefits of human milk are such that all preterm infants should receive human milk (Table 2). Mother’s own milk, fresh or frozen, should be the primary diet, and it should be fortified appropriately for the infant born weighing less than 1.5 kg. If mother’s own milk is unavailable despite significant lactation support, pasteurized donor milk should be used 93). Quality control of pasteurized donor milk is important and should be monitored. New data suggest that mother’s own milk can be stored at refrigerator temperature (4°C) in the NICU for as long as 96 hours 94). Data on thawing, warming, and prolonged storage need updating. Practices should involve protocols that prevent misadministration of milk.
Table 2. Recommendations on Breastfeeding Management for Preterm Infants
| 1. All preterm infants should receive human milk. |
| • Human milk should be fortified, with protein, minerals, and vitamins to ensure optimal nutrient intake for infants weighing <1500 g at birth. |
| • Pasteurized donor human milk, appropriately fortified, should be used if mother’s own milk is unavailable or its use is contraindicated. |
| 2. Methods and training protocols for manual and mechanical milk expression must be available to mothers. |
| 3. Neonatal intensive care units should possess evidence-based protocols for collection, storage, and labeling of human milk 95). |
| 4. Neonatal intensive care units should prevent the misadministration of human milk 96) |
| 5. There are no data to support routinely culturing human milk for bacterial or other organisms 97) |
Maternal Outcomes
Both short- and long-term health benefits accrue to mothers who breastfeed. Such mothers have decreased postpartum blood loss and more rapid involution of the uterus. Continued breastfeeding leads to increased child spacing secondary to lactational amenorrhea. Prospective cohort studies have noted an increase in postpartum depression in mothers who do not breastfeed or who wean early 99). A large prospective study on child abuse and neglect perpetuated by mothers found, after correcting for potential confounders, that the rate of abuse/neglect was significantly increased for mothers who did not breastfeed as opposed to those who did 100).
Studies of the overall effect of breastfeeding on the return of the mothers to their pre-pregnancy weight are inconclusive, given the large numbers of confounding factors on weight loss (diet, activity, baseline BMI, ethnicity) 101). In a covariate-adjusted study of more than 14 000 women postpartum, mothers who exclusively breastfed for longer than 6 months weighed 1.38 kg less than those who did not breastfeed 102). In mothers without a history of gestational diabetes, breastfeeding duration was associated with a decreased risk of type 2 diabetes mellitus; for each year of breastfeeding, there was a decreased risk of 4% to 12% 103). No beneficial effect for breastfeeding was noted in mothers who were diagnosed with gestational diabetes.
The longitudinal Nurses Health Study noted an inverse relationship between the cumulative lifetime duration of breastfeeding and the development of rheumatoid arthritis 104). If cumulative duration of breastfeeding exceeded 12 months, the relative risk of rheumatoid arthritis was 0.8, and if the cumulative duration of breastfeeding was longer than 24 months, the relative risk of rheumatoid arthritis was 0.5 105). An association between cumulative lactation experience and the incidence of adult cardiovascular disease was reported by the Women’s Health Initiative in a longitudinal study of more than 139 000 postmenopausal women 106). Women with a cumulative lactation history of 12 to 23 months had a significant reduction in hypertension (high blood pressure), hyperlipidemia, cardiovascular disease, and diabetes.
Cumulative lactation experience also correlates with a reduction in both breast (primarily premenopausal) and ovarian cancer 107). Cumulative duration of breastfeeding of longer than 12 months is associated with a 28% decrease in breast cancer and ovarian cancer 108). Each year of breastfeeding has been calculated to result in a 4.3% reduction in breast cancer 109).
Economic Benefits
A detailed pediatric cost analysis based on the Agency for Healthcare Research and Quality report concluded that if 90% of US mothers would comply with the recommendation to breastfeed exclusively for 6 months, there would be a savings of $13 billion per year 110). The savings do not include those related to a reduction in parental absenteeism from work or adult deaths from diseases acquired in childhood, such as asthma, type 1 diabetes mellitus, or obesity-related conditions. Strategies that increase the number of mothers who breastfeed exclusively for about 6 months would be of great economic benefit on a national level.
How does breastfeeding benefit society?
Society benefits overall when mothers breastfeed.
- Breastfeeding saves lives. Research shows that if 90% of families breastfed exclusively for six months, nearly 1,000 deaths among infants could be prevented each year 111).
- Breastfeeding saves money. Medical costs may be lower for fully breastfed infants than never-breastfed infants. Breastfed infants usually need fewer sick care visits, prescriptions, and hospitalizations.
- Breastfeeding also helps make a more productive workforce. Mothers who breastfeed may miss less work to care for sick infants than mothers who feed their infants formula. Employer medical costs may also be lower 112).
- Breastfeeding is better for the environment. Formula cans and bottle supplies create more trash and plastic waste. Your milk is a renewable resource that comes packaged and warmed.
Contraindications to Breastfeeding
There are a limited number of medical conditions in which breastfeeding is contraindicated, including an infant with the metabolic disorder of classic galactosemia. Alternating breastfeeding with special protein-free or modified formulas can be used in feeding infants with other metabolic diseases (such as phenylketonuria), provided that appropriate blood monitoring is available. Mothers who are positive for human T-cell lymphotrophic virus type I or II 113) or untreated brucellosis 114) should not breastfeed nor provide expressed milk to their infants. Breastfeeding should not occur if the mother has active (infectious) untreated tuberculosis or has active herpes simplex lesions on her breast; however, expressed milk can be used because there is no concern about these infectious organisms passing through the milk. Breastfeeding can be resumed when a mother with tuberculosis is treated for a minimum of 2 weeks and is documented that she is no longer infectious 115). Mothers who develop varicella 5 days before through 2 days after delivery should be separated from their infants, but their expressed milk can be used for feeding 116). In 2009, the CDC recommended that mothers acutely infected with H1N1 influenza should temporarily be isolated from their infants until they are afebrile, but they can provide expressed milk for feeding 117).
In the industrialized world, it is not recommended that HIV-positive mothers breastfeed. However, in the developing world, where mortality is increased in non-breastfeeding infants from a combination of malnutrition and infectious diseases, breastfeeding may outweigh the risk of the acquiring HIV infection from human milk. Infants in areas with endemic HIV who are exclusively breastfed for the first 3 months are at a lower risk of acquiring HIV infection than are those who received a mixed diet of human milk and other foods and/or commercial infant formula 118). Recent studies document that combining exclusive breastfeeding for 6 months with 6 months of antiretroviral therapy significantly decreases the postnatal acquisition of HIV-1 119).
There is no contraindication to breastfeeding for a full-term infant whose mother is seropositive for cytomegalovirus (CMV). There is a possibility that cytomegalovirus (CMV) acquired from mother’s milk may be associated with a late-onset sepsis-like syndrome in the extremely low birth weight (birth weight <1500 g) preterm infant. Although not associated with long-term abnormalities, such a syndrome may warrant antiviral therapy 120). The value of routinely feeding human milk from seropositive mothers to preterm infants outweighs the risks of clinical disease, especially because no long-term neurodevelopmental abnormalities have been reported 121). Freezing of milk reduces but does not eliminate CMV 122). Heating, either as Holder pasteurization (heating at 62.5°C for 30 minutes) or high-temperature short pasteurization (72°C for 5–10 seconds) eliminates the viral load from the milk but also affects bioactive factors and nutrients 123). Thus, fresh mother’s own milk is preferable for routinely feeding all preterm infants.
- Tobacco — you know that it is best for your health and that of your baby to avoid smoking tobacco, but if you cannot resist, keep the number of cigarettes as low as possible (preferably less than ½ pack per day) and never smoke around your baby. Nicotine gets into your breast milk, so try to wait several hours after you smoke before nursing your baby. Second hand smoke increases your baby’s risk for ear and respiratory infections, asthma, and even sudden infant death syndrome (SIDS). The immunoglobulins in your milk help to lessen those risks, which is why most experts still recommend breastfeeding even if a woman is smoking small amounts of tobacco.
- Marijuana – Tetrahydrocannabinol (THC), the active ingredient in marijuana, passes into breast milk. Marijuana production is not very well regulated, so there may be other dangerous contaminants. There are not many studies regarding use of marijuana and breastfeeding, but there are concerns that exposure to tetrahydrocannabinol (THC) via breast milk might affect baby’s development. Tetrahydrocannabinol (THC) can also reduce your milk supply. Until more is known, it is recommended that marijuana be avoided in breastfeeding women, and that an effort also be made not to expose the infant to second hand marijuana smoke. If you happen to use marijuana, waiting 1-2 days before resuming nursing will help reduce the amount in milk. Pump and throw away breast milk in the meantime for comfort and to maintain your breast milk supply.
Maternal substance abuse is not a categorical contraindication to breastfeeding. Adequately nourished narcotic-dependent mothers can be encouraged to breastfeed if they are enrolled in a supervised methadone maintenance program and have negative screening for HIV and illicit drugs 124). Street drugs such as PCP (phencyclidine), cocaine, and cannabis can be detected in human milk, and their use by breastfeeding mothers is of concern, particularly with regard to the infant’s long-term neurobehavioral development and thus are contraindicated 125). Alcohol is not a galactogogue; it may blunt prolactin response to suckling and negatively affects infant motor development 126). Thus, ingestion of alcoholic beverages should be minimized and limited to an occasional intake but no more than 0.5 g alcohol per kg body weight, which for a 60 kg mother is approximately 2 oz liquor, 8 oz wine, or 2 beers 127). Nursing should take place 2 hours or longer after the alcohol intake to minimize its concentration in the ingested milk 128). Maternal smoking is not an absolute contraindication to breastfeeding but should be strongly discouraged, because it is associated with an increased incidence in infant respiratory allergy 129) and SIDS 130). Smoking should not occur in the presence of the infant so as to minimize the negative effect of secondary passive smoke inhalation 131). Smoking is also a risk factor for low milk supply and poor weight gain 132).
Alcohol and breastfeeding
Alcohol, marijuana and tobacco are ‘recreational drugs’ because there is not any medical reason to use them.
“The effects of alcohol on the breastfeeding baby are directly related to the amount the mother ingests. When the breastfeeding mother drinks occasionally or limits her consumption to one drink or less per day, the amount of alcohol her baby receives has not been proven to be harmful” 133).
Alcohol — alcohol of all kinds (wine, beer, liquor) passes into your breast milk. Babies don’t like the taste of it, and, if it happens often enough, babies may show developmental delays from exposures to alcohol through breast milk. Fortunately, waiting 2-3 hours after drinking a single alcoholic beverage results in lower amounts in breast milk. If you have two drinks, wait 4-6 hours – you get the idea. You can pump for comfort and to maintain your milk supply, but be sure to throw away the breast milk since it likely has alcohol in it. Chronic or heavy users of alcohol probably should not breastfeed.
If consumed in large amounts alcohol can cause drowsiness, deep sleep, weakness, and abnormal weight gain in the infant, and the possibility of decreased milk-ejection reflex in the mother. Mothers who have been drinking should not bed-share with their babies as their natural reflexes will be affected.
Important Considerations
- Your baby’s age
- A newborn has an immature liver, and will be more affected by alcohol
- Up until around three months of age, infants metabolize alcohol at about half the rate of adults
- An older baby can metabolize alcohol more quickly than a young infant
- Your weight
- A person’s size has an impact on how quickly they metabolize alcohol
- A heavier person can metabolize alcohol more quickly than a lighter person
- Amount of alcohol
- The effect of alcohol on the baby is directly related to the amount of alcohol that is consumed
- The more alcohol consumed, the longer it takes to clear the body
- Will you be eating
- An alcoholic drink consumed with food decreases absorption.
Weighing the Risks and Benefits of drinking while breastfeeding
Many mothers find themselves in a situation where they may want to drink. Maybe you are going to an event where wine will be served. Or perhaps you are going out with friends, or on a date. No matter the reason, you may have concerns about drinking and any possible effects on your baby. It is a good idea to weigh the benefits of breastfeeding against the benefits and possible risks of consuming alcohol. You might find the following suggestions helpful.
- Plan Ahead
If you want to drink, but are concerned about the effect on your baby, you can store some expressed breastmilk for the occasion
You can choose to wait for the alcohol to clear your system before nursing
If your breasts become full while waiting for the alcohol to clear, you can hand express or pump, discarding the milk that you express
- Alternatives
If you’re concerned about consuming alcohol while breastfeeding you might prefer to stick to non-alcoholic drinks instead.
If you are sober enough to drive you should be sober enough to breastfeed.
Bottom line, by breastfeeding, you’re already taking the first step in providing continued important nutrition for your baby. Taking steps to make sure your breast milk stays as healthy as possible for the entire time you breastfeed will be well worth the effort. Stay strong, live well.
Can drinking an alcoholic beverage help me relax and stimulate milk production?
Alcohol consumption has not been shown to stimulate milk production. Studies have found that babies nurse more frequently, but consume less milk in the 3-4 hours after an alcoholic beverage is consumed.
Do I have to pump and dump after drinking an alcoholic beverage?
As alcohol leaves your bloodstream, it leaves your breastmilk. Since alcohol is not “trapped” in breastmilk (it returns to the bloodstream as mother’s blood alcohol level declines), pumping and dumping will not remove it. Pumping and dumping, drinking a lot of water, resting, or drinking coffee will not speed up the rate of the elimination of alcohol from your body.
What if I get drunk?
Mothers who are intoxicated should not breastfeed until they are completely sober, at which time most of the alcohol will have left the mother’s blood. Drinking to the point of intoxication, or binge drinking, by breastfeeding mothers has not been adequately studied. Since all of the risks are not understood, drinking to the point of intoxication is not advised.
Can alcohol abuse affect a breastfed baby?
Yes. Alcohol abuse (excessive drinking) by the mother can result in slow weight gain or failure to thrive in her baby. The let-down of a mother who abuses alcohol may be affected by her alcohol consumption, and she may not breastfeed enough. The baby may sleep excessively, or may not suck effectively leading to decreased milk intake. The baby may even suffer from delayed motor development. If you are concerned that you or someone you know is drinking alcohol excessively, contact your healthcare professional.
References [ + ]





{kind=link}