Contents
What is circumcision
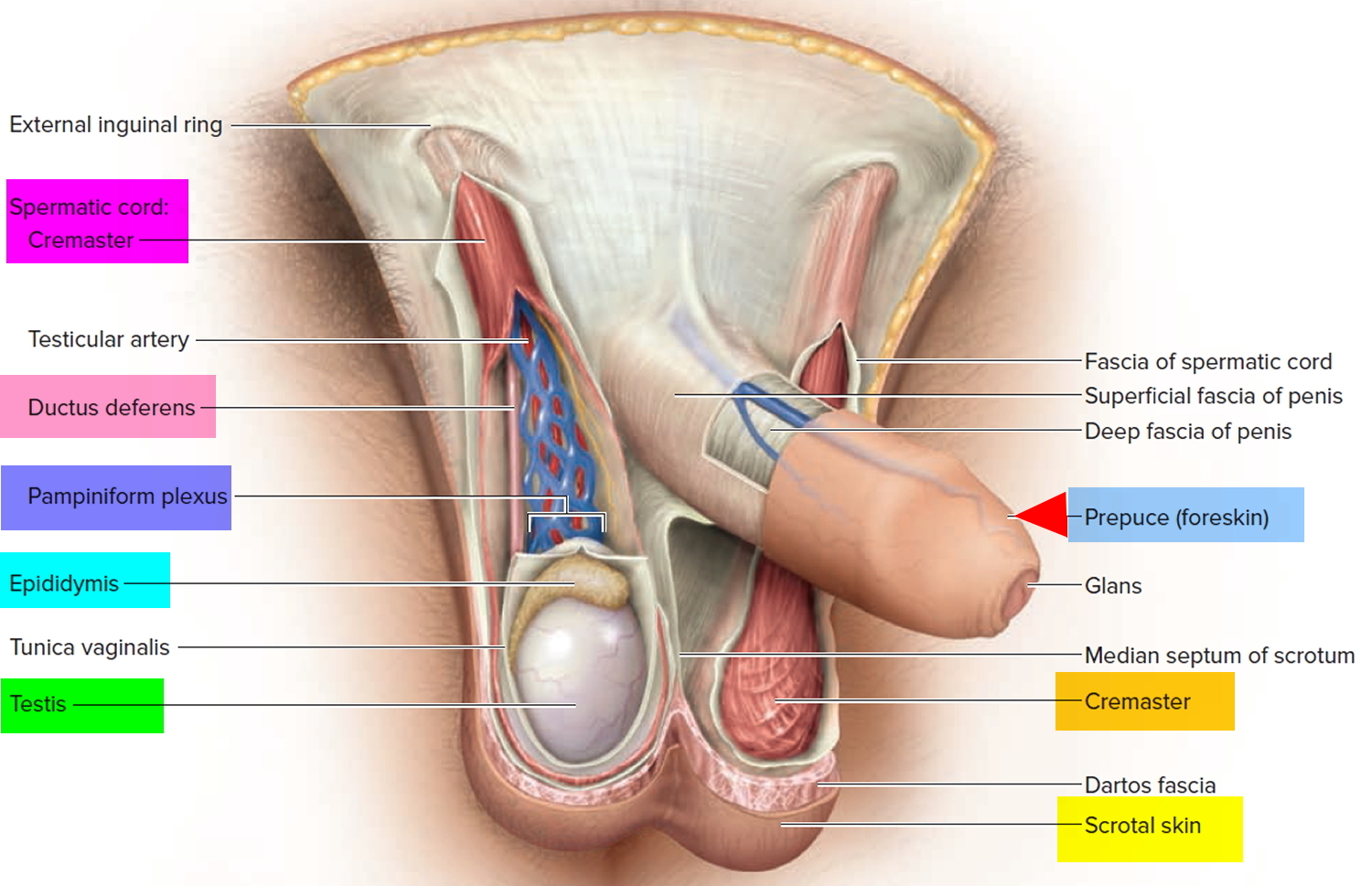
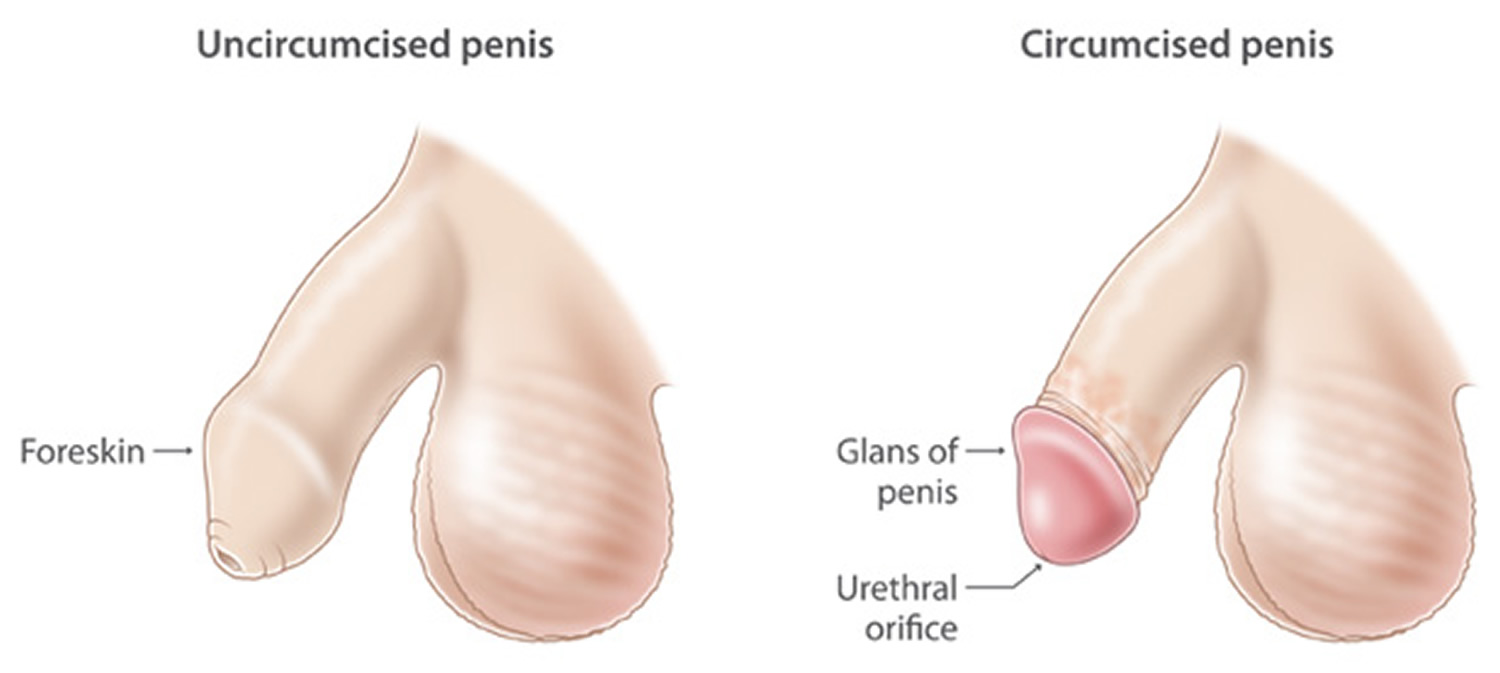
Male circumcision is the surgical procedure for the complete removal of the foreskin, the skin that covers the tip of the penis. The foreskin is the retractable fold of skin that covers the end of the penis. It’s a continuation of the skin that covers the whole penis (see Figure 2 below). Male circumcision procedure is fairly common for newborn boys in certain parts of the world, including the United States. Circumcision after the newborn period is possible, but it’s a more complex procedure.
For some families, male circumcision is a religious ritual. Male circumcision procedure can also be a matter of family tradition, personal hygiene or preventive health care. For others, however, circumcision seems unnecessary or disfiguring.
Contraindications of male circumcision procedure include congenital abnormalities of the penis such as hypospadias, epispadias, megalourethra, webbed penis, and any other condition in which prior circumcision renders treatment more difficult 1). Others are prematurity, bleeding problems, myelomeningocele, and anorectal anomaly 2).
Religious, cultural, medical, and recently public health reasons 3) are known to be the major indications of the procedure. Usually, male circumcision is done in neonatal period but can be performed at any age. To maximize its health benefits 4), to reduce procedural risks and cost 5), however, it is advocated to be offered in neonatal period. Surgical approaches to circumcision are extremely varied 6).
About 25-33% of the total world male population is circumcised 7). In the US, an average of a million newborn males are circumcised yearly 8). Circumcision rate in US is as high as 70%, while in Britain it is 6% 9). In Nigeria, circumcision rate is estimated to be 87% 10). Approximately, 1.2 million circumcisions were performed in the USA in 2009 alone 11) and the incidence of this procedure appears to be decreasing.
According to the American Academy of Pediatrics 12), there are medical benefits and risks to circumcision. Possible benefits include a lower risk of urinary tract infections, penile cancer, and sexually transmitted diseases or acquisition of HIV. There is a low risk of bleeding or infection. The baby might also feel some pain.
The American Academy of Pediatrics 13) said that because of the possible benefits, parents should have the option to circumcise their sons. They recommend that parents discuss circumcision with their baby’s health care provider. Parents should make their decision based on the benefits and risks, as well as their own religious, cultural, and personal preferences.
Circumcision might have various health benefits, including:
- Easier hygiene. Circumcision makes it simpler to wash the penis. However, boys with uncircumcised penises can be taught to wash regularly beneath the foreskin.
- Decreased risk of urinary tract infections. The risk of urinary tract infections in males is low, but these infections are more common in uncircumcised males. Severe infections early in life can lead to kidney problems later.
- Decreased risk of sexually transmitted infections. Circumcised men might have a lower risk of certain sexually transmitted infections, including HIV. Still, safe sexual practices remain essential.
- Prevention of penile problems. Occasionally, the foreskin on an uncircumcised penis can be difficult or impossible to retract (phimosis). This can lead to inflammation of the foreskin or head of the penis.
- Decreased risk of penile cancer. Although cancer of the penis is rare, it’s less common in circumcised men. In addition, cervical cancer is less common in the female sexual partners of circumcised men.
The risks of not being circumcised, however, are not only rare, but avoidable with proper care of the penis.
Key points
- It is imperative that those providing circumcision are adequately trained and that both sterile techniques and effective pain management are used. In general, untrained providers who perform circumcisions have more complications than well-trained providers who perform the procedure, regardless of whether the former are physicians, nurses, or traditional religious providers.
- Circumcision might not be an option if certain blood-clotting disorders are present. Also, circumcision might not be appropriate for premature babies who still require medical care in the hospital nursery or for babies born with abnormalities of the penis.
- Circumcision doesn’t affect fertility, nor is circumcision generally thought to enhance or detract from sexual pleasure for men or their partners.
- Circumcision is usually performed as a short-stay procedure under local or general anesthetic
- The entire foreskin is removed to leave the head of the penis exposed
- As well as looking different, your penis may feel different at first after the procedure
- The average length of a hospital stay during which circumcision was performed was 3.2 days in 2009, which was similar to 2005. This compares to an average length of a hospital stay of 3.8 for male newborn stays without circumcision in 2009 14)
- Circumcision rates were higher in the top income quartiles 15). In 2005, the circumcision rate for the highest income areas (66.1 percent) was 38 percent higher than the lowest income areas (47.8 percent). However, in 2009, the circumcision rate was only 17 percent higher in the highest income areas compared to the lowest (60.4 percent compared to 51.5 percent).
- Circumcision rates were lowest in large central metropolitan areas (41.2 percent). The highest rate was in rural areas (66.9 percent) 16).
- The lowest rate of male newborn circumcisions in 2009 occurred in the West (24.6 percent in 2009) compared to 75.2 percent in the Midwest, 67.0 percent in the Northeast, and 55.7 percent in the South 17).
- Among privately insured male newborns, 66.6 percent received a circumcision in 2009. This was 55 percent higher than for male newborns covered by Medicaid (42.9 percent received a circumcision) and 67 higher than for uninsured male newborns (39.8 percent received a circumcision). There were no significant changes since 2005 18).
Figure 1. Percentage of male circumcisions in newborns 1993-2009 United States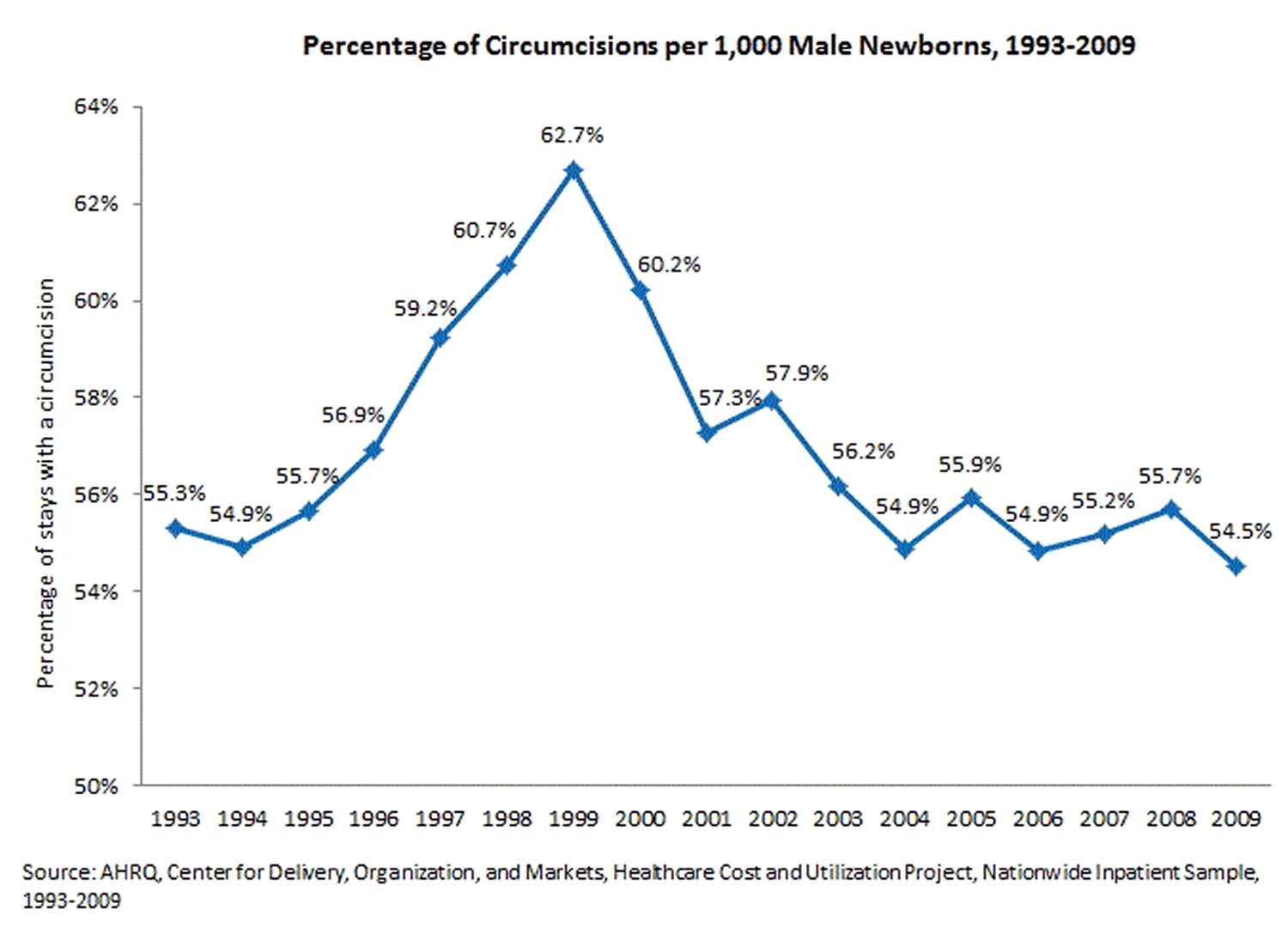 [Source 19)]
[Source 19)]
| Table 1. Characteristics of male newborn stays involving a circumcision, U.S. hospitals, 2005 and 2009 | |||
| Male newborn stays with a circumcision | Male newborn stays without a circumcision, 2009 | ||
|---|---|---|---|
| 2005 | 2009 | ||
| Number of hospital stays | 1,208,070 | 1,157,510 | 965,280 |
| Mean length of hospital stay, days | 3.1 | 3.2 | 3.8 |
| Average total cost per hospital stay* | $2,220 | $2,310 | $3,760 |
| Aggregate total hospital cost* (billions) | $2.7 | $2.7 | $3.6 |
| *2005 costs have been inflation-adjusted to 2009 dollars. Costs include the costs for the entire hospital stay, including room and board, laboratory tests, procedures, and all other services. Source: Agency for Healthcare Research and Quality, Center for Delivery, Organization, and Markets, Healthcare Cost and Utilization Project, Nationwide Inpatient Sample, 2005 and 2009. | |||
| Table 2. Percentage of male newborn stays involving a circumcision by region, U.S. hospitals, 2005 and 2009 | ||
| 2005 | 2009 | |
|---|---|---|
| All male newborn hospitals stays | 55.9 | 54.5 |
| Region | ||
| Northeast | 64.5* | 67.0§ |
| Midwest | 74.9* | 75.2§ |
| South | 56.3* | 55.7§ |
| West | 31.1* | 24.6§ |
| *The proportion of males with a circumcision in this region is significantly different from that in all other regions at p<0.05 in 2005. § The proportion of male newborns with a circumcision in this region is significantly different from that in all other regions at p<0.05 in 2009. Source: Agency for Healthcare Research and Quality, Center for Delivery, Organization, and Markets, Healthcare Cost and Utilization Project, Nationwide Inpatient Sample, 2005 and 2009. | ||
| Table 3. Percentage of male newborn stays involving a circumcision by location of patient residence, 2005 and 2009 | ||
| 2005 | 2009 | |
|---|---|---|
| All male newborn hospitals stays | 55.9 | 54.5 |
| Location of patient residence | ||
| Large central metro | 43.0* | 41.2a, b, c |
| Large fringe metro (suburbs)† | 68.8* | 62.3a |
| Medium and small metro | 57.2* | 55.9b,d |
| Micropolitan and noncore (rural) | 64.6* | 66.9c,d |
| †Differences between 2005 and 2009 are statistically significant at p<0.05. * The proportion of male newborns with a circumcision in this location of patient residence is significantly different from that in all other locations at p<0.05 in 2005. The following comparisons of the proportion of male newborns with a circumcision are significantly different at p<0.05 in 2009: a = large central metro and large fringe metro, b = large central metro and medium-small metro, c = large central metro and micropolitan-noncore, d = medium-small metro and micropolitan-noncore. Source: Agency for Healthcare Research and Quality, Center for Delivery, Organization, and Markets, Healthcare Cost and Utilization Project, Nationwide Inpatient Sample, 2005 and 2009. | ||
I’m not planning to have my newborn circumcised. How should I care for his uncircumcised penis?
In an uncircumcised penis, a fold of skin (foreskin) covers the head of the penis. If your baby isn’t circumcised, simply wash his penis with nonirritating soap and water during each bath. There’s no need to use cotton swabs or special cleansers.
At birth, the foreskin of most male babies doesn’t yet pull back (retract) fully. Treat the foreskin gently, being careful not to force it back. Forcing it could cause pain, tearing and bleeding.
Consult the doctor if your baby seems to have discomfort while urinating — especially if the foreskin fills with urine or balloons out during urination — or the foreskin becomes red, itchy or swollen.
As your child gets older, the foreskin of his uncircumcised penis will begin to separate from the tip of the penis. This allows the foreskin to be retracted. As soon as the foreskin can be retracted, it’s important to clean beneath it regularly. Teach him to:
- Gently pull back the foreskin
- Clean beneath the foreskin with mild soap and water
- Rinse and dry beneath the foreskin thoroughly
- Pull the foreskin back over the head of the penis
Encourage your child to follow the same procedure through adulthood as part of his daily bathing routine.
How the foreskin develops
It’s normal for a baby boy’s foreskin not to pull back (retract) for the first few years of life.
Around the age of two – or later, in some cases – the foreskin should start to separate naturally from the head of the penis (glans). Full separation occurs in most boys by the age of five years.
For some boys, the foreskin can take longer to separate, but this doesn’t mean there’s a problem, it will usually just detach at a later stage.
- Never try to force your son’s foreskin back, as it may be painful and damage the foreskin.
As the foreskin starts to separate from the head of the penis, you may see the foreskin “ballooning out” when your son passes urine. This can occasionally lead to infection (balanitis), but this ballooning usually settles down with time.
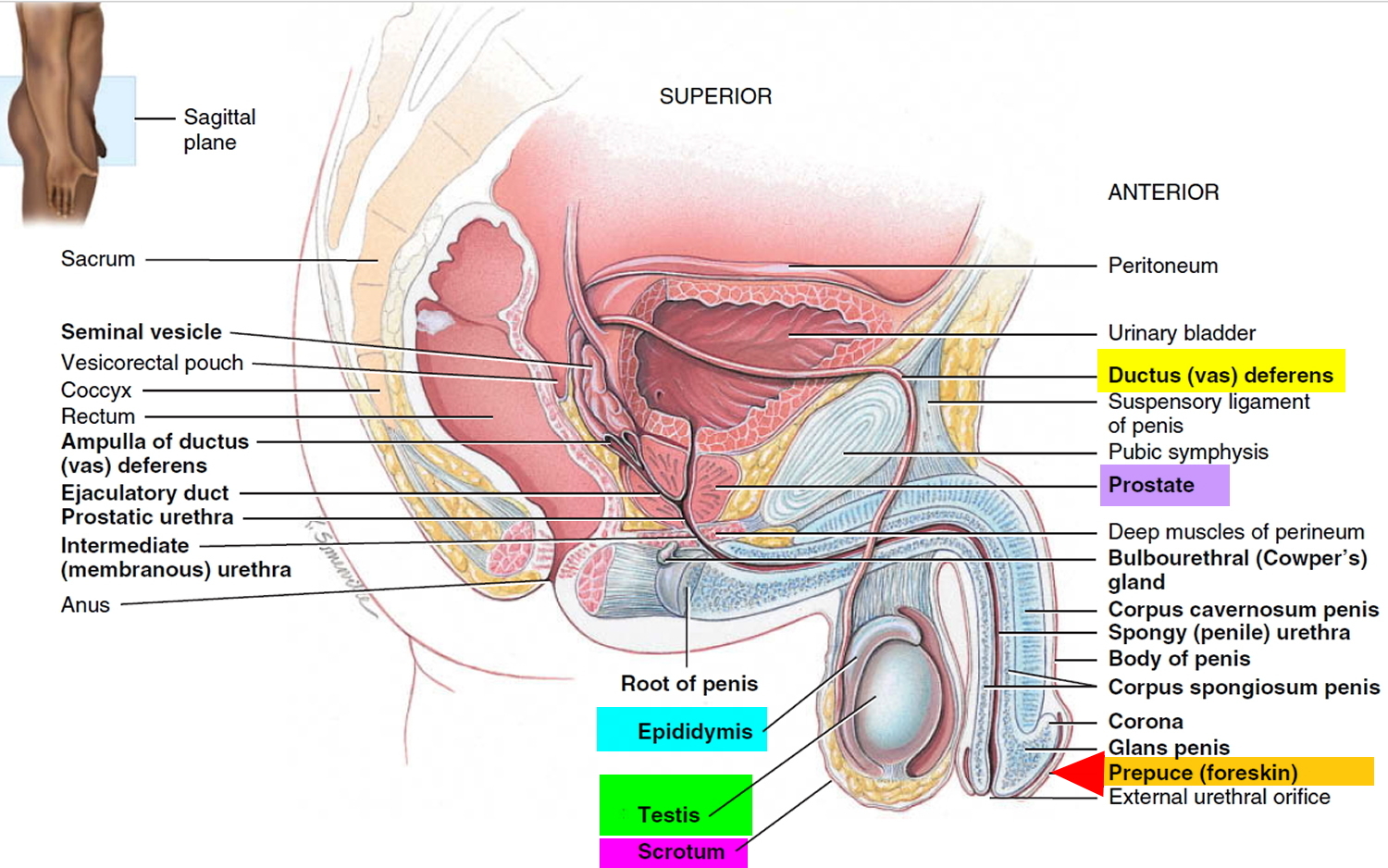
Figure 2. Penis and foreskin anatomy
Timing of circumcision
It has been widely reported that circumcision complications occur more frequently with increasing age of the patient 23). Bleeding becomes more common during the “minipuberty” of infancy that begins at 4 weeks of age and extends to 3 months of age. This is thought to be due to hormonally mediated increase in penile and prepuce size and vascularity 24). In a recent prospective observation-based study of 583 neonatal circumcisions, Banieghbal reported only two minor bleeding complications requiring sutures. Both occurred in infants aged 3 weeks. Based on use of the Neonatal Infant Pain Scale, he further reported that the ideal timeframe for a “pain free” circumcision is during the first week of life 25). This is further supported by Horowitz and Gershbein who reported zero complications in 98 infants circumcised with a Gomco clamp (see Figure 3 below) in their first month of life versus a 12/32 or a 30% bleeding complication rate requiring sutures or fulguration in those aged 3–8 months 26).
What is the purpose of circumcision
Why circumcision is carried out in men
Circumcision in men may be carried out for:
- medical reasons – in men, circumcision is most commonly carried out when the foreskin is tight and won’t pull back (retract), which is known as phimosis; however, alternative treatments, such as topical steroids, are sometimes preferred
- religious and cultural reasons – circumcision is a common practice in the Jewish and Islamic communities, and it’s also practised by many African communities; most cultural circumcisions are carried out on children
- HIV prevention – there’s evidence that circumcision reduces the risk of heterosexual men acquiring HIV, and it’s encouraged as part of HIV prevention programmes in some African countries with high rates of HIV
Medical reasons for men to have a circumcision
In men, circumcision is sometimes considered a possible treatment option for the following conditions:
- tight foreskin (phimosis) – where the foreskin is too tight to be pulled back over the head of the penis (glans); this can sometimes cause pain when the penis is erect and, in rare cases, passing urine may be difficult
- recurrent balanitis – where the foreskin and head of the penis become inflamed and infected
- paraphimosis – where the foreskin can’t be returned to its original position after being pulled back, causing the head of the penis to become swollen and painful; immediate treatment is needed to avoid serious complications, such as restricted blood flow to the penis
- balanitis xerotica obliterans (BXO)– a condition that causes phimosis and, in some cases, also affects the head of the penis, which can become scarred and inflamed
- cancer of the penis – a very rare type of cancer that can occur in men, where a red patch, wart-like growth or ulcer appears on the end of the penis or under the foreskin
In most cases, circumcision will only be recommended when other, less invasive and less risky treatments have been tried and haven’t worked.
Mild cases of phimosis can be treated with topical steroids to help soften the skin and make it easier for the foreskin to retract.
In paraphimosis, a healthcare professional may rub a local anesthetic gel on to the glans to help reduce pain and inflammation. They may then apply pressure to the head of the penis while pushing the foreskin forward.
In severe cases of paraphimosis, local anesthetic gel can be applied to the penis and a small slit is made in the foreskin to help relieve the pressure.
Balanitis and balanitis xerotica obliterans can sometimes be successfully treated using corticosteroid ointment, gel or cream, antibiotic creams or antifungal creams.
The three main treatment options for penile cancer are:
- surgery to remove the cancerous cells, and sometimes the surrounding tissue
- radiotherapy
- chemotherapy
If you’re considering circumcision for a medical reason, it’s worth discussing alternative treatment options with your GP or specialist.
HIV prevention
There’s evidence from several trials 27), 28) carried out in Africa that circumcised men have a lower risk of acquiring HIV from infected women.
The association of circumcision and the decreased likelihood of HIV acquisition applies to heterosexual males. Circumcision seems to be less likely to protect men who have sex with men, however, and has not been associated with decreased acquisition of HIV among men who have sex with men 29). There is fair evidence from 1 study that there is a protective effect of circumcision from HIV infection in men who have sex with men; however, this study used self-report to establish circumcision status 30). One study with fair evidence is neutral regarding the relationship between circumcision and HIV infection in men who have sex with men 31). It is probable that the differences found in the level of protection (or lack of protection) by studies of men who have sex with men are confounded by the fact that men who have sex with men commonly perform both receptive and insertive sex. It is not known to what extent circumcision may be protective against HIV transmission for men who have sex with men who practice insertive sex versus for those who engage in receptive sex.
However, it’s unclear whether male circumcision can help prevent other sexually transmitted infections (STIs).
There have been several studies into male circumcision and the risk of other sexually transmitted infections (STIs), but the evidence to date has been inconclusive and conflicting.
Reasons for circumcision is carried out in boys
Circumcision in boys may be carried out for:
- medical reasons – for example, as a treatment of last resort for conditions such as a tight foreskin (phimosis) and recurrent infection of the foreskin and head of the penis (balanitis)
- religious or cultural reasons – it’s a common practice in Jewish and Islamic communities, and it’s also practiced by many African communities; most cultural circumcisions are carried out in young boys
Medical reasons for a boy to have a circumcision
It’s rare for circumcision to be recommended for medical reasons in boys. This is because other less invasive and less risky treatments are usually available.
The following conditions affect the penis and, in rare cases, may require a circumcision:
- tight foreskin (phimosis) – where the foreskin is too tight to be pulled back over the head of the penis; this can sometimes cause pain when the penis is erect and, in rare cases, passing urine may be difficult
- recurrent infection (balanitis) – where the foreskin and head of the penis become inflamed and infected
- paraphimosis – where the foreskin can’t be returned to its original position after being pulled back, causing the head of the penis to become swollen and painful; immediate treatment is needed to avoid serious complications, such as restricted blood flow to the penis
- balanitis xerotica obliterans (BXO) – a condition that causes phimosis and, in some cases, also affects the head of the penis, which can become scarred and inflamed
- repeated urinary tract infections (UTIs) – in very rare cases, circumcision may be recommended as a treatment of last resort if a boy has repeated urinary tract infections (UTIs)
These conditions can often be treated successfully with non-surgical treatments, which will often be tried first before circumcision is considered.
Mild cases of phimosis can be treated with topical steroids to help soften the skin and make it easier for the foreskin to retract.
However, circumcision may be necessary if the foreskin is damaged and won’t slide back over the head of the penis. This is very rare before the age of five.
In paraphimosis, a healthcare professional may rub a local anesthetic gel on to the head of the penis (glans) to help reduce pain and inflammation. They may then apply pressure to the glans while pushing the foreskin forward.
In severe cases of paraphimosis, local anesthetic gel can be applied and a small slit made in the foreskin to help relieve the pressure.
Balanitis and balanitis xerotica obliterans can sometimes be successfully treated using corticosteroid ointment, gel or cream, antibiotic creams or antifungal creams.
Most urinary tract infections (UTIs) are mild and can be treated with antibiotics. However, repeated urinary tract infections (UTIs) can occasionally cause kidney damage.
For example, if a boy has a birth defect that causes urine to leak back up into the kidney, bacteria can spread from the foreskin, through the urine, and infect the kidney. Circumcision may be recommended in these cases.
Circumcision procedure
Circumcision surgery for men
Circumcision is usually carried out on a day patient basis. This means you’ll be admitted to hospital on the same day you have surgery and you won’t have to stay overnight.
You’ll be asked not to eat and drink for six hours before surgery if you’re having a general anesthetic.
After you’ve been admitted to hospital, you’ll be seen by the members of the medical team carrying out the procedure, including your surgeon and anesthetist.
This is a good opportunity to discuss any concerns you have and ask questions about anything you’re not sure about. You’ll be asked to sign a consent form to confirm you agree to the surgery.
You’ll usually either have a general anesthetic, which means you’ll be unconscious throughout the procedure, or a local anesthetic injection, which will numb your penis and the surrounding area.
In some cases, a spinal anesthetic, where you’re unable to feel anything below your waist, will be used.
Circumcision is a relatively simple procedure. The foreskin is removed just behind the head of the penis using a scalpel or surgical scissors.
Any bleeding can be stopped using heat (cauterised), and the remaining edges of skin will be stitched together using dissolvable stitches.
Circumcision surgery for boys
Circumcision is similar for older boys and adults. However, the procedure might need to be done under general anesthesia, recovery might take longer and the risk of complications might be greater when done later in life.
Circumcision is usually carried out on a day patient basis. This means your child will be admitted to hospital on the same day he has surgery and won’t need to stay overnight.
He won’t be able to eat or drink before having surgery – you’ll receive detailed information in a letter.
After being admitted to hospital, your child will be seen by the surgeon who will carry out the procedure. They’ll explain the operation in more detail, discuss any concerns and answer any questions you have.
They’ll also ask you to sign a consent form, giving your permission for the operation.
The anesthetist will also visit your child before the operation. They will usually have a general anesthetic, so they’ll be unconscious throughout the procedure and unable to feel any pain or discomfort.
Circumcision is a relatively simple procedure. The foreskin is removed just behind the head of the penis using a scalpel or surgical scissors.
Any bleeding can be stopped using heat (cauterised). The remaining edges of skin are stitched together using dissolvable stitches. It will take up to six weeks for your son’s penis to fully heal.
Newborn circumcision the procedure
Newborn circumcision is often done in the hospital nursery, usually within 10 days after birth.
For newborn circumcision, your son will lie on his back with his arms and legs restrained. After the penis and surrounding area are cleansed, an anesthetic will be injected into the base of the penis or applied to the penis as a cream. A special clamp or plastic ring will be attached to the penis, and the foreskin will be removed.
Afterward, the penis will be covered with an ointment, such as a topical antibiotic or petroleum jelly, and wrapped loosely with gauze. The procedure generally takes about 10 minutes.
Circumcision healing
Recovering after male circumcision in men
When you’re discharged from hospital, you’ll be given advice about your recovery at home, including when you can drive, return to work and have sex.
It usually takes at least 10 days for your penis to heal after circumcision. You’ll probably be advised to take at least one week off work to recover.
You should avoid having sex for at least four weeks after your operation.
Your medical team will give you a contact number to call in case you experience any problems or have any concerns. You should also be given details about your follow-up appointment, which may be at the hospital or with your doctor.
For three or four days after your operation, it’s likely you’ll experience some discomfort and swelling around the head of your penis. Before leaving hospital, you’ll be given painkilling medication, such as paracetamol or ibuprofen, to help ease this.
However, contact your doctor if you have a temperature, increased redness, bleeding, persistent pain or throbbing of your penis, as it could be a sign of infection.
Applying petroleum jelly (Vaseline) around the tip of your penis will stop it sticking to your underwear. Wearing light, loose-fitting clothing for two or three days after your operation will also help avoid irritation to your penis while it heals.
You shouldn’t feel any pain or discomfort while passing urine, but contact your medical team if you do.
Recovering after male circumcision in boys
After the operation, a dressing will be put over the penis to protect the wound. It will be removed before your child goes home.
He will be allowed home after he’s passed urine, which may be slightly uncomfortable at first.
The penis will be sore and inflamed for a few days after the operation. Ointment may be prescribed to use for a few days to help the area heal.
Your child will also need regular pain relief, in the form of paracetamol or ibuprofen, for at least three days.
It may be more comfortable to wear loose clothing – or no clothing at all – on his bottom half for a few days after the operation. Passing urine in the bath or shower may also be more comfortable.
Your child will be able to have a bath the day after the operation. He should avoid riding a bicycle or other toys you sit on until any swelling has gone down.
He should be able to return to school or nursery about a week after the operation. Make sure you tell the school or nursery about the operation.
In most cases, a follow-up appointment won’t be necessary.
However, you should contact your doctor or hospital care team if:
- the penis is bleeding
- the penis is still swollen two weeks after the operation
- passing urine is still painful a few days after the operation
Recovering after male circumcision in newborn / baby
It usually takes seven to 10 days for the penis to heal. The tip of the penis is likely to be sore at first, and the penis might look red, swollen or bruised. You might notice a small amount of yellow fluid on the tip of the penis as well.
If your newborn is fussy as the anesthetic wears off, hold him gently — being careful to avoid putting pressure on the penis.
It’s okay to wash the penis as it heals. For newborns, change the bandage with each diaper change, and apply a dab of petroleum jelly to the tip of the penis to keep it from sticking to the diaper. Change your baby’s diaper often, and make sure the diaper is loosely fastened.
If there’s a plastic ring instead of a bandage, it will drop off on its own — usually within about a week. Once the penis heals, wash it with soap and water during normal bathing.
Problems after circumcision are uncommon. Contact the doctor if:
- Normal urination doesn’t resume within 12 hours of the circumcision
- There’s persistent bleeding
- There’s foul-smelling drainage from the tip of the penis
- The plastic ring remains in place two weeks after the circumcision
Male circumcision risks
Adult male circumcision risks
In the US, complications after circumcisions carried out for medical reasons are rare and most men don’t experience any significant problems.
Apart from the initial swelling, bleeding and infection are the two most common problems associated with circumcision.
- There’s between a 1 in 10 and a 1 in 50 chance that you’ll experience bleeding or infection.
Other possible complications of circumcision can include:
- permanent reduction in sensation in the head of the penis, particularly during sex
- tenderness around the scar
- the need to remove stitches that haven’t dissolved
- occasionally, another operation is needed to remove some more skin from around the head of the penis
Boys circumcision risks
The risks associated with circumcisions when carried out by qualified and experienced doctors are small.
The main risk is bleeding, both during and after the operation. The surgeon will seal off any bleeding during the procedure, and the dressing applied afterwards will absorb any further bleeding.
However, seek medical advice if your child’s penis continues to bleed after they return home.
There are also risks associated with general anesthetic, such as having a serious allergic reaction (anaphylaxis). However, these risks are small.
The anesthetist will explain the risks to you before the operation. You can also read more about the complications and risks of general anesthetic.
You can also have a headache or feel sick or dizzy after having a general anesthetic. However, these side effects should pass quickly.
There’s also a small risk of infection after having a circumcision.
How is circumcision done
Various methods of circumcision are commonly used in the United States today. The choice of circumcision method depends on the physician’s level of comfort and training 32). The most commonly utilized techniques used in the newborn nursery setting are the Gomco clamp, the Mogen clamp, and the Plastibell 33). While all of these can be used in the operating room, the “free-hand circumcision” using either the sleeve technique or the dorsal-ventral slit technique is most commonly used. Each instrument and technique carries its own benefits and complication risks.
The Gomco clamp is a suture-less technique that utilizes a 4-piece device that protects the glans, provides hemostasis and a platform for resecting the prepuce (Figure 3). The circumcision starts by retracting the foreskin to free the adhesions and allow exposure and inspection of the glans for any abnormalities. The metal bell is placed completely over glans shielding it from damage, followed by placement of the platform over the bell and prepuce caring not to draw the skin up too much (the goal is to maintain the penoscrotal junction), placement of the crimping part which will provide hemostatic compression of the skin after tightening down the screw, excision of the prepuce, disassembly of the apparatus without unsealing the skin edges, and, finally, dressing the wound.
Complications from a Gomco circumcision are mainly related to technical factors. It is important to assure that the metal bell completely covers the glans, otherwise insufficient skin will be removed and accidental incision into the glans is possible. A bell which is too large will result in removal of too much skin. As mentioned, overly aggressive retraction of the skin through the platform can lead to excessive skin removal and subsequent corrective surgery; conversely, insufficient drawing up of the skin will lead to an incomplete circumcision, which may also require corrective surgery. Insufficient tightening of the screw results in inadequate compression of the skin and subsequent bleeding. One may consider keeping the screw tightened for several minutes of hemostatic compression before excising the skin.
Figure 3. The Gomco clamp technique for newborn circumcision
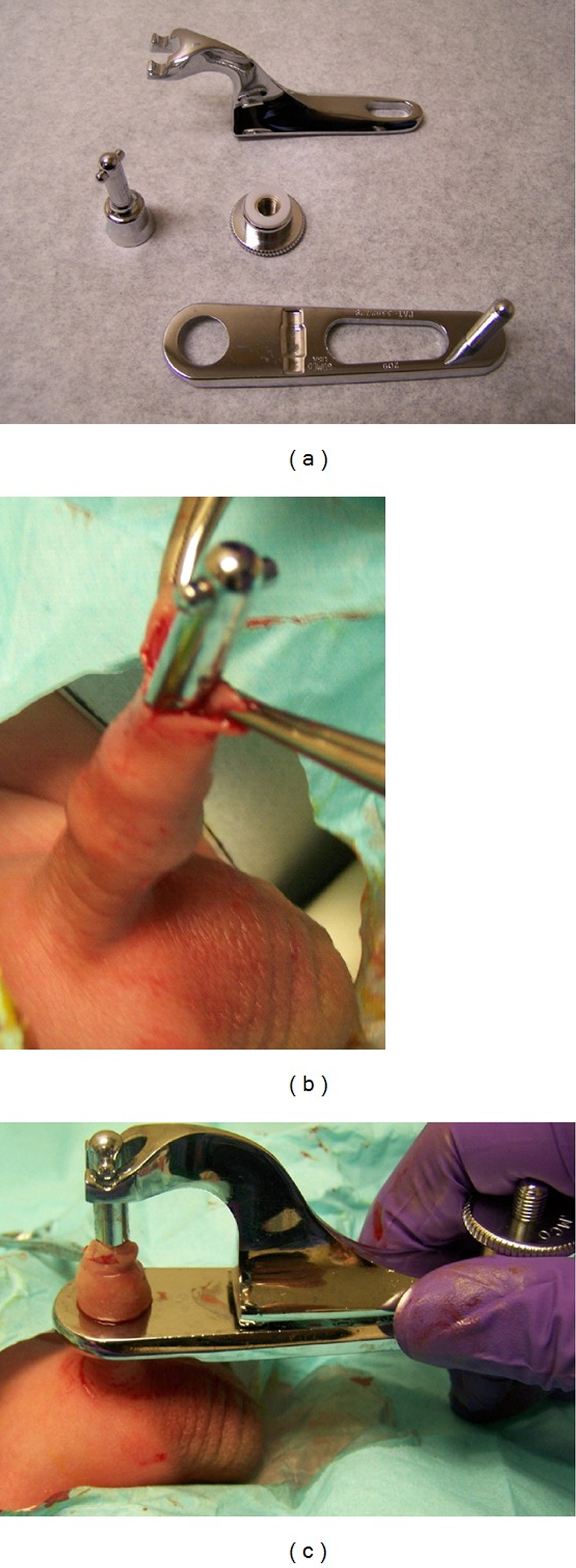
Notes: (a) The Gomco clamp consists of 4 pieces: the bell, platform, hooking arm, and screw. These are assembled after placing the bell completely over the glans (b) and the skin drawn through the hole in the platform. Hemostasis is obtained by tightening the screw (c) and the skin excised.
[Source 34)]The Mogen clamp (Figure 4) is a device used for Jewish ritual circumcisions and commonly used by obstetricians, that also serves to provide hemostasis and a platform for adequate skin removal. After lysis of adhesions and inspection of the glans, the edges of the prepuce are elevated and the V-shaped clamp is placed across the prepuce at the desired location assuring that the glans is positioned below the clamp. The clamp is then tightened to provide hemostasis and the skin is amputated. The complications specific to this techniques include injury to the glans if it is not below the inferior edge of the clamp, and an asymmetric incomplete circumcision due to mal-positioning of the clamp (typically more redundancy ventrally). The possible complications include insufficient or excessive skin removal or asymmetric redundancy and glans amputation all due to improper clamp placement.
Figure 4. Mogen clamp male circumcision technique for newborn

Note: The Mogen clamp is used by drawing the skin to be removed into the V and then providing hemostasis followed by amputation.
[Source 35)]The Plastibell (Figure 5) technique was developed in the 1950s and is a variation of the Gomco clamp. After lysis of penile adhesions, the plastic bell, similar in appearance to the metal Gomco bell, is placed completely over the glans. Hemostasis is then insured by placing a strangulating suture at the level of the corona and this is all left in place. The skin will slough after a few days and the Plastibell falls off 36). The associated complications include incomplete circumcision due to inadequate bell placement or slippage of the Plastibell while tying the hemostatic suture, and glans injury or bleeding due to inadequate hemostatic suture placement 37).
Figure 5. Plastibell male circumcision technique for newborn

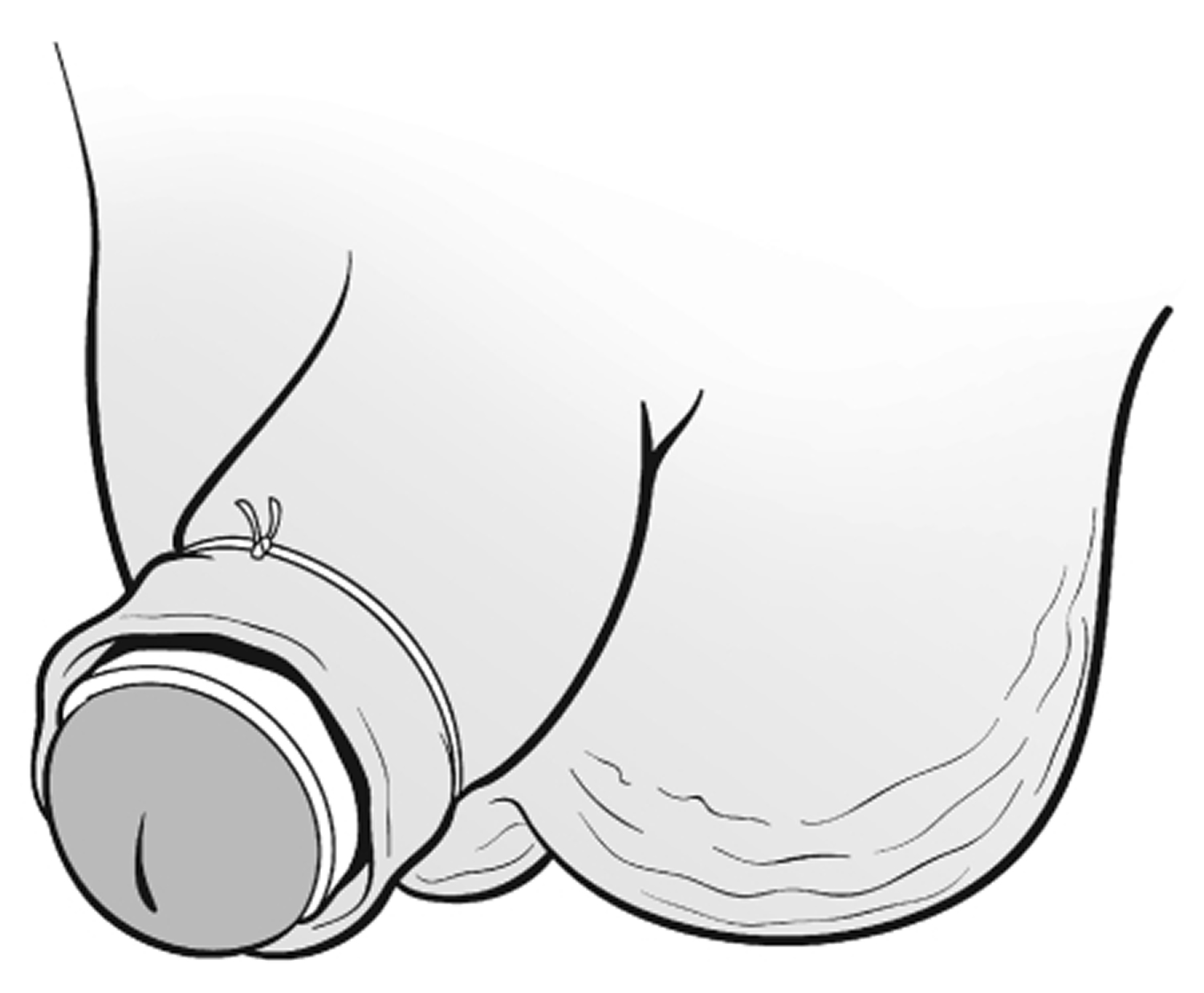
Note: The Plastibell is placed over the glans and a suture is secured over the skin. After several days, the skin will slough and the Plastibell falls off.
[Source 38)]The “free-hand circumcision” (Figure 6) is accomplished in the operating room and involves excising the skin as marked, hemostasis using electrocautery and then reapproximation of the skin edges using absorbable sutures or octyl-2-cyanoacrylate 39). The lines of incision for the “sleeve technique” are circumferential at the same distance from the corona on the inner and outer preputial surfaces (Figure 6 A). The sleeve of skin is removed and the procedure completed. For the dorsal-ventral slit technique (Figure 7), these incisions are made as their names infer down to the predetermined distance from the coronal edge, and then the incisions are connected leaving the two circumferential free-edges which are then closed after achieving hemostasis.
Figure 6. Free-hand male circumcision technique
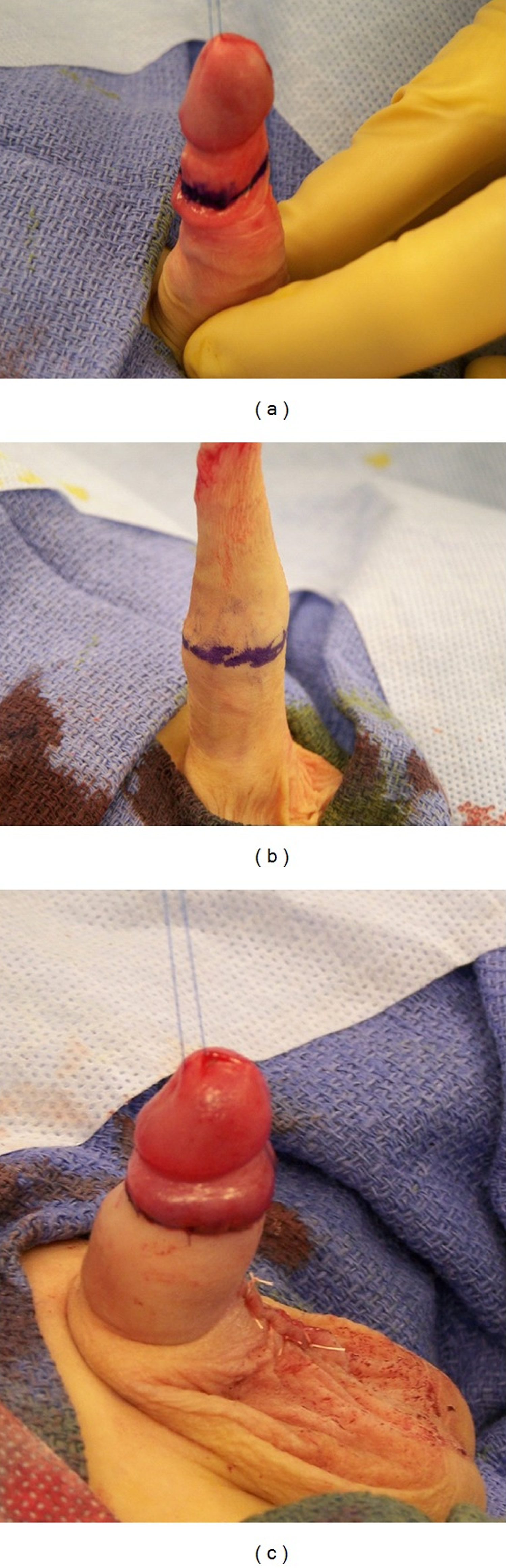
Note: The “sleeve” technique involves incising the inner preputial skin (a) and then the overlying outer preputial skin (b). Sutures are most commonly used to approximate the skin edges (c).
[Source 40)]Figure 7. Dorsal-ventral slit male circumcision technique
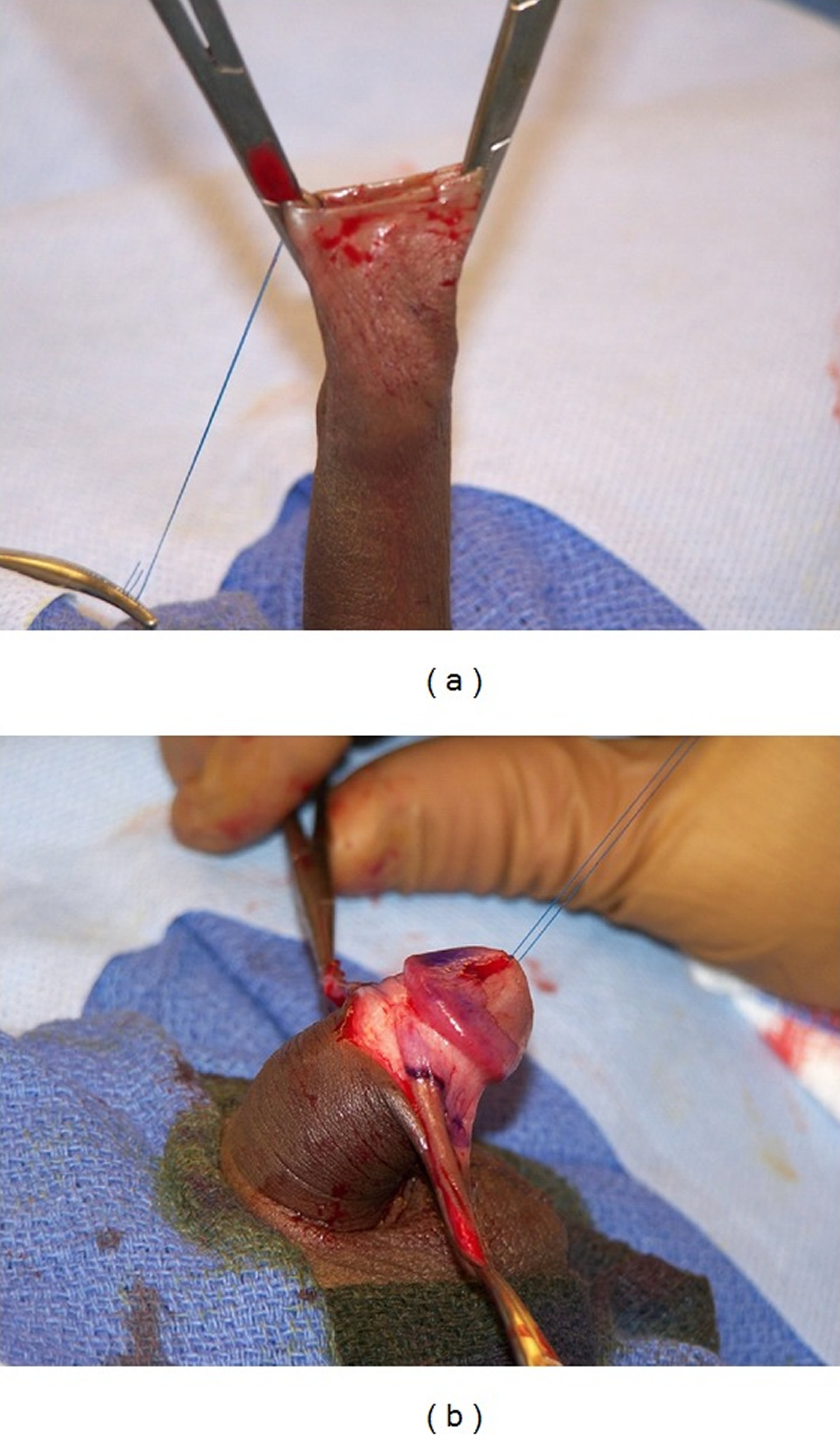
Note: (a) The dorsal-ventral slit technique of circumcision involves making these incisions and then (b) removal of the skin between them. Sutures are most commonly used to approximate the skin edges.
[Source 41)]Male circumcision complications
The rate of adverse events varies widely across reports, depending on the definition chosen for a postoperative complication. In a large meta-analysis of prospective and retrospective series, Weiss et al. reported a frequency of adverse events of and for serious adverse events 42). This can represent a significant cost in terms of utilization resources and healthcare dollars. During a five-year period at the Massachusetts General Hospital, 7.4% of all visits to a pediatric urologist were for circumcision complications. This translated to an average total cost per patient for redo procedures of $1,617 and an estimated annual cost of $137,122 to the institution 43).
For ease of discussion, adverse events following circumcision can be categorized as either early or late complications.
Early complications such as:
- bleeding,
- pain,
- inadequate skin removal, and
- surgical site infection tend to be minor and quite treatable.
However, postcircumcision bleeding in patients with coagulation disorders can be significant and sometimes even fatal. Other serious early complications include chordee, iatrogenic hypospadias, glanular necrosis, and glanular amputation. The latter, of course, requires prompt surgical intervention.
Late complications include:
- epidermal inclusion cysts,
- suture sinus tracts,
- chordee,
- inadequate skin removal resulting in redundant foreskin,
- penile adhesions,
- phimosis,
- buried penis,
- urethrocutaneous fistulae,
- meatitis, and meatal stenosis.
These are commonly treated in an outpatient setting. Most of the aforementioned conditions are avoidable giving attention to detail and proper technique. Mayer et al. found that some subtle anatomic variations are significantly associated with late circumcision complications, including penoscrotal webbing, suprapubic fat pads, and prematurity 44).
Death
Fortunately, death from neonatal circumcision is fortunately an extremely rare occurrence. King reported a period when 500,000 consecutive circumcisions were performed in New York city without a single fatality 45). However, a case of a misplaced Plastibell ring (see Figure 5) which caused complete meatal obstruction resulted in acute venous stasis and subsequent death from sepsis reported by the Ontario Pediatric Death Review Committee in 2007. In this situation, prompt recognition of the obstruction is critical and primary management should be immediate removal of the Plastibell ring and catheter placement 46). There are other reports in the international literature that describe mortalities from tetanus as a result of circumcisions performed under nonsterile conditions. Bennett et al. reported that topical antibiotics could decrease this risk of neonatal tetanus 4-fold 47).
Bleeding
Bleeding is the most common complication of circumcision, with an incidence of 1% in a large retrospective review 48). Bleeding may occur along the skin edges between sutures or from a discrete blood vessel, most commonly at the frenulum. Meticulous attention to hemostasis during an open procedure and adequate time for skin edge compression during newborn circumcisions should prevent the majority of cases although dislodging of a clot or cautery eschar can occur. The majority of postcircumcision bleeding can be controlled with application of direct pressure or careful application of silver nitrate. Rarely is wound exploration and suturing necessary. A hematologic workup is warranted only in patients who persistently bleed, or bleed significantly. In a retrospective review of the Mayo Clinic Pediatric Hemophilia database, 48 patients with a range of coagulopathies were circumcised. 21 patients had known coagulation disorders, while the remaining 27 patients were diagnosed after prolonged bleeding from their circumcision. There were 11 bleeding complications, three of which were severe and required transfusion of red blood cells for severe anemia despite preoperative factor replacement 49). In those patients with hemophilia who must undergo circumcision, preoperative and perioperative factor replacement is a definite requirement. Fibrin glue has also been shown to decrease the amount of recombinant factor replacement needed (and the cost of treatment, as well) without significantly altering bleeding complications 50).
Infection
Due to the good dual blood supply of the penis, wound infection occurs infrequently. In a series of 5,521 circumcisions comparing the Plastibell technique to the Gomco clamp, Gee and Ansell reported only 23 (0.4%) infections. Of those, the Plastibell group had significantly more infections, 19 versus four 51). All responded to a combination of topical treatment and oral antibiotic therapy. Causative organisms are usually skin flora, but due to the uniquely dirty environment of the diaper, colonic flora has also been reported. Most infections can be prevented with proper patient preparation, glove wearing and good local wound care including cleaning the penis, and application of antibiotic ointment with diaper changes 52)
Severe infections following Plastibell circumcision, including necrotizing fasciitis, have been reported as well. Several authors describe presenting signs and symptoms as erythema, induration, pain out of proportion to physical findings, coupled with tachycardia, leucocytosis, or bandemia. As in adults, this is usually a polymicrobial infection. Empiric broad spectrum antibiotics to cover Gram-negative, Gram-positive, and anaerobic organisms are essential. A suggested regimen is an aminoglycoside, nafcillin, or vancomycin and clindamycin. Prompt surgical evaluation and aggressive debridement of necrotic tissue is required 53).
Loss of Skin/Wound Dehiscence
Wound dehiscence and degloving injuries of the shaft are possible following using any of the techniques described above for neonatal circumcision. De-gloving injuries result from excess skin being drawn up into the clamp and then amputated. While, less likely, improper determination of the amount of skin to remove during free-hand circumcision may occur. Often these injuries are treated with local wound care and allowed to heal by secondary intention. There are reports of autografting the excised skin with good cosmetic result 54).
Trapped/Concealed Penis
Similarly, a concealed penis can result from overzealous removal of shaft skin coupled with a prominent suprapubic fat pad resulting in healing within the fat pad. Another consequence of this configuration is a secondary phimosis from the progressive closure of the skin over the glans penis. This can be avoided by firmly compressing the fat pad to the abdominal wall to best determine how much skin should be removed 55). In addition, the suprapubic fat should be compressed regularly after the procedure to allow the penis to be protrude. Corrective surgery may be necessary if there is absence or significant laxity of the penoscrotal angle or penoscrotal webbing that precludes adequate protrusion of the penis.
Redundant Foreskin/Circumcision Revision
Inadequate circumcision, or excess foreskin, is a fairly common indication for referral to a pediatric urologist. In a retrospective review of 476 late circumcision complications treated at Massachusetts General Hospital, 40% were for inadequate circumcision and another 5% were for phimosis requiring revision. The criteria for treatment are purely subjective and mainly cosmetic excepting those with phimosis, of course 56). Repair is scheduled electively under general anesthesia and is best accomplished using the “free-hand” skin sleeve technique removing the redundant skin.
Figure 8. Redundant foreskin following male circumcision
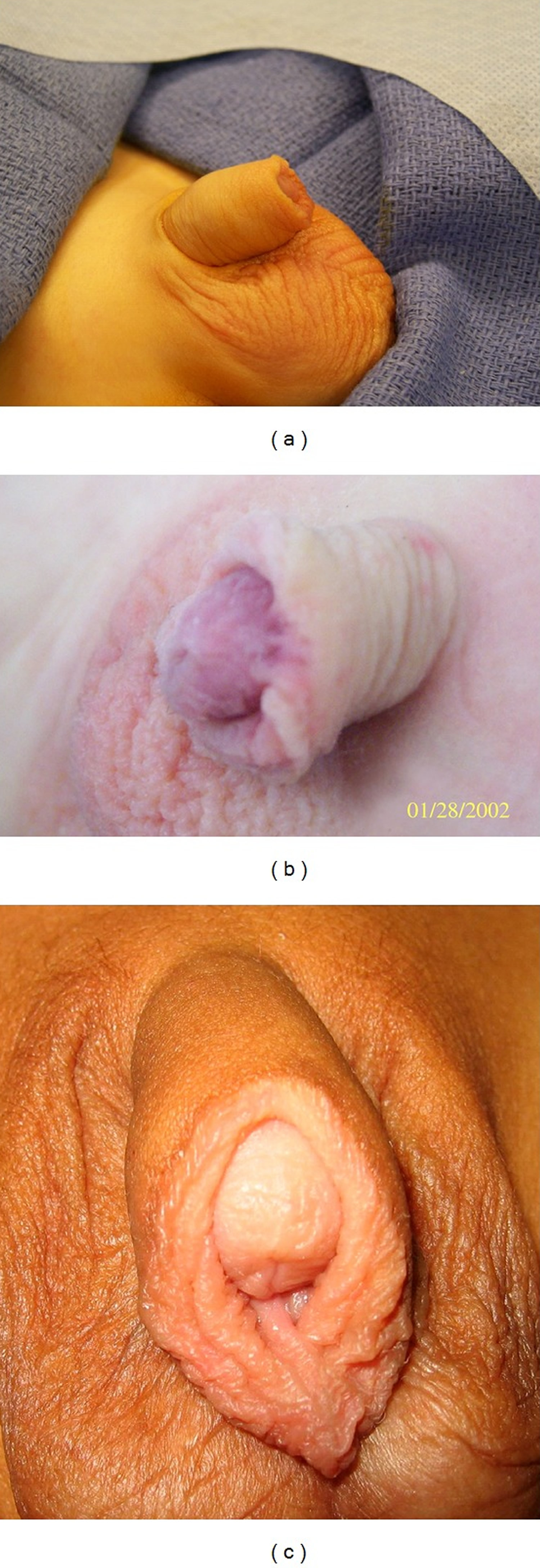
Note: Examples of redundant skin following circumcision (a,b,c).
[Source 57)]Preputial Adhesions/Skin Bridges
Preputial adhesions often result from either inadequate lysis of natural adhesions prior to circumcision or from distal migration of the skin from a prominent suprapubic fat pad. Williams et al. report that 63% of patients presenting for circumcision revision were found to have prominent suprapubic fat pads 58). The majority of adhesions should lyse spontaneously as the penis grows, suprapubic fat recedes, and erections become more frequent and firmer. Otherwise, lysis of preputial adhesions can be performed in the office by gently pushing away the adhesions from the glans after administering a topical anesthetic cream such as EMLA. EMLA is a mixture of two local anesthetics, lignocaine and prilocaine. Recurrence of these adhesions can be limited by regular compression of the suprapubic area to make the penis protrude and placement of petroleum jelly or any other such ointment. During healing, the circumferential incision can adhere to the glans and in some cases heal into an epithelialized skin bridge 59). If thin and transparent, they can be divided in the office. However, extensive adhesions and thick skin bridges require surgical intervention. These can be divided sharply after a period of compression with a hemostat. Skin bridges accounted for nearly 30% of the late complications reported by the Massachusetts General Hospital group 60).
Figure 9. Preputial Adhesions/Skin Bridges
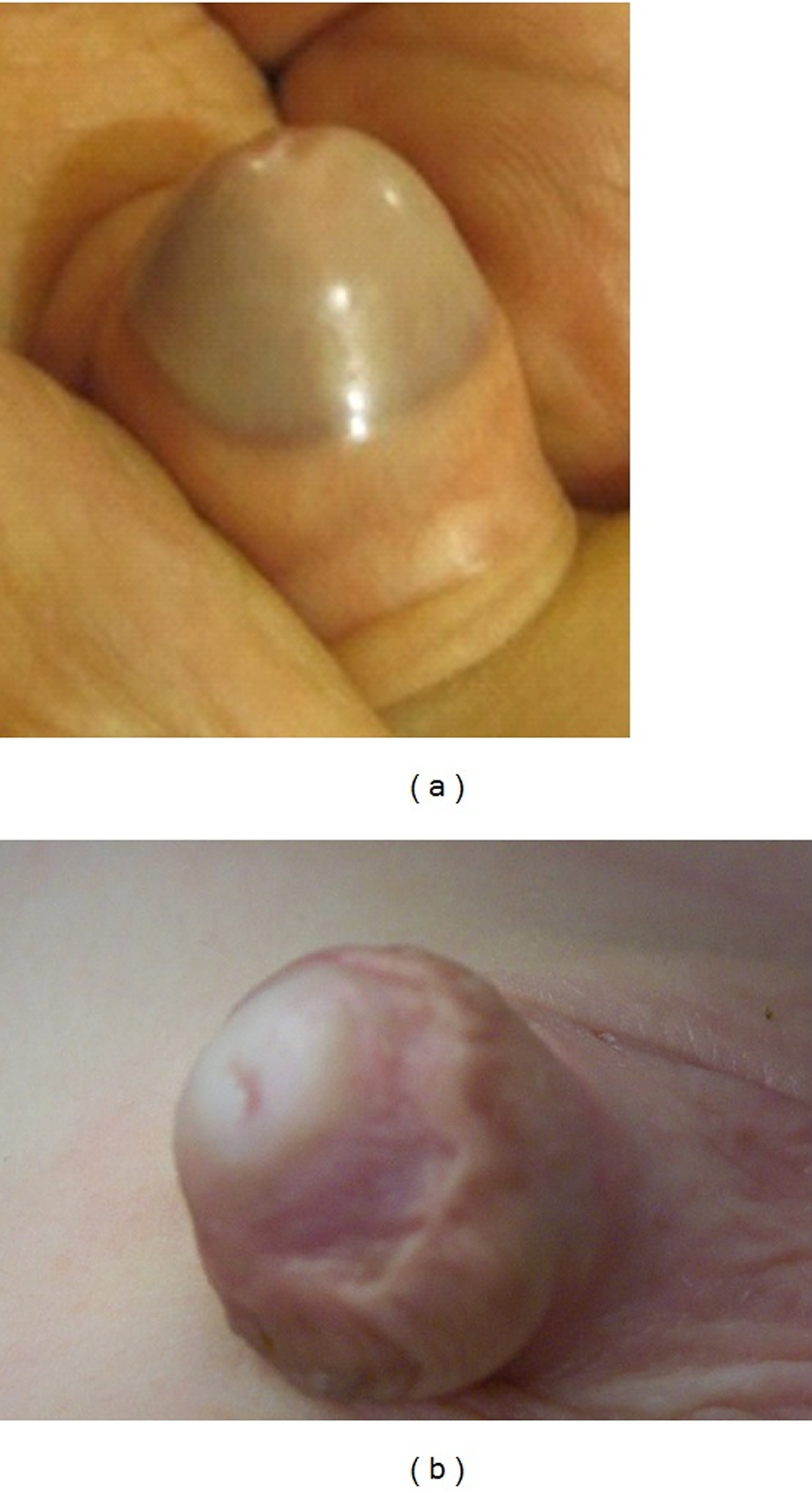
Note: Penile adhesions (a) between the shaft skin and the glans can be manually separated while penile skin bridges (b) cannot be manually separated and need to be excised—skin bridge.
[Source 61)]Meatitis/Meatal Stenosis
In the absence of the prepuce, the erythema of the meatus commonly occurs after circumcision as a result of irritation. Meatitis is commonly a self-limited problem but can be treated by application of an antibiotic ointment and keeping the area dry. Meatal stenosis has been postulated to be a result of ligation of the frenular artery or from ammoniacal meatitis 62) and account for 26% of the late complications 63). While the meatus may appear small, it can open adequately during voiding; this explains why most children with meatal stenosis do not present until after toilet training. Surgical treatment is indicated in the presence of symptoms such as deflection of the urine stream, dripping, dysuria, or urgency frequency from inadequate emptying. The treatment is meatotomy or meatoplasty, which can be accomplished under local anesthesia in the office or in the operating room.
Figure 10. Meatitis/Meatal Stenosis

Note: Meatal stenosis in a 3 year old circumcised male who presented with a narrow stream.
[Source 64)]Urethrocutaneous Fistula
Urethrocutaneous fistula is a rare complication, but nonetheless has been reported after both Plastibell and Gomco circumcisions 65). Fistulae may present as an obvious fistulous tract or as a split urine stream. Often this is a result of compression necrosis from a retained Plastibell ring or a direct injury from incorrect placement of the Gomco clamp. Injury to the urethra during any ventral dissection can occur during a “free-hand” circumcision. Delayed flap repair can be done electively after the child’s penis has grown enough for good tissue handling.
Glanular Necrosis/Glanular Amputation
Necrosis of the glans can occur as a result of cautery injury during a Gomco circumcision or from distal migration of an incorrectly sized Plastibell ring 66). Management of glans necrosis depends on its severity. Mild cases can be managed with local wound care and topical antibiotic ointment and allowing the necrotic skin to slough. Some authors report management of severe cases with suprapubic diversion and delayed urethroplasty 67). There are rare case reports of complete necrosis of the glans and phallus in which gender reassignment was performed after multiple attempts at staged repair 68). For this reason, the use of electrocautery is contraindicated in clamp circumcision.
Amputation of the glans occurs extremely rarely, but is a devastating complication of Mogen clamp circumcision. The Mogen clamp or shield seems uniquely susceptible to this particular injury given the surgeon’s inability to directly visualize the glans prior to incising the foreskin. Sherman et al. 69) report seven glanular reconstructions after traumatic amputations. The authors reported that minimal debridement and recovery of the amputated tissue were critical to the repair. Simple primary reanastomosis of glanular tissue was possible in 6 of 7 patients, the last patient required urethral reconstruction. The patient’s own tissue can remain viable up to 8 hours and used successfully for repair if adequately preserved by wrapping the tissue in moist saline gauze placed in a plastic bag and transported on ice 70).
Hypospadias
Isolated cases of iatrogenic hypospadias have been reported after the surgeon performed a ventral rather than a dorsal slit prior to initiation of circumcision 71). It is important that the proper plane be entered for the initial lysis of adhesions so that the meatus is not inadvertently entered and then damaged.
While not technically a complication, failure to recognize a hypospadias prior to circumcision may be problematic if there is insufficient skin for subsequent repair. While most cases of hypospadias are associated with a dorsally hooded prepuce, the megameatus with intact prepuce variant will have a configuration as described in its name. Thorough physical examination is imperative prior to circumcision regardless of the method employed.
References [ + ]





{kind=link}