
Contents
What is long QT syndrome
Long QT syndrome is a heart rhythm disorder due to problems with the heart’s electrical system that can cause sudden, uncontrollable, and irregular heartbeats (arrhythmia), which may lead to sudden death 1). However, not everyone who has long QT syndrome has dangerous heart rhythms. When they do occur, though, they can be fatal. Long QT syndrome occurs as the result of a defect in the ion channels, causing a delay in the time it takes for the electrical system to recharge after each heartbeat. In long QT syndrome, the lower chambers of the heart (ventricles) take too long to contract and release. The gap of time needed to complete a cycle can be measured and compared to normal averages. When the Q-T interval is longer than normal, it increases the risk for torsade de pointes, a life-threatening form of ventricular tachycardia.
Long QT syndrome is a rare disorder. Experts think that about 1 in 7,000 people in the United States has long QT syndrome. But no one knows for sure, because long QT syndrome often goes undiagnosed 2).
Long QT syndrome causes about 3,000 to 4,000 sudden deaths in children and young adults each year in the United States 3). Unexplained sudden deaths in children are rare. When they do occur, long QT syndrome often is the cause.
Inherited long QT syndrome usually is first detected during childhood or young adulthood. Half of all people who have long QT syndrome have their first abnormal heart rhythm by the time they’re 12 years old, and 90 percent by the time they’re 40 years old. The condition rarely is diagnosed after age 40.
In boys who have long QT syndrome, the QT interval (which can be seen on an EKG test) often returns toward normal after puberty. If this happens, the risk of long QT syndrome symptoms and complications goes down.
long QT syndrome is more common in women than men. Women who have long QT syndrome are more likely to faint or die suddenly from the disorder during menstruation and shortly after giving birth.
Children who are born deaf also are at increased risk for long QT syndrome. This is because the same genetic problem that affects hearing also affects the function of ion channels in the heart.
Long QT syndrome can be detected by electrocardiogram (EKG or ECG). Long QT syndrome is characterized by QT prolongation and T-wave abnormalities on the ECG that are associated with tachyarrhythmias, typically the ventricular tachycardia torsade de pointes 4). The Q-T interval is the section on the electrocardiogram (ECG) – that represents the time it takes for the electrical system to fire an impulse through the ventricles and then recharge. It is translated to the time it takes for the heart muscle to contract and then recover (see Figures 1 and 2).
There are two types of long QT syndrome. Long QT syndrome may be genetically inherited caused by a variety of different gene mutations (changes) and long QT syndrome can also be caused by certain medications you may be taking for other medical conditions.
Normally your heart circulates blood throughout your body during each heartbeat. Your heart’s chambers contract and relax to pump blood. These actions are controlled by electrical impulses that travel through your heart and cause it to beat. After each heartbeat, your heart’s electrical system recharges itself in preparation for the next heartbeat.
In long QT syndrome, your heart muscle takes longer than normal to recharge between beats. This electrical disturbance, which often can be seen on an electrocardiogram (ECG), is called a prolonged QT interval.
The electrical activity of the heart is produced by the flow of ions (electrically charged particles of sodium, calcium, potassium, and chloride) in and out of the cells of the heart. Tiny ion channels control this flow. In most cases, long QT syndrome delays the flow of potassium ions out of heart muscle cells. However, for a small number of people, the sodium channels are affected and too many sodium ions are allowed into the cells. This causes a delay in the electrical impulse known as ‘prolonged repolarization’. This shows up on an ECG as a lengthened QT interval, which is part of the heartbeat cycle.
The electrical activity that occurs between the Q and T waves is called the QT interval. This interval shows electrical activity in the heart’s lower chambers, the ventricles. The timing of the heart’s electrical activity is complex, and your body carefully controls it. Normally the QT interval is about a third of each heartbeat cycle. However, in people who have long QT syndrome, the QT interval lasts longer than normal.
A long QT interval can upset the careful timing of the heartbeat and trigger dangerous heart rhythms.
Beta blocker medication is the primary treatment for long QT syndrome; possible implantable cardioverter-defibrillators and/or left cardiac sympathetic denervation for those with beta-blocker-resistant symptoms, inability to take beta blockers, and/or history of cardiac arrest. Sodium channel blockers can be useful as additional pharmacologic therapy for patients with a QTc interval >500 ms (normal QTc interval is 440 ms).
Do You Need to be Screened for Long QT Syndrome?
Long QT Syndrome is a medical condition that can be passed on from generation to generation. It is important for you to be screened for this condition if you have a first-degree relative with long QT Syndrome. First-degree relatives are your parents, siblings and children.
The first step is to tell your doctor that you have a family history of this condition. He or she may want to do diagnostic tests to check your heart. If these tests are positive, you should be seen by a cardiologist who is familiar with this condition.
Can I live a normal life with long QT syndrome?
There are very few things you need to change if you have long QT syndrome. However, you should be aware that:
- Prolonged (longer than a day) or severe episodes of vomiting or diarrhoea can affect your sodium and potassium levels. You should discuss this situation with your doctor who may wish to prescribe oral rehydration supplements. These supplements can help to replenish sodium and potassium levels but should be used under medical supervision.
- Over-the-counter medicines and supplements should also first be discussed with your doctor. Some of these may induce symptoms or react with medicines you may be taking to help reduce your risk of abnormal heart rhythms.
- You should always inform medical staff that you have long QT syndrome when you speak to them.
What is the QT interval?
An ECG measures electrical impulses as five distinct waves (Figure 1). Doctors label these five waves using the letters P, Q, R, S and T. The waves labeled Q through T show electrical activity in your heart’s lower chambers (ventricles).
The space between the start of the Q wave and the end of the T wave (QT interval) corresponds to the time it takes for your heart to contract and then refill with blood before beginning the next contraction.
The QT interval is a time interval on the ECG. It represents the time from the electrical stimulation (depolarization) of the heart’s pumping chambers (ventricles), to the end of the recharging of the electrical system (repolarization). The interval between the letters Q and T defines the action of the ventricles. The QT interval is measured in milliseconds and closely approximates the time from the beginning of the heart ventricles’ contraction until the end of relaxation. Hence, long QT syndrome means that time period is too long, even if by fractions of a second.
An occasional prolonged QT interval can be precipitated by everyday circumstances, including:
- When startled by a noise
- Physical activity or exercise
- Intense emotion (such as fright, anger or pain)
In these instances, the heartbeat usually regains its normal contraction rhythm quickly.
Long QT syndrome results from abnormalities in the heart’s electrical recharging system. However, the heart’s structure is normal. Abnormalities in your heart’s electrical system might be inherited. Or, they may be acquired due to an underlying medical condition or a medication.
Figure 1. Normal ECG pattern
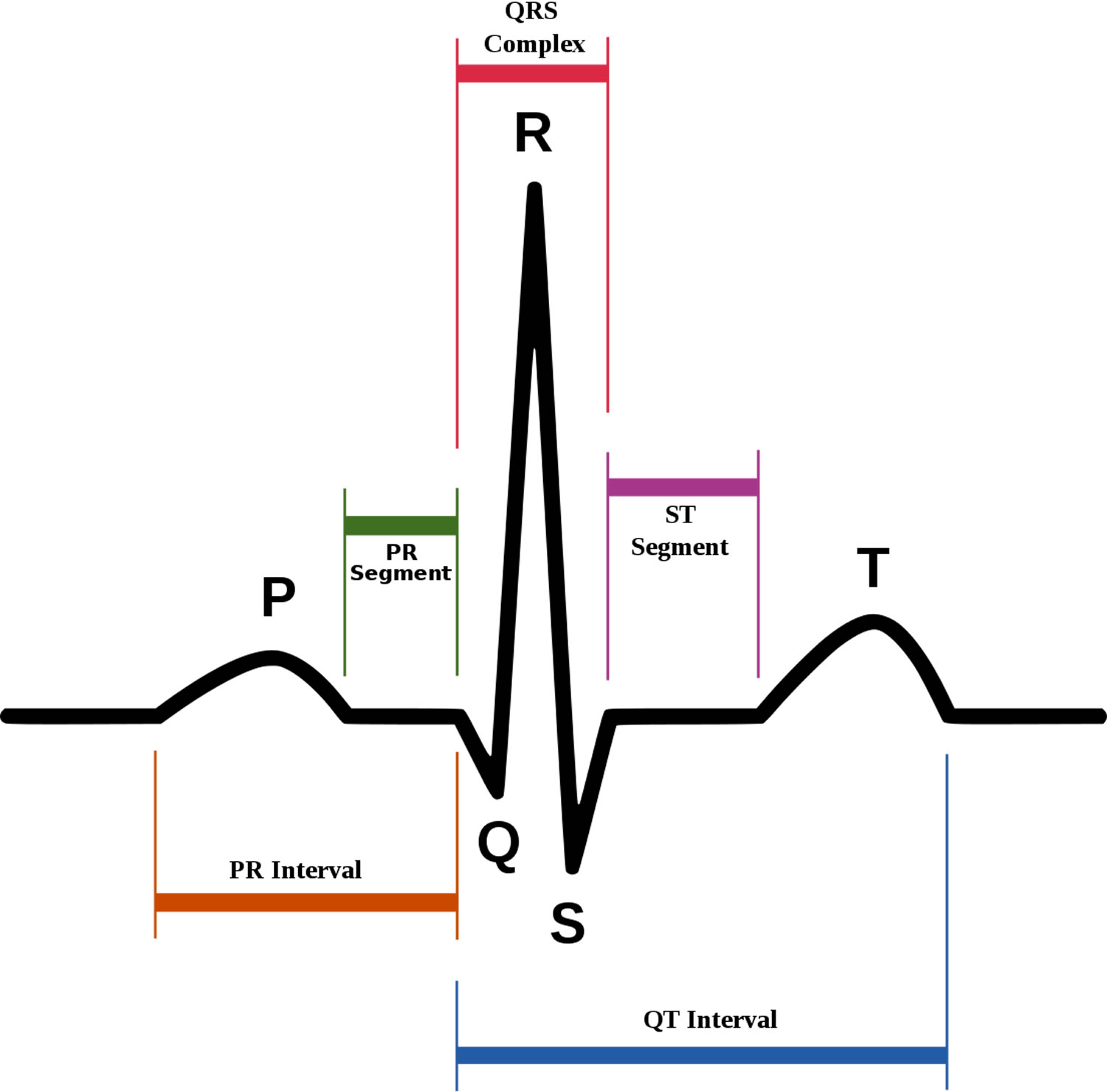
Figure 2. Long QT syndrome
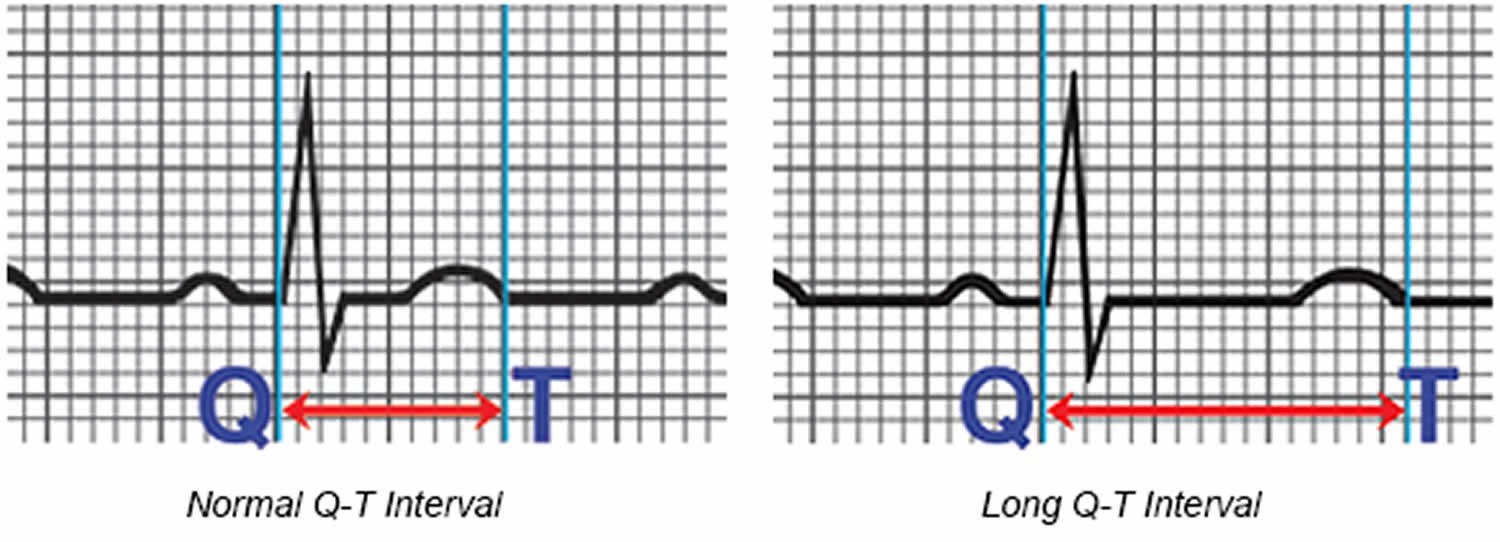
Figure 3. The heart’s electrical system

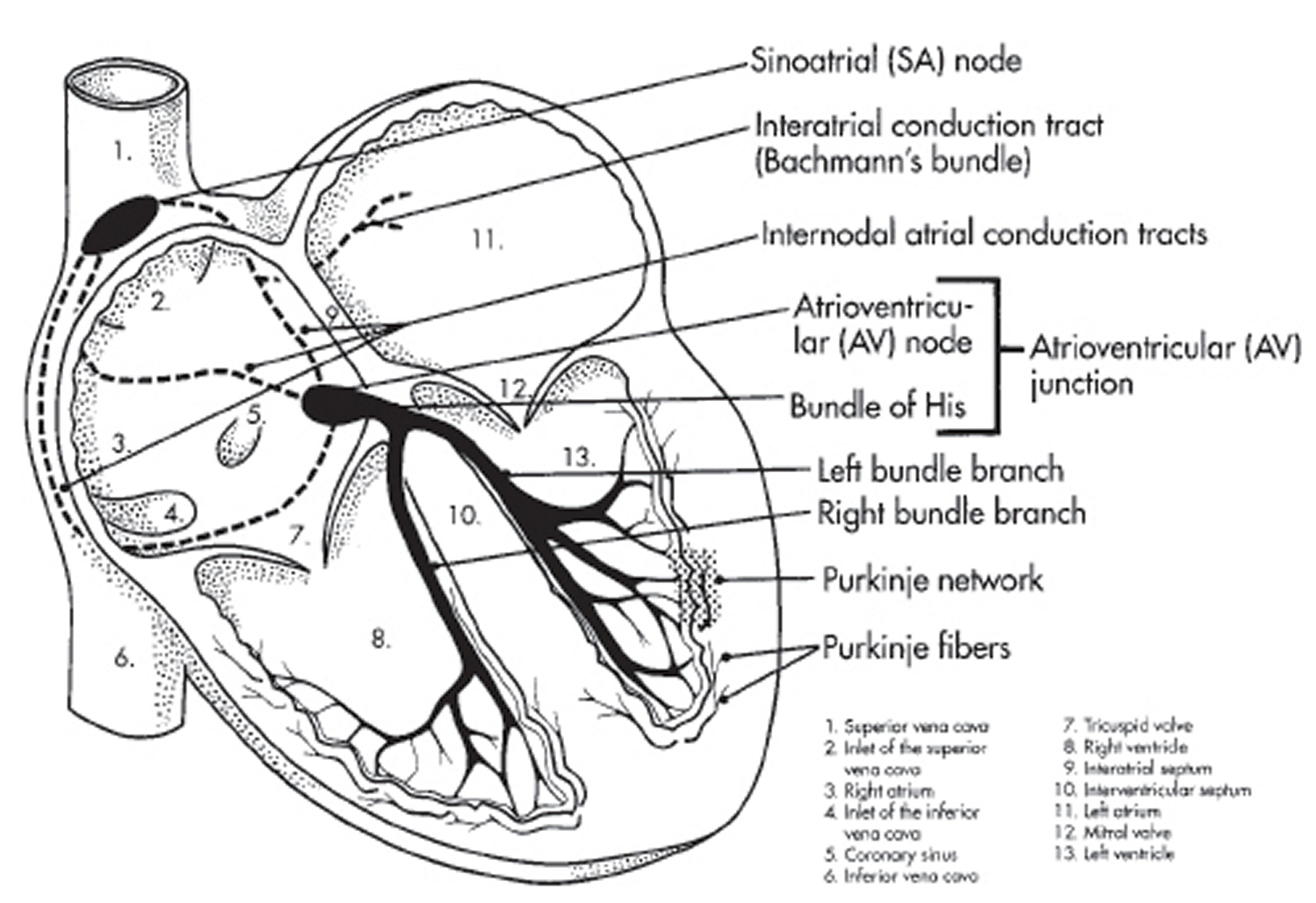 Figure 4. Normal ECG
Figure 4. Normal ECG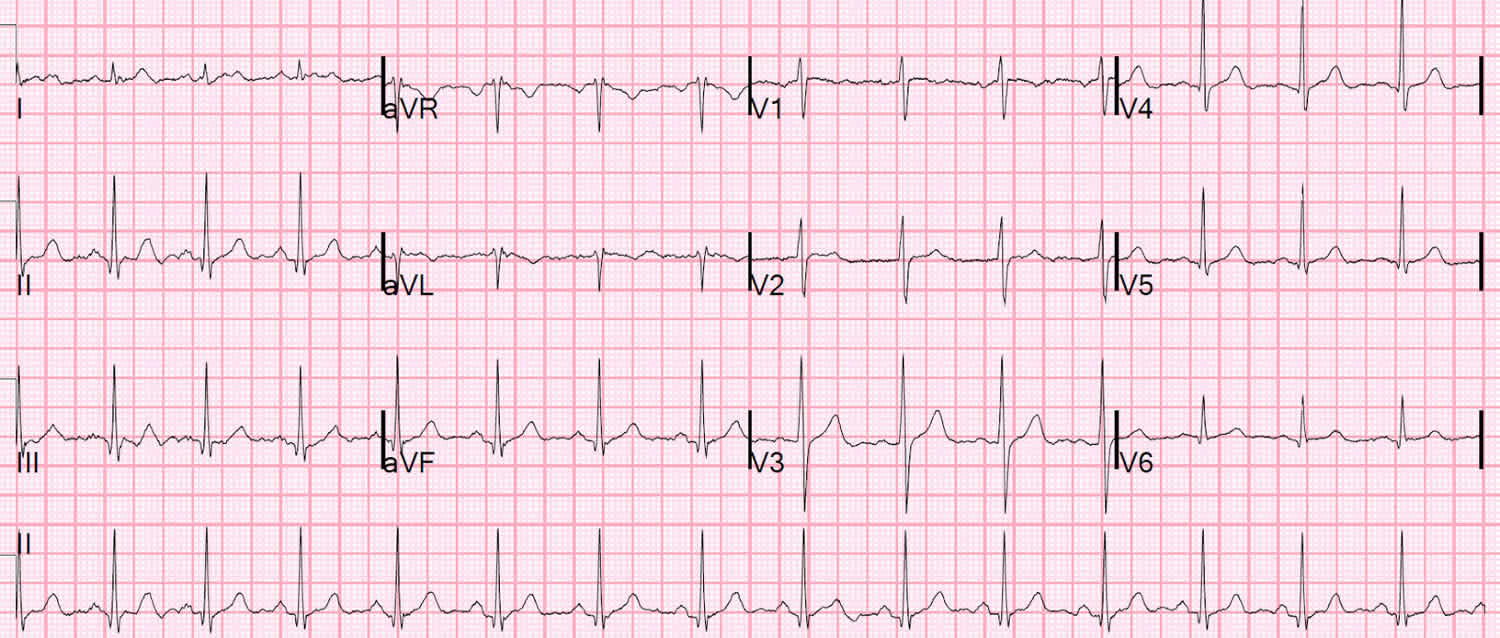
Long QT syndrome complications
Most of the time, prolonged QT intervals in people with long QT syndrome never cause problems. However, physical or emotional stress might “trip up” a heart that is sensitive to prolonged QT intervals. This can cause the heart’s rhythm to spin out of control, triggering life-threatening, irregular heart rhythms (arrhythmias) including:
Torsades de pointes — ‘twisting of the points.’ In this arrhythmia, your heart’s two lower chambers (ventricles) beat fast and chaotically, making the waves on an ECG monitor look twisted (Figure 5). Less blood is pumped out from your heart, so less blood reaches your brain, causing you to faint suddenly and, often, without any warning.
If a torsades de pointes episode is short — lasting less than one minute — your heart can correct itself and you regain consciousness on your own. However, if a torsades de pointes episode lasts longer, it can result in a sudden fainting spell followed by a full-body seizure. If the dangerous rhythm does not correct itself, then a life-threatening arrhythmia called ventricular fibrillation follows.
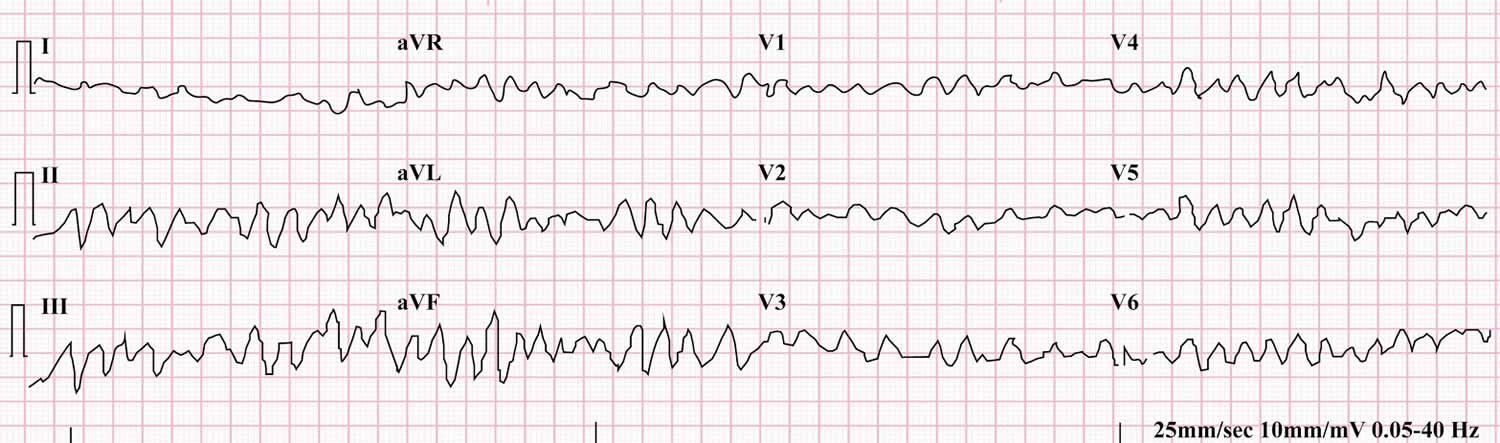
Ventricular fibrillation. This condition causes the ventricles to beat so fast that your heart quivers and ceases pumping blood. Unless your heart is shocked back into a normal rhythm by a defibrillator, ventricular fibrillation can lead to brain damage and sudden death.
It’s now known that long QT syndrome might explain some cases of sudden death in young people who otherwise appear healthy.
Figure 5. Torsades de pointes
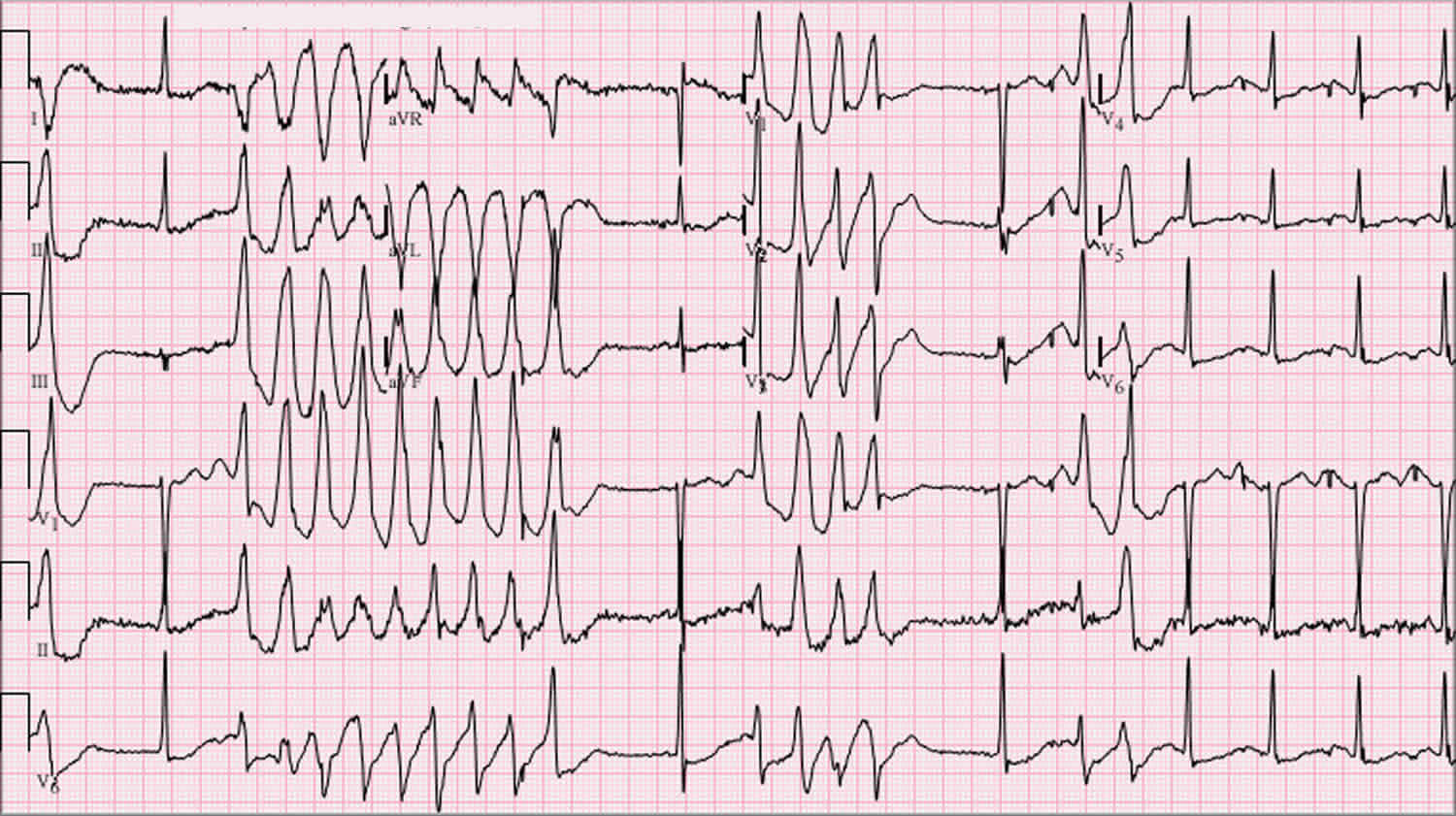
Figure 6. Ventricular fibrillation
Long QT syndrome drugs to avoid
There are many medications that can prolong the QT interval. Those with long QT syndrome may be more prone to the effects of these medications. If you have long QT syndrome, you should:
- NOT take over-the-counter medications (except for plain aspirin or acetaminophen) without first talking to your health care provider.
- Tell all your health care providers you have long QT syndrome, as there are many drugs you cannot take.
- Talk to your doctor before taking any medications prescribed for other medical conditions. The following types of medications may affect you if you have long QT syndrome:
- Antihistamines
- Antidepressants, mental illness medications
- Heart medications
- Antibiotics, antifungals, antivirals
- Intestinal medications
- Anticonvulsants
- Diuretics
- Antihypertensives
- Migraine medications
- Cholesterol lowering medications
Table 1. Long QT syndrome drugs to avoid
| Generic Name | Brand Names (Partial List) | Drug Class | Therapeutic Use |
| Abarelix (Only on Non US Market) | Plenaxis | GnRH Antagonist | Cancer (prostate) |
| Aclarubicin (Only on Non US Market) | Aclacin, Aclacinomycine, Aclacinon, Aclaplastin, Jaclacin | Anti-cancer | Cancer |
| Albuterol (salbutamol) | Proventil, Ventolin, Ventolin-HFA, Accuneb, Combivent, Vospire-ER, ProAir HFA, Duoneb | Bronchodilator | Asthma |
| Alfuzosin | Uroxatral | Alpha-1 adrenergic blocker | Benign prostatic hyperplasia |
| Amantadine | Symmetrel, Symadine | Antiviral | Viral infection (Influenza), Parkinson’s disease |
| Amiodarone | Cordarone, Pacerone, Nexterone | Antiarrhythmic | Arrhythmia |
| Amisulpride (Only on Non US Market) | Solian, Supitac, Soltus, Amitrex, Amazeo | Antipsychotic, atypical | Schizophrenia |
| Amitriptyline | Elavil (Discontinued 6/13), Tryptomer, Tryptizol, Laroxyl, Saroten, Sarotex Lentizol, Endep | Antidepressant, Tricyclic | Depression |
| Amphetamine (Amfetamine) | Adderal-XR, Dexedrine, Dextroamp | CNS stimulant | ADHD |
| Amphotericin B | Fungilin, Fungizone, Abelcet, AmBisome, Fungisome, Amphocil, Amphotec | Antifungal | Fungal infection |
| Amsacrine (acridinyl anisidide) (Only on Non US Market) | Amsidine | Antineoplastic Agent | Acute Lymphoblastic Leukemia |
| Anagrelide | Agrylin, Xagrid | Phosphodiesterase 3 inhibitor | Thrombocythemia |
| Apalutamide | Erleada | Nonsteroidal antiandrogen | Cancer (prostate) |
| Apomorphine | Apokyn, Ixense, Spontane, Uprima | Dopamine agonist | Parkinson’s disease |
| Arformoterol | Brovana | Bronchodilator | Asthma, COPD |
| Aripiprazole | Abilify, Aripiprex | Antipsychotic, atypical | Schizophrenia, depression (adjunct) |
| Arsenic trioxide | Trisenox | Anti-cancer | Cancer (leukemia) |
| Artenimol+piperaquine (Only on Non US Market) | Eurartesim | Antimalarial | Malaria |
| Asenapine | Saphris, Sycrest | Antipsychotic, atypical | Schizophrenia |
| Astemizole (Removed from Market) | Hismanal | Antihistamine | Allergic rhinitis |
| Atazanavir | Reyataz, Evotaz | Antiviral | Viral infection (HIV/AIDS) |
| Atomoxetine | Strattera | CNS stimulant | ADHD |
| Azithromycin | Zithromax, Zmax | Antibiotic | Bacterial infection |
| Bedaquiline | Sirturo | Antibiotic | Tuberculosis, Multi-drug resistant |
| Bendamustine | Treanda, Treakisym, Ribomustin, Levact | Anti-cancer | Cancer (Leukemia, lymphoma) |
| Bendroflumethiazide or bendrofluazide | Aprinox, Corzide | Diuretic, thiazide | Hypertension, diuresis |
| Benperidol (Only on Non US Market) | Anquil, Glianimon | Antipsychotic | Schizophrenia |
| Bepridil (Removed from Market) | Vascor | Antianginal | Angina Pectoris (heart pain) |
| Betrixaban | Bevyxxa | Anticoagulant | Anticoagulant |
| Bortezomib | Velcade, Bortecad | Proteasome inhibitor | Cancer (multiple myeloma,lymphoma) |
| Bosutinib | Bosulif | Anti-cancer | Cancer (leukemia) |
| Buprenorphine | Butrans, Belbuca, Bunavail, Buprenex, Suboxone, Zubsolv | Opiate | Narcotic addiction and pain |
| Cabozantinib | Cometriq | Anti-cancer | Cancer (renal cell) |
| Capecitabine | Xeloda | Anti-cancer | Cancer (GI, Breast) |
| Ceritinib | Zykadia | Anti-cancer | Cancer (Lung) |
| Chloral hydrate | Aquachloral, Novo-Chlorhydrate, Somnos, Noctec, Somnote | Sedative | Sedation, insomnia |
| Chloroquine | Aralen | Antimalarial | Malaria |
| Chlorpromazine | Thorazine, Largactil, Megaphen | Antipsychotic / Antiemetic | Schizophrenia, nausea, many others |
| Cilostazol | Pletal | Phosphodiesterase 3 inhibitor | Intermittent claudication |
| Cimetidine | Tagamet and others | Antacid | Gastric hyperacidity, GERD |
| Ciprofloxacin | Cipro, Cipro-XR, Neofloxin | Antibiotic | Bacterial infection |
| Cisapride (Removed from Market) | Propulsid | GI stimulant | Increase GI motility |
| Citalopram | Celexa, Cipramil | Antidepressant, SSRI | Depression |
| Clarithromycin | Biaxin, Prevpac | Antibiotic | Bacterial infection |
| Clofazimine (Only on Non US Market) | Lamprene | Antibiotic | Leprosy |
| Clomipramine | Anafranil | Antidepressant, Tricyclic | Depression |
| Clotiapine (Only on Non US Market) | Entumine | Antipsychotic, atypical | Psychosis |
| Clozapine | Clozaril, Fazaclo, Versacloz | Antipsychotic, atypical | Schizophrenia |
| Cocaine | Cocaine | Local anesthetic | Anesthesia (topical) |
| Crizotinib | Xalkori | Anti-cancer | Cancer (Non-small cell lung cancer, metastatic) |
| Cyamemazine (cyamepromazine) (Only on Non US Market) | Tercian | Antipsychotic | Schizophrenia, sedation |
| Dabrafenib | Tafinlar | Anti-cancer | Cancer (melanoma) |
| Dasatinib | Sprycel | Anti-cancer | Cancer (leukemia) |
| Degarelix | Firmagon, Ferring | Gonadotropin Releasing Hormone Agonist/antagonist | Cancer (prostate) |
| Delamanid (Only on Non US Market) | Deltyba | Antibiotic | Tuberculosis, Multi-drug resistant |
| Desipramine | Pertofrane, Norpramine | Antidepressant, Tricyclic | Depression |
| Deutetrabenazine | Austedo | Vesicular monamine transporter 2 inhibitor | Chorea (Huntington’s disease) |
| Dexmedetomidine | Precedex, Dexdor, Dexdomitor | Sedative | Sedation |
| Dexmethylphenidate | Focalin, Focalin-XR, Attenade | CNS stimulant | ADHD |
| Dextroamphetamine (Dexamfetamine) | Dexedrine, dexamphetamine, dexamfetamine, (S)-(+)-amphetamine, Dextrostat, Dexedrine, Metamina, Attentin, Zenzedi, Procentra, Amfexa | CNS stimulant | ADHD, obesity |
| Diphenhydramine | Benadryl, Nytol, Unisom, Sominex, Dimedrol, Daedalon | Antihistamine | Allergic rhinitis, insomnia |
| Disopyramide | Norpace | Antiarrhythmic | Arrhythmia |
| Dobutamine | Dobutrex | Inotrope | Heart failure, shock (low blood pressure) |
| Dofetilide | Tikosyn | Antiarrhythmic | Arrhythmia |
| Dolasetron | Anzemet | Antiemetic | Nausea, vomiting |
| Domperidone (Only on Non US Market) | Motilium, Motillium, Motinorm Costi, Nomit | Antiemetic | Nausea, vomiting |
| Donepezil | Aricept | Cholinesterase inhibitor | Dementia (Alzheimer’s Disease) |
| Dopamine | Intropine | Inotrope | Heart failure, shock (low blood pressure) |
| Doxepin | Sinequan, Silenor, Aponal, Adapine, Doxal, Deptran, Sinquan | Antidepressant, Tricyclic | Depression |
| Dronedarone | Multaq | Antiarrhythmic | Arrhythmia |
| Droperidol | Inapsine, Droleptan, Dridol, Xomolix | Antipsychotic / Antiemetic | Anesthesia (adjunct), nausea |
| Droxidopa | Northera | Adrenergic pro-drug | Hypotension (Neurogenic orthostatic) |
| Efavirenz | Sustiva and others | Antiviral | HIV/AIDS |
| Eliglustat | Cerdelga | Glucosylceramide synthase inhibitor | Gaucher’s disease |
| Eperisone (Only on Non US Market) | Myonal, Epry | Antispasmodic | Spasticity |
| Ephedrine | Rynatuss, Broncholate | Bronchodilator, decongestant | Allergic reaction, allergic rhinitis, asthma |
| Epinephrine (adrenaline) | Primatene, Bronkaid | Catecholamine, vasoconstrictor | Allergic reaction, anaphylaxis, cardiac arrest |
| Epirubicin | Ellence, Pharmorubicin, Epirubicin Ebewe | Anti-cancer | Cancer |
| Eribulin mesylate | Halaven | Anti-cancer | Cancer (breast, metastatic) |
| Erythromycin | E.E.S., Robimycin, EMycin, Erymax, Ery-Tab, Eryc Ranbaxy, Erypar, Eryped, Erythrocin Stearate Filmtab, Erythrocot, E-Base, Erythroped, Ilosone, MY-E, Pediamycin, Abboticin, Abboticin-ES, Erycin, PCE Dispertab, Stiemycine, Acnasol, Tiloryth | Antibiotic | Bacterial infection, increase GI motility |
| Escitalopram | Cipralex, Lexapro, Nexito, Anxiset-E (India), Exodus (Brazil), Esto (Israel), Seroplex, Elicea, Lexamil, Lexam, Entact (Greece), Losita (Bangladesh), Reposil (Chile), Animaxen (Colombia), Esitalo (Australia), Lexamil (South Africa) | Antidepressant, SSRI | Depression (major), anxiety disorders |
| Esomeprazole | Nexium, Nexum and others | Proton Pump Inhibitor | Gastric hyperacidity, GERD |
| Ezogabine (Retigabine) | Potiga, Trobalt | Anticonvulsant | Seizures, Partial |
| Famotidine | Pepcid, Fluxid, Quamatel | H2-receptor antagonist | Gastric hyperacidity, GERD |
| Felbamate | Felbatol | Anticonvulsant | Seizures |
| Fenfluramine (Removed from Market) | Pondimin, Ponderax, Adafax | Appetite suppressant | Obesity |
| Fingolimod | Gilenya | Sphingosine phospate receptor modulator | Multiple Sclerosis |
| Flecainide | Tambocor, Almarytm, Apocard, Ecrinal, Flécaine | Antiarrhythmic | Arrhythmia |
| Fluconazole | Diflucan, Trican | Antifungal | Fungal infection |
| Fluorouracil (5-FU) | Adrucil, Carac, Efudex, Efudix, others | Anti-cancer | Cancer |
| Fluoxetine | Prozac, Sarafem, Fontex | Antidepressant, SSRI | Depression |
| Flupentixol (Only on Non US Market) | Depixol, Fluanxol | Antipsychotic | Schizophrenia |
| Fluvoxamine | Faverin, Fevarin, Floxyfral, Dumyrox and Luvox | Selective Serotonin Reuptake Inhibitor | Depression, Obsessive Compulsive Disorder |
| Formoterol | Foradil, Foradile, Oxeze, Oxis, Atock, Atimos, Atimos Modulite, Perforomist, Dulera, Symbicort, Vannair, Quikhale FB | Bronchodilator | Asthma |
| Furosemide (frusemide) | Lasix, Fusid, Frumex | Diuretic | Hypertension, diuresis |
| Galantamine | Reminyl, Nivalin, Razadyne-ER, Lycoremine | Cholinesterase inhibitor | Dementia (Alzheimer’s Disease) |
| Garenoxacin (Only on Non US Market) | Geninax | Antibiotic | Bacterial infection |
| Gatifloxacin (Removed from Market) | Tequin | Antibiotic | Bacterial infection |
| Gemifloxacin | Factive | Antibiotic | Bacterial infection |
| Granisetron | Kytril, Sancuso, Granisol | Antiemetic | Nausea, vomiting |
| Grepafloxacin (Removed from Market) | Raxar | Antibiotic | Bacterial infection |
| Halofantrine (Only on Non US Market) | Halfan | Antimalarial | Malaria |
| Haloperidol | Haldol (US & UK), Aloperidin, Bioperidolo, Brotopon, Dozic, Duraperidol (Germany), Einalon S, Eukystol, Halosten, Keselan, Linton, Peluces, Serenace, Serenase, Sigaperidol | Antipsychotic | Schizophrenia, agitation |
| Hydrochlorothiazide | Apo-Hydro, Aquazide H, BP Zide, Dichlotride, Hydrodiuril, HydroSaluric, Hydrochlorot, Microzide, Esidrex, Oretic | Diuretic | Hypertension, diuresis |
| Hydrocodone – ER | Hysingla™ ER, Zohydro ER | Analgesic | Pain, severe |
| Hydroxychloroquine | Plaquenil, Quineprox | Antimalarial, Anti-inflammatory | Malaria, SLE, rheumatoid arthritis |
| Hydroxyzine | Atarax, Vistaril, Aterax, Alamon, Durrax, Equipose, Masmoran, Orgatrax, Paxistil Quiess, Tran-Q, Tranquizine | Antihistamine | Allergic reaction, anxiety disorders |
| Ibogaine (Only on Non US Market) | None | Psychedelic | Narcotic addiction, unproven |
| Ibutilide | Corvert | Antiarrhythmic | Arrhythmia |
| Iloperidone | Fanapt, Fanapta, Zomaril | Antipsychotic, atypical | Schizophrenia |
| Imipramine (melipramine) | Tofranil | Antidepressant, Tricyclic | Depression |
| Indacaterol | Arcapta Neohaler (US), Onbrez Breezhaler (Canada), Utibron (combo w/ glycopyrrolate) | Bronchodilator | Asthma, COPD |
| Indapamide | Lozol, Natrilix, Insig | Diuretic | Hypertension, diuresis |
| Inotuzumab ozogamicin | Besponsa | Anti-cancer | Cancer (acute lymphocytic leukemia} |
| Isoproterenol | Medihaler-Iso, Isuprel | Bronchodilator | Allergic reaction |
| Isradipine | Dynacirc | Antihypertensive | Hypertension |
| Itraconazole | Sporanox, Onmel | Antifungal | Fungal infection |
| Ivabradine | Procoralan, Coralan, Corlentor, Coraxan, Ivabid, Bradia | Antianginal | Angina Pectoris (heart pain) |
| Ketanserin (Only on Non US Market) | Sufrexal | Antihypertensive | Hypertension |
| Ketoconazole | Nizoral, Sebizole, Ketomed, Keton | Antifungal | Fungal infection |
| Lacidipine (Only on Non US Market) | Lacipil, Motens | Calcium channel blocker | Hypertension |
| Lansoprazole | Prevacid | Proton Pump Inhibitor | Gastric hyperacidity, GERD |
| Lapatinib | Tykerb, Tyverb | Anti-cancer | Cancer (breast, metastatic) |
| Lenvatinib | Lenvima | Anti-cancer | Cancer (Thyroid) |
| Leuprolide | Lupron, Eligard, Viadur, Carcinil, Enanton, Leuplin, Lucrin, Procren, Prostap and others | Gonadotropin receptor agonist/antogist | Cancer (prostate) |
| Levalbuterol (levsalbutamol) | Xopenex, Levolin, Axazest | Bronchodilator | Asthma |
| Levofloxacin | Levaquin, Tavanic | Antibiotic | Bacterial infection |
| Levomepromazine (methotrimeprazine) (Only on Non US Market) | Nosinan, Nozinan, Levoprome | Antipsychotic | Schizophrenia |
| Levomethadyl acetate (Removed from Market) | Orlaam | Opiate | Narcotic dependence |
| Levosulpiride (Only on Non US Market) | Lesuride, Levazeo, Enliva (with rabeprazole) | Antipsychotic | Schizophrenia |
| Lisdexamfetamine | Vyvanse | CNS stimulant | ADHD |
| Lithium | Eskalith, Lithobid | Antimanic | Bipolar disorder |
| Loperamide | Imodium and many other OTC and Rx brands | Opiate | Diarrhea |
| Lopinavir and ritonavir | Kaletra, Aluvia | Antiviral | HIV/AIDS |
| Maprotiline | Ludiomil and others | Anti-depressant, Tetracyclic | Depression |
| Melperone (Only on Non US Market) | Bunil, Buronil, Eunerpan | Antipsychotic, atypical | Schizophrenia |
| Memantine | Namenda XR and many others | NMDA receptor antagonist | Alzheimer’s disease |
| Mesoridazine (Removed from Market) | Serentil | Antipsychotic | Schizophrenia |
| Metaproterenol (orciprenaline) | Metaprel, Alupent | Bronchodilator | Asthma |
| Methadone | Dolophine, Symoron, Amidone, Methadose, Physeptone, Heptadon | Opiate | Narcotic dependence, pain |
| Methamphetamine (Metamfetamine) | Desoxyn, Pervitin, Anadrex, Methedrine, Syndrox | CNS stimulant | Obesity, ADHD |
| Methylphenidate | Ritalin, Concerta, Focalin, Daytrana, Methylin, Metadate CD | CNS stimulant | ADHD |
| Metoclopramide | Reglan, Afipran, Maxolon, Cerucal, Clopamon, Clopra, Maxeran, Maxolon, Metozolv, Plasil, Pramin, Primperan, Perinorm | Antiemetic | Nausea, vomiting |
| Metolazone | Zytanix, Zaroxolyn, and Mykrox | Diuretic | Hypertension, diuresis |
| Metronidazole | Flagyl and many others | Antibiotic | Trichomoniasis, amebiasis, bacterial infection |
| Midodrine | ProAmatine, Amatine, Gutron | Vasoconstrictor | Hypotension |
| Midostaurin | Rydapt | Anti-cancer | Cancer (Acute myeloid leukemia) |
| Mifepristone | Korlym, Mifeprex | Progesterone antagonist | Pregnancy termination |
| Mirabegron | Myrbetriq | Beta3 adrenergic antagonist | Bladder spasm |
| Mirtazapine | Remeron | Antidepressant, Tetracyclic | Depression |
| Moexipril/HCTZ | Uniretic, Univasc | Antihypertensive | Hypertension, diuresis |
| Moxifloxacin | Avelox, Avalox, Avelon | Antibiotic | Bacterial infection |
| Necitumumab | Portrazza | Anti-cancer | Cancer (Lung) |
| Nelfinavir | Viracept | Antiviral | Viral infection (HIV/AIDS) |
| Nicardipine | Cardene | Antihypertensive | Hypertension |
| Nilotinib | Tasigna | Anti-cancer | Cancer (leukemia) |
| Norepinephrine | Levophed | Vasconstrictor, Inotrope | Heart failure, shock (low blood pressure) |
| Norfloxacin (Removed from Market) | Noroxin, Ambigram | Antibiotic | Bacterial infection |
| Nortriptyline | Pamelor, Sensoval, Aventyl, Norpress, Allegron, Noritren, Nortrilen | Antidepressant, Tricyclic | Depression |
| Nusinersen | Spinraza | Antisense oligonucleotide | Spinal Muscular Atrophy |
| Ofloxacin | Floxin | Antibiotic | Bacterial infection |
| Olanzapine | Zyprexa, Zydis, Relprevv | Antipsychotic, atypical | Schizophrenia, bipolar disorder |
| Olodaterol | Striverdi Respimat | Bronchodilator | Asthma |
| Omeprazole | Losec, Prilosec, Zegerid | Proton Pump Inhibitor | Gastric hyperacidity, GERD |
| Ondansetron | Zofran, Anset, Ondemet, Zuplenz, Emetron, Ondavell, Emeset, Ondisolv, Setronax | Antiemetic | Nausea, vomiting |
| Osimertinib | Tagrisso | Anti-cancer | Cancer (EGFR pos. NSC Lung cancer) |
| Oxaliplatin | Eloxatin | Anti-cancer | Cancer |
| Oxytocin | Pitocin, Syntocinon | Oxytocic | Labor stimulation |
| Paliperidone | Invega, Xepilon | Antipsychotic, atypical | Schizophrenia |
| Palonosetron | Aloxi | Antiemetic | Nausea, vomiting |
| Panobinostat | Farydak | Histone deacetylase inhibitor | Cancer, Multiple myeloma |
| Pantoprazole | Protonix and others | Proton Pump Inhibitor | Gastric hyperacidity, GERD |
| Papaverine HCl (Intra-coronary) | none | Vasodilator, Coronary | Diagnostic adjunct |
| Paroxetine | Paxil, Aropax, Pexeva, Seroxat, Sereupin, Seroxat | Antidepressant, SSRI | Depression |
| Pasireotide | Signifor | Somatostatin analog | Cushings Disease |
| Pazopanib | Votrient | Anti-cancer | Cancer (renal cell, sarcoma) |
| Pentamidine | Pentam | Antifungal | Fungal infection (Pneumocystis pneumonia) |
| Perflutren lipid microspheres | Definity, Optison | Imaging contrast agent | Diagnostic adjunct |
| Perphenazine | Trilafon, Etrafon/Triavil, Decentan | Antipsychotic | Schizophrenia |
| Phentermine | Adipex P, Adiphene (India), Anoxine-AM, Ionamin, Duromine, Metermine, Miraprontv, Obephen, Obermine, Obestin-30, Phentremine, Phentrol, Phenterex, Phentromin, Pro-Fast SA, Redusa, Panbesy, Obenix, Oby-Trim, Teramine, Zantryl, Sinpet, Supremin, Suprenza, Umine, Weltmine | Appetite suppressant | Obesity |
| Phenylephrine | Neosynephrine | Vasoconstrictor | Shock (low blood pressure), allergic rhinitis, asthma |
| Phenylpropanolamine (Removed from Market) | Acutrim, Dexatrim | Appetite suppressant | Obesity |
| Pilsicainide (Only on Non US Market) | Sunrythm | Anti-arrhythmic | Arrhythmia |
| Pimavanserin | Nuplazid | Antipsychotic, atypical | Psychosis, Parkinson’s Disease |
| Pimozide | Orap | Antipsychotic | Tourette’s Disorder |
| Pipamperone (Only on Non US Market) | Dipiperon (E.U), Propitan (Japan), Dipiperal, Piperonil, Piperonyl | Antipsychotic | Schizophrenia |
| Piperacillin/Tazobactam | Tazosyn and Zosyn | Antibiotic | Bacterial infection |
| Posaconazole | Noxafil, Posamol | Antifungal | Fungal infection |
| Primaquine phosphate | Antimalarial | Malaria | |
| Probucol (Removed from Market) | Lorelco | Antilipemic | Hypercholesterolemia |
| Procainamide | Pronestyl, Procan | Antiarrhythmic | Arrhythmia |
| Promethazine | Phenergan | Antipsychotic / Antiemetic | Nausea, vomiting |
| Propafenone | Rythmol SR, Rytmonorm | Sodium channel blocker | Arrhythmia |
| Propofol | Diprivan, Propoven | Anesthetic, general | Anesthesia |
| Prothipendyl (Only on Non US Market) | Dominal, Largophren, Timoval, Timovan, Tumovan | Antipsychotic | Schizophrenia |
| Pseudoephedrine | PediaCare, Sudafed | Decongestant | Allergic reaction, allergic rhinitis, asthma |
| Quetiapine | Seroquel | Antipsychotic, atypical | Schizophrenia |
| Quinidine | Quinaglute, Duraquin, Quinact, Quinidex, Cin-Quin, Quinora | Antiarrhythmic | Arrhythmia |
| Quinine sulfate | Qualaquin | Antimalarial | Malaria, leg cramps |
| Ranolazine | Ranexa, Ranozex | Antianginal | Angina Pectoris (heart pain) |
| Ribociclib | Kisqali | Anti-cancer | Cancer (breast) |
| Rilpivirine | Edurant, Complera, Eviplera | Antiviral | Viral infection (HIV/AIDS) |
| Risperidone | Risperdal | Antipsychotic, atypical | Schizophrenia |
| Ritodrine (Removed from Market) | Yutopar | Muscle relaxant | Premature labor |
| Romidepsin | Istodax | Histone deacetylase inhibitor | Cancer (lymphoma) |
| Roxithromycin (Only on Non US Market) | Rulide, Xthrocin, Roxl-150, Roxo, Surlid, Rulide, Biaxsig, Roxar, Roximycinv, Roxomycin, Rulid, Tirabicin, Coroxin | Antibiotic | Bacterial infection |
| Salmeterol | Serevent, Advair | Bronchodilator | Asthma |
| Saquinavir | Invirase(combo) | Antiviral | Viral infection (HIV/AIDS) |
| Sertindole (Only on Non US Market) | Serdolect, Serlect | Antipsychotic, atypical | Schizophrenia, anxiety |
| Sertraline | Zoloft, Lustral, Daxid, Altruline, Besitran, Deprax, Elrval, Emergen, Gladem, Implicane, Sedoran, Sealdin, SerivoLowfin, Stimuloton, Tresleen, Sertralin Bluefish | Antidepressant, SSRI | Depression |
| Sevoflurane | Ultane, Sojourn | Anesthetic, general | Anesthesia |
| Sibutramine (Removed from Market) | Meridia | Appetite suppressant | Obesity |
| Solifenacin | Vesicare | Muscle relaxant | Bladder spasm |
| Sorafenib | Nexavar | Anti-cancer | Cancer (liver, renal cell, metastatic thyroid) |
| Sotalol | Betapace, Sotalex, Sotacor | Antiarrhythmic | Arrhythmia |
| Sparfloxacin (Removed from Market) | Zagam | Antibiotic | Bacterial infection |
| Sulpiride (Only on Non US Market) | Dogmatil, Dolmatil, Eglonyl, Espiride, Modal, Sulpor | Antipsychotic, atypical | Schizophrenia |
| Sultopride (Only on Non US Market) | Barnetil, Barnotil, Topral | Antipsychotic, atypical | Schizophrenia |
| Sunitinib | Sutent | Anti-cancer | Cancer (GIST, renal cell, pNET) |
| Tacrolimus | Prograf, Prograf, Advagraf, Protopic | Immunosuppressant | Immune suppression |
| Tamoxifen | Nolvadex(discontinued 6/13), Istubal, Valodex | Anti-cancer | Cancer (breast) |
| Telaprevir | Incivo, Incivek | Antiviral | Viral infection (hepatitis C) |
| Telavancin | Vibativ | Antibiotic | Bacterial infection |
| Telithromycin | Ketek | Antibiotic | Bacterial infection |
| Terbutaline | Brethine, Bricanyl, Brethaire, Terbulin | Bronchodilator | Asthma, premature labor |
| Terfenadine (Removed from Market) | Seldane | Antihistamine | Allergic rhinitis |
| Terlipressin (Only on Non US Market) | Teripress, Glypressin, Terlipin, Remestyp, Tresil, Teriss and others | Vasoconstrictor | Septic shock |
| Terodiline (Only on Non US Market) | Micturin, Mictrol (not bethanechol) | Muscle relaxant | Bladder spasm |
| Tetrabenazine | Nitoman, Xenazine | Vesicular Monoamine Transporter 2 Inhibitor | Chorea (Huntington’s disease) |
| Thioridazine | Mellaril, Novoridazine, Thioril | Antipsychotic | Schizophrenia |
| Tiapride (Only on Non US Market) | Tiapridal, Italprid, Sereprile, Tialaread, Tiaryl, Tiaprim, Tiaprizal, Sereprid, Tiapridex | Selective D2, D3 dopamine antagonist | Alcoholism, withdrawal |
| Tipiracil and Trifluridine | Lonsurf | Anti-cancer | Cancer (Metastatic colorectal cancer) |
| Tizanidine | Zanaflex, Sirdalud | Muscle relaxant | Muscle spasticity |
| Tolterodine | Detrol, Detrusitol | Muscle relaxant | Bladder spasm |
| Toremifene | Fareston | Estrogen agonist/antagonist | Cancer (breast, metastatic) |
| torsemide (torasemide) | Demadex, Diuver, Examide | Diuretic | Hypertension, diuresis |
| Tramadol | Crispin, Ralivia ER, Ralivia Flashtab, Tramadolum, Tramal, Tramodol, Tridural, Ultram, Ultram ER, Zydol | Analgesic | Pain |
| Trazodone | Desyrel (discontinued 6/13), Oleptro, Beneficat, Deprax, Desirel, Molipaxin, Thombran, Trazorel, Trialodine, Trittico, Mesyrel | Antidepressant, SARI | Depression, insomnia |
| Trimethoprim-Sulfamethoxazole | Septra, Bactrim, Sulfatrim, Biseptol, Co-trimoxazole, Cotrim, Septrin, Trisul | Antibiotic | Bacterial infection |
| Trimipramine | Surmontil, Rhotrimine, Stangyl | Antidepressant, Tricyclic | Depression |
| Tropisetron (Only on Non US Market) | Navoban, Setrovel | Antiemetic | Nausea, vomiting |
| Valbenazine | Ingrezza | Vesicular monamine transporter 2 inhibitor | Tardive Dyskinesia |
| Vandetanib | Caprelsa | Anti-cancer | Cancer (thyroid) |
| Vardenafil | Levitra | Phosphodiesterase 5 inhibitor | Erectile dysfunction |
| Vemurafenib | Zelboraf | Anti-cancer | Cancer (melanoma) |
| Venlafaxine | Effexor, Efexor | Antidepressant, SNRI | Depression |
| Vilanterol/fluticasone furoate | Breo Ellipta | Bronchodilator | Asthma |
| Voriconazole | VFend | Antifungal | Fungal infection |
| Vorinostat | Zolinza | Histone deacetylase inhibitor | Cancer (lymphoma) |
| Ziprasidone | Geodon, Zeldox | Antipsychotic, atypical | Schizophrenia |
| Zotepine (Only on Non US Market) | Losizopilon, Lodopin, Setous and Zoleptil | Antipsychotic, atypical | Schizophrenia |
| Zuclopenthixol, Zuclopentixol (Only on Non US Market) | Cisordinol, Clopixol, Acuphase | Antipsychotic | Psychosis |
Long QT syndrome life expectancy
More than half of the people who have untreated, inherited types of long QT syndrome die within 10 years 6). However, lifestyle changes and medicines can help people who have long QT syndrome prevent complications and live longer.
If you have long QT syndrome, talk with your doctor about which lifestyle changes and treatments are best for you.
Once you’ve been diagnosed with long QT syndrome, several steps can help you avoid serious consequences, including:
- Avoiding strenuous physical activity or startling noises.
- Adding more potassium to your diet (as your doctor advises).
- Taking heart medicines called beta blockers. These medicines help prevent sudden cardiac arrest.
- Having an implanted medical device, such as a pacemaker or implantable cardioverter defibrillator. These devices help control abnormal heart rhythms.
- Don’t overexert yourself. You might not need to give up sports if you have long QT syndrome. Your doctor might permit recreational activities as long as you have a buddy along in case you have a fainting episode. In general, people with long QT syndrome should never swim alone. Strenuous exercise might be dangerous and isn’t recommended for some people with long QT syndrome. However, others might have a lower risk of complications and may be able to continue strenuous exercise and even competitive sports. Discuss this issue with your doctor in detail.
- Know your symptoms. Be fully aware of symptoms that can warn you of irregular heart rhythms and decreased blood flow to your brain, such as feeling like you may faint.
- Inform other people. Make family, friends, teachers, neighbors and anyone else who has regular contact with you aware of your heart condition. Wear a medical alert identification to notify health care providers of your condition.
- Have plans in case of an emergency cardiac event. Family members may want to learn cardiopulmonary resuscitation (CPR) so they can provide immediate resuscitation if you ever need it. In some situations, it might be appropriate to have or be able to rapidly access an automatic external defibrillator. However, if your inherited long QT syndrome has been evaluated and treated carefully, you are generally unlikely to ever need CPR or an automatic external defibrillator.
- Control startling events as much as possible. Turn down the volume on doorbells and turn off the telephone ringer or your cellphone at night.
- Visit your doctor. Your cardiologist will likely recommend that you have regular follow-up appointments with him or her. Let your doctor know if you have symptoms of long QT syndrome or any changes in your condition. Your doctor may make changes to your treatment plan or suggest additional treatments for you.
Sexual intercourse doesn’t appear to increase the risk of long QT syndrome. Pregnancy and delivery aren’t associated with an increased risk of symptoms in women with long QT syndrome.
Still, if you have inherited long QT syndrome, your doctor will want to monitor you closely both during your pregnancy and after. Women with long QT syndrome, especially a form called LQT2, are at increased risk during the period following delivery and need careful monitoring.
Living With long QT syndrome
Long QT syndrome usually is a lifelong condition. The risk of having an abnormal heart rhythm that leads to fainting or sudden cardiac arrest may lessen as you age. However, the risk never completely goes away.
You’ll need to take certain steps for the rest of your life to prevent abnormal heart rhythms. You can:
- Avoid things that trigger abnormal heart rhythms
- Let others know you might faint or your heart might stop beating, and tell them what steps they can take
- Have a plan in place for how to handle abnormal heart rhythms
If an abnormal heart rhythm does occur, you’ll need to seek treatment right away.
Avoid Triggers
If exercise triggers an abnormal heart rhythm, your doctor may tell you to avoid any strenuous exercise, especially swimming. Ask your doctor what types and amounts of exercise are safe for you.
If you have a pacemaker or implantable cardioverter defibrillator, avoid contact sports that may dislodge these devices. You may want to exercise in public or with a friend who can help you if you faint.
Avoid medicines that can trigger an abnormal heart rhythm. This includes some medicines used to treat allergies, infections, high blood pressure, high blood cholesterol, depression, and arrhythmias. Talk with your doctor before taking any prescription, over-the-counter, or other medicines or drugs.
Seek medical care right away for conditions that lower the sodium or potassium level in your blood. These conditions include the eating disorders anorexia nervosa and bulimia, excessive vomiting or diarrhea, and certain thyroid disorders.
If you have long QT syndrome 2, try to avoid unexpected noises, such as loud or jarring alarm clock buzzers and telephone ringers.
Inform Others
You may want to wear a medical ID necklace or bracelet that states that you have long QT syndrome. This will help alert medical personnel and others about your condition if you have an emergency.
Let your roommates, coworkers, or other people with whom you have regular contact know that you have a condition that might cause you to faint or go into cardiac arrest. Tell them to call your local emergency services number right away if you faint.
Consider asking a family member and/or coworker to learn cardiopulmonary resuscitation (CPR) in case your heart stops beating.
You also may want to keep an automated external defibrillator with you at home or at work. This device uses electric shocks to restore a normal heart rhythm.
Someone at your home and/or workplace should be trained on how to use the automated external defibrillator, just in case your heart stops beating. If a trained person isn’t available, an untrained person also can use the automated external defibrillator to help save your life.
If you have long QT syndrome 3 and you sleep alone, you may want to have an intercom in your bedroom that’s connected to someone else’s bedroom. This will let others detect the noisy gasping that often occurs if you have an abnormal heart rhythm while lying down.
Ongoing Health Care Needs
You should see your cardiologist (heart specialist) regularly. He or she will adjust your treatment as needed. For example, if you still faint often while using less aggressive treatments, your doctor may suggest other treatment options.
Emotional Issues and Support
Living with long QT syndrome may cause fear, anxiety, depression, and stress. Talk about how you feel with your health care team. Talking to a professional counselor also can help. If you’re very depressed, your doctor may recommend medicines or other treatments that can improve your quality of life.
Joining a patient support group may help you adjust to living with long QT syndrome. You can see how other people have coped with the condition. Talk with your doctor about local support groups or check with an area medical center.
Support from family and friends also can help relieve stress and anxiety. Let your loved ones know how you feel and what they can do to help you.
Some people learn they have long QT syndrome because they’re tested after a family member dies suddenly from long QT syndrome. Grief counseling may help you cope if this has happened to you. Talk with your doctor about finding a grief counselor.
Long QT syndrome symptoms
Nearly half of patients with long QT syndrome NEVER have any signs or symptoms!
You might be aware of your condition only because of:
- Results of an electrocardiogram (ECG) done for an unrelated reason
- A family history of long QT syndrome
- Genetic testing results
Signs and symptoms of inherited or congenital long QT syndrome might start as a fetus, during the first weeks to months after birth, as late as older age, or never at all. Most people who experience signs or symptoms from long QT syndrome have their first episode by age 40.
Signs and symptoms of long QT syndrome might occur during sleep or arousal from sleep.
The most common symptoms of long QT syndrome include:
- Syncope (fainting): This is the most common sign of long QT syndrome. Long QT syndrome-triggered fainting spells (syncope) are caused by the heart temporarily beating in an erratic way. These fainting spells might happen when you’re excited, angry, scared or during exercise. You may lose consciousness without warning, for instance from being startled by a ringing telephone. If you have a normal fainting spell, you usually will have a warning sign first, such as lightheadedness, heart palpitations, irregular heartbeat, weakness or blurred vision. However, a fainting spell from long QT syndrome can occur with little to no warning.
- Seizures: If the heart continues to beat erratically, the brain will eventually not get enough oxygen, which can cause seizures.
- Sudden death: Generally, the heart returns to its normal rhythm. If this doesn’t happen by itself, or if an external defibrillator isn’t used in time to convert the rhythm back to normal, sudden death will occur. In about 1 out of 10 people who have long QT syndrome, sudden cardiac arrest or sudden death is the first sign of the disorder.
- Unexplained drowning or near drowning. This may be due to fainting while swimming.
- Often, people who have LQTS 3 develop an abnormal heart rhythm during sleep. This may cause noisy gasping while sleeping.
The symptoms of long QT syndrome are related to torsade de pointes (see Figure 5). During this arrhythmia, the ventricle beats very fast and irregularly. The heart is unable to pump blood effectively to the body. If the brain does not receive an adequate blood supply, syncope (fainting) and seizure-like activity can occur. If the arrhythmia continues, sudden death will occur. If the heart rhythm returns to normal, symptoms will stop.
- If you have potassium channel long QT syndrome, you carry the risk of sudden death if you are startled or awoken suddenly.
- If you have sodium channel long QT syndrome, you have an increased risk of sudden death whilst sleeping.
Symptoms are most common during:
- Exercise (or within a few minutes after)
- Emotional excitement, especially being startled
- During sleep or upon waking suddenly
Some people with congenital long QT syndrome never have symptoms. The diagnosis is made during a routine ECG or during an evaluation because a family member has it. Symptoms usually first appear during the early teen years.
Your doctor will advise you depending on the type of long QT syndrome you have. You may be advised not to take part in competitive sports, which can be difficult – especially for young people. Your doctor will help you arrive at a balance between being active and reducing your risk of making your condition worse.
The risk of sudden death is greater if you have a history of:
- previous cardiac arrest
- blackouts
- a very long QT interval on your ECG
- sodium channel mutations.
Strenuous exercise or severe exertion can increase the risk of sudden death for many people with long QT syndrome. Speak to your doctor if you have any questions about the risk of sudden death.
If you are with someone when they collapse suddenly, it is imperative to call your local emergency services number and try to perform CPR until an ambulance or medical help arrives. If you are untrained in CPR, the emergency services operator will be able to talk you through the process.
Silent long QT Syndrome
Sometimes long QT syndrome doesn’t cause any signs or symptoms. This is called silent long QT syndrome. For this reason, doctors often advise family members of people who have long QT syndrome to be tested for the disorder, even if they have no symptoms.
Medical and genetic tests may reveal whether these family members have long QT syndrome and what type of the condition they have.
Long QT syndrome causes
Long Q-T syndrome can be acquired or congenital:
- Acquired long QT syndrome is caused by many medications. Sensitivity to these medications may be related to genetic causes.
- Congenital long QT syndrome is usually inherited. It is caused by an abnormality in the gene code for the ion channels. The abnormality of the ion channels slows the recovery phase of the heartbeat. Forms of inherited long QT syndrome include:
- Recent Classifications – Multiple ion channel abnormalities have been discovered. The most common ones include LQT1, LQT2, LQT3, LQT4, LQT5; these are classified by the type of channel which causes the long QT syndrome. The type of long QT syndrome classification is related to the risk of future cardiac events, those with LQT3 having the highest risk of life-threatening arrhythmias.
- Jervell, Lange-Nielsen Syndrome (autosomal recessive inheritance pattern) – Both parents are carriers of the abnormal gene, but they may not manifest long QT syndrome. Each child has a 25-percent chance of inheriting long QT syndrome. This syndrome is associated with deafness at birth and is extremely rare, as there is a small chance that both parents would carry the long QT syndrome gene.
- Romano-Ward Syndrome (autosomal dominant inheritance pattern) – One parent has long QT syndrome and the other parent usually does not. Each child has a 50-percent chance of inheriting the abnormal gene. In this syndrome, hearing is normal; however the likelihood that children in this family would have long QT syndrome is greater. The gene may be present in all the couple’s children, some of them or none at all.
Those at risk for long QT syndrome include:
- Children who are deaf at birth
- Children and young adults who have unexplained sudden death or syncope in family members
- Blood relatives of family members with long QT syndrome
- Those with long QT syndrome taking medications that can further prolong the QT intervals.
Congenital long QT syndrome
At least 17 genes associated with long QT syndrome have been found so far, and hundreds of mutations within these genes have been identified. Mutations in three of these genes account for about 75 percent of long QT syndrome cases, while mutations in the other minor genes contribute a small percent of long QT syndrome cases.
About 20 to 25 percent of people who definitely have congenital long QT syndrome have a negative genetic test result. On the other hand, among families with genetically established long QT syndrome, between 10 percent and 37 percent of the relatives with a positive long QT syndrome genetic test have a normal QT interval.
Doctors have described two forms of inherited long QT syndrome:
- Romano-Ward syndrome. This more common form occurs in people who inherit only a single genetic variant from one parent.
- Jervell and Lange-Nielsen syndrome. This rare form usually occurs earlier and is more severe. In this syndrome, children inherit genetic variants from both parents. They have long QT syndrome and also are born deaf.
Additionally, scientists have been investigating a possible link between sudden infant death syndrome (SIDS) and long QT syndrome and have discovered that approximately five to 10 percent of babies affected by SIDS (sudden infant death syndrome) had a genetic defect or mutation for long QT syndrome.
Acquired long QT syndrome
Acquired long QT syndrome can be caused by certain medications, electrolyte abnormalities such as low body potassium (hypokalemia) or medical conditions. More than 100 medications — many of them common — can lengthen the QT interval in otherwise healthy people and cause a form of acquired long QT syndrome known as drug-induced long QT syndrome.
Medications that can lengthen the QT interval and upset heart rhythm include:
- Certain antibiotics
- Certain antidepressant and antipsychotic medications
- Some antihistamines
- Diuretics
- Medications used to maintain normal heart rhythms (antiarrhythmic medications)
- Cholesterol-lowering medicines and some diabetes medicines
- Some anti-nausea medications
People who develop drug-induced long QT syndrome might also have some subtle genetic defects in their hearts. These defects make them more likely to have disruptions in their heart rhythm from certain medications.
Some people who have medication-induced long QT syndrome also may have an inherited form of the disorder. They may not have symptoms unless they take medicines that lengthen the QT interval or lower potassium levels in the blood. When long QT syndrome doesn’t cause symptoms, it’s called silent long QT syndrome.
Other causes of Acquired Long QT Syndrome
Severe diarrhea or vomiting that causes a major loss of potassium or sodium ions from the bloodstream may cause long QT syndrome. The disorder lasts until these ion levels return to normal.
The eating disorders anorexia nervosa and bulimia and some thyroid disorders may cause a drop in potassium ion levels in the blood, causing long QT syndrome.
Risk factors for long QT syndrome
People who may have a higher risk of inherited or acquired long QT syndrome may include:
- Children, teenagers and young adults with unexplained fainting, unexplained near drownings or other accidents, unexplained seizures, or a history of cardiac arrest
- Family members of children, teenagers and young adults with unexplained fainting, unexplained near drownings or other accidents, unexplained seizures, or a history of cardiac arrest
- First-degree relatives of people with known long QT syndrome
- People taking medications known to cause prolonged QT intervals
- People with low potassium, magnesium or calcium blood levels — such as those with the eating disorder anorexia nervosa
Inherited long QT syndrome often goes undiagnosed or is misdiagnosed as a seizure disorder, such as epilepsy. However, long QT syndrome might be responsible for some otherwise unexplained deaths in children and young adults. For example, an unexplained drowning of a young person might be the first clue to inherited long QT syndrome in a family.
- You’re at risk of having long QT syndrome if anyone in your family has ever had it. Unexplained fainting or seizures, drowning or near drowning, and unexplained sudden death are all possible signs of long QT syndrome.
- You’re also at risk for long QT syndrome if you take medicines that make the QT interval longer. Your doctor can tell you whether your prescription or over-the-counter medicines might do this.
- You also may develop long QT syndrome if you have excessive vomiting or diarrhea or other conditions that cause low blood levels of potassium or sodium. These conditions include the eating disorders anorexia nervosa and bulimia, as well as some thyroid disorders.
Long QT syndrome prevention
If you have inherited long QT syndrome, be careful about which medications you take. Some medications — including certain appetite suppressants, decongestants and common antibiotics — might trigger dangerous heart rhythms. Ask your doctor what you can and can’t take safely. Illegal drugs, such as cocaine and amphetamines, pose a serious risk for people with long QT syndrome.
In addition, seek medical treatment right away for illnesses that could result in low blood-potassium levels, especially if you have a lot of vomiting and diarrhea. Such illnesses could trigger an episode of long QT syndrome. Your doctor might advise you not to take some drugs, such as diuretics, that lower blood-potassium levels.
Some people — especially older adults with long QT syndrome who haven’t had signs or symptoms of the condition in decades — may not need any treatment other than preventive measures.
Long QT syndrome diagnosis
If long QT syndrome is suspected, your doctor will want to ask questions about your medical history, as well as your family’s.
Your doctor will also ask you if you have a:
- Family history of long QT syndrome
- Family history of unexplained fainting, seizures, or cardiac arrest
- History of fainting, seizures or cardiac arrest, especially with exercise
For example, studies of otherwise healthy people with long QT syndrome indicate that they had at least one episode of fainting by age 10. The majority also had a family member with long QT syndrome.
Unexplained fainting episodes or a family history of heart-related death may warrant electrocardiogram (EKG or ECG) testing for you and your closes relatives. Your doctor may also recommend an exercise stress test.
If your doctor thinks you may have long QT syndrome, you might need several tests to confirm the diagnosis. These include:
- Electrocardiogram (ECG). During an ECG, doctors attach sensors to your chest (electrodes) that can detect the electrical activity of your heart. An ECG measures the timing and duration of each electrical phase in your heartbeat. You might have this test while at rest or during an exercise stress test, in which doctors monitor your heart activity as you exercise on a treadmill or a stationary bicycle. Your doctor may also suggest your family members have ECGs.
- Holter monitor. This portable ECG device can be worn for a day or more to record your heart’s activity as you go about your routine.
- Event monitor. This portable ECG device is attached to your body to monitor your heart activity over a few weeks to a few months. When you have symptoms, you press a button. This allows your doctor to check your heart rhythm at the time of your symptoms.
Long QT syndrome is usually diagnosed by measuring the Q-T interval on the ECG.
In some people with suspected long QT syndrome, the ECG doesn’t show an abnormally prolonged QT interval. You may need other tests, such as:
- Exercise stress test. Some people have a long QT interval only while they exercise. For this reason, your doctor may recommend that you have a stress test. During an exercise stress test, you exercise to make your heart work hard and beat fast. An EKG is done while you exercise. If you can’t exercise, you may be given medicine to increase your heart rate.
- A nonexercise (medication) stress test. This is an ECG test done while you’re given a medication such as epinephrine (Adrenalin) that stimulates your heart in a way similar to exercise. Doctors then monitor the effects of the medication on the way your heart recharges. This test can help doctors diagnose people with suspected long QT syndrome and may help determine which genes are associated with the condition. It may also be used to diagnose people with long QT syndrome who have a gene associated with long QT syndrome but who have a normal QT interval (recharging time) at rest.
- Genetic testing. A genetic test for long QT syndrome is available and may be covered by some private and governmental insurance plans. Genetic tests for long QT syndrome can generally find the genetic cause for about 3 out of every 4 cases of inherited long QT syndrome. However, genetic tests can’t detect all cases of long QT syndrome. So, even if you have long QT syndrome, the genetic tests may not show it. Also, some people who test positive for long QT syndrome don’t have any signs or symptoms of the disorder. These people may have silent long QT syndrome. Less than 10 percent of these people will faint or suddenly die from an abnormal heart rhythm. Even if you have silent long QT syndrome, you may be at increased risk of having an abnormal heart rhythm while taking medicines that affect potassium ion channels or blood levels of potassium. If your genetic cause of long QT syndrome is discovered through a positive genetic test, your doctor may recommend that your family members also be tested to determine whether they inherited the same genetic mutation.
- A second opinion. You might want to seek a second opinion before proceeding with treatment if your doctor diagnoses you with long QT syndrome. People can sometimes be misdiagnosed as having long QT syndrome when it’s not actually present.
Long QT syndrome treatment
Treatment is aimed at preventing sudden death and controlling symptoms.
Treatment for inherited long QT syndrome involves some simple preventive measures. It can also involve medications, as well as left cardiac sympathetic denervation surgery or implanting medical devices such as a defibrillator (ICD), or both.
The goal of treatment is either to prevent the long QT heart from ever beating out of control or to prevent sudden death. Your doctor will discuss with you the most appropriate treatment options for your condition based on your symptoms, your type of long QT syndrome, and your risk of fainting or sudden cardiac arrest.
For acquired long QT syndrome, treating the cause of the condition may eliminate it. Doctors will also treat heart rhythm disorders (arrhythmias) as needed.
If you are diagnosed with acquired long QT syndrome due to certain medications, your doctor may recommend that you stop taking the medication causing the condition and switching medications. Some people might need additional treatment.
Medications
Medications used to treat long QT syndrome may include:
- Beta blockers. These heart drugs include nadolol (Corgard) and propranolol (Inderal LA, InnoPran XL). They slow the heart rate and make the rhythm associated with long QT syndrome less likely. Beta blockers work by blunting the way your heart reacts to adrenaline. Most patients (even those without symptoms) are treated with a beta-blocker. Other medications may be used to shorten the Q-T interval. Your doctor will discuss what medications are best for you.
- Mexiletine. Taking this anti-arrhythmic drug in combination with beta blockers might help shorten the QT interval and decrease the likelihood of a long QT syndrome-triggered faint, seizure or sudden death. This medication is often used for the third-most common subtype of inherited long QT syndrome, LQT3. However, it may also be used for the two most common subtypes, LQT1 and LQT2.
- Spironolactone and potassium. For certain forms of long QT syndrome, spironolactone (Aldactone), a medication used to help the body hold on to potassium, or potassium supplements, or both, might improve the heart’s recharging system.
- Fish oil. In general, current evidence does not support supplementation with heart-healthy fish oil (omega-3 fatty acid) or eating fish high in omega-3 fatty acids to decrease the risk of cardiac events or death from abnormal heart rhythms. However, if you have inherited long QT syndrome, fish oil may be a reasonable complementary alternative medication to take in addition to other therapies. Talk to your doctor before starting fish oil or any other supplements or medications.
Your doctor might suggest treatment for long QT syndrome even if you don’t often experience signs or symptoms.
If you do need treatment, take the medications your doctor prescribes as directed. While medications won’t cure the condition, they provide some protection against possibly fatal disruptions of your heart rhythm. You might need to take a medication such as a beta blocker indefinitely.
Medical Devices
- Patients who have a history of cardiac arrest or symptoms, in spite of beta-blocker therapy, may receive an implantable cardioverter defibrillator (ICD). This device detects life-threatening arrhythmias and automatically shocks the heart to prevent sudden death. The implantable cardioverter-defibrillator (ICD) device is implanted under the skin of your chest, can stop a potentially fatal arrhythmia. An implantable cardioverter defibrillator (ICD) continuously monitors your heartbeat. If it detects an abnormal heart rhythm, it delivers electrical shocks to reset the heart to a normal rhythm. Implanting an implantable cardioverter defibrillator (ICD) is a major procedure and can result in inappropriate shocks and other complications. Therefore, the decision to implant an implantable cardioverter defibrillator, especially in children, needs to be carefully considered. Most people with inherited long QT syndrome do not need an implantable cardioverter defibrillator. Importantly, an implantable cardioverter defibrillator should not be implanted solely because of the tragic occurrence of a long QT syndrome-triggered sudden death in a relative.
- Patients who have an abnormally slow heart rate may receive a pacemaker.
Left cardiac sympathetic denervation surgery
In this procedure, surgeons cut specific nerves along the left side of your spine in your chest. These nerves are part of the body’s sympathetic nervous system, which helps regulate heart rhythm that prompt your heart to beat faster in response to physical or emotional stress. This type of surgery keeps the heart beating at a steady pace and lowers the risk of dangerous heart rhythms in response to stress or exercise. The surgery also significantly reduces the risk of sudden death.
This surgery is generally reserved for people who are considered at high risk of sudden death and are experiencing appropriate implantable cardioverter defibrillator (ICD) shocks, people who are continuing to experience fainting or seizures while taking their medications, or people unable to tolerate their medications because of side effects.
Lifestyle changes
In addition to medications or surgery, your doctor might recommend lifestyle changes to reduce your chances of a long QT syndrome-related fainting spell or sudden cardiac arrest. These could include:
- Family testing – All first-line relatives (brothers, sisters, parents and children) should have EKG testing. Any other family members who have a history of seizures or fainting should also undergo testing.
- Avoiding strenuous exercise or contact sports – If you have long QT syndrome, sometimes, fatal arrhythmias occur with exercise. The decision to participate in competitive sports should be managed by a heart rhythm expert and certain precautions may be suggested. Or have a safety plan in place if you continue in competitive sports
- Buddy system – Your family and friends should be told you have long QT syndrome. They should be told to call for emergency help (911) if you begin to have symptoms or faint.
- Avoiding medications that could cause prolonged QT intervals
- Getting plenty of liquids during illnesses that are causing vomiting or diarrhea
- Lowering your temperature if a fever occurs
- Reducing your exposure to loud or startling noises
- Staying away from situations that could make you excited or angry
Work with your doctor to balance these lifestyle recommendations against the clear, heart-healthy benefits of an active lifestyle. It may be possible to stay fully active in sports, including competitive sports, after carefully reviewing the risks and benefits with your doctor.
If your symptoms are mild or don’t occur very often, your doctor might recommend only simple preventive measures or lifestyle changes, and he or she might not prescribe any daily medications for you.
Future treatments will be geared toward more gene specific therapies. For example, certain types of long QT syndrome are more likely to initiate events during exercise, while others are more related to startling or emotional distress. Your doctor will be able to give you activity guidelines based on the specific type of long QT syndrome gene you carry. Therapies may be directed to treat the specific gene, rather than prevention of future complications.
References [ + ]





{kind=link}