
Contents
What is mycoplasma pneumoniae
Mycoplasma pneumoniae is a type of “atypical” bacteria that commonly causes mild infections of the respiratory system, with an estimated 2 million cases in the U.S. each year. Experts estimate that Mycoplasma pneumoniae infections account for between 1 and 10 in every 50 cases of community-acquired pneumonia. Mycoplasma pneumoniae is often called community-acquired “atypical pneumonia” because it does not respond to sulfonamides or penicillin (beta-lactams). Mycoplasma pneumoniae pneumonia is sometimes referred to as “walking pneumonia” since symptoms tend to be milder than pneumonia caused by other germs. Mycoplasma pneumoniae infections can occur at any time of the year, but outbreaks are more prevalent in the late summer and early autumn.
Pneumonia is inflammation or swollen lung tissue due to infection with a germ. The most common type of illness caused by Mycoplasma pneumoniae bacteria, especially in children, is tracheobronchitis, commonly called a chest cold. Symptoms often include being tired and having a sore throat, fever, and cough. However, sometimes Mycoplasma pneumoniae can cause a more serious pneumonia, which may require care in a hospital. Mycoplasma pneumoniae pneumonia is usually mild and responds well to treatment with antibiotics. Having a mycoplasma infection does not confer immunity. A person can become re-infected.
While Mycoplasma pneumoniae infections are uncommon in children younger than 5 years, they are a leading cause of pneumonia in school-aged children and young adults under 40 years of age. Community-wide epidemics of this illness occur every 4 to 7 years. Mycoplasma pneumoniae infection affects predominantly children and adolescents; only a few cases with adult onset have been reported 1), perhaps because the disease is underrecognized or milder in this age group. Mycoplasma pneumoniae infection may lead to associated extrapulmonary complications, including skin manifestations such as erythema multiforme major, in up to 25% of patients and hemolysis 2). Mycoplasma pneumoniae is spread from person to person in secretions such as phlegm from the respiratory passages and has an incubation period of 2 to 3 weeks. Transmission of Mycoplasma pneumoniae bacteria usually takes place through close contact. People who live or work in crowded places like schools, homeless shelters, and prisons are at higher risk for Mycoplasma pneumoniae pneumonia. Outbreaks have occurred and are common in summer camps and colleges, as well as within households among family members.
Key facts
- Mycoplasma pneumoniae is a small bacterium that infects the lungs and other parts of the respiratory tract. People can spread these bacteria to others by coughing or sneezing.
- Pneumonia caused by Mycoplasma pneumoniae is considered an atypical bacterial pneumonia because:
- It tends to cause milder illness but symptoms tend to last longer
- It can appear differently on an x-ray
- The antibiotics commonly used in the past to treat bacterial pneumonia did not work against it
- Symptoms of illness caused by Mycoplasma pneumoniae usually start gradually. It can take someone between 1 to 4 weeks to get sick after they are exposed to the bacteria.
- Most Mycoplasma pneumoniae infections are mild and get better on their own without treatment, but serious complications can occur.
- An estimated 2 million cases of Mycoplasma pneumoniae infections occur each year in the United States 3). The true number is unknown and likely underestimated.
- Mycoplasma pneumoniae is the second most common cause of pneumonia-related hospitalization in adults with community-acquired pneumonia (lung infections developed outside of a hospital) 4).
- Mycoplasma pneumoniae may cause between 1 and 10 in every 50 cases of community-acquired pneumonia in the United States 5).
Figure 1. Mycoplasma rash (erythema multiforme major)

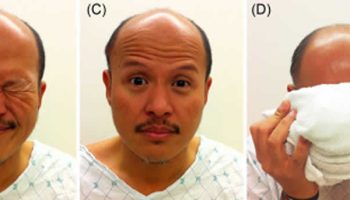
Figure 2. Mycoplasma mucositis (Stevens–Johnson syndrome)

Mycoplasma pneumoniae infections are most common in young adults and school-aged children, but can affect anyone. People at increased risk include those who live or work in crowded settings, such as:
- Schools
- College residence halls
- Military barracks
- Nursing homes
- Hospitals
People at increased risk for serious infections include people:
- Recovering from a respiratory illness
- With a weakened immune system
Mycoplasma pneumoniae infections can occur in the upper or lower respiratory tract. Mycoplasma pneumoniae bacterium can also cause a wide array of extrapulmonary manifestations without obvious respiratory disease. Therefore, patients may have a highly variable presentation. The incubation period is generally between 1 to 4 weeks; however, shorter and longer durations can occur.
Most cases of Mycoplasma pneumoniae infection are mild and self-limited, causing nonspecific symptoms such as bronchitis, a runny nose, and a nonproductive cough that may persist for several weeks. Symptoms may become more severe, causing fever, sore throat, headaches, and muscle aches, when the infection spreads to the lower respiratory tract and causes “walking pneumonia,” or, more rarely, spreads to other parts of the body. This is especially true in very young infants, in those who have underlying health conditions, such as asthma, or who have compromised immune systems, such as those with HIV/AIDS. Depending upon what parts of the body become infected, complications may range from meningitis to difficulty breathing, cardiac inflammation and arrhythmia, skin rashes, lesions or nodules, arthritis, anemia, or to Guillain-Barré syndrome.
Mycoplasma pneumoniae infection most commonly results in:
- Tracheobronchitis
- Pharyngitis
- Malaise
- Fever
- Cough
- Headache
Mycoplasma pneumoniae illness onset can be gradual and subacute, slowly progressing to a higher fever and a persistent cough. While the disease can persist for weeks or months, it is frequently mild and self-resolving. The Mycoplasma pneumoniae bacteria may persist for several weeks in the oropharynx despite completion of recommended antimicrobial therapy and resolution of clinical symptoms.
Younger patients often manifest with different clinical characteristics than patients over 5 years of age. For example, infections in younger patients may run subclinical, be mild, and not result in pneumonia. Infections in younger patients are often characterized by coryza (runny and blocked nose) and wheezing without concomitant fever, and sometimes include diarrhea and vomiting.
Mycoplasma pneumoniae bacterium
Mycoplasma pneumoniae was first isolated from the sputum of a patient with primary “atypical” pneumonia in 1944. Scientists thought the bacterium was a virus until they observed that antibiotics could be effective against it.
The cell volume of Mycoplasma pneumoniae is less than 5% of the cell volume of a typical bacillus. The small cellular mass means:
- It can pass through filters typically used to remove bacteria.
- Light microscopy cannot detect it.
- It does not produce visible turbidity in liquid growth media. In order to get a visual confirmation of growth, Mycoplasma pneumoniae cultures use specialized media.
Mycoplasma pneumoniae lacks a rigid cell wall, allowing it to alter its size and shape to suit its surrounding conditions. It is also intrinsically resistant to antimicrobials, like beta-lactams, that work by targeting the cell wall. Due to its lack of a cell wall, Mycoplasma pneumoniae is extremely susceptible to desiccation. Thus bacterial transmission from person to person by airborne droplets only occurs through close contact.
Mycoplasma pneumoniae spread through airborne droplets from person to person and is exclusively a human pathogen. Mycoplasma pneumoniae is primarily an extracellular pathogen that has evolved a specialized attachment organelle for close association with host cells. This attachment is critical to the bacteria’s survival and ability to infect. The close association between Mycoplasma pneumoniae and the host cells prevents the host’s mucociliary clearance mechanisms from removing the bacterium. The bacterium attaches to and damages the respiratory epithelial cells at the base of cilia. This activates the innate immune response and produces local cytotoxic effects.
Mycoplasma pneumoniae produces a unique virulence factor known as Community Acquired Respiratory Distress Syndrome toxin. The Community Acquired Respiratory Distress Syndrome toxin most likely aids in the colonization and pathogenic pathways of Mycoplasma pneumoniae, leading to inflammation and airway dysfunction. While Mycoplasma pneumoniae primarily lives on the surface of the respiratory epithelial cells, it can invade tissues and replicate intracellularly. The endocytosis of Mycoplasma pneumoniae by the host cells could:
- Aid in the establishment of a latent or chronic disease state
- Facilitate the bacterium in evading an immune response
- Interfere with the efficacy of certain drug therapies
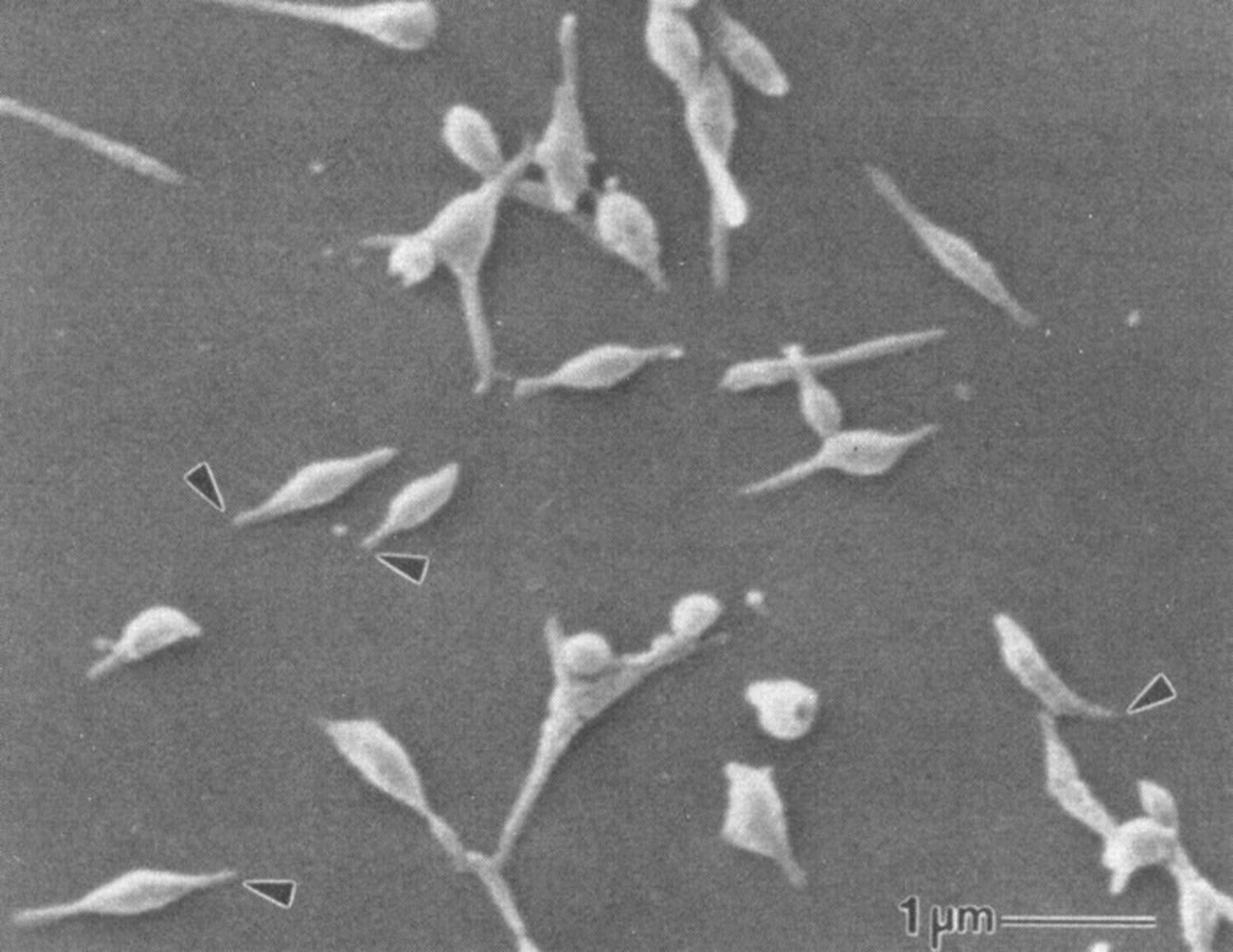
Figure 3. Mycoplasma pneumonie bacteria
How Mycoplasma pneumoniae spreads
Mycoplasma pneumoniae spread from person to person. People without symptoms may carry the bacteria in their nose or throat at one time or another. People spread Mycoplasma pneumoniae by coughing or sneezing, which creates small respiratory droplets in the air that contain the bacteria. Other people then breathe in the bacteria.
Most people who spend a short amount of time with someone who is sick with Mycoplasma pneumoniae do not become ill. However, it is common for the Mycoplasma pneumoniae bacteria to spread between people who live together. Mycoplasma pneumoniae infections usually have long incubation periods (the time between breathing in the bacteria and developing symptoms). The incubation period is usually between 1 to 4 weeks 6).
Mycoplasma pneumoniae outbreaks occur mostly in crowded settings like schools, college residence halls, military barracks, nursing homes, and hospitals. During school-based outbreaks, if people in the community get sick it is usually family members of ill school children 7).
Mycoplasma pneumoniae prevention
Like many respiratory germs, Mycoplasma pneumoniae spread by coughing and sneezing. Some tips to prevent the spread of Mycoplasma pneumoniae include:
- Cover your mouth and nose with a tissue when you cough or sneeze.
- Put your used tissue in a waste basket.
- If you don’t have a tissue, cough or sneeze into your upper sleeve or elbow, not your hands.
- Wash your hands often with soap and water for at least 20 seconds.
- If soap and water are not available, use an alcohol-based hand rub.
There is no vaccine to prevent Mycoplasma pneumoniae infections.
Previous Infections
Life-long immunity (defense to or protection from future infections) to Mycoplasma pneumoniae likely does not occur. If you get sick from Mycoplasma pneumoniae, you may get sick from it again in the future.
Antibiotics
Antibiotics can help treat patients with pneumonia caused by Mycoplasma pneumoniae. Doctors generally do not prescribe antibiotics to help prevent someone else from getting sick (for example, a close contact of an infected person).
Mycoplasma pneumoniae symptoms
In general, illness caused by Mycoplasma pneumoniae is mild with symptoms that appear and get worse over a period of 1 to 4 weeks. Mycoplasma pneumoniae bacteria can cause several types of infections.
The most common type of illness, especially in children, is tracheobronchitis, commonly known as a chest cold. Common symptoms of a chest cold include:
- Sore throat
- Fatigue (being tired)
- Fever
- Slowly worsening cough that can last for weeks or months
- Headache
Experts have estimated that up to 1 in 10 people who get ill from Mycoplasma pneumoniae get pneumonia. Common symptoms of pneumonia include:
- Cough that may produce mucus
- Fever and chills
- Shortness of breath
- Chest pain
- Fatigue
Children younger than 5 years old often do not run a fever when they have an illness caused by Mycoplasma pneumoniae. Instead they may have signs that appear more like a cold than pneumonia. They sometimes wheeze, vomit, or have diarrhea.
Extrapulmonary manifestations
As many as 25% of persons infected with Mycoplasma pneumoniae may experience extrapulmonary complications at variable time periods after onset of or even in the absence of respiratory illness 8). Autoimmune reactions have been suggested to be responsible for many of the extrapulmonary complications associated with mycoplasmal infection 9). However, the availability of PCR (polymerase chain reaction) has greatly enhanced understanding of how Mycoplasma pneumoniae can disseminate throughout the body. The presence of Mycoplasma pneumoniae in extrapulmonary sites such as blood, synovial fluid and cerebrospinal fluid, pericardial fluid, and skin lesions has been documented by polymerase chain reaction (PCR) as well as culture, so direct invasion must always be considered 10). However, the frequency of direct invasion of these sites is unknown because the organism is rarely sought for clinical purposes. It is also important to realize that extrapulmonary complications can be seen before, during, or after pulmonary manifestations or can occur in the complete absence of any respiratory symptoms 11).
Central nervous system (CNS) complications are recognized as among the most common of extrapulmonary manifestations of Mycoplasma pneumoniae infection 12) and have been known to occur since the first report appeared in 1943, even before the true identity of the causative organism was known 13). Approximately 6 to 7% of hospitalized patients with serologically confirmed cases of Mycoplasma pneumoniae pneumonia may experience neurological complications of varying severity 14). Such complications have included encephalitis, cerebellar syndrome and polyradiculitis, cranial nerve palsies, aseptic meningitis or meningoencephalitis, acute disseminated encephalomyelitis, coma, optic neuritis, diplopia, mental confusion, and acute psychosis secondary to encephalitis 15). A number of motor deficiencies have also been described, including cranial nerve palsy, brachial plexus neuropathy, ataxia, choreoathetosis, and ascending paralysis (Guillain-Barré Syndrome) 16). Encephalitis has been the most common neurological manifestation in children 17). Most patients with neurological complications experience them 1 to 2 weeks after the onset of respiratory signs, but 20% of patients or more have no preceding or concomitant diagnosis of respiratory infection 18). This figure may be higher yet in children 19).
Most of the first descriptions of CNS complications were based on serology and later on occasional isolation of Mycoplasma pneumoniae from the respiratory tract rather than the CNS. The lack of clear evidence that mycoplasmas were actually present in neurological tissues led to theories that damage to brain tissue occurred as a result of cross-reacting or autoimmune antibodies 20) and even to concern that neurological infections by other bacterial pathogens were causing false-positive mycoplasmal serology 21). The potential role of immunological sequelae of Mycoplasma pneumoniae infection that can lead to neurological complications cannot be discounted, and some CNS complications are very likely due to this mechanism as opposed to direct invasion 22). Antibodies against galactocerebroside, a component of CNS myelin, has been detected in 100% of patients with Mycoplasma pneumoniae and CNS involvement and in only 25% of those without CNS involvement 23). Postinfectious leukoencephalopathy due to Mycoplasma pneumoniae also suggests a role for autoimmunity in some cases 24).
Proof that viable organisms or Mycoplasma pneumoniae DNA can be detected directly in neural tissues and CSF provides convincing evidence that this organism does indeed disseminate from the respiratory tract in some instances 25). Neurological manifestations associated with Mycoplasma pneumoniae infections usually resolve completely, but they can result in chronic debilitating deficits in motor or mental function (384). These conditions can be severe and life threatening. Rautonen et al. 26) reported that children with Mycoplasma pneumoniae were seven times more likely to die or have severe neurological sequelae than other children, second only to cases of herpes simplex virus infection. The presence of peripheral neurological sequelae such as radiculitis and transverse myelitis has been identified as a risk factor for chronic CNS sequelae 27). Central nervous system effects due to mycoplasmas have been reviewed in detail by Talkington 28).
Whereas neurological disorders may be the most severe extrapulmonary manifestations of Mycoplasma pneumoniae infections, dermatological disorders, including erythematous maculopapular and vesicular rashes, are perhaps the most common clinically significant complications, occurring in up to 25% of patients. Although the disorders are usually self-limited, severe forms of Stevens-Johnson syndrome, conjunctivitis, ulcerative stomatitis, and bullous exanthems have been reported, and the organism has been detected directly in the cutaneous lesions 29). Clinicians should keep in mind that the presence of erythematous maculopapular rashes in Mycoplasma pneumoniae patients can also be caused by a number of antibiotics commonly used to treat respiratory tract infections.
Nonspecific myalgias, arthralgias, and polyarthropathies occur in approximately 14% of patients with acute Mycoplasma pneumoniae infection and may sometimes persist for long periods 30). Septic arthritis with detection of the organism directly in synovial fluid has been reported numerous times, occurring most commonly in hypogammaglobulinemic patients but sometimes in immunocompetent persons 31). In view of the well-known associations of animal mycoplasmas and their ability to produce chronic, naturally occurring infection of the joints and the experimental models, joint involvement by Mycoplasma pneumoniae is not unexpected. Little attention has been paid to invasive infections of bones due to Mycoplasma pneumoniae, but at least one report of osteomyelitis in a splenectomized patient with hypogammaglobulinemia has been attributed to Mycoplasma pneumoniae, in which the infection was detected by PCR 32).
Cardiac complications associated with Mycoplasma pneumoniae are relatively uncommon, but involvement has been reported at rates of from 1 to 8.5% in persons with serological evidence of infection, somewhat more commonly in adults than in children 33). Pericarditis, myocarditis, and pericardial effusion with and without cardiac tamponade have all been described, and the organism has been detected in pericardial fluid 34). According to one study 35), almost half of the patients with Mycoplasma pneumoniae infection had symptoms or signs of heart abnormalities an average of 16 months later.
Hemolytic anemia is recognized as a rare but severe complication of mycoplasmal pneumonia, occurring more often in children than in adults 36). The mechanism by which Mycoplasma pneumoniae causes this complication has been attributed to cross-reacting cold agglutinins 37). Two cases of aplastic anemia associated with Mycoplasma pneumoniae have also been reported 38). A recent report suggests that thrombotic thrombocytopenic purpura associated with Mycoplasma pneumoniae infection may be the result of cross-reactive antibodies inactivating plasma von Willebrand factor-cleaving protease 39). Fulminant infection leading to fatal disseminated intravascular coagulation has also been reported 40), as has a case of priapism in a 12-year-old boy that was felt to be due to the hypercoagulable state that sometimes occurs in association with Mycoplasma pneumoniae infection 41). If subclinical forms of hemolytic anemia and intravascular coagulation are considered, over 50% of patients with Mycoplasma pneumoniae infections may be affected.
Acute glomerulonephritis, renal failure, tubulointerstitial nephritis, and IgA nephropathy, as well as other conditions, have been sporadically reported in association with Mycoplasma pneumoniae infections 42). Kanayama et al. 43) reported cases of IgA nephropathy in persons in whom the mycoplasma infection was diagnosed serologically. Attempts to demonstrate mycoplasma antigen in damaged renal tissue by immunohistochemical techniques have not been uniformly successful, once again leading to theories that an antibody-mediated pathogenesis is responsible 44). A recent attempt to use PCR to identify mycoplasmas in renal tissue from four children with acute nephritis concomitant with serological evidence of recent Mycoplasma pneumoniae infection also failed 45). However, the presence of mycoplasma antigen has been demonstrated by immunoperoxidase staining in renal tissue in a patient with acute interstitial nephritis 46).
Mycoplasma pneumoniae infection may be associated with a variety of nonspecific complaints related to the gastrointestinal system. These include nausea, vomiting, and diarrhea. Rarely, cholestatic hepatitis and pancreatitis have been associated with respiratory infections 47).
Up to one-third of patients with Mycoplasma pneumoniae infection may have nonspecific ear symptoms, including otitis externa, otitis media, and myringitis 48). Acute rhabdomyolysis was recently reported in association with Mycoplasma pneumoniae infection in a 15-year-old patient 49). Ocular manifestations have been reported in children occasionally and include conjunctivitis, anterior uveitis, optic neuropathy, retinitis and retinal hemorrhages, iritis, and optic disk swelling, with or without permanent degradation of vision 50). Mycoplasma pneumoniae has been isolated from the urogenital tracts of males and females and has been cultured from a tubo-ovarian abscess 51). Given the apparent ability of the organism to invade the bloodstream, infections in almost any organ system are possible. Higuchi et al. 52) reported the detection of Mycoplasma pneumoniae by PCR in ruptured atherosclerotic plaques and stenotic heart valves and speculated about its possible association, along with Chlamydia pneumoniae, as a risk factor for embolization and myocardial infarction. Additional data are necessary to determine the significance of these preliminary reports.
Mycoplasma pneumoniae complications
While Mycoplasma pneumoniae usually causes mild disease, severe complications can occur, resulting in needing care in a hospital. Mycoplasma pneumoniae infections can cause or worsen the following complications:
- Serious pneumonia
- Asthma attacks or new asthma symptoms
- Encephalitis (swelling of the brain)
- Hemolytic anemia (too few red blood cells, which means fewer cells to deliver oxygen in the body)
- Renal dysfunction (kidney problems)
- Skin disorders (Stevens-Johnson syndrome, erythema multiforme, toxic epidermal necrolysis)
Mycoplasma test
Clinical laboratories can provide diagnostic testing for Mycoplasma pneumoniae infections using culture, serology, or nucleic acid amplification methods (see chart below). Currently, there are two commercially available kits cleared by the U.S. Food and Drug Administration (FDA) for the detection of M. pneumoniae. When additional or specialized testing is necessary, local or state public health laboratories can provide diagnostic support or forward specimens to Centers for Disease Control and Prevetion (CDC).
Table 1. Mycoplasma pneumoniae Diagnostic Tests – Advantages, Disadvantages, and Availability
| Method | Advantages | Disadvantages | Test Setting |
|---|---|---|---|
| Culture |
|
|
|
| Serology |
|
|
|
| Molecular |
|
|
|
Footnotes:
- 1 Provided that appropriate additional procedures are used to identify the recovered isolate to species level.
- 2 Other tests performed at Centers for Disease Control and Prevetion (CDC) for special investigations include: culture, strain typing, P1 adhesin typing, multiple-locus variable number tandem repeat analysis typing, whole genome sequencing.
- 3 State and local departments of public health may offer these diagnostic tests for the detection of Mycoplasma pneumoniae
- 4 Use of trade names or commercial sources is for identification only and does not imply endorsement by the Centers for Disease Control and Prevention or the Department of Health and Human Services.
Abbreviation: PCR = polymerase chain reaction; CSF = cerebrospinal fluid
How is Mycoplasma test used?
Mycoplasma testing is primarily used to help determine if Mycoplasma pneumoniae is the cause of a respiratory tract infection. It may also be used to help diagnose a systemic infection that is thought to be due to mycoplasma.
Blood tests for antibody to Mycoplasma pneumoniae
Two types of antibodies produced in response to an Mycoplasma pneumoniae infection may be measured in the blood, IgM and IgG.
- IgM antibodies are the first to be produced by the body in response to infection. Levels of IgM rise for a short time period and then decline, often remaining detectable in the blood for several months.
- IgG antibody production follows IgM production, rising over time, and then stabilizing. Once a person has had a mycoplasma infection, they will typically have some measurable amount of mycoplasma IgG antibody in their blood for the rest of their life.
In order to diagnose an active Mycoplasma pneumoniae infection, a health practitioner may order both Mycoplasma pneumoniae IgM and IgG antibody tests as acute samples and then collect another Mycoplasma pneumoniae IgG test two to four weeks later as a convalescent sample. This combination of tests is ordered so that the change in the amount of IgG can be evaluated and because some people, especially infants and those with compromised immune systems, may not produce expected amounts of IgG or IgM.
Direct detection
Mycoplasma pneumoniae detection involves finding the microbe in the respiratory secretions, blood, fluid, or tissue sample. This can be done either by culturing the mycoplasma in a supportive environment or by detecting its genetic material (DNA).
A mycoplasma culture is the traditional method of detection, but it can be challenging and is not always successful. Culturing mycoplasma is more difficult than culturing common bacteria such as staphylococci or streptococci. Mycoplasma lack cell walls and do not grow well on routine bacterial culture media. They lack cell walls and cannot be visualized with a Gram stain as done with most bacteria. Growing mycoplasma involves incubating the patient’s sample in a special nutrient media to promote the growth of these microbes, which are slow to grow.
A negative Mycoplasma pneumoniae culture must be held for 3-4 weeks to confirm that a mycoplasma is not present, compared to 2-4 days for most bacteria. Antibody testing, or sometimes DNA testing, is usually ordered in addition to, or instead of, a Mycoplasma pneumoniae culture because of this long incubation period before results can be released.
DNA testing is rapid and sensitive but was not routinely offered in many microbiology laboratories because there was not a commercial source for the test. Now there are syndromic panels available that allow the detection of multiple respiratory pathogens that include Mycoplasma pneumoniae and that will increase the ability of laboratories to test for this microbe. However, the detection of mycoplasma DNA does not confirm a current infection. The presence of mycoplasma DNA may indicate the microbe is colonizing a person or mycoplasma DNA may be detectable after the symptoms of infection have resolved and the organisms are no longer viable.
Mycoplasma pneumoniae DNA testing may sometimes be ordered, along with other tests, such as testing for Chlamydia pneumoniae, Bordetella pertussis, and Legionella species to help distinguish between these organisms as the cause of a respiratory infection.
Occasionally, testing may be used to determine if Mycoplasma hominis, Mycoplasma genitalium, or Ureaplasma urealyticum is the cause of an infection of the genital or urinary tract. Mycoplasma hominis and Ureaplasma urealyticum genital samples are typically tested using a culture method that takes several days to recover the microbes, but Mycoplasma genitalium, which can take 1-2 months to grow, may be more reliably detected with DNA testing.
The choice of tests and body samples collected depends on the age of the person being tested, their general health status and symptoms, and on the healthcare practitioner’s clinical findings and suspicions of organ involvement. A person with a suspected mycoplasma infection may be treated based upon clinical findings and imaging studies with or without laboratory testing.
When is Mycoplasma test ordered?
Mycoplasma pneumoniae testing may be ordered when someone has severe respiratory symptoms that are not due to a typical bacterial infection, such as pneumococcal pneumonia. Some of these symptoms may include:
- Nonproductive cough that may persist for several weeks
- Fever
- Sore throat
- Headaches and muscle aches
Testing may be done when an infection spreads to the lower respiratory tract, causing “walking pneumonia,” and/or spreads to other parts of the body and causes complications such as rash, arthritis, encephalitis, inflammation of the heart muscle or the lining that surrounds the heart or hemolytic anemia, and when a person is not responding to standard treatments. It may also be ordered to help track and control the spread of Mycoplasma pneumoniae infections during an outbreak.
Testing for other species of mycoplasma may be performed, in addition to Mycoplasma pneumoniae testing, when very young infants and those with compromised immune systems have lung and/or systemic infections or complications that could be due to a mycoplasma infection.
In general, IgM and IgG testing are performed when a health practitioner suspects that a person has an active Mycoplasma pneumoniae infection, and another IgG test may be performed 2-4 weeks later to document a rise in antibody levels in response to an infection. A Mycoplasma pneumoniae culture and a DNA test may also be ordered when an active infection is suspected.
Testing of genital samples is not often done because mycoplasmas are frequently part of the normal flora of the genital tract. However, a culture for Mycoplasma hominis and Ureaplasma urealyticum may sometimes be ordered when a sexually active male has inflammation of the urethra that is not due to gonorrhea or chlamydia (non-gonococcal urethritis) or when a female is suspected of having a genital mycoplasma infection, after tests for gonorrhea and chlamydia have come back negative.
What does the Mycoplasma test result mean?
Antibody testing
Significant concentrations of Mycoplasma pneumoniae IgM and/or a four-fold increase in IgG levels between the initial sample and the convalescent sample indicate an active or recent Mycoplasma pneumoniae infection. Increases in IgG, without IgM, can also be seen with a re-infection.
If neither IgM or IgG are present in detectable concentrations, then it means that a person being tested either does not have an active infection, has not had a mycoplasma infection (recent or in the past), or that the person’s immune system has not produced antibodies in response to the microbe.
Direct detection
The detection of one of the mycoplasmas or Ureaplasma urealyticum in a cultured sample may indicate that the person being tested has a mycoplasma infection, particularly if the sample is from a body site that is normally sterile, such as joint fluid or blood. However, if the sample is from the respiratory tract or the genital tract, a positive culture may also mean that the mycoplasma is present as part of their normal flora. For example, Ureaplasma urealyticum is present in the genital tract of about 60% of healthy women and Mycoplasma hominis is present in about 20%.
If mycoplasma is not detected in a culture, then it may mean that the person is not infected by that microbe or that the organism was not present in sufficient quantity to be detected in the sample tested.
With DNA testing for Mycoplasma pneumoniae, if the mycoplasma is present in the sample, then the person may have Mycoplasma pneumoniae or may be colonized by the organism. If it is not detected, then the person may not have a Mycoplasma pneumoniae infection or the microbe was present in numbers too low to be detected.
How is the sample collected for testing?
The sample required depends on the method being used and on the health status of the person being tested:
- Antibody testing requires a blood sample, obtained by inserting a needle into a vein in the arm.
- Direct detection of mycoplasma may be done on a variety of samples. For a respiratory infection, samples may include sputum, a washing of the bronchi in the lungs, or throat swab. If a systemic infection is being diagnosed, blood, joint fluid, body fluids, or tissues samples may be cultured. Some samples may require a special procedure to collect them. To detect a genital infection, a swab of the cervix or urethra may be collected.
Collecting an oropharyngeal and nasopharyngeal swab specimen
Use only sterile Dacron, rayon, or nylon swabs with plastic shafts. If available, use flocked swabs. DO NOT use calcium alginate swabs or swabs with wooden sticks, as they may contain substances that inactivate some agents and inhibit some molecular assays.
For oropharyngeal swab specimens:
- Insert swab into the posterior pharynx and tonsillar areas. Rub swab over both tonsillar pillars and posterior oropharynx and avoid touching the tongue, teeth, and gums.
For nasopharyngeal swab specimens:
- Insert flexible shaft swab through the nares parallel to the palate (not upwards) until it contacts the nasopharynx. Indications of contact include encountering resistance and the distance equaling that from the ear to the patient’s nostril. Gently rub and roll the swab.
Can testing for mycoplasma be performed in my doctor’s office?
Samples may be collected in your healthcare practitioner’s office, but testing requires specialized equipment and will need to be done in a hospital or reference laboratory.
Mycoplasma pneumoniae treatment
Most people will recover from an illness caused by Mycoplasma pneumoniae without medicine. However, if someone develops pneumonia (lung infection) caused by Mycoplasma pneumoniae, doctors usually prescribe antibiotics as treatment. Antibiotics can help patients recover from the illness faster if started early on.
There are several types of antibiotics available to treat pneumonia caused by Mycoplasma pneumoniae. If a doctor diagnoses you or your child with an Mycoplasma pneumoniae illness, your doctor will explain how to treat it.
Some Mycoplasma pneumoniae are resistant to some antibiotics used for treatment.
There are no evidence-based guidelines for treatment of Mycoplasma pneumoniae–associated mucositis 53). Empiric antibiotic therapy is an effective first-line approach 54). Systemic corticosteroids and intravenous immunoglobulins may limit disease duration and severity and should be considered in severe cases, to limit the potential for complications associated with mucous membrane adhesions, especially ocular sequelae.
Antibiotic Treatment
Most Mycoplasma pneumoniae infections are self-limiting; however, clinicians routinely treat pneumonia caused by Mycoplasma pneumoniae with antibiotics. All mycoplasmas lack a cell wall and, therefore, all are inherently resistant to beta-lactam antibiotics (e.g., penicillin).
Clinicians treat Mycoplasma pneumoniae infection with macrolide, tetracycline, or fluoroquinolone classes of antibiotics, taking age of the patient and local antibiotic resistance patterns into consideration:
- Macrolides (e.g., azithromycin): Children and adults
- Fluoroquinolones: Adults
- Tetracyclines (e.g., doxycycline): Older children and adults
Clinicians should not prescribe fluoroquinolones and tetracyclines for young children under normal circumstances. Macrolides are generally considered the treatment of choice. However, clinicians should practice prudent use of macrolide drugs due to the emergence of macrolide-resistant strains of Mycoplasma pneumoniae.
Antibiotic Resistance
Resistance to macrolides has been emerging in Mycoplasma pneumoniae since 2000. This issue is especially troubling in Asia, where resistance rates have been as high as 90%. The United States and Europe have also reported macrolide resistance. Current data suggest that the prevalence of macrolide resistance in Mycoplasma pneumoniae is probably rising in the United States. The increased use of azithromycin in recent years to treat a number of illnesses could help explain this rise.
Studies have reported that patients with infections due to macrolide-resistant strains may have fever and cough for a longer duration than patients infected with macrolide-sensitive strains.
Experts need to learn more about the extent of macrolide resistance and its clinical implications to inform prescribing decisions.
References [ + ]



{kind=link}