Contents
What is fibromuscular dysplasia
Fibromuscular dysplasia is a disease that causes the muscle and fibrous tissues in one or more arteries in your body to have abnormal cell development in the artery wall. As a result, areas of narrowing (stenosis), aneurysms, or tears (dissection) may occur. If narrowing or a tear causes a decrease in blood flow through the artery, symptoms may result. Fibromuscular dysplasia is most commonly found in the arteries that supply the kidneys with blood (renal arteries) and the arteries called the carotid and vertebral arteries which are found in the neck and supply the brain with blood. Less commonly, fibromuscular dysplasia affects the arteries in the abdomen (supplying the liver, spleen and intestines) and extremities (legs and arms). In more than one-half of people with this disease, there will be evidence of fibromuscular dysplasia in more than one artery.
Most cases of fibromuscular dysplasia—60 to 75 percent—occur in the renal artery, the artery leading from the abdominal aorta to the kidneys. Approximately 30 percent of cases involve the carotid arteries, the arteries in the neck that connect the heart and the brain. Fibromuscular dysplasia also can affect the arteries to the legs, or less frequently, arteries in other parts of the body.
Recently, studies have shown that some women who were healthy and who have a sudden tearing of a coronary artery called spontaneous coronary artery dissection (SCAD) probably have undiagnosed fibromuscular dysplasia. Spontaneous coronary artery dissection was previously thought to be a separate condition to fibromuscular dysplasia, but now scientists are starting to understand that many people have fibromuscular dysplasia as the main reason for their coronary tear.
It is difficult to determine how common fibromuscular dysplasia is in the general population, due to a number of reasons. Individuals with mild fibromuscular dysplasia are often asymptomatic and so the disease often goes undetected. Most studies examining the prevalence of fibromuscular dysplasia have looked at specific patient populations in whom individuals may have already suffered from serious consequences of the disease, such as patients with carotid dissection. Since there is a delay in diagnosis of fibromuscular dysplasia among fibromuscular dysplasia patients and since there may be decreased awareness of signs and symptoms of fibromuscular dysplasia among health care providers, it is likely that fibromuscular dysplasia is underdiagnosed and is more common than previously thought.
The majority (more than 90%) of patients with fibromuscular dysplasia are women. However, men, children and the elderly can also have fibromuscular dysplasia, and those who do have a higher risk of complications such as aneurysms (bulging) or dissections (tears) in the arteries. Fibromuscular dysplasia is most common in women between the ages of 40 of and 60. In children with fibromuscular dysplasia, the disease seems to more commonly present with significant narrowing rather than tears of arteries and also seems to involve the arteries to the kidneys and intestines more commonly than the carotid vessels. In the pediatric population, fibromuscular dysplasia affects both boys and girls.
The vascular subtype of Ehlers-Danlos syndrome (type IV) has been associated with the most common type of fibromuscular dysplasia, known as multifocal fibromuscular dysplasia. This syndrome should be suspected in patients with multiple aneurysms and/or tears (dissections) in arteries in addition to the typical angiographic findings of fibromuscular dysplasia. There have been isolated reports of fibromuscular dysplasia associated with other disorders, including Alport syndrome, pheochromocytoma, Marfan syndrome, and moyamoya disease.
There is no cure for fibromuscular dysplasia. Treatments are focused on managing symptoms and complications of fibromuscular dysplasia, including high blood pressure and headaches. Antiplatelet medications, such as aspirin, may be prescribed along with medications to treat high blood pressure (anti hypertensives). Many patients with fibromuscular dysplasia suffer from headaches, and a number of medications are available to help control and prevent headaches. All patients with fibromuscular dysplasia who use tobacco should be encouraged to quit.
Fibromuscular dysplasia classification
Fibromuscular dysplasia is classified as either multifocal or focal fibromuscular dysplasia.
Multifocal fibromuscular dysplasia
- Affects approximately 90% of patients with fibromuscular dysplasia
- Patients have multiple lesions; most often appears as a “string of beads,” which is caused by alternating areas of widening and narrowing along the artery
- Includes medial fibroplasia and perimedial fibroplasia types of fibromuscular dysplasia
- Medial fibroplasia is the most common type of fibromuscular dysplasia in this category
Focal fibromuscular dysplasia
- Affects less than 10% of patients with fibromuscular dysplasia
- Patients have distinct focal lesions or tubular narrowing (stenosis)
- Includes intimal fibroplasia, periarterial fibroplasia, and medial hyperplasia types of fibromuscular dysplasia
- Intimal fibroplasia is the most common type of fibromuscular dysplasia in this category
Are there activity restrictions for patients with fibromuscular dysplasia?
Advice regarding physical activity should always be customized to each individual patient and depends on factors such as vascular location and severity of disease, history of artery dissection or aneurysm, and blood pressure control. In general, experts recommend against contact sports, skydiving, scuba diving, and heavy weight lifting for patients with carotid fibromuscular dysplasia, prior dissection, or aneurysms, because these put added stress on arteries that are already prone to injury. Because of sudden jerking motions of the head, most advise against roller coaster or thrill rides at the amusement park and chiropractic manipulation or deep tissue massage of the neck for patients with carotid artery fibromuscular dysplasia. Although regular aerobic exercise (such as walking or cycling) is an important part of vascular health for fibromuscular dysplasia patients, every patient should discuss exercise plans with a physician who is familiar with fibromuscular dysplasia.
Figure 1. Fibromuscular dysplasia renal artery
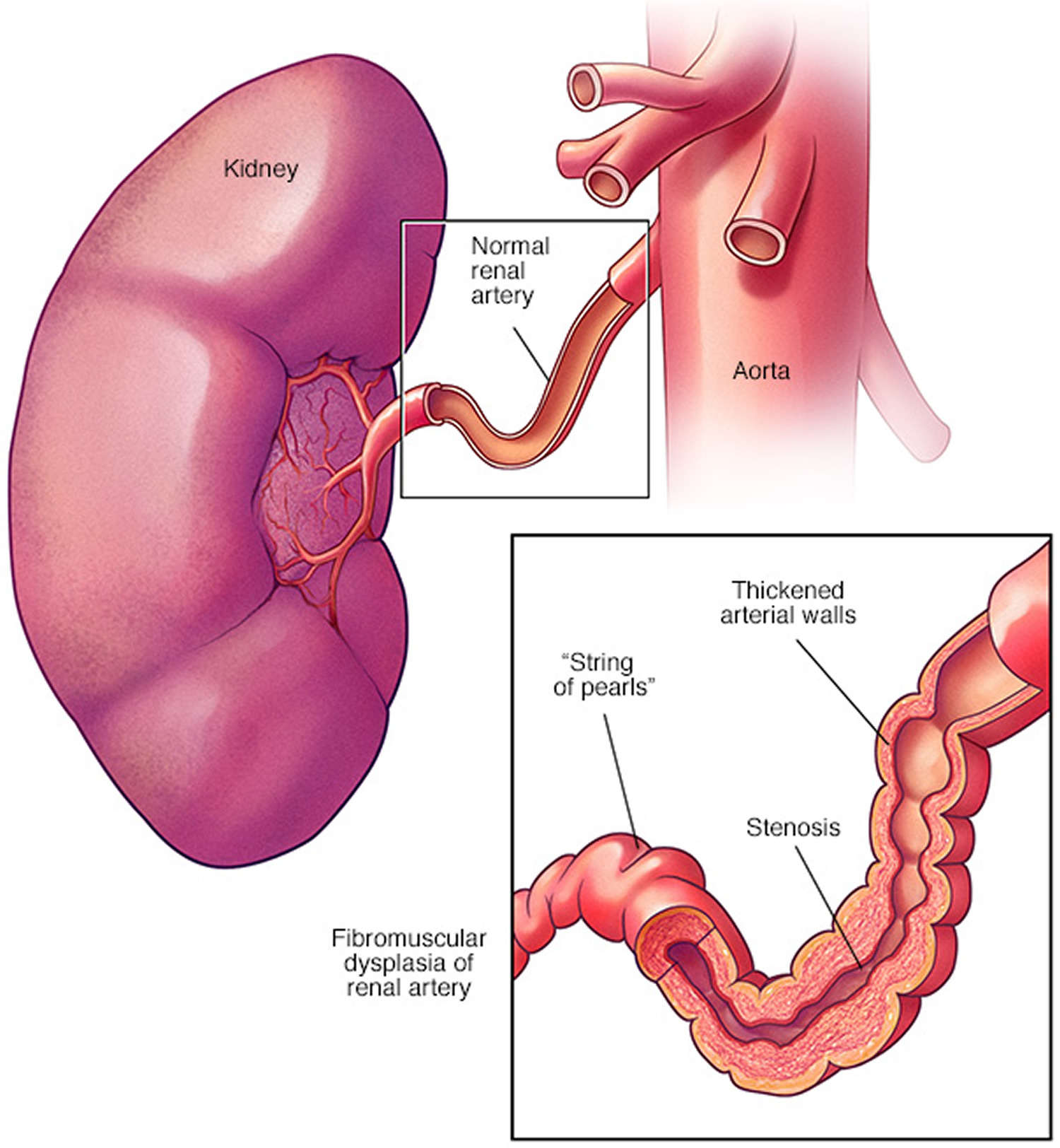 Figure 2. Fibromuscular dysplasia renal artery (CT angiography showing typical “beaded” appearance to the right renal artery as seen in fibromuscular dysplasia. Note that the right kidney is a little smaller than the left and that the left renal artery is normal as are other branches of the abdominal aorta.)
Figure 2. Fibromuscular dysplasia renal artery (CT angiography showing typical “beaded” appearance to the right renal artery as seen in fibromuscular dysplasia. Note that the right kidney is a little smaller than the left and that the left renal artery is normal as are other branches of the abdominal aorta.)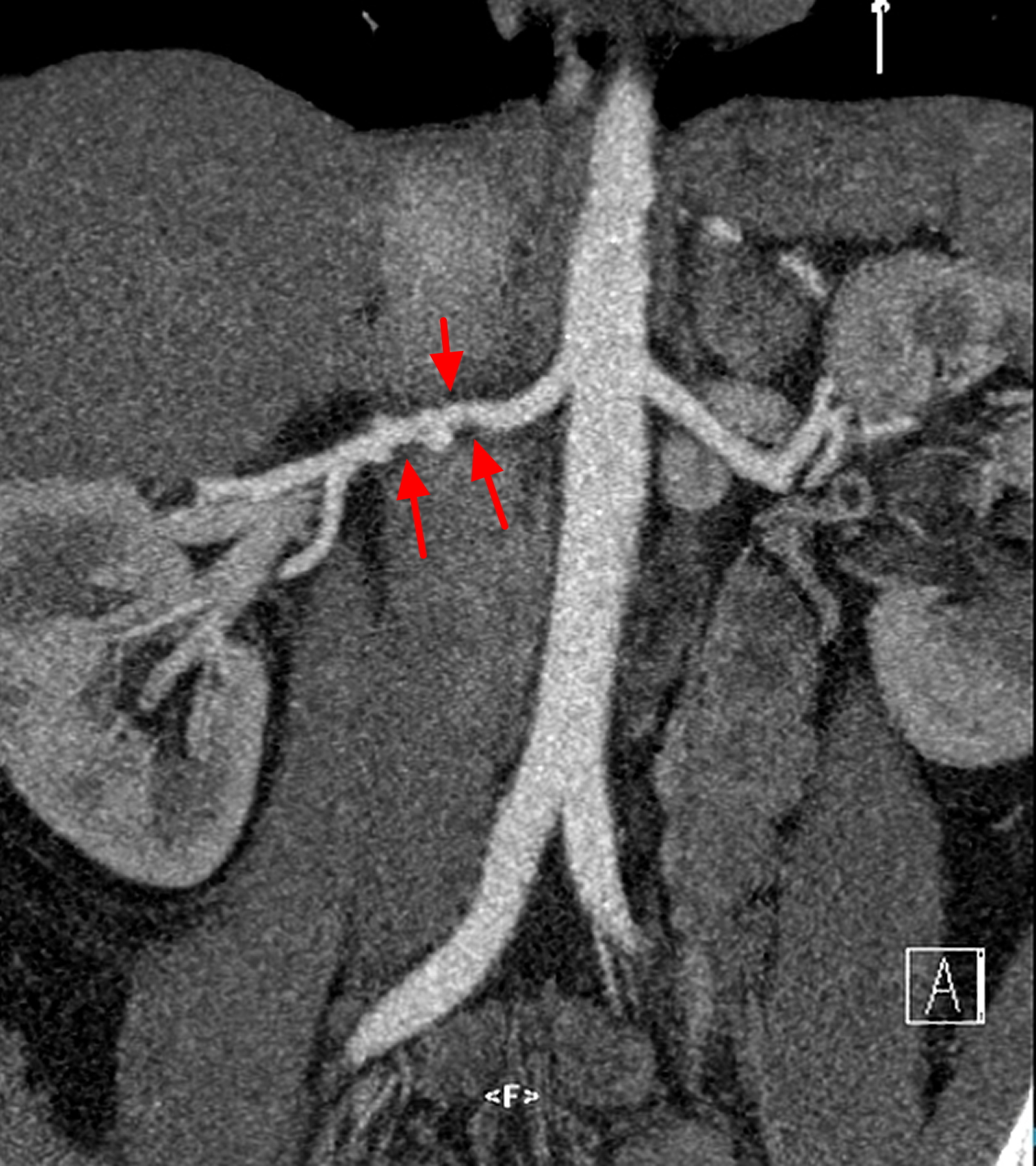
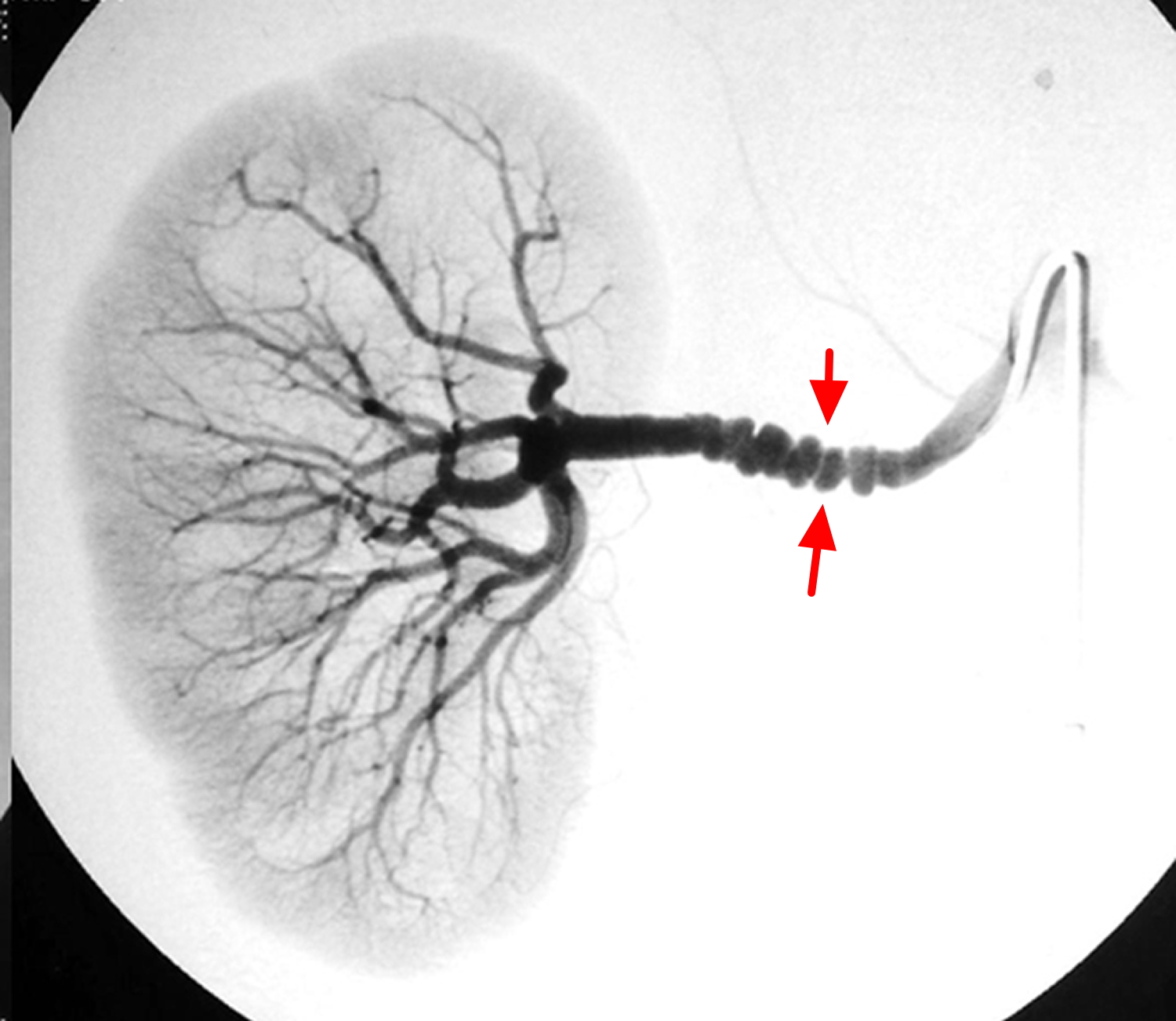
Figure 3. Fibromuscular dysplasia renal artery
Fibromuscular dysplasia complications
Fibromuscular dysplasia can cause a number of complications. These include:
- High blood pressure. A common complication of fibromuscular dysplasia is high blood pressure. The narrowing of the arteries causes higher pressure on your artery walls, which can lead to further artery damage, heart disease or heart failure.
- Dissected artery. Fibromuscular dysplasia can cause tears in the walls of your arteries, causing blood to leak into the artery wall. This process, called arterial dissection or spontaneous coronary artery dissection (SCAD), can limit blood flow to the organ supplied by the injured artery.
- Aneurysms. Fibromuscular dysplasia can weaken the walls of your arteries, creating a bulge called an aneurysm. If an aneurysm ruptures, it can be a life-threatening emergency. An aneurysm can occur in any artery affected by fibromuscular dysplasia.
- Stroke. If you have a dissected artery leading to your brain or if an aneurysm in an artery to your brain ruptures, you can have a stroke. High blood pressure can also increase your risk of a stroke.
Fibromuscular dysplasia life expectancy
Currently there is no cure for fibromuscular dysplasia. Medicines and angioplasty can reduce the risk of initial or recurrent stroke. In rare cases, fibromuscular dysplasia-related aneurysms can burst and bleed into the brain, causing stroke, permanent nerve damage, or death.
There are presently no specific studies or reports on the long-term prognosis and life expectancy of fibromuscular dysplasia adults and in children. The causes, natural history, management and long-term outcomes of fibromuscular dysplasia require further research and evaluation. However there are anecdotal evidence of patients with fibromuscular dysplasia who are in their 80s and 90s.
Fibromuscular dysplasia causes
The cause of fibromuscular dysplasia is not yet known, but several theories have been suggested.
Genetics
About 7-11% of cases of fibromuscular dysplasia are inherited. In addition about a quarter of patients with fibromuscular dysplasia have had a family member with an aneurysm. A number of case reports in the literature have identified the disease in multiple members of the same family including twins. As a result, it is felt that there may be a genetic cause. However, a relative may have different artery involvement, different disease severity, or not develop fibromuscular dysplasia at all. In fact, most individuals with fibromuscular dysplasia do not have a family member who also has the disease. Among some individuals with fibromuscular dysplasia, there is a family history of other vascular problems, such as blood vessel aneurysms.
Hormones
Fibromuscular dysplasia is far more commonly seen in women than in men, resulting in the theory that hormones may play an important role in disease development. However, in small population studies, one’s reproductive history (number of pregnancies and when they occurred) as well as use of birth control pills did not correlate with the development of fibromuscular dysplasia.
Abnormally formed arteries
Other possible causes of fibromuscular dysplasia include abnormal development of the arteries that supply the vessel wall with blood, resulting in inadequate oxygen supply; the anatomic position or movement of the artery within the body; certain medications, and tobacco use. It is possible that many factors contribute to the development of fibromuscular dysplasia. This area requires further research.
Risk factors for fibromuscular dysplasia
Although the cause of fibromuscular dysplasia is unknown, there are several factors that appear to increase the risk of developing the disorder, including:
- Sex. Women have a much greater risk of fibromuscular dysplasia than do men.
- Age. Fibromuscular disorder tends to be diagnosed in people in their early 50s.
- Smoking. People who smoke appear to have an increased risk of developing fibromuscular dysplasia. For those already diagnosed with the disease, smoking is a risk factor for more serious fibromuscular dysplasia.
Fibromuscular dysplasia prevention
Generally, fibromuscular dysplasia isn’t preventable. However, if you smoke, quitting smoking may reduce your likelihood of developing fibromuscular dysplasia.
Fibromuscular dysplasia symptoms
Some people with this disease do not have symptoms or findings on a physical examination. The signs and/or symptoms that a person with fibromuscular dysplasia may experience depend on the arteries affected and whether there is narrowing, tears, or aneurysms within them. Any pain or clinical sign related to fibromuscular dysplasia typically comes from the organ that is supplied by that artery. For example, fibromuscular dysplasia in the kidney arteries may cause high blood pressure. Fibromuscular dysplasia in the carotid arteries may cause headaches or a swooshing sound in the ears (called pulsatile tinnitus). Some patients with fibromuscular dysplasia may have no symptoms at all but are diagnosed with this disease when a physician hears a noise over one of the arteries due to disturbed or turbulent blood flow within the vessel. This noise is known as a bruit.
A person with severe carotid fibromuscular dysplasia causing severe narrowing or a tear in a carotid or vertebral artery may have neurologic symptoms involving the facial nerves (drooping of the eye lid, unequal size of the pupils, for example), stroke or transient ischemic attack. People with carotid fibromuscular dysplasia have a higher risk for aneurysms of the arteries in the brain (intracranial aneurysms). Bleeding in the brain (intracranial hemorrhage) may occur if an aneurysm ruptures, and it is important to identify and treat brain aneurysms early to prevent this.
Fibromuscular dysplasia involving the arteries that supply the intestines, liver and spleen with blood (mesenteric arteries) can result in abdominal pain after eating and unintended weight loss. Fibromuscular dysplasia in the arms and legs can cause limb discomfort with exercise or can lead to unequal blood pressures in the arms.
Fibromuscular dysplasia can affect the arteries of the heart – also called the coronary arteries. Similar to fibromuscular dysplasia in other arteries, fibromuscular dysplasia of the coronary arteries can cause abnormal areas of narrowing (stenosis) or tearing (called dissection). Both stenosis and dissection from fibromuscular dysplasia can lead to reduced blood flow in the coronary arteries, which can cause chest pain or in some people very rarely it can cause heart attack.
Recently, studies have shown that a high percentage of women who were healthy and who have a sudden tearing of a coronary artery called spontaneous coronary artery dissection or “SCAD”, probably have undiagnosed fibromuscular dysplasia. Spontaneous coronary artery dissection was previously thought to be a separate condition to fibromuscular dysplasia, but now we are starting to understand that many people have fibromuscular dysplasia as the main reason for their coronary tear. Like fibromuscular dysplasia in the rest of the body, spontaneous coronary artery dissection is most common in middle aged females. However, it also seems that women are more likely to have a sudden coronary artery dissection within weeks of childbirth.
Kidney signs and symptoms
If the arteries leading to your kidneys (renal arteries) are affected, you may have:
- High blood pressure
- Tissue damage in your kidneys (ischemic renal atrophy)
- Chronic kidney failure, rarely
Brain signs and symptoms
If the arteries leading to your brain (carotid arteries) are affected, you may have:
- Headache
- Dizziness
- Vertigo (room spinning)
- Blurred vision or temporary loss of vision
- Pulsating ringing in your ears (tinnitus)
- Neck pain
- Facial weakness or numbness
- Transient ischemic attack
- Stroke
- Horner’s syndrome
Abdominal signs and symptoms
If the arteries leading to your abdomen (mesenteric arteries) are affected, you may have:
- Abdominal pain after eating
- Unintended weight loss
Arm and leg signs and symptoms
If the arteries leading to your arms or legs (peripheral arteries) are affected, you may have:
- Discomfort when moving your arms, legs, hands or feet
- Cold limbs
- Weakness
- Numbness
- Skin changes in color or appearance
Heart signs and symptoms
If the arteries leading to your heart (coronary arteries) are affected, you may have:
- Chest pain
- Rarely, a heart attack
Fibromuscular dysplasia can cause tears in the walls of your coronary arteries, also called arterial dissection or spontaneous coronary artery dissection. Signs and symptoms of spontaneous coronary artery dissection may include:
- Chest pain
- Shortness of breath
- Sweating
- Nausea
Some people with fibromuscular dysplasia have more than one narrowed artery.
Children with fibromuscular dysplasia
The most prevalent form of fibromuscular dysplasia identified in children and young adults is intimal fibroplasia, which is described by long, irregular or smooth, focal stenosis.
Children often report various non-specific symptoms including headache, insomnia, fatigue and chest or abdominal pain, which may be indicative of hypertension, depending on which artery(s) is affected. A minority of children with hypertension present with neurological symptoms including seizures, transient ischemic attacks, cerebral infarctions (stroke), subarachnoid hemorrhages, and cranial nerve palsies. fibromuscular dysplasia of the head and neck arteries is increasingly recognized as a cause of stroke in children.
If you have any of the other signs or symptoms listed and are concerned about your risk of fibromuscular dysplasia, see your doctor.
Because fibromuscular dysplasia can be hereditary, tell your doctor about your family history of the disease, even before you show any symptoms so that he or she can be alert to changes that might suggest you have fibromuscular dysplasia. There’s currently no genetic test for fibromuscular dysplasia.
Fibromuscular dysplasia diagnosis
Before you’re tested for fibromuscular dysplasia, your doctor may also want to check for atherosclerosis, another condition that can narrow your arteries.
Tests for atherosclerosis usually include:
- A physical exam
- A fasting blood test to check your blood sugar and cholesterol levels
The tests you’ll have to diagnose fibromuscular dysplasia could include:
- Catheter-based angiography. During this commonly used test for fibromuscular dysplasia, a thin tube (catheter) is inserted into one of your arteries and moved until it reaches the location your doctor wants to examine. A tiny amount of dye is injected and X-rays are used to examine the location.
- Doppler ultrasound. Doppler ultrasound can determine if an artery is narrowed by fibromuscular dysplasia. In this noninvasive test, an instrument called a transducer is pressed to your skin to send sound waves into your body. The sound waves bounce off red blood cells and body structures, showing how fast your blood flows and the size and shape of the blood vessels.
- Computerized tomography (CT) angiogram. A CT angiogram allows your doctor to check your arteries to see if they’re narrowed or blocked. You’ll receive an injection of a dye, and the doughnut-shaped CT scanner will be moved to take images of the artery your doctor believes is narrowed.
- Magnetic resonance imaging (MRI). This test allows your doctor to see the soft tissues in your body. During an MRI, you lie on a table inside a long tubelike machine that uses a magnetic field and radio waves to capture images from inside your body. Using the images from the test, your doctor may be able to see the cluster of cells narrowing your artery.
The most common form of fibromuscular dysplasia looks like a “string of pearls” on imaging tests. Other, more-aggressive forms of fibromuscular dysplasia have a smooth appearance.
Once you’ve been diagnosed with fibromuscular dysplasia, your doctor may repeat a Doppler ultrasound exam, a CT angiogram or an MRI angiogram from time to time to see if your condition is getting worse.
Fibromuscular dysplasia treatment
In some cases of fibromuscular dysplasia, an attempt should be made to improve the flow of blood through a severely narrowed vessel. The kind of treatment used for narrowing due to fibromuscular dysplasia depends largely upon which arteries are affected and the presence and severity of the symptoms. In most cases, such procedures are done using balloon angioplasty, a procedure known as percutaneous transluminal angioplasty (PTA). Percutaneous transluminal angioplasty (PTA) is often performed at the same time as an arteriogram.
If an angioplasty is performed, a catheter is extended into the affected artery and a small balloon is inflated in the artery. A metal stent is typically not required to keep the vessel open, but may be needed in some cases, such as for treatment of a tear (dissection) of a blood vessel. If angioplasty is performed, the procedure and recovery period may be longer than an arteriogram done for diagnosis only. Occasionally, traditional open surgery is performed to treat severe narrowing due to fibromuscular dysplasia, particularly those that cannot be treated with angioplasty.
Patients with fibromuscular dysplasia who are found to have a significant aneurysm within the brain or renal arteries may need to undergo surgery even without symptoms. In such cases, it is recommended that the aneurysm be treated to prevent rupture which can be potentially life threatening. The type of treatment for an arterial aneurysm depends on its location and size. Treatment options for aneurysms include traditional open surgery or a less invasive angiogram-based procedure which treats the aneurysm using special vascular coils and/or stents.
The appropriate treatment will vary with each individual and severity, location, and extent of disease. The treatment plan should be discussed in depth with a specialist who is very knowledgeable about fibromuscular dysplasia and its natural history.
Medical procedures and surgery
For otherwise healthy people with fibromuscular dysplasia, repairing the affected artery is often recommended. The procedures to improve blood flow can include:
- Percutaneous transluminal angioplasty (PTA). This procedure is usually preferred over surgery. It is often performed at the same time as a catheter-based angiogram. Once the dye from the angiogram shows the narrowed area of the artery, a wire is threaded to the artery and a catheter with a balloon is inserted in the narrowed area. The balloon is then inflated to open the narrowed part of the artery. Unlike the angioplasty procedures performed on people with heart disease, a stent may not be necessary to keep the artery open.
- Surgical revascularization. If percutaneous transluminal angioplasty (PTA) is not an option, and the narrowing of your arteries is severe, your doctor may recommend more-invasive surgery to repair the narrowed portion of the artery. The type of surgery you’ll need depends on the location of the narrowed artery and how damaged the artery is. The most commonly performed type of revascularization surgery is an aortorenal bypass. This type of procedure involves replacing the artery that leads to the kidney with a vein from the leg.
If your doctor finds serious damage related to fibromuscular dysplasia, such as an aneurysm, he or she may recommend placing a metal mesh tube (stent) inside the weakened part of the artery to help prevent it from rupturing.
Medicines
Treatment with high blood pressure medications is recommended for most people with fibromuscular dysplasia, even if they also have a procedure to correct the condition. These could include medications from several categories:
- Angiotensin-converting enzyme (ACE) inhibitors, such as benazepril (Lotensin), enalapril (Vasotec) or lisinopril (Prinivil, Zestril), stop the narrowing of your blood vessels.
- Angiotensin II receptor blockers. These medications help relax your blood vessels by blocking the action of a natural chemical that narrows blood vessels. Examples of this class of medications include candesartan (Atacand), irbesartan (Avapro), losartan (Cozaar) and valsartan (Diovan).
- Diuretics. These drugs, such as hydrochlorothiazide (Microzide, others), help remove excess fluid from your body and may be used in conjunction with other blood pressure medications.
- Calcium channel blockers, such as amlodipine (Norvasc) or nifedipine (Adalat CC, Afeditab CR, Procardia) and others, help relax your blood vessels.
- Beta blockers, such as metoprolol (Lopressor, Toprol-XL) or atenolol (Tenormin) and others, slow your heartbeat and block adrenaline.
Because some of these drugs can affect the way your kidneys work, your doctor may recommend blood tests and a urine test (urinalysis) to make sure your kidneys work normally once these medications have been started.
Your doctor may also suggest you take a daily aspirin to reduce your risk of stroke. But don’t start taking an aspirin without discussing it with your doctor first.
If you smoke, another part of your treatment plan is to stop smoking. Smoking may make fibromuscular dysplasia worse.
Follow-Up Care
Depending on symptoms and clinical signs (such as high blood pressure or headaches), patients diagnosed with renal artery fibromuscular dysplasia may be advised to undergo an imaging study to test for involvement of the carotid arteries. Those with carotid artery disease may be advised to undergo imaging of the renal arteries. It is recommended that patients with carotid fibromuscular dysplasia undergo an imaging test (such as magnetic resonance angiography) at least once to rule out brain aneurysms. Imaging of other blood vessels (such as the arteries in the arms, legs, and intestines) is typically performed only in those with signs or symptoms of disease.
For fibromuscular dysplasia patients with stable symptoms, periodic clinical follow-up visits will focus on symptom control, blood pressure, and the vascular examination. Imaging studies are performed periodically to assess for progression of disease. Some patients with stable fibromuscular dysplasia will not need to be seen more frequently than yearly. In contrast, follow-up should take place more often for those with severe or worsening symptoms. The type of imaging study used for follow-up of fibromuscular dysplasia (eg, magnetic resonance angiography versus ultrasound) depends on the arteries that are affected, whether the arteries can be well imaged with the ultrasound probe, and the particular imaging expertise of the facility.





{kind=link}