Contents
What is megaloblastic anemia
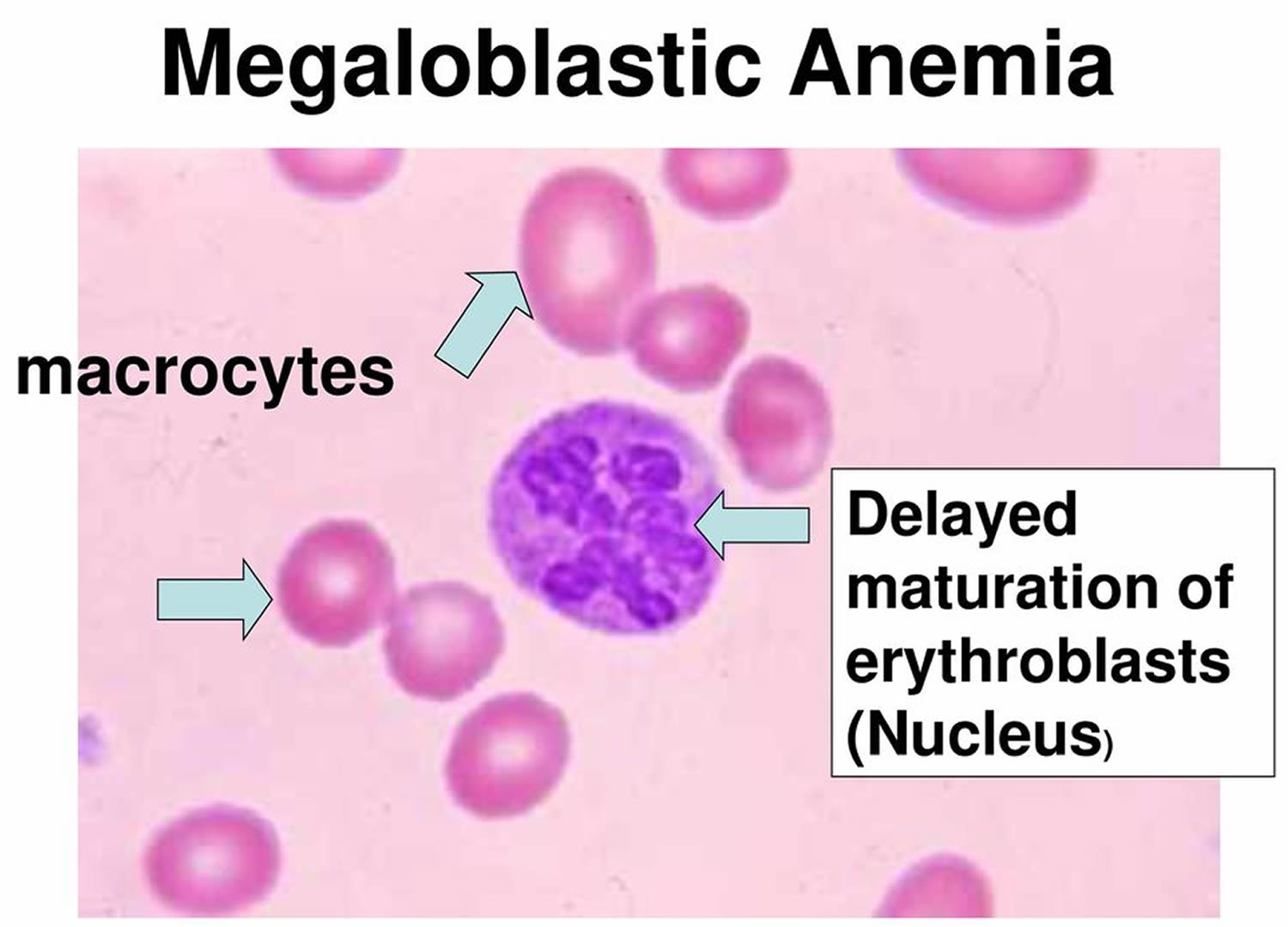
Megaloblastic anemia also known as macrocytic anemia, is a disorder of the bone marrow characterized by ineffective hematopoiesis, frequently manifested by reduction in the number of mature healthy red blood cells as well as the presence of unusually large, abnormal and poorly developed erythrocytes (megaloblasts), which fail to enter blood circulation due to their larger size. Megaloblastic anemia are usually caused by nutritional deficiencies (most common) of either vitamin B12 or folate (Vitamin-B9) or both, inherited disorders of DNA synthesis or following certain drug therapy 1).
There is a presence of erythroblasts in the bone marrow with delayed nuclear maturation because of defective DNA synthesis (megaloblasts).
Vitamin B12 deficiency is the most common cause of megaloblastic anemia. Vitamin B12 deficiency is caused by insufficient dietary intake, as in the cases of vegetarians or malnutrition, malabsorption due to the absence of intrinsic factor caused by pernicious anemia or following gastric surgery, congenital disorders, such as transcobalamin II deficiency, or exposure to nitrous oxide.
The result of one study, conducted in Japan, indicated that the most common cause of megaloblastic anemia is pernicious anemia (61%), followed by vitamin B12 deficiency due to gastrectomy (34%), vitamin B12 deficiency due to other causes (2%), and folate deficiency (2%) 2). Vitamin B12 is contained in animal foods, and the daily intake is approximately 3‐30 μg. The daily required amount is approximately 1‐3 μg, and except for stomach or intestinal obstruction, or being a strict vegetarian, vitamin B12 deficiency is rare.
Vitamin B12 binds to intrinsic factor secreted by the gastric parietal cells, and it is absorbed in the terminal ileum. Once absorbed, vitamin B12 acts as a coenzyme in the enzymatic reaction that produces methionine from homocysteine. As a result, folic acid is converted into its active form. When vitamin B12 is deficient, active folic acid is also deficient. As a result, the intracellular reaction involving the coenzyme form of folic acid is affected. Thus, not only vitamin B12 but also folate deficiencies impair DNA synthesis. Because a large amount of vitamin B12 is stored in the liver, it takes 5‐10 years for clinical problems to manifest following decreased intake or absorption of vitamin B12 3).
The signs and symptoms induced by megaloblastic anemia due to vitamin B12 deficiency are fatigue, headache, palpitations, and dyspnea, and neurological symptoms such as dysesthesia and hypoesthesia may also be present. In severe cases, ataxia, decreased proprioception, and vibratory sensation, collectively known as subacute combined degeneration, may be present. Neurologic symptoms are not generally seen in folate deficiency. Vitamin B12 deficiency does not necessarily lead to anemia and macrocytosis. Other symptoms include Hunter’s glossitis and gray hair.
Peripheral blood smear reveals macrocytic anemias and pancytopenia, and hypersegmented neutrophils may be present in severe cases. Megaloblastic changes in erythroblasts and giant metamyelocytes are seen in bone marrow, resulting from impaired nuclear differentiation. Biochemical analysis of blood shows increased levels of indirect bilirubin and lactate dehydrogenase (LDH), and a decreased level of haptoglobin. Vitamin B12 deficiency is treated with parenteral administration of vitamin B12, and hematological levels generally return to normal within one month. For patients with a permanent decrease in the ability to absorb dietary vitamin B12, such as associated with pernicious anemia or total gastrectomy, lifelong treatment is necessary.10 During hematopoietic recovery, an iron deficiency may develop. Although it is not an established treatment, recently it has been reported that oral treatment is effective, because 1%‐5% of vitamin B12 absorption in the terminal ileum is by passive diffusion, which does not involve intrinsic factor 4).
Most, but not all, megaloblastic anemia is produced by “ineffective erythropoiesis” in the bone marrow due to either folic acid or vitamin B12 deficiency 5). In folic acid deficiency the cause frequently is inadequate dietary intake, whereas vitamin B12 deficiency is almost always conditioned by some specific type of malabsorption. Anemia with oval macrocytes, few reticulocytes, moderate leukopenia, and thrombocytopenia is typical of both. Aplastic anemia, refractory anemias with cellular marrow, preleukemia, aleukemia, and erythroleukemia may have somewhat similar blood findings but are usually recognizable from bone marrow biopsy. Decreased levels of folate or vitamin B12 are the most reliable criteria of megaloblastic anemia. With these available in advance, therapy with the appropriate vitamin can be begun at once. If serum levels are unavailable or available only in retrospect, initial treatment, especially of severe anemia, should be with both vitamins. Differentiation between folate and vitamin B12 deficiency is important but impossible by blood and bone marrow morphology alone. Thus, if serum levels are unavailable, the distinction must be made, sometimes retrospectively, on the basis of other laboratory examinations, such as gastric analysis, small-bowel x-ray films, and the Schilling test.
Megaloblastic anemia is most common in the elderly with 1 in 8000. Megaloblastic anemia can be seen in all races, but is particularly common in Nordic people. There is an association with other autoimmune diseases, particularly thyroid disease, Addison’s disease and vitilgo.
Prognosis of Megaloblastic Anaemia
- Neurological changes if left untreated, can be irreversible.
- Neuorological abnormalities only occur with very low levels of serum B12.
- Patients present with symmetrical tingling sensation in the fingers and toes, early loss of vibration sense and propioception, and progressive weakness and ataxia.
- Paraplegia may result.
- Dementia and optic atrophy also occur from vitamin B12 deficiency.
Megaloblastic anemia causes
- Vitamin B12 deficiency;
- Folic acid deficiency;
- Conditions with neither B12 nor folate deficiency, e.g. orotic aciduria, where there is a defect in pyrimidine synthesis, therapy with drugs interfering with DNA synthesis and myelodysplasia.
A deficiency of folate or vitamin B12 may cause megaloblastic anaemia by reducing the supply of the coenzyme methylene tetrahydrofolate.
Other congenital and acqiuired forms of megaloblastic anaemia are due to interference with purine or pyrimidine causing an inhibition in DNA synthesis.
Megaloblastic anemia symptoms
The most common symptom of all types of anemia is fatigue (tiredness). Fatigue occurs because your body doesn’t have enough red blood cells to carry oxygen to its various parts.
A low red blood cell count also can cause shortness of breath, dizziness, headache, coldness in your hands and feet, pale or yellowish skin, and chest pain.
A lack of red blood cells also means that your heart has to work harder to move oxygen-rich blood through your body. This can lead to irregular heartbeats called arrhythmias, heart murmur, an enlarged heart, or even heart failure.
Other signs and symptoms of megaloblastic anemia include:
- Desire to eat ice or other non-food things (pica)
- Diarrhea or constipation
- Fatigue, lack of energy, or lightheadedness when standing up or with exertion
- Loss of appetite
- Pale skin
- Problems concentrating
- Shortness of breath, mostly during exercise
- Swollen, red tongue or bleeding gums.
Signs and Symptoms of Vitamin B12 Deficiency
Vitamin B12 deficiency may lead to nerve damage. This can cause tingling and numbness in your hands and feet, muscle weakness, and loss of reflexes. You also may feel unsteady, lose your balance, and have trouble walking. Vitamin B12 deficiency can cause weakened bones and may lead to hip fractures.
Severe vitamin B12 deficiency can cause neurological problems, such as confusion, dementia, depression, and memory loss.
Other symptoms of vitamin B12 deficiency involve the digestive tract. These symptoms include nausea (feeling sick to your stomach) and vomiting, heartburn, abdominal bloating and gas, constipation or diarrhea, loss of appetite, and weight loss. An enlarged liver is another symptom.
A smooth, thick, red tongue also is a sign of vitamin B12 deficiency and pernicious anemia.
Infants who have vitamin B12 deficiency may have poor reflexes or unusual movements, such as face tremors. They may have trouble feeding due to tongue and throat problems. They also may be irritable. If vitamin B12 deficiency isn’t treated, these infants may have permanent growth problems.
If you have a low vitamin B12 level for a long time, you can have nervous system damage. Symptoms can include:
- Confusion
- Depression
- Loss of balance
- Numbness and tingling that start first in the hands and feet (from nerve damage)
- Muscle weakness
- Slow reflexes
- Loss of balance
- Unsteady walking
- Confusion, memory loss, depression, and/or dementia in severe cases
How is Megaloblastic Anemia Diagnosed?
Primary care doctors—such as family doctors, internists, and pediatricians (doctors who treat children)—often diagnose and treat pernicious anemia. Other kinds of doctors also may be involved, including:
- A neurologist (nervous system specialist)
- A cardiologist (heart specialist)
- A hematologist (blood disease specialist)
- A gastroenterologist (digestive tract specialist)
Medical and Family Histories
Your doctor may ask about your signs and symptoms. He or she also may ask:
- Whether you’ve had any stomach or intestinal surgeries
- Whether you have any digestive disorders, such as Celiac disease or Crohn’s disease
- About your diet and any medicines you take
- Whether you have a family history of anemia or pernicious anemia
- Whether you have a family history of autoimmune disorders (such as Addison’s disease, type 1 diabetes, Graves’ disease, or vitiligo). Research suggests a link may exist between these autoimmune disorders and pernicious anemia that’s caused by an autoimmune response.
Physical Exam
During the physical exam, your doctor may check for pale or yellowish skin and an enlarged liver. He or she may listen to your heart for rapid or irregular heartbeats or a heart murmur.
Your doctor also may check for signs of nerve damage. He or she may want to see how well your muscles, eyes, senses, and reflexes work. Your doctor may ask questions or do tests to check your mental status, coordination, and ability to walk.
The health care provider will perform investigations and blood tests.
- A deoxyuridine suppression test can be used to rapidly determine the nature and severity of the vitamin B12 or folate deficiency in severe or complex cases of megaloblastic anemia.
- Blood samples will show the typical features of megaloblastic anemia.
- Serum bilirubin may be raised as a result of ineffective erythropoeisis.
- Serum vitamin B12 can be assayed using radioisotope dilution or immunological assays.
Pernicious anemia test
- Bone marrow examination (only needed if diagnosis is unclear)
- Complete blood count (CBC)
- Reticulocyte count
- Schilling test
- LDH level
- Methylmalonic acid (MMA) level
- Vitamin B12 level
- Levels of antibodies against intrinsic factor (IF) or the cells which make intrinsic factor.
Complete Blood Count
Often, the first test used to diagnose many types of anemia is a complete blood count (CBC). This test measures many parts of your blood. For this test, a small amount of blood is drawn from a vein (usually in your arm) using a needle.
A complete blood count (CBC) checks your hemoglobin and hematocrit levels. Hemoglobin is an iron-rich protein that helps red blood cells carry oxygen from the lungs to the rest of the body. Hematocrit is a measure of how much space red blood cells take up in your blood. A low level of hemoglobin or hematocrit is a sign of anemia.
The normal range of these levels may be lower in certain racial and ethnic populations. Your doctor can explain your test results to you.
The complete blood count (CBC) also checks the number of red blood cells, white blood cells, and platelets in your blood. Abnormal results may be a sign of anemia, another blood disorder, an infection, or another condition.
Finally, the complete blood count (CBC) looks at mean corpuscular volume (MCV). Mean corpuscular volume (MCV) is a measure of the average size of your red blood cells. Mean corpuscular volume (MCV) can be a clue as to what’s causing your anemia. In pernicious anemia, the red blood cells tend to be larger than normal.
Other Blood Tests
If the complete blood count (CBC) results confirm that you have anemia, you may need other blood tests to find out what type of anemia you have.
A reticulocyte count measures the number of young red blood cells in your blood. The test shows whether your bone marrow is making red blood cells at the correct rate. People who have pernicious anemia have low reticulocyte counts.
Serum folate, iron, and iron-binding capacity tests also can help show whether you have pernicious anemia or another type of anemia.
Another common test, called the Combined Binding Luminescence Test, sometimes gives false results. Scientists are working to develop a more reliable test.
Your doctor may recommend other blood tests to check:
- Your vitamin B12 level. A low level of vitamin B12 in the blood indicates pernicious anemia. However, a falsely normal or high value of vitamin B12 in the blood may occur if antibodies interfere with the test.
- Your homocysteine and methylmalonic acid (MMA) levels. High levels of these substances in your body are a sign of pernicious anemia.
- For intrinsic factor antibodies and parietal cell antibodies. These antibodies also are a sign of pernicious anemia.
Bone Marrow Tests
Bone marrow tests can show whether your bone marrow is healthy and making enough red blood cells. The two bone marrow tests are aspiration and biopsy.
For aspiration, your doctor removes a small amount of fluid bone marrow through a needle. For a biopsy, your doctor removes a small amount of bone marrow tissue through a larger needle. The samples are then examined under a microscope.
In pernicious anemia, the bone marrow cells that turn into blood cells are larger than normal.
Megaloblastic anemia treatment
- Treatment depends on whether Vitamin B12 or folate deficiency is present.
- Vitamin B12 deficiency is treated with hydroxycobalamin 1000ug intramuscularly to a total of 5000-6000ug over the course of 3 weeks. 1000ug is then necessary every 3 months for the rest of the patients life.
- Folate deficiency is treated with 5mg of folic acid daily. Prophylactic folate may be given in pregnancy or in chronic hematological disorders where there is rapid cell turnover.
- In severely ill patients, it may be necessary to treat with both folic acid an vitamin B12 while awaiting serum levels.
References [ + ]





{kind=link}