Contents
- What is dermatitis
- What is Atopic Dermatitis
- What is Contact Dermatitis
- Causes of contact dermatitis
- Allergic contact dermatitis
- Irritant contact dermatitis
- When to seek immediate medical care for contact dermatitis
- Risk factors for contact dermatitis
- Signs and symptoms of Contact dermatitis
- Complications of contact dermatitis
- Prevention of contact dermatitis
- Diagnosis of Contact dermatitis
- Contact dermatitis treatment
- Outcome for patients with contact dermatitis
- What is nummular dermatitis
- What is stasis dermatitis
- What is seborrheic dermatitis
- What is perioral dermatitis
- What is dermatitis herpetiformis
What is dermatitis
Dermatitis also called eczema is a term for several different types of skin swelling 1.
Most dermatitis types cause dry, itchy skin and rashes on the face, inside the elbows and behind the knees, and on the hands and feet. Scratching the skin can cause it to turn red, and to swell and itch even more.
Dermatitis is not contagious. The cause is not known. It is likely caused by both genetic and environmental factors. Dermatitis may get better or worse over time, but it is often a long-lasting disease. People who have it may also develop hay fever and asthma.
The most common type of eczema is atopic dermatitis. It is most common in babies and children but adults can have it too. As children who have atopic dermatitis grow older, this problem may get better or go away. But sometimes the skin may stay dry and get irritated easily.
Treatments may include medicines, skin creams, light therapy, and good skin care. You can prevent some types of eczema by avoiding:
- Things that irritate your skin, such as certain soaps, fabrics, and lotions
- Stress
- Things you are allergic to, such as food, pollen, and animals
What is Atopic Dermatitis
This is a common chronic skin disease in children characterized by itchy, inflamed skin that can weep clear fluid when scratched. Atopic dermatitis is a non-contagious inflammatory skin condition 2. People with eczema also may be particularly susceptible to bacterial, viral, and fungal skin infections. Atopic dermatitis is so common that people have given it a few names 3:
- Eczema (name most people use)
- Dermatitis
- Atopic eczema
- Atopic dermatitis
To avoid confusion, we’ll use the medical term atopic dermatitis.
Children often get atopic dermatitis during their first year of life. If a child gets atopic dermatitis during this time, dry and scaly patches appear on the skin. These patches often appear on the scalp, forehead, and face. These patches are very common on the cheeks.
No matter where it appears, atopic dermatitis is often very itchy. Infants may rub their skin against bedding or carpeting to relieve the itch.
In children of all ages, the itch can be so intense that a child cannot sleep. Scratching can lead to a skin infection.
Because atopic dermatitis can be long lasting, it is important to learn how to take care of the skin. Treatment and good skin care can alleviate much of the discomfort.
Figure 1. Atopic dermatitis

Signs and symptoms of atopic dermatitis
Atopic dermatitis looks different in infants, children and adults. The following gives you the signs (what you see) and symptoms (what you feel) for each age group.
Infants atopic dermatitis
Atopic dermatitis can begin early. A child may be 2 or 3 months old when atopic dermatitis begins. When atopic dermatitis begins early, it often causes:
A rash that appears suddenly and:
- makes the skin dry, scaly, and itchy.
- forms on the scalp and face, especially on the cheeks (can appear on other areas of the body).
- can bubble up, then ooze and weep fluid.
- causes itching that may come and go.
Rubbing against bedding, carpeting, and other things in order to scratch the itch.
Trouble sleeping.
Skin infections, common due to rubbing and scratching.
Parents often worry that their babies are getting atopic dermatitis in the diaper area. A babies rarely gets atopic dermatitis in his or her diaper area. The skin stays too moist for atopic dermatitis.
Children atopic dermatitis
When atopic dermatitis begins between 2 years of age and puberty, the child often has these signs and symptoms:
- A rash that often begins in the creases of the elbows or knees. Other common places for the rash to appear are the neck, wrists, ankles, and/or crease between the buttocks and legs.
Itchy, scaly patches where the rash appeared.
In time, the skin with atopic dermatitis can:
- Get bumpy, looking like permanent goose bumps.
- Lighten (or darken) where atopic dermatitis appears.
- Thicken, turning leathery to protect itself from constant scratching.
- Develop knots (only on the thickened skin).
- Itch all the time (only on the thickened skin).
The thickened skin can itch even when the atopic dermatitis is not flaring.
When talking about the thickened skin, your dermatologist may use the word lichenification. This word means thickened skin.
Adults atopic dermatitis
It is rare for adults to get atopic dermatitis. Most people (90%) get atopic dermatitis before age 5. About half (50%) of people who get atopic dermatitis during childhood continue to have milder signs and symptoms of atopic dermatitis as an adult. When an adult has atopic dermatitis, it often looks different from the atopic dermatitis of childhood. For adults, atopic dermatitis often:
- Appears in the creases of the elbows or knees and nape of neck.
- Covers much of the body.
- Can be especially noticeable on the neck and face.
- Can be especially bad around the eyes.
- Causes very dry skin.
- Causes non-stop itch.
- Causes scaly skin — more scaly than in infants and children.
- Leads to skin infections.
If a person has had atopic dermatitis for years, patches of skin may be thick and darker than the rest of the skin (or lighter). Thickened skin can itch all the time.
Adults who had atopic dermatitis. as a child and no longer have atopic dermatitis. can have the following:
- Extremely dry skin.
- Skin that is easily irritated.
- Hand eczema.
- Eye problems (eczema on eyelids, cataracts).
Who gets atopic dermatitis ?
Around the world, between 10% and 20% of children have atopic dermatitis. About 1% to 3% of adults have atopic dermatitis. People of all skin colors get atopic dermatitis.
Most people (90%) get atopic dermatitis before their 5th birthday. Atopic dermatitis rarely starts when a person is an adult.
Atopic dermatitis is much more common today than it was 30 years ago. Dermatologists are not sure why. They do know that some children have a greater risk of getting atopic dermatitis. The following seem to increase a child’s risk of getting atopic dermatitis:
- Family members have atopic dermatitis, asthma, or hay fever: Does the child’s mother or father have atopic dermatitis ? Does a parent have asthma or hay fever? A family history of these diseases remains the strongest risk factor. If one or both parents have atopic dermatitis or an allergic condition, the child is much more likely to get atopic dermatitis. Some children get all 3 diseases. Asthma and hay fever usually appear before the age of 30. People often have asthma and hay fever for life.
- Where child lives: Living in a developed country, city (especially one with higher levels of pollution), or a cold climate seems to increase the risk. For example, Jamaican children living in London are twice as likely to develop atopic dermatitis as those who live in Jamaica.
- Gender: Females are slightly more likely than males to get atopic dermatitis.
- Mother’s age when child born: When the mother gives birth to the child later in her childbearing years, a child is more likely to get atopic dermatitis.
- Social class: atopic dermatitis seems more common in higher social classes.
What causes atopic dermatitis ?
Researchers are still studying what causes atopic dermatitis. A combination of genetic and environmental factors appears to be involved in the development of eczema.
The condition often is associated with other allergic diseases such as asthma, hay fever, and food allergy. Children whose parents have asthma and allergies are more likely to develop atopic dermatitis than children of parents without allergic diseases. Approximately 30 percent of children with atopic dermatitis have food allergies, and many develop asthma or respiratory allergies. People who live in cities or drier climates also appear more likely to develop the disease.
Through their studies, they have learned that atopic dermatitis:
- Is not contagious: There is no need to worry about catching it or giving it to someone.
- Runs in families: People who get atopic dermatitis usually have family members who have atopic dermatitis, asthma, or hay fever. This means that genes play a role in causing atopic dermatitis.
+ Children are more likely to develop atopic dermatitis if one or both parents have atopic dermatitis, asthma, or hay fever.
+ About half (50%) of the people with severe atopic dermatitis (covers a large area of the body or is very troublesome) will get asthma and about two-thirds (66%) will get hay fever.
The condition tends to worsen when a person is exposed to certain triggers, such as:
- Pollen, mold, dust mites, animals, and certain foods (for allergic individuals)
- Cold and dry air
- Colds or the flu
- Skin contact with irritating chemicals
- Skin contact with rough materials such as wool
- Emotional factors such as stress
- Fragrances or dyes added to skin lotions or soaps.
Taking too many baths or showers and not moisturizing the skin properly afterward may also make eczema worse.
Can certain foods cause atopic dermatitis ?
Foods do not cause atopic dermatitis. But some studies suggest that food allergies can make atopic dermatitis worse. Children who have atopic dermatitis often have food allergies to these foods — milk and foods that contain milk (e.g., yogurt and cheese), nuts, and shellfish.
Before you stop feeding your child any foods, talk about this with your child’s dermatologist. Children need certain foods to grow and develop normally.
Researchers continue to study what causes this complex disease. They believe that many things interact to cause atopic dermatitis. These things include our genes, where we live, and the way our immune system works.
Prevention of atopic dermatitis
The following tips may help prevent bouts of dermatitis (flares) and minimize the drying effects of bathing:
Moisturize your skin at least twice a day. Creams, ointments and lotions seal in moisture. Choose a product or products that work well for you. Using petroleum jelly on your baby’s skin may help prevent development of atopic dermatitis.
Try to identify and avoid triggers that worsen the condition. Things that can worsen the skin reaction include sweat, stress, obesity, soaps, detergents, dust and pollen. Reduce your exposure to your triggers.
Infants and children may experience flares from eating certain foods, including eggs, milk, soy and wheat. Talk with your child’s doctor about identifying potential food allergies.
Take shorter baths or showers. Limit your baths and showers to 10 to 15 minutes. And use warm, rather than hot, water.
Take a bleach bath. The American Academy of Dermatology recommends considering a bleach bath to help prevent flares. A diluted-bleach bath decreases bacteria on the skin and related infections. Add 1/2 cup (118 milliliters) of household bleach, not concentrated bleach, to a 40-gallon (151-liter) bathtub filled with warm water. Measures are for a U.S.-standard-sized tub filled to the overflow drainage holes.
Soak from the neck down or just the affected areas of skin for about 10 minutes. Do not submerge the head. Take a bleach bath no more than twice a week.
Use only gentle soaps. Choose mild soaps. Deodorant soaps and antibacterial soaps can remove more natural oils and dry your skin.
Dry yourself carefully. After bathing gently pat your skin dry with a soft towel and apply moisturizer while your skin is still damp.
Eczema (Atopic Dermatitis) Treatment
Atopic dermatitis can be persistent. You may need to try various treatments over months or years to control it. And even if treatment is successful, signs and symptoms may return (flare).
It’s important to recognize the condition early so that you can start treatment. If regular moisturizing and other self-care steps don’t help, your doctor may suggest one or more of the following treatments:
Skin Care at Home
You and your doctor should discuss the best treatment plan and medications for your atopic dermatitis. But taking care of your skin at home may reduce the need for prescription medications. Some recommendations include:
- Avoid scratching the rash or skin. Rather than scratching when you itch, try pressing on the skin. Cover the itchy area if you can’t keep from scratching it. For children, it might help to trim their nails and have them wear gloves at night.
- Apply bandages. Covering the affected area with bandages helps protect the skin and prevent scratching.
- Relieve the itch by using a moisturizer or topical steroids.
- Take an oral allergy or anti-itch medication to reduce severe itching. Options include nonprescription allergy medicines (antihistamines) — such as cetirizine (Zyrtec) or fexofenadine (Allegra). Also, diphenhydramine (Benadryl, others) may be helpful if itching is severe. But it causes drowsiness, so it’s better for bedtime.
- Keep your fingernails cut short. Consider light gloves if nighttime scratching is a problem.
- Lubricate or moisturize the skin two to three times a day using ointments such as petroleum jelly. Moisturizers should be free of alcohol, scents, dyes, fragrances, and other skin-irritating chemicals. You might try bath oils, creams, ointments or sprays. For a child, the twice-a-day regimen might be an ointment before bedtime and a cream before school. Ointments are greasier and sting less when applied.
- A humidifier in the home also can help. Hot, dry indoor air can parch sensitive skin and worsen itching and flaking. A portable home humidifier or one attached to your furnace adds moisture to the air inside your home.
- Avoid anything that worsens symptoms, including
- Irritants such as wool and lanolin (an oily substance derived from sheep wool used in some moisturizers and cosmetics)
- Strong soaps or detergents
- Sudden changes in body temperature and stress, which may cause sweating
- When washing or bathing
- Keep water contact as brief as possible and use gentle body washes and cleansers instead of regular soaps. Lukewarm baths are better than long, hot baths.
- Do not scrub or dry the skin too hard or for too long.
- After bathing, apply lubricating ointments to damp skin. This will help trap moisture in the skin.
- Apply an anti-itch cream to the affected area. A nonprescription hydrocortisone cream, containing at least 1 percent hydrocortisone, can temporarily relieve the itch. Apply it no more than twice a day to the affected area, after moisturizing. Using the moisturizer first helps the medicated cream penetrate the skin better. Once your reaction has improved, you may use this type of cream less often to prevent flare-ups.
- Take a warm bath. Sprinkle the bath water with baking soda, uncooked oatmeal or colloidal oatmeal — a finely ground oatmeal that is made for the bathtub (Aveeno, others). Soak for 10 to 15 minutes, then pat dry. Apply moisturizer while the skin is still damp.
- Choose mild soaps without dyes or perfumes. Use soap that’s superfatted and nonalkaline. Be sure to rinse off the soap completely.
- Wear cool, smooth-textured clothing. Reduce irritation by avoiding clothing that’s rough, tight or scratchy. Also, wear appropriate clothing in hot weather or during exercise to prevent excessive sweating.
- Treat stress and anxiety. Stress and other emotional disorders can worsen atopic dermatitis. Acknowledging those and trying to improve your emotional health can help.
Tips for choosing a moisturizer
- When selecting a moisturizer, consider choosing a thick cream or ointment.
- Some children do better with fragrance-free products, so consider petroleum jelly — an inexpensive, fragrance-free product that works well for many children.
- When selecting a product, “trial and error” sampling of different types may help to identify the best moisturizer for your child.
Bathing tips
- Bathe your child in warm — not hot — water.
- Limit your child’s time in the bath to 5 or 10 minutes.
- Use cleanser only when needed and make sure the cleanser is mild and fragrance-free. Do not use bubble bath.
- If your child’s eczema is frequently infected, twice-weekly bleach baths may be beneficial. Discuss this option with your child’s dermatologist.
- After bathing, gently pat your child’s skin partially dry.
- If your child has medicine that you apply to the skin, apply medicine when your child’s skin is almost dry and use the medicine as directed.
- Apply moisturizer on top of the medicine and to the rest of your child’s skin.
Bleach Bath therapy tips
If your child’s skin doctor recommends bleach baths, follow these important steps for giving a bleach bath:
- Use regular strength – 6 percent – bleach for the bath. Do not use concentrated bleach.
- Use a measuring cup or measuring spoon to add the bleach to the bath. Adding too much bleach to the bath can irritate your children’s skin. Adding too little bleach may not help.
- Measure the amount of bleach before adding it to the bath water. For a full bathtub of water, use a half cup of bleach. For a half-full tub of water, add a quarter cup of bleach. For a baby or toddler bathtub, add one teaspoon of bleach per gallon of water.
- Never apply bleach directly to your child’s eczema. While the tub is filling, pour the bleach into the water. Be sure to wait until the bath is fully drawn and bleach is poured before your child enters the tub.
- Talk with your skin doctor about how long your child should soak in the tub. Most dermatologists recommend a five- to 10-minute soak.
- Pat your child’s skin dry after the bath. If your child uses eczema medication, apply it immediately after the bath. Then moisturize your child’s skin.
Talk with a board-certified dermatologist before beginning bleach bath therapy with your child. If you have questions or concerns about caring for your child’s eczema, you should make an appointment to see a dermatologist.
Wet Wrap Therapy
Researchers are studying an innovative treatment for severe eczema called wet wrap therapy. It includes three lukewarm baths a day, each followed by an application of topical medicines and moisturizer that is sealed in by a wrap of wet gauze.
Infant eczema
Treatment for eczema in babies (infantile eczema) includes:
- Identifying and avoiding skin irritants
- Avoiding extreme temperatures
- Lubricating your baby’s skin with bath oils, creams or ointments
See your baby’s doctor if these measures don’t improve the rash or if the rash looks infected. Your baby may need a prescription medication to control the rash or to treat an infection. Your doctor may also recommend an oral antihistamine to help lessen the itch and to cause drowsiness, which may be helpful for nighttime itching and discomfort.
How do skin doctors treat atopic dermatitis ?
Treatment cannot cure atopic dermatitis, but it can control atopic dermatitis. Treatment is important because it can:
- Prevent the atopic dermatitis from getting worse.
- Calm the skin, relieving pain and itch.
- Reduce emotional stress.
- Prevent infections.
- Stop the skin from thickening. Thickened skin often itches all the time — even when the atopic dermatitis is not flaring.
A treatment plan often includes medicine, skin care, and lifestyle changes. Skin care and lifestyle changes can help prevent flare-ups. Many patients receive tips for coping. Doing all of this may seem bothersome, but sticking to the plan can make a big difference.
A dermatologist will create a treatment plan tailored to the patient’s needs. Medicine and other therapies will be prescribed as needed to:
- Control itching.
- Reduce skin inflammation (redness and swelling).
- Clear infection.
- Loosen and remove scaly lesions.
- Reduce new lesions from forming.
Medications
Creams that control itching and help repair the skin. Your doctor may prescribe a corticosteroid cream or ointment. Apply it as directed, after you moisturize. Overuse of this drug may cause side effects, including thinning skin.
Other creams containing drugs called calcineurin inhibitors — such as tacrolimus (Protopic) and pimecrolimus (Elidel) — affect your immune system. They are used by people older than age 2 to help control the skin reaction. Apply it as directed, after you moisturize. Avoid strong sunlight when using these products.
These drugs have a black box warning about a potential risk of cancer. But the American Academy of Allergy, Asthma & Immunology has concluded that the risk-to-benefit ratios of topical pimecrolimus and tacrolimus are similar to those of most other conventional treatments of persistent eczema and that the data don’t support the use of the black box warning.
Drugs to fight infection. Your doctor may prescribe an antibiotic cream if your skin has a bacterial infection, an open sore or cracks. He or she may recommend taking oral antibiotics for a short time to treat an infection.
Oral drugs that control inflammation. For more-severe cases, your doctor may prescribe oral corticosteroids — such as prednisone. These drugs are effective but can’t be used long term because of potential serious side effects.
Newer option for severe eczema. The Food and Drug Administration (FDA) has recently approved a new, injectable biologic (monoclonal antibody) called dupilumab (Dupixent). It is used to treat people with severe disease who do not respond well to other treatment options. This is a newer medication, so it doesn’t have a long track record in terms of how well it helps people. Studies have shown it to be safe if used as directed. It is very expensive.
Light therapy. This treatment is used for people who either don’t get better with topical treatments or who rapidly flare again after treatment. The simplest form of light therapy (phototherapy) involves exposing the skin to controlled amounts of natural sunlight. Other forms use artificial ultraviolet A (UVA) and narrow band ultraviolet B (UVB) either alone or with medications.
Though effective, long-term light therapy has harmful effects, including premature skin aging and an increased risk of skin cancer. For these reasons, phototherapy is less commonly used in young children and not given to infants. Talk with your doctor about the pros and cons of light therapy.
Counseling. Talking with a therapist or other counselor may help people who are embarrassed or frustrated by their skin condition.
Relaxation, behavior modification and biofeedback. These approaches may help people who scratch habitually.
Outcome
Studies have found that when atopic dermatitis develops in an infant or young child, the child tends to get better with time. For some children, the condition completely disappears by age 2.
About half (50%) of the children who get atopic dermatitis will have it as an adult. The good news is that the atopic dermatitis often becomes milder with age.
There is no way to know whether the atopic dermatitis will go away or be a lifelong disease. This makes treatment very important. Treatment can stop the atopic dermatitis from getting worse. Treatment also helps to relieve the discomfort.
What is Contact Dermatitis
Almost everyone gets this type of eczema at least once. You get contact dermatitis when something that your skin touches causes a rash. The contact dermatitis red, itchy rash is caused by direct contact with a substance or an allergic reaction to it. The rash isn’t contagious or life-threatening, but it can be very uncomfortable. Some rashes happen immediately. Most take time to appear.
To treat contact dermatitis successfully, you need to identify and avoid the cause of your reaction. If you can avoid the offending substance, the rash usually clears up in two to four weeks. You can try soothing your skin with cool, wet compresses, anti-itch creams and other self-care steps.
Causes of contact dermatitis
Contact dermatitis is caused by a substance you’re exposed to that irritates your skin or triggers an allergic reaction. The substance could be one of thousands of known allergens and irritants. Some of these substances may cause both irritant contact dermatitis and allergic contact dermatitis.
Allergic contact dermatitis
Allergic contact dermatitis occurs when a substance to which you’re sensitive (allergen) triggers an immune reaction in your skin. It usually affects only the area that came into contact with the allergen. But it may be triggered by something that enters your body through foods, flavorings, medicine, or medical or dental procedures (systemic contact dermatitis). Some people have an allergic skin reaction.
More than 3,600 substances can cause allergic contact dermatitis. These substances include preservatives in cosmetics, antibiotics applied to the skin, animal dander, dyes in clothing and shoes, and rubber.
With thousands of causes, successfully treating this skin condition can take a bit of detective work. Dermatologists frequently treat this condition. In fact, this is one of the most common reasons to see a dermatologist.
You have had this type of contact dermatitis if you had a rash caused by:
- Plants such as poison ivy and mango, which contain a highly allergenic substance called urushiol
- Nickel
- Makeup you applied once or few times
- Jewelry you wore for a long time without a reaction, such as a wedding ring
- Jewelry you wore for only a few hours or days
- Latex gloves
- Medications, such as antibiotic creams and oral antihistamines
- Balsam of Peru, which is used in many products, such as perfumes, cosmetics, mouth rinses and flavorings
- Formaldehyde, which is in preservatives, disinfectants and clothing
- Personal care products, such as deodorants, body washes, hair dyes, cosmetics and nail polish
- Airborne substances, such as ragweed pollen and spray insecticides
- Products that cause a reaction when you’re in the sun (photoallergic contact dermatitis), such as some sunscreens and oral medications
You may become sensitized to a strong allergen such as poison ivy after a single exposure. Weaker allergens may require multiple exposures over several years to trigger an allergy. Once you develop an allergy to a substance, even a small amount of it can cause a reaction.
Irritant contact dermatitis
This is the most common type. This nonallergic skin reaction occurs when a substance damages your skin’s outer protective layer. It develops when something irritates the skin. With enough contact, most things will irritate your skin.
Almost any chemical, including water, can damage the skin with enough contact. Toxic substances like fiberglass and turpentine quickly damage the skin. Many people develop irritant contact dermatitis when they work with hair dyes, solvents, oils, paints, varnishes, foods, or metalworking fluids.
A person diagnosed with any of the following has irritant contact dermatitis:
- Diaper rash
- Acid burn
- Dry, cracked hands due to lots of contact with water
- Irritated skin around the mouth due to lip licking
When a toxic substance touches your skin, the skin is quickly irritated. You’ve had irritant contact dermatitis if your skin reacted to a toxic substance like:
- Battery acid
- Bleach
- Pepper spray
You can also develop irritant contact dermatitis when you have lots of contact with less irritating substances like:
- Water
- Foods
- Soap
People often develop irritant contact dermatitis at work. Beauticians, nurses, bartenders, and others who spend lots of time with wet hands get this. It often starts with dry, cracked hands. In time, the skin on their hands may begin to sting and burn. The skin becomes very tender. Sometimes, the skin itches and bleeds.
When a rash does not clear within a few weeks, you should see a dermatologist.When contact dermatitis develops, treatment is important. It can prevent the contact dermatitis from worsening and help your skin heal.
When to seek immediate medical care for contact dermatitis
A few people develop a severe allergic reaction known as anaphylaxis. Symptoms occur within seconds or minutes. A person may have:
- Difficulty breathing due to swelling in the throat
- Swollen face and/or eyes
- Confusion
In short, the entire body reacts. If you have any of these symptoms, you need immediate medical care.
Seek immediate medical care in the following situations:
- You think your skin is infected. Clues include fever and pus oozing from blisters.
- Your lungs, eyes or nasal passages are painful and inflamed, perhaps from inhaling an allergen.
- You think the rash has damaged the mucous lining of your mouth and digestive tract.
See your doctor if:
- The rash is so uncomfortable that you are losing sleep or are distracted from your daily activities
- The rash is sudden, painful, severe or widespread
- You’re embarrassed by the way your skin looks
- The rash doesn’t get better within three weeks
- The rash affects your face or genitals
Risk factors for contact dermatitis
Some jobs and hobbies put you at higher risk of contact dermatitis. Examples include:
- Nurses (and other health care workers) and dental employees
- Metalworkers
- Construction workers
- Hairdressers and beauticians cosmetologists
- Auto mechanics
- Scuba divers or swimmers, due to the rubber in face masks or goggles
- Cleaners
- Janitors
- Plumbers
- Gardeners and agricultural workers
- Bartenders
- Cooks and others who work with food
- Florists (and others who work with plants).
Nurses and beauticians often develop dry, cracked skin on their palms and fingers. Wearing latex gloves frequently throughout the day causes some people to develop an allergy to latex. A common sign of this allergy is itchy, inflamed hands.
You also have a greater risk of developing contact dermatitis if you have (or had) one of these medical conditions:
- Asthma
- Hay fever
- Atopic dermatitis (often called eczema)
Your environment also plays a role. Extreme heat or cold, high humidity, and very dry air make the skin more vulnerable.
Signs and symptoms of Contact dermatitis
Allergic contact dermatitis
This skin condition occurs when you have an allergic reaction to something that comes in contact with your skin.
Signs and symptoms rarely appear on contact. It may take a few hours for your skin to react. If this is your first time that your skin has an allergic reaction to that substance, weeks may pass before you notice anything.
When signs and symptoms appear, you may have:
- Itchy skin (often intense)
- Rash (skin red, swollen, and hot)
- Excessively dry skin
- Burning
- Stinging
- Hives (round welts on the skin that itch intensely)
- Fluid-filled blisters
- Oozing blisters that leave crusts and scales
If exposure to the allergen continues, your skin may:
- Flake and crack
- Become scaly
- Darken, thicken, and feel leathery
Figure 2. Allergic contact dermatitis

Irritant contact dermatitis
Many substances can irritate our skin. Soap, shampoo, food, and water are mild irritants. With lots of exposure, these can cause irritant contact dermatitis. Getting a strong irritant like battery acid or fiberglass on your skin just once also can cause irritant contact dermatitis.
The signs and symptoms differ for mild and strong irritants.
Mild irritant: The signs and symptoms develop over time. You’ll gradually notice:
- Dry, chapped skin.
- With repeat exposure, patches of itchy, red, swollen, and scaly skin develop. By this time, each time something that can irritate the skin touches the affected skin, you may feel stinging and burning right away.
- If exposure continues, the skin may crack, get scaly, and become excessive dry.
- Sores and blisters may develop and erupt, causing crusts and scales.
Strong irritant: On contact or within a few hours, the skin can:
- Burn, sting, and/or itch
- Become inflamed (red and swollen)
- Develop fluid-filled blisters
When you have irritant contact dermatitis, many things can irritate your skin. You may feel pain on contact. With repeat exposure, the condition worsens.
Reduced quality of life
This skin condition often affects a person’s quality of life. The rash can make many daily activities painful, especially when the rash forms on the hands. The rash can cause:
- Missed work days
- Inability to enjoy leisure activities
- Loss of sleep
Figure 3. Irritant contact dermatitis

Complications of contact dermatitis
Contact dermatitis can lead to an infection if you repeatedly scratch the affected area, causing it to become wet and oozing. This creates a good place for bacteria or fungi to grow and may cause an infection.
Prevention of contact dermatitis
General prevention steps include the following:
- Avoid irritants and allergens. Try to identify and avoid substances that irritate your skin or cause an allergic reaction.
- Wash your skin. You might be able to remove most of the rash-causing substance if you wash your skin right away after coming into contact with it. Use a mild, fragrance-free soap and warm water. Rinse completely. Also wash any clothing or other items that may have come into contact with a plant allergen, such as poison ivy.
- Wear protective clothing or gloves. Face masks, goggles, gloves and other protective items can shield you from irritating substances, including household cleansers.
- Apply an iron-on patch to cover metal fasteners next to your skin. This can help you avoid a reaction to jean snaps, for example.
- Apply a barrier cream or gel. These products can provide a protective layer for your skin. For example, an over-the-counter skin cream containing bentoquatam (IvyBlock) may prevent or lessen your skin’s reaction to poison ivy.
- Use moisturizer. Regularly applying moisturizing lotions can help restore your skin’s outermost layer and keep your skin supple.
- Take care around pets. Allergens from plants, such as poison ivy, can cling to pets and then be spread to people.
Diagnosis of Contact dermatitis
Patch testing
Your doctor may be able to diagnose contact dermatitis and identify its cause by talking to you about your signs and symptoms, questioning you to uncover clues about the trigger substance, and examining your skin to note the pattern and intensity of your rash.
Your doctor may recommend a patch test to see if you’re allergic to something. This test can be useful if the cause of your rash isn’t apparent or if your rash recurs often.
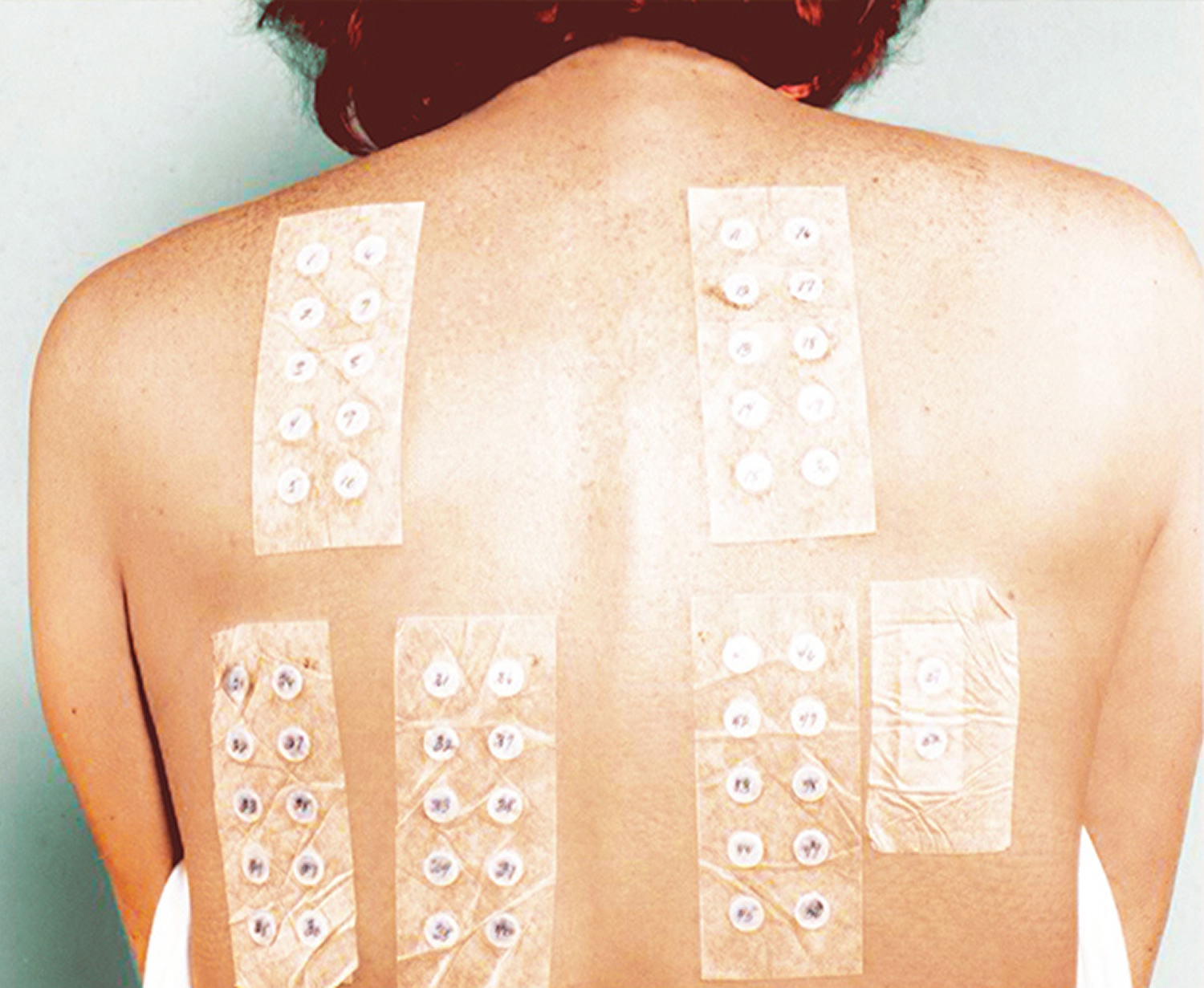
During a patch test, small amounts of potential allergens are applied to adhesive patches, which are then placed on your skin. The patches remain on your skin for two to three days, during which time you’ll need to keep your back dry.
Skin patch testing can be helpful in determining if you’re allergic to a specific substance. Small amounts of different substances are placed on your skin under an adhesive coating. Your doctor then checks for a skin reaction under the patches and determines whether further testing is needed.
What happens during patch testing ?
If patch testing is recommended, the following will happen:
- Patches containing small amounts of substances to which you may be allergic will be applied to your skin, usually on your back.
- You keep the substances on your skin for a specific amount of time, usually 2 days.
- You return to your doctor’s office so that the doctor can check your skin for reactions.
- You may need to keep some patches on your skin for a longer time and see your doctor again in a few days.
To find out if the allergen is causing your rash, you will need to avoid that substance. For example, if the test shows that you have a nickel allergy, you may need to:
- Stop wearing jewelry and clothing (zippers, fasteners) that contains nickel.
- Cover your cell phone with a case to avoid touching the metal.
- Get a pair of eyeglasses made without nickel.
If your skin clears when you avoid the allergen, it is likely the cause of your rash.
Figure 4. Contact dermatitis – skin patch testing
Contact dermatitis treatment
Treatment is the same for both types of contact dermatitis.
Your doctor may prescribe medications. Examples include:
- Steroid creams or ointments. These topically applied creams or ointments help soothe the rash of contact dermatitis. A topical steroid may be applied one or two times a day for two to four weeks.
- Oral medications. In severe cases, your doctor may prescribe oral corticosteroids to reduce inflammation, antihistamines to relieve itching or antibiotics to fight a bacterial infection.
Avoid what is causing your rash. If avoiding the cause will be difficult, ask your dermatologist for help.
For example, if you are allergic to latex but must wear exam gloves, your dermatologist can recommend another type of glove that you can wear. If you must work outdoors where poison ivy grows, your dermatologist can recommend a protective barrier cream and clothing that can help.
Treat the rash. Once you can avoid the cause, your rash should clear. To relieve your symptoms, a dermatologist may recommend the following:
Mild reaction: Antihistamine pills, moisturizer, and a corticosteroid that you can apply to your skin. Most patients apply the medicine twice a day for 1 week and once a day for 1 to 2 weeks.
Oatmeal baths can relieve discomfort.
Severe reaction: If you have a lot of swelling, your face swells, or the rash covers much of your body, you may need a strong medication. Your dermatologist may prescribe prednisone. It is important to take this medication exactly as directed to avoid another flare.
Wet dressings can help soothe skin that has lots of oozing and crusting. If your dermatologist recommends wet dressings, you’ll receive instructions to help you make these at home.
If you have an infection, your dermatologist may prescribe an antibiotic.
Some patients need light therapy to calm their immune system. Your dermatologist may refer to this as phototherapy.
If you avoid what caused the rash, your skin will clear. Most people see clear skin within 1 to 3 weeks.
Clearing may take longer if poison ivy, poison oak, or poison sumac caused your rash. The first time you have an allergic reaction to one of these plants, the rash may linger for 6 weeks. If you get another rash, your skin should clear within 10 to 21 days.
Once your skin clears, you must continue to avoid what caused your rash.
If your rash does not clear, you should tell your dermatologist. You may need extra help.
Systemic contact dermatitis
Some people develop a rash even when they avoid touching the allergen. A rash can appear when the substance to which you have an allergy gets inside your body. The medical term for this condition is systemic contact dermatitis.
The allergen can get inside your body in different ways. You could:
- Eat food that contains the allergen
- Inhale or inject a medicine that contains the allergen
- Use birth control (IUD or spermicide) that contains the allergen
While rare, some people develop a rash because the fillings in their mouth contain mercury. They could only get rid of the rash when a dentist replaced their fillings with fillings that did not contain mercury.
Trying to find everything that contains the allergen can be a challenge. Your dermatologist may be able to help you create a list of things you need to avoid. The list often varies from region to region.
Lifestyle and home remedies for contact dermatitis
To help reduce itching and soothe inflamed skin, try these self-care approaches:
- Avoid the irritant or allergen. The key to this is identifying what’s causing your rash and staying away from it. Your doctor may give you a list of products that typically contain the substance that affects you. Also ask for a list of products that are free of the substance that affects you.
If you’re allergic to the metal in a piece of jewelry, you may be able to wear it by putting a barrier between you and the metal. For example, line the inside of a bracelet with a piece of clear tape or paint it with clear nail polish.
- Apply an anti-itch cream or lotion to the affected area. A nonprescription cream containing at least 1 percent hydrocortisone can temporarily relieve your itch. A steroid ointment may be applied one or two times a day for two to four weeks. Or try calamine lotion.
- Take an oral anti-itch drug. A nonprescription oral corticosteroid or antihistamine, such as diphenhydramine (Benadryl), may be helpful if your itching is severe.
- Apply cool, wet compresses. Moisten soft washcloths and hold them against the rash to soothe your skin for 15 to 30 minutes. Repeat several times a day.
- Avoid scratching. Trim your nails. If you can’t keep from scratching an itchy area, cover it with a dressing.
- Soak in a comfortably cool bath. Sprinkle the water with baking soda or an oatmeal-based bath product.
- Protect your hands. Rinse and dry hands well and gently after washing. Use moisturizers throughout the day. And choose gloves based on what you’re protecting your hands from. For example, plastic gloves lined with cotton are good if your hands are often wet.
Outcome for patients with contact dermatitis
By avoiding what caused the rash, most people can avoid flare-ups.
If you work with substances that caused the rash, you can still avoid a rash. Your dermatologist can recommend ways to work and products to use. More than 80% of people diagnosed with occupational dermatitis successfully manage the condition and recover without any problems.
What is nummular dermatitis
People who get this skin nummular dermatitis often see distinct, coin-shaped (nummular) or oval sores on their skin 4. Nummular dermatitis often appears after a skin injury, such as a burn, abrasion (from friction), or insect bite. A person may see 1 or many patches. These patches can last for weeks or months.
Your dermatologist may refer to this skin condition as:
- Nummular dermatitis.
- Nummular eczema.
- Discoid eczema.
Men get nummular dermatitis more often than women get it. Men often have their first outbreak between 55 and 65 years of age. When women get it, they are usually younger. They tend to be teenagers or young adults.
Figure 5. Nummular dermatitis

Signs and symptoms of nummular dermatitis
Patches on the skin tend to begin as a group of tiny, reddish spots and blister-like sores that weep fluid. Then the sores enlarge and grow together to form a coin-shaped patch.
The patches tend to have these signs and symptoms:
- Range in size from smaller than 1 inch to bigger than 4 inches.
- Occur most often on the legs but also occur on the torso (middle of the body), arms, hands, and feet.
- Be pink, red, or brown and well-defined.
- Itch and burn: These symptoms range from very mild to severe. The itch may be worse at night, disturbing sleep.
- Become crusty after the blisters leak fluid and, after a long time, become scaly.
A yellowish crust may develop on the patches if a Staphylococcus aureus (staph) infection occurs. This may require treatment with an antibiotic.
The skin between the patches often remains clear, but it can be dry and easily irritated.
Who gets nummular dermatitis ?
This skin problem is more common in men than in women. Men tend to have their first outbreak between 55 and 65 years of age. Women are more likely to get it between the ages of 15 and 25 years. It is rare in children.
What causes nummular dermatitis ?
While the cause is unknown, researchers think that sensitivity plays a role in some cases. A person may be sensitive to:
- Metals, including nickel and rarely mercury, such as from dental fillings.
- Formaldehyde.
- Medicines, such as neomycin (an antibiotic that you apply to the skin).
If the person has a sensitivity to something, the skin will only clear when the person avoids that substance.
Research also suggests that your risk of getting nummular dermatitis increases if you live in a cold, dry climate or have:
- Very dry skin (xerosis).
- Another type of eczema, mainly atopic dermatitis or stasis dermatitis.
- Poor blood flow and/or swelling in the legs.
- Injured your skin (insect bite, contact with chemicals, or abrasion).
- A skin infection caused by bacteria.
- Taken certain medicines, such as isotretinoin and interferon. Isotretinoin, a prescription medicine sometimes used to treat severe acne, seems to increase the risk for this skin problem. Interferon can cause severe widespread nummular dermatitis.
How is nummular dermatitis diagnosed ?
Dermatologists often diagnose nummular dermatitis by looking at the patient’s skin. During the exam, the dermatologist may swab the sores if the doctor thinks you have a skin infection.
If your dermatologist thinks you have an allergy, patch testing (skin tests to find allergies) may be recommended. Your dermatologist also may recommend patch testing if treatment does not fully clear your skin. An allergy can prevent the skin from clearing.
Nummular dermatitis prevention
To prevent nummular dermatitis from returning once your skin clears, dermatologists recommend the following:
- Moisturize. Apply a moisturizer at least once a day. The best time is just after bathing while your skin is damp. A moisturizer helps trap water in the skin. A dermatologist can recommend products that will not irritate your skin.
- Avoid activities that bother your skin. Anything that dries, heats, or irritates your skin can cause a flare-up. To avoid flare-ups, dermatologists recommend using lukewarm water for showers and baths, getting out of the shower or bath after 20 minutes, and not sitting next to a fire or heater.
- Skip the soap. Using a mild, gentle cleanser to clean your skin instead of soap will help. Soap can dry the skin.
- Use a humidifier. When you heat or air-condition your home, use a humidifier to add moisture to the air.
- Dress for success. You are less likely to irriate your skin if you wear loose clothing. You also should not wear rough fabrics, such as wool, which can bother your skin.
How is nummular dermatitis treated ?
These sores can be stubborn, so seeing a dermatologist for treatment is recommended. Treatment for nummular dermatitis consists of the following:
- Protect your skin from getting scraped, cut, or injured in any other way. A skin injury can worsen nummular dermatitis.
- Hydrate your skin. You can do this by taking a 20-minute lukewarm bath or shower once a day. Within 3 minutes of getting out of the water, apply a moisturizer to your still-damp skin. This helps hydrate dry skin. It also relieves the itch and scaling. Adding bath oil to the water also may help. Beware that some oils can irritate your skin. A dermatologist can recommend bath oil that will not irritate your skin.
- Use medicine as directed by your dermatologist. Medicine prescribed to treat the skin includes corticosteroid ointments and tar creams. These help reduce inflammation (redness and swelling) and itch. If a bacterial skin infection occurs, your dermatologist will prescribe an antibiotic. An oral (by mouth) antihistamine that makes you drowsy can help you sleep.
If you have a bad case or widespread nummular dermatitis, you may need:
- Medicated dressings (bandages).
- Phototherapy (treatment with light).
- Oral antibiotics.
- Systemic (taken by mouth or injected) corticosteroids.
- Bed rest in a cool and moist room. You can keep the room moist with a humidifier.
Outcome of nummular dermatitis
With proper treatment, nummular dermatitis can clear completely. Sores on the thighs, legs, and feet often take longer to heal and tend to leave behind darker or lighter spots.
Some patients’ skin clears within a year. Others have these patches for many years. Sometimes the patches go away and then return. Patches that return after clearing tend to appear in the same place as the first outbreak.
What is stasis dermatitis
Stasis dermatitis is also called gravitational dermatitis, venous eczema, and venous stasis dermatitis 5.
This condition develops in people who have poor circulation. Because poor blood flow usually occurs in the lower legs, this is where stasis dermatitis often develops. It may occur in one or both legs. Stasis dermatitis can develop in other areas, but this is rare.
Stasis dermatitis is most common in the lower legs because leg veins have one-way valves, which play an important role in circulating our blood. These valves push blood up the legs. As we age, these valves can weaken and stop working properly. Some blood can leak out and pool in the legs. Your dermatologist may refer to this as “venous insufficiency.”
If you’ve been diagnosed with venous insufficiency, it does not mean that you will get stasis dermatitis. Watching for signs and symptoms of stasis dermatitis is important though. Treatment and self-care can prevent the stasis dermatitis from becoming severe.
Swelling around the ankle is often the first sign of stasis dermatitis. The swelling tends to clear while you sleep — and return during the day. Other early signs are discolored skin and varicose veins.
Figure 6. Stasis dermatitis

Signs and symptoms of stasis dermatitis
Early signs and symptoms
Most people develop stasis dermatitis on their lower legs. When it begins in the legs, you may notice the following in one or both legs:
- Heaviness or aching when you stand or walk for a long time
- Swelling, often on the inside of the ankle, at the end of the day
- Swelling clears when you sleep, but re-appears during the day
- Varicose veins
- Itchy, dry skin over the varicose veins
Skin may feel irritated — red, swollen, and sore
Signs and symptoms as disease progresses
As the stasis dermatitis progresses, people often notice the following:
- Swelling spreads beyond the ankle to the calf
- Dry, cracked, itchy skin
- Red to violet-colored open sores (medical term: venous ulcer), which can appear on the lower legs and tops of the feet
- Sores leak fluid and scab as they heal
- Sores can cause scars when they heal
- Shiny skin
Severe stasis dermatitis
Left untreated, stasis dermatitis can worsen over the years and cause the following:
- Area feels hard
- Lower part of the calf shrinks, often making the calf look like an upside-down wine bottle
- Skin becomes deeply pigmented
- Redness and scale cover the area, including the top of the foot
- Intensely itchy skin
Other medical conditions can develop where a person has stasis dermatitis. Two common conditions are:
- Contact dermatitis (skin becomes very sensitive to almost everything that touches it, including medicines and ingredients in moisturizers, such as lanolin)
- Cellulitis (a serious infection that extends deep into the skin)
Who gets stasis dermatitis ?
Stasis dermatitis is most likely to develop in someone who has the following traits:
Age: Because poor circulation leads to stasis dermatitis, this type of dermatitis usually develops in people who are middle aged or older. In the United States, stasis dermatitis:
- Tends to develop in people 50 years of age and older
- Rarely occurs before 40 years of age
Gender: Women are slightly more likely to develop stasis dermatitis.
Medical history: Having one or more of the following increases your risk of developing stasis dermatitis:
- Venous insufficiency (your body has trouble returning blood from your legs to your heart, so some blood pools in your legs)
- Varicose veins (or blood relatives who have them)
- High blood pressure
- Previous blood clot, especially a blood clot in a leg like deep vein thrombosis
- Previous injury to the area
- Many pregnancies
- Surgery (to the area or removing a vein from the area)
- A heart condition, such as congestive heart failure (a weakened heart cannot pump blood effectively)
- Kidney failure
- Being very overweight
Lifestyle: Having any of the following also increase your risk of developing stasis dermatitis:
- Standing or sitting for long periods of time, such as at work
- Getting little or no exercise
- Excess body fat
You can reduce your risk
If you get little or no exercise, becoming more active may reduce your risk of developing stasis dermatitis. Exercise can improve your blood flow, help you shed excess body fat, and possibly reduce high blood pressure.
Before beginning any exercise, you should talk with your doctor to make sure it’s safe for you.
What causes stasis dermatitis ?
Poor circulation leads to stasis dermatitis. Because poor circulation most commonly develops in the lower legs and feet, this is the most common area of the body for stasis dermatitis to develop.
If you have stasis dermatitis, an accurate diagnosis and treatment are essential. Treatment can prevent the disease from worsening.
How is stasis dermatitis diagnosed ?
To diagnose this condition, your dermatologist will examine your skin, looking closely at the skin that shows signs of stasis dermatitis. Your dermatologist will also want to know about your medical history.
It is important to mention the following:
- Past blood clot
- Injury to the area
- Heart disease
- Surgeries
Medical tests may be necessary to find out exactly why you have poor circulation in the area. Your dermatologist may refer you to another doctor or recommend one or more of following tests:
- Blood tests
- Doppler ultrasound (to look at how your blood flows)
- Tests to rule out problems with your heart
- Allergy testing (stasis dermatitis increases the risk of developing an allergic reaction on your skin)
If you have stasis dermatitis, your dermatologist will create a treatment plan that addresses your specific needs.
How is stasis dermatitis treated ?
When treating stasis dermatitis, the goal is to get it under control. Your treatment plan will include treatment for each of your signs and symptoms, which may include:
Swelling: To reduce the swelling in a lower leg, most patients wear a compression stocking, compression dressing, or Unna boot. Compression can reduce swelling as well as improve your circulation.
Because it is so important to reduce swelling, it helps to elevate your legs throughout the day. If possible, dermatologists recommend that you elevate your legs above your heart:
- Once every 2 hours for 15 minutes
- While you sleep (keep your legs elevated with pillows)
Inflammation (redness, swelling, and pain): To treat this, most patients apply medicine to the stasis dermatitis. Your dermatologist may prescribe a medicine called a corticosteroid or a topical calcineurin inhibitor.
Infection: If you have an infection, taking an antibiotic or applying an antibiotic to the stasis dermatitis can help clear the infection.
Wounds: You may need to apply a special dressing to the wound to help it heal.
Itch: Taking an antihistamine can help calm an intense itch.
Dry skin: Applying a moisturizer a few times per day can help get rid of the dry skin.
Because stasis dermatitis makes the skin so sensitive, you’ll want to use a moisturizer that is free of:
- Fragrance
- Dyes
- Perfumes
Good options include petroleum jelly and a thick cream that says “fragrance free” on the label. Your dermatologist may also recommend a moisturizer.
Varicose veins: Sometimes varicose veins — those large blue or purple veins that rise above the skin’s surface — can cause discomfort and pain. In rare cases, they can cause bleeding leg sores.
Removing troublesome vein can alleviate your discomfort and may reduce bleeding leg sores. If vein removal is recommended, your dermatologist can recommend an appropriate procedure for you. Many procedures are minimally invasive.
About the skin discoloration: Stasis dermatitis can cause the affected skin to turn a brownish color. This discoloration often remains even when the swelling, sores, and other signs clear. If the discoloration bothers you, ask your dermatologist about treatment options that could reduce the discoloration.
What is the outcome for a person who has stasis dermatitis ?
You may have stasis dermatitis for life. Many patients are able to manage the disease on their own once they get the stasis dermatitis under control. Managing the disease often involves 6:
- Wearing compression stockings
- Elevating your legs as needed
- Following a skin care plan
- Applying medicine when you have a flare
You’ll also need to see your dermatologist for follow-up appointments.
Self-care plays an important role in getting stasis dermatitis under control. It is essential to keep it under control.
Home remedy for stasis dermatitis
If you have stasis dermatitis, self-care is essential for getting stasis dermatitis under control and preventing it from worsening. Dermatologists often recommend the following tips to their patients who have stasis dermatitis 7:
Elevate your legs above the heart: You’ll want to do this throughout the day. If possible, dermatologists recommend that you elevate your legs above your heart:
- Once every 2 hours for 15 minutes
- While you sleep (keep your legs elevated with pillows)
Take breaks when you must sit or stand for long periods. If you must sit or stand for long periods, take a break every hour and walk briskly for 10 minutes.
Get physical. Exercise can improve your circulation and strengthen your calf muscles. Ask your dermatologist how often you should exercise.
Wear loose-fitting cotton clothing. Wearing cotton clothes help to avoid irritation. Rough fabrics like wool, polyester, and rayon can irritate your skin.
Loose-fitting clothing is important, too. Tight waistbands and snug pants interfere with your circulation. When clothing rubs against the stasis dermatitis, it can irritate the sensitive skin.
Wear your compression garment if your dermatologist recommends one. Compression can:
- Improve the circulation in your legs
- Prevent open sores
- Reduce your risk of another flare.
Most patients stop wearing a compression garment (compression stockings or Unna boots) because it feels uncomfortable. The discomfort tends to lessen as the swelling subsides.
Avoid anything that could aggravate the stasis dermatitis. The skin with stasis dermatitis is very sensitive, so you want to prevent the stasis dermatitis from touching anything that could irritate it, such as:
- Pet hair
- Plants
- Grass
- Cleaning products
- Perfume
- Any skin care product that does not say “fragrance free.”
Apply moisturizer when your skin feels dry. Moisturizer helps prevent scaly skin and irritation. Petroleum jelly works well for most patients. If you prefer to use another moisturizer, choose an ointment or thick cream that says “fragrance free” on the container.
Avoid scratching the stasis dermatitis. Scratching can worsen stasis dermatitis and lead to an infection. To reduce the itch, apply your medicine as directed. Other ways to calm the itch include:
- Applying a cool compress
- Spreading on a fragrance-free moisturizer
- Adding colloidal oatmeal to a cool bath
Take care when bathing. Soaps and rough-textured towels can irritate the stasis dermatitis. Dermatologists recommend the following to their patients with stasis dermatitis:
- Use a mild, fragrance-free cleanser rather than soap. When you shower or take a bath, use this cleanser. Rinsing soap from other parts of your body can irritate the stasis dermatitis.
- After bathing, gently pat the water from your skin with a clean towel. You’ll want to keep a bit of water on the skin with stasis dermatitis.
- Within 2 minutes of bathing, apply petroleum jelly or a thick, creamy moisturizer that is fragrance free. This helps to keep moisture in your skin. Keeping your skin moisturized helps to prevent scaly skin and irritation.
What is seborrheic dermatitis
Seborrheic dermatitis is a common skin condition that mainly affects your scalp 8. It causes scaly patches, red skin and stubborn dandruff. Seborrheic dermatitis can also affect oily areas of the body, such as the face, sides of the nose, eyebrows, ears, eyelids and chest.
Seborrheic dermatitis may go away without treatment. Or you may need many repeated treatments before the symptoms go away. And they may return later. Daily cleansing with a gentle soap and shampoo can help reduce oiliness and dead skin buildup.
Seborrheic dermatitis is also called dandruff, seborrheic eczema and seborrheic psoriasis. For infants, the condition is known as cradle cap and causes crusty, scaly patches on the scalp.
Figure 7. Seborrheic dermatitis (scalp)

Symptoms and signs of Seborrheic dermatitis
Seborrheic dermatitis signs and symptoms may include:
- Skin flakes (dandruff) on your scalp, hair, eyebrows, beard or mustache
- Patches of greasy skin covered with flaky white or yellow scales or crust on the scalp, face, sides of the nose, eyebrows, ears, eyelids, chest, armpits, groin area or under the breasts
- Red skin
- Itching
The signs and symptoms may be more severe if you’re stressed, and they tend to flare in cold, dry seasons.
When to see a doctor
See your doctor if:
- You’re so uncomfortable that you’re losing sleep or being distracted from your daily routines
- Your condition is causing embarrassment and anxiety
- You suspect your skin is infected
- You’ve tried self-care steps without success
Causes of Seborrheic dermatitis
Doctors don’t yet know the exact cause of seborrheic dermatitis. It may be related to:
A yeast (fungus) called malassezia that is in the oil secretion on the skin
An irregular response of the immune system
Risk factors for Seborrheic dermatitis
A number of factors increase your risk of developing seborrheic dermatitis, including:
- Neurologic and psychiatric conditions, such as Parkinson’s disease and depression
- A weakened immune system, such as seen in organ transplant recipients and people with HIV/AIDS, alcoholic pancreatitis and some cancers
- Recovery from stressful medical conditions, such as a heart attack
- Some medications
Diagnosis of seborrheic dermatitis
Your doctor will likely be able to determine whether you have seborrheic dermatitis by examining your skin. He or she may scrape off skin cells for examination (biopsy) to rule out conditions with symptoms similar to seborrheic dermatitis, including:
- Psoriasis. This disorder also causes dandruff and red skin covered with flakes and scales. With psoriasis, usually you’ll have more scales, and they’ll be silvery white.
- Atopic dermatitis (eczema). This skin reaction causes itchy, inflamed skin in the folds of the elbows, on the backs of the knees or on the front of the neck. It often recurs.
- Tinea versicolor. This rash appears on the trunk but usually isn’t red like seborrheic dermatitis patches.
- Rosacea. This condition usually occurs on the face and has very little scaliness.
Seborrheic dermatitis treatment
Medicated shampoos, creams and lotions are the main treatments for seborrheic dermatitis. Your doctor will likely recommend you try home remedies, such as over-the-counter dandruff shampoos, before considering prescription remedies. If home remedies don’t help, talk with your doctor about trying these treatments.
Creams, shampoos or ointments that control inflammation. Prescription-strength hydrocortisone, fluocinolone (Capex, Synalar), clobetasol (Clobex, Cormax) and desonide (Desowen, Desonate) are corticosteroids you apply to the scalp or other affected area. They are effective and easy to use, but should be used sparingly. If used for many weeks or months without a break, they can cause side effects, such as thinning skin or skin showing streaks or lines.
Creams or lotions containing the calcineurin inhibitors tacrolimus (Protopic) and pimecrolimus (Elidel) may be effective and have fewer side effects than corticosteroids do. But they are not first-choice treatments because the Food and Drug Administration has concerns about a possible association with cancer. In addition, tacrolimus and pimecrolimus cost more than mild corticosteroid medications.
Antifungal gels, creams or shampoos alternated with another medication. Depending on the affected area and the severity of your symptoms, your doctor might prescribe a product with 2 percent ketoconazole (Nizoral) or 1 percent ciclopirox. Or you doctor may prescribe both products to be used alternately.
Antifungal medication you take as a pill. If your condition isn’t improving with other treatments, your doctor may recommend an antifungal medication in pill form. These aren’t a first choice for treatment because of possible side effects and drug interactions.
Home remedies for seborrheic dermatitis
You may be able to control seborrheic dermatitis with lifestyle changes and home remedies. Many of these are available in over-the-counter (nonprescription) forms. You may need to try different products or a combination of products before your condition improves.
The best approach for you depends on your skin type, the severity of your condition, and whether your symptoms affect your scalp or other areas of your body. But even if your condition clears up, it is likely to come back at some point. Watch for the symptoms and resume treating the condition when it recurs.
Wash your scalp regularly
If regular shampoo doesn’t help with dandruff, try over-the-counter dandruff shampoos. They are classified according to the active ingredient they contain:
- Pyrithione zinc (Dermazinc, Head & Shoulders)
- Selenium sulfide (Selsun Blue)
- Ketoconazole (Nizoral A-D)
- Tar (Neutrogena T/Gel, DHS Tar)
- Salicylic acid (Neutrogena T/Sal)
Use a product daily until your signs and symptoms begin to subside, and then use it one to three times a week as needed. Shampoo that contains tar can discolor light-colored hair, so you may want to use other products.
If one type of shampoo works for a time and then seems to lose its effectiveness, try alternating between two or more types. Be sure to leave your shampoo on for the full recommended time — this allows its ingredients to work. These shampoos may be rubbed gently on the face, ears and chest and rinsed off completely.
Other home remedies
The following over-the-counter treatments and self-care tips may help you control seborrheic dermatitis:
- Soften and remove scales from your hair. Apply mineral oil or olive oil to your scalp. Leave it in for an hour or so. Then comb or brush your hair and wash it.
- Wash your skin regularly. Rinse the soap completely off your body and scalp. Avoid harsh soaps and use a moisturizer.
- Apply a medicated cream. First try a mild corticosteroid cream on affected areas, keeping it away from the eyes. If that doesn’t work, try the antifungal cream ketoconazole.
- Avoid styling products. Stop using hair sprays, gels and other styling products while you’re treating the condition.
- Avoid skin and hair products that contain alcohol. These can cause the disease to flare up.
- Wear smooth-textured cotton clothing. This helps keep air circulating around your skin and reduces irritation.
- If you have a beard or mustache, shampoo facial hair regularly. Seborrheic dermatitis can be worse under mustaches and beards. Shampoo with 1 percent ketoconazole daily until your symptoms improve. Then switch to shampooing once a week. Or shaving might ease your symptoms.
- Gently clean your eyelids. If your eyelids show signs of redness or scaling, wash them each night with baby shampoo and wipe away scales with a cotton swab. Warm or hot compresses also may help.
- Gently wash your baby’s scalp. If your infant has cradle cap, wash the scalp with nonmedicated baby shampoo once a day. Gently loosen the scales with a small, soft-bristled brush before rinsing out the shampoo. If scaling persists, first apply mineral oil to the scalp for a couple of hours.
Alternative medicine
Many alternative therapies, including those listed below, have helped some people manage their seborrheic dermatitis. But evidence for their effectiveness isn’t conclusive. It’s always a good idea to check with your doctor before adding any alternative medicines to your self-care routine.
- Tea tree oil. Tea tree oil, either alone or in a shampoo, may be used on the affected area. Some studies suggest that tea tree oil may trigger an allergic reaction.
- Fish oil supplements. These types of pills contain omega-3 fatty acids.
- Aloe vera. Apply to the affected area aloe vera gel, either in a product or directly from a cut leaf of the plant.
What is perioral dermatitis
Perioral dermatitis presents as an eruption of erythematous papules, pustules and papulovesicles, most frequently seen in women 9. The cause of perioral dermatitis is unknown but it is associated with direct or indirect use of topical steroids for minor skin problems. Indirect use involves transfer to the face when steroids are being used elsewhere on the body. It is also associated with use of cosmetics, moisturisers and sunscreens 10
The incidence is estimated to be 0.5-1% 11. The incidence has decreased in recent years and this is
likely to be due to greater awareness of the problems of prolonged use of topical steroids. Perioral dermatitis is not a life-threatening disease. However, unexpectedly long period of treatment may be required to achieve a cosmetically satisfactory skin condition.
Predominantly it affects women aged 15-45 years but can affect any age group, including children. In adults, perioral dermatitis predominantly affects young females, who account for an estimated 90% of the cases.
The number of male cases is increasing and this is assumed to be because of changes in their use of cosmetics.
The clinical and histologic features of the perioral dermatitis lesions resemble those of rosacea. Patients require systemic and/or topical treatment and an evaluation of the underlying factors.
Figure 8. Perioral dermatitis

What causes perioral dermatitis
An underlying cause cannot be detected in all patients. The aetiology of perioral dermatitis is unknown. Apparent
causes include:
- Topical steroid preparations. No clear correlation exists between the risk of perioral dermatitis and the strength of the steroid or duration of use.
- Cosmetics.
- High-factor sun protection creams
- Physical factors: ultraviolet (UV) light, heat and wind worsen perioral dermatitis.
- Candidiasis has been suggested as a provoking factor.
- Miscellaneous: hormonal factors are suspected because there may be a premenstrual deterioration.
- Oral contraceptives may also be a factor.
Signs and symptoms of perioral dermatitis
Clinical presentation of papulovesicular eruption in the perioral region with a typical narrow spared zone around the edge of the lips is characteristic.
Clinical findings
Distribution
- Nasolabial erythema can be the first sign
- Perioral skin (with relative sparing of the lip margins) ie perioral dermatitis
- Periocular skin involvement ie periocular dermatitis is less common.
Morphology
- Monomorphic small papules and pustules
- Erythema
- Occasional scaling
- Unlike rosacea, facial flushing and telangiectasia are not features of perioral dermatitis
Treatment of Perioral dermatitis
- Take care if using topical steroids at a site distant to the face eg if being used to treat eczema. Make sure hands are washed after application so that the steroid is not transferred on to the face
- Discontinue any topical steroids being used on the face, or other facial creams that may be causing the symptoms. Warn patients that after withdrawal of the steroid cream the symptoms are likely to get worse for a few days before starting to improve. This flare can be avoided by advising the patient to reduce the frequency of topical steroid application over 1-2 weeks before stopping
- Patients require treatment with:
+ Milder cases – a topical antibiotic eg clindamycin, erythromycin or metronidazole
+ Other patients – a systemic antibiotic for 4-6 weeks eg a tetracycline (oxytetracycline 500 mg BD an hour before food, lymecycline 408 mg OD with food) or erythromycin 500 mg BD - + Systemic isotretinoin should be considered as a therapeutic option for patients refractory to all standard therapies.
+ Recurrent symptoms can be managed in the same way.
The use of all topical preparations, including cosmetics, should be avoided except the prescribed medication.
The patient should be advised that remission might not occur for many weeks, despite correct treatment.
What is dermatitis herpetiformis
Dermatitis herpetiformis is a rare, and intensely itchy, chronic skin condition associated with gluten enteropathy (Celiac disease), although few patients have significant gastrointestinal symptoms.
Dermatitis herpetiformis is found mainly in adults and is more common in men and people of northern European descent; dermatitis herpetiformis is rarely found in African Americans and Asian Americans 12.
- It is an immunobullous condition ie a blistering eruption caused by an abnormal immunological reaction
- Up to 10% of patients have a positive family history of dermatitis herpetiformis or Coeliac disease (gluten enteropathy)
- There is an association with thyroid and other autoimmune conditions
Symptoms of dermatitis herpetiformis
Dermatitis herpetiformis is characterized by small, clustered papules and vesicles that erupt symmetrically on the elbows, knees, buttocks, back, or scalp. The face and groin can also be involved. A burning sensation may precede lesion formation. Lesions are usually scratched off by the time a patient comes in for a physical exam, and the rash may appear as erosions and excoriations.
Patients with dermatitis herpetiformis may also experience dental enamel defects to permanent teeth, which is another manifestation of celiac disease. Less than 20 percent of people with dermatitis herpetiformis have symptoms of celiac disease 13.
Causes of dermatitis herpetiformis
Dermatitis herpetiformis is caused by the deposit of immunoglobulin A (IgA) in the skin, which triggers further immunologic reactions resulting in lesion formation. Dermatitis herpetiformis is an external manifestation of an abnormal immune response to gluten, in which IgA antibodies form against the skin antigen epidermal transglutaminase.
Family studies show that 5 percent of first-degree relatives of a person with dermatitis herpetiformis will also have dermatitis herpetiformis. An additional 5 percent of first-degree relatives of a person with dermatitis herpetiformis will have celiac disease 14. Various other autoimmune diseases are associated with dermatitis herpetiformis, the most common being hypothyroidism.
Diagnosis of dermatitis herpetiformis
A skin biopsy is the first step in diagnosing DH. Direct immunofluorescence of clinically normal skin adjacent to a lesion shows granular IgA deposits in the upper dermis. Histology of lesional skin may show microabscesses containing neutrophils and eosinophils. However, histology may reveal only excoriation due to the intense itching that patients experience.
Blood tests for antiendomysial or anti-tissue transglutaminase antibodies may also suggest celiac disease. Blood tests for epidermal transglutaminase antibodies are positive in more than 90 percent of cases 15. All of these tests will become negative with prolonged adherence to a gluten-free diet.
A positive biopsy and serology confirm dermatitis herpetiformis and should be taken as indirect evidence of small bowel damage. A biopsy of the small bowel is usually not needed for dermatitis herpetiformis diagnosis. However, if clinical signs of gastrointestinal disease are evident on examination, further workup may be required. Whether or not intestinal damage is evident, a gluten-free diet should be implemented because the rash of dermatitis herpetiformis is gluten sensitive.
Treatment for dermatitis herpetiformis
The sulfone dapsone can provide immediate relief of symptoms. For patients who cannot tolerate dapsone, sulfapyridine or sulfamethoxypyridazine may be used, although these medications are less effective than dapsone. A strict gluten-free diet is the only treatment for the underlying disease. Even with a gluten-free diet, medication therapy may need to be continued from a few months to 2 years.
Dermatitis herpetiformis can go into remission, which is defined as absence of skin lesions and symptoms of dermatitis herpetiformis for more than 2 years while not taking sulfones or other treatments and not adhering to a gluten-free diet. Cohort studies showing dermatitis herpetiformis remission provide support for reducing sulfone therapy and weaning from a gluten-free diet in patients with well-controlled dermatitis herpetiformis 16.
- Eczema. Medline Plus. https://medlineplus.gov/eczema.html[↩]
- Eczema (Atopic Dermatitis). National Institute of Allergy and Infectious Diseases. https://www.niaid.nih.gov/diseases-conditions/eczema-atopic-dermatitis[↩]
- Atopic dermatitis. American Academy of Dermatology. https://www.aad.org/public/diseases/eczema/atopic-dermatitis[↩]
- Nummular dermatitis. American Academy of Dermatology. https://www.aad.org/public/diseases/eczema/nummular-dermatitis[↩]
- Stasis dermatitis. American Academy of Dermatology. https://www.aad.org/public/diseases/eczema/stasis-dermatitis[↩]
- Fritsch PO and Reider N. “Other eczematous eruptions: Stasis dermatitis.” In: Bologna JL, Jorizzo JL, et. al. Dermatology (second edition), Elsevier Mosby, 2008:201-2.[↩]
- Trayes KP, Studdiford JS, et. al. “Edema: Diagnosis and management.” Am Fam Physician. 2013 Jul 15;88(2):102-10.[↩]
- [↩]
- PERIORAL DERMATITIS: STILL A THERAPEUTIC CHALLENGE. Acta Clin Croat. 2015 Jun;54(2):179-85. https://www.ncbi.nlm.nih.gov/pubmed/26415314[↩]
- Perioral dermatitis. The Primary Care Dermatology Society. http://www.pcds.org.uk/clinical-guidance/perioral-dermatitis-periocular-dermatitis-syn.-periorifacial-dermatitis[↩]
- https://emedicine.medscape.com/article/1071128-overview[↩]
- Bolotin D, Petronic-Rosic V. Dermatitis herpetiformis: part II. Diagnosis, management, and prognosis. Journal of the American Academy of Dermatology. 2011;64(6):1027–1033.[↩]
- Alonzo-Llamazares J, Gibson LE, Rogers RS. Clinical, pathologic, and immunopathologic features of dermatitis herpetiformis: review of the Mayo Clinic experience. International Journal of Dermatology. 2007;46(9):910–919.[↩]
- Sapone A, Bai JC, Ciacci C, et al. Spectrum of gluten-related disorders: consensus on new nomenclature and classification. https://bmcmedicine.biomedcentral.com/articles/10.1186/1741-7015-10-13[↩]
- Rose C, Armbruster FP, Ruppert J, Igl B-W, Zillikens D, Shimanovich I. Autoantibodies against epidermal transglutaminase are a sensitive diagnostic marker in patients with dermatitis herpetiformis on a normal or gluten-free diet. Journal of the American Academy of Dermatology. 2009;61(1):39–43.[↩]
- Paek SY, Steinberg SM, Katz SI. Remission in dermatitis herpetiformis: a cohort study. Archives of Dermatology. 2011;147(3):301–305.[↩]





{kind=link}