Contents
- What is MCHC blood test
What is MCHC blood test
MCHC blood test short for mean corpuscular hemoglobin concentration (MCHC), is a calculation of the average concentration or percentage of hemoglobin inside a single red blood cell. MCHC correlates the hemoglobin content with the volume of the red blood cell. MCHC is most useful in monitoring the treatment of anemia. MCHC is expressed as g/dl of red blood cells or as a percentage value. The normal values for MCHC are 34 ± 2 g/dl – adult all ages = 32 to 36 g /dl and newborn = 32 to 33 g /dl.
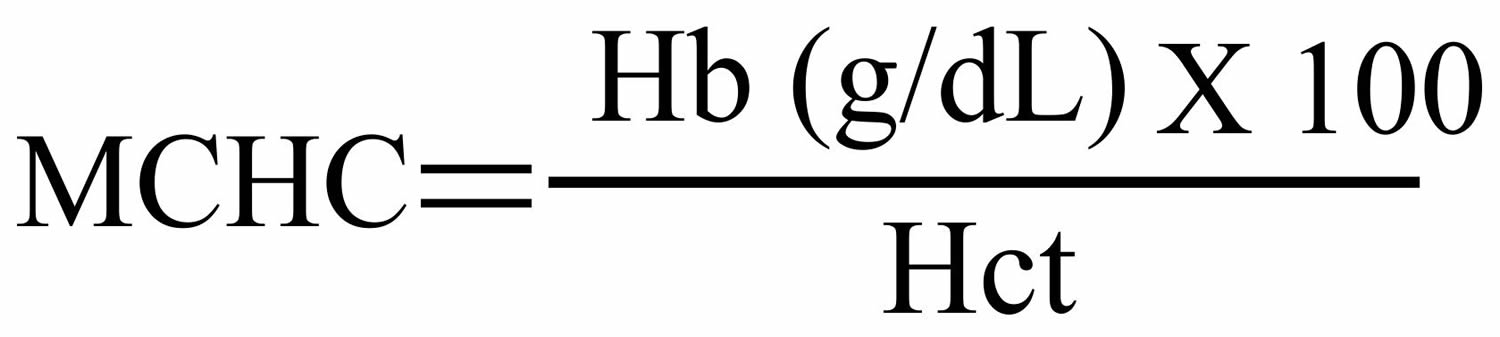
MCHC is calculated by dividing the hemoglobin (Hb) concentration by hematocrit (Hct). A hematocrit (Hct) is a test that measures the proportion of a person’s blood that is made up of red blood cells (RBCs). Blood consists of RBCs, white blood cells (WBCs), and platelets suspended in a fluid portion called plasma. The hematocrit is a ratio of the volume of red blood cells to the volume of all these components together, called whole blood. The value is expressed as a percentage or fraction. For example, a hematocrit value of 40% means that there are 40 milliliters of red blood cells in 100 milliliters of blood. When the values of hemoglobin (Hb), red cell count (the RBC count totals the number of red blood cells that are present in a person’s sample of blood), and mean corpuscular volume (MCV) are affected, MCHC also become abnormal, since MCHC is calculated and are not directly measured.
Figure 1. MCHC calculation
Red blood cells with normal concentration of hemoglobin (MCHC adult all ages = 32 to 36 g /dl) are called normochromic.
- Red blood cells with lower than normal concentration of hemoglobin (MCHC <32% or <32 g/dl) are called hypochromic, it usually means iron deficiency anemia.
- Red blood cells with normal concentration (MCHC 32 to 36% or 32 to 36 g/dl) of hemoglobin anemia could be due to blood loss or a chronic disease.
- Red blood cells with higher than normal concentration of hemoglobin (MCHC >36% or >36 g/dl) are called hyperchromic, it usually means folic acid deficiency, vitamin B12 deficiency or myelodysplastic leukemias. In spherocytosis, the MCHC is increased due to loss of membrane and the consequent spherical shape assumed by the cell.
MCHC is one of the measurement or calculation of the components of the Complete Blood Count (CBC), a commonly requested test used to determine your general health status. MCHC (mean corpuscular hemoglobin concentration) measurement is combined with mean corpuscular volume (MCV), mean corpuscular hemoglobin (MCH) and red cell distribution width (RDW) measurement to screen for, diagnose, or monitor any one of a variety of diseases and conditions that affect blood cells, such as anemia, infection, inflammation, bleeding disorder or cancer.
- Mean corpuscular volume (MCV) is a measurement of the average size of a single red blood cell. MCV defines the size of the red blood cells and is expressed as femtoliters (10−15; fl) or as cubic microns (μm3). The normal values for MCV are 87 ± 7 fl.
- Mean corpuscular hemoglobin (MCH) is a calculation of the average amount of hemoglobin inside a single red blood cell. Mean corpuscular hemoglobin (MCH) quantifies the amount of hemoglobin per red blood cell. The normal values for mean corpuscular hemoglobin (MCH) are 29 ± 2 picograms (pg) per cell.
- Red cell distribution width (RDW) is a calculation of the variation in the size of red blood cells. Red cell distribution width (RDW) represents the coefficient of variation of the red blood cell volume distribution (size) and is expressed as a percentage. The normal value for RDW is 13 ± 1.5%.
Hemoglobin is the iron-containing protein found in all red blood cells (RBCs) that gives the cells their characteristic red color (see Figure 3). Hemoglobin enables red blood cells to bind to oxygen in the lungs and carry it to tissues and organs throughout the body. It also helps transport a small portion of carbon dioxide, a product of cell metabolism, from tissues and organs to the lungs, where it is exhaled.
The hemoglobin test measures the amount of hemoglobin in a person’s sample of blood. A hemoglobin level can be performed alone or with a hematocrit, a test that measures the proportion of blood that is made up of red blood cells, to quickly evaluate an individual’s red blood cells. Red blood cells, which make up about 40% (ranging 37-49%) of the blood’s volume, are produced in the bone marrow and are released into the bloodstream when they are, or nearly are, mature. The typical lifespan of an red blood cell is 120 days, and the bone marrow must continually produce new red blood cells to replace those that age and degrade or are lost through bleeding.
Several diseases and conditions can affect red blood cells and consequently the level of hemoglobin in the blood. In general, the hemoglobin level and hematocrit rise when the number of red blood cells increases. The hemoglobin level and hematocrit fall to less than normal when there is a drop in production of red blood cells by the bone marrow, an increase in the destruction of red blood cells, or if blood is lost due to bleeding. A drop in the red blood cell count, hemoglobin and hematocrit can result in anemia, a condition in which tissues and organs in the body do not get enough oxygen, causing fatigue and weakness. If too many red blood cells are produced, polycythemia results and the blood can become thickened, causing sluggish blood flow and related problems.
What red blood cells do?
Your body makes three types of blood cells — white blood cells to fight infection, platelets to help your blood clot and red blood cells to carry oxygen throughout your body.
Red blood cells (RBCs) contain hemoglobin — an iron-rich protein that gives blood its red color. Hemoglobin enables red blood cells to carry oxygen from your lungs to all parts of your body and to carry carbon dioxide from other parts of the body to your lungs so that it can be exhaled.
Most blood cells, including red blood cells, are produced regularly in your bone marrow — a spongy material found within the cavities of many of your large bones. To produce hemoglobin and red blood cells, your body needs iron, vitamin B-12, folate and other nutrients from the foods you eat.
Figure 2. Red blood cells
Figure 3. Red blood cell hemoglobin
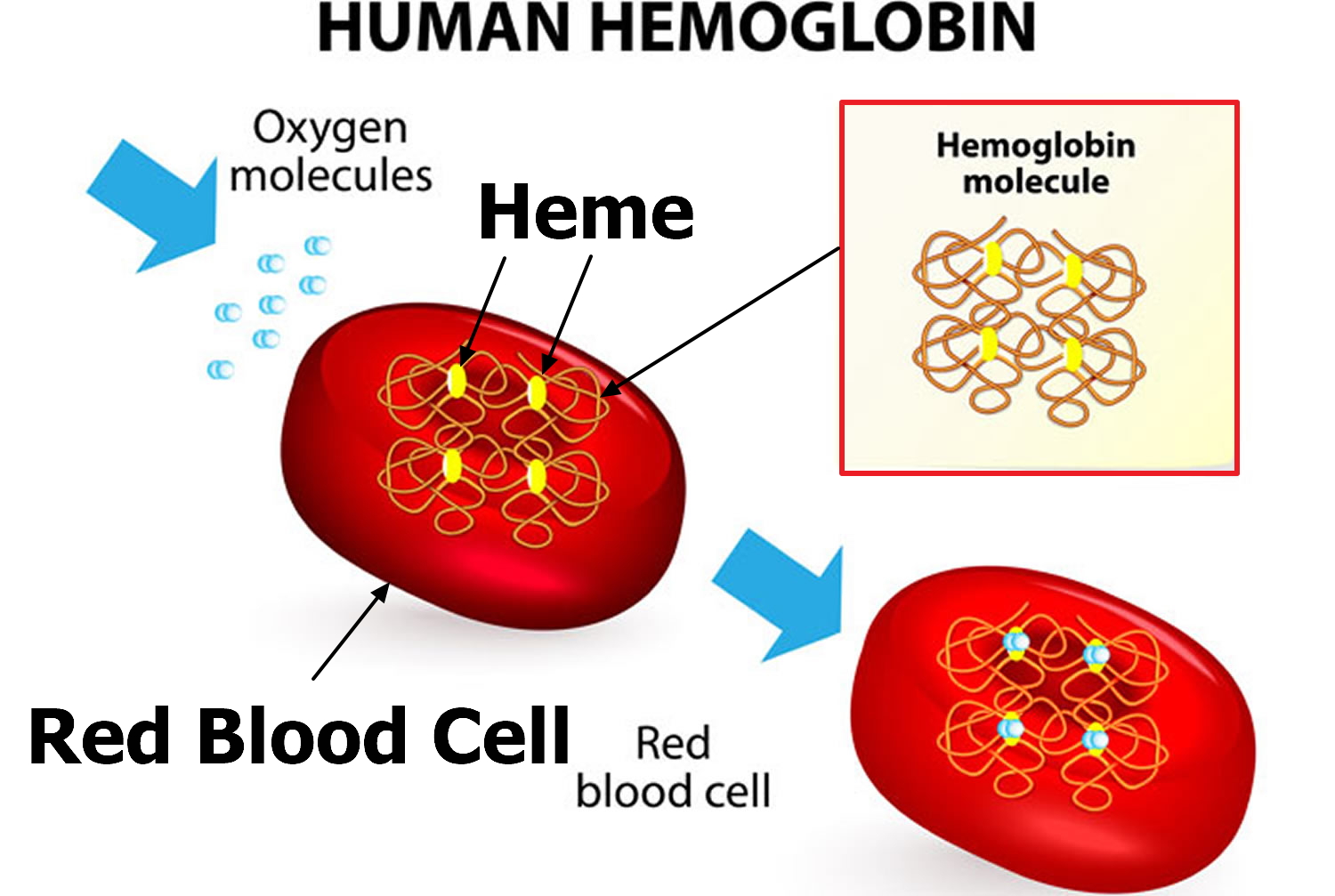
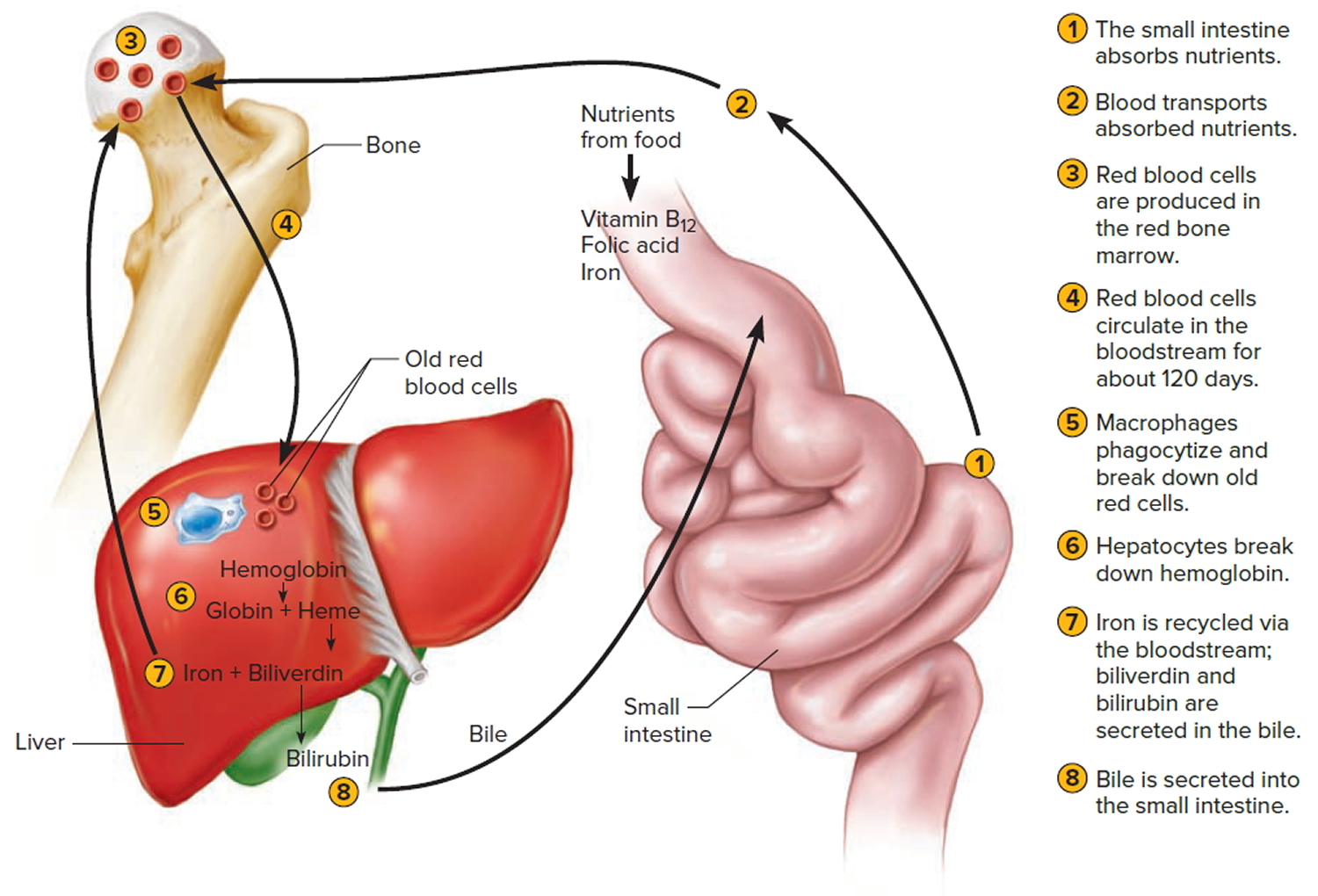
Figure 4. Lifecycle of a red blood cell
What is anemia?
Anemia is a condition in which you don’t have enough healthy red blood cells (RBCs) to carry adequate oxygen to the body’s tissues. Anemia occurs when the amount of hemoglobin in a person’s blood drops below normal. A decrease in hemoglobin is often associated with a decrease in the number of red blood cells (RBCs) and hematocrit. Hemoglobin is contained within red blood cells (RBCs) and is necessary to transport and deliver oxygen from the lungs to the rest of the body. Without a sufficient supply of oxygen, many tissues and organs throughout the body can be adversely affected. People with anemia may experience fatigue, weakness, lack energy, lightheadedness, headache, pallor/jaundice, tachycardia/palpitations, chest pain, dyspnea, and cold distal extremities, and claudication. These symptoms can be quite limiting and are primary negative consequences of anemia. The cause of the anemia modulates the presence and magnitude of these symptoms. The greater the lethal underlying pathology, the more dramatic the symptomatology.
There are many forms of anemia, each with its own cause. Anemia can be temporary or long term, and it can range from mild to severe. See your doctor if you suspect you have anemia because it can be a warning sign of serious illness.
Anemias may be classified based on their etiology (e.g., hemolytic, hemorrhagic, etc.), erythropoietic response (e.g., hypoproliferative, ineffective), or cell morphology (e.g., macrocytic, microcytic-hypochromic). Anemias are classified, according to the size of the red cell, as being normocytic (normal MCV), macrocytic (increased MCV), or microcytic (decreased MCV). Microcytic anemias were also often described as being hypochromic based on peripheral smear examination and MCHC when this value was determined manually. MCHC as measured by the electronic machines is mostly normal in microcytic anemias, however, and the value of MCH closely parallels the value of MCV. The optical properties of the small, thin microcytes make them appear hypochromic on the blood smear, while the hemoglobin concentration remains in the normal range (microcytic, normochromic anemias).
Anemia is a fairly common condition, affecting both men and women of all ages, races, and ethnic groups. However, certain people have increased risk of developing anemia. These include people with diets poor in iron and vitamins, chronic diseases such as kidney disease, diabetes, cancer, inflammatory bowel disease, a family history of inherited anemia, chronic infections such as tuberculosis or HIV, and those who have had significant blood loss from injury or surgery. Anemia can be mild, moderate, or severe depending on how much the RBC count and/or hemoglobin levels are decreased.
The presence of anemia in conjunction with other pathology adds additional concern. Anemia frequently complicates diabetes, various cancers, chronic kidney disease, cardiovascular disease, hepatitis C, HIV/AIDS, inflammatory bowel disease, rheumatoid arthritis and, despite compensatory polycythemia, chronic obstructive pulmonary disease (COPD).
Treatments for anemia range from taking supplements to undergoing medical procedures. You may be able to prevent some types of anemia by eating a healthy, varied diet.
Anemia signs and symptoms
Though different types of anemia have different causes, the signs and symptoms can be very similar. Mild or moderate forms of anemia may cause few, if any, symptoms. Some of the most common symptoms are:
- General feeling of tiredness or weakness (fatigue)
- Lack of energy
- Pale skin (pallor) or yellowish skin
- Dizziness or lightheadedness
- Headaches
- Fatigue
Other signs and symptoms that may develop as the anemia becomes more severe include a feeling of cold or numbness in hands and/or feet, shortness of breath, fast or irregular heartbeat, and chest pain.
Anemia causes
Anemia occurs when your blood doesn’t have enough red blood cells. This can happen if:
- Your body doesn’t make enough red blood cells
- Bleeding causes you to lose red blood cells more quickly than they can be replaced
- Your body destroys red blood cells
In general, the main causes of anemia include:
- Impaired or decreased production of RBCs by the bone marrow due to nutritional deficiency (e.g., iron deficiency, B vitamin deficiencies), bone marrow failure (e.g., aplastic anemia, myelodysplastic syndrome), or diseases that involve the bone marrow (e.g., infection, lymphoma, solid tumor)
- Loss of RBCs due to bleeding or to increased destruction of RBCs as in hemolytic anemia
Anemia may be acute or chronic. Chronic anemia may develop slowly over a period of time with long-term illnesses such as diabetes, chronic kidney disease, or cancer. In these situations, the anemia-related symptoms may not be apparent because the underlying disease masks its symptoms and/or the body adapts to anemia when it develops over a period of time. The presence of anemia in chronic conditions may often go undetected for a period of time and sometimes may only be discovered during tests or examinations for other conditions.
Anemia may also occur in acute episodes such as with substantial blood loss (extensive injury or invasive surgery) or with certain anemias in which a significant number of RBCs are destroyed known as hemolytic anemia. Signs and symptoms may become apparent very quickly, and the cause can be determined from a combination of physical examination, medical history, and testing.
Types of anemia
Anemias can also be described based on the RBC size and concentration of hemoglobin in them. If cell size is much smaller than normal, it is known as microcytic anemia. If it is much bigger than normal, then it is macrocytic anemia. Likewise, if the concentration of hemoglobin is much lower than normal, it is hypochromic anemia; if the concentration is much higher than normal, the RBCs are called hyperchromic.
Within the two broad categories of general causes of anemia, there are several types with different specific causes. Some of the most common types are summarized in the table below.
Table 1. Anemia types
| Type of Anemia | Description | Examples of Causes |
| Iron Deficiency | Deficiency of iron leads to decreased production of hemoglobin; low levels of hemoglobin in turn leads to production of smaller and hypochromic red blood cells. | Blood loss; diet low in iron; poor absorption of iron |
| Pernicious Anemia and B Vitamin Deficiency | Red blood cells do not develop as they normally would because of a lack of B vitamins (B12 and folate); leads to decreased production of red blood cells. | Lack of intrinsic factor (needed for B12 absorption); diet low in B vitamins; decreased absorption of B vitamins |
| Aplastic | Bone marrow is unable to produce enough blood cells; a life-threatening condition. | Cancer therapy, exposure to toxins, autoimmune disease, viral infections |
| Hemolytic | Red blood cells are destroyed faster than the bone marrow can replace them. | Inherited causes such as sickle cell disease and hereditary spherocytosis; other causes include transfusion of incompatible blood, autoimmune disease, certain drugs (penicillin) |
| Anemia of Chronic Diseases | Various conditions over the long term can cause decreased production of red blood cells. | Kidney disease, rheumatoid arthritis, diabetes, tuberculosis, HIV, Crohn disease, cancer, and others |
Table 2. Anemia classified according to cell morphology
| Red cell size as defined by MCV | |||
|---|---|---|---|
| RDW | Decreased (microcytic; low MCV) | Normal (normocytic; MCV = N) | Increased (macrocytic; high MCV) |
| Normal (little or no anisocytosis) | Heterozygous thalassemias | Poor iron utilization | Liver disease |
| Acute blood loss | Aplastic anemia | ||
| Anemia of chronic disease (hypoproliferative) | Enzyme defects (e.g., G6PD deficiency) | Myelodysplastic syndrome | |
| Acute hemolysis | |||
| Liver disease | |||
| Increased (anisocytosis) | Iron deficiency | Early iron deficiency | Megaloblastic |
| Red cell fragmentation | Early megaloblastic | Sideroblastic | |
| Sideroblastic | Myelodysplastic syndrome | ||
| Myelophthisis | Secondary to chemotherapy | ||
| Combined deficiency | |||
| Sickle cell anemia | |||
| Immune hemolysisa | |||
| Secondary to chemotheraphy | |||
- a MCV may be falsely elevated due to cell agglutination, usually with cold agglutinins.
Different types of anemia and their causes include:
- Iron deficiency anemia
This is the most common type of anemia worldwide. Iron deficiency anemia is caused by a shortage of iron in your body. Your bone marrow needs iron to make hemoglobin. Without adequate iron, your body can’t produce enough hemoglobin for red blood cells.
Without iron supplementation, this type of anemia occurs in many pregnant women. It is also caused by blood loss, such as from heavy menstrual bleeding, an ulcer, cancer and regular use of some over-the-counter pain relievers, especially aspirin.
- Vitamin deficiency anemia
In addition to iron, your body needs folate and vitamin B-12 to produce enough healthy red blood cells. A diet lacking in these and other key nutrients can cause decreased red blood cell production.
Additionally, some people may consume enough B-12, but their bodies aren’t able to process the vitamin. This can lead to vitamin deficiency anemia, also known as pernicious anemia.
- Anemia of chronic disease
Certain diseases — such as cancer, HIV/AIDS, rheumatoid arthritis, kidney disease, Crohn’s disease and other chronic inflammatory diseases — can interfere with the production of red blood cells.
- Aplastic anemia
This rare, life-threatening anemia occurs when your body doesn’t produce enough red blood cells. Causes of aplastic anemia include infections, certain medicines, autoimmune diseases and exposure to toxic chemicals.
- Anemias associated with bone marrow disease
A variety of diseases, such as leukemia and myelofibrosis, can cause anemia by affecting blood production in your bone marrow. The effects of these types of cancer and cancer-like disorders vary from mild to life-threatening.
- Hemolytic anemias
This group of anemias develops when red blood cells are destroyed faster than bone marrow can replace them. Certain blood diseases increase red blood cell destruction. You can inherit a hemolytic anemia, or you can develop it later in life.
- Sickle cell anemia
This inherited and sometimes serious condition is an inherited hemolytic anemia. It’s caused by a defective form of hemoglobin that forces red blood cells to assume an abnormal crescent (sickle) shape. These irregular blood cells die prematurely, resulting in a chronic shortage of red blood cells.
- Other anemias
There are several other forms of anemia, such as thalassemia and malarial anemia.
There are many other conditions that can, for various reasons, result in some level of anemia, such as:
- Bleeding—significant bleeding resulting from, for example, trauma or surgery (acute) or from gastrointestinal bleeding (ulcers) occurring over time (chronic)
- Leukemia (acute or chronic)
- Lymphoma
- Myelodysplastic syndrome
- Multiple myeloma
- Myeloproliferative neoplasms (e.g., myelofibrosis)
- Infections (e.g., HIV)
Anemia prevention
Eat a vitamin-rich diet
Many types of anemia can’t be prevented. But iron deficiency anemia and vitamin deficiency anemias can be avoided by having a diet that includes a variety of vitamins and nutrients, including:
- Iron. Iron-rich foods include beef and other meats, beans, lentils, iron-fortified cereals, dark green leafy vegetables, and dried fruit.
- Folate. This nutrient, and its synthetic form folic acid, can be found in fruits and fruit juices, dark green leafy vegetables, green peas, kidney beans, peanuts, and enriched grain products, such as bread, cereal, pasta and rice.
- Vitamin B-12. Foods rich in vitamin B-12 include meat, dairy products, and fortified cereal and soy products.
- Vitamin C. Foods rich in vitamin C include citrus fruits and juices, peppers, broccoli, tomatoes, melons and strawberries. These items help increase iron absorption.
Consider a multivitamin
If you’re concerned about getting enough vitamins from the food you eat, ask your doctor whether a multivitamin may be right for you.
Consider genetic counseling
If you have a family history of an inherited anemia, such as sickle cell anemia or thalassemia, talk to your doctor and possibly a genetic counselor about your risk and what risks you may pass on to your children.
Prevent malaria
Anemia can be a complication of malaria. If you plan on traveling to a place where malaria is common, talk with your doctor beforehand about taking preventive drugs. In areas where malaria is common, prevention involves reducing exposure to mosquitoes, for example, by using bed nets treated with insecticide.
Risk factors for developing anemia
These factors place you at increased risk of anemia:
- A diet lacking in certain vitamins. Having a diet that is consistently low in iron, vitamin B-12 and folate increases your risk of anemia.
- Intestinal disorders. Having an intestinal disorder that affects the absorption of nutrients in your small intestine — such as Crohn’s disease and celiac disease — puts you at risk of anemia.
- Menstruation. In general, women who haven’t experienced menopause have a greater risk of iron deficiency anemia than do men and postmenopausal women. That’s because menstruation causes the loss of red blood cells.
- Pregnancy. If you’re pregnant and aren’t taking a multivitamin with folic acid, you’re at an increased risk of anemia.
- Chronic conditions. If you have cancer, kidney failure or another chronic condition, you may be at risk of anemia of chronic disease. These conditions can lead to a shortage of red blood cells. Slow, chronic blood loss from an ulcer or other source within your body can deplete your body’s store of iron, leading to iron deficiency anemia.
- Family history. If your family has a history of an inherited anemia, such as sickle cell anemia, you also may be at increased risk of the condition.
- Other factors. A history of certain infections, blood diseases and autoimmune disorders, alcoholism, exposure to toxic chemicals, and the use of some medications can affect red blood cell production and lead to anemia.
- Age. People over age 65 are at increased risk of anemia.
Anemia complications
Left untreated, anemia can cause many health problems, such as:
- Severe fatigue. When anemia is severe enough, you may be so tired that you can’t complete everyday tasks.
- Pregnancy complications. Pregnant women with folate deficiency anemia may be more likely to experience complications, such as premature birth.
- Heart problems. Anemia can lead to a rapid or irregular heartbeat (arrhythmia). When you’re anemic your heart must pump more blood to compensate for the lack of oxygen in the blood. This can lead to an enlarged heart or heart failure.
- Death. Some inherited anemias, such as sickle cell anemia, can be serious and lead to life-threatening complications. Losing a lot of blood quickly results in acute, severe anemia and can be fatal.
Anemia diagnosis
To diagnose anemia, your doctor may ask you about your medical and family history, perform a physical exam, and run the following tests:
Tests
Several routine laboratory tests may be used to help diagnose anemia as well as help to determine the underlying cause. These are listed below. Depending on the results of these, the medical history of the person, and signs and symptoms, other tests may be done as follow up to help diagnose the cause of anemia and to help guide treatment.
Complete Blood Count (CBC)
Anemia may first be detected when a routine test that counts the number and relative proportion of each of the different types of cells in the blood stream, called a complete blood count (CBC), is done during a health exam or as part of testing for other conditions. A CBC is often ordered as part of a yearly physical exam and helps to evaluate overall health and to screen for a wide variety of disorders.
With anemia, some of the components of the CBC that may show abnormal results include:
- RBC count—typically low
- Hemoglobin—low
- Hematocrit—low
- RBC indices—these include mean corpuscular volume (MCV), mean corpuscular hemoglobin (MCH), and mean corpuscular hemoglobin concentration (MCHC). They give a healthcare practitioner information about the size of the red blood cells and the amount and concentration of hemoglobin in RBCs present in someone’s blood at that moment. For example, the size and hemoglobin concentration of RBCs can help with diagnosing anemia because those characteristics can vary for different kinds of anemia.
Blood Smear and Differential
If results of the complete blood count (CBC) indicate anemia, it may be followed up with an examination of a blood smear or a differential, which counts white blood cells. The smear review can provide additional information, such as the shape of red blood cells and the presence of abnormal cells, which can help diagnose and classify anemia.
Reticulocyte Count
This test provides information on the number of relatively immature red blood cells in a person’s blood sample. When someone has anemia (low RBC count, hemoglobin, and hematocrit), the results of this test can help determine the cause and/or help classify the type of anemia. For example, for a person with anemia, an inappropriately low reticulocyte count often indicates decrease in red blood cell production in the bone marrow.
Results from these tests may give clues as to the cause. Several other tests may be run to help determine the cause of the anemia and to guide treatment. See the individual discussions of the different types of anemia for more on these.
Additional diagnostic tests
If you receive a diagnosis of anemia, your doctor may order additional tests to determine the underlying cause. For example, iron deficiency anemia can result from chronic bleeding of ulcers, benign polyps in the colon, colon cancer, tumors or kidney problems.
Occasionally, it may be necessary to study a sample of your bone marrow to diagnose anemia.
Anemia treatment
Anemia treatment depends on the cause.
- Iron deficiency anemia. Treatment for this form of anemia usually involves taking iron supplements and making changes to your diet. If the underlying cause of iron deficiency is loss of blood — other than from menstruation — the source of the bleeding must be located and stopped. This may involve surgery.
- Vitamin deficiency anemias. Treatment for folic acid and B-12 deficiency involves dietary supplements and increasing these nutrients in your diet. If your digestive system has trouble absorbing vitamin B-12 from the food you eat, you may need vitamin B-12 shots. At first, you may receive the shots every other day. Eventually, you’ll need shots just once a month, which may continue for life, depending on your situation.
- Anemia of chronic disease. There’s no specific treatment for this type of anemia. Doctors focus on treating the underlying disease. If symptoms become severe, a blood transfusion or injections of synthetic erythropoietin, a hormone normally produced by your kidneys, may help stimulate red blood cell production and ease fatigue.
- Aplastic anemia. Treatment for this anemia may include blood transfusions to boost levels of red blood cells. You may need a bone marrow transplant if your bone marrow is diseased and can’t make healthy blood cells.
- Anemias associated with bone marrow disease. Treatment of these various diseases can include medication, chemotherapy or bone marrow transplantation.
- Hemolytic anemias. Managing hemolytic anemias includes avoiding suspect medications, treating related infections and taking drugs that suppress your immune system, which may be attacking your red blood cells. Depending on the severity of your anemia, a blood transfusion or plasmapheresis may be necessary. Plasmapheresis is a type of blood-filtering procedure. In certain cases, removal of the spleen can be helpful.
- Sickle cell anemia. Treatment for this anemia may include the administration of oxygen, pain-relieving drugs, and oral and intravenous fluids to reduce pain and prevent complications. Doctors also may recommend blood transfusions, folic acid supplements and antibiotics. A bone marrow transplant may be an effective treatment in some circumstances. A cancer drug called hydroxyurea (Droxia, Hydrea) also is used to treat sickle cell anemia.
- Thalassemia. This anemia may be treated with blood transfusions, folic acid supplements, medication, removal of the spleen (splenectomy), or a blood and bone marrow stem cell transplant.
Iron-deficiency anemia
Iron deficiency anemia is a common type of anemia and it has many causes. Symptoms are related to the overall decrease in the number of red blood cells (RBCs) and the level of hemoglobin. If the iron deficiency anemia is mild to moderate, there may be no signs or symptoms. In addition to the most common signs and symptoms, there are some that are more unique to iron deficiency and may appear as iron stores in the body are chronically depleted. These may include:
- Brittle or spoon-shaped nails
- Swollen or sore tongue
- Cracks or ulcers at the corners of the mouth
- Difficulty in swallowing
- Craving to eat unusual non-food substances such as ice or dirt (also known as “pica”)
Iron is an essential trace element and is necessary for the production of healthy RBCs. It is one component of heme, a part of hemoglobin, which is the protein in RBCs that binds to oxygen and allows RBCs to transport oxygen throughout the body. If not enough iron is taken in compared to what the body needs, then iron stored in the body begins to be used up. As iron stores are depleted, the body makes fewer RBCs with decreased amounts of hemoglobin in them, resulting in anemia.
Iron deficiency anemia causes
Some of the causes of iron deficiency include:
- Chronic bleeding—if bleeding is excessive over a period of the time (chronic), the body’s stored iron is gradually depleted and, as a result, the body cannot produce enough hemoglobin and red blood cells. In women, iron deficiency may be due to heavy menstrual periods or bleeding fibroids. In older women and in men, the bleeding is usually from disease of the intestines such as ulcers and cancer.
- Dietary deficiency—iron deficiency may be due to a diet poor in iron. Meat, poultry, fish, and iron-fortified foods or dark leafy greens and certain beans are good sources of iron. Children and pregnant or nursing women especially need more iron due to increased requirements. In pregnant women, lack of iron can lead to low birth weight babies and premature delivery. Women who are pregnant or planning to become pregnant routinely take iron supplements to prevent these complications. Newborns who are nursing from deficient mothers tend to have iron deficiency anemia as well.
- Absorption problem—certain conditions affect the absorption of iron from food in the gastrointestinal (GI) tract and over time can result in anemia. These include celiac disease, Crohn disease, intestinal surgery such as gastric bypass, and reduced stomach acid from taking prescription medications.
Iron-deficiency anemia laboratory tests
Initial blood tests typically include a complete blood count (CBC). Results may show:
- Hemoglobin (Hb)—may be normal early in the disease but will decrease as anemia worsens
- Red blood cell indices—early on, the RBCs may be a normal size and color (normocytic, normochromic) but as the anemia progresses, the RBCs become smaller (microcytic) and paler (hypochromic) than normal.
- Average size of RBCs (mean corpuscular volume, MCV)—decreased
- Average amount of hemoglobin in RBCs (mean corpuscular hemoglobin, MCH)—decreased
- Hemoglobin concentration (mean corpuscular hemoglobin concentration, MCHC)—decreased
- Increased variation in the size of RBCs (red cell distribution width, RDW)
A blood smear may reveal RBCs that are smaller and paler than normal as well as RBCs that vary in size (anisocytosis) and shape (poikilocytosis).
If a healthcare provider suspects that someone’s anemia is due to iron deficiency, several follow-up tests may be run to confirm the iron deficiency. These may include:
- Serum iron—the level of iron in someone’s blood, which is usually decreased
- Ferritin—a protein used to store iron; the small quantity of ferritin that is released into the blood is a reflection of the amount of stored iron in the body and is usually low with iron deficiency anemia. It is considered to be the most specific test for identifying iron deficiency anemia, unless infection or inflammation are present.
- Transferrin and total iron-binding capacity (TIBC)—transferrin is a protein that binds to and carries iron through the blood; TIBC is a reflection of how much transferrin is available to bind to iron. In iron deficiency anemia, the transferrin level and TIBC are high.
- Reticulocyte count—reticulocytes are young, immature red blood cells; the number of reticulocytes in iron deficiency anemia is low because there is insufficient iron to produce new RBCs.
- Soluble transferrin receptor (sTfR)—this test is primarily ordered to help distinguish between anemia that is caused by iron deficiency and anemia that is caused by inflammation or a chronic illness. It may be ordered as an alternative to ferritin when a person has a chronic illness and/or inflammation is present or suspected. It will be high in iron deficiency.
If the iron deficiency is thought to be due to chronic blood loss, such as GI (gastrointestinal) tract bleeding, then other tests and procedures may be performed. Laboratory tests that may be able to detect GI (gastrointestinal) bleeding are the fecal occult blood test (FOBT) or fecal immunochemical test (FIT).
A test for Helicobacter pylori may detect a bacterium that can cause ulcers in the GI tract that may be a cause of chronic bleeding. If any of these tests are positive or if it is strongly suspected that a GI bleed exists, then procedures such as endoscopy or colonoscopy may be done to find the location of the bleeding so that it can be treated.
Iron-deficiency anemia treatment
Treatment of iron deficiency typically involves iron supplements and/or a change in diet. Vitamin C also helps with iron absorption. However, if iron-deficiency is suspected to result from abnormal blood loss, further testing is often required to determine the reason for the bleeding. People with severe iron deficiency may require a transfusion of blood cells or iron therapy through intravenous (IV) or injections. When the underlying cause is found and treated, then the anemia usually resolves.
Pernicious Anemia
Pernicious anemia is a condition in which the body doesn’t absorb enough vitamin B12 to make enough red blood cells (RBCs). This happens when the body doesn’t make enough of a substance called “intrinsic factor.” Intrinsic factor is a protein produced by cells in the stomach lining that bind to vitamin B12 and allow it to be absorbed in the small intestine. Without enough intrinsic factor, the body cannot absorb vitamin B12 from the diet and cannot produce enough normal RBCs, which leads to anemia. In addition to lack of intrinsic factor, other causes of vitamin B12 deficiency and anemia include dietary deficiency and conditions that affect absorption of the vitamin from the small intestine such as surgery, certain drugs, digestive disorders (celiac disease, Crohn disease), and infections. Of these, pernicious anemia is the most common cause of B12 deficiency.
Vitamin B12 deficiency signs and symptoms
Vitamin B12 deficiency can result in general symptoms of anemia as well as nerve problems. These may include:
- Numbness and tingling that start first in the hands and feet (from nerve damage)
- Muscle weakness
- Slow reflexes
- Loss of balance
- Unsteady walking
- Confusion, memory loss, depression, and/or dementia in severe cases
Folic acid is another B vitamin, and deficiency in this vitamin may also lead to anemia. Folic acid, also known as folate, is found in many foods, especially in green, leafy vegetables. Folic acid is added to most grain products in the United States so that deficiency in folic acid is rarely seen in the U.S. nowadays. Folic acid is needed during pregnancy for normal development of the brain and spinal cord. It is important for women considering pregnancy to take appropriate amounts of folate supplements before they get pregnant and during pregnancy to make sure that they are not folate-deficient.
Anemia resulting from vitamin B12 or folate deficiency are often referred to as “megaloblastic anemia” because red blood cells are larger than normal. A lack of these vitamins does not allow RBCs to develop normally, which leads to their large size. This results in a reduced number of abnormally large RBCs and anemia.
Vitamin B12 deficiency laboratory tests
Symptoms of anemia will usually be investigated initially with a complete blood count (CBC) and differential. In pernicious anemia, other causes of vitamin B12 deficiency, or folate deficiency, these usually reveal:
- A low hemoglobin level
- Red cell indices—the mean corpuscular volume (MCV), which is the average size of RBCs, is high. Mean corpuscular hemoglobin (MCH) is also high, but mean corpuscular hemoglobin concentration (MCHC) is typically normal.
- A blood smear will reveal RBCs that are abnormally large and oval-shaped.
- The numbers of neutrophils (a type of white blood cell) and platelets may also be decreased.
Defects in nuclear maturation, as seen in megaloblastic anemias due to folate or B12 deficiency, result in large oval erythrocytes (macroovalocytes) with a normal hemoglobin content. The MCV and MCH are increased, while the MCHC remains normal. There is anisocytosis, and RDW is often increased. In the macrocytosis of liver disease, where there is no defect in nuclear maturation, the cells are large due to an excess red cell membrane. These cells are round, rather than oval, and the RDW is normal.
Additional tests are usually done to make the diagnosis. Some of these include:
- Vitamin B12 level—blood level may be low when deficient in B12
- Folic acid level—blood level may be low if deficient in this B vitamin
- Methylmalonic acid (MMA)—may be high with vitamin B12 deficiency
- Homocysteine—may be high with either folate or vitamin B deficiency
- Reticulocyte count—the number of young RBCs, or reticulocytes, is low
- Antibodies against intrinsic factor and/or parietal cell—may be present in pernicious anemia
Sometimes a bone marrow aspiration or biopsy may be performed to see if the marrow appearance is consistent with megaloblastic anemia and to rule out other bone marrow disorders that may also cause anemia with larger RBCs.
Vitamin B12 deficiency treatment
Treatment in these conditions involves supplementation with the vitamin that is deficient. If the cause of deficiency is the inability to absorb vitamin B12 from the digestive tract, then the vitamin may be given as injections. Treatment of underlying causes such as a digestive disorder or infection may help to resolve the anemia.
Aplastic anemia
Aplastic anemia is a rare disease caused by a decrease in the number of all types of blood cells that bone marrow produces. Normally, the bone marrow produces a sufficient number of new red blood cells (RBCs), white blood cells (WBCs), and platelets for normal body function. Each type of cell enters the blood, circulates, and then dies within a certain time frame. For example, the normal lifespan of RBCs is about 120 days. If the bone marrow is not able to produce enough blood cells to replace those that die, a number of symptoms, including those due to anemia, may result. This form of anemia can be severe or even fatal.
Aplastic anemia signs and symptoms
Symptoms of aplastic anemia can appear abruptly or can develop more slowly. Some general symptoms that are common to different types of anemia may appear first and are due to the decrease in number of RBCs.
Some additional signs and symptoms that occur with aplastic anemia include those due to decreased platelets:
- Prolonged bleeding
- Frequent nosebleeds and bleeding gums
- Easy bruising
- Pinpoint red spots on skin
- Blood in the stool
- Heavy menstrual bleeding
There may also be signs and symptoms due to a low WBC count:
- Increased frequency and severity of infections
- Fever
Aplastic anemia causes
Causes of aplastic anemia usually have to do with damage to the stem cells in the bone marrow that are responsible for blood cell production. Some factors that may be involved with bone marrow damage and that can lead to aplastic anemia include:
- Exposure to toxic substances like arsenic, benzene (found in gasoline), or pesticides
- Cancer therapy (radiation or chemotherapy)
- Autoimmune disorders such as lupus or rheumatoid arthritis
- Viral infections such as hepatitis, HIV, EBV, or CMV
- Medicines such as chloramphenicol (an antibiotic rarely used in the U.S.)
Rarely, aplastic anemia is due to an inherited (genetic) disorder such as Fanconi anemia. Other genetic disorders leading to aplastic anemia include Shwachman-Diamond syndrome and dyskeratosis congenita.
Aplastic anemia laboratory tests
The initial test for anemia, the complete blood count (CBC), may reveal many abnormal results.
- Hemoglobin and/or hematocrit may be low.
- RBC and WBC counts are low.
- Platelet count is low.
- Red blood cell indices are usually normal.
- The differential white blood count shows a decrease in most types of cells but not lymphocytes.
Some additional tests that may be performed to help determine the type and cause of anemia include:
- Reticulocyte count—result is low
- Erythropoietin—usually increased in aplastic anemia
- Bone marrow aspiration or biopsy will show a decrease in the number of all types of cells.
- Tests for infections such as hepatitis, HIV, EBV, CMV help to determine the cause.
- Tests for arsenic (a heavy metal) and other toxins
- Iron tests or tests for vitamin B12 may be done to rule out other causes.
- ANA—to determine if the cause is autoimmune disease
Aplastic anemia treatment
A physical examination or complete medical history may reveal possible causes for aplastic anemia, such as exposure to toxins or certain drugs (e.g., chloramphenicol) or prior treatment for cancer. Some cases of aplastic anemia are temporary while others have lasting damage to the bone marrow. Therefore, the treatment depends on the cause. Reducing or eliminating exposure to certain toxins or drugs may help resolve the condition. Medications may be given to stimulate bone marrow production, to treat infections, or to suppress the immune system in cases of autoimmune disorders. Blood transfusions and a bone marrow transplant may be needed in severe cases.
Hemolytic Anemia
Rarely, anemia is due to problems that cause the red blood cells (RBCs) to die or be destroyed prematurely. Normally, RBCs live in the blood for about four months. In hemolytic anemia, this time is shortened, sometimes to only a few days. The bone marrow is not able to produce new RBCs quickly enough to replace those that have been destroyed, leading to a decreased number of RBCs in the blood, which in turn leads to a diminished capacity to supply oxygen to tissues throughout the body. This results in the typical symptoms of anemia.
Depending on the cause, hemolytic anemia can be chronic, developing and lasting over a long period or lifetime, or may be acute. The various forms can have a wide range of signs and symptoms. See the discussions of the various types below for more on this.
The different causes of hemolytic anemia fall into two main categories:
- Inherited forms in which a gene or genes are passed from one generation to the next that result in abnormal RBCs or hemoglobin
- Acquired forms in which some factor results in the early destruction of RBCs
Inherited Hemolytic Anemia
Two of the most common causes of inherited hemolytic anemia are sickle cell anemia and thalassemia:
- Sickle cell anemia is a disorder where the body makes abnormal hemoglobin, which in turn causes red blood cells to become crescent-shaped, sickle cells under certain conditions. The “trait” (when you carry one mutated gene from one of your parents) can cause minor difficulties; the “disease” (when you carry two mutated genes, one from each of your parents) causes severe clinical problems. Misshapen blood cells are unstable (leading to hemolysis) and can block blood vessels, causing pain and anemia. Newborns are usually screened for sickle cell anemia, particularly those of African descent, because they are more likely to possess the inherited trait. Sometimes screening is done prenatally on a sample of amniotic fluid. Follow-up tests for hemoglobin variants may be performed to confirm a diagnosis. Treatment is usually based on the type, frequency, and severity of symptoms.
- Thalassemia is an inherited blood disorder where there is an imbalance in hemoglobin globin chain production that results in anemia and smaller red blood cells. Only in its most severe form do the RBCs break apart (hemolysis) and have a shortened life span. This “beta major” form (also called Cooley’s anemia) may result in growth problems, jaundice, and severe anemia. In milder forms, there is no significant hemolysis. This “beta minor” form (sometimes called beta thal trait) causes a mild anemia and no obvious symptoms.
Other less common types of inherited forms of hemolytic anemia include:
- Hereditary spherocytosis—results in abnormally shaped RBCs (so called spherocytes) that may be seen on a blood smear. These cells are very rigid, cannot pass through the spleen as normal red cells would, and thus get destroyed prematurely.
- Hereditary elliptocytosis—another cause of abnormally oval-shaped RBCs seen on a blood smear.
- Glucose-6-phospate dehydrogenase (G6PD) deficiency—G6PD is an enzyme that is necessary for RBC survival and, if deficient, RBCs come into contact with certain substances in the blood, the cells rupture and get destroyed. Those substances could include naphthalene, antimalarial medications, or fava beans. G6PD deficiency may be diagnosed with a test for its activity.
- Pyruvate kinase deficiency—pyruvate kinase is another enzyme important for RBC survival and its deficiency causes significant anemia. It is a rare disease that may be diagnosed with a test for the enzyme activity.
Inherited Hemolytic Anemia laboratory tests
Since some of these inherited forms may have mild symptoms, they may first be detected on a routine complete blood count (CBC) and blood smear, which can reveal various abnormal results that give clues as to the cause. Follow-up tests are then usually performed to make a diagnosis. Some of these include:
- Hemoglobinopathy evaluation
- DNA analysis—not routinely done but can be used to help diagnose hemoglobin variants, thalassemia, and to determine carrier status
- G6PD test—to detect deficiency in this enzyme
- Osmotic fragility test—detects RBCs that are more fragile than normal, which may be found in hereditary spherocytosis
These genetic disorders cannot be cured, but often the symptoms resulting from the anemia may be alleviated with treatment as necessary.
Acquired Hemolytic Anemia
Some of the conditions or factors involved in acquired forms of hemolytic anemia include:
- Autoimmune disorders—conditions in which the body produces antibodies against its own red blood cells; it is not well understood why this may happen, but it accounts for about half of all cases of hemolytic anemia. Certain diseases such as lupus, HIV and hepatitis can increase a person’s risk for it.
- Transfusion reaction—result of blood donor-recipient incompatibility; this occurs very rarely, but when it does, it can have some serious complications.
- Infections, such as malaria and infectious mononucleosis (mono)
- Mother-baby blood group incompatibility—may result in hemolytic disease of the newborn
- Medications—certain medications such as penicillin can trigger the body to produce antibodies directed against RBCs or cause the direct destruction of RBCs.
- Physical destruction of RBCs by, for example, an artificial heart valve or cardiac bypass machine used during open-heart surgery
- Paroxysmal Nocturnal Hemoglobinuria (PNH)—a rare condition in which the different types of blood cells including RBCs, white blood cells, and platelets are abnormal due to lack of certain surface proteins; because the RBCs are defective, the body destroys them earlier than the normal lifespan. This disease occurs due to a change or mutation in a gene called PIGA in the stem cells that make blood. Though it is a genetic disorder, it is not passed from one generation to the next (it is not an inherited condition). Those affected will often pass dark urine due to the hemoglobin released by destroyed RBCs being cleared from the body by the kidneys. This is most noticeable first thing in the morning when urine is most concentrated.
Acquired Hemolytic Anemia laboratory tests
Hemolytic anemias are often first identified by signs and symptoms, during physical examination, and by medical history. A medical history can reveal, for example, a recent transfusion, treatment with penicillin, or cardiac surgery. A CBC and/or blood smear may show various abnormal results. Depending on those findings, additional follow-up tests may be performed. Some of these may include:
- Tests for autoantibodies for suspected autoimmune disorders
- Direct antiglobulin test (DAT) in the case of transfusion reaction, mother-baby blood type incompatibility, or autoimmune hemolytic anemia
- Haptoglobin—usually low
- Reticulocyte count—typically high
- Flow cytometry for suspected PNH
Hemolytic anemia treatment
Treatments for hemolytic anemia are as varied as the causes. However, the goals are the same: to treat the underlying cause of the anemia, to decrease or stop the destruction of RBCs, and to increase the RBC count and/or hemoglobin level to alleviate symptoms. This may involve, for example:
- Drugs used to suppress production of autoantibodies that destroy RBCs
- Blood transfusions to increase the number of healthy RBCs
- Bone marrow transplant—to increase production of normal RBCs
- Avoiding triggers that cause the anemia such as the cold in some forms of autoimmune hemolytic anemia or fava beans, naphthalene and certain medicines for those with G6PD deficiency.
Anemia Caused by Chronic Diseases
Some chronic (long-term) illnesses can cause anemia. Often, anemia caused by chronic diseases goes undetected until a routine test such as a complete blood count (CBC) reveals abnormal results. Several follow-up tests may be used to determine the underlying cause. There are many chronic conditions and diseases that can result in anemia. Some examples of these include:
- Kidney disease—red blood cells are produced by the bone marrow in response to a hormone called erythropoietin, made primarily by the kidneys. Chronic kidney disease can cause anemia resulting from too little production of this hormone; the anemia can be treated by giving erythropoietin injections.
- Anemia of chronic disease—whenever there are chronic diseases that stimulate the body’s inflammatory response, the ability of the bone marrow to respond to erythropoietin is decreased, mainly due to impairment in body iron regulation. For example, rheumatoid arthritis (a severe form of joint disease caused by the body attacking its own joints, called an autoimmune disease) can cause anemia by this mechanism. Other diseases that can produce anemia in the same way include chronic infections such as HIV or tuberculosis (TB).
Anemia of chronic disease laboratory tests
A number of tests may be used as follow up to abnormal results of initial tests such as a CBC and blood smear to determine the underlying cause of chronic anemia. Some of these may include:
- Reticulocyte count—will typically be low
- Comprehensive metabolic panel—used to detect evidence of chronic disorders
Tests for anemia of chronic disease may include:
- Tests for inflammation such as CRP
- Erythropoietin (EPO) —is typically mildly increased
- Tests for infections such as HIV and TB
- Iron and transferrin (TIBC)—are typically both low
- Soluble transferrin receptor (sTfR)—is typically normal or low
Anemia of chronic disease treatment
Treatment of anemia due to chronic conditions usually involves determining and/or resolving the underlying disease. Blood transfusions may be used to treat the condition in the short term.





{kind=link}