
Contents
- What is blepharoplasty
What is blepharoplasty
Blepharoplasty or eyelid surgery is a surgical procedure that removes extra eyelid skin or repositions excess fatty deposits and/or sagging skin and muscle from the upper and lower eyelids. Upper and lower eyelid blepharoplasty are indicated for the treatment of excess skin and/or orbital fat. As you age, your eyelids stretch, and the muscles supporting them weaken. As a result, excess fat may gather above and below your eyelids, causing sagging eyebrows, droopy upper lids and bags under your eyes. Besides making you look older, severely sagging skin around your eyes can reduce your side vision (peripheral vision), especially the upper and outer parts of your field of vision. Blepharoplasty can reduce or eliminate these vision problems and make your eyes appear younger and more alert.
The aim of blepharoplasty or eyelid surgery is to improve facial appearance and reduce the signs of ageing by treating:
- Loose or sagging skin that creates folds or disturbs the natural contour of the upper eyelid, sometimes impairing vision
- Excess fatty deposits that appear as puffiness in the upper eyelids
- Bags under the eyes
- Droopiness of the lower eyelids, showing white below the iris (coloured portion of the eye)
- Excess skin and fine wrinkles of the lower eyelid
Blepharoplasty is one of the most common plastic surgery operation. Eyelid surgery can be done alone or at the same time as other facial surgery, such as facelift surgery or brow lift surgery.
Proper patient selection is a critical first step in achieving optimal eyelid surgical results. Preoperative evaluation of patients who are considering blepharoplasty aesthetic procedures should include a thorough medical and ophthalmic history, along with a detailed cutaneous and eye examination and various psychiatric, emotional, and physical issues must be assessed to determine whether the patient is an appropriate candidate for blepharoplasty surgery 1). Symptoms of preexisting dry eye should be elicited preoperatively, as they directly correlate with postoperative complications. Physical examination should take into account brow position, eyelid ptosis, lower eyelid position, and cheek projection. Blepharoplasty can be performed by many operative approaches.
Blepharoplasty may be performed under either local or general anesthesia depending upon the surgical plan, patient and surgeon preference, and need for concomitant operations. A simple upper or lower eyelid blepharoplasty where only skin or fat is excised can be performed under local anesthesia. Other more invasive procedures, such as lower blepharoplasty combined with fat repositioning, mid-face lift, or endoscopic browlift may need intravenous sedation, or general anesthesia.
In the past, the average ophthalmic plastic surgeon focused mainly on the functional disciplines, with few surgeons showing any interest in cosmetic surgery. This trend is gradually changing, and today, most ophthalmic plastic surgeons perform cosmetic surgeries and many specialize in this area of practice 2).
The eye is an important component of facial aesthetics, and eyelid surgery (blepharoplasty) can play a vital positive role in facial harmony and the perception of aging 3). Blepharoplasty is one of the most commonly performed facial cosmetic procedures. Symptoms such as tired-looking eyes, excess skin, droopy eyelids, or circles around the eyes may benefit from blepharoplasty 4). It can also be combined with other facial and skin rejuvenation procedures such as brow or mid-face lift, lasers or chemical skin resurfacing 5).
Eyelid surgery results
Many people express satisfaction with the results of blepharoplasty, such as a more rested and youthful appearance and more self-confidence. For some people, results of surgery may last a lifetime. For others, droopy eyelids may recur.
Will I need anaesthesia?
Eyelid surgery can be performed under general anaesthesia or local anaesthesia.
Modern anaesthesia is safe and effective, but does have some risks. Ask your specialist plastic surgeon and anaesthetist for more information. Your surgeon and/or anaesthetist will ask you about all the medications you are taking or have taken, and any allergies you may have. Make sure you have an up to date list before the surgery.
Will I have scarring?
Scars are an inevitable part of any invasive surgery. Your plastic surgeon will endeavour to minimize scarring and to keep your scars as inconspicuous as possible by locating the incisions in easily hidden sites. That way, scars will be along natural skin lines and creases. Scars may fade with time and become barely noticeable. If you are prone to scarring, you should advise your surgeon.
Figure 1. How blepharoplasty is done
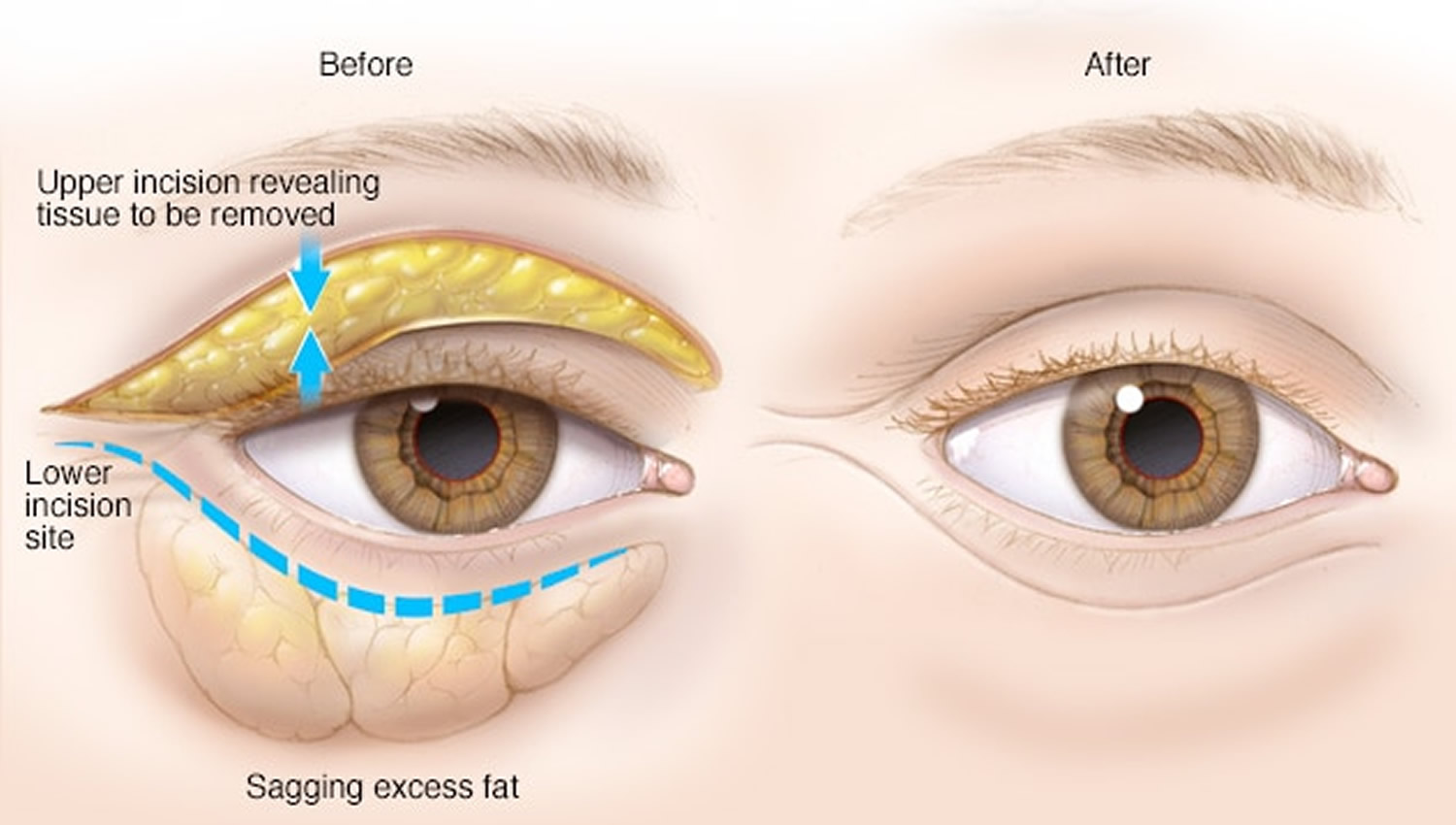
Is eyelid surgery right for me?
Eyelid surgery (blepharoplasty) is a highly individualized procedure and may not be suitable for everyone. Always talk to your specialist plastic surgeon before making a decision. Your surgeon will assess your condition and general health, and plan the treatment that is best suited to you.
Before you decide on eyelid reduction surgery, there are some important issues to keep in mind:
- Upper eyelid surgery is often carried out separately from lower eyelid surgery. Be prepared for two separate operations
- Eyelid reduction cannot remove dark circles under the eyes, lift sagging eyebrows or get rid of crow’s feet
- Smokers are at increased risk of complications. If you are serious about undergoing surgery, you should quit smoking
Eyelid surgery may not be a good option for you if you are:
- Not able to have an anaesthetic
- Prone to bleeding tendencies or have poor healing ability
- Too high risk of having surgical complications
Eyelid surgery may be a good option for you if:
- You are physically healthy and you do not have medical conditions that can impair healing or increase risk of surgery
- You do not have any serious eye conditions
- You have realistic expectations of what eyelid reduction surgery can accomplish
- You are a non-smoker or have stopped smoking
Where will the eyelid surgery take place?
Depending upon your general health and the extent of the blepharoplasty procedure, eyelid reduction surgery can be performed either as a day case or alternatively with a short hospital stay. Your plastic surgeon will advise on the best option for you.
Eyelid surgery risks and complications
Modern surgery is generally safe but does have the potential for risks and complications to occur.
Specific risks and complications associated with eyelid reduction surgery include:
- Bruising and swelling
- Pain and discomfort
- Removal of too much skin, possibly exposing the cornea to injury
- Asymmetry of the eyelids
- Noticeable scarring of the incisions
- Itchiness, watering or dryness of the eyes
- Drooping of the lower eyelid which will usually recover but occasionally requires further surgery
- Temporary changes in vision. In rare cases, changes in vision may be long lasting or permanent
- In extremely rare cases, eyelid reduction surgery can lead to blindness. Smoking, pre-existing eye disease, straining, lifting and coughing can add to this risk.
What do I need to do before my eyelid surgery?
Before undergoing surgery, it is important that you:
- Be as fit as possible to help the recovery process
- Check with your surgeon about your medications as some may need to be stopped
- Stop smoking
You will also be asked to provide a complete medical history for your Specialist Plastic Surgeon including any health problems you have had, any medication you are taking or have taken, and any allergies you may have. In addition, tell your surgeon if you have had:
- Previous eyelid or facial surgery
- Dry eyes, use of eye drops or visual disturbances
- Any use of glasses or contact lenses
You may be advised to stop taking certain medicines such as non-steroidal anti-inflammatory drugs (NSAIDs), aspirin, and medicines that contain aspirin. You may also be asked to stop taking naturopathic substances such as garlic, ginkgo, ginseng and St John’s Wort as they may affect clotting and anaesthesia. Always tell your surgeon EVERYTHING you are taking.
You may be given medicines to take before the surgery, such as antibiotics.
Unless your surgeon advises differently, you will be able to continue taking most medicines that you have been taking.
If you decide to have eyelid reduction surgery, your surgeon will ask you to sign a consent form. Make sure you read the consent form carefully before signing. If you have any questions, ask your surgeon.
Prepare a “recovery area” in your home. This may include pillows, ice packs, a thermometer and a telephone within easy reach. Make sure you arrange for a relative or friend to drive you to and from the hospital or clinic. Someone should also stay with you for at least 24 hours after you return home.
Your surgeon should give detailed preoperative instructions. Follow them carefully.
Anatomy of the upper eyelid
A thorough understanding of the upper eyelid anatomy is essential when evaluating patients for possible upper blepharoplasty. The skin and orbicularis oculi muscle form the anterior layers of the upper eyelid. Deep to these layers is the orbital septum, which originates from the arcus marginalis at the superior orbital rim and inserts on the levator aponeurosis. The point of attachment of the orbital septum to the levator aponeurosis varies in different ethnic populations, with Caucasians having a higher insertion than Asians. Immediately posterior to the orbital septum resides 2 preponeurotic fat pads (nasal and central) as well as the lacrimal gland laterally. The levator aponeurosis is posterior to the preaponeurotic fat and measures approximately 10-15mm in length. Deep to the levator aponeurosis lies Muller’s muscle, which is a sympathetically innervated elevator of the upper eyelid. The tarsus, composed of dense connective tissue, is located posterior to the orbicularis at the eyelid margin and measures approximately 25 mm x 10mm. The rigidity of the tarsus is important in maintaining the structural stability and proper orientation of the eyelid margin and eyelashes. The conjunctiva lines the posterior aspect of the eyelid.
Figure 2. Eye anatomy
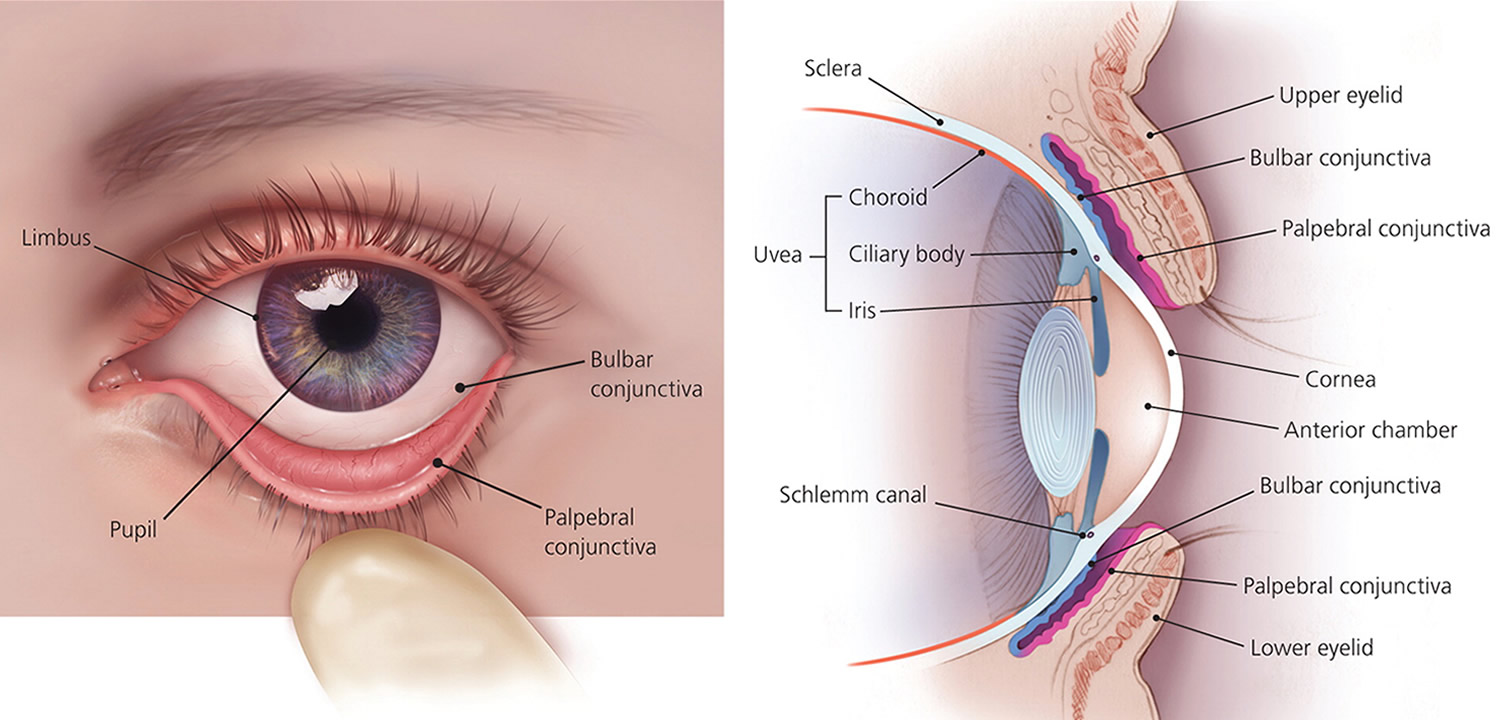
Figure 3. Lacrimal apparatus
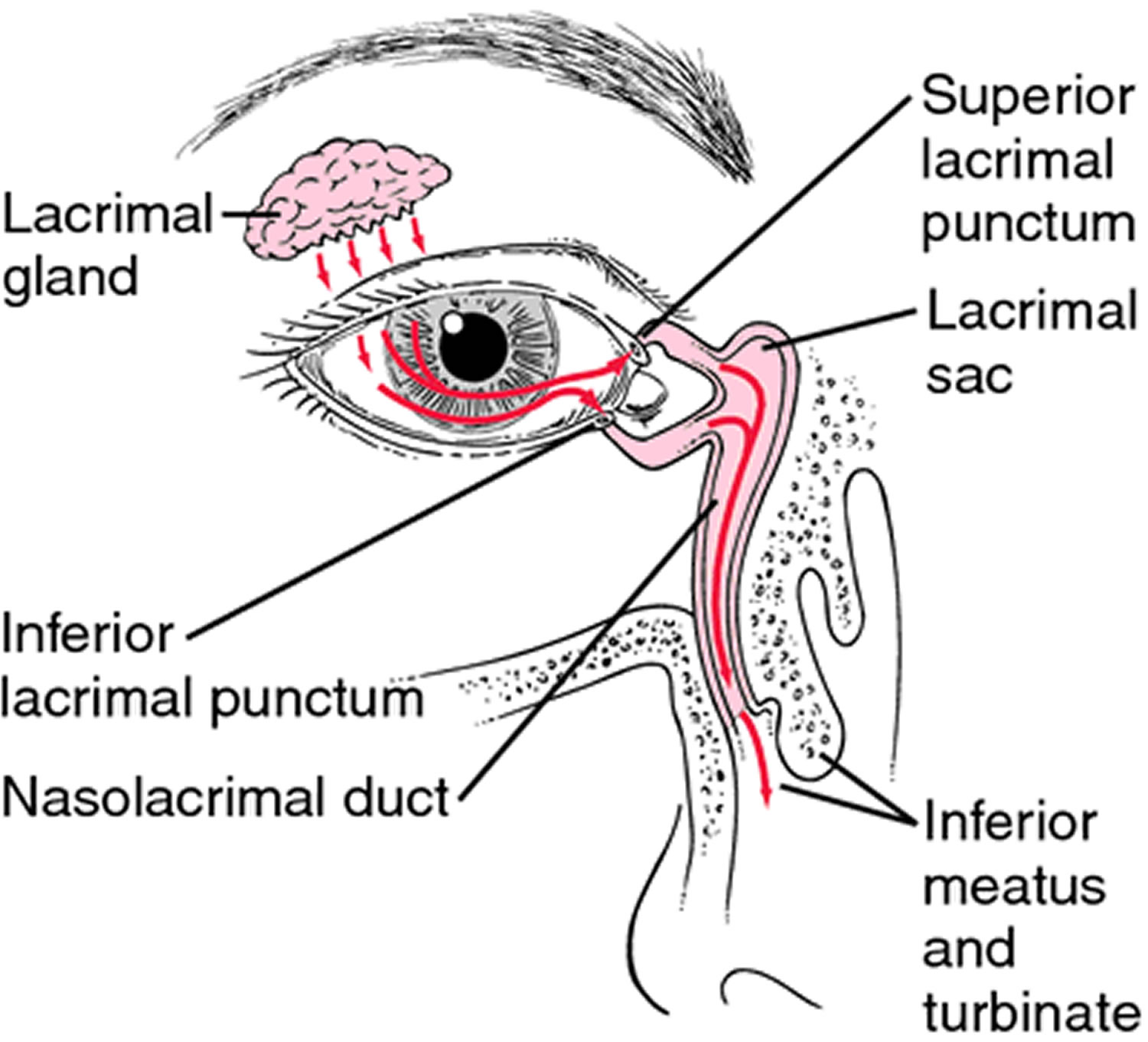
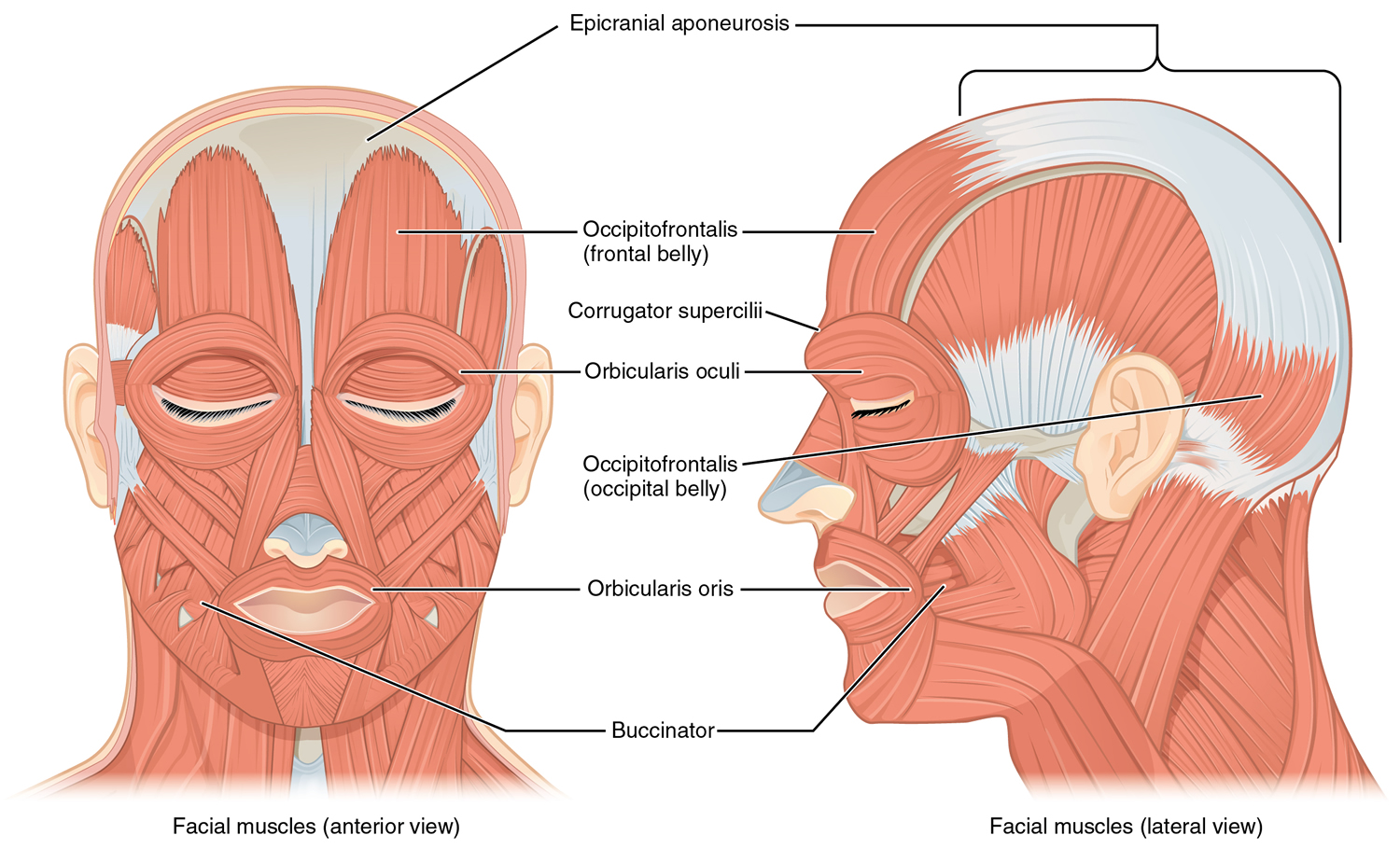
Figure 4. Orbicularis oculi muscle
Why blepharoplasty surgery is done
You might consider blepharoplasty if droopy or sagging eyelids keep your eyes from opening completely or pull down your lower eyelids. Removing excess tissue from your upper eyelids can improve your vision. Upper and lower lid blepharoplasty can make your eyes appear younger and more alert.
Blepharoplasty may be an option if you have:
- Baggy or droopy upper eyelids
- Excess skin of the upper eyelids that interferes with your peripheral vision
- Excess skin on the lower eyelids
- Bags under your eyes
You may undergo blepharoplasty at the same time as another procedure, such as a brow lift, face-lift or skin resurfacing.
Insurance coverage may depend on whether the surgery repairs a condition that impairs vision. If you have the surgery only to improve your appearance, the cost probably won’t be covered by insurance. Lower lid blepharoplasty is almost always done just for cosmetic reasons.
How much does eyelid surgery – blepharoplasty cost?
Cost is always a consideration in elective surgery. The cost of blepharoplasty varies widely from one patient to another and prices for individual procedures can vary widely between plastic surgeons. Generally, blepharoplasty is a cosmetic procedure and not covered by insurance. However, some carriers will cover a portion of the cost for functional and/or restorative blepharoplasty. To qualify, the redundant skin must cause a significant visual impairment. Insurance may also cover reconstructive aspects for the removal of skin cancer, tumors, etc. Lower eyelid surgery is generally considered cosmetic with a few exceptions. Please consult with your individual insurance carrier and benefits details for specific information about your plan.
Some factors that may influence the cost include the surgeon’s experience, the type of procedure used and the geographic location of the office.
Costs associated with the eyelid procedure may include:
- Surgeon’s fee
- Hospital or surgical facility costs
- Anaesthesia fees
- Prescriptions for medication
- Post-surgery garments
- Medical tests
Your surgeon should welcome any questions you may have regarding fees.
What are alternatives to eyelid surgery?
There is no alternative to a surgical eyelid lift if you have significant excess skin or fat bulging. However, for patients with mild or moderate signs of eyelid aging, there are alternatives that are also very effective at eliminating the “tired” eyelid appearance.
- Dermal Fillers
Dermal fillers are one of the most popular non-surgical treatments to rejuvenate the eyes. Fillers can be used to eliminate the appearance of under eye bags, smooth away wrinkles, crows feet and fine lines around the eyes. A new filler, Voluma™, can be used to restore volume to the cheeks, which can also improve the appearance of the lower eyelids.
- Botox® & Botulinum Injections
Botox®, Xeomin®, and Dysport® injections can be used to lessen the appearance of crow’s feet, and in some patients have a similar effect to an eyelid lift or brow lift. These cosmetic injectables work by temporarily disable the nerves in the muscles of the brows that cause a worried expression.
- Laser Skin Rejuvenation
Our fractional laser can be used around the eyes to minimize fine lines and wrinkles and improve the tone and texture of skin. Laser skin resurfacing can have a skin tightening effect that can make the area around the eyes look lifted and more youthful.
- Fat Transfer
Fat Transfer is a safe, natural and more long lasting alternative to fillers to eliminate the appearance of upper eyelid hallowing and lower eyelid bags. Fat can be removed from practically anywhere on the body, purified and then carefully grafted into the eyelid region to restore youthful volume.
Blepharoplasty surgery risks
Possible risks of eyelid surgery include:
- Infection and bleeding
- Dry, irritated eyes
- Difficulty closing your eyes or other eyelid problems
- Noticeable scarring
- Injury to eye muscles
- Skin discoloration
- The need for a follow-up surgery
- Temporarily blurred vision or, rarely, loss of eyesight
- Risks associated with surgery in general, including reaction to anesthesia and blood clots
Complications of eyelid surgery include:
- Scarring at incision site
- Asymmetry
- Overcorrection
- Undercorrection
- Medial canthal webbing
- Lagophthalmos
- Ocular surface exposure
- Retrobulbar hematoma/loss of vision
- Perforation of globe
- Ptosis
- Numbness beneath incision
- Patient dissatisfaction with outcome
Talk to your doctor about how surgical risks apply to you. Understanding what’s involved in blepharoplasty and weighing the benefits and risks can help you decide if this procedure is a good option.
How you prepare for eyelid surgery
Before scheduling blepharoplasty, you will meet with a plastic surgeon and an eye specialist (ophthalmologist) or a plastic surgeon who specializes in eye surgeries (oculoplastic surgeon) to discuss:
- Your medical history. Your surgeon will ask questions about previous surgeries and past or current conditions, such as dry eyes, glaucoma, allergies, circulatory problems, thyroid problems and diabetes. Your doctor will also ask about your use of medications, vitamins, herbal supplements, alcohol, tobacco and drugs.
- A complete medical and ophthlamic history should be obtained that includes:
- Previous ocular conditions and surgeries
- Prior cosmetic procedures
- Dry eye symptoms and treatments
- Complete list of medications including blood thinners and herbal supplements
- Psychiatric history.
- A complete medical and ophthlamic history should be obtained that includes:
- Your expectations. An honest discussion of your hopes and motivation for surgery will help set the stage for a satisfactory outcome. Your surgeon will discuss with you whether the procedure is likely to work well for you.
Before your eyelid surgery, you’ll undergo:
- A physical examination. Your surgeon will conduct a physical examination, which may include testing your tear production and measuring parts of your eyelids.
- A vision examination. Your eye doctor will examine your eyes and test your vision, including your peripheral vision. This is needed to support an insurance claim.
- Eyelid photography. Your eyes will be photographed from different angles. These photos help with planning the surgery, assessing its immediate and long-term effects, and supporting an insurance claim.
- Eyelid examination
- Quality, quantity and relative symmetry of redundant skin
- Eyelid crease height and symmetry
- Grading of medial and central preponeurotic fat pad herniation
- Evaluation for lacrimal gland prolapse
- Evaluation for presence of concurrent ptosis (palpebral fissure width, margin reflex distances, levator function, eyelid crease height)
- Measurement of brow position as patients with significant brow ptosis should be considered for a concurrent brow lifting procedure at the time of
- blepharoplasty
- Lagophthalmos on attempted eyelid closure
- Presence of intact Bell’s phenomenon
- Evaluation of lower lid laxity/eyelid or eyelash malposition
- Orbicularis strength
- Orbital symmetry
And you’ll be asked to:
- Stop taking warfarin (Coumadin, Jantoven), aspirin, ibuprofen (Advil, Motrin IB, others), naproxen sodium (Aleve, others), naproxen (Naprosyn), and any other medication or herbal supplement associated with increased bleeding. Ask your doctor how long before surgery you need to stop taking these medicines. Take only medications approved by your surgeon.
- Quit smoking several weeks before your surgery. Smoking can reduce your ability to heal after surgery.
- Arrange for someone to drive you to and from surgery if you’re having outpatient surgery. Plan to have someone stay with you for the first night after returning home from surgery.
What you can expect from eyelid surgery
Before the blepharoplasty surgical procedure
Blepharoplasty is usually done in an outpatient setting. Your surgeon injects numbing medication into your eyelids and administers intravenous medication to help you relax.
During the blepharoplasty surgical procedure
If you have surgery on your upper and lower eyelids, the surgeon generally works on your upper lids first. He or she cuts along the fold of the eyelid, removes some excess skin, muscle and possibly fat, and closes the cut.
On the lower lid, the surgeon makes a cut just below the lashes in your eye’s natural crease or inside the lower lid. He or she removes or redistributes excess fat, muscle and sagging skin, and closes the cut.
If your upper eyelid droops close to your pupil, your surgeon may do blepharoplasty with a procedure called ptosis that provides additional support to the eyebrow muscle.
After the blepharoplasty surgical procedure
After surgery you spend time in a recovery room, where you are monitored for complications. You can leave later that day to recuperate at home.
You can usually drink fluids and eat a light meal within two or three hours after surgery. You may have some pain and discomfort, particularly around the incisions. Your plastic surgeon will prescribe pain medication as required.
After surgery you may temporarily experience:
- Blurred vision from the lubricating ointment applied to your eyes
- Watering eyes
- Light sensitivity
- Double vision
- Puffy, numb eyelids
- Swelling and bruising similar to having black eyes
- Pain or discomfort
Your doctor will likely suggest you take the following steps after surgery:
- Use ice packs on your eyes for 10 minutes every hour the night after surgery. The following day, use ice packs on your eyes four to five times throughout the day.
- Gently clean your eyelids and use prescribed eyedrops or ointments.
- Avoid straining, heavy lifting and swimming for a week.
- Avoid strenuous activities, such as aerobics and jogging, for a week.
- Avoid smoking.
- Avoid rubbing your eyes.
- If you use contact lenses, don’t put them in for about two weeks after surgery.
- Wear darkly tinted sunglasses to protect the skin of your eyelids from sun and wind.
- Sleep with your head raised higher than your chest for a few days.
- Apply cool compresses to reduce swelling.
- After a few days, return to the doctor’s office to have stitches removed, if needed.
- For about a week, avoid aspirin, ibuprofen (Advil, Motrin IB, others), naproxen sodium (Aleve, others), naproxen (Naprosyn), and other medications or herbal supplements that may increase bleeding. If needed, use acetaminophen (Tylenol, others) to control pain.
Seek medical attention immediately if you experience any of the following:
- Shortness of breath
- Chest pain
- An unusual heart rate
- Severe new eye pain
- Bleeding
- Vision problems
Eyelid surgery recovery
Bruising and swelling generally subside in 10 to 14 days, which may be when you feel comfortable going out in public again. Sleeping with your head elevated will help to reduce the swelling.
You may be required to clean your eyes as they sometimes become crusty and itchy. You may need to use lubricating drops. Your eyes may be sensitive to light for a few days so you may need to wear sunglasses. Do not wear contact lenses for at least two weeks.
Depending on the extent of your procedure, you may need to take a few days off work to rest. Avoid heavy lifting, strenuous exercise, swimming and strenuous sports until advised by your surgeon.
Scars from the surgical cuts may take months to fade. Take care to protect your delicate eyelid skin from too much sun exposure.
- Use ice compresses frequently for the first 3 days after surgery and warm compresses afterward
- Antibiotic ointment is prescribed for the incision sites 3-4 times/day
- Avoid lifting, bending, straining, exercise during the first 10 days after surgery
- Call if experiencing loss of vision, double vision, bleeding, severe swelling or pain
- Follow up within 1 week of surgery for a postoperative evaluation
If you experience any of the following symptoms, notify your surgeon immediate:
- Temperature higher than 100 °F (38 °C) or chills
- Heavy bleeding from the incisions
- Worsening redness around the incision sites
- Increasing pain or tenderness, or other problems that appear to be worsening
Preoperative evaluation
Preoperative patient evaluation for blepharoplasty should document medical and ophthalmologic history such as chronic systemic diseases and medications. Ophthalmologic history should be obtained, including vision, corrective lenses, trauma, glaucoma, allergic reactions, excess tearing, and dry eyes. No cosmetic surgery of the periorbital region should be performed for a minimum of six months following corneal refractory surgery. Schirmer’s test should be considered if there is history of dry eye.
In addition to complete eye examination, the evaluation of the periorbital area should take into account skin quality and quantity, underlying three-dimensional soft-tissue contours, and the bony skeletal support.
Assessment of the upper eyelid
Upper eyelid dermatochalasis is the loss of elasticity and support in the skin. This can create a fold of excess upper eyelid skin, which can impair the function of the eye, including supero-lateral visual field obstruction [Figure 5, top left and right]. Evaluation of pre-septal and eyebrow fat pads is important in redefining the superior sulcus. Assessment of patient’s old photographs aids the surgeon in restoring the youthful look. Upper eyelid ptosis should also be noted, since it can be corrected simultaneously.
Figure 5. Typical aging changes in the eyelid – Note: Overhanging upper eyelid skin (top left and right), with prominent orbital rim hollow and lower eyelid fat prolapse (top right). Lower eyelid fat prolapse becomes less prominent in downgaze (bottom left) and more prominent in upgaze (bottom right)

Assessment of the lower eyelid
Lower eyelids should be assessed for skin excess and fat herniation, which typically presents as medial, central, and lateral fat pads. Lower eyelid fat becomes more prominent in upgaze and less prominent in downgaze [Figure 5, bottom left and right]. Downward displacement of the lateral canthus can result from disinsertion, laxity, or the presence of a prominent eye [Figure 5, top right]. Lower lid distraction test can determine the degree of laxity and guide lower eyelid canthal repositioning. The posterior displacement of the orbital rim in relation to the anterior cornea and lower lid margin, a negative vector, should be noted preoperatively. Prominent or deep-set eyes should be documented with exophthalmometry. Malar anatomy needs to be evaluated for periorbital hollows.
Assessment of the eyebrow
Brow ptosis is assessed by evaluating the position of the eyebrow in relation to the superior orbital rim. Asymmetry in the upper and lower eyelids and brow position is common and should be recognized and addressed individually.
Upper eyelid surgery
Preoperative markings should be made with the patient sitting upright in neutral gaze with the brow properly positioned. The eyelid crease is situated above the ciliary margin approximately 8 to 9 mm in women and 7 to 8 mm in men. The lower limit of excision should be along the eyelid crease, and the lateral extent of the marking should be limited by an imaginary line joining the lateral end of the brow to the lateral canthus [Figure 6, top right]. The extent of excision should be at least 10 mm from the inferior border of the brow, making a pattern of skin excision as shown in the Figure 6. A skin pinch test can confirm the preoperative markings. A minimum of 20mm of vertical lid height should be preserved for normal eye closure. The location of fat should be determined and marked preoperatively.
Figure 6. Upper eyelid blepharoplasty – Note: Measurement is performed to leave minimum 20 mm vertical lid height (top left). Skin marking for upper eyelid blepharoplasty (top right). Subcutaneous injection of local anesthetic agent (bottom left). Skin incision with radiofrequency fine monopolar empire tip (bottom right)

Upper eyelid surgical technique
The upper eyelids should be injected superficially, with 2% lidocaine with 1:100,000 epinephrine using a 27 to 30-gauge needle [Figure 6, bottom left]. Skin incision can be made either with a No 15 Bard Parker blade or the Empire tip of radiofrequency monopolar cautery [Figure 6, bottom right]. Conservative fat excision can be performed as part of upper eyelid blepharoplasty [Figure 7, top right]. There are two fat compartments, medial and central that can be accessed through small incisions in the septum, teased out, and resected using radiofrequency monopolar tip. Of the medial and central fat, only the fat that comes easily into the wound is excised. It is important not to aggressively pull fat from the orbit.
Retro-orbicularis oculi fat can be accessed beneath the lateral orbicularis overlying the superior orbital rim. Resection has been described to help decrease heaviness of the upper lid and lateral brow. The sub-brow fat pad can be repositioned during wound closure with use of eyelid suspension sutures. This can be done with two to three absorbable sutures that incorporate the orbicularis from the lower and upper edge of the incision along with the superolateral arcus marginalis [Figure 7, bottom left]. These sutures might result in early over-correction of the upper eyelid leading to lagophthalmos, which improves within days after the surgery. The transconjunctival approach has very limited application in upper eyelid blepharoplasty 6). The skin incision can be closed using running or interrupted sutures with various absorbable or permanent materials [Figure 7, bottom right], or cyanoacrylate glue to achieve an aesthetic outcome [Figure 8 Upper Blepharoplasty Before and After].
Figure 7. Upper eyelid blepharoplasty surgical technique – Note: Skin undermining and excision with radiofrequency monopolar tip (top left). Fat pad excision after incising the orbital septum (top right). Periosteal anchoring suture which helps in restoring brow fat pad fullness (bottom left). Skin closure with 6-0 Prolene™ continuous suture (bottom right)

Figure 8. Upper Blepharoplasty Before and After



Upper eyelid postoperative care
Postoperatively, patients should be advised to use ice packs on the surgical site for three days to minimize postoperative swelling, and topical ciprofloxacin ophthalmic ointment on the incision sites for two weeks. Non-absorbable sutures, if used, can be removed after one week.
Upper eyelid complications
Possible complications include upper eyelid retraction with scleral show from anterior lamellar inadequacy, lagophthalmos, acquired diplopia and corneal exposure. The most common complication of cosmetic surgery is failure to meet the patient’s expectations. This can be avoided by preoperative counseling and identifying reasonable expectations.
Lower eyelid surgery
Aging can lead to a number of aesthetic changes in the lower eyelid including skin laxity or excess, orbital septum laxity, orbicularis laxity or hypertrophy, herniation of the orbital fat, canthal laxity, malar festoons, crow’s feet, and periocular wrinkles 7). Common complaints include eyelid bags, circles under the eye, wrinkles around the eye, or a tired look. Anatomically, relaxation of the orbital septum, orbicularis muscle, and skin can cause protrusion of intraorbital fat leading to eyelid bags [Figure 5, top right]. Typical periorbital hollows have a distinct anatomic basis that needs attention during treatment 8). Lower eyelid rejuvenation is more complex and has several treatment options such as fillers, lower eyelid blepharoplasty and skin resurfacing. Most cosmetic surgeons today have developed a customized approach to eyelid surgery in which the specific anatomic problems are identified and the operation is individualized to address these problems.
The traditional procedure in lower eyelid blepharoplasty was to remove the pseudo-herniated fat via skin incision. A recent, more conservative approach includes repositioning of the herniated fat in cases of tear trough deformity into the subperiosteal space. Both these approaches may be accompanied by strengthening procedures for the attenuated septum or septorrhaphy and tightening of the orbicularis muscle and skin 9). Defocused CO2 laser irradiation of the undersurface of the orbicularis results in persistent shortening and tightening of the muscle tissue 10).
The approach to the lower eyelid remains a controversial issue within plastic surgery. The transconjunctival approach had reduced chances of eyelid retraction, scleral show, and postoperative ectropion compared to other methods 11). Some surgeons prefer a transcutaneous approach in patients who have hypertrophy of the orbicularis oculi muscle and therefore require muscle excision 12).
Lower eyelid blepharoplasty surgical technique
Transconjunctival lower lid blepharoplasty
For transconjunctival lower lid blepharoplasty, the inferior fornix, eyelid skin, and lateral canthus are anesthetized with 1% lidocaine containing 1:100,000 epinephrine [Figure 9, top left]. Surgery is performed through an incision made 4-6 mm below the lid margin through the conjunctiva and lower eyelid retractors [Figure 9, top right]. This can be done by sharp dissection with scissors, radiofrequency monopolar cautery, or laser. Gentle pressure on the eyeball prolapses the fat compartments and aids in identification of the medial, central, and lateral fat pads. Conservative fat removal is achieved using radiofrequency monopolar or bipolar cautery [Figure 9, bottom left and right]. Care is taken not to damage the inferior oblique muscle that separates the medial from the central fat pocket. The endpoint for excision is reached when gentle pressure on the globe results in the anterior aspect of the orbital fat being flush with the orbital rim. The tarsoconjunctival incision is left unclosed, but the inferior and superior edges of the conjunctival epithelium are well apposed to avoid overlap. The incision usually heals within a week to give an aesthetic result [Figure 10, Lower Blepharoplasty Before and After].
Some surgeons perform lateral canthopexy along with lower eyelid blepharoplasty. It eliminates unnecessary skin resection, and is believed to restore tone and youthful contour of the lower eyelid 13).
Wrinkles and excess of vertical skin can be dealt with by skin resurfacing techniques, such as chemical peeling and CO2 or Erbium-YAG laser resurfacing. These techniques are applicable only to patients with Fitzpatrick skin Type I-III. Patients with darker skin are at risk of pigmentary changes; hence these can be managed with surgical excision by the pinch technique (see below).
Figure 9. Transconjunctival lower eyelid blepharoplasty – Note: Injection of local anesthetic into the inferior conjunctival fornix (top left). Forniceal incision to expose orbital fat (top right). Conservative fat excision with radiofrequency monopolar tip (bottom left). Assessment of contours on table (bottom right)
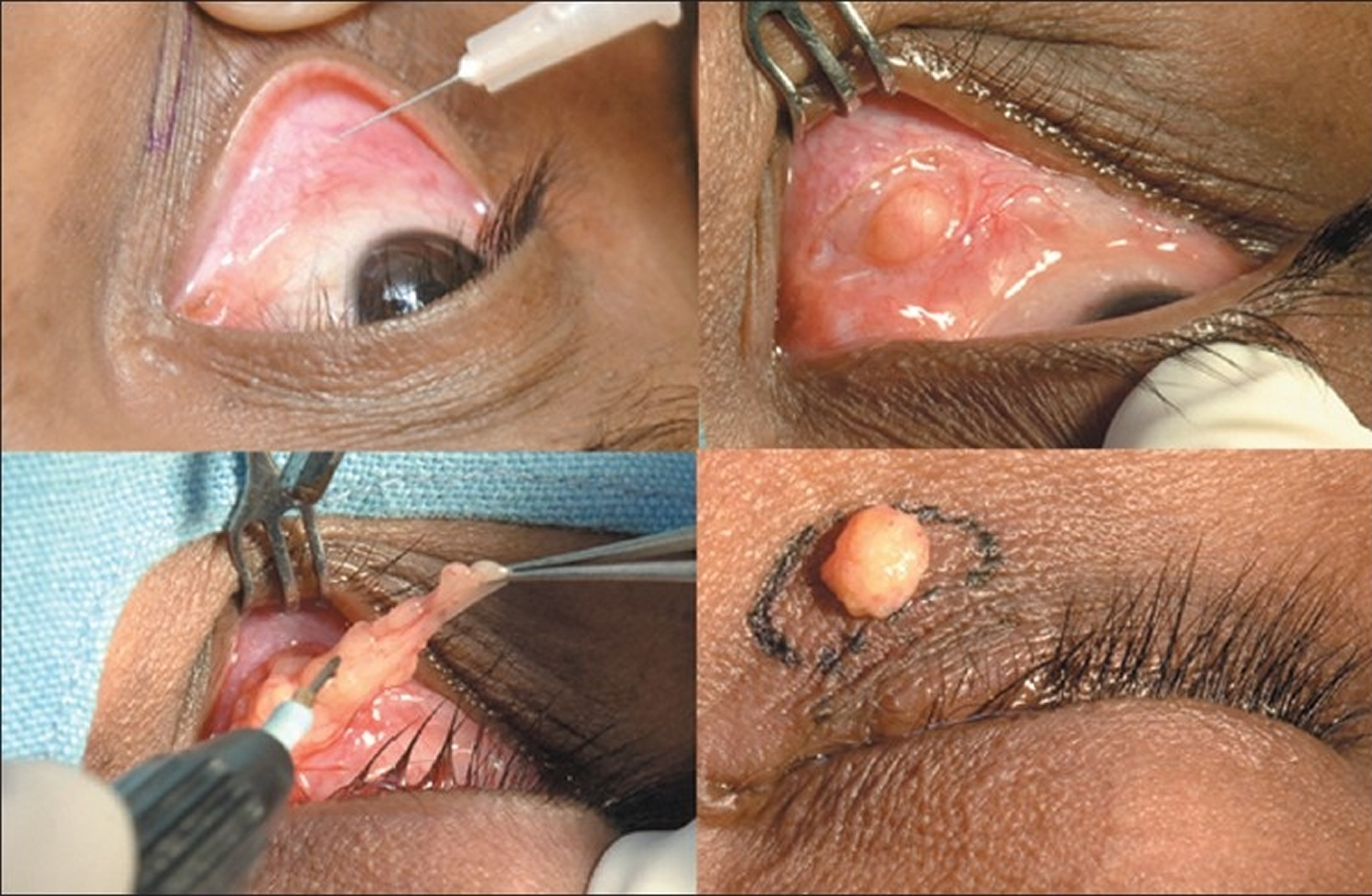
Figure 10. Lower Blepharoplasty Before and After



Transcutaneous lower lid blepharoplasty
The ‘skin pinch’ technique is ideal for skin laxity alone, with no fat prolapse 14). It is approached through a subciliary incision with the skin elevated off the orbicularis. The amount of skin to be resected can be estimated with a skin pinch between forceps. Redundant skin can be removed conservatively and redraped without disturbing the underlying orbicularis.
The more aggressive ‘skin-muscle flap’ method is also approached through a subciliary incision, undermining the skin and orbicularis. The pretarsal orbicularis fibers should remain intact, and the skin and preseptal orbicularis are elevated as one flap. Dissection can be continued along the orbital septum to the level of the orbital rim. Periorbital fat is approached through small incisions in the septum. Orbicularis muscle fibers and skin can be excised at closure; however, damage to the orbicularis may lead to lower lid malposition and orbicularis denervation.
Transcutaneous lower lid blepharoplasty complications
Severe complications, such as visual loss from orbital hemorrhage, orbital injection, or posterior optic nerve infarction are extremely rare, but have been described 15). Other possible complications are lower eyelid retraction with scleral show, lagophthalmos, corneal exposure and acquired strabismus.
Lower eyelid fat repositioning
In youth, the eyelid-cheek complex has a single smooth convex profile. With advancing age, thinning of septum, receding bony orbital rim, and pseudo-herniation of intraorbital fat occurs producing a double convex deformity on the lower eyelid 16). Simple removal of orbital fat in this situation can result in a hollow appearance of the lower eyelid. Preservation of the lower orbital fat is a new concept in facial rejuvenation, and such preservation creates a smooth transition to the malar eminence [Figure 10 Lower Blepharoplasty Before and After], blending nicely into the upper face 17).
Lower eyelid fat repositioning surgical technique
Fat repositioning surgery includes release of the arcus marginalis and advancement of the orbital fat beyond the infraorbital rim underneath the orbicularis muscle with the help of temporary exteriorized sutures [Figure 11]. The fat can be placed either in the subperiosteal or supra-periosteal plane, with no apparent effect on aesthetic results. This technique camouflages the lower orbital rim anatomy and provides more youthful rejuvenation of the mid-face 18).
Other methods suggested to correct tear trough deformity include orbital fat removal, fat injections or grafts, and alloplastic cheek implants. In general, transconjunctival fat repositioning results in leveling of the tear trough deformity, a smooth contour of the lower eyelid, and high patient satisfaction 19).
Lower eyelid fat repositioning complications
Complications include persistence of dark circles, temporary skin irregularities from fat and edema, fat granulomas, restricted ocular motility, or new-onset diplopia 20).
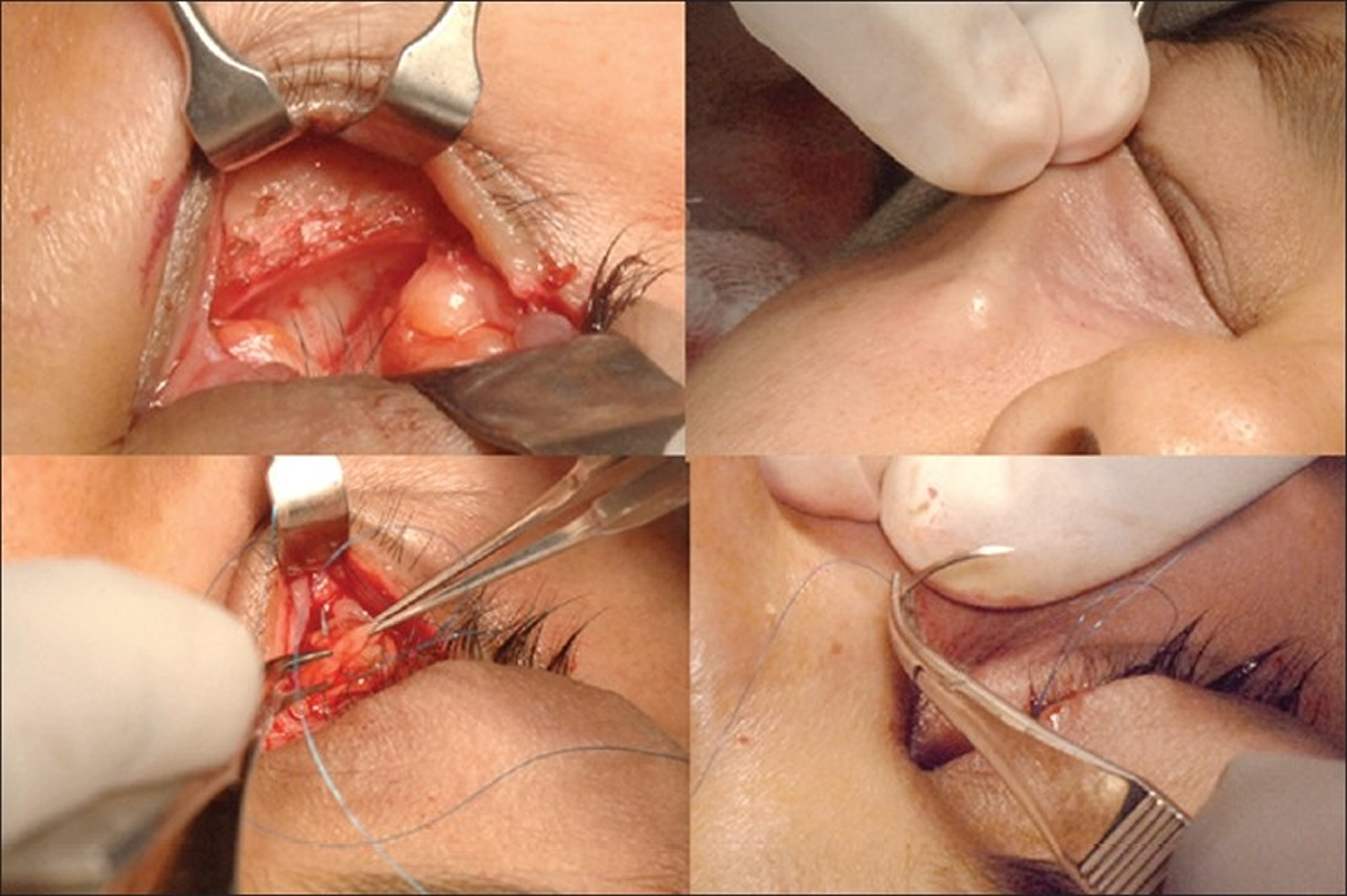
Figure 11. Transconjunctival lower eyelid fat repositioning – Note: Surgeon’s view showing exposed orbital fat and inferior orbital rim (top left). Release of orbitomalar ligament and creation of supra-periosteal pocket for fat repositioning (top right). Prolene™ 6-0 sutures passed through orbital fat pads (bottom left). Exteriorization of Prolene™ sutures to reposit fat within the orbital rim hollow (bottom right)
Combination blepharoplasty
Variations to these standard blepharoplasty approaches are numerous, and often a combination therapy is needed based on patient findings 21). Fillers, such as hyaluronic acid, can be used especially in the lower eyelid to correct volume deficiency that could not be addressed by blepharoplasty alone. Autologous fat transfer into this area is also an option, with long-lasting results. Orbicularis repositioning can be used to eliminate hypotonic and herniated orbicularis muscle, soften palpebral depressions, and shorten the lower lid to cheek distance. Lower eyelid skin resurfacing can be performed with chemical peels or ablative laser for conservative lid tightening as an adjunct to a transconjunctival fat excision. Lateral canthal resuspension is often combined with lower eyelid blepharoplasty as described earlier. Mid-face cheek and orbicularis repositioning, and subperiosteal mid-face-lifting procedures are often combined, but are beyond the scope of this article. Concomitant endoscopic brow lift if performed should be done before upper blepharoplasty so that correct brow position is ensured before upper lid skin excision.
References [ + ]





{kind=link}