
Contents
What is MCT oil
MCT oil is short for medium chain triglyceride oil or medium-chain triacylglycerol. MCT oil contained octanoate and decanoate only (100% saturated medium-chain fatty acids) 1). Clinical studies have shown that consumption of medium-chain triacylglycerols (MCTs) leads to greater energy expenditure than does consumption of long-chain triacylglycerols (LCTs) 2), 3), 4), 5), 6). Such studies suggest that MCT oil consumption may be useful for weight management. MCT oil based diet has also been shown to reverse hypertrophic cardiomyopathy in a patient with very long chain acyl-coA dehydrogenase deficiency 7). Very long chain acyl-CoA dehydrogenase (VLCAD) deficiency is one of the genetic defects of mitochondrial fatty acid beta-oxidation presenting in early infancy or childhood. If undiagnosed and untreated, very long chain acyl-coA dehydrogenase deficiency deficiency may be fatal, secondary to cardiac involvement 8). Treatment is essentially dietary modification, with avoidance of long-chain fatty acids and supplementation with medium chain triglycerides, so that the enzyme-deficient step can be bypassed 9).
Dietary fat is the most important source of energy of all the nutrients, supplying 9 kcal/g, about double that contributed by either protein or carbohydrate at 4 kcal/g 10). Fatty acids, stored as triglycerides (also called triacylglycerols) in the body, are an important reservoir of stored energy. Fatty acids are composed of two major types: saturated and unsaturated fatty acids, and the presence or absence of carbon-carbon double bonds in the hydrocarbon chain is the only difference between them. Saturated fatty acids do not have double bonds in the hydrocarbon chain and unsaturated fatty acids contain at least one double bond. The unsaturated fatty acids are often divided into two subgroups: monounsaturated fatty acids with a single double bond and polyunsaturated fatty acids with two or more double bonds. The basic formulae of saturated and monounsaturated species are CH3(CH2)nCOOH and CH3(CH2)nCH=CH(CH2)nCOOH, respectively. In addition, based on chain length, they are often categorized as short-chain, medium-chain, or long-chain fatty acids. Short-chain fatty acids have aliphatic tails of fewer than eight carbons (<C8). Fatty acids with aliphatic tails of 8–12 carbons (C8-C12) are classified as medium-chain fatty acids, and long-chain fatty acids have aliphatic tails longer than 12 carbons (>C12). Sometimes, fatty acids with aliphatic tails longer than 22 carbons (>C22) are defined as very-long-chain fatty acids 11).
The four major types of fats 12) are:
- Monounsaturated fats (Good)
- Polyunsaturated fats (Good)
- Saturated fats (Bad)
- Trans fats (Very Bad)
Monounsaturated and polyunsaturated fats are known as “healthy fats” because they are good for your heart, cholesterol levels, and overall health. Monounsaturated and polyunsaturated fats do not raise LDL “bad” cholesterol and are beneficial when consumed in moderation. These fats tend to be “liquid” at room temperature. Olive oil and canola oil are examples of a type of oil that contains monounsaturated fats.
Monounsaturated fats (MUFAs) can help reduce bad cholesterol levels in your blood which can lower your risk of heart disease and stroke 13). They also provide nutrients to help develop and maintain your body’s cells. Oils rich in monounsaturated fats also contribute vitamin E to the diet, an antioxidant vitamin most Americans need more of.
Polyunsaturated fats (PUFAs) are simply fat molecules that have more than one unsaturated carbon bond in the molecule, this is also called a double bond. Oils that contain polyunsaturated fats are typically liquid at room temperature but start to turn solid when chilled. Soybean oil and flax seed oil are examples of a type of oil that contains polyunsaturated fats. Polyunsaturated fats can help reduce bad cholesterol levels in your blood which can lower your risk of heart disease and stroke 14). They also provide nutrients to help develop and maintain your body’s cells. Oils rich in polyunsaturated fats also contribute vitamin E to the diet, an antioxidant vitamin most Americans need more of.
Oils rich in polyunsaturated fats also provide essential fats that your body needs but can’t produce itself – such as omega-6 and omega-3 fatty acids. You must get essential fats through food. Omega-6 and omega-3 fatty acids are important for many functions in the body.
For good health, the majority of the fats that you eat should be monounsaturated or polyunsaturated. Consider eating more of the beneficial polyunsaturated fats containing Omega-3 fatty acids found in fatty fish, flaxseed, chia seeds and walnuts 15). Eat foods containing monounsaturated fats and/or polyunsaturated fats instead of foods that contain saturated fats and/or trans fats.
The majority of saturated fat comes from animal products such as beef, lamb, pork, poultry with skin, butter, cream, cheese and other dairy products made from whole or 2 percent milk. All of these foods also contain dietary cholesterol. Foods from plants that contain saturated fat include coconut, coconut oil, palm oil and palm kernel oil (often called tropical oils) and cocoa butter. Replacing foods that are high in saturated fat with healthier monounsaturated and polyunsaturated fats (oils) can lower your blood cholesterol levels and improve your blood lipid profiles 16). The American Heart Association recommends you don’t eat more than 5% to 6% of calories from saturated fat 17). For example, if you need about 2,000 calories a day, no more than 120 of them should come from saturated fat. That’s about 13 grams of saturated fat per day.
Trans fats (or trans fatty acids) are created in an industrial process that adds hydrogen to liquid vegetable oils to make them more solid. Another name for trans fats is “partially hydrogenated oils.” Partially hydrogenated oils (trans fats) are used by food manufacturers to improve the texture, shelf life and flavor stability of foods. Partially hydrogenated oils should not be confused with “fully hydrogenated oils,” or saturated fats which are solid fats that contain very low levels of trans fat. Trans fats are found in many fried foods and baked goods such as pastries, pizza dough, pie crust, cookies and crackers. And trans fat are also formed naturally and is found in small amounts in some animal products, such as meats and dairy products 18).
Trans fats raise your bad (LDL) cholesterol levels and lower your good (HDL) cholesterol levels 19). These changes are associated with a higher risk of heart disease.
There are two sources of trans fat:
- Trans fat formed naturally – this type of trans fat is produced in the gut of some grazing animals (such as cattle and sheep).
- Trans fat formed artificially during food processing – this type of trans fat is created during a process called “partial hydrogenation” in which hydrogen is added to liquid vegetable oil to make it more solid, and therefore more resistant to becoming spoiled or rancid. The process generally does not make the oil completely solid, resulting in “partially” hydrogenated oils.
Since 2006, the U.S. Food and Drug Administration (FDA) has required trans fat content to be listed on the Nutrition Facts panel of packaged foods 20). In recent years, many major national fast-food chains and casual-dining restaurant chains have announced they will no longer use trans fats to fry or deep-fry foods. Many smaller local and regional restaurant chains have made similar announcements.
On June 16, 2015, the U.S. Food and Drug Administration (FDA) took action that will significantly reduce the use of partially hydrogenated oils, the major source of artificial trans fats in the food supply. The FDA announcement to eliminate trans fats from processed foods and their action is expected to reduce cardiovascular disease and prevent thousands of fatal heart attacks each year in the U.S. 21). According to the FDA, “On June 18, 2018, manufacturers must ensure that their products no longer contain partially hydrogenated oils (trans fats) for uses that have not been otherwise authorized by FDA.”
To find the amount of trans fats in a particular packaged food, look at the Nutrition Facts panel. Companies must list any measurable amount of trans fat (0.5 grams or more per serving) in a separate line in the “Total Fat” section of the panel, directly beneath the line for “Saturated Fat.” This means if a food package states 0 gram of trans fats, it might still have some trans fats if the amount per serving is less than 0.5 g. Make sure to check the ingredients list for “partially hydrogenated oil.”
Saturated fats are considered to be unhealthy and several health authorities recommend limiting their intake in the diet 22). These recommendations stem from studies linking higher intakes of saturated fat and heart disease 23). Replacing saturated fat with healthier fat could lower cardiovascular risks 24). However, saturated fats are quite heterogeneous in nature and potentially also in their health effects. In fact, based on their structure, saturated fats can be sub-classified into short chain, medium chain, and long chain fats whereas mono- and polyunsaturated fats are all long chain fats. Short chain fatty acids are considered to have 6 or fewer carbon atoms, medium chain fatty acids (MCFA) have 8–10 carbons, and long chain fatty acids (LCFA) generally have 12 or more carbon chains. In the US, the average consumption of medium chain fatty acids (MCFA) is approximately 2% of total fat intake 25).
Most studies comparing the effects of saturated fats to unsaturated fats have focused on fats that contained a large proportion of their fatty acids as long chain fatty acids (LCFA). Very few clinical studies have examined the impact of medium chain fatty acids (MCFA) on cardiovascular disease risk factors 26), 27). Some of those studies have found that medium chain fatty acids (MCFA) consumption increased total cholesterol and low-density lipoprotein cholesterol (LDL-C) to the same extent as palm oil 28) and led to higher levels of triglycerides (TG) than palm oil and sunflower oil 29), an other diet rich in long chain fatty acids (LCFA) 30), or soybean oil 31). Reductions in HDL-C “good” cholesterol 32) and absence of effects on total cholesterol, LDL-C “bad” cholesterol, and HDL-C “good” cholesterol have also been noted with medium chain fatty acids (MCFA) soybean oil consumption 33). Previous studies with medium chain triglyceride (MCT) oil showed reductions in total cholesterol and LDL-C “bad” cholesterol and no change in HDL-C “good” cholesterol or triglycerides 34), 35) but the MCT oil was fed along with plant sterols, which are known to reduce total cholesterol and “bad” cholesterol 36), 37) and safflower oil, an oil rich in n-3 polyunsaturated fats (omega 3 fatty acids). Hu et al. 38), however, have found that MCT oil did not increase the risk of coronary heart disease in the Nurses’ Health Study whereas consumption of long chain saturated fats did. Therefore, whether MCT oil truly has a negative impact on cardiovascular disease risk remains to be firmly established. This is particularly important since MCT oil has been taunted as a potential weight-lowering agent 39).
MCT oil weight loss
Dietary fat is often blamed for the rising prevalence of obesity 40). However, all fats are not equal in their metabolic effects. For example, MCT (medium-chain triacylglycerols), which typically contain fatty acids with chain lengths of ≤10 carbon atoms, are processed differently from long-chain triacylglycerols (LCTs) by the body 41). Because of their chain length, medium-chain fatty acids can be absorbed in the gastrointestinal tract and transported to the liver via the portal circulation without incorporation into chylomicrons. As a result, it is hypothesized that MCTs are oxidized to a greater extent than are long-chain triacylglycerols (LCTs) and have less opportunity for deposition into adipose tissue 42). These characteristics of MCTs have been well demonstrated in animal studies, in which rats were shown to have smaller adipose tissue mass if fed MCTs than if fed long-chain triacylglycerides (LCTs) 43), 44). Human studies have also long shown that MCTs increase fat oxidation and thermogenesis compared with LCTs in short-term feeding studies 45), 46), 47), 48). More recently, St Onge et al. showed in women 49) and in men 50) that this remains the case even over prolonged consumption periods of up to 4 weeks. Furthermore, St Onge et al. showed that when men consume a diet rich in MCTs, they lose more fat mass than when they consume an equicaloric diet rich in LCTs from olive oil 51).
As a result of data showing increased thermogenesis and lower fat deposition with MCT consumption, it has been hypothesized that MCT oil may be a useful adjunct to a weight-loss diet.
This very small randomized clinical study with 31 healthy overweight and obese subjects (body mass index: 29.8 ± 0.4, in kg/m2) 52) shows that long-term consumption of moderate amounts of saturated fats, in the form of MCT oil, does not have adverse effects on cardiovascular disease risk factors. In that small study, thirty-one men and women, age 19–50 y and body mass index 27–33 kg/m2, were randomized to a 16-week weight loss program 53). The weight loss program (EatRight program) is a 12-week program that teaches good nutrition habits and provides tips for better weight control and weight loss. Four lessons were added to the basic program to account for the longer duration of this weight-loss study. The sequence and topics for each counseling session are shown in Table 2. The subjects were provided EatRight materials weekly and discussed the weight-loss principles taught with the dietitian.
As part of the weight-loss program, the subjects were counseled to reduce their caloric intakes to 1500 kcal/d for women and 1800 kcal/d for men 54). Within this diet, all subjects received study muffins (either cranberry or blueberry; Krusteaz, Seattle, WA) that contained 10 g of their assigned oil and 8 or 14 g of liquid oil, for women and men, respectively, to incorporate into their foods during cooking. Therefore, all subjects received ≈12% of their prescribed weight-loss energy requirements in the form of the study oil (18 g for women and 24 g for men) in their foods during cooking. This level of oil was chosen because it was found to produce significant increases in energy expenditure 55), which is believed to be the main mechanism of action for weight loss with MCT oil.
The subjects, along with the dietitian and clinical coordinator, were unaware of the oil each person was consuming. Muffins were given to the clinical coordinator in bags labeled with the subject’s study ID code and A or B to designate group. Oil was provided in opaque plastic containers, which were also labeled with the subject’s study ID code and A or B. Neither the dietitian nor the clinical coordinator knew which oil was A and which one was B. The oils did not impart any particular taste to the study muffins. Also, because the subjects were instructed to consume the liquid oil in stir-frying and with foods, it is unlikely that they could identify which study oil they were being provided. Another point of note is that none of the subjects had previously tasted MCT oil and therefore had no point of reference to determine whether it tasted any different from olive oil.
Body weight and waist circumference were measured at each weekly session by the clinical coordinator.
MCT oil consumption resulted in lower endpoint body weight than did olive oil (−1.67 ± 0.67 kg) after the 16 week study [see Table 3] 56). This agrees with the study authors previous data 57) and hypothesis put forth previously concerning the potential for enhanced weight management with MCT consumption 58). Tsuji et al 59) found that overweight subjects consuming a diet containing ≈10 g MCT oil/d for 12 wk lost 1.34 kg more than did a group consuming 10 g of an LCT oil (rapeseed oil–soybean oil blend). Similar results were also obtained with subjects consuming 5 g of MCT or LCT oil/day 60). In that study, weight loss over a 12-week period was enhanced by 1.3 kg, which could extrapolate to 1.7 kg over a 16-week period. Weight-loss data from these 2 studies, extrapolated to 16 week, are similar to those obtained in the present study 61).
The 16 week weight loss study comparing MCT oil and olive oil combined with a weight loss program that includes reduced calories consumption and diet counseling, showed the inclusion of MCT oil in a weight-loss program leads to greater weight loss than does the inclusion of a similar amount of olive oil. The addition of an enhanced thermic effect of food and reduced food intake would result in a lower caloric retention of 107.5 kcal/d. This lower caloric retention, if maintained over a 16-wk period, would lead to an additional loss of 1.55 kg body wt with MCT consumption than with long-chain triacylglyceride (LCT). However, the study was not able to show differences in adipose tissue distribution between the different diets 62).
There was a trend toward greater loss of fat mass and trunk fat mass with MCT oil consumption than with olive oil. Endpoint trunk fat mass, total fat mass, and intraabdominal adipose tissue were all lower with MCT oil consumption than with olive oil consumption 63). The results also show that MCT oil consumption leads to comparable effects on cardiovascular disease risk factors as an equal amount of olive oil, an oil considered to have beneficial health effects 64).
Table 1. Fatty acid profile of MCT oil and Olive oil per 100 g of oil used in the weight loss study
| Fatty acid | MCT oil | Olive oil |
|---|---|---|
| C8:0 | 55.0 | 0 |
| C10:0 | 45.0 | 0 |
| C12:0 | 0 | 0 |
| C14:0 | 0 | 0 |
| C16:0 | 0 | 11.290 |
| C16:1 | 0 | 1.255 |
| C17:0 | 0 | 0.022 |
| C17:1 | 0 | 0.125 |
| C18:0 | 0 | 1.953 |
| C18:1 | 0 | 71.269 |
| C18:2 | 0 | 9.761 |
| C18:3 | 0 | 0.761 |
| C20:0 | 0 | 0.414 |
| C20:1 | 0 | 0.311 |
| C22:0 | 0 | 0.125 |
Table 2. EatRight weight-loss program study topics by week
| Lesson number | Topic |
|---|---|
| 1 | Study muffins and oil use; low-fat and fat-free ideas |
| 2 | ChooseRight |
| 3 | RecordRight |
| 4 | Healthy recipes |
| 5 | Goal setting |
| 6 | PlanRight |
| 7 | ShopRight (in class) |
| 8 | ShopRight (grocery store tour) |
| 9 | HeartSmart |
| 10 | CookRight |
| 11 | DineRight |
| 12 | Healthy fast food choices |
| 13 | ThinkRight |
| 14 | Stress management |
| 15 | StartRight |
| 16 | Sharing healthy recipes |
Figure 1. MCT oil versus Olive oil weight loss
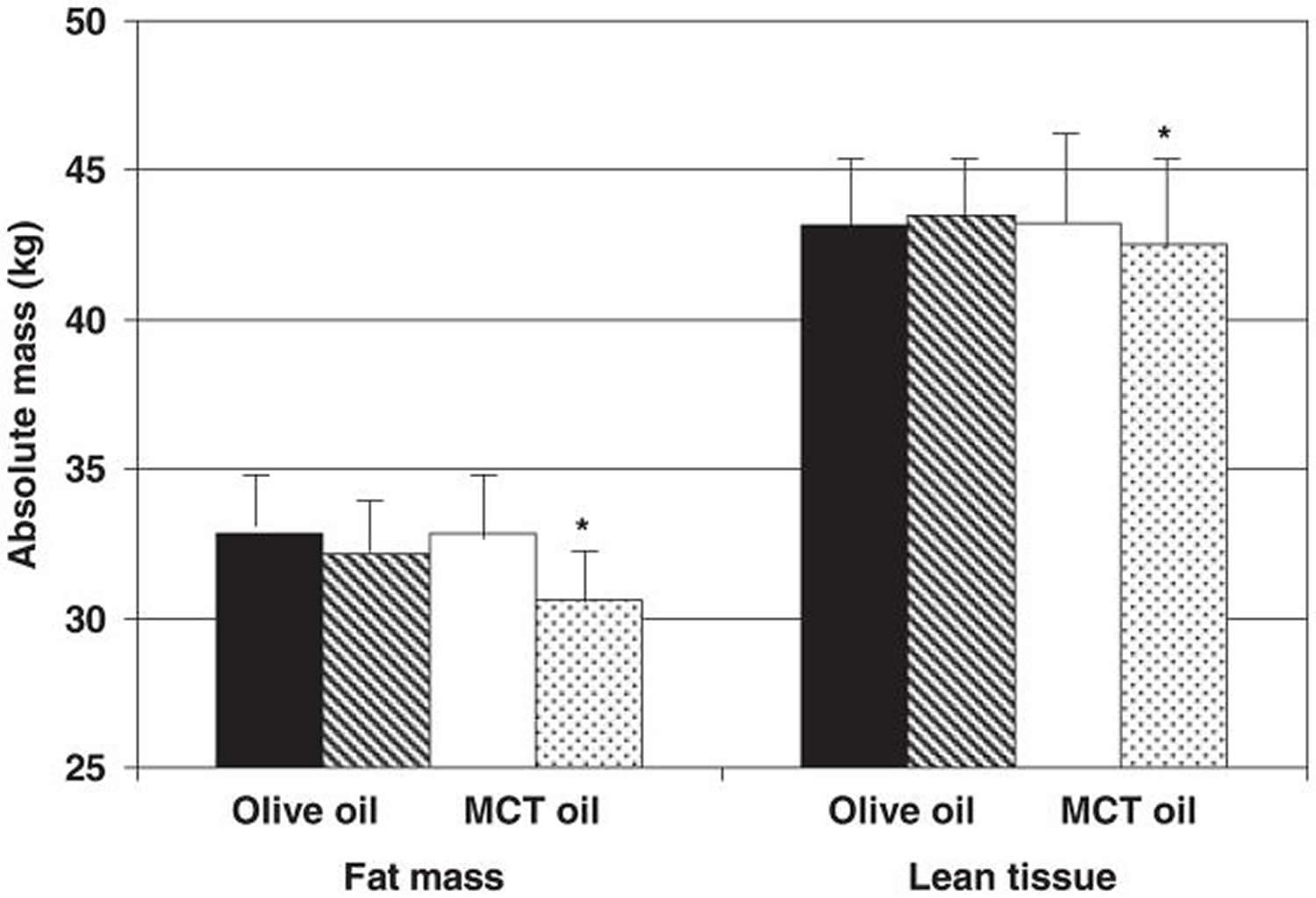
Footnotes: Mean absolute body composition, assessed by dual-energy X-ray absorptiometry, at baseline and at the endpoint of a 16-week weight-loss program that included either olive oil (baseline = black bars; endpoint = dark gray bars; n = 15) or medium-chain triacylglycerol (MCT) oil (baseline = white bars; endpoint = light gray bars; n = 16). There was a trend for a diet-by-week interaction on lean tissue. There was a trend for a diet-by-week interaction on absolute total fat mass and fat massand a trend for a diet effect on fat mass. There was a significant effect of week on fat mass (P = 0.0013).
[Source 67)]Table 3. Change in adipose tissue compartments, assessed by dual-energy X-ray absorptiometry and computed tomography, during consumption of either olive oil or medium-chain triacylglycerol (MCT) oil as part of a weight-loss diet for 16 week
| Change in body compartment | MCT oil (n = 16) | Olive oil (n = 15) |
|---|---|---|
| Total fat mass (%) | −1.46 ± 0.45 | −0.58 ± 0.46 |
| Total fat mass (kg) | −2.23 ± 0.57 | −0.69 ± 0.58 |
| Trunk fat mass (%) | −1.23 ± 0.73 | −0.49 ± 0.75 |
| Trunk fat mass (kg) | −1.20 ± 0.35 | −0.34 ± 0.36 |
| Intraabdominal adipose tissue (cm2) | −8.85 ± 3.92 | −1.32 ± 4.19 |
| Subcutaneous abdominal adipose tissue (cm2) | −24.76 ± 9.37 | −11.29 ± 10.02 |
Summary
The thought process behind MCT’s is that they are rapidly broken, go straight to the liver and may play a role in weight loss. They are also considered to not adversely affect blood cholesterol levels. Although MCT oil plus weight loss program study 69) cannot distinguish which side of the energy balance equation played a bigger role in weight loss (enhanced suppression of food intake or enhanced thermic effect of food), the data complement the body of literature concluding that MCT oil can be successfully used in a weight-management program to enhance weight loss. However, a recent study 70) looking at MCT oil in adolescents showed no increase in thermogenesis, or a decrease in appetite or satiety. More research is needed into the use of MCT oil as a tool in weight management in overweight and obesity. Furthermore, previous studies have shown that MCT oil can used as a special-purpose food as a supportive nutritional therapy in the management of childhood diarrhea 71). MCT oil may be also used to increase the calorie value, improve the palatability, digestibility, absorption and transport of a diet indicated for diseases with maldigestion/malabsorption 72), 73). The effect of MCT oil on malabsorption states is related to the circumstance that the molecularly small medium chain fatty acids are more easily hydrolyzed by pancreatic lipase and, therefore, more rapidly absorbed than conventional fats 74). In that study on children with dairrhea 75), MCT oil supplemented group was heavier (10.3 kg versus 8.9 kg), had greater proportion of weight gain, lesser proportion of weight loss (14.3% versus 55.6%) and with no weight change (14.3% vs. 22.2%) compared to the non-MCT supplemented group. There was a statistical significant difference in the rate of weight gain among subjects in the MCT group compared to subjects in the non-MCT group (0.22 + 0.22 kg/day vs. -.048 + .26 kg/day). In this childhood diarrhea study 76), MCT oil was administered equally throughout the day, incorporated into the milk formula or meals, with a dosage of 15 ml per day, which was on the average 46.8% of the total fat calorie. During the course of MCT oil administration, no significant clinical symptoms warranted the discontinuation of therapy. These MCT oil studies show that fats have a place in a weight-loss diet and that choosing MCT oil is interesting, especially in light of the effects of MCT oil consumption on energy balance and weight control – MCT oil may provide weight loss or even weight gain benefits wihout the adverse effects of saturated fats.
MCT oil side effects
Therapeutic use of MCT oil has been limited due to the occasional occurrence of mild gastrointestinal symptoms, including crampy abdominal pain, nausea and diarrhea. Reportedly, these symptoms can be ameliorated with cautious administration of MCT oil. The oil should be introduced in small amounts, given at room temperature, diluted with an equal volume of water or fruit juice, and taken slowly 77).
MCT oil vs Coconut oil
Coconut oil, extracted from the meat of what can loosely be called a seed, a fruit or a nut, is mostly saturated fat, about 82 percent 78). Coconut oil also has 6% monounsaturated fat (oleic acid) and 1.7% polyunsaturated fat (linoleic acid). One tablespoon adds up to more than 11 grams of saturated fats, according to the federal National Nutrient Database 79). That’s nearly the total daily limit of 13 grams recommended by the American Heart Association. Replacing saturated fat with healthier fat in the diet lowers cardiovascular disease risk as much as cholesterol-lowering statin drugs, according to an American Heart Association 2017 Presidential Advisory 80). When you look at biomarkers of cardiovascular disease such as serum lipid profiles, studies 81) show that coconut oil consistently raises cholesterol higher than monounsaturated (Oleic acid) and polyunsaturated oils (linoleic acid).
The MCT oil used in the MCT Oil Consumption as Part of a Weight Loss Diet study 82) was a special 100 percent medium-chain coconut oil. Most coconut oils typically have 13 percent to 14 percent of this medium-chain triglyceride, the study author said. So, people would have to eat large quantities to replicate the results. “No one eats 150 grams (10 tablespoons) of coconut oil in a day,” said the study author. Nor should they.
A lot of the benefits of coconut oil are attributed to coconut oil’s concentration of MCTs (capric and caprylic acid). However, only 13 to 15% of coconut oil is medium chain triglycerides (MCT’s). So, you would need to take a lot of coconut oil to match the amount used in studies on MCT’s.
The thought process behind MCT’s is that they are rapidly broken, go straight to the liver and may play a role in weight loss. They are also considered to not adversely affect blood cholesterol levels. However, a recent study 83) looking at MCT in adolescents showed no increase in thermogenesis, or a decrease in appetite or satiety. In another study 84) comparing virgin coconut oil to extra virgin olive oil, there was also no difference in metabolism or fat oxidation.
The cardiovascular health benefits of coconut oil are cited from the studies looking at indigenous populations from India, Sri Lanka, Philippines, Polynesia and Melanesia. However, most of these populations rely on coconuts and not coconut oil. The remainder of their diet tends to be higher in whole foods and lower in sugar and processed foods. It should be noted that coconuts are a high fiber food. One cup of coconut flesh has 7 grams of fiber. Eating coconuts are not linked to cardiovascular disease.
In the case of the Pukapukans and Tokelauans, their overall diet is very low in sugar and rich in high fiber foods. It consists mainly of coconuts, breadfruit, and fish. There is little, if any, consumption of coconut oil 85).
The Kitava studies examined the Melanesian people in Papua New Guinea. Their overall fat intake is only 21%. In addition, their diet is mostly whole coconuts, tubers, fish, and fruit. Their intake of oils, margarine, and sugar is very little. In other words, mostly whole-food, plant-based diet.
When looking at Samoans, their traditional diet also consists of coconuts along with seafood, low intake of processed foods. Of course, all that has changed now with the widely available processed food, refined sugars and red meat (beef, spam) 86).
The bottom line is that coconut oil increases LDL cholesterol, does not increase thermogenesis or weight loss. Based on all the current research we have so far, regular use of coconut oil should not be advised. As always, a whole foods diet consisting of mainly plants should be the foundation of a healthy eating pattern.
Table 4. Coconut oil nutrition facts
| Nutrient | Unit | Value per 100 g | Tablespoon 13.6 g | ||||||
| Approximates | |||||||||
| Water | g | 0.03 | 0 | ||||||
| Energy | kcal | 892 | 121 | ||||||
| Protein | g | 0 | 0 | ||||||
| Total lipid (fat) | g | 99.06 | 13.47 | ||||||
| Carbohydrate, by difference | g | 0 | 0 | ||||||
| Fiber, total dietary | g | 0 | 0 | ||||||
| Sugars, total | g | 0 | 0 | ||||||
| Minerals | |||||||||
| Calcium, Ca | mg | 1 | 0 | ||||||
| Iron, Fe | mg | 0.05 | 0.01 | ||||||
| Magnesium, Mg | mg | 0 | 0 | ||||||
| Phosphorus, P | mg | 0 | 0 | ||||||
| Potassium, K | mg | 0 | 0 | ||||||
| Sodium, Na | mg | 0 | 0 | ||||||
| Zinc, Zn | mg | 0.02 | 0 | ||||||
| Vitamins | |||||||||
| Vitamin C, total ascorbic acid | mg | 0 | 0 | ||||||
| Thiamin | mg | 0 | 0 | ||||||
| Riboflavin | mg | 0 | 0 | ||||||
| Niacin | mg | 0 | 0 | ||||||
| Vitamin B-6 | mg | 0 | 0 | ||||||
| Folate, DFE | µg | 0 | 0 | ||||||
| Vitamin B-12 | µg | 0 | 0 | ||||||
| Vitamin A, RAE | µg | 0 | 0 | ||||||
| Vitamin A, IU | IU | 0 | 0 | ||||||
| Vitamin E (alpha-tocopherol) | mg | 0.11 | 0.01 | ||||||
| Vitamin D (D2 + D3) | µg | 0 | 0 | ||||||
| Vitamin D | IU | 0 | 0 | ||||||
| Vitamin K (phylloquinone) | µg | 0.6 | 0.1 | ||||||
| Lipids | |||||||||
| Fatty acids, total saturated | g | 82.475 | 11.217 | ||||||
| Fatty acids, total monounsaturated | g | 6.332 | 0.861 | ||||||
| Fatty acids, total polyunsaturated | g | 1.702 | 0.231 | ||||||
| Fatty acids, total trans | g | 0.028 | 0.004 | ||||||
| Cholesterol | mg | 0 | 0 | ||||||
| Other | |||||||||
| Caffeine | mg | 0 | 0 | ||||||
What does MCT oil do
Although MCT oil are thought to lead to increases in triacylglyceride concentrations 88), this small study 89) did not observe this in their results. This finding confirms previous findings that MCT do not raise triacylglyceride concentrations when consumed at levels 12–20% of energy intakes 90), 91). This also agrees with Asakura et al. 92) who did not observe any change in fasting triacylglyceride concentrations with increasing MCT consumption up to maximum of 24 g/d for periods of 2 weeks each. It is possible that dose may have played a role in the earlier findings that MCT raise triacylglyceride concentrations. In fact, in the studies by Hill et al. 93) and Swift et al. 94), where triacylglyceride concentrations increased by 200 and 42%, respectively, subjects consumed 40% of energy in the form of MCT. The studies provided either 150% of weight-maintenance energy requirements 95) or 100% of weight-maintenance energy requirements 96). In the study by Cater et al. 97), triacylglyceride concentrations were higher after 3 weeks of MCT oil consumption at a level of 43% of energy intake compared to equivalent amounts of palm oil and high oleic sunflower oil. Swift et al. 98) had also recognized a potential dose effect when one of their study groups consuming half of the MCT dose of the MCT group (ie. 20% of energy intake) had no significant increase in fasting triacylglyceride. Therefore, it is highly possible that MCT consumption at a level of 20–60 g/d, or 12–20% of energy intake, does not result in adverse effects on triacylglyceride levels.
The data also agree with those of Hill et al. 99) who found that overfeeding men with MCT oil for 6 days did not result in any change in total cholesterol or HDL-C “good” cholesterol. However, that study was very short in duration and potentially not long enough to effect changes in lipid parameters. Similarly, in a weight maintenance setting, the same group did not find any effect of MCT consumption for 6 days on total cholesterol or LDL-C “bad” cholesterol but found reductions in HDL-C “good” cholesterol with MCT oil consumption 100). Data show that MCT oil consumption has a similar effect on plasma total cholesterol and LDL-C “bad” cholesterol as olive oil when consumed at similar levels. This is in contrast with data comparing MCT oil consumption and high oleic sunflower oil 101). In that study 102), MCT oil consumption led to higher total cholesterol and LDL-C “bad” cholesterol concentrations than high oleic sunflower oil consumption after a 3 week period. This may be partly attributed to the higher plant sterol content of sunflower oil compared to olive oil 103); plant sterols being well known for their hypocholesterolemic effect 104).
MCT oil consumption had no effect on glucose or insulin concentrations 105). This is similar to the observations of Hill et al. 106) in their overfeeding study with MCT and soybean oil and in a 12-week weight loss study comparing MCT and rapeseed oil/soybean oil consumption 107). An early study by Yost et al. 108) also found that MCT oil consumption, at a level of 77.5% of total fat intake for 30 days, did not lead to reductions in fasting glucose or insulin concentrations in type 2 diabetics. It therefore appears that MCT oil consumption has little impact on glycemic control.
Olive oil consumption at a level of approximately 12% of energy intake did not have any significant impact on fasting plasma lipid concentrations. This is in agreement with earlier work showing that monounsaturated fatty acids are not as effective as polyunsaturated fatty acids in reducing plasma cholesterol concentrations 109). Studies have, however, shown that olive oil consumption results in lower total cholesterol and LDL-C “bad” cholesterol and triacylglyceride than consumption of an average American diet 110). More recently, studies have shown that olive oil results in higher total cholesterol and LDL-C “bad” cholesterol and triacylglyceride than sunflower oil or rapeseed oil consumption 111) or not different from an average American diet with regards to effects on total cholesterol and LDL-C “bad” cholesterol, HDL-C “good” cholesterol or triacylglyceride 112). MCT oil consumption does not differ from olive oil in its effects on cardiovascular disease risk and may thus be considered to be a neutral dietary fat as well.
MCT oil keto
The keto diet (often termed ketogenic diet) is a very low-carb, high-fat diet that shares many similarities with the Atkins and low-carb diets. It lowers blood sugar and insulin levels, and shifts the body’s metabolism away from carbs and towards fat and ketones.
It involves drastically reducing carbohydrate intake, and replacing it with fat. Ketogenic diets are characterized by a reduction in carbohydrates (usually to less than 50 g/day) and a relative increase in the proportions of protein and fat 113). The reduction in carbs puts your body into a metabolic state called ketosis. When this happens, your body becomes incredibly efficient at burning fat for energy. It also turns fat into ketones in the liver, which can supply energy for the brain.
Ketogenic diets have undoubtedly been shown to be effective, at least in the short to medium term, as a tool to fight obesity including people with diabetes who are obese 114), hyperlipidemia and some cardiovascular risk factors 115), 116), 117), but ketogenic diets also raise some concerns among physicians 118). Many of the concerns about the use of ketogenic diet as therapeutic tools could be attributed to a broad lack of knowledge about the physiological mechanisms involved. Ketogenic diets induce a metabolic condition named “physiological ketosis” by Hans Krebs, to distinguish it from the pathological diabetic ketosis 119).
Under normal diet with average amount of carbohydrates and fat, insulin activates key enzymes in the glucose metabolic pathways, which store energy derived from carbohydrates, and when there is an absence or scarcity of dietary carbohydrates the resulting reduced insulin level leads to a reduction in lipogenesis and fat accumulation. After a few days of fasting, or of drastically reduced carbohydrate consumption (below 20 g/day), glucose reserves become insufficient both for normal fat oxidation via the supply of oxaloacetate in the Krebs cycle (which gave origin to the phrase ‘fat burns in the flame of carbohydrate’) and for the supply of glucose to the central nervous system 120), 121), 122), 123).
Figure 2. Metabolic pathway of ketosis and tissues ketolysis.
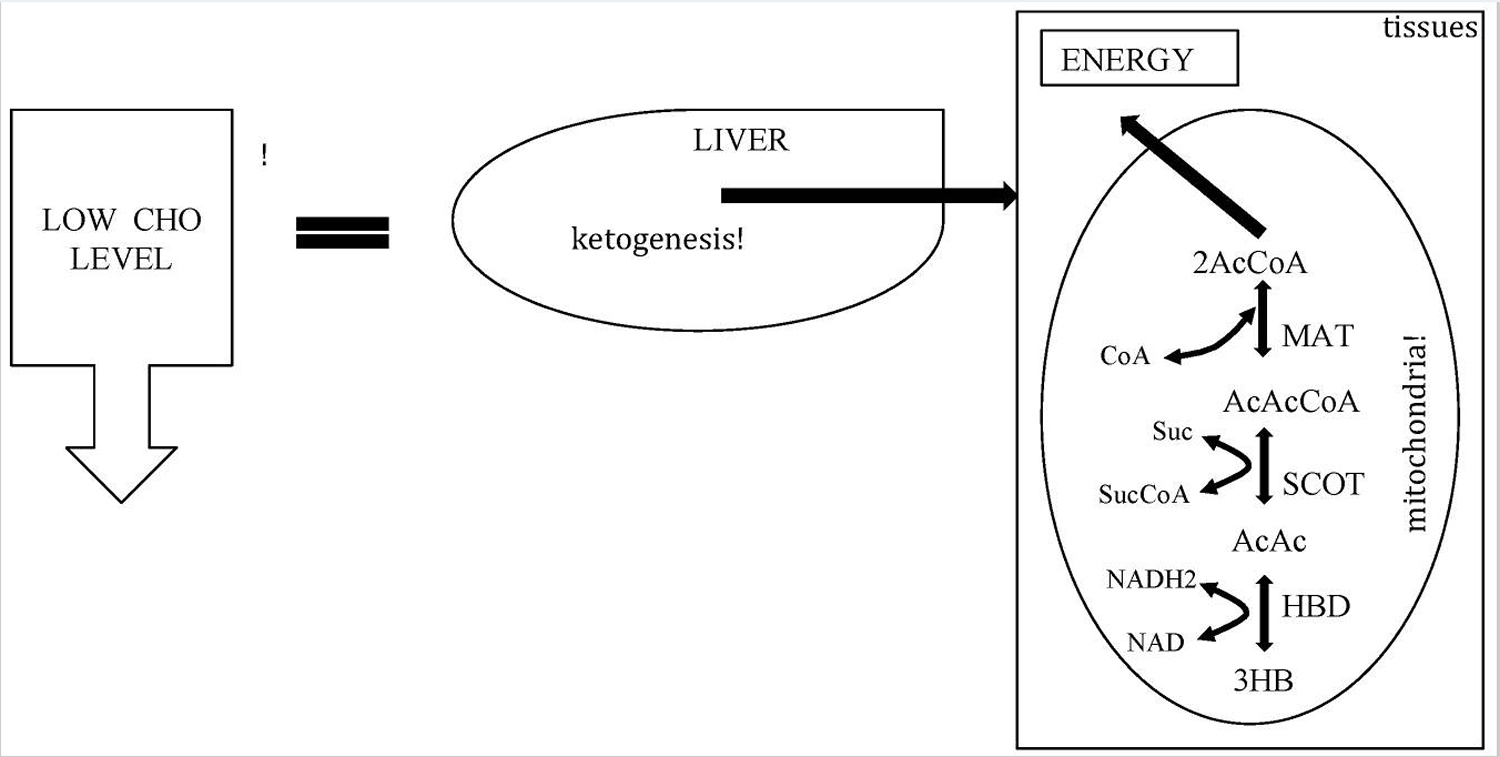
Figure 3. Ketone bodies formation from acetyl-CoA (acetyl coenzyme A).
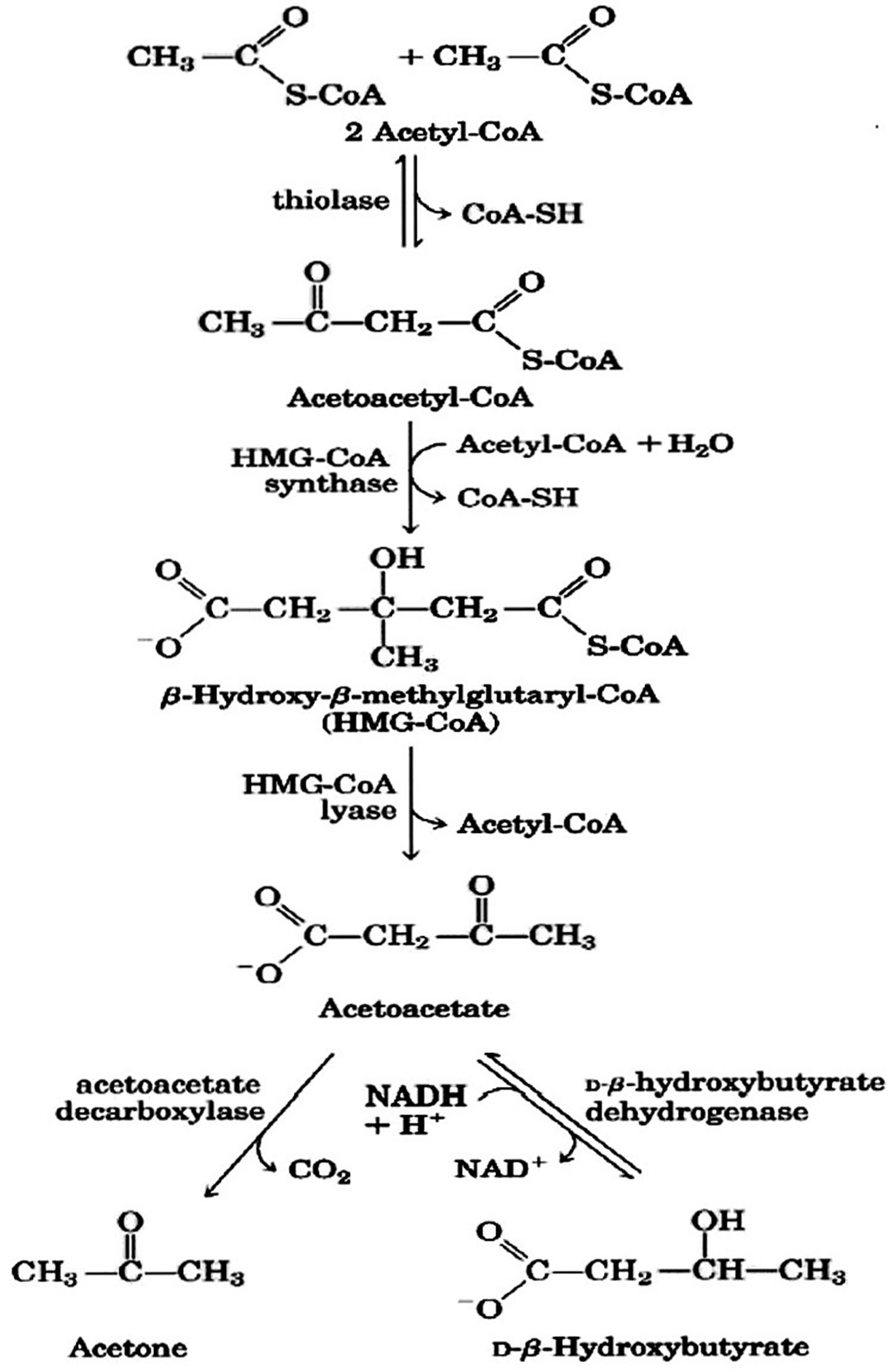
Note (Figure 3): Ketone bodies are used by tissues as a source of energy through a pathway that involves firstly that β-hydroxybutyric acid is converted back to acetoacetate (AcAc) this is then transformed into acetoacetyl-CoA and, finally, two molecules of acetyl-CoA are formed from acetoacetyl-CoA which are used in the Krebs cycle or Citric Acid cycle.
Different Types of Keto Diets
There are several versions of the keto diet, the standard keto diet (SKD) is the most researched and most recommended.
- Standard keto diet (SKD): This is a very low-carb, moderate-protein and high-fat diet. It typically contains 75% fat, 20% protein and only 5% carbs. A standard keto diet is an effective way to lose weight and lower risk factors for disease.
- Cyclical keto diet (CKD): This diet involves periods of higher-carb refeeds, such as 5 keto days followed by 2 high-carb days.
- Targeted keto diet (TKD): This diet allows you to add carbs around workouts.
- High-protein keto diet: This is similar to a standard ketogenic diet, but includes more protein. The ratio is often 60% fat, 35% protein and 5% carbs.
However, only the standard and high-protein ketogenic diets have been studied extensively. Cyclical or targeted ketogenic diets are more advanced methods, and primarily used by bodybuilders or athletes. The information in this article mostly applies to the standard ketogenic diet, although many of the same principles also apply to the other versions.
**The keto diet can boost insulin sensitivity and cause fat loss, leading to drastic improvement for type 2 diabetes and prediabetes.
Studies have now shown that the diet can have benefits for a wide variety of different health conditions. However, keep in mind that research into many of these areas is far from conclusive:
- Heart disease: The keto diet can improve risk factors like body fat, HDL levels, blood pressure and blood sugar.
- Cancer: The diet is currently being used to treat several types of cancer and slow tumor growth.
- Alzheimer’s disease: The diet may reduce symptoms of Alzheimer’s and slow down the disease’s progression.
- Epilepsy: Research has shown that the ketogenic diet can cause massive reductions in seizures in epileptic children.
- Parkinson’s disease: One study found that the diet helped improve symptoms of Parkinson’s disease.
- Polycystic ovary syndrome: The ketogenic diet can help reduce insulin levels, which may play a key role in polycystic ovary syndrome.
- Brain injuries: One animal study found that the diet can reduce concussions and aid recovery after brain injury.
- Acne: Lower insulin levels and eating less sugar or processed foods may help improve acne.
Summary
A keto diet may provide many health benefits, especially with metabolic, neurological or insulin-related diseases. You should check with your physician if you have any concerns about starting a ketogenic diet plan with pre-existing health conditions, especially if those conditions involve kidney, bone or heart problems. People with kidney disease should definitely consult with their physician about starting a ketogenic diet.
Talk to your doctor about implementing a ketogenic diet if you have any of these conditions:
- History of pancreatitis
- Active gall bladder disease
- Impaired liver function
- Impaired fat digestion
- Poor nutritional status
- Gastric bypass surgery
- Abdominal tumors
- Decreased gastrointestinal motility; this may be in conjunction with conventional cancer treatment and associated drugs
- History of kidney failure
- Pregnancy and lactation
A period of low carbohydrate ketogenic diet may help to control hunger and may improve fat oxidative metabolism and therefore reduce body weight. Furthermore new kinds of ketogenic diets using meals that mimic carbohydrate rich foods could improve the compliance to the diet. Attention should be paid to patient’s renal function and to the transition phase from ketogenic diet to a normal diet that should be gradual and well controlled. The duration of ketogenic diet may range from a minimum (to induce the physiological ketosis) of 2–3 weeks to a maximum (following a general precautionary principle) of many months (6–12 months). Correctly understood the ketogenic diet can be a useful tool to treat obesity in the hands of the physician.
References [ + ]





{kind=link}