Contents
What is a colonoscopy
Colonoscopy is a procedure that lets your doctor look inside your entire large intestine (colon) to detect changes or abnormalities in the large intestine and rectum. Doctors (gastroenterologists) use an instrument called colonoscope that have a tiny video camera and light source attached to a long, thin flexible tube, so that the large intestine (colon) can be viewed in detail. During a colonoscopy, a long, flexible tube (colonoscope) is inserted into your rectum/anus. The colonoscope is flexible and can be turned around corners so it can travel along the length of the large bowel. The colonoscopy procedures let your doctor see things such as inflamed tissue, abnormal growths (e.g. polyps, cancers) and ulcers. And if necessary, polyps or other types of abnormal tissue can be removed through the colonoscope during a colonoscopy. Tissue samples (biopsies) can be taken during a colonoscopy as well.
Your doctor may recommend a colonoscopy:
- To look for early signs of cancer in the colon and rectum. It may be part of a routine colon cancer screening, which usually starts at age 50. If you’re age 50 or older and at average risk of colon cancer — you have no colon cancer risk factors other than age — your doctor may recommend a colonoscopy every 10 years or sometimes sooner to screen for colon cancer. Colonoscopy is one option for colon cancer screening. Talk with your doctor about your options.
- To look for causes of unexplained changes in bowel habits
- To evaluate symptoms like abdominal pain, rectal bleeding, and weight loss
- Investigate intestinal signs and symptoms. A colonoscopy can help your doctor explore possible causes of abdominal pain, rectal bleeding, chronic constipation, chronic diarrhea and other intestinal problems.
- Look for more colon polyps. If you have had colon polyps before, your doctor may recommend a follow-up colonoscopy to look for and remove any additional polyps. This is done to reduce your risk of colon cancer.
You will get written bowel prep instructions to follow at home before the colonoscopy procedure. The bowel prep cleans out your intestine so your doctor can see everything clearly. During a colonoscopy, you get medicines to keep you relaxed.
Afterwards, you may feel drowsy, and it is best to arrange somebody to help you get home.
Your doctor may give you a brief report on what they saw, but you probably won’t get full results and further advice until later at a follow up appointment.
What should I expect after a colonoscopy?
After a colonoscopy, you can expect the following:
- The anesthesia takes time to wear off completely. You’ll stay at the hospital or outpatient center for 1 to 2 hours after the procedure.
- You may feel cramping in your abdomen or bloating during the first hour after the procedure.
- After the procedure, you—or a friend or family member—will receive instructions on how to care for yourself after the procedure. You should follow all instructions.
- You’ll need your pre-arranged ride home, since you won’t be able to drive after the procedure.
- You should expect a full recovery and return to your normal diet by the next day.
After the sedatives or anesthesia wear off, your doctor may share what was found during the procedure with you or, if you choose, with a friend or family member.
If the doctor removed polyps or performed a biopsy, you may have light bleeding from your anus. This bleeding is normal. A pathologist will examine the biopsy tissue, and results take a few days or longer to come back. A health care professional will call you or schedule an appointment to go over the results.
Colonoscopy Results
Your doctor will review the results of the colonoscopy and then share the results with you.
Negative result
A colonoscopy is considered negative if the doctor doesn’t find any abnormalities in the colon.
Your doctor may recommend that you have another colonoscopy:
- In 10 years, if you’re at average risk of colon cancer — you have no colon cancer risk factors other than age
- In five years, if you have a history of polyps in previous colonoscopy procedures
- In one year, if there was residual stool in the colon that prevented complete examination of your colon
Positive result
A colonoscopy is considered positive if the doctor finds any polyps or abnormal tissue in the colon.
Most polyps aren’t cancerous, but some can be precancerous. Polyps removed during colonoscopy are sent to a laboratory for analysis to determine whether they are cancerous, precancerous or noncancerous.
Depending on the size and number of polyps, you may need to follow a more rigorous surveillance schedule in the future to look for more polyps.
If your doctor finds one or two polyps less than 0.4 inch (1 centimeter) in diameter, he or she may recommend a repeat colonoscopy in five to 10 years, depending on your other risk factors for colon cancer.
Your doctor will recommend another colonoscopy sooner if you have:
- More than two polyps
- A large polyp — larger than 0.4 inch (1 centimeter)
- Polyps and also residual stool in the colon that prevents complete examination of the colon
- Polyps with certain cell characteristics that indicate a higher risk of future cancer
- Cancerous polyps
If you have a polyp or other abnormal tissue that couldn’t be removed during the colonoscopy, your doctor may recommend a repeat exam with a gastroenterologist who has special expertise in removing large polyps, or surgery.
Problems with your exam
If your doctor is concerned about the quality of the view through the scope, he or she may recommend a repeat colonoscopy or a shorter time until your next colonoscopy. If your doctor wasn’t able to advance the scope through your entire colon, a barium enema or virtual colonoscopy may be recommended to examine the rest of your colon.
Screening for Colon and Rectal Cancer
Your doctor will recommend screening for colon and rectal cancer —also called colorectal cancer—starting at age 50 if you don’t have health problems or risk factors that make you more likely to develop colon cancer 1).
You have risk factors for colorectal cancer if you 2):
- are male
- are African American
- or someone in your family has had polyps or colorectal cancer
- have a personal history of inflammatory bowel disease, such as ulcerative colitis and Crohn’s disease
- have Lynch syndrome , or another genetic disorder that increases the risk of colorectal cancer
- have other factors, such as that you weigh too much or smoke cigarettes
If you are more likely to develop colorectal cancer, your doctor may recommend screening at a younger age, and more often.
If you are older than age 75, talk with your doctor about whether you should be screened. For more information, read the current colorectal cancer screening guidelines from the U.S. Preventive Services Task Force 3).
Government health insurance plans, such as Medicare, and private insurance plans sometimes change whether and how often they pay for cancer screening tests. Check with your insurance plan to find out how often your plan will cover a screening colonoscopy.
Colon cancer screening: At what age can you stop?
People older than age 75 who have been getting regular colon cancer screening since age 50 and who have had consistently negative screenings — no polyps (adenomas) or colon cancer — and are not at an increased risk of colon cancer because of family history may not need to continue getting routine screening. That’s according to colon cancer screening guidelines issued by the U.S. Preventive Services Task Force and the American College of Physicians.
The upper age limit was set after studies determined that the net benefit of screening after age 75 was small. However, the U.S. Preventive Services Task Force guidelines 4) do recommend colon cancer surveillance for people older than age 75 who have an increased risk of colon cancer, such as family history, a previously diagnosed colon cancer or adenomatous polyps.
- Adults aged 50 to 75 years: The U.S. Preventive Services Task Force recommends screening for colorectal cancer starting at age 50 years and continuing until age 75 years 5).
- Adults aged 76 to 85 years: The decision to screen for colorectal cancer in adults aged 76 to 85 years should be an individual one, taking into account the patient’s overall health and prior screening history 6).
- Adults in this age group who have never been screened for colorectal cancer are more likely to benefit.
- Screening would be most appropriate among adults who 1) are healthy enough to undergo treatment if colorectal cancer is detected and 2) do not have comorbid conditions that would significantly limit their life expectancy.
The American Cancer Society and the American College of Gastroenterology don’t specify an upper age limit beyond which colon cancer screening is no longer recommended.
The U.S. Preventive Services Task Force and American College of Physicians recommend that colon cancer screening be done using one or a combination of screening strategies:
- Colonoscopy
- Fecal occult blood testing (FOBT)
- Fecal immunochemical testing (FIT)
- Stool DNA testing
- Sigmoidoscopy
- Computed tomography colonography (virtual colonoscopy)
Talk with your doctor about what colon cancer screening option is best for you. Together, you can decide based on your overall health when screening may no longer be of benefit.
Colonoscopy risks and side effects
A colonoscopy poses few risks. Rarely, complications of a colonoscopy may include:
- Adverse reaction to the sedative used during the colonoscopy, including breathing or heart problems
- Bleeding from the site where a tissue sample (biopsy) was taken or a polyp or other abnormal tissue was removed
- A tear in the colon or rectum wall (perforation)
- Severe pain in your abdomen
- Death, although this risk is rare
A study of screening colonoscopies found roughly 4 to 8 serious complications for every 10,000 procedures 7).
Bleeding and perforation are the most common complications from colonoscopy. Most cases of bleeding occur in patients who have polyps removed. The doctor can treat bleeding that happens during the colonoscopy right away.
You may have delayed bleeding up to 2 weeks after the procedure. The doctor can diagnose and treat delayed bleeding with a repeat colonoscopy. The doctor may need to treat perforation with surgery.
After discussing the risks of colonoscopy with you, your doctor will ask you to sign a consent form authorizing the procedure.
Seek Care Right Away
If you have any of the following symptoms after a colonoscopy, seek medical care right away:
- severe pain in your abdomen
- fever
- bloody bowel movements that do not get better
- bleeding from the anus that does not stop
- dizziness
- weakness
Large intestine
The large intestine extends from the distal end of the ileum to the anus, a distance of approximately 1.5 m in adults (5 ft) long and 6.5 cm (2.5 in.) in diameter. The large intestine is named for its relatively large diameter, not its length. The large intestine absorbs fluids and salts from the gut contents, thus forming feces. The large intestine consists of the cecum, appendix, colon, rectum, and anal canal.
Beginning in the right groin as the cecum, with its associated appendix, the large intestine continues upward as the ascending colon through the right flank and into the right hypochondrium. The ascending colon begins at the ileocecal valve and passes up the right side of the abdominal cavity. It makes a 90° turn at the right colic (hepatic) flexure, near the right lobe of the liver, and crosses the abdomen as the transverse colon to the left hypochondrium. At this position, just below the spleen, the large intestine bends downward, forming the left colic flexure (splenic flexure) and continues as the descending colon through the left flank and into the left groin. Ascending, transverse, and descending colons thus form a squarish, three-sided frame around the small intestine.
The cecum is a blind pouch in the lower right abdominal quadrant inferior to the ileocecal valve. Attached to its lower end is the appendix, a blind tube 2 to 7 cm long. The appendix is densely populated with lymphocytes and is a significant source of immune cells.
The pelvic cavity is narrower than the abdominal cavity, so at the hip bone, the colon turns medially and travels along the iliac fossa before turning downward at the pelvic inlet into the pelvic cavity. The resulting S-shaped portion of the tract is called the sigmoid colon. Visual examination of this region is performed with an instrument called a sigmoidoscope. In the pelvic cavity, the large intestine continues as the rectum, about 15 cm long. Despite its name, the rectum is not quite straight but has three lateral curves as well as an anteroposterior curve. It has three infoldings called transverse rectal folds (rectal valves), which enable it to retain feces while passing gas.
The final 3 cm of the large intestine is the anal canal, which passes through the levator ani muscle of the pelvic floor and terminates at the anus. Here, the mucosa forms longitudinal ridges called anal columns with depressions between them called anal sinuses. As feces pass through the canal, they press the sinuses and cause them to exude extra mucus and lubricate the canal during defecation. Prominent hemorrhoidal veins form superficial plexuses in the anal columns and around the orifice. Unlike veins in the limbs, they lack valves and are particularly subject to distension and venous pooling. Hemorrhoids are permanently distended veins that protrude into the anal canal or form bulges external to the anus. They can result from the impaired venous return that occurs in obesity and pregnancy.
Figure 1. Large intestine
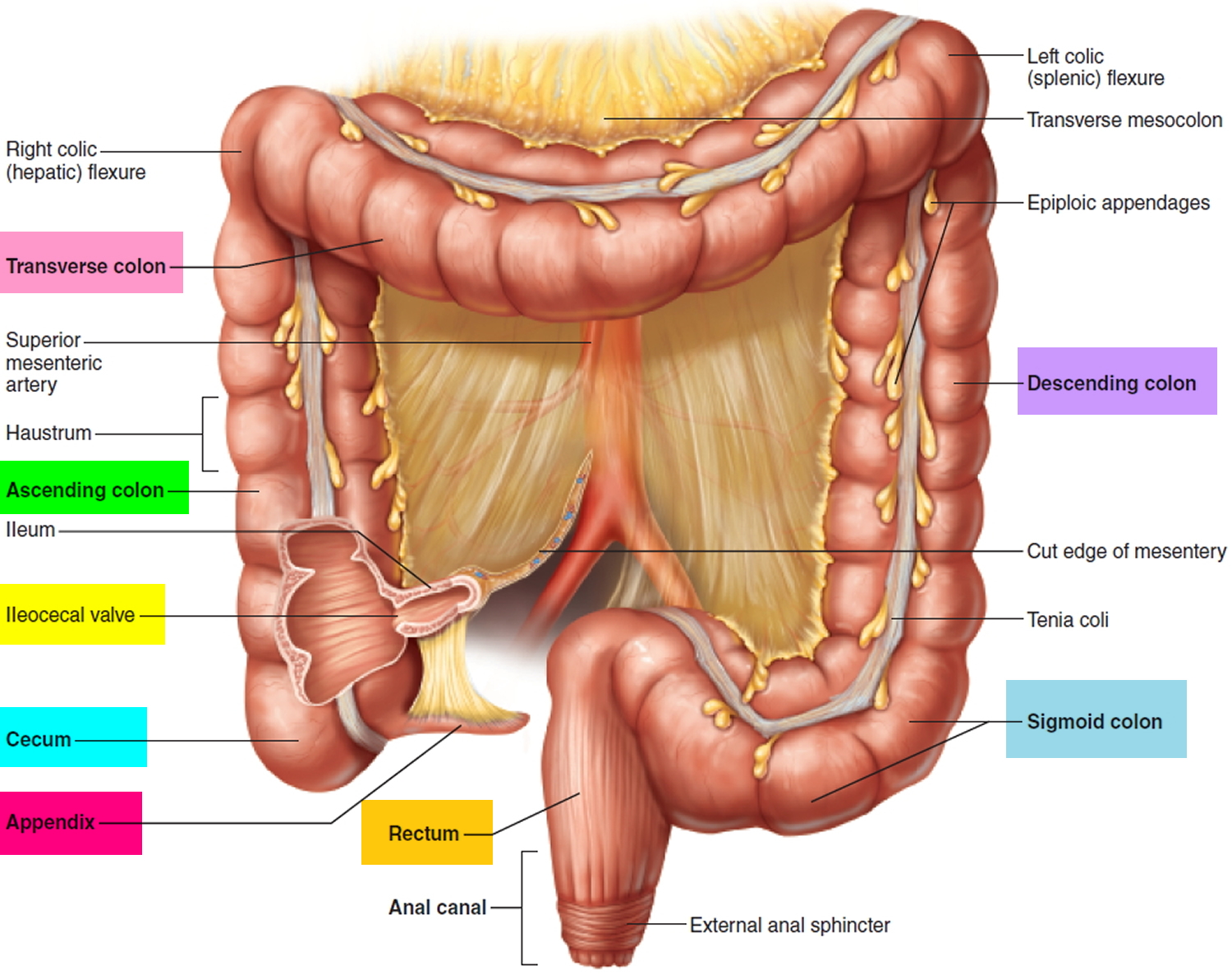
Figure 2. Large intestine and small intestine
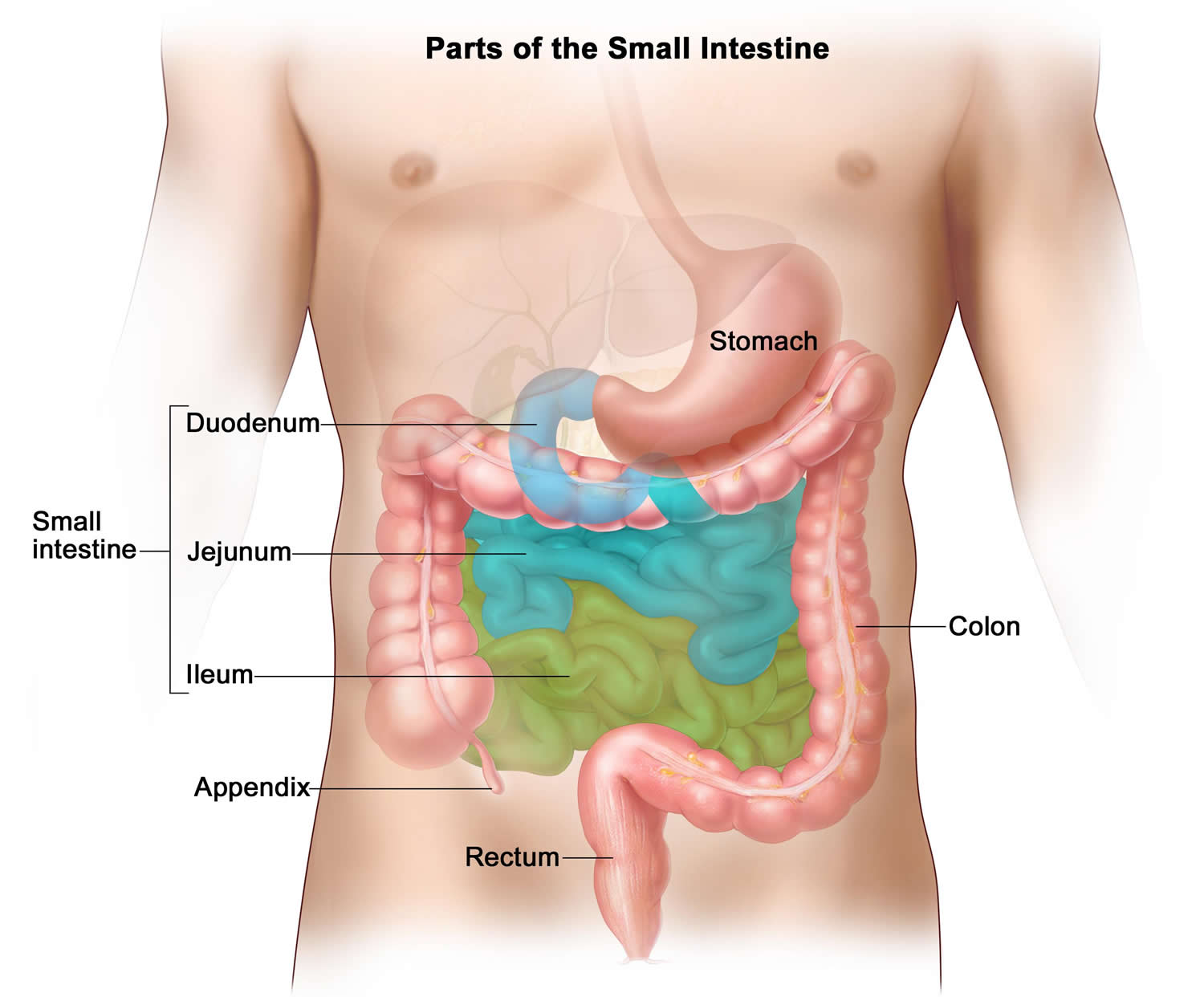
Figure 3. Colonoscopy
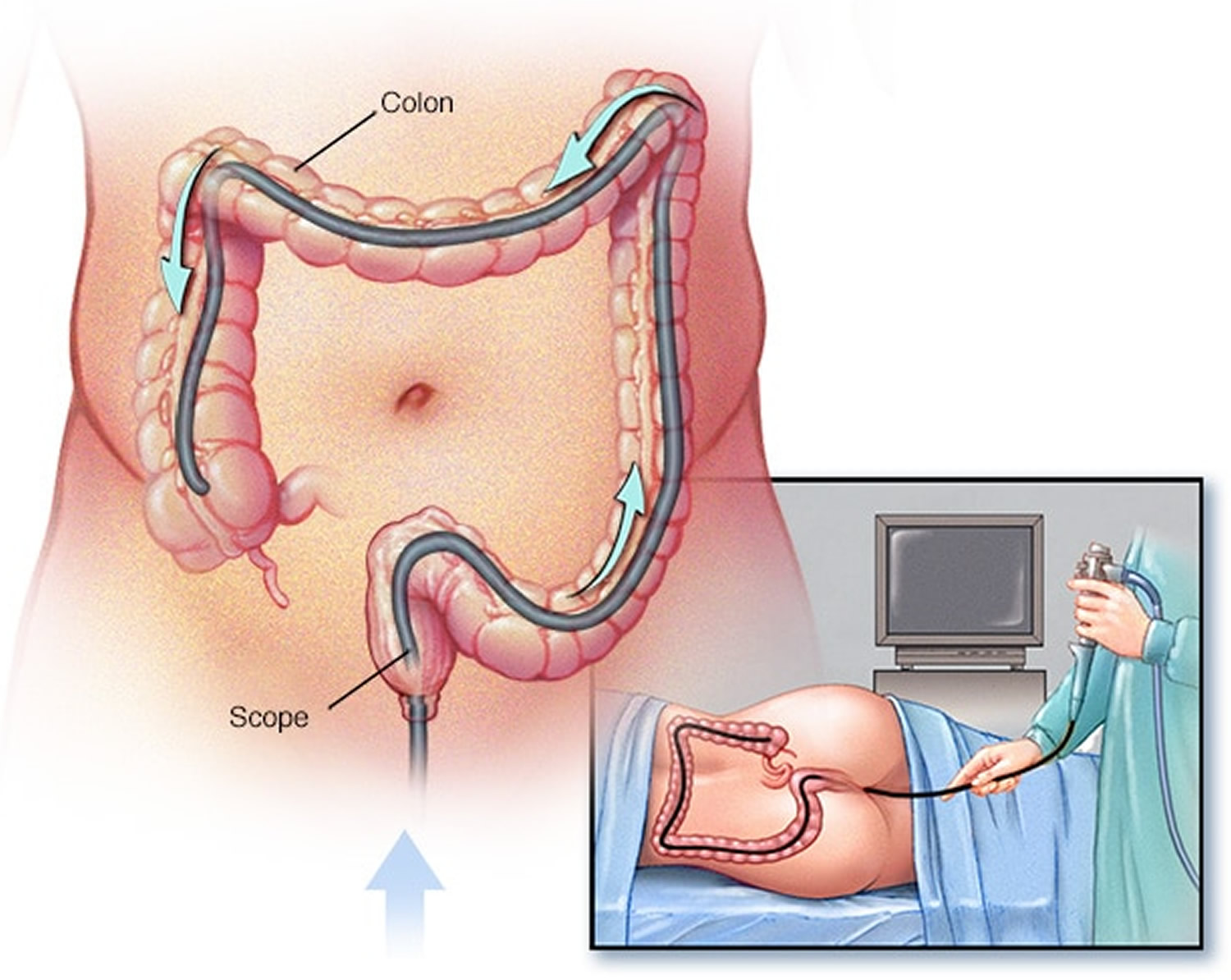 Figure 4. Colonoscopy polyps
Figure 4. Colonoscopy polyps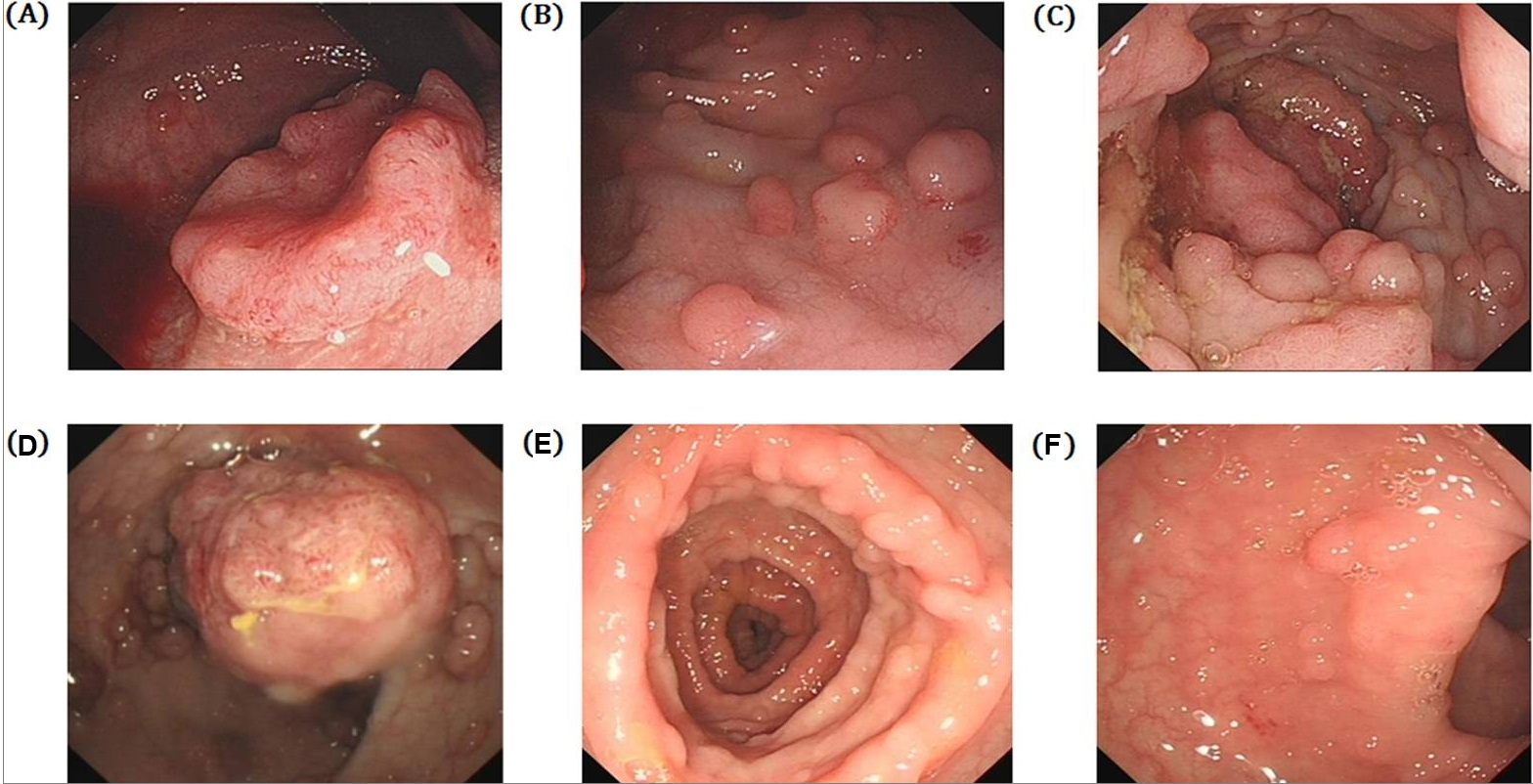
Notes: (A) Lower rectum, (B) Sigmoid colon, (C) Upper rectum, (D) Rectum. (F and G). Familial adenomatous polyposis (FAP), there are nearly 100 polps in colorectum, distributed dispersively, maximum diameter is 0.5 cm. (A to C) There are nearly 100 polyps in sigmoid colon and rectum, the polyps of rectum are malignant transformation, the sigmoid colon is consisting of multiple polyps.
[Source 8)]How to prepare for a colonoscopy
If you are having a colonoscopy, there are a number of steps that need to be followed to get the best result.
Before a colonoscopy, you’ll need to clean out (empty) your colon. Any fecal residue in your colon may obscure the view of your colon and rectum during the colonoscopy procedure.
The preparations vary between clinics but the aim is to clear the colon of feces so the doctor can get the best view on examination.
Arrange for a ride home
For safety reasons, you can’t drive for 24 hours after the procedure, as the sedatives or anesthesia need time to wear off. You will need to make plans for getting a ride home after the procedure.
Colonoscopy prep instructions
You should talk with your doctor about any health problems you have and all prescribed and over-the-counter medicines, vitamins, and supplements you take, including:
- arthritis medicines
- aspirin or medicines that contain aspirin
- blood thinners
- diabetes medicines
- nonsteroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen or naproxen
- vitamins that contain iron or iron supplements
Colonoscopy Diet
Your doctor will give you written bowel prep instructions to follow at home before the procedure so that little or no stool remains in your intestine. A complete bowel prep lets you pass stool that is clear and liquid. Stool inside your intestine can prevent your doctor from clearly seeing the lining.
Follow a special diet the day before the exam. Typically, you won’t be able to eat solid food the day before the exam. Drinks may be limited to clear liquids — plain water, tea and coffee without milk or cream, broth, and carbonated beverages. Avoid red liquids, which can be confused with blood during the colonoscopy. You may not be able to eat or drink anything after midnight the night before the exam.
You may need to follow a clear liquid diet for 1 to 3 days before the procedure. You should avoid red and purple-colored drinks or gelatin. The instructions will include details about when to start and stop the clear liquid diet. In most cases, you may drink or eat the following:
- fat-free bouillon or broth
- gelatin in flavors such as lemon, lime, or orange
- plain coffee or tea, without cream or milk
- sports drinks in flavors such as lemon, lime, or orange
- strained fruit juice, such as apple or white grape—avoid orange juice
- water
To empty your colon
Different bowel preps may contain different combinations of laxatives—pills that you swallow or powders that you dissolve in water or clear liquids. Some people will need to drink a large amount, often a gallon, of liquid laxative over a scheduled amount of time—most often the night before and the morning of the procedure. Your doctor may also prescribe an enema.
The bowel prep will cause diarrhea, so you should stay close to a bathroom. You may find this part of the bowel prep hard; however, finishing the prep is very important. Call a health care professional if you have side effects that keep you from finishing the prep.
Your doctor will tell you how long before the procedure you should have nothing by mouth.
- The day before the colonoscopy, you may be asked to drink a bowel preparation, a laxative. This is a flavored powder that is mixed with water. It causes diarrhea to empty the colon. Your doctor will usually recommend you take a laxative, in either pill form or liquid form. You may be instructed to take the laxative the night before your colonoscopy, or you may be asked to use the laxative both the night before and the morning of the procedure. It’s best to do the bowel preparation at home. The area around your anus may become irritated from diarrhea. Showering, and using moist wipes instead of toilet paper, may ease this discomfort. It is important to drink only clear fluids on the day before, and not eat solid foods or dairy products like milk. You will be allowed to have fluids like water, clear fruit juice, clear carbonated drinks and clear soup. You will probably be told to have no fluids in the 6 hours before the colonoscopy.
- Use an enema kit. In some cases, you may need to use an over-the-counter enema kit — either the night before the exam or a few hours before the exam — to empty your colon. This is generally only effective in emptying the lower colon and is usually not recommended as a primary way of emptying your colon.
- If you take regular medication, talk to your doctor. Some medications should be taken and some can be delayed. It is particularly important to talk to your doctor if you take blood-thinning medications.
- Adjust your medications. Remind your doctor of your medications at least a week before the exam — especially if you have diabetes, high blood pressure or heart problems or if you take medications or supplements that contain iron.
- Also tell your doctor if you take aspirin or other medications that thin the blood, such as warfarin (Coumadin, Jantoven); newer anticoagulants, such as dabigatran (Pradaxa) or rivaroxaban (Xarelto), used to reduce risk of blot clots or stroke; or heart medications that affect platelets, such as clopidogrel (Plavix). You may need to adjust your dosages or stop taking the medications temporarily.
Split Dose Regimen for colonoscopy preparation
“Splitting” implies that roughly half of the bowel cleansing dose is given on the day of the colonoscopy. Overwhelmingly consistent data show superior efficacy with a split dose compared with the traditional regimen of administering the preparation the day before the procedure 9). Split dosing leads to higher adenoma detection rates 10). Four guidelines have endorsed split dosing of preparations for colonoscopy 11), 12), 13), 14).
To make bowel preparation more tolerable, many doctors recommend splitting the dose of bowel preparation. This regimen may not be possible if your colonoscopy is scheduled for early in the morning, because you should consume the morning dose four to six hours prior to the procedure.
If your procedure is scheduled at a time that allows you to split the dose, take the recommended amount of the bowel cleansing liquid the night before the exam, and the remainder in the morning before the test. Depending on the type of preparation, your doctor may recommend splitting the dose 1-to-1 or 3-to-1.
The biggest reason for poor colonoscopy preparation is people’s distaste for having to drink large quantities of bowel cleaning solution. The most common colonoscopy preparation calls for drinking 1 gallon (4 liters) of a polyethylene glycol solution. Some studies have shown that more than a third of people don’t complete the full preparation.
Studies have shown that the split-dose approach not only is more tolerable, but also does a better job of cleaning the colon. Better cleaning will lead to better results. One study found that doctors detected more benign tumors (adenomas) in people who prepared with split doses than in people who prepared with single doses.
Cleaning as much waste material as possible from your large intestine (colon) is crucial to a successful colonoscopy exam. Poor colonoscopy preparation can keep your doctor from finding polyps, tumors and other problems. It also increases the length of the exam and the risk of complications. In many cases, the exam has to be redone.
Ask your doctor about split-dose preparation for your next colonoscopy.
During the colonoscopy procedure
A doctor performs a colonoscopy in a hospital or an outpatient center. The colonoscopy procedure is painless and lasts about 30 to 60 minutes. Most people have a mild anesthetic/sedation and can remember nothing or very little. A health care professional will place an intravenous (IV) needle in a vein in your arm or hand to give you sedatives, anesthesia, or pain medicine, so you won’t be aware or feel pain during the procedure. The health care staff will check your vital signs and keep you as comfortable as possible.
During a colonoscopy, you’ll wear a gown, but likely nothing else. Sedation is usually recommended. Sometimes a mild sedative is given in pill form. In other cases, the sedative is combined with an intravenous pain medication to minimize any discomfort.
For the procedure, you’ll lie on your side on the exam table, usually with your knees drawn toward your chest while the doctor inserts a colonoscope through your anus and into your rectum and colon. The scope inflates your large intestine with air for a better view.
The colonoscope — which is long enough to reach the entire length of your colon — contains a light and a tube (channel) that allows the doctor to pump air or carbon dioxide into your colon. The air or carbon dioxide inflates the colon, which provides a better view of the lining of the colon.
When the colonoscope is moved or air is introduced, you may feel abdominal cramping or the urge to have a bowel movement.
The colonoscope also contains a tiny video camera at its tip. The camera sends images to an external monitor so that the doctor can study the inside of your colon.
The doctor can also insert instruments through the channel to take tissue samples (biopsies) or remove polyps or other areas of abnormal tissue.
The doctor may move you several times on the table to adjust the scope for better viewing. Once the colonoscope reaches the opening to your small intestine, the doctor slowly removes the colonoscope and examines the lining of your large intestine again.
During the procedure, the doctor may remove polyps and will send them to a lab for testing. You will not feel the polyp removal. Colon polyps are common in adults and are harmless in most cases. However, most colon cancer begins as a polyp, so removing polyps early helps to prevent cancer.
If your doctor finds abnormal tissue, he or she may perform a biopsy. You won’t feel the biopsy.
How long does a colonoscopy take?
A colonoscopy typically takes about 30 to 60 minutes.
Colonoscopy recovery
After the colonoscopy procedure, it takes about an hour for you to begin to recover from the sedative. You’ll need someone to take you home because it can take up to a day for the full effects of the sedative to wear off. Don’t drive or make important decisions or go back to work for the rest of the day.
If your doctor removed a polyp during your colonoscopy, you may be advised to eat a special diet temporarily.
You may feel bloated or pass gas for a few hours after the exam, as you clear the air from your colon. Walking may help relieve any discomfort.
You may also notice a small amount of blood with your first bowel movement after the exam. Usually this isn’t cause for alarm. Consult your doctor if you continue to pass blood or blood clots or if you have persistent abdominal pain or a fever. While unlikely, this may occur immediately or in the first few days after the procedure, but may be delayed for up to one to two weeks.
Alternative to colonoscopy
Virtual colonoscopy is also called computerized tomography (CT) colonography, is a procedure in which a radiologist uses x-rays and a computer to create images of your rectum and colon from outside the body. Virtual colonoscopy can show ulcers, polyps, and cancer 15).
How is virtual colonoscopy different from colonoscopy?
Virtual colonoscopy and colonoscopy are different in several ways:
- Virtual colonoscopy is an x-ray test, takes less time, and you don’t need anesthesia.
- With virtual colonoscopy, your doctor doesn’t view the entire length of your colon.
- Virtual colonoscopy may not find certain polyps as easily as a colonoscopy can.
- Doctors can’t remove polyps or treat certain other problems during a virtual colonoscopy.
- Your health insurance coverage may be different for the two procedures.
Why do doctors use colonoscopy?
A colonoscopy can help a doctor find the cause of symptoms, such as:
- bleeding from your anus
- changes in your bowel activity, such as diarrhea
- pain in your abdomen
- unexplained weight loss
Doctors also use colonoscopy as a screening tool for colon polyps and cancer . Screening is testing for diseases when you have no symptoms. Screening may find diseases at an early stage, when a doctor has a better chance of curing the disease.
Why do doctors use virtual colonoscopy?
Doctors mainly use virtual colonoscopy to screen for polyps or cancer. Screening may find diseases at an early stage, when a doctor has a better chance of curing the disease.
Occasionally, doctors may use virtual colonoscopy when colonoscopy is incomplete or not possible due to other medical reasons.
What are the risks of a virtual colonoscopy?
Inflating the colon with air has a small risk of perforating the lining of the large intestine. The doctor may need to treat perforation with surgery.
Seek care right away
If you have any of the following symptoms after a virtual colonoscopy, you should seek medical attention right away:
- severe pain in your abdomen
- fever
- bloody bowel movements or bleeding from your anus
- dizziness
- weakness
How do I prepare for a virtual colonoscopy?
To prepare for a virtual colonoscopy, you will need to talk with your doctor, change your diet, clean out your bowel, and drink a special liquid called contrast medium. The contrast medium makes your rectum and colon easier to see in the x-rays.
Talk with your doctor
You should talk with your doctor about any medical conditions you have and all prescribed and over-the-counter medicines, vitamins, and supplements you take, including:
- arthritis medicines
- aspirin or medicines that contain aspirin
- blood thinners
- diabetes medicines
- nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen or naproxen
- vitamins that contain iron or iron supplements
X-rays may interfere with personal medical devices. Tell your doctor if you have any implanted medical devices, such as a pacemaker.
Doctors don’t recommend x-rays for pregnant women because x-rays may harm the fetus. Tell your doctor if you are, or may be, pregnant. Your doctor may suggest a different procedure, such as a colonoscopy.
Change your diet and clean out your bowel
As in colonoscopy, a health care professional will give you written bowel prep instructions to follow at home before the procedure. A health care professional orders a bowel prep so that little or no stool is present in your intestine. A complete bowel prep lets you pass stool that is clear and liquid. Stool inside your colon can prevent the x-ray machine from taking clear images of the lining of your intestine.
You may need to follow a clear liquid diet the day before the procedure. The instructions will provide specific direction about when to start and stop the clear liquid diet. In most cases, you may drink or eat the following:
- fat-free bouillon or broth
- gelatin in flavors such as lemon, lime, or orange
- plain coffee or tea, without cream or milk
- sports drinks in such flavors as lemon, lime, or orange
- strained fruit juice, such as apple or white grape—doctors recommend avoiding orange juice and red or purple beverages
- water
Your doctor will tell you how long before the procedure you should have nothing by mouth.
A health care professional will ask you to follow the directions for a bowel prep before the procedure. The bowel prep will cause diarrhea, so you should stay close to a bathroom.
Different bowel preps may contain different combinations of laxatives—pills that you swallow or powders that you dissolve in water and other clear liquids, and enemas. Some people will need to drink a large amount, often a gallon, of liquid laxative over a scheduled amount of time—most often the night before the procedure.
You may find this part of the bowel prep difficult; however, completing the prep is very important. The images will not be clear if the prep is incomplete.
You may find this part of the bowel prep difficult; however, completing the prep is very important. The images will not be clear if the prep is incomplete.
Drink contrast medium
The night before the procedure, you will drink a contrast medium. Contrast medium is visible on x-rays and can help your doctor tell the difference between stool and polyps.
The virtual colonoscopy procedure
A specially trained x-ray technician performs a virtual colonoscopy at an outpatient center or a hospital. You do not need anesthesia.
For the procedure, you will lie on a table while the technician inserts a thin tube through your anus and into your rectum. The tube inflates your large intestine with air for a better view. The table slides into a tunnel-shaped device where the technician takes the x-ray images. The technician may ask you to hold your breath several times during the procedure to steady the images. The technician will ask you to turn over on your side or stomach so he or she can take different images of the large intestine. The procedure lasts about 10 to 15 minutes.
What should I expect after a virtual colonoscopy?
After a virtual colonoscopy, you can expect to:
- feel cramping or bloating during the first hour after the test
- resume your regular activities right after the test
- return to a normal diet
After the test, a radiologist looks at the images to find any problems and sends a report to your doctor. If the radiologist finds problems, your doctor may perform a colonoscopy the same day or at a later time.
References [ + ]





{kind=link}