
Contents
- What is liver function test
- Substances measured in liver function testing
- Why would I need a liver function test?
- The Liver
- When is liver function test ordered?
- Liver function test normal values
- What does abnormal liver function test result mean?
- Liver function test results explained
- Liver function test interpretation
- Alanine Aminotransferase (ALT)
- Aspartate Aminotransferase (AST)
- Alkaline Phosphatase (ALP)
- Gamma-Glutamyl Transferase (GGT)
- Bilirubin
- Lactate Dehydrogenase (LDH)
- Total Protein
- Albumin
- Prothrombin Time and International Normalized Ratio (PT/INR)
- Lactate Dehydrogenase (LDH)
- Alpha-fetoprotein (AFP) Tumor Marker
- Antinuclear Antibody (ANA)
- Smooth Muscle Antibody (SMA)
- Anti-Liver/Kidney Microsomal Antibodies Type 1 (Anti-LKM-1)
- Liver function test interpretation
What is liver function test
Liver function test (also called LFT or liver panel test) is a blood test that can provide information about how your liver is working. Liver test gives an indication of whether the liver is functioning properly. Liver function test examines the levels of a number of proteins, enzymes and other substances that are either produced by liver cells or released into the blood when liver cells are damaged. Liver function tests measure the amount of particular chemicals in the blood. This gives a gauge of possible damage to liver cells. A liver function test (LFT) is also very useful to see if there is active damage in the liver (hepatitis) or sluggish bile flow (cholestasis). So a more correct term for a liver test would actually be a liver dysfunction test.
The liver is a large organ that is located in the upper right-hand side of the abdominal area just beneath the rib cage. The liver is a vital organ that is involved in more than 500 functions. Among them, the liver processes drugs and alcohol, filters toxic chemicals, stores vitamins and minerals, and makes bile, proteins and enzymes. The liver helps to process the body’s nutrients, manufactures bile to help digest fats, produces many important proteins such as blood clotting factors, and breaks down potentially toxic substances into harmless ones that the body can use or excrete.
Liver function blood test examines the proteins, enzymes, that indicate how well your liver is working. They can show if there is damage to liver cells or a blockage near the liver.
It’s important to remember that diagnosis of liver disease depends on a combination of patient history, physical examination, laboratory testing, biopsy and sometimes imaging studies such as ultrasound scans. Diagnosis of hepatitis C usually also involves antibody tests or PCR tests.
People reading this page should keep in mind that abnormalities within liver tests don’t necessarily point to specific diseases. Only a physician who knows all the aspects of a specific case can reliably make a diagnosis.
Substances measured in liver function testing
A liver panel is a group of tests that are performed together to detect, evaluate, and monitor liver disease or damage. The liver is one of the largest organs in the body and is located in the upper right-hand part of the abdomen and behind the lower ribs. The liver metabolizes and detoxifies drugs and substances that are harmful to the body. It produces blood clotting factors, proteins, and enzymes, helps maintain hormone balances, and stores vitamins and minerals. Bile, a fluid produced by the liver, is transported through ducts directly to the small intestine to help digest fats or to the gallbladder to be stored and concentrated for later use.
A variety of diseases and infections can cause acute or chronic damage to the liver, causing inflammation (hepatitis), scarring (cirrhosis), bile duct obstructions, liver tumors, and liver dysfunction. Alcohol, drugs, some herbal supplements, and toxins can also pose a threat. A significant amount of liver damage may be present before symptoms such as jaundice, dark urine, light-colored stools, itching (pruritus), nausea, fatigue, diarrhea, and unexplained weight loss or gain emerge. Early detection is essential in order to minimize damage and preserve liver function.
The liver panel measures enzymes, proteins, and substances that are produced, processed or eliminated by the liver and are affected by liver injury. Some are released by damaged liver cells and some reflect a decrease in the liver’s ability to perform one or more of its functions. When performed together, these tests give a healthcare practitioner a snapshot of the health of a person’s liver, an indication of the potential severity of any liver injury, change in liver status over time, and a starting place for further diagnostic testing.
Total protein
Total protein is simply a combined measure of the concentrations of proteins in the blood. This information can provide clues to several diagnostic possibilities.
There are 2 major types of protein: albumin and globulin.
- Albumin
Albumin provides a gauge of nutritional status. It can be reduced due to liver damage and kidney disease. Because albumin is made in the liver, levels tend to drop with cirrhosis.
- Globulin
This describes the specific level of globulins — which include antibodies. This measure can be raised when liver cells are damaged due to autoimmune liver damage or to long-standing liver disease of many types, particularly when cirrhosis exists.
Bilirubin
Bilirubin is a by-product of the breakdown of red blood cells. It is the yellowish pigment responsible for jaundice.
Bilirubin levels can be raised due to many different liver diseases, as well as conditions other than liver disease, e.g. gallstones. In cases of long-term liver illness (chronic hepatitis), the level usually stays within the normal range until significant liver damage has occurred and cirrhosis is present.
In cases of short-term liver illness (acute hepatitis), elevated bilirubin levels indicate the severity of the acute illness.
GGT
GGT (Gamma Glutamyl Transpeptidase) is an enzyme produced in bile ducts that may be elevated due to bile duct illness. The GGT test is extremely sensitive and may be elevated due to any type of liver disease or by different drugs, including alcohol, even when liver disease is minimal. GGT levels are sometimes elevated even in the case of a normally functioning liver.
ALK Phos
ALK Phos refers to Alkaline Phosphatase, a family of enzymes produced in the bile ducts, intestine, kidneys, placenta and bones. These levels may rise when disease of the bile ducts or bone disorders occur.
ALT
ALT (Alanine Transaminase) also called SGPT (Serum Glutamic-Pyruvic Transaminase), is an enzyme produced in hepatocytes (the major type of liver cells). ALT level in the blood is increased when hepatocytes are damaged or die — all types of hepatitis (viral, alcoholic, drug-induced etc) cause hepatocyte damage.
Levels of ALT may equate to the degree of cell damage but this is not always the case, particularly with hepatitis C. An accurate estimate of liver cell damage can only be made by liver biopsy.
AST
AST (Aspartate Transaminase) also called SGOT (Serum Glutamic-Oxaloacetic Transaminase), is similar to ALT above, but less specific for liver disease because it is also produced in body muscle cells. It does tend to be higher than ALT in cases of alcohol-related liver disease.
Platelet count
Platelets are the smallest of all blood cells and are involved in promoting clotting of the blood — normally a process of healing. In cases of chronic liver disease where cirrhosis exists, the platelet count can be lowered — although this can occur due to many conditions other than liver disease.
Why would I need a liver function test?
Your doctor will order a liver test to screen for, detect, evaluate, and monitor acute and chronic liver inflammation (hepatitis), liver infection, liver disease and/or and damage.
Your doctor will periodically to evaluate your liver function; whenever you are at risk for liver injury; when you are taking medications that may affect your liver; when you have a liver disease; when you have symptoms associated with liver damage, such as jaundice.
Doctors often request these liver function tests for people who:
- have liver disease or damage
- are, or might be, infected with hepatitis viruses
- are heavy drinkers
- have a family history of liver disease
- take drugs that can damage the liver.
Your doctor might order liver function tests if you have:
- jaundice
- dark urine
- weakness or tiredness
- loss of appetite
- nausea and vomiting
- abdominal pain or swelling
- itching.
How to prepare for liver test
No preparation is needed for liver function test. However, your doctor may instruct you to fast overnight with only water permitted. Follow any instructions you are given. Inform the healthcare provider about all prescription and over-the-counter medications, herbal medications, vitamins and supplements you are taking.
Can I have liver disease if I feel fine?
Yes, early acute liver disease and chronic liver disease often cause no symptoms or mild nonspecific symptoms, such as fatigue and nausea.
Is there anything else I should know?
In order to diagnose a liver disease, a healthcare practitioner will evaluate the liver panel test results, order follow-up tests such as hepatitis virus testing, and may order a liver biopsy and/or imaging scans to help confirm a diagnosis and determine the extent of liver damage.
Can I have abnormal test results and not have liver disease?
Yes, many temporary conditions, such as shock, burns, severe infections, muscle trauma, dehydration, pancreatitis, hemolysis, and pregnancy, can cause one or more of the liver function tests to be abnormal.
Why does my doctor want to know all of the medications and supplements I am taking?
Your healthcare provider will want to evaluate everything you are taking as a whole. Many over-the-counter drugs and herbal or dietary supplements have the potential to affect the liver. Excessive amounts of a drug, and/or a decreased ability to metabolize a drug, and/or a combination of drugs (including over-the-counter drugs and supplements) may injure the liver. For instance, both excessive acetaminophen use and the combination of acetaminophen and alcohol can cause severe liver damage.
Why is my family history important?
Some liver conditions, such as hemochromatosis and Wilson disease, may be inherited and can progressively damage the liver. Early detection of these conditions allows them to be treated and managed appropriately.
The Liver
Your liver is the largest organ inside your body, weighing about 1.4 kg (3 pounds) in an average adult. The liver is in the right upper quadrant of the abdominal cavity, just inferior to the diaphragm in the right superior part of the abdominal cavity and under your right ribs just beneath your right lung – filling much of the right hypochondriac and epigastric regions and extending into the left hypochondriac region. The liver is partially surrounded by the ribs, and extends from the level of the fifth intercostal space to the lower margin of the right rib cage, which protects this highly vascular organ from blows that could rupture it. The liver is shaped like a wedge, the wide base of which faces right and the narrow apex of which lies just inferior to the level of the left nipple. The reddish-brown liver is well supplied with blood vessels.
Figure 1. Location of the human liver
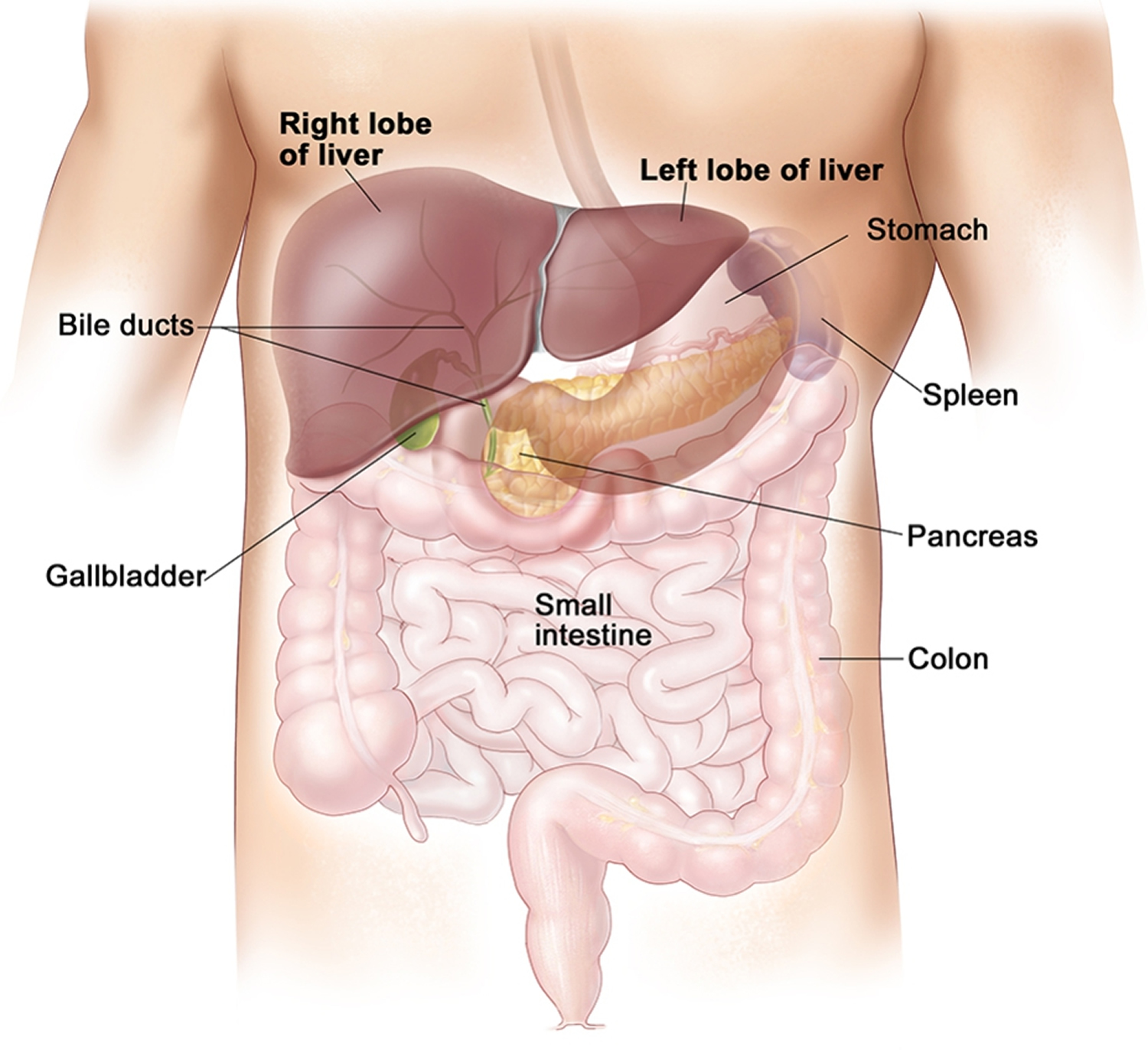
Figure 2. Liver anatomy
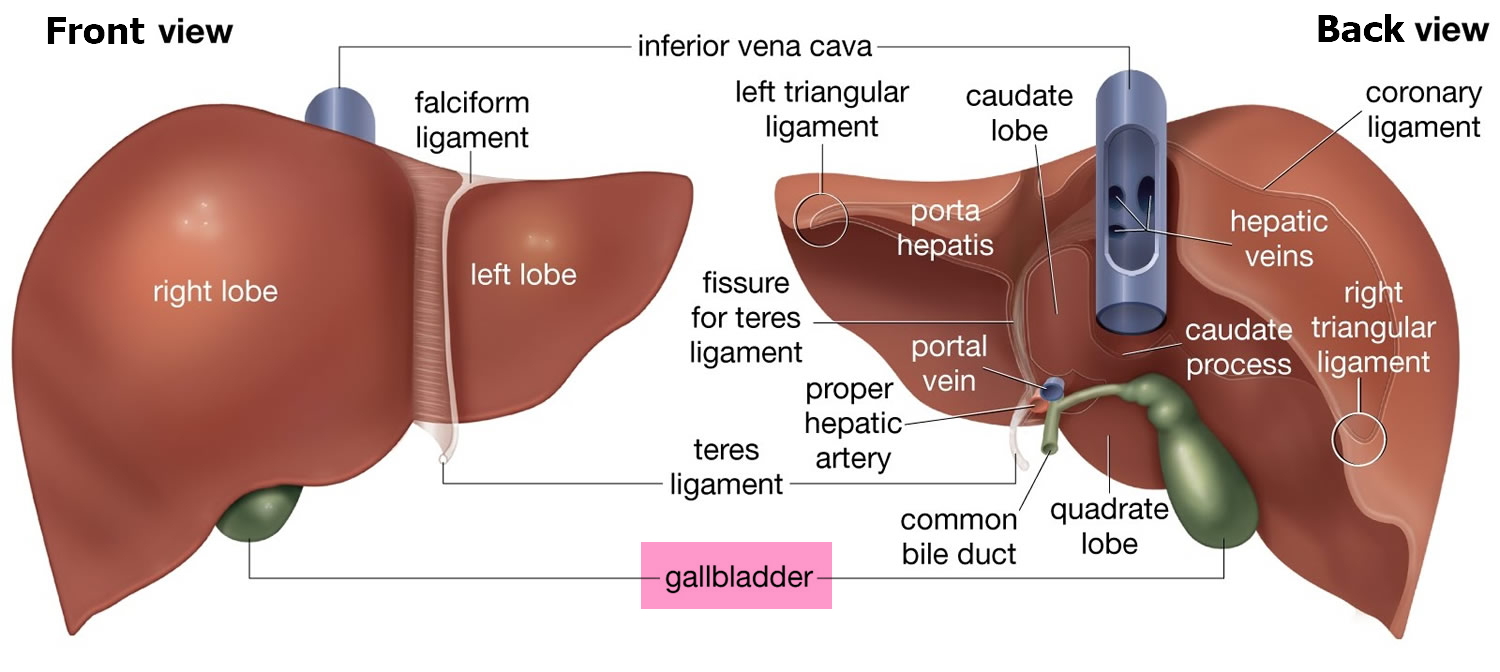
Figure 3. Liver lobule
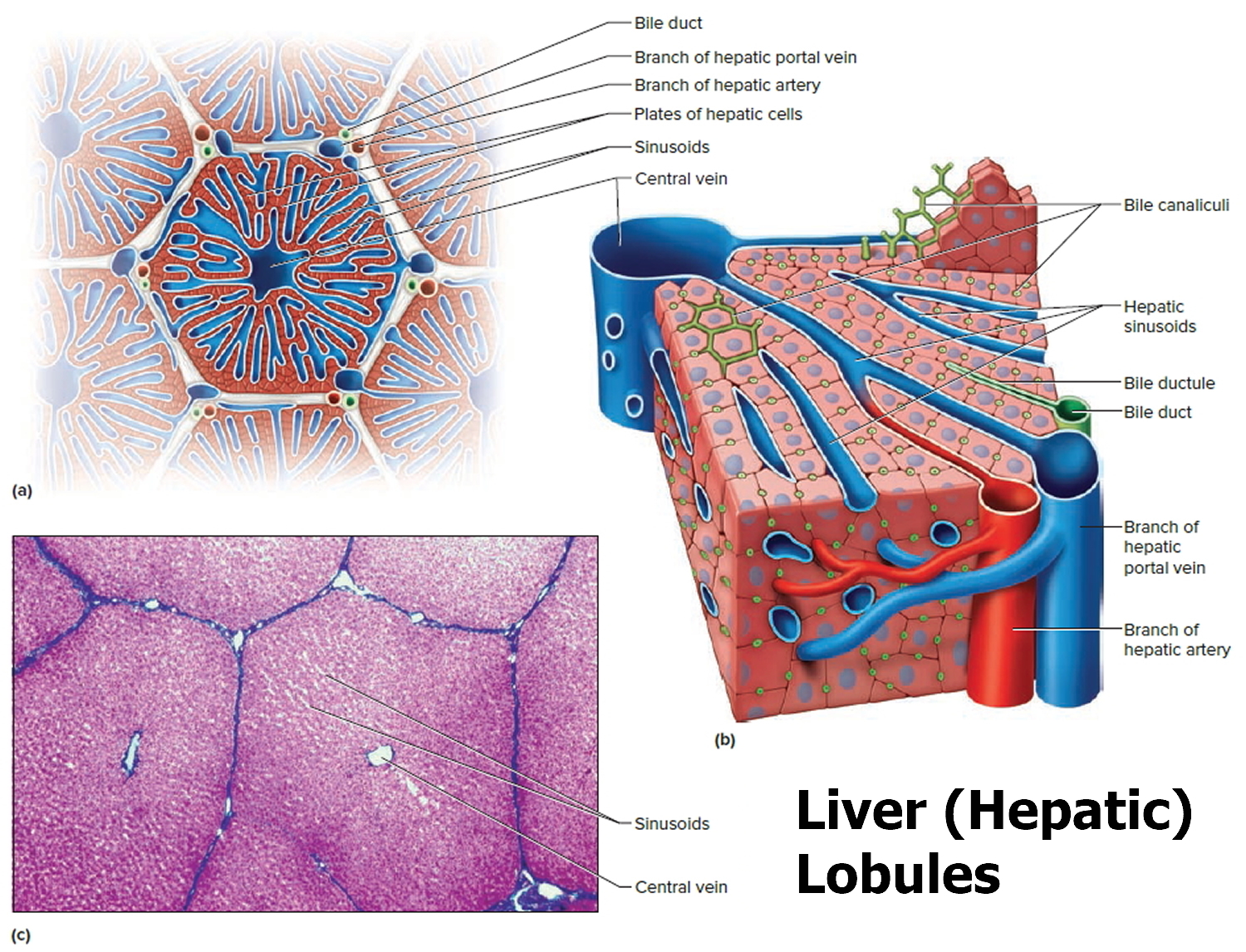
Note: (a) Cross section of a hepatic lobule. (b) Enlarged longitudinal section of a hepatic lobule. (c) Light micrograph of hepatic lobules in cross section.
Liver functions
Amazingly versatile, your liver performs over 500 complex biochemical functions. Its digestive function is to produce bile, a green alkaline liquid that is stored in the gallbladder and secreted into the duodenum. Bile salts emulsify fats in the small intestine; that is, they break up fatty nutrients into tiny particles, just as dish detergent breaks up a pool of fat drippings in a roasting pan. These smaller particles are more accessible to digestive enzymes from the pancreas. The liver also performs many metabolic functions and you cannot live without your liver:
- Picks up glucose from nutrient-rich blood returning from the alimentary canal and stores this carbohydrate as glycogen for subsequent use by the body.
- Processes fats and amino acids and stores certain vitamins.
- Detoxifies many poisons and drugs in the blood.
- Makes the blood proteins.
- It breaks down and stores many of the nutrients absorbed from the intestine that your body needs to function. Some nutrients must be changed (metabolized) in the liver before they can be used for energy or to build and repair body tissues.
- It makes most of the clotting factors that keep you from bleeding too much when you are cut or injured.
- It secretes bile into the intestines to help absorb nutrients (especially fats).
- It breaks down alcohol, drugs, and toxic wastes in the blood, which then pass from the body through urine and stool.
Almost all of these functions are carried out by a type of cell called a hepatocyte or simply a liver cell.
The liver carries on many important metabolic activities. The liver plays a key role in carbohydrate metabolism by helping maintain concentration of blood glucose within the normal range. Liver cells responding to the hormone insulin lower the blood glucose level by polymerizing glucose to glycogen. Liver cells responding to the hormone glucagon raise the blood glucose level by breaking down glycogen to glucose or by converting noncarbohydrates into glucose.
The liver’s effects on lipid metabolism include oxidizing (breaking down) fatty acids at an especially high rate; synthesizing lipoproteins, phospholipids, and cholesterol; and converting excess portions of carbohydrate molecules into fat molecules. The blood transports fats synthesized in the liver to adipose tissue for storage.
Other liver functions concern protein metabolism. They include deaminating amino acids; forming urea; synthesizing plasma proteins such as clotting factors; and converting certain amino acids into other amino acids.
The liver also stores many substances, including glycogen, iron, and vitamins A, D, and B12. In addition, macrophages in the liver help destroy damaged red blood cells and phagocytize foreign antigens. The liver also removes toxic substances such as alcohol and certain drugs from blood (detoxification).
A liver function important to digestion is bile secretion. Table 1 summarizes the major functions of the liver.
Table 1. Major Functions of the Liver
| General Function | Specific Function |
| Carbohydrate metabolism | Polymerizes glucose to glycogen; breaks down glycogen to glucose; converts noncarbohydrates to glucose |
| Lipid metabolism | Oxidizes fatty acids; synthesizes lipoproteins, phospholipids, and cholesterol; converts excess portions of carbohydrate molecules into fats |
| Protein metabolism | Deaminates amino acids; forms urea; synthesizes plasma proteins; converts certain amino acids into other amino acids |
| Storage | Stores glycogen, iron, and vitamin A, vitamin D and vitamin B12 |
| Blood filtering | Removes damaged red blood cells and foreign substances by phagocytosis |
| Detoxification | Removes toxins from blood |
| Secretion | Produces and secretes bile |
The Bile
Bile is a yellowish-green liquid continuously secreted from hepatic cells. In addition to water, bile contains bile salts, bile pigments (bilirubin and biliverdin), cholesterol, and electrolytes. Of these, bile salts are the most abundant and are the only bile components that have a digestive function.
Bile pigments are breakdown products of hemoglobin from red blood cells and are normally secreted in the bile.
Jaundice, a yellowing of the skin and mucous membranes due to accumulation of bile pigment, has several causes. In obstructive jaundice bile ducts are blocked, perhaps by gallstones or tumors. In hepatocellular jaundice the liver is diseased, as in cirrhosis or hepatitis. In hemolytic jaundice red blood cells are destroyed too rapidly, as happens with an incompatible blood transfusion or a blood infection.
Regulation of Bile Release
Normally bile does not enter the duodenum until cholecystokinin stimulates the gallbladder to contract. The intestinal mucosa releases this hormone in response to proteins and fats in the small intestine. The hepatopancreatic sphincter usually remains contracted until a peristaltic wave in the duodenal wall approaches it. Then the sphincter relaxes, and bile is squirted into the duodenum.
Functions of Bile Salts
Bile salts aid digestive enzymes. Bile salts affect fat globules (clumped molecules of fats) much like a soap or detergent would affect them. That is, bile salts break fat globules into smaller droplets that are more soluble in water. This action, called emulsification, greatly increases the total surface area of the fatty substance. The resulting fat droplets disperse in water. Fat-splitting enzymes (lipases) can then digest the fat molecules more effectively. Bile salts also enhance absorption of fatty acids, cholesterol, and the fat-soluble vitamins A, D, E, and K.
Low levels of bile salts result in poor lipid absorption and vitamin deficiencies.
When is liver function test ordered?
A liver panel, or one or more of its components, may be ordered when someone is at risk for liver dysfunction. Some examples include:
- People who take medications that may potentially damage the liver
- Those who are alcoholics or heavy drinkers
- Those who have a history of known or possible exposure to hepatitis viruses
- Individuals whose families have a history of liver disease
- People who are overweight, especially if they have diabetes and/or high blood pressure
A liver panel may be ordered when a person has signs and symptoms of liver disease; however, most people who have liver disease do not have any of these symptoms until the disease has been present for many years or is very severe. Some of these include:
- Weakness, fatigue
- Loss of appetite
- Nausea, vomiting
- Abdominal swelling and/or pain
- Jaundice (yellowing of eyes or skin)
- Dark urine, light-colored stool
- Itching (pruritus)
- Diarrhea
Usually no one single set of liver tests is used to make a diagnosis. Often, several liver panels will be ordered over a few days or weeks to help determine the cause of the liver disorder and evaluate its severity.
When liver disease is detected, it may be monitored on a regular basis over time with the liver panel or with one or more of its components. A liver panel may also be ordered regularly to monitor the effectiveness of treatment for the liver disorder.
Liver function test normal values
- Total protein: Total protein should be between 63-80g/L (6.3 to 8.0 g/dL)
- Albumin: Normal values for albumin are between 35-50 g/L [3.5 to 5.0 grams per deciliter (g/dL)]
- Bilirubin: Normal values for total plasma bilirubin are quoted as less than 20 umol/L [0.1 to 1.2 milligrams per deciliter (mg/dL)]
- Alkaline Phosphatase (ALP): A normal ALP is between 45 to 115 U/L
- Gamma Glutamyl Transpeptidase (GGT): GGT should be less than 60U/L (9 to 48 U/L) in a normal individual
- Alanine aminotransferase (ALT) or SGPT (Serum Glutamic-Pyruvic Transaminase): ALT are less than 36U/L [7 to 55 units per liter (U/L)]
- Aspartate Amino Transferase (AST) or SGOT (Serum Glutamic-Oxaloacetic Transaminase): A normal AST is less than 42U/L (8 to 48 U/L)
- Lactate dehydrogenase (LD): 122 to 222 U/L
- Prothrombin time (PT): 9.5 to 13.8 seconds
These results are typical for adult men. Normal results vary from laboratory to laboratory and might be slightly different for women and children.
Your doctor will use these results to help diagnose your condition or determine treatment you might need. If you already have liver disease, liver function tests can help determine how your disease is progressing and if you’re responding to treatment.
What does abnormal liver function test result mean?
Liver function test results are not diagnostic of a specific condition; they indicate that there may be a problem with the liver. In a person who does not have symptoms or identifiable risk factors, abnormal liver test results may indicate a temporary liver injury or reflect something that is happening elsewhere in the body – such as in the skeletal muscles, pancreas, or heart. It may also indicate early liver disease and the need for further testing and/or periodic monitoring.
Results of liver function tests are usually evaluated together. Several sets of results from tests performed over a few days or weeks are often assessed together to determine if a pattern is present. Each person will have a unique set of test results that will typically change over time. A healthcare practitioner evaluates the combination of liver test results to gain clues about the underlying condition. Often, further testing is necessary to determine what is causing the liver damage and/or disease.
This table shows examples of some combinations of results that may be seen in certain types of liver conditions or diseases.
Table 2. Liver function test interpretation
| Type of liver condition or disease | Bilirubin | ALT and AST | ALP | Albumin | PT |
| Acute liver damage (due, for example, to infection, toxins or drugs, etc.) | Normal or increased usually after ALT and AST are already increased | Usually greatly increased (> 10 times); ALT is usually higher than AST | Normal or only moderately increased | Normal | Usually normal |
| Chronic forms of various liver disorders | Normal or increased | Mildly or moderately increased; ALT is persistently increased | Normal to slightly increased | Normal | Normal |
| Alcoholic Hepatitis | Normal or increased | AST is moderately increased, usually at least twice the level of ALT | Normal or moderately increased | Normal | Normal |
| Cirrhosis | May be increased but this usually occurs later in the disease | AST is usually higher than ALT but levels are usually lower than in alcoholic disease | Normal or increased | Normal or decreased | Usually prolonged |
| Bile duct obstruction, cholestasis | Normal or increased; increased in complete obstruction | Normal to moderately increased | Increased; often greater than 4 times what is normal | Usually normal but if the disease is chronic, levels may decrease | Usually normal |
| Cancer that has spread to the liver (metastasized) | Usually normal | Normal or slightly increased | Usually greatly increased | Normal | Normal |
| Cancer originating in the liver (hepatocellular carcinoma, HCC) | May be increased, especially if the disease has progressed | AST higher than ALT but levels lower than that seen in alcoholic disease | Normal or increased | Normal or decreased | Usually prolonged |
| Autoimmune | Normal or increased | Moderately increased; ALT usually higher than AST | Normal or slightly increased | Usually decreased | Normal |
Abbreviations: Alanine aminotransferase (ALT); Alkaline phosphatase (ALP); Aspartate aminotransferase (AST); Total protein (TP); Gamma-glutamyl transferase (GGT); Lactate dehydrogenase (LD); Prothrombin time (PT); Partial Thromboplastin Time (PTT)
If a person is taking drugs that may affect their liver, then abnormal test results may indicate a need to reevaluate the dosage or choice of medication. When a person with liver disease is being monitored, then the healthcare practitioner will evaluate the results of the liver panel together to determine if liver function or damage is worsening or improving. For example, increasingly abnormal bilirubin, albumin, and/or PT may indicate a deterioration in liver function, while stable or improving results of these tests may indicate liver function preservation or improvement.
What tests may be done in follow up to an abnormal liver panel to help determine the cause of liver injury?
Depending on the results of the liver panel and other factors such as signs, symptoms and clinical and family history, a healthcare practitioner may suspect a particular cause of liver disorder and order follow-up tests. Some examples include:
Table 3. Follow up tests for abnormal liver function test results
| Suspected type of liver disorder | Other or follow-up tests |
| Viral infection | Hepatitis A, B, C, or E |
| Alcohol abuse/hepatitis | GGT, Ethanol |
| Toxic or drug-induced | Tests for toxins, drugs including drugs of abuse, acetaminophen |
| Wilson disease | Copper, Cerulosplasmin |
| Autoimmune | ANA, SMA, anti-LKM-1 |
| Chronic | Liver biopsy |
| Liver cancer | AFP, DCP |
Abbreviations: Alpha-fetoprotein (AFP); Antinuclear Antibody (ANA); Anti-Liver/Kidney Microsomal Antibodies Type 1 (Anti-LKM-1); Des-gamma-carboxy prothrombin (DCP); Gamma-glutamyl transferase (GGT); Smooth Muscle Antibody (SMA)
Liver function test results explained
Each of the liver function tests gives different information about your liver function. The results do not indicate a specific condition, but their combined results can indicate patterns usually seen with liver disease or damage.
If your liver function tests are abnormal, further testing might be necessary to work out what is causing the liver damage and/or disease.
Some liver function tests can be affected by conditions in the bones or elsewhere in the body. It is also possible that some liver function test results can be mildly abnormal when there is no problem at all.
You should discuss the results with your doctor to see what they mean in your particular situation.
Liver function test interpretation
A liver panel or liver function test may be used to screen for liver damage, especially if someone has a condition or is taking a drug that may affect the liver. A comprehensive metabolic panel, which is often performed as part of a general health checkup, may be ordered instead of a liver panel for routine screening. This group of tests includes most of the liver panel as well as additional tests that evaluate other organs and systems within the body.
A liver panel or one or more of its component tests may be used to help diagnose liver disease if a person has signs and symptoms that indicate possible liver dysfunction. If a person has a known condition or liver disease, testing may be performed at intervals to monitor the health of the liver and to evaluate the effectiveness of any treatments. A series of bilirubin tests, for instance, may be ordered to evaluate and monitor a jaundiced newborn.
Abnormal tests on a liver panel may prompt a repeat analysis of one or more tests, or of the whole panel, to see if the elevations or decreases persist and/or may indicate the need for additional testing to determine the cause of the liver dysfunction.
The liver panel usually consists of several tests that are run at the same time on a blood sample. These typically include:
- Alanine aminotransferase (ALT) – an enzyme mainly found in the liver; the best test for detecting hepatitis
- Alkaline phosphatase (ALP) – an enzyme related to the bile ducts but also produced by the bones, intestines, and during pregnancy by the placenta (afterbirth); often increased when bile ducts are blocked.
- Aspartate aminotransferase (AST) – an enzyme found in the liver and a few other organs, particularly the heart and other muscles in the body
- Bilirubin – two different tests of bilirubin often used together (especially if a person has jaundice): total bilirubin measures all the bilirubin in the blood; direct bilirubin measures a form that is conjugated (combined with another compound) in the liver.
- Albumin – measures the main protein made by the liver; the level can be affected by liver and kidney function and by decreased production or increased loss.
- Total protein (TP) – measures albumin and all other proteins in blood, including antibodies made to help fight off infections
Depending on the healthcare provider and the laboratory, other tests that may be included in a liver panel are:
- Gamma-glutamyl transferase (GGT) – another enzyme found mainly in liver cells
- Lactate dehydrogenase (LD) – an enzyme released with cell damage; found in cells throughout the body
- Prothrombin time (PT) – the liver produces proteins involved in the clotting (coagulation) of blood; the PT measures clotting function and, if abnormal, may indicate liver damage.
- Alpha-feto protein (AFP) – associated with regeneration or proliferation of liver cell
- Autoimmune antibodies (e.g., ANA, SMA, anti-LKM-1) – associated with autoimmune hepatitis
Alanine Aminotransferase (ALT)
Alanine aminotransferase (ALT) also called SGPT (Serum Glutamic-Pyruvic Transaminase) or GPT (Glutamic-Pyruvic Transaminase), is an enzyme found mostly in the cells of the liver and kidney. Much smaller amounts of it are also found in the heart and muscles. This test measures the level of ALT in the blood.
The function of ALT is to convert alanine, an amino acid found in proteins, into pyruvate, an important intermediate in cellular energy production. In healthy individuals, ALT levels in the blood are low. When the liver is damaged, ALT is released into the blood, usually before more obvious signs of liver damage occur, such as jaundice. This makes ALT a useful test for early detection of liver damage.
The liver is a vital organ located in the upper right-hand side of the abdominal area, just beneath the rib cage. It is involved in many important functions in the body. The liver helps to process the body’s nutrients, manufactures bile to help digest fats, produces many important proteins such as blood clotting factors and albumin, and breaks down potentially toxic substances into harmless ones that the body can use or eliminate.
A number of conditions can cause damage to liver cells, resulting in an increase in ALT. The test is most useful in detecting damage due to hepatitis or as a result of drugs or other substances that are toxic to the liver.
ALT is commonly tested in conjunction with aspartate aminotransferase (AST), another liver enzyme, as part of a liver panel. Both ALT and AST levels usually rise whenever the liver is being damaged, although ALT is more specific for the liver and, in some cases, may be the only one of the two to be increased. An AST/ALT ratio may be calculated to aid in distinguishing between different causes and severity of liver injury and to help distinguish liver injury from damage to heart or muscles.
When is ALT (alanine aminotransferase) ordered?
ALT may be ordered as part of a comprehensive metabolic panel when a person has a routine health examination.
A healthcare practitioner usually orders an ALT test (and several others) to evaluate a person who has signs and symptoms of a liver disorder. Some of these signs and symptoms may include:
- Weakness, fatigue
- Loss of appetite
- Nausea, vomiting
- Abdominal swelling and/or pain
- Jaundice
- Dark urine, light-colored stool
- Itching (pruritus)
ALT may also be ordered, either by itself or with other tests, for people who are at an increased risk for liver disease since many people with mild liver damage will have no signs or symptoms. Even without other symptoms, ALT will be increased with mild liver damage. Some examples include:
- Persons who have a history of known or possible exposure to hepatitis viruses
- Those who are heavy drinkers
- Individuals whose families have a history of liver disease
- Persons who take drugs that might damage the liver
- Persons who are overweight and/or have diabetes
A shot or injection of medicine into the muscle tissue, or strenuous exercise, may increase ALT levels.
Many drugs may raise ALT levels by causing liver damage in a very small percentage of patients taking the drug. This is true of both prescription drugs and some “natural” health products. Be sure to tell your healthcare provider about all of the drugs and/or health supplements you are taking.
When ALT is used to monitor the treatment of people who have liver disease, it may be ordered on a regular basis during the course of treatment to determine whether the therapy is effective.
How is ALT (alanine aminotransferase) used?
The alanine aminotransferase (ALT) test is typically used to detect liver injury. It is often ordered in conjunction with aspartate aminotransferase (AST) as part of a liver panel or comprehensive metabolic panel to screen for and/or help diagnose liver disease.
ALT is an enzyme found mostly in the cells of the liver and kidney. When the liver is damaged, ALT is released into the blood. This makes ALT a useful test for early detection of liver damage.
AST and ALT are considered to be two of the most important tests to detect liver injury, although ALT is more specific to the liver than is AST. Sometimes AST is compared directly to ALT and an AST/ALT ratio is calculated. This ratio may be used to distinguish between different causes of liver damage and to help recognize heart or muscle injury.
ALT values are often compared to the results of other tests such as alkaline phosphatase (ALP), total protein, and bilirubin to help determine which form of liver disease is present.
ALT is often used to monitor the treatment of persons who have liver disease, to see if the treatment is working, and may be ordered either by itself or along with other tests for this purpose.
What does abnormal ALT test result mean?
A low level of ALT in the blood is normal. Liver disease is the most common reason for higher than normal levels of ALT.
Very high levels of ALT (more than 10 times normal) are usually due to acute hepatitis, sometimes due to a viral infection. In acute hepatitis, ALT levels usually stay high for about 1-2 months but can take as long as 3-6 months to return to normal. Levels of ALT may also be markedly elevated (sometimes over 100 times normal) as a result of exposure to drugs or other substances that are toxic to the liver or in conditions that cause decreased blood flow (ischemia) to the liver.
ALT levels are usually not as high in chronic hepatitis, often less than 4 times normal. In this case, ALT levels often vary between normal and slightly increased, so the test may be ordered frequently to see if there is a pattern. Other causes of moderate increases in ALT include obstruction of bile ducts, cirrhosis (usually the result of chronic hepatitis or bile duct obstruction), heart damage, alcohol abuse, and with tumors in the liver.
ALT is often performed together with a test for AST or as part of a liver panel. For more about ALT results in relation to other liver tests, see the Liver Panel article.
In most types of liver diseases, the ALT level is higher than AST and the AST/ALT ratio will be low (less than 1). There are a few exceptions; the AST/ALT ratio is usually greater than 1 in alcoholic hepatitis, cirrhosis, and with heart or muscle injury and may be greater than 1 for a day or two after onset of acute hepatitis.
What conditions other than liver problems can cause increased ALT?
ALT is more specific for the liver than AST and so is much less affected by conditions affecting other parts of the body. Nevertheless, injury to organs other than the liver, such as the heart and skeletal muscle, can cause elevations of ALT. For example, small increases may be seen with skeletal muscle damage or heart attacks.
What other tests may be performed to help determine the cause of liver damage?
After a thorough physical exam and evaluation of a person’s medical history, there are several other tests that may be performed as follow up depending on what is suspected to be the cause of liver damage. Some of these include:
- Tests for hepatitis A, hepatitis B, and hepatitis C
- Testing for exposure to drugs and other substances toxic to the liver (see Drug Abuse Testing and Emergency and Overdose Drug Testing)
- Ethanol level
- Copper and ceruloplasmin for Wilson disease
- Iron tests and genetic tests for hereditary hemochromatosis
A liver biopsy may be performed to help determine the cause of liver injury and to evaluate the extent of liver damage.
How is the sample collected for testing?
A blood sample is drawn from a vein in the arm.
Is any test preparation needed to ensure the quality of the sample?
No test preparation is needed.
Aspartate Aminotransferase (AST)
Aspartate aminotransferase (AST) also called SGOT (Serum Glutamic-Oxaloacetic Transaminase) or GOT (Glutamic-Oxaloacetic Transaminase), is an enzyme found in cells throughout your body but mostly in your heart and liver and, to a lesser extent, in the kidneys and muscles. In healthy individuals, levels of AST in the blood are low. When liver or muscle cells are injured, they release AST into the blood. This makes AST a useful test for detecting or monitoring liver damage.
A number of conditions can cause injury to liver cells and may cause increases in AST. The test is most useful in detecting liver damage due to hepatitis, drugs toxic to the liver, cirrhosis, or alcoholism. AST, however, is not specific for the liver and may be increased in conditions affecting other parts of the body.
An aspartate aminotransferase (AST) test is often performed along with an alanine aminotransferase (ALT) test. Both are enzymes found in the liver that become elevated in the blood when the liver is damaged. A calculated AST/ALT ratio is useful for differentiating between different causes of liver injury and in recognizing when the increased levels may be coming from another source, such as heart or muscle injury.
When is AST (aspartate aminotransferase) ordered?
AST may be ordered as part of a comprehensive metabolic panel when someone has a routine health examination.
An AST test may be ordered along with several other tests when a person has signs and symptoms of a liver disorder. Some of these may include:
- Weakness, fatigue
- Loss of appetite
- Nausea, vomiting
- Abdominal swelling and/or pain
- Jaundice
- Dark urine, light-colored stool
- Itching (pruritus)
- Swelling in the legs and ankles
- Tendency to bruise easily
AST may also be ordered, either by itself or with other tests, for people who are at an increased risk for liver disease since many people with mild liver damage will have no signs or symptoms. Some examples include:
- Persons who might have been exposed to hepatitis viruses
- Persons who are heavy drinkers
- Persons who have a history of liver disease in their family
- Persons taking drugs that can damage the liver
- Persons who are overweight and/or have diabetes
Pregnancy, a shot or injection of medicine into muscle tissue, or even strenuous exercise may increase AST levels. Acute burns, surgery, and seizures may raise AST levels as well.
In rare instances, some drugs can damage the liver or muscle, increasing AST levels. This is true of both prescription drugs and some “natural” health products. Be sure to tell your healthcare practitioner about all of the drugs and/or health supplements that you are taking.
When AST is used to monitor treatment of persons with liver disease, it may be ordered on a regular basis during the course of treatment to determine whether the therapy is effective.
What does abnormal AST test result mean?
Low levels of AST in the blood are normal.
Very high levels of AST (more than 10 times normal) are usually due to acute hepatitis, sometimes due to a viral infection. With acute hepatitis, AST levels usually stay high for about 1-2 months but can take as long as 3-6 months to return to normal. Levels of AST may also be markedly elevated (often over 100 times normal) as a result of exposure to drugs or other substances that are toxic to the liver as well as in conditions that cause decreased blood flow (ischemia) to the liver.
With chronic hepatitis, AST levels are usually not as high, often less than 4 times normal, and are more likely to be normal than are ALT levels. AST often varies between normal and slightly increased with chronic hepatitis, so the test may be ordered frequently to determine the pattern. Such moderate increases may also be seen in other diseases of the liver, especially when the bile ducts are blocked, or with cirrhosis or certain cancers of the liver. AST may also increase after heart attacks and with muscle injury, usually to a much greater degree than ALT.
AST is often performed together with the ALT test or as part of a liver panel. For more about AST results in relation to other liver tests, see the Liver Panel article.
In most types of liver disease, the ALT level is higher than AST and the AST/ALT ratio will be low (less than 1). There are a few exceptions; the AST/ALT ratio is usually increased in alcoholic hepatitis, cirrhosis, hepatitis C virus-related chronic liver disease, and in the first day or two of acute hepatitis or injury from bile duct obstruction. With heart or muscle injury, AST is often much higher than ALT (often 3-5 times as high) and levels tend to stay higher than ALT for longer than with liver injury.
What conditions other than liver problems can cause increased AST?
Conditions that affect other organs, such as the heart and skeletal muscle, can cause elevations of AST. Mild to moderate increases may be seen with vigorous exercise and skeletal muscle injury or in conditions such as acute pancreatitis and heart attacks.
What other tests may be used to help determine the cause of liver damage?
After a thorough physical exam and evaluation of a person’s medical history, there are several other tests that may be performed as follow up depending on what is suspected to be the cause of liver damage. Some of these include:
- Tests for hepatitis A, hepatitis B, and hepatitis C
- Testing for exposure to drugs and other substances toxic to the liver
- Ethanol level
- Copper and ceruloplasmin for Wilson disease
- Iron tests and genetic tests for hereditary hemochromatosis
A liver biopsy may be performed to help determine the cause of liver injury and to evaluate the extent of liver damage.
How is the sample collected for testing?
A blood sample is drawn by needle from a vein in the arm.
Is any test preparation needed to ensure the quality of the sample?
No test preparation is needed.
Alkaline Phosphatase (ALP)
Alkaline phosphatase (ALP) is an enzyme found in several tissues throughout the body. The highest concentrations of ALP are present in the cells that comprise bone and the liver. Elevated levels of ALP in the blood are most commonly caused by liver disease or bone disorders. This test measures the level of ALP in the blood.
In the liver, ALP is found on the edges of cells that join to form bile ducts, tiny tubes that drain bile from the liver to the bowels, where it is needed to help digest fat in the diet. ALP in bone is produced by special cells called osteoblasts that are involved in the formation of bone. Each of the various tissue types produces distinct forms of ALP called isoenzymes.
Alkaline phosphatase (ALP) blood levels can be greatly increased, for example, in cases where one or more bile ducts are blocked. This can occur as a result of inflammation of the gallbladder (cholecystitis) or gallstones. Smaller increases of blood ALP are seen in liver cancer and cirrhosis, with use of drugs toxic to the liver, and in hepatitis.
Any condition causing excessive bone formation, including bone disorders such as Paget’s disease, can cause increased ALP levels. Children and adolescents typically have higher blood ALP levels because their bones are still growing. As a result, the ALP test must be interpreted with different reference (normal) values for children and for adults.
It is possible to distinguish between the different forms (isoenzymes) of ALP produced by different types of tissues in the body. If it is not apparent from clinical signs and symptoms whether the source of a high ALP test result is from liver or bone disease, then a test may be performed to determine which isoenzyme is increased in the blood.
When is ALP (alkaline phosphatase) ordered?
An ALP test may be ordered as part of routine laboratory testing, often with a group of other tests called a liver panel. It is also usually ordered along with several other tests when a person has symptoms of a liver or bone disorder.
Signs and symptoms of liver involvement may include:
- Weakness, fatigue
- Loss of appetite
- Nausea, vomiting
- Abdominal swelling and/or pain
- Jaundice
- Dark urine, light-colored stool
- Itching (pruritus)
Some examples of the signs and symptoms suggesting a bone disorder include:
- Bone and/or joint pain
- Increased frequency of fractures
- Deformed bones
How is ALP (alkaline phosphatase) used?
The alkaline phosphatase test (ALP) is used to help detect liver disease or bone disorders.
- In conditions affecting the liver, damaged liver cells release increased amounts of ALP into the blood. This test is often used to detect blocked bile ducts because ALP is especially high in the edges of cells that join to form bile ducts. If one or more of them are obstructed, for example by a tumor, then blood levels of ALP will often be high.
- Any condition that affects bone growth or causes increased activity of bone cells can affect ALP levels in the blood. An ALP test may be used, for example, to detect cancers that have spread to the bones or to help diagnose Paget’s disease, a condition that causes malformed bones. This test may also sometimes be used to monitor treatment of Paget’s disease or other bone conditions, such as vitamin D deficiency.
Pregnancy can increase ALP levels. Temporary elevations are also seen with healing fractures.
Children and adolescents normally have higher ALP levels than adults because their bones are growing, and ALP is often very high during a growth spurt, which occurs at different ages in boys and girls.
Some drugs may affect ALP levels. For example, oral contraceptives may decrease ALP levels while anti-epileptics may increase ALP levels.
If ALP results are increased but it is not clear whether this is due to liver or bone disease, tests for ALP isoenzyme may be done to determine the cause. A GGT test and/or a test for 5′-nucleotidase may also be done to differentiate between liver and bone disease. GGT and 5′-nucleotidase levels are increased in liver disease but not in bone disorders.
What does abnormal ALP test result mean?
High ALP usually means that either the liver has been damaged or a condition causing increased bone cell activity is present.
If other liver tests such as bilirubin, aspartate aminotransferase (AST), or alanine aminotransferase (ALT) are also high, usually the increased ALP is coming from the liver. If GGT or 5′-nucleotidase is also increased, then the high ALP is likely due to liver disease. If either of these two tests is normal, then the high ALP is likely due to a bone condition. Likewise, if calcium and/or phosphorus measurements are abnormal, usually the ALP is coming from bone.
If it is not clear from signs and symptoms or from other routine tests whether the high ALP is from liver or bone, then a test for ALP isoenzymes may be necessary to distinguish between bone and liver ALP.
- ALP in liver disease
ALP results are usually evaluated along with other tests for liver disease. In some forms of liver disease, such as hepatitis, ALP is usually much less elevated than AST and ALT. When the bile ducts are blocked (usually by gallstones, scars from previous gallstones or surgery, or by cancers), ALP and bilirubin may be increased much more than AST or ALT. ALP may also be increased in liver cancer.
- ALP in bone disease
In some bone diseases, such as Paget’s disease, where bones become enlarged and deformed, or in certain cancers that spread to bone, ALP may be increased.
If a person is being successfully treated for Paget’s disease, then ALP levels will decrease or return to normal over time. If someone with bone or liver cancer responds to treatment, ALP levels should decrease.
Moderately elevated ALP may result from other conditions, such as Hodgkin’s lymphoma, congestive heart failure, ulcerative colitis, and certain bacterial infections.
Low levels of ALP may be seen temporarily after blood transfusions or heart bypass surgery. A deficiency in zinc may cause decreased levels. A rare genetic disorder of bone metabolism called hypophosphatasia can cause severe, protracted low levels of ALP. Malnutrition or protein deficiency as well as Wilson disease could also be possible causes for lowered ALP.
What other tests are used to evaluate liver disorders?
There are other commonly used liver tests that measure other enzymes found in liver cells, such as alanine aminotransferase (ALT) and aspartate aminotransferase (AST). A test for bilirubin, a substance produced by the breakdown of red blood cells and removed from the body by the liver, may also be performed. Sometimes these tests (along with albumin and total protein testing) are run together as a liver panel. Other tests that may be performed individually or as part of a liver panel to detect or monitor liver disease include gamma-glutamyl transferase (GGT), lactate dehydrogenase (LDH), and prothrombin time (PT).
How is the sample collected for testing?
A blood sample is drawn by needle from a vein in the arm.
Is any test preparation needed to ensure the quality of the sample?
Fasting is preferred but not required for ALP test. Eating a meal can increase the ALP level slightly for a few hours in some people. It is usually better to do the test after fasting overnight. In this case, only water is permitted.
Gamma-Glutamyl Transferase (GGT)
Gamma-glutamyl transferase (GGT) is an enzyme found in many organs throughout your body, with the highest concentrations found in the liver. GGT is elevated in the blood in most diseases that cause damage to the liver or bile ducts. This test measures the level of GGT in a blood sample.
Normally, GGT is present in low levels, but when the liver is injured, the GGT level can rise. Gamma-glutamyl transferase (GGT) is usually the first liver enzyme to rise in the blood when any of the bile ducts that carry bile from the liver to the intestines become obstructed, for example, by tumors or stones. This makes it the most sensitive liver enzyme test for detecting bile duct problems.
However, the GGT test is not very specific and is not useful in differentiating between various causes of liver damage because it can be elevated with many types of liver diseases, such as liver cancer and viral hepatitis, as well as other non-hepatic conditions, such as acute coronary syndrome. For this reason, the GGT test is not recommended for routine use by itself. However, it can be useful in conjunction with other tests and in determining the cause of a high alkaline phosphatase (ALP) level, another enzyme found in the liver.
Both GGT and ALP are increased in liver diseases, but only ALP will be increased with diseases affecting bone tissue. Therefore, GGT can be used as a follow up to an elevated ALP to help determine if the high ALP result is due to liver or bone disease.
GGT levels are sometimes increased with consumption of even small amounts of alcohol. Higher levels are found more commonly in chronic heavy drinkers than in people who consume less than 2 to 3 drinks per day or who only drink heavily on occasion (binge drinkers). The GGT test may be used in evaluating someone for acute or chronic alcohol abuse.
When is GGT ordered?
A GGT test may be ordered when someone has an elevated ALP level. An ALP test may be ordered alone or as part of a routine liver panel to screen for liver damage, even if no symptoms are present. A GGT test may be ordered when results of the ALP test are high but other tests that are part of the liver panel (such as AST and ALT) are not increased.
GGT may be ordered along with or as a follow up to other liver function tests when a person has signs or symptoms that suggest liver disease. Some signs and symptoms of liver damage include:
- Weakness, fatigue
- Loss of appetite
- Nausea and vomiting
- Abdominal swelling and/or pain
- Jaundice
- Dark urine, light-colored stool
- Itching (pruritus)
GGT may also be ordered when someone with a history of alcohol abuse has completed alcohol treatment in order to monitor compliance with the treatment program.
Even small amounts of alcohol within 24 hours of a GGT test may cause a temporary increase in the GGT.
Smoking can also increase GGT.
Elevated GGT levels may be an indicator of cardiovascular disease and/or hypertension. Some studies have shown that people with increased GGT levels have an elevated risk of dying from heart disease, but the reason for this association is not yet known.
Drugs that may cause an elevated GGT level include phenytoin, carbamazepine, and barbiturates such as phenobarbital. Use of many other prescription and non-prescription drugs, including nonsteroidal anti-inflammatory drugs (NSAIDs), lipid-lowering drugs, antibiotics, histamine receptor blockers (used to treat excess stomach acid production), antifungal agents, antidepressants, and hormones such as testosterone, can increase GGT levels. Clofibrate and oral contraceptives can decrease GGT levels.
Levels of GGT increase with age in women, but not in men, and are always somewhat higher in men than in women.
How is GGT used?
The gamma-glutamyl transferase (GGT) test may be used to determine the cause of elevated alkaline phosphatase (ALP). Both ALP and GGT are elevated in disease of the bile ducts and in some liver diseases, but only ALP will be elevated in bone disease. Therefore, if the GGT level is normal in a person with a high ALP, the cause of the elevated ALP is most likely bone disease.
The GGT test is sometimes used to help detect liver disease and bile duct obstructions. It is usually ordered in conjunction with or as follow up to other liver tests such as ALT, AST, ALP, and bilirubin. (Read also about the Liver Panel.) In general, an increased GGT level indicates that a person’s liver is being damaged but does not specifically point to a condition that may be causing the injury.
GGT can be used to screen for chronic alcohol abuse (it will be elevated in about 75% of chronic drinkers) and to monitor for alcohol use and/or abuse in people who are receiving treatment for alcoholism or alcoholic hepatitis.
What does abnormal GGT test result mean?
An elevated GGT level suggests that a condition or disease is damaging the liver but does not indicate specifically what. In general, the higher the level, the greater the damage to the liver. Elevated GGT levels may be due to liver diseases, such as hepatitis or cirrhosis, but they may also be due to other conditions, such as congestive heart failure, diabetes, or pancreatitis. They may also be caused by alcohol abuse or use of drugs that are toxic to the liver.
A low or normal GGT test result indicates that it is unlikely that a person has liver disease or has consumed any alcohol.
A high GGT level can help rule out bone disease as the cause of an increased ALP level, but if GGT is low or normal, then an increased ALP is more likely due to bone disease.
Can my GGT level be elevated if I don’t have any symptoms?
Yes, GGT is very sensitive and can be increased when you don’t have symptoms. This elevation may be temporary, perhaps due to medications that you are taking or alcohol ingested within 24 hours of the test. If other liver enzymes are normal, your healthcare practitioner may just wait and then repeat the GGT test. If the GGT is very high and/or your other liver enzymes are elevated, it may be necessary to have more extensive testing to identify the cause.
I am an alcoholic, but I have quit drinking. Will my GGT ever go back to normal?
Over time, your GGT level will fall from whatever level it was at when you stopped drinking alcohol to within the normal range. This can take several weeks to more than a month. Abstaining from alcohol will decrease your chances of further damaging your liver and should allow your liver function to improve.
How is the sample collected for testing?
A blood sample is obtained by inserting a needle into a vein in the arm.
Is any test preparation needed to ensure the quality of the sample?
GGT levels fall after meals. You may be instructed to fast (have nothing to eat or drink except water) for at least 8 hours prior to the test. Alcohol and certain prescription medications can affect GGT levels, so you may be asked to abstain from them prior to the test as well.
Bilirubin
Bilirubin is an orange-yellow pigment, a waste product primarily produced by the normal breakdown of heme. Heme is a component of hemoglobin, which is found in red blood cells (RBCs). Bilirubin is ultimately processed by the liver to allow its elimination from the body. This test measures the amount of bilirubin in the blood to evaluate a person’s liver function or to help diagnose anemias caused by red blood cell destruction (hemolytic anemia).
Red blood cells normally degrade after about 120 days in circulation. As heme is released from hemoglobin, it is converted to bilirubin. This form of bilirubin is also called unconjugated bilirubin. Unconjugated bilirubin is carried by proteins to the liver; there, sugars are attached (conjugated) to bilirubin to form conjugated bilirubin. Conjugated bilirubin enters the bile and passes from the liver to the small intestines; there, it is further broken down by bacteria and eventually eliminated in the stool. Thus, the breakdown products of bilirubin give stool its characteristic brown color.
A small amount (approximately 250 to 350 milligrams) of bilirubin is produced daily in a normal, healthy adult. Most (85%) of bilirubin is derived from damaged or degraded red blood cells (RBCs), with the remaining amount derived from the bone marrow or liver. Normally, small amounts of unconjugated bilirubin are released into the blood, but virtually no conjugated bilirubin is present. Both forms can be measured or estimated by laboratory tests, and a total bilirubin result (a sum of these) may also be reported.
If the bilirubin level increases in the blood, a person may appear jaundiced, with a yellowing of the skin and/or whites of the eyes. The pattern of bilirubin test results can give the health practitioner information regarding the condition that may be present. For example, unconjugated bilirubin may be increased when there is an unusual amount of red blood cell destruction destruction (hemolysis) or when the liver is unable to process bilirubin (i.e., with liver diseases such as cirrhosis or inherited problems). Conversely, conjugated bilirubin can increase when the liver is able to process bilirubin but is not able to pass the conjugated bilirubin to the bile for removal; when this happens, the cause is often acute hepatitis or blockage of the bile ducts.
Increased total and unconjugated bilirubin levels are relatively common in newborns in the first few days after birth. This finding is called “physiologic jaundice of the newborn” and occurs because the newborn’s liver is not mature enough to process bilirubin yet. Usually, physiologic jaundice of the newborn resolves itself within a few days. However, in hemolytic disease of the newborn, red blood cell destructions may be destroyed because of blood incompatibilities between the baby and the mother; in these cases, treatment may be required because high levels of unconjugated bilirubin can damage the newborn’s brain.
A rare (about 1 in 10,000 births) but life-threatening congenital condition called biliary atresia can cause increased total and conjugated bilirubin levels in newborns. This condition must be quickly detected and treated, usually with surgery, to prevent serious liver damage that may require liver transplantation within the first few years of life. Some children may require liver transplantation despite early surgical treatment.
When is bilirubin test ordered?
A health practitioner usually orders a bilirubin test in conjunction with other laboratory tests (alkaline phosphatase [ALP], aspartate aminotransferase [AST], alanine aminotransferase [ALT]) when someone shows signs of abnormal liver function. A bilirubin level may be ordered when a person:
- Shows evidence of jaundice
- Has a history of drinking excessive amounts of alcohol
- Has suspected drug toxicity
- Has been exposed to hepatitis-causing viruses
Other symptoms that may be present include:
- Dark, amber-colored urine
- Nausea/vomiting
- Abdominal pain and/or swelling
- Fatigue and general malaise that often accompany chronic liver disease
Measuring and monitoring bilirubin in newborns with jaundice is considered standard medical care.
Tests for bilirubin may also be ordered when someone is suspected of having (or known to have) hemolytic anemia as a cause of anemia. In this case, it is often ordered along with other tests used to evaluate hemolysis, such as complete blood count, reticulocyte count, haptoglobin, and lactate dehydrogenase (LDH).
How is bilirubin test used?
A bilirubin test is used to detect an increased level in the blood. It may be used to help determine the cause of jaundice and/or help diagnose conditions such as liver disease, hemolytic anemia, and blockage of the bile ducts.
Bilirubin is an orange-yellow pigment, a waste product primarily produced by the normal breakdown of heme. Heme is a component of hemoglobin, which is found in red blood cells (RBCs). Bilirubin is ultimately processed by the liver to allow its elimination from the body. Any condition that accelerates the breakdown of RBCs or affects the processing and elimination of bilirubin may cause an elevated blood level.
Two forms of bilirubin can be measured or estimated by laboratory tests:
- Unconjugated bilirubin—when heme is released from hemoglobin, it is converted to unconjugated bilirubin. It is carried by proteins to the liver. Small amounts may be present in the blood.
- Conjugated bilirubin—formed in the liver when sugars are attached (conjugated) to bilirubin. It enters the bile and passes from the liver to the small intestines and is eventually eliminated in the stool. Normally, no conjugated bilirubin is present in the blood.
Usually, a chemical test is used to first measure the total bilirubin level (unconjugated plus conjugated bilirubin). If the total bilirubin level is increased, the laboratory can use a second chemical test to detect water-soluble forms of bilirubin, called “direct” bilirubin. The direct bilirubin test provides an estimate of the amount of conjugated bilirubin present. Subtracting direct bilirubin level from the total bilirubin level helps estimate the “indirect” level of unconjugated bilirubin. The pattern of bilirubin test results can give the healthcare provider information regarding the condition that may be present.
Though unconjugated bilirubin may be toxic to brain development in newborns (up to 2-4 weeks of age), it does not pose the same threat to older children and adults. In older children and adults, the “blood-brain barrier” is more developed and prevents bilirubin from gaining access to brain cells. Nevertheless, elevated bilirubin strongly suggests that a medical condition is present that must be evaluated and treated.
Bilirubin is not normally present in the urine. However, conjugated bilirubin is water-soluble and may be eliminated from the body through the urine if it cannot pass into the bile. Measurable bilirubin in the urine usually indicates blockage of liver or bile ducts, hepatitis, or some other form of liver damage and may be detectable early in disease; for this reason, bilirubin testing is integrated into common dipstick testing used for routine urinalysis.
Bilirubin concentrations tend to be slightly higher in males than females. African Americans routinely show lower bilirubin concentrations than non-African Americans. Strenuous exercise may increase bilirubin levels.
Drugs that can decrease total bilirubin include barbiturates, caffeine, penicillin, and high doses of salicylates (e.g. aspirin). The drug atazanavir increases unconjugated (indirect) bilirubin.
In adults and older children, bilirubin is measured to:
- Diagnose and/or monitor diseases of the liver and bile duct (e.g., cirrhosis, hepatitis, or gallstones)
- Evaluate people with sickle cell disease or other causes of hemolytic anemia; these people may have episodes called crises when excessive RBC destruction increases bilirubin levels.
In newborns with jaundice, bilirubin is used to distinguish the causes of jaundice.
- In both physiologic jaundice of the newborn and hemolytic disease of the newborn, only unconjugated (indirect) bilirubin is increased.
- In much less common cases, damage to the newborn’s liver from neonatal hepatitis and biliary atresia will increase conjugated (direct) bilirubin concentrations as well, often providing the first evidence that one of these less common conditions is present.
It is important that an elevated level of bilirubin in a newborn be identified and quickly treated because excessive unconjugated bilirubin damages developing brain cells. The consequences of this damage include mental retardation, learning and developmental disabilities, hearing loss, eye movement problems, and death.
What does abnormal bilirubin test result mean?
Adults and children
Increased total bilirubin that is mainly unconjugated (indirect) bilirubin may be a result of:
- Hemolytic or pernicious anemia
- Transfusion reaction
- Cirrhosis
- A relatively common inherited condition called Gilbert syndrome, due to low levels of the enzyme that produces conjugated bilirubin
If conjugated (direct) bilirubin is elevated more than unconjugated (indirect) bilirubin, there typically is a problem associated with decreased elimination of bilirubin by the liver cells. Some conditions that may cause this include:
- Viral hepatitis
- Drug reactions
- Alcoholic liver disease
Conjugated (direct) bilirubin is also elevated more than unconjugated (indirect) bilirubin when there is blockage of the bile ducts. This may occur, for example, with:
- Gallstones present in the bile ducts
- Tumors
- Scarring of the bile ducts
Rare inherited disorders that cause abnormal bilirubin metabolism such as Rotor, Dubin-Johnson, and Crigler-Najjar syndromes, may also cause increased levels of bilirubin.
Low levels of bilirubin are generally not concerning and are not monitored.
Newborns
An elevated bilirubin level in a newborn may be temporary and resolve itself within a few days to two weeks. However, if the bilirubin level is above a critical threshold or increases rapidly, an investigation of the cause is needed so appropriate treatment can be initiated. Increased bilirubin concentrations may result from the accelerated breakdown of red blood cells due to:
- Blood type incompatibility between the mother and her newborn
- Certain congenital infections
- Lack of oxygen (hypoxia)
- Diseases that can affect the liver
In most of these conditions, only unconjugated (indirect) bilirubin is increased. An elevated conjugated (direct) bilirubin is seen in the rare conditions of biliary atresia and neonatal hepatitis. Biliary atresia requires surgical intervention to prevent liver damage.
Are some people more at genetic risk of abnormal bilirubin levels?
Several inherited chronic conditions increase bilirubin levels in the blood and include Gilbert syndrome, Dubin-Johnson syndrome, Rotor syndrome, and Crigler-Najjar syndrome. The first three are usually mild, chronic conditions that can be aggravated under certain conditions but in general cause no significant health problems. For example, Gilbert syndrome is very common; about 1 in every 6 people has this genetic abnormality, but usually people with Gilbert syndrome do not have elevated bilirubin. Crigler-Najjar syndrome is the most serious inherited condition listed; this disorder is relatively rare, and some people with it may die.
How do you treat abnormal bilirubin levels and/or jaundice?
Treatment depends on the cause of the jaundice. In newborns, phototherapy (special light therapy), blood exchange transfusion, and/or certain drugs may be used to reduce the bilirubin level. In Gilbert, Rotor, and Dubin-Johnson syndromes, no treatment is usually necessary. Crigler-Najjar syndrome may respond to certain enzyme drug therapy or may require a liver transplant. Jaundice caused by an obstruction is often resolved by surgery. Jaundice due to cirrhosis is a result of long-term liver damage and does not respond well to any type of therapy other than liver transplantation.
How is the sample collected for testing?
In adults, blood is typically collected from a vein in the arm using a needle. In newborns, blood is often collected from a heelstick. Heelstick is a technique that uses a small, sharp blade to cut the skin on the infant’s heel so that a few drops of blood can be collected in a small tube. Non-invasive technology that measures bilirubin through the skin is available in some healthcare facilities; this instrument is called a transcutaneous bilirubin meter.
Is any test preparation needed to ensure the quality of the sample?
You may need to fast (nothing but water) for several hours before the test; fasting requirements vary by laboratory. Ask your lab or healthcare provider for instructions.
Lactate Dehydrogenase (LDH)
Lactate dehydrogenase (LDH or LD) is an enzyme involved in energy production that is found in almost all of the body’s cells, with the highest levels found in the cells of the heart, liver, muscles, kidneys, lungs, and in blood cells; bacteria also produce lactate dehydrogenase. This test measures the level of LDH in the blood or sometimes other body fluids.
Blood LDH (lactate dehydrogenase)
Only a small amount of lactate dehydrogenase (LDH) is usually detectable in the fluid portion of the blood (serum or plasma). Lactate dehydrogenase (LDH) is released from the cells into the serum when cells are damaged or destroyed. Thus, an lactate dehydrogenase (LDH) blood level is a non-specific marker for the presence of tissue damage somewhere in the body. By itself, it cannot be used to identify the underlying cause or location of the cellular damage. However, it may be used, in conjunction with other blood tests, to help evaluate for and/or monitor conditions that lead to tissue damage, such as liver or blood diseases or cancer.
Fluid LDH (lactate dehydrogenase)
Sometimes when there is injury, inflammation, or infection within a specific area of the body, such as the brain, heart or lungs, fluid will accumulate or constituents of the fluid present will change. The level of lactate dehydrogenase present in the fluid may be useful in determining the cause. For example, lactate dehydrogenase is typically high in cerebrospinal fluid when an individual has bacterial meningitis. The lactate dehydrogenase test can also be used, along with other tests, to determine whether fluid accumulation, for example around the heart or lungs or in the abdominal cavity, is due to injury or inflammation (exudate) or due to an imbalance of fluid pressure inside blood vessels and the protein level in blood (transudate).
When is LDH (lactate dehydrogenase) ordered?
Blood test
An lactate dehydrogenase level may be ordered, along with other tests such as a comprehensive metabolic panel, when a health practitioner suspects that a disease or condition is causing some degree of cellular or tissue damage. If lactate dehydrogenase is elevated, then more specific tests, such as ALT, AST or ALP, may help diagnose the condition and help determine which organs are involved. Once the acute or chronic problem is diagnosed, total lactate dehydrogenase levels may be ordered at regular intervals to monitor its progress and/or resolution.
Lactate dehydrogenase levels may also occasionally be ordered when an individual has experienced muscle trauma or injury or when a person has signs and symptoms of hemolytic anemia.
Lactate dehydrogenase testing may be ordered on a regular basis when an individual has been diagnosed with cancer.
Body fluid test
This test may be ordered, for example, when a person has signs and symptoms of meningitis or when someone has a buildup of fluid around the heart, lungs or in the abdomen.
Total Protein
Proteins are important building blocks of all cells and tissues; they are important for body growth, development, and health. They form the structural part of most organs and make up enzymes and hormones that regulate body functions. This test measures the total amount of the various types of proteins in the liquid (serum or plasma) portion of the blood.
Two classes of proteins are found in the blood, albumin and globulin. Albumin makes up about 60% of the total protein. Produced by the liver, albumin serves a variety of functions including as a carrier protein for many small molecules and ions, as a source of amino acids for tissue metabolism, and as the principle component involved in maintaining osmotic pressure (preventing fluid from leaking out of blood vessels).
The remaining 40% of proteins in the plasma are referred to as globulins. The globulin proteins are a varied group. They include enzymes, antibodies, hormones, carrier proteins, and numerous other types of proteins.
The level of total protein in the blood is normally a relatively stable value, reflecting a balance in loss of old protein molecules and production of new protein molecules.
Total protein may decrease in conditions:
- Where production of albumin or globulin proteins is impaired, such as malnutrition or severe liver disease
- That accelerate the breakdown or loss of protein, such as kidney disease (nephrotic syndrome)
- That increase/expand plasma volume (diluting the blood), such as congestive heart failure
Total protein may increase with conditions that cause:
- Abnormally high production of protein (e.g., inflammatory disorders, multiple myeloma)
- Dehydration
Prolonged application of a tourniquet during blood collection can result in a blood sample with a falsely elevated total protein (higher than the actual concentration in the circulation).
Drugs that may decrease protein levels include estrogens and oral contraceptives.
Some laboratories report total protein, albumin, and the calculated ratio of albumin to globulins, termed the albumin/globulin ratio. The albumin/globulin ratio is calculated from measured total protein, measured albumin, and calculated globulin (total protein – albumin).
Normally, there is a little more albumin than globulins, giving a normal albumin/globulin ratio of slightly over 1. The albumin/globulin ratio may change whenever the proportions of albumin and other proteins shift (increase or decrease) in relationship to each other. Because disease states affect the relative amounts of albumin and globulin, the albumin/globulin ratio may provide a clue as to the cause of the change in protein levels.
What are globulin proteins and how are they measured in blood?
Globulins are all the proteins in the blood other than albumin, and this group is comprised of hundreds of different types. These proteins are larger than albumin and are divided into alpha, beta and gamma globulins.
A protein electrophoresis test can be used to quantify the different groups of globulin proteins (see the article on Protein Electrophoresis and the table on Protein Groups). An immunofixation electrophoresis test can measure the different types of immunoglobulins (e.g., IgG, IgM, IgA) as can a quantitative immunoglobulins test.
Some globulin proteins can be measured directly using specific tests for the protein of interest. The tests are most valuable in instances where a specific protein is associated with a disease or condition. The specific protein tests may be ordered to provide information to the healthcare practitioner when particular signs and symptoms are present that suggest one of these diseases or conditions. A few examples of proteins associated with specific conditions are C-reactive protein (inflammation), fibrinogen (clotting disorders), ferritin (iron deficiency), and ceruloplasmin (Wilson disease).
When is total protein test ordered?
A total protein test is frequently ordered as part of a comprehensive metabolic panel when an individual undergoes a routine health checkup. Total protein may also be ordered to provide general information about a person’s nutritional status, such as when someone has undergone a recent, unexplained weight loss. It can be ordered along with several other tests to provide information when someone has symptoms that suggest a liver, kidney, or bone marrow disorder, or to investigate the cause of abnormal pooling of fluid in tissue (edema).
How is total protein test used?
Total protein and albumin tests are routinely included in the panels of tests performed as part of a health examination, such as a comprehensive metabolic panel, so they are frequently used to help evaluate a person’s overall health status.
Additionally, since total protein can be low, increased, or the component globulin proteins altered with many different diseases and disorders, total protein and albumin tests may be ordered in a variety of settings to help diagnose disease, to monitor changes in health status, and as a screen that may indicate the need for various follow-up tests.
Total protein measurements can reflect nutritional status and may be used to screen for and help diagnose kidney disease or liver disease, for example. Sometimes conditions are detected with routine testing before symptoms appear. If total protein is abnormal, further testing must be performed to identify which specific protein is abnormally low or high so that a specific diagnosis can be made. Some examples of follow-up tests include protein electrophoresis and quantitative immunoglobulins.
Some laboratories report total protein, albumin, and the calculated ratio of albumin to globulins, termed the albumin/globulin ratio. The albumin/globulin ratio is calculated from measured total protein, measured albumin, and calculated globulin (total protein – albumin). Because disease states affect the relative amounts of albumin and globulin, the albumin/globulin ratio may provide a clue as to the cause of the change in protein levels.
What does abnormal total protein test result mean?
Results of a total protein test are usually considered along with those from other tests of the comprehensive metabolic panel and will give the healthcare practitioner information on a person’s general health status with regard to nutrition and/or conditions involving major organs, such as the kidney and liver. However, if results are abnormal, further testing is usually required to help diagnose the disease affecting protein levels in the blood.
- A low total protein level can suggest a liver disorder, a kidney disorder, or a disorder in which protein is not digested or absorbed properly. Low levels may be seen in severe malnutrition and with conditions that cause malabsorption, such as celiac disease or inflammatory bowel disease (IBD).
- A high total protein level may be seen with chronic inflammation or infections such as viral hepatitis or HIV. It also may be associated with bone marrow disorders such as multiple myeloma.
- A low albumin/globulin ratio may reflect overproduction of globulins, such as seen in multiple myeloma or autoimmune diseases, or underproduction of albumin, such as may occur with cirrhosis, or selective loss of albumin from the circulation, as may occur with kidney disease (nephrotic syndrome).
- A high albumin/globulin ratio suggests underproduction of immunoglobulins as may be seen in some genetic deficiencies and in some leukemias.
- With a low total protein that is due to plasma expansion (dilution of the blood), the albumin/globulin ratio will typically be normal because both albumin and globulin will be diluted to the same extent.
Following an abnormal total protein result and depending on the suspected cause, more specific tests are typically performed to make an accurate diagnosis. Some examples include liver enzyme tests, renal panel, serum protein electrophoresis, or tests for celiac disease or inflammatory bowel disease.
Will a high protein diet raise my total protein level?
No, increasing your intake of protein will not increase your total protein test result.
Can protein be measured in samples other than blood?
Yes, a test for protein can be performed on many different types of body fluids. The purpose for testing and the meaning of results vary.
How is the sample collected for testing?
A blood sample is obtained by inserting a needle into a vein in the arm or by a fingerstick (for children and adults) or heelstick (for newborns).
Is any test preparation needed to ensure the quality of the sample?
No test preparation is needed.
Albumin
Albumin is a protein made by the liver. It makes up about 60% of the total protein in the blood and plays many roles. This test measures the level of albumin in the blood.
Albumin keeps fluid from leaking out of blood vessels; nourishes tissues; and transports hormones, vitamins, drugs, and substances like calcium throughout the body. Levels of albumin may decrease, to a greater or lesser degree, when conditions interfere with its production by the liver, increase protein breakdown, increase protein loss via the kidneys, and/or expand plasma volume (diluting the blood).
Two important causes of low blood albumin include:
- Severe liver disease—since albumin is produced by the liver, its level can decrease with loss of liver function; however, this typically occurs only when the liver has been severely affected.
- Kidney disease—one of the many functions of the kidneys is to conserve plasma proteins such as albumin so that they are not released along with waste products when urine is produced. Albumin is present in high concentrations in the blood, and when the kidneys are functioning properly, virtually no albumin is lost in the urine. However, if a person’s kidneys become damaged or diseased, they begin to lose their ability to conserve albumin and other proteins. This is frequently seen in chronic diseases, such as diabetes and hypertension. In nephrotic syndrome, very high amounts of albumin are lost through the kidneys.
When is albumin test ordered?
An albumin test is frequently ordered as part of a panel of tests performed for a health screening.
Albumin may be ordered, along with other tests, when a person has symptoms of a liver disorder, such as:
- Yellowing of eyes or skin (jaundice)
- Weakness, fatigue
- Unexplained weight loss
- Loss of appetite
- Abdominal swelling and/or pain
- Dark urine, light-colored stool
- Itching (pruritus)
This test may be ordered when a person has symptoms of nephrotic syndrome, such as:
- Swelling or puffiness, particularly around the eyes or in the face, wrists, abdomen, thighs or ankles
- Urine that is foamy, bloody, or coffee-colored
- A decrease in the amount of urine
- Problems urinating, such as a burning feeling or abnormal discharge during urination, or a change in the frequency of urination, especially at night
- Mid-back pain (flank), below the ribs, near where the kidneys are located
- High blood pressure (hypertension)
A healthcare practitioner may also order an albumin test to check or monitor a person’s nutritional status. However, since albumin concentrations respond to a variety of conditions in addition to malnutrition, a decrease in albumin needs to be evaluated carefully.
How is albumin test used?
An albumin test is routinely included in the panels of tests performed as part of a health examination, such as a comprehensive metabolic panel, so it is frequently used to help evaluate a person’s overall health status.
Additionally, since albumin can be low in many different diseases and disorders, it may be used in a variety of settings to help diagnose disease, to monitor changes in health status with treatment or with disease progression, and as a screen that may indicate the need for other kinds of testing.
Albumin is a protein made by the liver that keeps fluid from leaking out of blood vessels, nourishes tissues, and transports hormones, vitamins, drugs, and substances like calcium throughout the body.
An albumin test may be ordered as part of a liver panel to evaluate liver function or with a creatinine, blood urea nitrogen (BUN), or renal panel to evaluate kidney function. Albumin may also be ordered to evaluate a person’s nutritional status.
What does abnormal albumin test result mean?
Results of albumin testing are evaluated along with those from other tests done at the same time, such as the tests included in a comprehensive metabolic panel, or in follow up.
A low albumin level may be a warning and an indication that further investigation may be warranted. A low albumin may reflect a temporary condition that will resolve itself or may suggest an acute or chronic condition that requires medical intervention.
Levels of albumin may decrease, to a greater or lesser degree, when conditions interfere with its production, increase protein breakdown, increase protein loss, and/or expand plasma volume (diluting the blood). Depending on the person’s medical history, signs and symptoms, and physical exam, additional testing may be done to investigate a low result.
A low albumin can suggest liver disease. Liver enzyme tests or a liver panel may be ordered to determine exactly which type of liver disease may be present. A person may, however, have normal or near normal albumin levels with liver disease until the condition has reached an advanced stage. For example, in people with cirrhosis, albumin is typically (but not always) low whereas in most chronic liver diseases that have not progressed to cirrhosis, albumin is usually normal.
Low albumin levels can reflect diseases in which the kidneys cannot prevent albumin from leaking from the blood into the urine and being lost. In this case, the amount of albumin or protein in the urine also may be measured or tests for creatinine and blood urea nitrogen (BUN) or a renal panel may be ordered.
Low albumin levels can also be seen in inflammation, shock, and malnutrition. They may be seen with conditions in which the body does not properly absorb and digest protein, such as Crohns disease or celiac disease, or in which large volumes of protein are lost from the intestines.
A low albumin may also be seen in several other conditions, such as:
- Infection
- Burns
- Surgery
- Chronic illness
- Cancer
- Diabetes
- Hypothyroidism
- Carcinoid syndrome
- Plasma volume expansion due to congestive heart failure, sometimes pregnancy
High albumin levels can be seen with dehydration, although the test is not typically used to monitor or detect this condition.
Certain drugs increase albumin in the blood, including anabolic steroids, androgens, growth hormones, and insulin.
If someone is receiving large amounts of intravenous fluids, the results of this test may be inaccurate.
Is anyone at high risk for abnormal albumin levels?
Individuals who have chronic liver disease and kidney disorders are at highest risk for developing abnormal albumin levels. In addition, individuals whose gastrointestinal tract doesn’t absorb nutrients properly and individuals who have prolonged diarrhea can develop abnormal albumin levels.
Is there a home test for albumin levels?
Not for blood albumin; you can test for high albumin levels in urine with a dipstick purchased in a drug store.
What is the difference between serum/plasma albumin, prealbumin, and urine albumin tests?
Although the names are similar, albumin and prealbumin are completely different molecules. They are both proteins made by the liver, however, and both have been used historically to evaluate nutritional status. Serum/plasma (or blood) albumin is now more often used to screen for and help diagnose liver or kidney disease and is tested on a blood sample. The urine albumin test (in the past, called a microalbumin test) detects and measures albumin in the urine as an early indicator of kidney damage.
How is the sample collected for testing?
A blood sample is taken by a needle from a vein in the arm.
Is any test preparation needed to ensure the quality of the sample?
No test preparation is needed.
Prothrombin Time and International Normalized Ratio (PT/INR)
The prothrombin time (PT) is a test that helps evaluate a person’s ability to appropriately form blood clots. The international normalized ratio or INR is a calculation based on results of a PT that is used to monitor individuals who are being treated with the blood-thinning medication (anticoagulant) warfarin (Coumadin®).
A PT measures the number of seconds it takes for a clot to form in a person’s sample of blood after substances (reagents) are added. The PT is often performed with a partial thromboplastin time (PTT) and together they assess the amount and function of proteins called coagulation factors that are an important part of proper blood clot formation.
In the body, when there is an injury and bleeding occurs, the clotting process called hemostasis begins. This process involves in part a series of sequential chemical reactions called the coagulation cascade, in which coagulation or “clotting” factors are activated one after another and result in the formation of a clot. There must be a sufficient quantity of each coagulation factor, and each must function properly, in order for normal clotting to occur. Too little can lead to excessive bleeding; too much may lead to excessive clotting.
In a test tube during a laboratory test, there are two “pathways” that can initiate clotting, the so-called extrinsic and intrinsic pathways. Both of these then merge into a common pathway to complete the clotting process. The PT test evaluates how well all of the coagulation factors in the extrinsic and common pathways of the coagulation cascade work together. Included are: factors I (Fibrinogen), II (Prothrombin), V, VII and X. The PTT test evaluates those protein factors that are part of the intrinsic and common pathways: XII, XI, IX, VIII, X, V, II (prothrombin), and I (fibrinogen) as well as prekallikrein (PK) and high molecular weight kininogen (HK). The PT and PTT evaluate the overall ability to produce a clot in a reasonable amount of time and, if any of these factors are deficient in quantity or not functioning properly, the test results will be prolonged.
The prothrombin time (PT) test is usually measured in seconds and is compared to a normal range that reflects PT values in healthy individuals. Because the reagents used to perform the prothrombin time (PT) test vary from one laboratory to another and even within the same laboratory over time, the normal ranges also will fluctuate. To standardize results across different laboratories in the U.S. and the world, a World Health Organization (WHO) committee developed and recommended the use of the International Normalized Ratio (INR), calculated based on the PT test result, for people who are receiving the anticoagulant warfarin (Coumadin®).
The INR is a calculation that adjusts for changes in the prothrombin time (PT) reagents and allows for results from different laboratories to be compared. Most laboratories report both prothrombin time (PT) and INR values whenever a PT test is performed. The INR should be only applicable, however, for those taking the blood-thinning medication warfarin.
When is PT and INR ordered?
A prothrombin time (PT) and International Normalized Ratio (INR) are ordered on a regular basis when a person is taking the anticoagulant drug warfarin to ensure that the prescription is working properly and that the PT/INR is appropriately prolonged. There is no set frequency for doing the test. A health practitioner will order them often enough to make sure that the drug is producing the desired effect – that it is increasing the person’s clotting time to a therapeutic level without significant risk of excessive bleeding or bruising.
The PT may be ordered when a person who is not taking anticoagulant drugs has signs or symptoms of excessive bleeding or clotting, such as:
- Unexplained bleeding or easy bruising
- Nosebleeds
- Bleeding gums
- A blood clot in a vein or artery
- An acute condition such as disseminated intravascular coagulation (DIC) that may cause both bleeding and clotting as coagulation factors are used up at a rapid rate
- A chronic condition such as severe liver disease that may affect hemostasis
PT, along with partial thromboplastin time (PTT), may be ordered prior to surgery when the surgery carries an increased risk of blood loss and/or when the person has a clinical history of bleeding, such as frequent or excessive nosebleeds and easy bruising, which may indicate the presence of a bleeding disorder.
How is prothrombin time (PT) used?
The prothrombin time (PT) is used, often along with a partial thromboplastin time (PTT), to help diagnose the cause of unexplained bleeding or inappropriate blood clots. The international normalized ratio (INR) is a calculation based on results of a PT and is used to monitor individuals who are being treated with the blood-thinning medication (anticoagulant) warfarin (Coumadin®).
Several proteins called coagulation factors are involved in the process that the body uses to form blood clots to help stop bleeding (hemostasis). When an injury occurs and bleeding begins, some coagulation factors are activated in a sequence of steps (coagulation cascade) that eventually help to form a clot. There must be a sufficient quantity of each coagulation factor, and each must function properly, in order for normal clotting to occur. Too little can lead to excessive bleeding; too much may lead to excessive clotting. (See the “What is being tested?” section for more on this.)
The PT and INR are used to monitor the effectiveness of the anticoagulant warfarin. This drug affects the function of the coagulation cascade and helps inhibit the formation of blood clots. It is prescribed on a long-term basis to people who have experienced recurrent inappropriate blood clotting. The goal of warfarin therapy is to maintain a balance between preventing clots and causing excessive bleeding. This balance requires careful monitoring. The INR can be used to adjust a person’s drug dosage to get the PT into the desired range that is right for the person and his or her condition.
Warfarin may be prescribed for conditions such as:
- Irregular heartbeat (atrial fibrillation)
- The presence of artificial heart valves
- Deep vein thrombosis (DVT), pulmonary embolism (PE)
- Antiphospholipid syndrome
- Occasionally, in heart attacks with certain risk factors
The PT test may be used along with a PTT as the starting points for investigating excessive bleeding or clotting disorders. The PT evaluates the coagulation factors VII, X, V, II and I (fibrinogen). The PTT test evaluates coagulation factors XII, XI, IX, VIII, X, V, II (prothrombin), and I (fibrinogen) as well as prekallikrein (PK) and high molecular weight kininogen (HK). By evaluating the results of the PT and PTT together, a health practitioner can gain clues as to what bleeding or clotting disorder may be present. These tests are not diagnostic by themselves but usually provide information on whether further tests may be needed.
Examples of other testing that may be done along with a PT and PTT or in follow up to abnormal results include:
- Platelet count – to determine if platelets are decreased, which can cause excessive bleeding
- Thrombin time testing – sometimes ordered to help rule out a fibrinogen abnormality
- Fibrinogen testing – may be done to rule out a low level or dysfunction of fibrinogen as a cause of a prolonged PT
- Coagulation factor tests – these measure the activity (function) of coagulation factors. They can detect reduced levels of the protein or proteins that don’t work properly (have reduced function). Rarely, the antigen level (quantity) of a coagulation factor may also be measured.
- von Willebrand factor – sometimes ordered to help determine if von Willebrand disease is the cause of a prolonged PTT
Based on carefully obtained patient histories, the PTT and PT tests are sometimes selectively performed as pre-surgical or before other invasive procedures to screen for potential bleeding tendencies.
What does abnormal prothrombin time (PT) test result mean?
For people taking warfarin, most laboratories report prothrombin time (PT) results that have been adjusted to the INR. These people should have an INR of 2.0 to 3.0 for basic “blood-thinning” needs. For some who have a high risk of a blood clot, the INR needs to be higher – about 2.5 to 3.5.
The test result for a PT depends on the method used, with results measured in seconds and compared to the normal range established and maintained by the laboratory that performs the test. This normal range represents an average value of healthy people who live in that area and will vary somewhat from lab to lab. Someone who is not taking warfarin would compare their PT test result to the normal range provided with the test result by the laboratory performing the test.
A prolonged prothrombin time (PT) means that the blood is taking too long to form a clot. This may be caused by conditions such as liver disease, vitamin K deficiency, or a coagulation factor deficiency. The prothrombin time (PT) result is often interpreted with that of the partial thromboplastin time (PTT) in determining what condition may be present.
Table 4. Interpretation of PT and PTT in Patients with a Bleeding or Clotting Syndrome
| PT result | PTT result | Examples of conditions that may be present |
|---|---|---|
| Prolonged | Normal | Liver disease, decreased vitamin K, decreased or defective factor VII, chronic low-grade disseminated intravascular coagulation (DIC), anticoagulation drug (warfarin) therapy |
| Normal | Prolonged | Decreased or defective factor VIII, IX, XI, or XII, von Willebrand disease (severe type), presence of lupus anticoagulant, autoantibody against a specific factor (e.g., factor VIII) |
| Prolonged | Prolonged | Decreased or defective factor I, II, V or X, severe liver disease, acute DIC, warfarin overdose |
| Normal | Normal or slightly prolonged | May indicate normal hemostasis; however, PT and PTT can be normal in conditions such as mild deficiencies in coagulation factor(s) and mild form of von Willebrand disease. Further testing may be required to diagnose these conditions. |
Some consumed substances, such as alcohol, can affect the PT and INR tests. Some antibiotics can increase the PT and INR. Barbiturates, oral contraceptives and hormone-replacement therapy (HRT), and vitamin K (either in a multivitamin or liquid nutrition supplement) may decrease PT. Certain foods, such as beef and pork liver, green tea, broccoli, chickpeas, kale, turnip greens, and soybean products, contain large amounts of vitamin K and can alter PT results. It is important that a healthcare provider know about all of the drugs, supplements, and foods that a person has ingested recently so that the PT and INR results are interpreted and used correctly.
Some laboratories will report a PT as a percentage of normal, although this is not a common practice.
Can I do prothrombin time (PT) and INR test at home?
Yes, if you will be taking warfarin for an extended period of time. The Food and Drug Administration has approved several home PT and INR testing systems. However, home testing is usually done in the context of a home-based coagulation management program that involves patient training and defined response and management protocols.
Should I have it done at the same time of day?
It is not generally necessary to have your PT and INR measured at a particular time of day. It is, however, important that you take your warfarin medication at the same time each day to maintain a continuous level. If your healthcare provider increases or decreases your dosage, he or she may want you to have your blood rechecked in a couple of days or so to judge the effect of the dosage change on your PT/INR (it is not an immediate effect).
My PT results vary sometimes, yet my doctor doesn’t change my prescription. Why?
Illness, change in diet, and some medications (as mentioned above) can alter PT results. Certain foods, such as beef and pork liver, green tea, broccoli, chickpeas, kale, turnip greens, and soybean products contain large amounts of vitamin K and can alter PT results. The blood collection technique and the difficulty in obtaining the blood sample can also affect test results. If your healthcare provider has concerns about the stability of your PT/INR, he or she may test your blood more frequently.
How is the sample collected for testing?
A blood sample is obtained by inserting a needle into a vein in the arm or, sometimes, from a fingerstick.
Is any test preparation needed to ensure the quality of the sample?
No test preparation is needed. If a person is receiving anticoagulant therapy, the specimen should be collected before the daily dose is taken.
Lactate Dehydrogenase (LDH)
Lactate dehydrogenase (LDH or LD) is an enzyme involved in energy production that is found in almost all of the body’s cells, with the highest levels found in the cells of the heart, liver, muscles, kidneys, lungs, and in blood cells; bacteria also produce lactate dehydrogenase. This test measures the level of lactate dehydrogenase in the blood or sometimes other body fluids.
Blood lactate dehydrogenase
Only a small amount of lactate dehydrogenase is usually detectable in the fluid portion of the blood (serum or plasma). Lactate dehydrogenase is released from the cells into the serum when cells are damaged or destroyed. Thus, an lactate dehydrogenase blood level is a non-specific marker for the presence of tissue damage somewhere in the body. By itself, it cannot be used to identify the underlying cause or location of the cellular damage. However, it may be used, in conjunction with other blood tests, to help evaluate for and/or monitor conditions that lead to tissue damage, such as liver or blood diseases or cancer.
Fluid lactate dehydrogenase
Sometimes when there is injury, inflammation, or infection within a specific area of the body, such as the brain, heart or lungs, fluid will accumulate or constituents of the fluid present will change. The level of lactate dehydrogenase present in the fluid may be useful in determining the cause. For example, lactate dehydrogenase is typically high in cerebrospinal fluid when an individual has bacterial meningitis. The lactate dehydrogenase test can also be used, along with other tests, to determine whether fluid accumulation, for example around the heart or lungs or in the abdominal cavity, is due to injury or inflammation (exudate) or due to an imbalance of fluid pressure inside blood vessels and the protein level in blood (transudate).
When is LDH (lactate dehydrogenase) ordered?
Blood test
An lactate dehydrogenase level may be ordered, along with other tests such as a comprehensive metabolic panel, when a health practitioner suspects that a disease or condition is causing some degree of cellular or tissue damage. If lactate dehydrogenase is elevated, then more specific tests, such as ALT, AST or ALP, may help diagnose the condition and help determine which organs are involved. Once the acute or chronic problem is diagnosed, total lactate dehydrogenase levels may be ordered at regular intervals to monitor its progress and/or resolution.
lactate dehydrogenase levels may also occasionally be ordered when an individual has experienced muscle trauma or injury or when a person has signs and symptoms of hemolytic anemia.
lactate dehydrogenase testing may be ordered on a regular basis when an individual has been diagnosed with cancer.
Body fluid test
This test may be ordered, for example, when a person has signs and symptoms of meningitis or when someone has a buildup of fluid around the heart, lungs or in the abdomen.
How is LDH (lactate dehydrogenase) test used?
A lactate dehydrogenase test is a non-specific test that may be used in the evaluation of a number of diseases and conditions. Lactate dehydrogenase is an enzyme that is found in almost all of the body’s cells (as well as in bacteria) and is released from cells into the fluid portion of blood (serum or plasma) when cells are damaged or destroyed. Thus, the blood level of lactate dehydrogenase is a general indicator of tissue and cellular damage. The level of lactate dehydrogenase may also rise in other types of body fluids (e.g., cerebrospinal fluid, pleural fluid, etc.) in the presence of certain diseases.
A lactate dehydrogenase blood test may be used:
- As a general indicator of the existence and severity of acute or chronic tissue damage
- To detect and monitor progressive conditions such as anemia, including hemolytic anemia and megaoloblastic anemia, or severe infections
- To help stage, determine prognosis, and/or monitor treatment (i.e., chemotherapy) of cancers, such as germ cell tumors (e.g., some types of testicular cancer and ovarian cancer), lymphoma, leukemia, melanoma, and neuroblastoma
An lactate dehydrogenase test is performed on body fluids for a few different reasons:
- To help evaluate cerebrospinal fluid and distinguish between bacterial or viral meningitis
- To evaluate other body fluids such as pleural, peritoneal or pericardial fluid and help determine whether the accumulation of fluid is due to injury and inflammation (exudate) or due to an imbalance of pressure within blood vessels and the amount of protein in the blood (transudate). This information is helpful in guiding treatment.
What does abnormal LDH (lactate dehydrogenase) test result mean?
Blood test
Elevated levels of lactate dehydrogenase usually indicate some type of tissue damage. lactate dehydrogenase levels typically will rise as the cellular destruction begins, peak after some time period, and then begin to fall. lactate dehydrogenase levels are elevated in a wide variety of conditions, reflecting its widespread tissue distribution.
An elevated level of lactate dehydrogenase may be seen with:
- Hemolytic anemia
- Pernicious anemia (megaloblastic anemia)
- Infections such as infectious mononucleosis (mono), meningitis, encephalitis, HIV
- Sepsis
- Intestinal and lung (pulmonary) infarction
- Acute kidney disease
- Acute liver disease
- Acute muscle injury
- Pancreatitis
- Bone fractures
- Testicular cancer, lymphoma or other cancers
A high lactate dehydrogenase in the blood may indicate that treatment for cancer (e.g., chemotherapy) has not been successful. A high level is predictive of a poorer outlook for survival for those with cancer. With some chronic and progressive conditions, moderately elevated lactate dehydrogenase blood levels may persist. Low and normal levels of lactate dehydrogenase do not usually indicate a problem. Low levels are sometimes seen when someone ingests large amounts of ascorbic acid (vitamin C).
Many things can affect blood lactate dehydrogenase results that are not necessarily a cause for concern. For example:
- Strenuous exercise can cause temporary elevations in lactate dehydrogenase.
- Hemolysis of the blood specimen can cause falsely elevated results. This may happen if the specimen is handled roughly, stored in extreme temperatures, or if the sample was difficult to collect.
- If a person’s platelet count is increased, serum lactate dehydrogenase can be artificially high and not reflective of the lactate dehydrogenase actually present in the circulation.
Historically, the lactate dehydrogenase test was used to help diagnose and monitor a heart attack, but the test for troponin has largely replaced lactate dehydrogenase in this role. lactate dehydrogenase is not specific for damage to the heart and is no longer recommended for evaluating people with suspected acute coronary syndrome.
Body fluids:
- Cerebrospinal fluid—a high lactate dehydrogenase indicates that meningitis is likely caused by bacteria, while a low or normal level indicates viral meningitis is more likely.
- A high lactate dehydrogenase indicates that pericardial fluid, peritoneal or pleural fluid is an exudate, while a low level indicates it is transudate. Transudates are usually caused by congestive heart failure or cirrhosis. Exudates have several possible causes and usually require additional testing to determine the cause. Read more about these tests by accessing the specific fluid article listed under Related Tests (above).
If the lactate dehydrogenase test is not specific, then how can it be clinically useful?
The lactate dehydrogenase test can be useful to a health practitioner as a warning because it indicates that cellular injury is occurring. In a similar fashion, tests such as a C-reactive protein (CRP) warn that inflammation is occurring somewhere in the body.
Is there anything I can do to lower my lactate dehydrogenase level?
No, LDH is an indicator of injury that will typically return to normal when the underlying condition resolves. If someone has a chronic condition with ongoing tissue damage, such as may occur with liver disease, then increased lactate dehydrogenase concentrations may persist.
What is an lactate dehydrogenase isoenzymes test?
A test for lactate dehydrogenase isoenzymes is rarely ordered and not widely available nowadays. In the past, the test was used to help diagnose and monitor heart attacks, but it has been replaced by the test for troponin. Though not a routine test, it may be used in differential diagnosis to help determine which organs are likely affected by tissue damage when the cause of an elevated total lactate dehydrogenase is not clear and cannot be determined using other specific tests.
Lactate dehydrogenase exists in five different forms called isoenzymes. Although there is some overlap, each of the five lactate dehydrogenase isoenzymes tends to be concentrated in specific body tissues. In general, the isoenzyme locations tend to be:
- LD-1: heart, red cells, kidneys, germ cells
- LD-2: heart, red blood cells, kidneys (lesser amounts than LD-1)
- LD-3: lungs and other tissues
- LD-4: white blood cells, lymph nodes, muscles, liver (lesser amounts than LD-5)
- LD-5: liver, skeletal muscle
Determining which isoenzyme is elevated in the blood may give clues to where tissue damage is occurring in the body and/or which organs may be affected.
How is the sample collected for testing?
A blood sample is obtained by inserting a needle into a vein in the arm. Sometimes a special procedure may be performed to collect body fluid from the site affected (e.g., cerebrospinal fluid, pleural fluid, peritoneal fluid, etc.).
Is any test preparation needed to ensure the quality of the sample?
No test preparation is needed.
Alpha-fetoprotein (AFP) Tumor Marker
Alpha-fetoprotein (AFP) is a protein produced primarily by the liver in a developing baby (fetus) and the portion of a developing embryo that is similar to the yolk cavity in bird eggs (yolk sac tissues). AFP levels are typically elevated when a baby is born and then decline rapidly. Liver damage and certain cancers can increase AFP concentrations significantly. This test measures the level of AFP in the blood.
Alpha-fetoprotein (AFP) is produced whenever liver cells are regenerating. With chronic liver diseases, such as hepatitis and cirrhosis, AFP may be chronically elevated. Very high concentrations of AFP may be produced by certain tumors. This characteristic makes the AFP test useful as a tumor marker. Increased amounts of AFP are found in many people with a type of liver cancer called hepatocellular carcinoma and in a liver cancer occurring in infants called hepatoblastoma. They are also found in some people with cancers of the testicles or ovaries.
Alpha-fetoprotein (AFP) exists in several different variants. The standard AFP test is for a total AFP, one that measures all of the AFP variants together. This is the primary AFP test used in the United States.
One of the AFP variants is called L3 because of its ability, in the laboratory, to bind to a particular protein called Lens culinaris agglutinin. The AFP-L3% test is a relatively new test that compares the amount of AFP-L3 to the total amount of AFP. An increase in the percentage of L3 is associated with increased risk of developing hepatocellular carcinoma in the near future and of having a poorer prognosis, as the L3-related cancers tend to be more aggressive.
Among patients with low total AFP, AFP-L3 can be higher in those with hepatocellular carcinoma than patients with benign liver diseases. Tumor markers including total AFP and AFP-L3 are used in addition to ultrasound for surveillance of hepatocellular carcinoma in Japan. This practice is different from that in the U.S. and Europe, but the two tests are occasionally ordered by healthcare practitioners in the U.S.
When is Alpha-fetoprotein (AFP) ordered?
A healthcare practitioner may order an AFP blood test:
- When it is suspected that someone has liver cancer or certain cancers of the testicles or ovaries; cancer may be suspected when, for example, lumps are felt in the abdominal area during a physical exam or when imaging tests detect possible tumors.
- When someone who has been diagnosed with and treated for a cancer of the liver, testicles, or ovaries is being monitored for the effectiveness of treatment
- When someone is being monitored for cancer recurrence
- To follow up patients with chronic hepatitis or liver cirrhosis
An AFP-L3% is sometimes ordered to help evaluate the risk of hepatocellular carcinoma when a person has chronic liver disease or to test the effectiveness of treatment of hepatocellular carcinoma or monitor for its recurrence.
How is alpha-fetoprotein (AFP) used?
Alpha-fetoprotein (AFP) is used as a tumor marker to help detect and diagnose cancers of the liver, testicles, and ovaries. Though the test is often ordered to monitor people with chronic liver diseases such as cirrhosis, chronic hepatitis B or hepatitis C because they have an increased lifetime risk of developing liver cancer, most current guidelines do not recommend this use. A healthcare practitioner may order an AFP test, along with imaging studies, to try to detect liver cancer when it is in its earliest and most treatable stages.
If a person has been diagnosed with hepatocellular carcinoma or another form of AFP-producing cancer, an AFP test may be ordered periodically to help monitor the person’s response to therapy and to monitor for cancer recurrence.
An AFP-L3% is sometimes also ordered to compare the amount of the AFP variant called AFP-L3 to the total amount of AFP. The AFP-L3% test is not yet widely used in the U.S. but has gained wider acceptance in other countries such as Japan. The test is used to help evaluate the risk of developing hepatocellular carcinoma, especially in those with chronic liver disease, and also to evaluate response of hepatocellular carcinoma to treatment.
What does abnormal alpha-fetoprotein (AFP) test result mean?
Increased alpha-fetoprotein (AFP) levels may indicate the presence of cancer, most commonly liver cancer, cancer of the ovary, or germ cell tumor of the testicles. However, not every liver, ovarian, or testicular cancer will produce significant quantities of AFP.
Elevated levels may sometimes be seen with other cancers such as stomach, colon, lung, breast, and lymphoma, although it is rarely ordered to evaluate these conditions. Other diseases such as cirrhosis and hepatitis can also cause increased levels.
When AFP is used as a monitoring tool, decreasing levels indicate a response to treatment. If concentrations after cancer treatment do not significantly decrease, usually to normal or near normal levels, then some of the tumor tissue may still be present.
If AFP concentrations begin to increase, then it is likely that the cancer is recurring. However, since AFP can be increased in hepatitis or cirrhosis, AFP levels can sometimes be misleading. If AFP levels are not elevated prior to treatment, then the test will not generally be useful to monitor the effectiveness of treatment or to monitor for recurrence.
When the AFP concentrations of people with chronic liver disease go from normal or moderately elevated to greatly elevated, their risk of developing liver cancer increases. When total AFP and AFP-L3% are significantly elevated, then the affected person has an increased risk of having or developing hepatocellular carcinoma in the next year or two. However, both AFP and AFP-L3% concentrations can be elevated, and fluctuate, in people with chronic hepatitis and cirrhosis. In these cases, a sharp increase in AFP is more important than the actual numerical value of the test result.
Not every person with increased AFP and AFP-L3% test results has cancer or will develop liver cancer. The AFP and AFP-L3% tests are not diagnostic per se; they are indicators. They must be used in conjunction with information from a medical history and physical examination as well as histopathological examination and imaging studies to look for the development of tumors.
Although these tests can provide useful information, they are not as specific or sensitive as healthcare practitioners would wish. AFP can temporarily increase whenever the liver is injured and regenerating, and moderate elevations can be seen with a variety of conditions. Because of this, AFP testing cannot be used solely to diagnose cancer. In addition, not every cancer will produce AFP, so a person could still have cancer even when the AFP is normal. For these reasons, the AFP test should not be used to screen the general population for cancer.
AFP is not only a tumor marker. Because AFP is produced by the fetus, levels are normally higher in pregnant women and in their newborns.
If my AFP is abnormal, do I need other tests?
If you have chronic liver infection or damage and your AFP suddenly rises, or if it is very elevated, your healthcare practitioner will usually ask for a study to look at your liver, such as an ultrasound exam, a CT scan, an MRI scan, or a biopsy for histopathological evaluation of tumor tissues. The scans can usually spot liver cancers if they are present. Your healthcare practitioner may also order a blood test for des-gamma carboxy prothrombin (DCP), which is also known as prothrombin induced by vitamin K absence-II (PIVKA-II), to help detect liver cancer and monitor patients with hepatocellular carcinoma.
What are the risk factors for hepatocellular carcinoma?
This cancer usually occurs in people who have chronic scarring of the liver, called cirrhosis. Most commonly, this is caused by chronic infection from one of two viruses: hepatitis B or hepatitis C. Alcohol abuse also increases the risk of developing cirrhosis. Some inherited diseases, especially a disorder called hemochromatosis (in which the body absorbs too much iron, which gets deposited in liver among other organs), can cause cirrhosis and, in time, hepatocellular carcinoma, as can non-alcoholic steatohepatitis (NASH), which is fat deposition in the liver, along with inflammation and damage.
How is the sample collected for testing?
A blood sample is taken by needle from a vein in the arm.
Is any test preparation needed to ensure the quality of the sample?
No test preparation is needed.
Can an AFP test be performed at home or in my healthcare practitioner’s office?
AFP is not available as a home test and it is not typically performed in a healthcare practitioner’s office. Testing is done by either a hospital laboratory or a reference laboratory.
Antinuclear Antibody (ANA)
Antinuclear antibodies (ANA) are a group of antibodies produced by a person’s immune system when it fails to adequately distinguish between “self” and “nonself.” Antinuclear antibodies (ANA) are autoantibodies that are directed against certain components found in the nucleus of a cell, hence the name “antinuclear”. These antibodies, known as autoantibodies, attack the body’s own healthy cells and cause signs and symptoms such as tissue and organ inflammation, joint and muscle pain, and fatigue. ANA specifically target substances found in the nucleus of a cell, hence the name “antinuclear.” The ANA test identifies the presence of these autoantibodies in the blood.
The presence of ANA may be a marker of an autoimmune process and is associated with several autoimmune disorders but is most commonly seen with the autoimmune disorder systemic lupus erythematosus (SLE).
The ANA test is one of the primary tests for helping to diagnose a suspected autoimmune disorder or ruling out other conditions with similar signs and symptoms. As such, it is often followed by other tests for autoantibodies that may help to establish a diagnosis. These may include, for example, an ENA panel, anti-dsDNA, anti-centromere and/or anti-histone test.
When is antinuclear antibody (ANA) ordered?
The antinuclear antibody (ANA) test is ordered when someone shows signs and symptoms that are associated with a systemic autoimmune disorder. People with autoimmune disorders can have a variety of symptoms that are vague and non-specific and that change over time, progressively worsen, or alternate between periods of flare ups and remissions. Some examples of signs and symptoms include:
- Low-grade fever
- Persistent fatigue, weakness
- Arthritis-like pain in one or more joints
- Red rash (for lupus, one resembling a butterfly across the nose and cheeks)
- Skin sensitivity to light
- Hair loss
- Muscle pain
- Numbness or tingling in the hands or feet
- Inflammation and damage to organs and tissues, including the kidneys, lungs, heart, lining of the heart, central nervous system, and blood vessels
How is antinuclear antibody (ANA) used?
The antinuclear antibody (ANA) test is used as a primary test to help evaluate a person for autoimmune disorders that affect many tissues and organs throughout the body (systemic) and is most often used as one of the tests to help diagnose systemic lupus erythematosus (SLE).
Antinuclear antibody (ANA) are a group of autoantibodies produced by a person’s immune system when it fails to adequately distinguish between “self” and “nonself.” They target substances found in the nucleus of a cell and cause organ and tissue damage.
Depending on a person’s signs and symptoms and the suspected disorder, ANA testing may be used along with or followed by other autoantibody tests. Some of these tests are considered subsets of the general ANA test and detect the presence of autoantibodies that target specific substances within cell nuclei, including anti-dsDNA, anti-centromere, anti-nucleolar, anti-histone and anti-RNA antibodies. An ENA panel may also be used in follow up to an ANA.
These supplemental tests are used in conjunction with a person’s clinical history to help diagnose or rule out other autoimmune disorders, such as Sjögren syndrome, polymyositis and scleroderma.
Different laboratories may use different test methods to detect ANA. Two common methods include immunoassay and indirect fluorescent antibody (IFA). IFA is considered the gold standard. Some laboratories will use immunoassay to screen for ANA and use IFA to confirm positive or equivocal results.
- Indirect fluorescent antibody (IFA)—this is a method in which a person’s blood sample is mixed with cells that are affixed to a slide. Autoantibodies that may be present in the blood react with the cells. The slide is treated with a fluorescent antibody reagent and examined under a microscope. The presence (or absence) and pattern of fluorescence is noted.
- Immunoassays–these methods are usually performed on automated instrumentation but may be less sensitive than IFA in detecting ANA.
Other laboratory tests associated with the presence of inflammation, such as erythrocyte sedimentation rate (ESR) and/or C-reactive protein (CRP), may also be used to evaluate a person for SLE or other autoimmune disese.
What does abnormal antinuclear antibody (ANA) test result mean?
A positive ANA test result means that autoantibodies are present. In a person with signs and symptoms, this suggests the presence of an autoimmune disease, but further evaluation is required to assist in making a final diagnosis.
Tests for antinuclear antibody (ANA)
Amount of autoantibody present
Two types of tests are commonly performed to detect and measure ANA:
- Immunoassay (enzyme linked immunosorbent assay, ELISA, or enzyme immunoassay, EIA)—the results are usually reported as a number with an arbitrary unit of measure (abbreviated as a “U” on the report, for example).
- Indirect fluorescent antibody (IFA)—the results of this method are reported as a titer. Titers are expressed as ratios. For example, the result 1:320 means that one part blood sample was mixed with 320 parts of a diluting substance and ANA was still detectable.
Patterns of cellular fluorescence
In addition to a titer, positive results on IFA will include a description of the particular type of fluorescent pattern seen. Different patterns have been associated with different autoimmune disorders, although some overlap may occur. Some of the more common patterns include:
- Homogenous (diffuse)—associated with systemic lupus erythematosus (SLE), mixed connective tissue disease, and drug-induced lupus
- Speckled—associated with SLE, Sjögren syndrome, scleroderma, polymyositis, rheumatoid arthritis, and mixed connective tissue disease
- Nucleolar—associated with scleroderma and polymyositis
- Centromere pattern (peripheral)—associated with scleroderma and CREST (Calcinosis, Raynaud syndrome, Esophogeal dysmotility, Sclerodactyly, Telangiectasia)
A positive result from the ELISA or EIA method will be a number of units that is above the laboratory’s reference number (cutoff) for the lowest possible value that is considered positive.
An example of a positive result using the IFA method would give the dilution titer and a description of the pattern, such as “Positive at 1:320 dilution with a homogenous pattern.”
For either method, the higher the value reported, the more likely the result is a true positive.
ANA test results can be positive in people without any known autoimmune disease and thus need to be evaluated carefully in conjunction with an individual’s signs and symptoms.
An ANA test may become positive before signs and symptoms of an autoimmune disease develop, so it may take time to tell the meaning of a positive ANA in a person who does not have symptoms.
Conditions associated with a positive antinuclear antibody (ANA) test
The most common condition is systemic lupus erythematosus (SLE).
- SLE—antinuclear antibody (ANA) are most commonly seen with SLE. About 95% of those with SLE have a positive ANA test result. If someone also has symptoms of SLE, such as arthritis, a rash, and skin sensitivity to light, then the person probably has SLE. A positive anti-dsDNA and anti-SM (often ordered as part of an ENA panel) help confirm that the condition is SLE.
Other conditions in which a positive ANA test result may be seen include:
- Drug-induced lupus—a number of medications may trigger this condition, which is associated with systemic lupus erythematosus (SLE) symptoms. When the drugs are stopped, the symptoms usually go away. Although many medications have been reported to cause drug-induced lupus, those most closely associated with this syndrome include hydralazine, isoniazid, procainamide, and several anticonvulsants. Because this condition is associated with the development of autoantibodies to histones, an anti-histone antibody test may be ordered to support the diagnosis.
- Sjögren syndrome—40-70% of those with this condition have a positive ANA test result. While this finding supports the diagnosis, a negative result does not rule it out. A health practitioner may want to test for two subsets of ANA: Anti-SS-A (Ro) and Anti-SS-B (La). About 90% or more of people with Sjögren syndrome have autoantibodies to SSA.
- Scleroderma (systemic sclerosis)—About 60-90% of those with scleroderma have a positive ANA. In people who may have this condition, ANA subset tests can help distinguish two forms of the disease, limited versus diffuse. The diffuse form is more severe. The limited form is most closely associated with the anticentromere pattern of ANA staining (and the anticentromere test), while the diffuse form is associated with autoantibodies to Scl-70.
- Less commonly, ANA may occur in people with Raynaud syndrome, arthritis, dermatomyositis or polymyositis, mixed connective tissue disease, and other autoimmune conditions. For more on these, read the article on Autoimmune Diseases.
A health practitioner must rely on test results, clinical symptoms, and the person’s history for diagnosis. Because symptoms may come and go, it may take months or years to show a pattern that might suggest SLE or any of the other autoimmune diseases.
A negative ANA result makes SLE an unlikely diagnosis. It usually is not necessary to immediately repeat a negative ANA test; however, due to the episodic nature of autoimmune diseases, it may be worthwhile to repeat the ANA test at a future date if symptoms recur.
Aside from rare cases, further autoantibody (subset) testing is not necessary if a person has a negative ANA result.
Is there anything else I should know?
ANA testing is not used to track or monitor the clinical course of SLE, thus serial ANA tests for diagnosed patients are not commonly ordered.
Use of a number of drugs, some infections, autoimmune hepatitis and primary biliary cirrhosis as well as other conditions mentioned above can give a positive result for the ANA test.
About 3-5% of healthy Caucasians may be positive for ANA, and it may reach as high as 10-37% in healthy individuals over the age of 65 because ANA frequency increases with age. These would be considered false-positive results because they are not associated with an autoimmune disease. Such instances are more common in women than men.
My doctor told me my ANA test is positive, but he isn’t sure if I have lupus. How can this be?
A positive ANA result means that you have a higher than normal concentration of these antibodies. This is one of the tools in diagnosing lupus as well as several other autoimmune diseases, so a positive result may be related to lupus or to another disease. Or you may simply have a higher than normal concentration of these autoantibodies that may not have any impact on your health. Even among people with lupus, ANA results can vary widely; one person can be in remission at a certain titer of ANA while another can be extremely ill at the same titer. Autoimmune diseases often have a systemic effect on the body and are very complex by nature. Your healthcare provider will interpret what the test results mean for you and may need to compare your test results as well as the severity of your symptoms over a period of time in order to make a definitive diagnosis. This additional time may also allow your healthcare provider to eliminate other possible causes of your symptoms. Another diagnostic tool is to perform additional testing for the autoantibodies Smith and ds-DNA, which, if possitive, would confirm SLE.
Is SLE the same thing as lupus?
There are actually several forms of lupus. SLE is the form that is most commonly referred to when someone mentions “lupus.” Systemic lupus means that almost any organ or system in your body can be affected. This is the most severe form. There are other forms of lupus that are primarily limited to skin, such as discoid and subacute cutaneous lupus. Symptoms include rashes that may be found in many shapes and locations on the body. A butterfly-shaped rash is commonly seen on or near the face.
Smooth Muscle Antibody (SMA)
Smooth muscle antibodies (SMA) are autoantibodies, proteins produced by the body’s immune system that recognize and attack its own actin, a protein found in smooth muscle and other tissues, especially the liver. This test detects and measures the amount (titer) of SMA (or antibody against actin) in the blood.
The production of smooth muscle or actin antibodies is strongly associated with autoimmune hepatitis. It may also sometimes be seen in other forms of liver disease, such as primary biliary cholangitis (PBC), but usually at lower antibody titers.
Autoimmune hepatitis occurs when the immune system attacks the body’s liver cells. It presents as an acute or chronic inflammation of the liver that is not due to another cause, such as a viral infection, exposure to a drug or toxin, a hereditary disorder, or alcohol abuse. It can lead to liver cirrhosis and, in some cases, to liver failure. Autoimmune hepatitis can affect anyone at any age, but about 80% of patients are women. In the United States, more than 70% of people with this disorder will have SMA or actin antibodies, either alone or along with antinuclear antibodies (ANA).
The majority of smooth muscle antibodies produced with autoimmune hepatitis is specifically directed against a protein called actin or F-actin. Testing is available for specific actin autoantibodies, but it is not available in every laboratory. Tests for actin antibodies detect more cases of autoimmune hepatitis but, in some studies, give more false-positive results than tests for smooth muscle antibodies.
When is smooth muscle antibody (SMA) ordered?
The SMA (or actin antibody), ANA, and rarely LKM1 tests are ordered when a healthcare practitioner suspects that someone has autoimmune hepatitis. They are usually ordered when a person presents with symptoms such as fatigue and jaundice along with abnormal findings on routine liver tests such as aspartate aminotransferase (AST) and/or bilirubin.
These autoantibody tests may be ordered along with other testing when a healthcare practitioner is investigating liver disease and wants to distinguish between different causes of liver injury, including viral infections, drugs, alcohol abuse, toxins, genetic conditions, metabolic conditions, and autoimmune disorders.
How is smooth muscle antibody (SMA) used?
The smooth muscle antibody (SMA) or actin antibody test is primarily ordered along with antinuclear antibodies (ANA) and liver kidney microsomal type 1 (LKM-1) antibodies to help diagnose autoimmune hepatitis and to differentiate between the two major types of autoimmune hepatitis, type 1 and type 2.
What does abnormal smooth muscle antibody (SMA) test result mean?
A significant increase in the blood titer of SMA or actin antibody and/or ANA is usually due to autoimmune hepatitis type 1. A small increase in SMA or actin antibody may be present in up to 50% of patients with primary biliary cholangitis (PBC). The SMA autoantibody may also be found in other conditions, such as infectious mononucleosis, hepatitis C, and some cancers.
A negative SMA or actin antibody test and an increased titer of LKM1 may indicate autoimmune hepatitis type 2. Type 2 is uncommon in the United States.
If the SMA or actin antibody test and other antibody tests are negative, then symptoms and liver injury may be due to causes other than autoimmune hepatitis.
Titers of SMA may be lower in children and in those with compromised immune systems. The levels may vary over the course of the disease and are not closely related to the severity of autoimmune symptoms or to a person’s prognosis.
The presence of SMA, F-actin antibodies, and ANA are highly suggestive of autoimmune hepatitis but not diagnostic. When significant concentrations of both are present and the healthcare practitioner suspects autoimmune hepatitis, then a liver biopsy may be performed to look for characteristic signs of damage and scarring in the liver tissue.
Will smooth muscle antibody (SMA) ever go away?
If it is due to a temporary condition, such as infectious mononucleosis, SMA may drop below detectable levels once the condition has resolved. If SMA is produced because of autoimmune hepatitis, then it will be present throughout a person’s life, although levels may vary over time.
Can I have more than one cause of hepatitis?
Yes. For instance, autoimmune hepatitis can co-exist with a viral hepatitis, such as hepatitis B or hepatitis C, and can be exacerbated by liver damage caused by alcohol abuse. Since the treatment of hepatitis depends on the cause, it is very important that your healthcare practitioner understand the underlying cause(s) of your condition.
How fast does autoimmune hepatitis progress?
The course and severity of autoimmune hepatitis is hard to predict. It may be acute or chronic. Some people will have no or few symptoms for many years and are diagnosed when routine liver tests are abnormal.
Anti-Liver/Kidney Microsomal Antibodies Type 1 (Anti-LKM-1)
Liver kidney microsome type 1 (anti-LKM-1) antibodies are autoantibodies, proteins produced by the body’s immune system that recognize and target its own enzyme called cytochrome P450 2D6 (CYP2D6), a protein found primarily in liver cells. The development of anti-LKM-1 antibodies is strongly associated with type 2 autoimmune hepatitis. This test detects and measures the amount (titer) of anti-LKM-1 (or antibody against CYP2D6) in the blood.
Autoimmune hepatitis is an acute or chronic inflammation of the liver that can lead to liver cirrhosis and, in some cases, to liver failure. It is hepatitis that is not due to another identifiable cause, such as a viral infection, exposure to a drug or toxin, a hereditary disorder, or alcohol abuse. Anyone can develop the disorder, but the majority of those affected are women.
There is general agreement that there are two main types of autoimmune hepatitis (debate continues as to whether there is a distinct third type). Type 1 is the most common form of autoimmune hepatitis in the United States and is associated with the presence of smooth muscle antibodies (SMA) in the blood. Type 2 is less common and tends to be more severe. It is associated with anti-LKM-1 antibodies and primarily affects young girls and is more common in Europe than in the United States.
When is Anti-LKM-1 test ordered?
The Anti-Liver/Kidney Microsomal Antibodies Type 1 (Anti-LKM-1) test may be ordered when a healthcare practitioner is investigating an individual’s liver disease and wants to distinguish between different causes of liver injury. It may be ordered along with other testing, such as an SMA and ANA test. These tests are usually ordered when a person presents with signs and symptoms, such as fatigue, weakness, and jaundice, and has abnormal findings on routine liver tests.
Signs and symptoms associated with autoimmune hepatitis may also include:
- Itching
- An enlarged liver
- Joint aches
- Abdominal discomfort
- Abnormal blood vessels in the skin (spider angiomas)
- Nausea or vomiting
- Dark urine
- Loss of appetite
- Pale or clay-colored stools
- Muscle pain (myalgia)
- In women, lack of menstrual periods (amenorrhea)
- Skin rashes
- Fluid buildup (edema)
Many of these signs and symptoms are not specific for autoimmune hepatitis; they are also seen with other causes of liver injury and with other conditions.
How is Anti-LKM-1 test used?
The liver kidney microsome type 1 antibody (anti-LKM-1 or CYP2D6 antibody) test is primarily used along with a smooth muscle antibody (SMA) and an antinuclear antibodies (ANA) test to help diagnose autoimmune hepatitis and to differentiate between the two major types, type 1 and type 2.
These tests may be used to follow up abnormal liver test findings, such as persistently increased alanine aminotransferase (ALT), aspartate aminotransferase (AST), or bilirubin. Additional tests may be ordered, such as immunoglobulins, as these may be increased with autoimmune hepatitis and/or hepatitis B and/or hepatitis C, to rule out viral hepatitis.
What does abnormal anti-LKM-1 test result mean?
A high amount or titer of anti-LKM-1 indicates that it is likely that the person tested has type 2 autoimmune hepatitis, but the result is not definitive. A liver biopsy may be performed to evaluate liver tissue for damage and scarring to help confirm the diagnosis.
If the anti-LKM-1 test is negative, but SMA and/or ANA are positive, then the person likely has type 1 autoimmune hepatitis.
If both are negative, then the person’s symptoms are likely due to a cause other than autoimmune hepatitis. However, the condition is not entirely ruled out. Not all people with autoimmune hepatitis will produce anti-LKM-1 or SMA antibodies; some people produce other autoantibodies that are rarely tested.
Levels of anti-LKM-1 are not closely related to the severity of a person’s symptoms or to that person’s prognosis. Levels may vary over time.
Those with type 2 autoimmune hepatitis may also have other autoimmune disorders, such as diabetes or thyroiditis.
People with chronic hepatitis C may sometimes develop a different type of anti-LKM antibody, sometimes referred to as anti-LKM3. This type of antibody is not detected with the usual anti-LKM-1 test methods and is not typically tested for.
The ANA test is often performed along with an SMA test. It is a marker of an autoimmune process and is associated with several autoimmune disorders, including type 1 autoimmune hepatitis.
Should everyone with liver damage be tested for liver kidney microsome type 1 antibodies (anti-LKM-1)?
This is not usually necessary. Most cases of hepatitis will be due to another identifiable cause. However, if the person with symptoms is a young girl without other risk factors and/or the healthcare practitioner suspects an autoimmune process, then anti-LKM-1, ANA, and SMA testing may be performed.
Will anti-LKM-1 ever go away?
No. Levels may vary over time, but once the autoantibodies have developed, they will be present throughout a person’s life.
Can I have more than one cause of hepatitis?
Yes. For instance, autoimmune hepatitis can co-exist with a viral hepatitis, such as hepatitis B or hepatitis C, and can become worse with liver damage caused by alcohol abuse. Since the treatment of hepatitis depends on the cause, it is very important that your healthcare practitioner understand the underlying cause(s) of your condition.
How fast does autoimmune hepatitis progress?
The course and severity of autoimmune hepatitis is hard to predict. It may be acute or chronic. Some people will have no or few symptoms for many years and are diagnosed when routine liver tests are abnormal. Those with type 2 autoimmune hepatitis often have a more severe case, but it is usually manageable with proper treatment. Appropriate treatment is important to limit liver damage.
If this antibody targets CYP450 2D6, why is it called anti-liver kidney microsome-1 (anti-LKM-1)?
This antibody was originally detected using tissue from the liver and kidney, hence the name anti-LKM-1. However, the specific protein in those tissues that the antibody targets (the major antigen) has since been identified as cytochrome P450 2D6 (CYP2D6). This protein is a major enzyme that metabolizes about 25% of drugs as well as toxic substances. It is primarily found in cells of the liver and kidney, mainly within structures called microsomes.





{kind=link}