Contents
What is an LVAD
LVAD or left ventricular assist device is a kind of artificial heart pump. Left ventricular assist device is sometimes called a “bridge to transplant,” but is now used in long-term therapy. LVAD is used to treat people with severe heart failure and is sometimes given to people on the waiting list for a heart transplant. People awaiting a heart transplant often must wait a long time before a suitable heart becomes available. During this wait, the patient’s already-weakened heart may deteriorate and become unable to pump enough blood to sustain life. An LVAD can help a weak heart and “buy time” for the patient or eliminate the need for a heart transplant. Most recently, LVADs are being used longer-term as ‘destination therapy’ in end-stage heart failure patients when heart transplantation is not an option.
Normally, the left ventricle, one of your heart’s four chambers, pumps blood into your aorta (the large artery leaving the heart) and around your body. In the event that someone has severe heart failure, the heart is too weak to pump enough blood around the body.
Having an LVAD involves open heart surgery. Surgeons attach one end of the LVAD pump to the left ventricle and the other end to the aorta. Blood flows from the left ventricle into the LVAD. The left ventricular assist device pumps the blood out into the aorta, where it then flows to the rest of your body.
These are continuous flow centrifugal pumps, of which the HeartWare and Heartmate 3 are most popular 1. They are designed for long durability (5 to 10 years), easy surgical placement, and low risk of hemolysis or thrombosis. Smaller devices are currently in the testing phase.
Some patients being considered for a heart transplant may need to have an LVAD implanted if they are unlikely to survive until a suitable donor heart becomes available. The left ventricular assist device helps the failing heart and aims to restore normal blood flow.
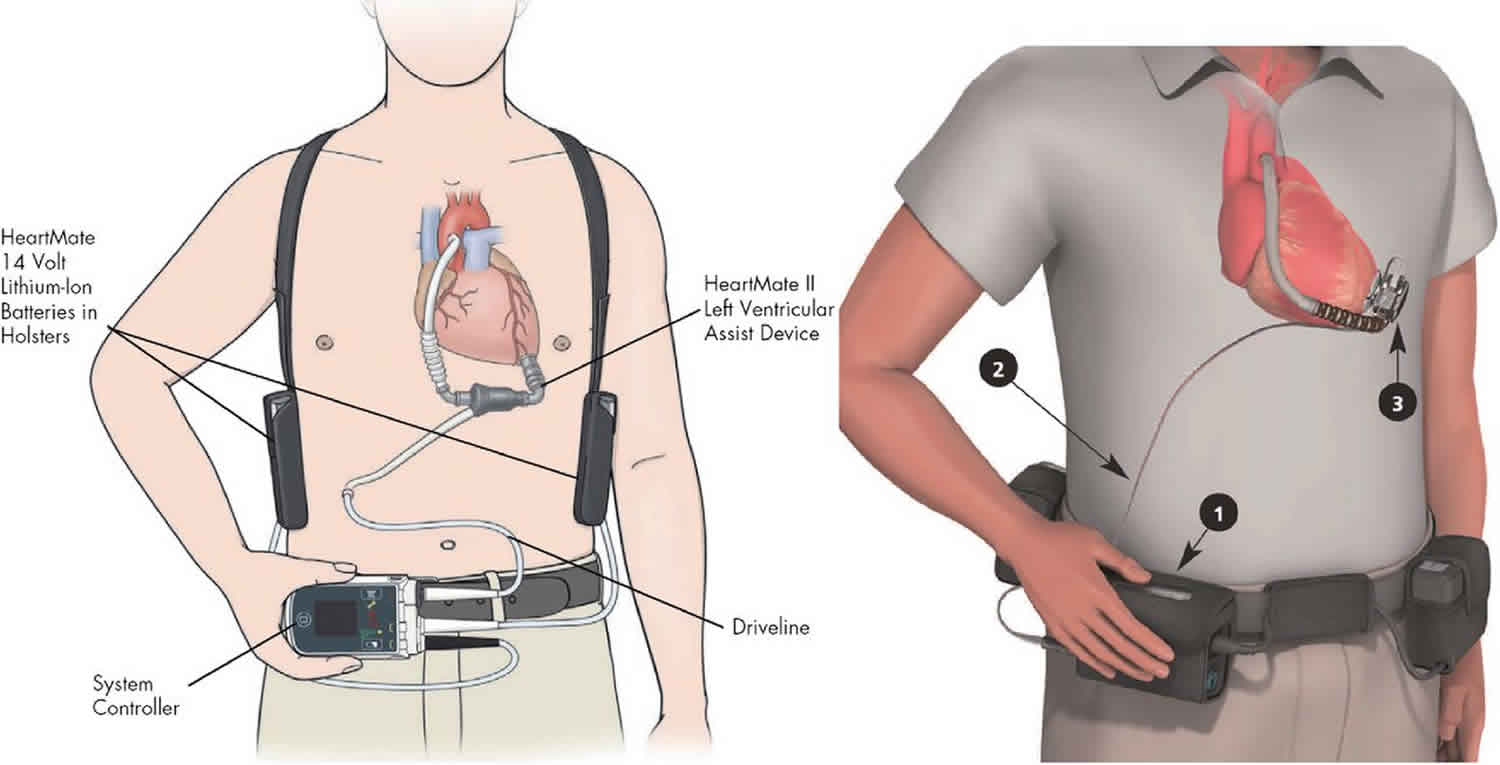
A LVAD has 3 parts:
- A pump. The pump weighs 1 to 2 pounds (0.5 to 1 kilogram). It is placed inside or outside of your belly.
- An electronic controller. The controller is like a small computer that controls how the pump works.
- Batteries or another power source. The batteries are carried outside your body. They are connected to the pump with a cable that goes into your belly.
How does an LVAD work?
A common type of LVAD has a tube that pulls blood from the left ventricle into a pump. The pump then sends blood into the aorta (the large blood vessel leaving the left ventricle). This effectively helps the weakened ventricle. The pump is placed in the upper part of the abdomen. Another tube attached to the pump is brought out of the abdominal wall to the outside of the body and attached to the pump’s battery and control system.
A fine cable called the driveline connects the LVAD, which is inside your body, through the skin and to a controller, which is outside your body. The controller senses the function of the LVAD and controls the power to make it work. The controller connects to an external battery pack.
LVADs are now portable and are often used for weeks to months. Patients with LVADs can be discharged from the hospital and have an acceptable quality of life while waiting for a donor heart to become available.
How reliable is LVAD battery power?
People’s lives depend on their LVADs working properly, so the left ventricular assist device needs to be extremely reliable and have built-in safety systems.
Average number of hours that an LVAD battery lasts 4-6.
If the battery starts to run low, an alarm sounds to let the person know that it needs changing. An additional battery is always connected to the controller, so if one battery runs down, there is another to power the LVAD for several more hours. Additionally, there is back-up circuitry in the controller, so if the primary circuitry happens to fail, the back-up system kicks in. Modern LVADs are, therefore, very reliable and can support patients for years.
People can choose how they wear their controller and the two batteries. They can put everything into one pack and carry it as a shoulder bag or rucksack. Or they can separate the components and wear them on a belt with a loop, like you might with a camera or mobile phone.
Everyone is given a portable charger when they leave hospital, so they can charge the batteries anywhere. They are also given an adapter to plug the charger into a car cigarette lighter, so the battery can be recharged during long journeys.
Is everyone with heart failure considered for an LVAD?
Heart failure usually develops because the heart has been damaged by a heart attack or as a result of other conditions such as cardiomyopathy – a disease of the heart muscle. Some patients who have very severe heart failure, which cannot be managed with medicines or other treatments may be considered for a heart transplant.
However, during the wait for a suitable donor, some patients continue to deteriorate. In these cases, implanting an LVAD can be life saving and buys more time for the patient until we can find a suitable donor heart.
LVAD Indications
Bridge-to-Transplantation
The purpose of Bridge-to-Transplantation (BTT) is to provide circulatory support to transplant-eligible patients with HFrEF until a donor’s heart becomes available.
Destination therapy
Destination therapy (DT) is used in patients with HFrEF who are ineligible for cardiac transplantation. The newer devices with improved durability have shown increased survival rates in this category of patients.
Bridge-to-the-Decision
LVADs have been used as a temporary measure in patients with end-organ dysfunction due to HF (relative contraindication to transplantation). Stabilization of hemodynamics with improvement in renal function, nutritional status, and reduction in pulmonary hypertension can help make them transplant eligible.
Bridge-to-Recovery
Bridge-to-Recovery (BTR) provides temporary ventricular support in some HF patients has shown to improve myocardial function and promote recovery.
Strong indications for either Bridge-to-Transplantation, Destination Therapy or Bridge-to-Recovery are as follows. All must be applicable 1:
- NYHA class 4 for 60 to 90 days
- Maximal tolerated medical therapy and certified respiratory therapy/implantable cardioverter-defibrillator if indicated
- Chronic dependence on inotropic agents
- LVEF less than 25%
- Pulmonary capillary wedge pressure greater than or equal to 20 mmHg
- Systolic BP less than or equal to 80 to 90 mmHg or cardiac index less than or equal to 2 L/min/m2, evidence of declining renal or right ventricular function.
LVAD Contraindications
- Right ventricular dysfunction: Either primarily or right heart failure not secondary to left heart failure. Improper function of the right ventricle leads to insufficient filling of the left heart which may lead to inadequate inflow in the device and ultimately device malfunction.
- Acute cardiogenic shock with a neurological compromise: Without adequate higher functions, LVAD placement is not recommended as it would only increase morbidity and decrease the quality of life.
- Coexisting severe terminal comorbidity: Severe renal, pulmonary, liver or neurological disease or evidence of advanced metastatic cancer are considered contraindications.
- Bleeding: Active bleeding or thrombocytopenia (platelet count less than 50000 x 10 per L) or confirmed heparin-induced thrombocytopenia. Not just the bleeding but also the inability to be placed on anticoagulation makes this a contraindication.
- Anatomical factors: Hypertrophic cardiomyopathy or a large ventricular septal defect are a hindrance to devise placement and function.
- Technical limitations: Body surface area less than 1.2 to 1.5 m2 or any other factor.
- Social considerations: LVAD management requires a high degree of patient compliance which necessitates adequate psychological function to comply with medications and device maintenance. It also requires family education in interpreting basic function and alarms. Thus, any difficulty posed by such factors could pose a contraindication to LVAD placement.
LVAD procedure
If you are having an implanted LVAD placed, you will need general anesthesia. This will make you sleep and be pain-free during the procedure.
During surgery:
- The heart surgeon opens the middle of your chest with a surgical cut and then separates your breastbone. This allows access to your heart.
- Next, the surgeon will make space for the pump under your skin and tissue in the upper part of your belly wall.
- The surgeon will then place the pump in this space.
A tube will connect the pump to your heart. Another tube will connect the pump to your aorta or one of your other major arteries. Another tube will be passed through your skin to connect the pump to the controller and batteries.
The LVAD will take blood from your left ventricle (the main pumping chamber of the heart) through the tube that leads to the pump. Then the device will pump the blood back out into the aorta and through your body.
Surgery most often lasts 4 to 6 hours.
There are other types of VADs (called percutaneous ventricular assist devices) which can be placed with less invasive techniques to help the left or right ventricle. However, these typically cannot provide as much flow (support) as the surgically implanted ones.
After the LVAD procedure
Most people who are put on a LVAD spend from a few to several days in the intensive care unit (ICU) after surgery. You may stay in the hospital from 2 to 8 weeks after you have had the pump placed. During this time you will learn how to care for the pump.
Less invasive ventricular assist devices are not designed for ambulatory patients and those patients need to stay in the ICU for the duration of their use. They are sometimes used as a bridge to a surgical ventricular assist device or heart recovery.
LVAD complications
Risks for LVAD surgery are:
- Blood clots in the legs that may travel to the lungs
- Blood clots that form in the device and can travel to other parts of the body
- Breathing problems
- Heart attack or stroke
- Allergic reactions to the anesthesia medicines used during surgery
- Infections
Hematological
Bleeding is the most common complication, occurring in both the perioperative period as well as later due to the need for anticoagulation with warfarin. Cardiopulmonary bypass perioperatively alters the coagulation cascades and impairs the normal clotting mechanism, leading to bleeding. Also, bleeding has been attributed to the association of acquired von Willebrand disease in LVAD patients, typically more than a week after the procedure. This is usually reversible if the LVAD is removed.
Bleeding may occur due to a leak at the pump site from polyester grafts in the conduits, the gastrointestinal mucosal surfaces, and intracranial vessels. The target INR in outpatients is usually 1.5 to 2.5.
Thrombosis is another significant hematological complication Patients may develop pump thrombosis, embolic events, or stroke. It is usually due to subtherapeutic anticoagulation, atrial fibrillation, or infection that predisposes to a hypercoagulative state.
Hemolysis is another possibility due to technical complications involving the design of the pump, malpositioned cannulae, or development of heparin-induced thrombocytopenia and pump thrombosis.
Right Heart Failure
Anatomic changes following LVAD placement cause right ventricular geometric alterations. With left ventricular (LV) unloading, the septum shifts to the left. The increased cardiac output from the LVAD results in an increased venous return to the right ventricle, which now has improved compliance. However, in patients with chronic heart failure, there is pre-existing pulmonary hypertension. This can result in right ventricular (RV) failure.
This may necessitate the use of milrinone to reduce pulmonary vascular resistance or epoprostenol as a selective pulmonary vasodilator. In some circumstances, use of RV mechanical support or ECMO may be required.
Infection
The International Society of Heart and Lung Transplantation has classified infections based on their relationship to the LVAD. Infections usually occur at the pump site, pump pocket, or the driveline. They typically present with localized warmth and erythema at the pump site, along with fever and leukocytosis. Ultrasound of the local region can diagnose such collections and also guide aspiration. Swabs are helpful in guiding treatment.
Most commonly, the gram-positive Staphylococcus aureus is isolated, but Enterococcus and other Staphylococcal species may be present. The most common gram-negative organism is Pseudomonas aeruginosa. Aggressive treatment is indicated with the use of appropriate antibiotics to cover the involved pathogen. Surgical revision of the driveline away from the infection may be needed. However, the pump usually needs to be replaced. Surgical debridement may be needed for deeper infections, with use of omental or muscle flaps or vacuum-assisted closure techniques described. Infection is associated with significantly increased mortality rates. Hence, severe infections may warrant device explantation with use of extracorporeal membrane oxygenation (ECMO) or cardiac transplantation as definitive treatment.
Neurological
Stroke is one of the most dreaded complications of LVAD placement. Both ischemic and hemorrhagic strokes are known to occur, either immediately postoperatively or after several months. Strokes more commonly affect the right hemisphere, indicating a cardioembolic source. Ischemic events have been attributed to partial obstruction of the inflow cannula, deformation of blood in the pump apparatus, outflow graft obstruction, subtherapeutic anticoagulation or infection. The risk of hemorrhagic stroke is due to anticoagulation. Hence, a fine balance is necessary to achieve optimum anticoagulation.
Arrhythmias
Ventricular arrhythmias are common after the procedure. Placement of the cannula can cause reentrant circuits. Suction can lead to contact between the cannula and ventricular septum, triggering an arrhythmia. Significant changes in weight or development of scar tissue can create malposition of the cannula, leading to arrhythmias. Usually, development of such arrhythmias can be managed by a change in device settings, such as reducing the speed of the LVAD to allow adequate ventricular filling. Management with a variety of medications is usually successful, however refractory cases require catheter ablation or device exchange.
LVAD heart pump life expectancy
Most people will already be in the hospital for treatment of their heart failure. A LVAD may help people who have heart failure live longer. It may also help improve patients’ quality of life. However, not everyone with severe heart failure is a good candidate for this procedure.
You may get LVAD while you are on a waiting list for a heart transplant. Some people who get a LVAD are very ill and may already be on a heart-lung support machine.
The landmark REMATCH trial 2 that compared LVADs with optimal medical therapy in class 4 heart failure patients found a 48% reduction in mortality from any cause. There was also a significant increase in the survival rates at one year (52% versus 25%) and two years (23% versus 8%) 1.
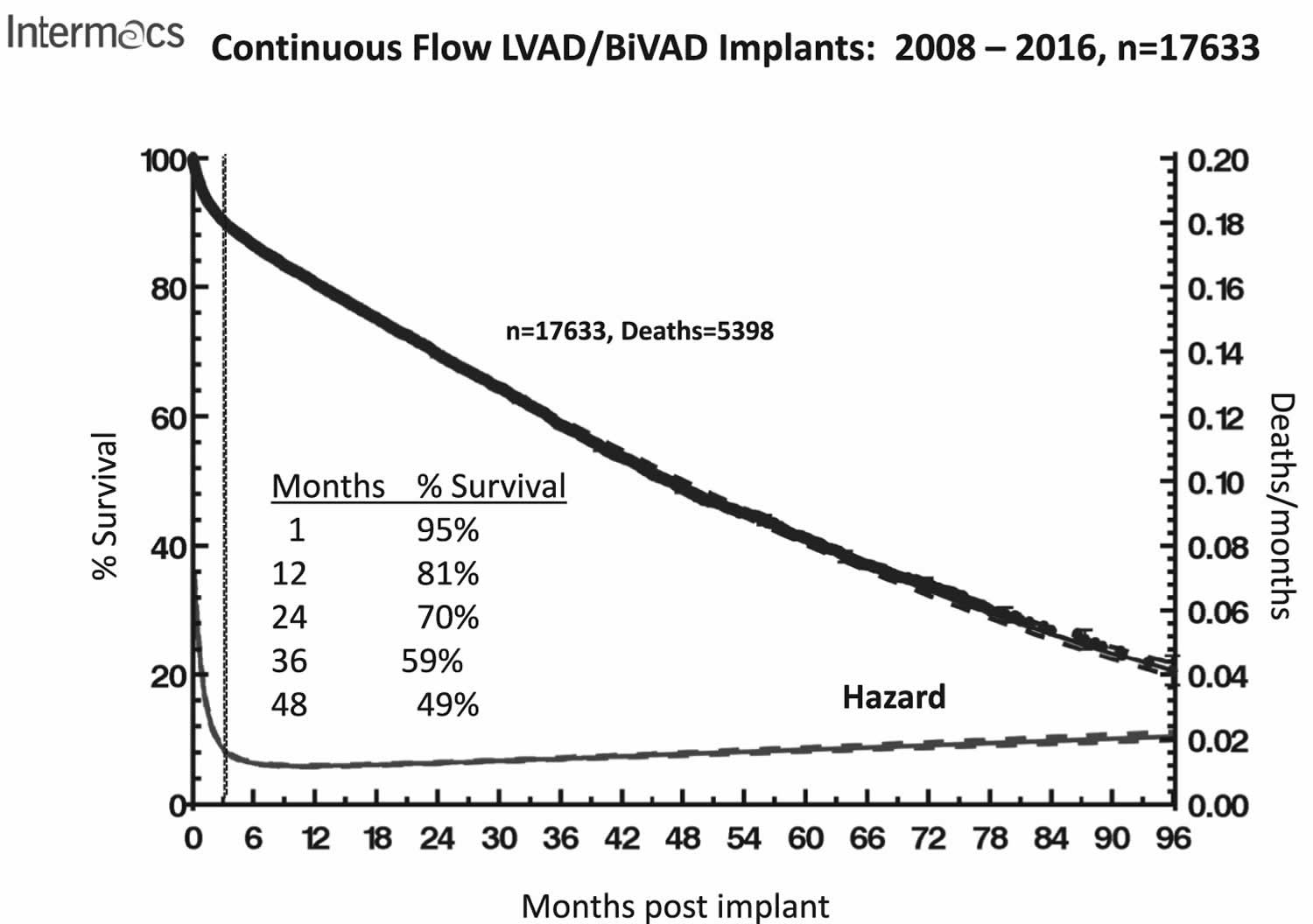
Figure 1. LVAD heart pump life expectancy (the overall survival curve has remained essentially unchanged since 2013)
How long can you live with an LVAD?
Implanting an LVAD can be life saving and buys more time for the patient until your heart transplant team can find a suitable donor heart. According to the Interagency Registry for Mechanically Assisted Circulatory Support (INTERMACS) report which has >20,000 patients from >180 hospitals 3. Of the 18,987 primary left ventricular assist device (LVAD) implants, >90% have been continuous flow devices. Overall survival continues to remain 81% at 1 year, 70% at 2 years, 59% at 36 months and 49% at 4 years 3. Review of major adverse events shows minimal advantage for patients with ambulatory heart failure pre-implant. Stroke, major infection, and continued inotrope requirement during the first 3 months have a major effect on subsequent survival.
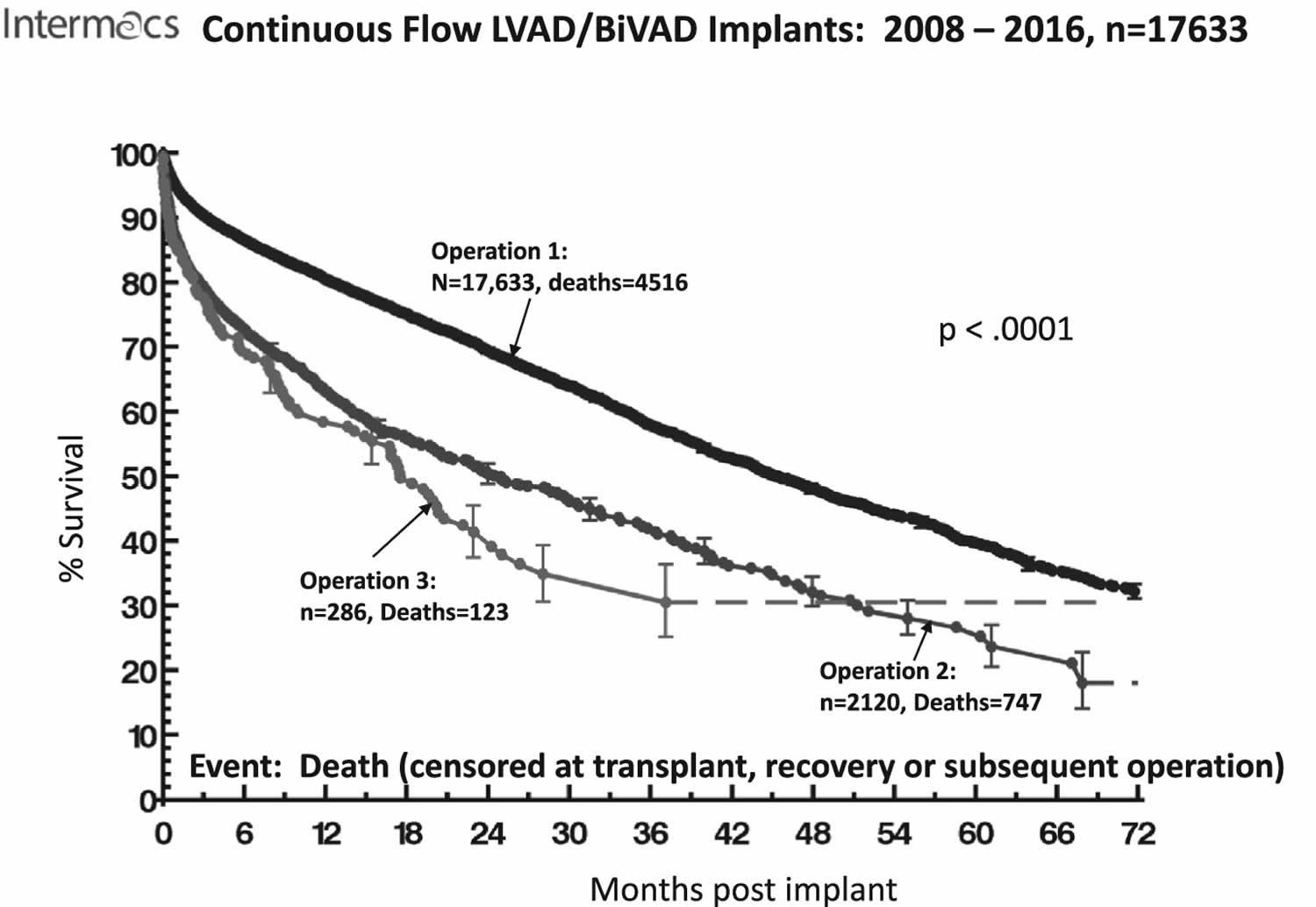
The negative survival impact of reoperations (most commonly for pump exchange) is highlighted in Figure 2.
Figure 1. LVAD heart pump life expectancy according to pump replacement operation
- Vaidya Y, Dhamoon AS. Left Ventricular Assist Devices (LVAD) [Updated 2018 Oct 27]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK499841[↩][↩][↩]
- Rose EA, Gelijns AC, Moskowitz AJ, et al. Long-term use of a left ventricular assist device for end-stage heart failure. N Engl J Med. 2001;345:1435–1443 https://www.nejm.org/doi/10.1056/NEJMoa012175[↩]
- Eighth annual INTERMACS report: Special focus on framing the impact of adverse events. Kirklin, James K. et al. The Journal of Heart and Lung Transplantation , Volume 36 , Issue 10 , 1080 – 1086 https://www.jhltonline.org/article/S1053-2498(17)31896-X/pdf[↩][↩][↩][↩]





{kind=link}