
Contents
What is ischemic heart disease ?
Ischemia is a condition in which the blood flow and thus oxygen is restricted or reduced in a part of the body 1. Cardiac ischemia is the name for decreased blood flow and oxygen to the heart muscle. Heart ischemia often causes chest pain or discomfort known as angina pectoris 1.
Ischemic heart disease is the term given to heart problems caused by narrowed coronary heart arteries 1. When the coronary arteries are narrowed, less blood and oxygen reaches the heart muscle. Ischemic heart disease is also called coronary artery disease or coronary heart disease 2. Although the narrowing can be caused by a blood clot or by constriction of the coronary arteries, most often it is caused by buildup of plaque, called atherosclerosis. When the blood flow to the heart muscle is completely blocked, the heart muscle cells die, which is termed a heart attack or myocardial infarction (MI). Most people with early (less than 50 percent narrowing) coronary heart disease do not experience symptoms or limitation of blood flow 2. However, as the atherosclerosis progresses, especially if left untreated, symptoms may occur. They are most likely to occur during exercise or emotional stress, when the demand for the oxygen carried by the blood increases 2.
Other names for Ischemic Heart Disease 3
- Coronary heart disease
- Atherosclerosis
- Coronary artery disease
- Hardening of the arteries
- Heart disease
- Narrowing of the arteries
Coronary heart disease is a common term for the buildup of plaque in the heart’s arteries that could lead to heart attack 4. But what about coronary heart disease ? Is there a difference ? The answer is no — health professionals frequently use the terms interchangeably. Ischemic heart disease is actually a result of coronary artery disease.
Coronary artery disease develops when the major blood vessels (coronary arteries) that supply your heart with blood, oxygen and nutrients become damaged or diseased. The coronary arteries supply oxygen-rich blood to your heart muscle. The discomfort experienced when the heart muscle is deprived of adequate oxygen is called angina pectoris. This is a clinical syndrome characterized by discomfort in the chest, jaw, shoulder, back, or arms that is typically aggravated by exertion or emotional stress and relieved promptly with rest or by taking nitroglycerin. Angina usually occurs in patients with coronary heart disease, but also can occur in individuals with valvular heart disease, hypertrophic cardiomyopathy, and uncontrolled hypertension. Infrequently, patients with normal coronary arteries may experience angina related to coronary spasm or endothelial dysfunction 5.
Ischemic heart disease is vast, affecting ≈15.5 million Americans ≥20 years of age, with a lower prevalence rate for women (5.0%) compared with men (7.6%) 6. However, after 45 years of age for men and 55 years of age for women, the risk for ischemic heart disease increases similarly in both groups. Although it has been assumed that premenopausal women (usually before 55 years of age) possess cardioprotective effects of estrogen, surprisingly, hormone replacement therapy has not been shown to be effective in protecting against ischemic heart disease in postmenopausal women and in fact may be harmful 7.
The life expectancy for women is greater than that of men, contributing to an increased aged female population with greater ischemic heart disease risk 8. However, it is particularly worrisome that the ischemic heart disease death rate in younger women 35 to 44 years of age continues to increase, while it is decreasing in their male counterparts 9, 10. Although risk factors such as obesity, diabetes mellitus, hypertension, smoking, and metabolic syndrome in younger women are thought to be the primary culprit in these troubling ischemic heart disease trends, lack of recognition of prodromal symptoms and failure to assess for ischemic heart disease in these younger women may contribute to this disturbing trend 9.
Although the annual death rate from ischemic heart disease between 2000 and 2010 declined 39.2% 10, disparities exist and women have notably poorer outcomes than men after the initial ischemic heart disease presentation. Pooled data from the National Heart, Lung, and Blood Institute–sponsored cohort studies (1986–2007) indicate substantial disparities between men and women: 1 year after acute myocardial infarction (heart attack), 19% of men and 26% of women ≥45 years of age will die 11. Within 5 years after a first heart attack, 36% of men and 47% of women will die. Higher in-hospital mortality rates have also been reported for women with stable angina and acute coronary syndrome compared with men 12, 13. This disparity in deaths after a first heart attack preferentially affects older women because women tend to present with ischemic heart disease at older ages, but as stated earlier, ischemic heart disease death rates in younger women continue to escalate 6.
Additionally, women have more complications after having a first heart attack such as increased bleeding risk after a first heart attack treated with percutaneous coronary intervention (2.4% versus 1.2% for men) 14. At 45 to 64 years of age, 15% of men and 22% of women have a recurrent heart attack or fatal cardiovascular event within 5 years. Furthermore, 8% of men and 18% of women develop heart failure within 5 years of a first heart attack. As women and men age, the rates of a subsequent heart attack and heart failure equalize 10.
Sex differences also exist with acute coronary syndrome symptoms (unstable angina or heart attack). A greater proportion of women than men with anginal symptoms and acute coronary syndrome have nonobstructive ischemic heart disease 15; however, more women than men have adverse outcomes. Women with nonobstructive ischemic heart disease and stable angina have greater major adverse event rates than men with nonobstructive ischemic heart disease 16. Furthermore, data from the Women’s Ischemia Syndrome Evaluation study showed 5-year annualized event rates for cardiovascular events of 16% and 7.9% in symptomatic women with nonobstructive ischemic heart disease and normal coronary arteries, respectively 17. Adverse outcomes continue over the long term for women in the WISE cohort with cardiovascular death or heart attack at 10 years in 6.7%, 12.8%, and 25.9% of women with no, nonobstructive, and obstructive ischemic heart disease, respectively 18.
Women with suspected acute coronary syndrome are less likely to be diagnosed with acute coronary syndrome, which has often been attributed to atypical symptoms and less reliable ECG findings 19. However, a recent investigation reported that the use of a high-sensitivity troponin assay with sex-specific cutoffs increased diagnostic accuracy for women. In a study of 1126 patients with acute coronary syndrome (46% women), the high-sensitivity troponin I assay increased the diagnosis of heart attack in women but had a minimal effect in men compared with contemporary assays with a single diagnostic threshold 19, 20. Additional studies are needed to determine whether the use of a high-sensitivity troponin I assay with sex-specific diagnostic thresholds will improve outcomes for women with acute coronary syndrome.
Finally, women with documented ischemic heart disease and those who have experienced a heart attack have poorer self-reported health-related quality of life and depression compared with men 21. In the WISE study, depression, symptom severity, and history of depression treatment were associated with a greater risk of mortality and hospitalization 22.
What is silent ischemia ?
Many Americans may have ischemic episodes without knowing it. These people have ischemia without pain — silent ischemia 1. As many as 3 to 4 million Americans may have silent ischemia, or ischemia without pain, or a heart attack without prior warning. People with angina may also have undiagnosed episodes of silent ischemia. They may have a heart attack with no prior warning. People with angina also may have undiagnosed episodes of silent ischemia. In addition, people who have had previous heart attacks or those with diabetes are especially at risk for developing silent ischemia 1.
Having an exercise stress test or wearing a Holter monitor – a battery-operated portable tape recording that measures and records your electrocardiogram (ECG) continuously, usually for 24-48 hours – are two tests often used to diagnose this problem. Other tests also may be used – see ischemic heart disease diagnosis section below.
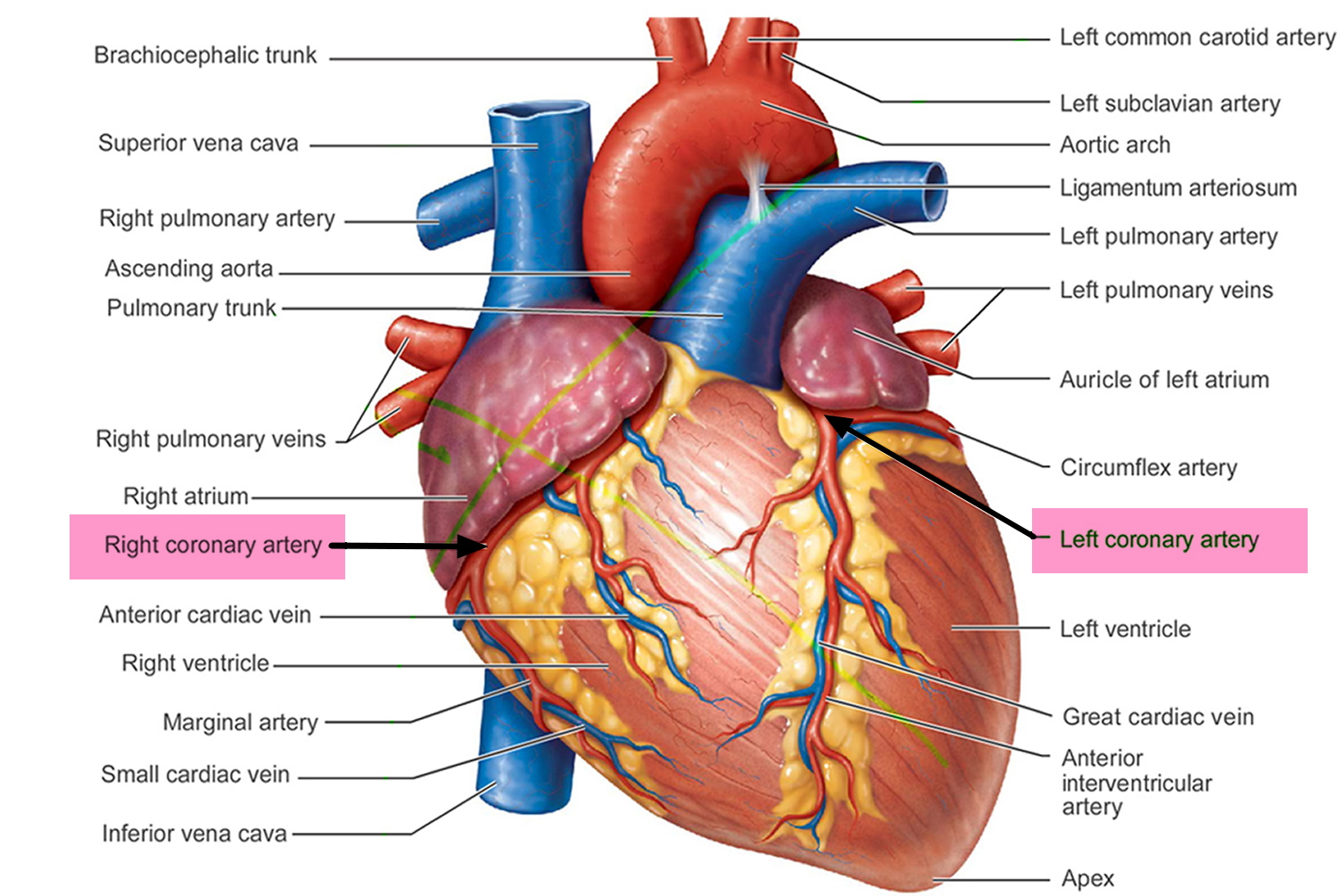
Figure 1. Coronary Arteries supplying blood, oxygen & nutrients to your heart
Coronary heart disease or coronary artery disease is a condition in which a waxy substance called plaque builds up inside of the coronary arteries 23.
Plaque is made up of fat, cholesterol, calcium, and other substances found in the blood. Over time, plaque hardens and narrows your arteries. This limits the flow of oxygen-rich blood to your organs and other parts of your body.
When plaque builds up in the arteries, the condition is called atherosclerosis. Atherosclerosis can lead to serious problems, including heart attack, stroke, or even death.
Atherosclerosis is a disease in which plaque builds up inside your arteries. The buildup of plaque occurs over many years.
Atherosclerosis plaque narrows the coronary arteries and reduces blood flow to your heart muscle. Plaque narrows and stiffens the coronary arteries. This reduces the flow of oxygen-rich blood to the heart muscle, causing chest pain.
Plaque buildup also makes it more likely that blood clots will form in your arteries. Blood clots can partially or completely block blood flow, which can cause a heart attack.
- If blood flow to your heart muscle is reduced or blocked, you may have angina (chest pain or discomfort) or a heart attack.
Plaque also can form in the heart’s smallest arteries. This disease is called coronary microvascular disease. In coronary microvascular disease, plaque doesn’t cause blockages in the arteries as it does in coronary heart disease.
Coronary artery disease can lead to:
- Chest pain (angina). When your coronary arteries narrow, your heart may not receive enough blood when demand is greatest — particularly during physical activity. This can cause chest pain (angina) or shortness of breath.
- Heart attack. If a cholesterol plaque ruptures and a blood clot forms, complete blockage of your heart artery may trigger a heart attack. The lack of blood flow to your heart may damage your heart muscle. The amount of damage depends in part on how quickly you receive treatment.
- Heart failure. If some areas of your heart are chronically deprived of oxygen and nutrients because of reduced blood flow, or if your heart has been damaged by a heart attack, your heart may become too weak to pump enough blood to meet your body’s needs. This condition is known as heart failure.
- Abnormal heart rhythm (arrhythmia). Inadequate blood supply to the heart or damage to heart tissue can interfere with your heart’s electrical impulses, causing abnormal heart rhythms.
Figure 2. Atherosclerosis plaque
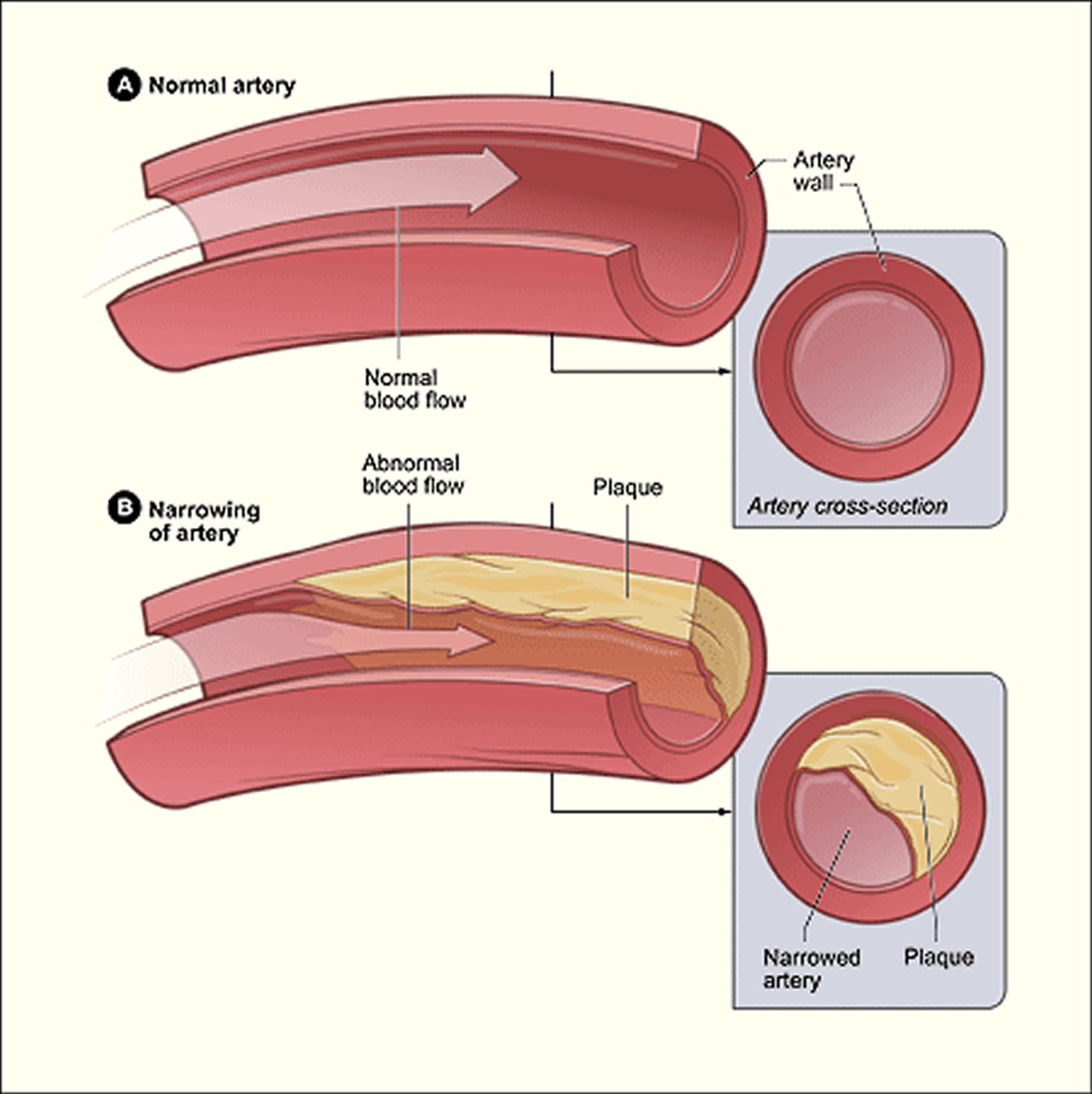
Figure 3. Atherosclerosis blocking the coronary artery in your heart
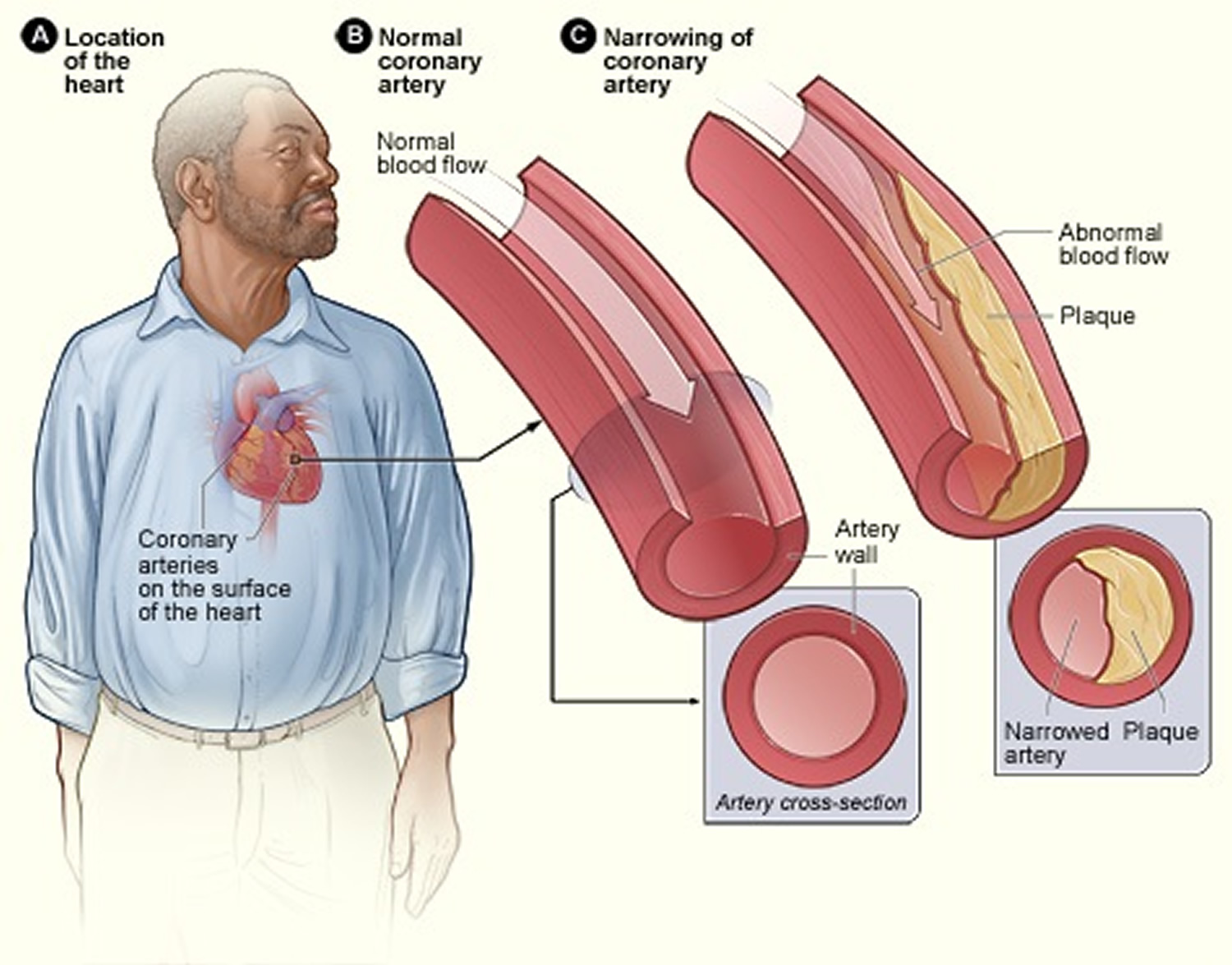
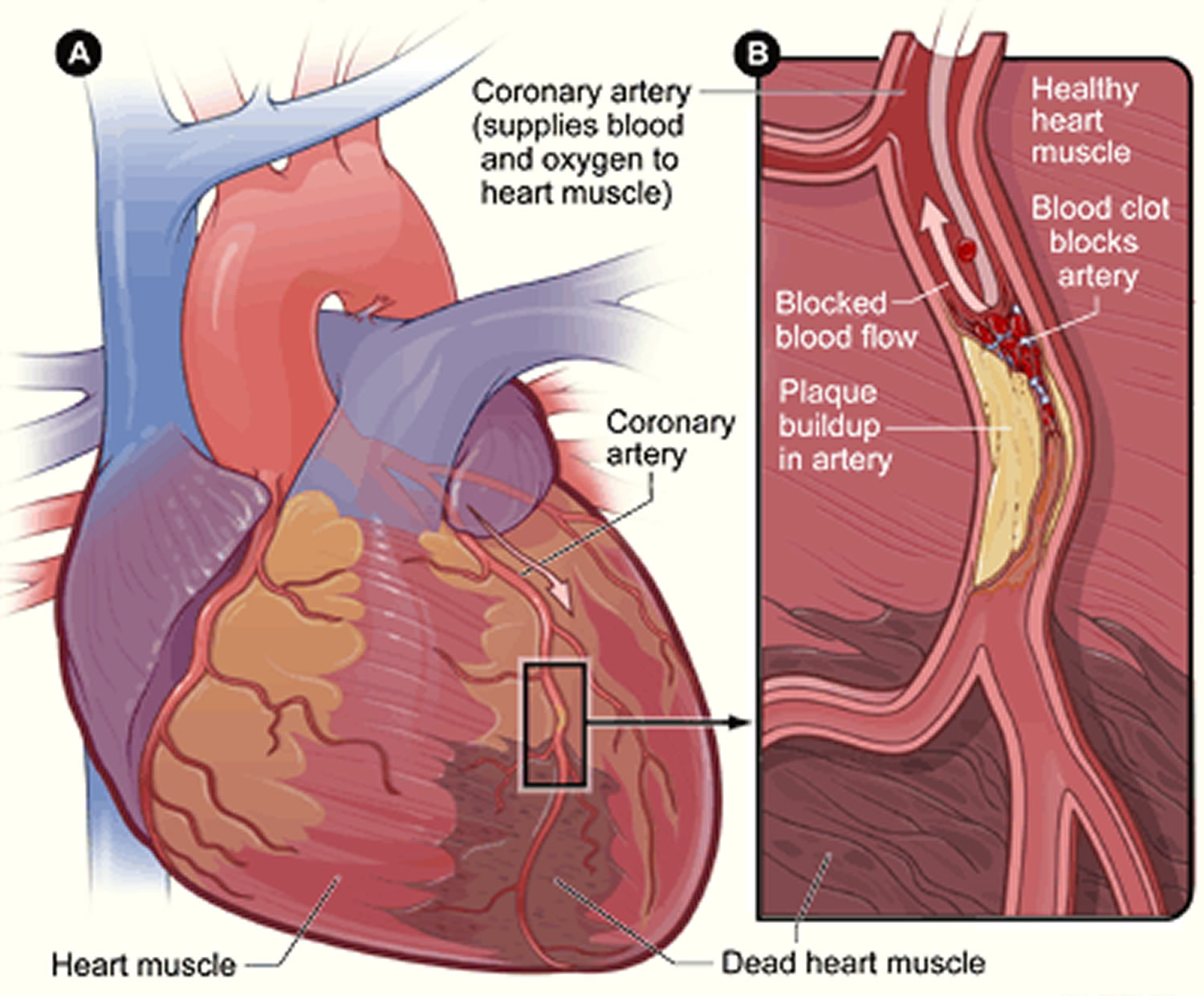
Figure 4. Heart With Muscle Damage and a Blocked Left Coronary Artery
When plaque builds up in the arteries, the condition is called atherosclerosis. Because coronary artery disease often develops over decades, you might not notice a problem until you have a significant blockage or a heart attack.
Eventually, an area of plaque can rupture (break open) inside of an artery. This causes a blood clot to form on the plaque’s surface. If the clot becomes large enough, it can mostly or completely block blood flow through a coronary artery.
If the blockage isn’t treated quickly, the portion of heart muscle fed by the artery begins to die. Healthy heart tissue is replaced with scar tissue. This heart damage may not be obvious, or it may cause severe or long-lasting problems.
A heart attack happens if the flow of oxygen-rich blood to a section of heart muscle suddenly becomes blocked and the heart can’t get oxygen. Most heart attacks occur as a result of coronary heart disease 23.
Over time, coronary heart disease can weaken the heart muscle and lead to heart failure and heart arrhythmias. Heart failure is a condition in which your heart can’t pump enough blood to meet your body’s needs. Heart arrhythmias are problems with the rate or rhythm of the heartbeat.
Coronary artery disease begins in childhood, so that by the teenage years, there is evidence that plaques that will stay with us for life are formed in most people 4. But there’s plenty you can do to prevent and treat coronary artery disease. A healthy lifestyle can make a big impact. The traditional risk factors for coronary artery disease are high LDL cholesterol, low HDL cholesterol, high blood pressure, family history, diabetes, smoking, being post-menopausal for women and being older than 45 for men. Obesity may also be a risk factor.
Who is at Risk for Ischemic Heart Disease ?
In the United States, coronary heart disease is a leading cause of death for both men and women. Each year, about 370,000 Americans die from coronary heart disease 26.
Certain traits, conditions, or habits may raise your risk for coronary heart disease. The more risk factors you have, the more likely you are to develop the disease.
You can control many risk factors, which may help prevent or delay coronary heart disease.
Major Risk Factors
- Unhealthy blood cholesterol levels. This includes high LDL cholesterol (sometimes called “bad” cholesterol) and low HDL cholesterol (sometimes called “good” cholesterol).
- High blood pressure. Blood pressure is considered high if it stays at or above 140/90 mmHg over time. If you have diabetes or chronic kidney disease, high blood pressure is defined as 130/80 mmHg or higher. (The mmHg is millimeters of mercury—the units used to measure blood pressure.)
- Smoking. Smoking can damage and tighten blood vessels, lead to unhealthy cholesterol levels, and raise blood pressure. Smoking also can limit how much oxygen reaches the body’s tissues.
- Insulin resistance. This condition occurs if the body can’t use its own insulin properly. Insulin is a hormone that helps move blood sugar into cells where it’s used for energy. Insulin resistance may lead to diabetes.
- Diabetes. With this disease, the body’s blood sugar level is too high because the body doesn’t make enough insulin or doesn’t use its insulin properly.
Overweight or obesity. The terms “overweight” and “obesity” refer to body weight that’s greater than what is considered healthy for a certain height. - Metabolic syndrome. Metabolic syndrome is the name for a group of risk factors that raises your risk for coronary heart disease and other health problems, such as diabetes and stroke.
- Lack of physical activity. Being physically inactive can worsen other risk factors for coronary heart disease, such as unhealthy blood cholesterol levels, high blood pressure, diabetes, and overweight or obesity.
- Unhealthy diet. An unhealthy diet can raise your risk for coronary heart disease. Foods that are high in saturated and trans fats, cholesterol, sodium, and sugar can worsen other risk factors for coronary heart disease.
- Older age. Genetic or lifestyle factors cause plaque to build up in your arteries as you age. In men, the risk for coronary heart disease increases starting at age 45. In women, the risk for coronary heart disease increases starting at age 55.
- A family history of early coronary heart disease is a risk factor for developing coronary heart disease, specifically if a father or brother is diagnosed before age 55, or a mother or sister is diagnosed before age 65.
Although older age and a family history of early heart disease are risk factors, it doesn’t mean that you’ll develop coronary heart disease if you have one or both. Controlling other risk factors often can lessen genetic influences and help prevent coronary heart disease, even in older adults.
Emerging Risk Factors
Researchers continue to study other possible risk factors for coronary heart disease.
High levels of a protein called C-reactive protein (CRP) in the blood may raise the risk of coronary heart disease and heart attack. High levels of CRP are a sign of inflammation in the body.
Inflammation is the body’s response to injury or infection. Damage to the arteries’ inner walls may trigger inflammation and help plaque grow.
Research is under way to find out whether reducing inflammation and lowering CRP levels also can reduce the risk of coronary heart disease and heart attack.
High levels of triglycerides in the blood also may raise the risk of coronary heart disease, especially in women. Triglycerides are a type of fat.
Other Risks Related to Ischemic Heart Disease
Other conditions and factors also may contribute to coronary heart disease, including:
- Sleep apnea. Sleep apnea is a common disorder in which you have one or more pauses in breathing or shallow breaths while you sleep. Untreated sleep apnea can increase your risk for high blood pressure, diabetes, and even a heart attack or stroke.
- Stress. Research shows that the most commonly reported “trigger” for a heart attack is an emotionally upsetting event, especially one involving anger.
- Alcohol. Heavy drinking can damage the heart muscle and worsen other coronary heart disease risk factors. Men should have no more than two drinks containing alcohol a day. Women should have no more than one drink containing alcohol a day.
- Preeclampsia. This condition can occur during pregnancy. The two main signs of preeclampsia are a rise in blood pressure and excess protein in the urine. Preeclampsia is linked to an increased lifetime risk of heart disease, including coronary heart disease, heart attack, heart failure, and high blood pressure.
Following a healthy lifestyle can help you and your children prevent or control many coronary heart disease risk factors.
Because many lifestyle habits begin during childhood, parents and families should encourage their children to make heart healthy choices. For example, you and your children can lower your risk of coronary heart disease if you maintain a healthy weight, follow a healthy diet, do physical activity regularly, and don’t smoke.
If you already have CHD, lifestyle changes can help you control your risk factors. This may prevent coronary heart disease from worsening. Even if you’re in your seventies or eighties, a healthy lifestyle can lower your risk of dying from coronary heart disease.
If lifestyle changes aren’t enough, your doctor may recommend other treatments to help control your risk factors.
Your doctor can help you find out whether you have coronary heart disease risk factors. He or she also can help you create a plan for lowering your risk of CHD, heart attack, and other heart problems.
If you have children, talk with their doctors about their heart health and whether they have coronary heart disease risk factors. If they do, ask your doctor to help create a treatment plan to reduce or control these risk factors.
What causes ischemic heart disease
Coronary artery disease is preventable 4. Cigarette and tobacco smoke, high blood cholesterol, high blood pressure, physical inactivity, obesity and diabetes are the six major independent risk factors for coronary heart disease that you can modify or control. Living a healthy lifestyle that incorporates good nutrition, weight management and getting plenty of physical activity can play a big role in avoiding coronary artery disease.
Research suggests that coronary heart disease starts when certain factors damage the inner layers of the coronary arteries. These factors include:
- Smoking
- High levels of certain fats and cholesterol in the blood
- High blood pressure
- High levels of sugar in the blood due to insulin resistance or diabetes
- Blood vessel inflammation
Plaque might begin to build up where the arteries are damaged. The buildup of plaque in the coronary arteries may start in childhood.
Over time, plaque can harden or rupture (break open). Hardened plaque narrows the coronary arteries and reduces the flow of oxygen-rich blood to the heart. This can cause angina (chest pain or discomfort).
If the plaque ruptures, blood cell fragments called platelets stick to the site of the injury. They may clump together to form blood clots.
Blood clots can further narrow the coronary arteries and worsen angina. If a clot becomes large enough, it can mostly or completely block a coronary artery and cause a heart attack.
Major Risk Factor of Ischemic Heart Disease 4
Smoking
Smokers’ risk of developing coronary heart disease is much higher than that of nonsmokers. Cigarette smoking is a powerful independent risk factor for sudden cardiac death in patients with coronary heart disease. Cigarette smoking also acts with other risk factors to greatly increase the risk for coronary heart disease. Exposure to other people’s smoke increases the risk of heart disease even for nonsmokers.
Cigarette smoking is the most important preventable cause of premature death in the United States. It accounts for more than 440,000 of the more than 2.4 million annual deaths. Cigarette smokers have a higher risk of developing several chronic disorders. These include fatty buildups in arteries, several types of cancer and chronic obstructive pulmonary disease (lung problems). Atherosclerosis (buildup of fatty substances in the arteries) is a chief contributor to the high number of deaths from smoking. Many studies detail the evidence that cigarette smoking is a major cause of coronary heart disease, which leads to heart attack.
The more you smoke, the greater your risk of heart attack. The benefits of quitting smoking occur no matter how long or how much you’ve smoked. Heart disease risk associated with smoking begins to decrease soon after you quit, and for many people it continues to decrease over time.
Most people who smoke start when they’re teens. Parents can help prevent their children from smoking by not smoking themselves. Talk with your child about the health dangers of smoking and ways to overcome peer pressure to smoke.
High blood cholesterol
As blood cholesterol rises, so does risk of coronary heart disease. When other risk factors (such as high blood pressure and tobacco smoke) are present, this risk increases even more. A person’s cholesterol level is also affected by age, sex, heredity and diet. Here’s the lowdown on:
- Total Cholesterol: Your total cholesterol score is calculated using the following equation: HDL + LDL + 20 percent of your triglyceride level.
- Low-density-lipoprotein (LDL) cholesterol = “bad” cholesterol
A low LDL cholesterol level is considered good for your heart health. However, your LDL number should no longer be the main factor in guiding treatment to prevent heart attack and stroke, according to the latest guidelines from the American Heart Association. For patients taking statins, the guidelines say they no longer need to get LDL cholesterol levels down to a specific target number. Lifestyle factors, such as a diet high in saturated and trans fats can raise LDL cholesterol.
- High-density-lipoprotein (HDL) cholesterol = “good” cholesterol
With HDL (good) cholesterol, higher levels are typically better. Low HDL cholesterol puts you at higher risk for heart disease. People with high blood triglycerides usually also have lower HDL cholesterol. Genetic factors, type 2 diabetes, smoking, being overweight and being sedentary can all result in lower HDL cholesterol.
Many factors affect your cholesterol levels. For example, after menopause, women’s LDL cholesterol levels tend to rise, and their HDL cholesterol levels tend to fall 27. Other factors—such as age, gender, diet, and physical activity—also affect your cholesterol levels.
Healthy levels of both LDL and HDL cholesterol will prevent plaque from building up in your arteries. Routine blood tests can show whether your blood cholesterol levels are healthy. Talk with your doctor about having your cholesterol tested and what the results mean.
Children also can have unhealthy cholesterol levels, especially if they’re overweight or their parents have high blood cholesterol 27. Talk with your child’s doctor about testing your child’ cholesterol levels.
To learn more about high blood cholesterol and how to manage the condition, go to the What is Cholesterol and Is there good and bad cholesterol article.
- Triglycerides
Triglyceride is the most common type of fat in the body. Normal triglyceride levels vary by age and sex. A high triglyceride level combined with low HDL cholesterol or high LDL cholesterol is associated with atherosclerosis, the buildup of fatty deposits in artery walls that increases the risk for heart attack and stroke. Some studies suggest that a high level of triglycerides in the blood may raise the risk of coronary heart disease, especially in women 27.
High blood pressure
Blood pressure is the force of blood pushing against the walls of your arteries as your heart pumps blood. If this pressure rises and stays high over time, it can damage your heart and lead to plaque buildup. High blood pressure also increases the heart’s workload, causing the heart muscle to thicken and become stiffer. This stiffening of the heart muscle is not normal, and causes the heart not to work properly. It also increases your risk of stroke, heart attack, kidney failure and congestive heart failure. When high blood pressure exists with obesity, smoking, high blood cholesterol levels or diabetes, the risk of heart attack or stroke increases even more.
All levels above 120/80 mmHg raise your risk of coronary heart disease 27. This risk grows as blood pressure levels rise. Only one of the two blood pressure numbers has to be above normal to put you at greater risk of coronary heart disease and heart attack 27.
Most adults should have their blood pressure checked at least once a year. If you have high blood pressure, you’ll likely need to be checked more often. Talk with your doctor about how often you should have your blood pressure checked.
Children also can develop high blood pressure, especially if they’re overweight. Your child’s doctor should check your child’s blood pressure at each routine checkup.
Both children and adults are more likely to develop high blood pressure if they’re overweight or have diabetes.
Physical inactivity
Inactive people are nearly twice as likely to develop coronary heart disease as those who are active 27. A lack of physical activity can worsen other coronary heart disease risk factors, such as high blood cholesterol and triglyceride levels, high blood pressure, diabetes and prediabetes, and overweight and obesity.
It’s important for children and adults to make physical activity part of their daily routines. One reason many Americans aren’t active enough is because of hours spent in front of TVs and computers doing work, schoolwork, and leisure activities.
Some experts advise that children and teens should reduce screen time because it limits time for physical activity. They recommend that children aged 2 and older should spend no more than 2 hours a day watching TV or using a computer (except for school work).
Being physically active is one of the most important things you can do to keep your heart healthy. The good news is that even modest amounts of physical activity are good for your health. The more active you are, the more you will benefit.
For more information, go to Healthy Exercise and The Truth About Exercise articles.
An inactive lifestyle is a risk factor for coronary heart disease. Regular, moderate-to-vigorous physical activity helps reduce the risk of heart and blood vessel disease. Even moderate-intensity activities help if done regularly and long term. Physical activity can help control blood cholesterol, diabetes and obesity, as well as help lower blood pressure in some people.
Obesity and overweight
The terms “overweight” and “obesity” refer to body weight that’s greater than what is considered healthy for a certain height. More than two-thirds of American adults are overweight, and almost one-third of these adults are obese.
The most useful measure of overweight and obesity is body mass index (BMI).
You can calculate your BMI by dividing your weight in kilograms by your height in meters squared (kg/m2). You can also use an online BMI calculator or BMI table.
To find out about your body mass index (BMI), you can use a FREE online BMI calculators from the Centers for Disease Control and Prevention (CDC) :
- Adults 28
For children and adolescents (younger than 20 years of age), overweight and obesity are based on the Centers for Disease Control and Prevention’s (CDC’s) BMI-for-age growth charts, which are available at 29.
The CDC has a BMI percentile calculator for children and teens at 30.
- Children 31
Body Mass Index for Men and Women Adults
The body mass index is an attempt to quantify the amount of tissue mass (muscle, fat, and bone) in an individual, and then categorize that person as underweight, normal weight, overweight, or obese based on that value. Commonly accepted body mass index ranges are:
A) Underweight: under 18.5 kg/m2,
B) Normal (Healthy BMI) weight: 18.5 to 25 kg/m2,
C) Overweight: 25 to 30 kg/m2,
D) Obese: over 30 to 39.9 kg/m2.
E) Severely Obese: over 40 kg/m2.
Waist size matters, too. In people who are not overweight, waist size may be an even more telling warning sign of increased health risks than BMI 32. An expert panel convened by the National Institutes of Health identified these useful benchmarks: Men should aim for a waist size below 40 inches (102 cm) and women should aim for a waist size below 35 inches (88 cm) 33.
Overweight is defined differently for children and teens than it is for adults. Children are still growing, and boys and girls mature at different rates. Thus, BMIs for children and teens compare their heights and weights against growth charts that take age and gender into account. This is called BMI-for-age percentile.
Being overweight or obese can raise your risk of coronary heart disease and heart attack. This is mainly because overweight and obesity are linked to other coronary heart disease risk factors, such as high blood cholesterol and triglyceride levels, high blood pressure, and diabetes.
For more information, go to Obesity and What is Body Mass Index and Waist Hip Ratio articles.
People who have excess body fat — especially if a lot of it is at the waist — are more likely to develop heart disease and stroke even if they have no other risk factors. Overweight and obese adults with risk factors for cardiovascular disease such as high blood pressure, high cholesterol, or high blood sugar can make lifestyle changes to lose weight and produce clinically meaningful reductions in triglycerides, blood glucose, HbA1c, and risk of developing Type 2 diabetes. Many people may have difficulty losing weight. But a sustained weight loss of 3 to 5% body weight may lead to clinically meaningful reductions in some risk factors, larger weight losses can benefit blood pressure, cholesterol, and blood glucose.
Diabetes and Prediabetes
Diabetes is a disease in which the body’s blood sugar level is too high. The two types of diabetes are type 1 and type 2.
In type 1 diabetes, the body’s blood sugar level is high because the body doesn’t make enough insulin. Insulin is a hormone that helps move blood sugar into cells, where it’s used for energy. In type 2 diabetes, the body’s blood sugar level is high mainly because the body doesn’t use its insulin properly.
Over time, a high blood sugar level can lead to increased plaque buildup in your arteries. Having diabetes doubles your risk of coronary heart disease.
Prediabetes is a condition in which your blood sugar level is higher than normal, but not as high as it is in diabetes. If you have prediabetes and don’t take steps to manage it, you’ll likely develop type 2 diabetes within 10 years. You’re also at higher risk of coronary heart disease.
Being overweight or obese raises your risk of type 2 diabetes. With modest weight loss and moderate physical activity, people who have prediabetes may be able to delay or prevent type 2 diabetes. They also may be able to lower their risk of coronary heart disease and heart attack. Weight loss and physical activity also can help control diabetes.
Even children can develop type 2 diabetes. Most children who have type 2 diabetes are overweight.
Type 2 diabetes develops over time and sometimes has no symptoms. Go to your doctor or local clinic to have your blood sugar levels tested regularly to check for diabetes and prediabetes.
Diabetes seriously increases your risk of developing cardiovascular disease. Even when glucose levels are under control, diabetes increases the risk of heart disease and stroke, but the risks are even greater if blood sugar is not well controlled. At least 68% of people >65 years of age with diabetes die of some form of heart disease and 16% die of stroke. If you have diabetes, it’s extremely important to work with your healthcare provider to manage it and control any other risk factors you can. Persons with diabetes who are obese or overweight should make lifestyle changes (e.g., eat better, get regular physical activity, lose weight ) to help manage blood sugar.
Stress
Individual response to stress may be a contributing factor. Some scientists have noted a relationship between coronary heart disease risk and stress in a person’s life, their health behaviors and socioeconomic status.
Stress and anxiety also can trigger your arteries to tighten. This can raise your blood pressure and your risk of heart attack.
The most commonly reported trigger for a heart attack is an emotionally upsetting event, especially one involving anger. Stress also may indirectly raise your risk of coronary heart disease if it makes you more likely to start smoking or smoke more than they otherwise would or overeat foods high in fat and sugar.
Alcohol
Drinking too much alcohol can raise blood pressure, increase risk of cardiomyopathy and stroke, cancer and other diseases. It can contribute to high triglycerides, and produce irregular heartbeats. Excessive alcohol consumption contributes to obesity, alcoholism, suicide and accidents. However, there is a cardioprotective effect of moderate alcohol consumption. If you drink, limit your alcohol consumption to no more than two drinks per day for men and no more than one drink per day for women. The National Institute on Alcohol Abuse and Alcoholism defines one drink as 1-1/2 fluid ounces (fl oz) of 80-proof spirits (such as bourbon, Scotch, vodka, gin, etc.), 5 fl oz of wine or 12 fl oz of regular beer. It’s not recommended that nondrinkers start using alcohol or that drinkers increase the amount they drink.
Diet and Nutrition
An unhealthy diet can raise your risk of coronary heart disease. For example, foods that are high in saturated and trans fats and cholesterol raise LDL cholesterol. Thus, you should try to limit these foods.
It’s also important to limit foods that are high in sodium (salt) and added sugars. A high-salt diet can raise your risk of high blood pressure.
Added sugars will give you extra calories without nutrients like vitamins and minerals. This can cause you to gain weight, which raises your risk of coronary heart disease. Added sugars are found in many desserts, canned fruits packed in syrup, fruit drinks, and nondiet sodas.
A healthy diet is one of the best weapons you have to fight cardiovascular disease. The food you eat (and the amount) can affect other controllable risk factors: cholesterol, blood pressure, diabetes and overweight. Choose nutrient-rich foods — which have vitamins, minerals, fiber and other nutrients but are lower in calories — over nutrient-poor foods. Choose a diet that emphasizes intake of vegetables, fruits, and whole grains; includes low-fat dairy products, poultry, fish, legumes, nontropical vegetable oils, and nuts; and limits intake of sweets, sugar-sweetened beverages, and red meats. And to maintain a healthy weight, coordinate your diet with your physical activity level so you’re using up as many calories as you take in.
Homocysteine
Homocysteine is an amino acid your body uses to make protein and to build and maintain tissue. But high levels of homocysteine may increase your risk of coronary artery disease.
Other risk factors you can’t change
The risk factors on this list are ones you’re born with and cannot be changed. The more of these risk factors you have, the greater your chance of developing coronary heart disease. Since you can’t do anything about these risk factors, it’s even more important for you to manage the risk factors that can be changed.
Increasing Age
In men, the risk for coronary heart disease increases starting around age 45. In women, the risk for coronary heart disease increases starting around age 55. Most people have some plaque buildup in their heart arteries by the time they’re in their 70s. However, only about 25 percent of those people have chest pain, heart attacks, or other signs of coronary heart disease.
The majority of people who die of coronary heart disease are 65 or older. At older ages, women who have heart attacks are more likely than men are to die from them within a few weeks.
Male Sex (Gender)
Some risk factors may affect coronary heart disease risk differently in women than in men. For example, estrogen provides women some protection against coronary heart disease, whereas diabetes raises the risk of coronary heart disease more in women than in men.
Also, some risk factors for heart disease only affect women, such as preeclampsia, a condition that can develop during pregnancy. Preeclampsia is linked to an increased lifetime risk of heart disease, including coronary heart disease, heart attack, heart failure, and high blood pressure. Likewise, having heart disease risk factors, such as diabetes or obesity, increases a woman’s risk of preeclampsia.
Men have a greater risk of heart attack than women do, and they have attacks earlier in life. Even after menopause, when women’s death rate from heart disease increases, it’s not as great as men’s.
Heredity (Including Race)
A family history of early coronary heart disease is a risk factor for developing coronary heart disease, specifically if a father or brother is diagnosed before age 55, or a mother or sister is diagnosed before age 65. African Americans have more severe high blood pressure than Caucasians and a higher risk of heart disease. Heart disease risk is also higher among Mexican Americans, American Indians, native Hawaiians and some Asian Americans. This is partly due to higher rates of obesity and diabetes. Most people with a strong family history of heart disease have one or more other risk factors. Just as you can’t control your age, sex and race, you can’t control your family history. Therefore, it’s even more important to treat and control any other risk factors you have.
Ischemic heart disease symptoms
If your coronary arteries narrow, they can’t supply enough oxygen-rich blood to your heart — especially when it’s beating hard, such as during exercise. At first, the decreased blood flow may not cause any coronary artery disease symptoms. As plaque continues to build up in your coronary arteries, however, you may develop coronary artery disease signs and symptoms, including:
- A common symptom of coronary heart disease is angina (chest pain). You may feel pressure, squeezing or tightness in your chest, as if someone were standing on your chest. This pain, referred to as angina, usually occurs on the middle or left side of the chest. You also may feel it in your shoulders, arms, neck, jaw, or back. Angina pain may even feel like indigestion. Angina tends to get worse with activity and go away with rest. Emotional stress also can trigger the pain.
The pain usually goes away within minutes after stopping the stressful activity. In some people, especially women, this pain may be fleeting or sharp and felt in the neck, arm or back.
- Shortness of breath. This symptom occurs if coronary heart disease causes heart failure. When you have heart failure, your heart can’t pump enough blood to meet your body’s needs. Fluid builds up in your lungs, making it hard to breathe. If your heart can’t pump enough blood to meet your body’s needs, you may develop shortness of breath or extreme fatigue with exertion.
- Heart attack. A completely blocked coronary artery may cause a heart attack. The classic signs and symptoms of a heart attack include crushing pressure in your chest and pain in your shoulder or arm, sometimes with shortness of breath and sweating.
Women are somewhat more likely than men are to experience less typical signs and symptoms of a heart attack, such as neck or jaw pain. Sometimes a heart attack occurs without any apparent signs or symptoms.
The severity of these symptoms varies. They may get more severe as the buildup of plaque continues to narrow the coronary arteries.
Some people who have coronary heart disease have no signs or symptoms—a condition called silent coronary heart disease. The disease might not be diagnosed until a person has signs or symptoms of a heart attack, heart failure, or an arrhythmia (an irregular heartbeat).
Heart Attack
A heart attack occurs if the flow of oxygen-rich blood to a section of heart muscle is cut off. This can happen if an area of plaque in a coronary artery ruptures (breaks open).
Blood cell fragments called platelets stick to the site of the injury and may clump together to form blood clots. If a clot becomes large enough, it can mostly or completely block blood flow through a coronary artery.
If the blockage isn’t treated quickly, the portion of heart muscle fed by the artery begins to die. Healthy heart tissue is replaced with scar tissue. This heart damage may not be obvious, or it may cause severe or long-lasting problems.
Ischemic Heart Disease Diagnosis
Your doctor will diagnose coronary heart disease based on your medical and family histories, your risk factors for coronary heart disease, a physical exam, and the results from tests and procedures.
No single test can diagnose coronary heart disease. If your doctor thinks you have coronary heart disease, he or she may recommend one or more of the following tests.
EKG (Electrocardiogram)
An EKG is a simple, painless test that detects and records the heart’s electrical activity. The test shows how fast the heart is beating and its rhythm (steady or irregular). An EKG also records the strength and timing of electrical signals as they pass through the heart.
An EKG can show signs of heart damage due to coronary heart disease and signs of a previous or current heart attack.
Stress Testing
During stress testing, you exercise to make your heart work hard and beat fast while heart tests are done. If you can’t exercise, you may be given medicine to raise your heart rate.
When your heart is working hard and beating fast, it needs more blood and oxygen. Plaque-narrowed arteries can’t supply enough oxygen-rich blood to meet your heart’s needs.
A stress test can show possible signs and symptoms of coronary heart disease, such as:
- Abnormal changes in your heart rate or blood pressure
- Shortness of breath or chest pain
- Abnormal changes in your heart rhythm or your heart’s electrical activity
If you can’t exercise for as long as what is considered normal for someone your age, your heart may not be getting enough oxygen-rich blood. However, other factors also can prevent you from exercising long enough (for example, lung diseases, anemia, or poor general fitness).
As part of some stress tests, pictures are taken of your heart while you exercise and while you rest. These imaging stress tests can show how well blood is flowing in your heart and how well your heart pumps blood when it beats.
Echocardiography
Echocardiography (echo) uses sound waves to create a moving picture of your heart. The picture shows the size and shape of your heart and how well your heart chambers and valves are working.
Echo also can show areas of poor blood flow to the heart, areas of heart muscle that aren’t contracting normally, and previous injury to the heart muscle caused by poor blood flow.
Chest X Ray
A chest x ray takes pictures of the organs and structures inside your chest, such as your heart, lungs, and blood vessels.
A chest x ray can reveal signs of heart failure, as well as lung disorders and other causes of symptoms not related to coronary heart disease.
Blood Tests
Blood tests check the levels of certain fats, cholesterol, sugar, and proteins in your blood. Abnormal levels might be a sign that you’re at risk for coronary heart disease.
Coronary Angiography and Cardiac Catheterization
Your doctor may recommend coronary angiography if other tests or factors show that you’re likely to have coronary heart disease. This test uses dye and special x rays to show the insides of your coronary arteries.
To get the dye into your coronary arteries, your doctor will use a procedure called cardiac catheterization.
A thin, flexible tube called a catheter is put into a blood vessel in your arm, groin (upper thigh), or neck. The tube is threaded into your coronary arteries, and the dye is released into your bloodstream.
Special x rays are taken while the dye is flowing through your coronary arteries. The dye lets your doctor study the flow of blood through your heart and blood vessels.
Cardiac catheterization usually is done in a hospital. You’re awake during the procedure. It usually causes little or no pain, although you may feel some soreness in the blood vessel where your doctor inserts the catheter.
Ischemic heart disease treatment
Treatments for coronary heart disease include heart-healthy lifestyle changes, medicines, medical procedures and surgery, and cardiac rehabilitation 34. Treatment goals may include:
- Lowering the risk of blood clots forming (blood clots can cause a heart attack)
- Preventing complications of coronary heart disease
- Reducing risk factors in an effort to slow, stop, or reverse the buildup of plaque
- Relieving symptoms
- Widening or bypassing clogged arteries
Heart-Healthy Lifestyle Changes
Your doctor may recommend heart-healthy lifestyle changes if you have coronary heart disease. Heart-healthy lifestyle changes include:
- Heart-healthy eating
- Maintaining a healthy weight
- Managing stress
- Physical activity
- Quit smoking
Heart-Healthy Eating
Your doctor may recommend heart-healthy eating, which should include:
- Fat-free or low-fat dairy products, such as fat-free milk
- Fish high in omega-3 fatty acids, such as salmon, tuna, and trout, about twice a week
- Fruits, such as apples, bananas, oranges, pears, and prunes
- Legumes, such as kidney beans, lentils, chickpeas, black-eyed peas, and lima beans
- Vegetables, such as broccoli, cabbage, and carrots
- Whole grains, such as oatmeal, brown rice, and corn tortillas
When following a heart-healthy diet, you should avoid eating:
- A lot of red meat
- Palm and coconut oils
- Sugary foods and beverages
Two nutrients in your diet make blood cholesterol levels rise:
- Saturated fat—found mostly in foods that come from animals
- Trans fat (trans fatty acids)—found in foods made with hydrogenated oils and fats, such as stick margarine; baked goods, such as cookies, cakes, and pies; crackers; frostings; and coffee creamers. Some trans fats also occur naturally in animal fats and meats.
Saturated fat raises your blood cholesterol more than anything else in your diet. When you follow a heart-healthy eating plan, only 5 percent to 6 percent of your daily calories should come from saturated fat. Food labels list the amounts of saturated fat.
Not all fats are bad. Monounsaturated and polyunsaturated fats actually help lower blood cholesterol levels.
Some sources of monounsaturated and polyunsaturated fats are:
- Avocados
- Corn, sunflower, and soybean oils
- Nuts and seeds, such as walnuts
- Olive, canola, peanut, safflower, and sesame oils
- Peanut butter
- Salmon and trout
- Tofu
Sodium
You should try to limit the amount of sodium that you eat. This means choosing and preparing foods that are lower in salt and sodium. Try to use low-sodium and “no added salt” foods and seasonings at the table or while cooking. Food labels tell you what you need to know about choosing foods that are lower in sodium. Try to eat no more than 2,300 milligrams of sodium a day. If you have high blood pressure, you may need to restrict your sodium intake even more.
Dietary Approaches to Stop Hypertension
Your doctor may recommend the Dietary Approaches to Stop Hypertension (DASH) eating plan if you have high blood pressure. The DASH eating plan focuses on fruits, vegetables, whole grains, and other foods that are heart healthy and low in fat, cholesterol, and sodium and salt.
The DASH eating plan is a good heart-healthy eating plan, even for those who don’t have high blood pressure. Read more about What is the DASH Diet.
Alcohol
Try to limit alcohol intake. Too much alcohol can raise your blood pressure and triglyceride levels, a type of fat found in the blood. Alcohol also adds extra calories, which may cause weight gain.
Men should have no more than two drinks containing alcohol a day. Women should have no more than one drink containing alcohol a day. One drink is:
- 12 ounces of beer
- 5 ounces of wine
- 1½ ounces of liquor
Maintaining a Healthy Weight
Maintaining a healthy weight is important for overall health and can lower your risk for coronary heart disease. Aim for a Healthy Weight by following a heart-healthy eating plan and keeping physically active.
Knowing your body mass index (BMI) helps you find out if you’re a healthy weight in relation to your height and gives an estimate of your total body fat.
- Below 18.5 is a sign that you are underweight.
- Between 18.5 and 24.9 is in the normal range.
- Between 25 and 29.9 is considered overweight.
- Of 30 or more is considered obese.
A general goal to aim for is a BMI of less than 25. Your doctor or health care provider can help you set an appropriate BMI goal.
Measuring waist circumference helps screen for possible health risks. If most of your fat is around your waist rather than at your hips, you’re at a higher risk for heart disease and type 2 diabetes. This risk may be high with a waist size that is greater than 35 inches for women or greater than 40 inches for men. To learn how to measure your waist, visit Waist Hip Ratio.
If you’re overweight or obese, try to lose weight. A loss of just 3 percent to 5 percent of your current weight can lower your triglycerides, blood glucose, and the risk of developing type 2 diabetes. Greater amounts of weight loss can improve blood pressure readings, lower LDL cholesterol, and increase HDL cholesterol.
Managing Stress
Research shows that the most commonly reported “trigger” for a heart attack is an emotionally upsetting event—particularly one involving anger. Also, some of the ways people cope with stress—such as drinking, smoking, or overeating—aren’t healthy.
Learning how to manage stress, relax, and cope with problems can improve your emotional and physical health. Consider healthy stress-reducing activities, such as:
- A stress management program
- Meditation
- Physical activity
- Relaxation therapy
- Talking things out with friends or family
Physical Activity
Routine physical activity can lower many coronary heart disease risk factors, including LDL (“bad”) cholesterol, high blood pressure, and excess weight. Physical activity also can lower your risk for diabetes and raise your HDL cholesterol level. HDL is the “good” cholesterol that helps prevent coronary heart disease.
Everyone should try to participate in moderate-intensity aerobic exercise at least 2 hours and 30 minutes per week, or vigorous aerobic exercise for 1 hour and 15 minutes per week. Aerobic exercise, such as brisk walking, is any exercise in which your heart beats faster and you use more oxygen than usual. The more active you are, the more you will benefit. Participate in aerobic exercise for at least 10 minutes at a time spread throughout the week.
Read more about physical activity at:
Talk with your doctor before you start a new exercise plan. Ask your doctor how much and what kinds of physical activity are safe for you.
Quit Smoking
If you smoke, quit. Smoking can raise your risk for coronary heart disease and heart attack and worsen other coronary heart disease risk factors. Talk with your doctor about programs and products that can help you quit smoking. Also, try to avoid secondhand smoke.
If you have trouble quitting smoking on your own, consider joining a support group. Many hospitals, workplaces, and community groups offer classes to help people quit smoking.
Medicines
Sometimes lifestyle changes aren’t enough to control your blood cholesterol levels. For example, you may need statin medications to control or lower your cholesterol. By lowering your cholesterol level, you can decrease your chance of having a heart attack or stroke. Doctors usually prescribe statins for people who have:
- Coronary heart disease, peripheral artery disease, or had a stroke
- Diabetes
- High LDL cholesterol levels
Doctors may discuss beginning statin treatment with those who have an elevated risk for developing heart disease or having a stroke.
Various drugs can be used to treat coronary artery disease, including:
- Cholesterol-modifying medications. By decreasing the amount of cholesterol in the blood, especially low-density lipoprotein (LDL, or the “bad”) cholesterol, these drugs decrease the primary material that deposits on the coronary arteries. Your doctor can choose from a range of medications, including statins, niacin, fibrates and bile acid sequestrants.
- Aspirin. Your doctor may recommend taking a daily aspirin or other blood thinner. This can reduce the tendency of your blood to clot, which may help prevent obstruction of your coronary arteries.
If you’ve had a heart attack, aspirin can help prevent future attacks. There are some cases where aspirin isn’t appropriate, such as if you have a bleeding disorder or you’re already taking another blood thinner, so ask your doctor before starting to take aspirin.
- Beta blockers. These drugs slow your heart rate and decrease your blood pressure, which decreases your heart’s demand for oxygen. If you’ve had a heart attack, beta blockers reduce the risk of future attacks.
- Nitroglycerin. Nitroglycerin tablets, sprays and patches can control chest pain by temporarily dilating your coronary arteries and reducing your heart’s demand for blood.
- Angiotensin-converting enzyme (ACE) inhibitors and angiotensin II receptor blockers (ARBs). These similar drugs decrease blood pressure and may help prevent progression of coronary artery disease.
Your doctor also may prescribe other medications to:
- Decrease your chance of having a heart attack or dying suddenly.
- Lower your blood pressure.
- Prevent blood clots, which can lead to heart attack or stroke.
- Prevent or delay the need for a stent or percutaneous coronary intervention (PCI) or surgery, such as coronary artery bypass grafting (CABG).
- Reduce your heart’s workload and relieve coronary heart disease symptoms.
Take all medicines regularly, as your doctor prescribes. Don’t change the amount of your medicine or skip a dose unless your doctor tells you to. You should still follow a heart healthy lifestyle, even if you take medicines to treat your coronary heart disease.
Alternative medicine
Omega-3 fatty acids are a type of unsaturated fatty acid that’s thought to reduce inflammation throughout the body, a contributing factor to coronary artery disease. However, recent studies have not shown them to be beneficial. More research is needed.
- Fish and fish oil. Fish and fish oil are the most effective sources of omega-3 fatty acids. Fatty fish — such as salmon, herring and light canned tuna — contain the most omega-3 fatty acids and, therefore, the most benefit. Fish oil supplements may offer benefit, but the evidence is strongest for eating fish.
- Flax and flaxseed oil. Flax and flaxseed oil also contain beneficial omega-3 fatty acids, though studies have not found these sources to be as effective as fish. The shell on raw flaxseeds also contains soluble fiber, which can help lower blood cholesterol.
- Other dietary sources of omega-3 fatty acids. Other dietary sources of omega-3 fatty acids include canola oil, soybeans and soybean oil. These foods contain smaller amounts of omega-3 fatty acids than do fish and fish oil, and evidence for their benefit to heart health isn’t as strong.
Other supplements may help reduce your blood pressure or cholesterol level, two contributing factors to coronary artery disease. These include:
- Alpha-linolenic acid (ALA)
- Artichoke
- Barley
- Beta-sitosterol (found in oral supplements and some margarines, such as Promise Activ)
- Blond psyllium
- Cocoa
- Coenzyme Q10
- Garlic
- Oat bran (found in oatmeal and whole oats)
- Sitostanol (found in oral supplements and some margarines, such as Benecol)
Medical Procedures and Surgery
You may need a procedure or surgery to treat coronary heart disease. Both Percutaneous Coronary Intervention and coronary artery bypass grafting (CABG) are used to treat blocked coronary arteries. You and your doctor can discuss which treatment is right for you.
- Percutaneous Coronary Intervention
Percutaneous coronary intervention, commonly known as angioplasty, is a nonsurgical procedure that opens blocked or narrowed coronary arteries. A thin, flexible tube with a balloon or other device on the end is threaded through a blood vessel to the narrowed or blocked coronary artery. Once in place, the balloon is inflated to compress the plaque against the wall of the artery. This restores blood flow through the artery.
During the procedure, the doctor may put a small mesh tube called a stent in the artery. The stent helps prevent blockages in the artery in the months or years after angioplasty.
- Coronary Artery Bypass Grafting
CABG is a type of surgery in which arteries or veins from other areas in your body are used to bypass (that is, go around) your narrowed coronary arteries. CABG can improve blood flow to your heart, relieve chest pain, and possibly prevent a heart attack.
Cardiac Rehabilitation
Your doctor may prescribe cardiac rehabilitation (rehab) for angina or after CABG, angioplasty, or a heart attack. Nearly everyone who has coronary heart disease can benefit from cardiac rehab. Cardiac rehab is a medically supervised program that may help improve the health and well-being of people who have heart problems.
The cardiac rehab team may include doctors, nurses, exercise specialists, physical and occupational therapists, dietitians or nutritionists, and psychologists or other mental health specialists.
Rehab has two parts:
- Education, counseling, and training. This part of rehab helps you understand your heart condition and find ways to reduce your risk for future heart problems. The rehab team will help you learn how to cope with the stress of adjusting to a new lifestyle and how to deal with your fears about the future.
- Exercise training. This part helps you learn how to exercise safely, strengthen your muscles, and improve your stamina. Your exercise plan will be based on your personal abilities, needs, and interests.
Living With Ischemic Heart Disease
Coronary heart disease can cause serious complications. However, if you follow your doctor’s advice and adopt healthy lifestyle habits, you can prevent or reduce the risk of:
- Dying suddenly from heart problems
- Having a heart attack and damaging your heart muscle
- Damaging your heart because of reduced oxygen supply
- Having arrhythmias (irregular heartbeats)
Ongoing Care
Lifestyle changes and medicines can help control coronary heart disease. Lifestyle changes include following a healthy diet, being physically active, maintaining a healthy weight, quitting smoking, and managing stress.
Work closely with your doctor to control your blood pressure and manage your blood cholesterol and blood sugar levels.
A blood test called a lipoprotein panel will measure your cholesterol and triglyceride levels. A fasting blood glucose test will check your blood sugar level and show whether you’re at risk for or have diabetes.
These tests show whether your risk factors are controlled, or whether your doctor needs to adjust your treatment for better results.
Talk with your doctor about how often you should schedule office visits or blood tests. Between those visits, call your doctor if you have any new symptoms or if your symptoms worsen.
Heart Attack Warning Signs
Coronary heart disease raises your risk for a heart attack. Learn the signs and symptoms of a heart attack, and call your local emergency number if you have any of these symptoms:
- Chest pain or discomfort. This involves uncomfortable pressure, squeezing, fullness, or pain in the center or left side of the chest that can be mild or strong. This pain or discomfort often lasts more than a few minutes or goes away and comes back.
- Upper body discomfort in one or both arms, the back, neck, jaw, or upper part of the stomach.
- Shortness of breath, which may occur with or before chest discomfort.
- Nausea (feeling sick to your stomach), vomiting, light-headedness or fainting, or breaking out in a cold sweat.
Symptoms also may include sleep problems, fatigue (tiredness), and lack of energy.
The symptoms of angina can be similar to the symptoms of a heart attack. Angina pain usually lasts for only a few minutes and goes away with rest.
Chest pain or discomfort that doesn’t go away or changes from its usual pattern (for example, occurs more often or while you’re resting) can be a sign of a heart attack. If you don’t know whether your chest pain is angina or a heart attack, call your local emergency number.
Let the people you see regularly know you’re at risk for a heart attack. They can seek emergency care for you if you suddenly faint, collapse, or have other severe symptoms.
Emotional Issues and Support
Living with coronary heart disease may cause fear, anxiety, depression, and stress. You may worry about heart problems or making lifestyle changes that are necessary for your health.
Talk about how you feel with your health care team. Talking to a professional counselor also can help. If you’re very depressed, your doctor may recommend medicines or other treatments that can improve your quality of life.
Joining a patient support group may help you adjust to living with coronary heart disease. You can see how other people who have the same symptoms have coped with them. Talk with your doctor about local support groups or check with an area medical center.
Support from family and friends also can help relieve stress and anxiety. Let your loved ones know how you feel and what they can do to help you.
- American Heart Association. Silent Ischemia and Ischemic Heart Disease. http://www.heart.org/HEARTORG/Conditions/HeartAttack/PreventionTreatmentofHeartAttack/Silent-Ischemia-and-Ischemic-Heart-Disease_UCM_434092_Article.jsp[↩][↩][↩][↩][↩]
- Institute of Medicine (US) Committee on Social Security Cardiovascular Disability Criteria. Cardiovascular Disability: Updating the Social Security Listings. Washington (DC): National Academies Press (US); 2010. 7, Ischemic Heart Disease. Available from: https://www.ncbi.nlm.nih.gov/books/NBK209964/[↩][↩][↩]
- National Institutes of Health. National Heart, Lung and Blood Institute. Other Names for Coronary Heart Disease. https://www.nhlbi.nih.gov/health/health-topics/topics/cad/names[↩]
- American Heart Association. Coronary Artery Disease – Coronary Heart Disease. http://www.heart.org/HEARTORG/Conditions/More/MyHeartandStrokeNews/Coronary-Artery-Disease—The-ABCs-of-CAD_UCM_436416_Article.jsp[↩][↩][↩][↩]
- Gibbons, R. J., G. J. Balady, J. T. Bricker, B. R. Chaitman, G. F. Fletcher, V. F. Froelicher, D. B. Mark, B. D. McCallister, A. N. Mooss, M. G. O’Reilly, W. L. Winters Jr., and Task Force members, E. M. Antman, J. S. Alpert, D. P. Faxon, V. Fuster, G. Gregoratos, L. F. Hiratzka, A. K. Jacobs, R. O. Russell, and S. C. Smith Jr. 2002. b. ACC/AHA 2002 guideline update for exercise testing: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Update the 1997 Exercise Testing Guidelines). Circulation 106:1883–1892. http://circ.ahajournals.org/content/106/14/1883.long[↩]
- Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, de Ferranti S, Després JP, Fullerton HJ, Howard VJ, Huffman MD, Judd SE, Kissela BM, Lackland DT, Lichtman JH, Lisabeth LD, Liu S, Mackey RH, Matchar DB, McGuire DK, Mohler ER 3rd., Moy CS, Muntner P, Mussolino ME, Nasir K, Neumar RW, Nichol G, Palaniappan L, Pandey DK, Reeves MJ, Rodriguez CJ, Sorlie PD, Stein J, Towfighi A, Turan TN, Virani SS, Willey JZ, Woo D, Yeh RW, Turner MB. on behalf of the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2015 update: a report from the American Heart Association [published correction appears in Circulation. 2015;131:e535]. Circulation. 2015;131:e29–e322. doi: 10.1161/CIR.0000000000000152. http://circ.ahajournals.org/content/131/4/e29[↩][↩]
- Yang XP, Reckelhoff JF. Estrogen, hormonal replacement therapy and cardiovascular disease. Curr Opin Nephrol Hypertens. 2011;20:133–138. doi: 10.1097/MNH.0b013e3283431921. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3123884/[↩]
- Mosca L, Barrett-Connor E, Wenger NK. Sex/gender differences in cardiovascular disease prevention: what a difference a decade makes. Circulation. 2011;124:2145–2154. doi: 10.1161/CIRCULATIONAHA.110.968792. http://circ.ahajournals.org/content/124/19/2145[↩]
- Ford ES, Capewell S. Coronary heart disease mortality among young adults in the U.S. from 1980 through 2002: concealed leveling of mortality rates. J Am Coll Cardiol. 2007;50:2128–2132. doi: 10.1016/j.jacc.2007.05.056. https://www.ncbi.nlm.nih.gov/pubmed/18036449[↩][↩]
- Go AS, Mozaffarian D, Roger VL, Benjamin EJ, Berry JD, Blaha MJ, Dai S, Ford ES, Fox CS, Franco S, Fullerton HJ, Gillespie C, Hailpern SM, Heit JA, Howard VJ, Huffman MD, Judd SE, Kissela BM, Kittner SJ, Lackland DT, Lichtman JH, Lisabeth LD, Mackey RH, Magid DJ, Marcus GM, Marelli A, Matchar DB, McGuire DK, Mohler ER 3rd., Moy CS, Mussolino ME, Neumar RW, Nichol G, Pandey DK, Paynter NP, Reeves MJ, Sorlie PD, Stein J, Towfighi A, Turan TN, Virani SS, Wong ND, Woo D, Turner MB. on behalf of the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2014 update: a report from the American Heart Association. Circulation. 2014;129:e28–e292. doi: 10.1161/01.cir.0000441139.02102.80. http://circ.ahajournals.org/content/129/3/e28[↩][↩][↩]
- Preventing and Experiencing Ischemic Heart Disease as a Woman: State of the Science. A Scientific Statement From the American Heart Association. Circulation. 2016;133:1302-1331. Originally published February 29, 2016. http://circ.ahajournals.org/content/133/13/1302[↩]
- Shehab A, Al-Dabbagh B, AlHabib KF, Alsheikh-Ali AA, Almahmeed W, Sulaiman K, Al-Motarreb A, Nagelkerke N, Al Suwaidi J, Hersi A, Al Faleh H, Asaad N, Al Saif S, Amin H. Gender disparities in the presentation, management and outcomes of acute coronary syndrome patients: data from the 2nd Gulf Registry of Acute Coronary Events (Gulf RACE-2). PLoS One. 2013;8:e55508. doi: 10.1371/journal.pone.0055508. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3566183/[↩]
- Shaw LJ, Shaw RE, Merz CN, Brindis RG, Klein LW, Nallamothu B, Douglas PS, Krone RJ, McKay CR, Block PC, Hewitt K, Weintraub WS, Peterson ED. American College of Cardiology-National Cardiovascular Data Registry Investigators. Impact of ethnicity and gender differences on angiographic coronary artery disease prevalence and in-hospital mortality in the American College of Cardiology-National Cardiovascular Data Registry. Circulation. 2008;117:1787–1801. doi: 10.1161/CIRCULATIONAHA.107.726562. http://circ.ahajournals.org/content/117/14/1787[↩]
- Lichtman JH, Wang Y, Jones SB, Leifheit-Limson EC, Shaw LJ, Vaccarino V, Rumsfeld JS, Krumholz HM, Curtis JP. Age and sex differences in inhospital complication rates and mortality after percutaneous coronary intervention procedures: evidence from the NCDR(®). Am Heart J. 2014;167:376–383. doi: 10.1016/j.ahj.2013.11.001. https://www.ncbi.nlm.nih.gov/pubmed/24576523[↩]
- Gehrie ER, Reynolds HR, Chen AY, Neelon BH, Roe MT, Gibler WB, Ohman EM, Newby LK, Peterson ED, Hochman JS. Characterization and outcomes of women and men with non-ST-segment elevation myocardial infarction and nonobstructive coronary artery disease: results from the Can Rapid Risk Stratification of Unstable Angina Patients Suppress Adverse Outcomes with Early Implementation of the ACC/AHA Guidelines (CRUSADE) quality improvement initiative. Am Heart J. 2009;158:688–694. doi: 10.1016/j.ahj.2009.08.004. https://www.ncbi.nlm.nih.gov/pubmed/19781432[↩]
- Sedlak TL, Lee M, Izadnegahdar M, Merz CN, Gao M, Humphries KH. Sex differences in clinical outcomes in patients with stable angina and no obstructive coronary artery disease. Am Heart J. 2013;166:38–44. doi: 10.1016/j.ahj.2013.03.015. https://www.ncbi.nlm.nih.gov/pubmed/23816019[↩]
- Gulati M, Cooper-DeHoff RM, McClure C, Johnson BD, Shaw LJ, Handberg EM, Zineh I, Kelsey SF, Arnsdorf MF, Black HR, Pepine CJ, Merz CN. Adverse cardiovascular outcomes in women with nonobstructive coronary artery disease: a report from the Women’s Ischemia Syndrome Evaluation Study and the St James Women Take Heart Project. Arch Intern Med. 2009;169:843–850. doi: 10.1001/archinternmed.2009.50. https://www.ncbi.nlm.nih.gov/pubmed/19433695[↩]
- Sharaf B, Wood T, Shaw L, Johnson BD, Kelsey S, Anderson RD, Pepine CJ, Bairey Merz CN. Adverse outcomes among women presenting with signs and symptoms of ischemia and no obstructive coronary artery disease: findings from the National Heart, Lung, and Blood Institute-sponsored Women’s Ischemia Syndrome Evaluation (WISE) angiographic core laboratory. Am Heart J. 2013;166:134–141. doi: 10.1016/j.ahj.2013.04.002. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3703586/[↩]
- Shah AS, Griffiths M, Lee KK, McAllister DA, Hunter AL, Ferry AV, Cruikshank A, Reid A, Stoddart M, Strachan F, Walker S, Collinson PO, Apple FS, Gray AJ, Fox KA, Newby DE, Mills NL. High sensitivity cardiac troponin and the under-diagnosis of myocardial infarction in women: prospective cohort study [published correction appears in BMJ. 2015;350:h626]. BMJ. 2015;350:g7873. http://www.bmj.com/content/350/bmj.g7873[↩][↩]
- Shah AS, Newby DE, Mills NL. High sensitivity cardiac troponin in patients with chest pain. BMJ. 2013;347:f4222. http://www.bmj.com/content/347/bmj.f4222[↩]
- Norris CM, Ghali WA, Galbraith PD, Graham MM, Jensen LA, Knudtson ML. APPROACH Investigators. Women with coronary artery disease report worse health-related quality of life outcomes compared to men. Health Qual Life Outcomes. 2004;2:21–31. doi: 10.1186/1477-7525-2-21. https://www.ncbi.nlm.nih.gov/pubmed/15128455[↩]
- Rutledge T, Reis SE, Olson M, Owens J, Kelsey SF, Pepine CJ, Mankad S, Rogers WJ, Sopko G, Cornell CE, Sharaf B, Merz CN. Depression is associated with cardiac symptoms, mortality risk, and hospitalization among women with suspected coronary disease: the NHLBI-sponsored WISE study. Psychosom Med. 2006;68:217–223. doi: 10.1097/01.psy.0000195751.94998.e3. http://circ.ahajournals.org/lookup/content/68/2/217[↩]
- National Institutes of Health. National Heart, Lung and Blood Institute. What Causes a Heart Attack ? https://www.nhlbi.nih.gov/health/health-topics/topics/heartattack/causes[↩][↩]
- National Institutes of Health. National Heart, Lung and Blood Institute. Coronary Heart Disease. https://www.nhlbi.nih.gov/health/health-topics/topics/cad[↩][↩]
- National Institutes of Health. National Heart, Lung and Blood Institute. Heart Attack. https://www.nhlbi.nih.gov/health/health-topics/topics/heartattack[↩]
- National Institutes of Health. National Heart, Lung and Blood Institute. Who Is at Risk for Coronary Heart Disease ? https://www.nhlbi.nih.gov/health/health-topics/topics/cad/atrisk[↩]
- National Institutes of Health. National Heart, Lung and Blood Institute. Coronary Heart Disease Risk Factors. https://www.nhlbi.nih.gov/health/health-topics/topics/hd/atrisk[↩][↩][↩][↩][↩][↩]
- BMI Calculator Adults. https://www.cdc.gov/healthyweight/assessing/bmi/adult_BMI/english_bmi_calculator/bmi_calculator.html[↩]
- Centers for Disease Control and Prevention. CDC Clinical Growth Charts. https://www.cdc.gov/growthcharts/clinical_charts.htm[↩]
- Centers for Disease Control and Prevention. BMI Percentile Calculator for Child and Teen. https://nccd.cdc.gov/dnpabmi/Calculator.aspx[↩]
- BMI Calculator Children. https://nccd.cdc.gov/dnpabmi/Calculator.aspx[↩]
- Zhang C, Rexrode KM, van Dam RM, Li TY, Hu FB. Abdominal obesity and the risk of all-cause, cardiovascular, and cancer mortality: sixteen years of follow-up in US women. Circulation. 2008;117:1658-67. http://circ.ahajournals.org/content/117/13/1658.long[↩]
- National Heart, Lung, and Blood Institute. Clinical guidelines on the identification, evaluation, and treatment of overweight and obesity in adults: the evidence report. Bethesda, MD; 1998. https://www.nhlbi.nih.gov/health/health-topics/topics/obe[↩]
- National Heart, Lung, and Blood Institute. How Is Coronary Heart Disease Treated ? https://www.nhlbi.nih.gov/health/health-topics/topics/cad/treatment[↩]





{kind=link}