Contents
What is pectus carinatum
Pectus carinatum refers to a chest wall abnormality in which the breastbone (the sternum and/or ribs) is pushed outward 1. Pectus carinatum is often described as giving the person a bird-like (pigeon) appearance. Pectus carinatum is the second most common congenital deformity of the anterior chest wall and comprises 5–20% of all anterior chest wall deformities 2, which generally presents during childhood and worsens through adolescence. Sometimes the deformity isn’t noticeable until after the adolescent growth spurt. If the condition occurs in isolation, it is often not associated with any additional signs or symptoms.
Two subtypes of pectus carinatum have been described 3:
- The chondrogladiolar variant, which comprises up to 95% of the cases, and presents with protrusion of the sternal body, and
- The chondromanubrial variant, showing protrusion of the superior component of the sternum (manubrium).
The underlying cause of isolated pectus carinatum is unknown. Among the several proposed causes of pectus carinatum, exaggerated growth of the costal cartilage is the most widely accepted explanation, similar to pectus excavatum 4. However, evidence for this hypothesis is lacking, and the aetiology of the potential cartilage overgrowth is also uncertain 5.
People with pectus carinatum generally develop a normal heart and lungs. However, the deformity may prevent these from functioning as well as they could (see Figures 1 to 3). There is some evidence that pectus carinatum may prevent complete emptying of air from the lungs in children. These young people may have less stamina, even if they do not recognize it. Chest pain or discomfort, especially when lying in prone position, intolerance to physical exercise, scoliosis, impaired shoulders and kyphotic position are some of the physical signs and symptoms 3. Rarely, affected people report shortness of breath during exercise, frequent respiratory infections, and/or asthma.
Pectus carinatum can also have an impact on a child’s self-image and reduced quality of life 6. Some children live happily with pectus carinatum. For others, the shape of the chest can damage their self-image and self-confidence. Many patients refer feelings of discomfort, shame, shyness, anxiety, anguish, and even depression, which can lead to social isolation.
Pectus carinatum can also be associated with a variety of genetic disorders and syndromes, including Marfan syndrome, Noonan syndrome, Morquio syndrome, homocystinuria, osteogenesis imperfecta, Coffin-Lowery syndrome, cardiofaciocutaneous syndrome, and certain chromosome abnormalities. In these cases, the condition has an underlying genetic cause and is associated with additional features that are characteristic of the genetic disease. Pectus carinatum is primarily a cosmetic concern and treatment, therefore, depends on the severity of the condition and the interests of the affected person and their family. In those who choose to pursue treatment, bracing and/or surgery may be an option.
While surgical repair is an option for people with severe pectus carinatum, the use of a brace to help flatten the chest is the preferred treatment for children whose bones are still growing. The brace is worn up to 23 hours a day, and results can begin to be seen in just a few months.
Figure 1. Pectus carinatum

Figure 2. Sternum and chest wall anatomy
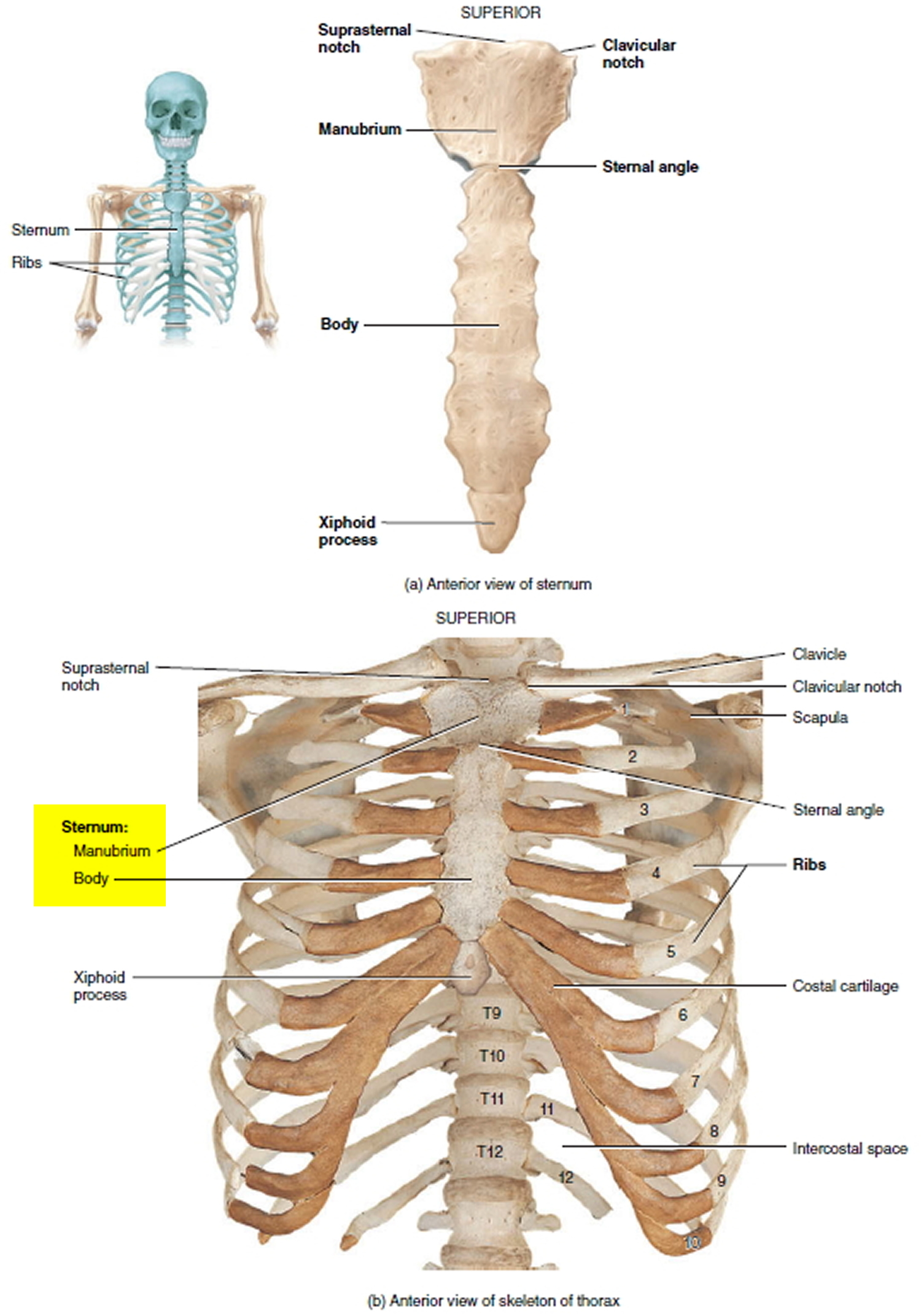
Figure 3. Important organs behind the sternum
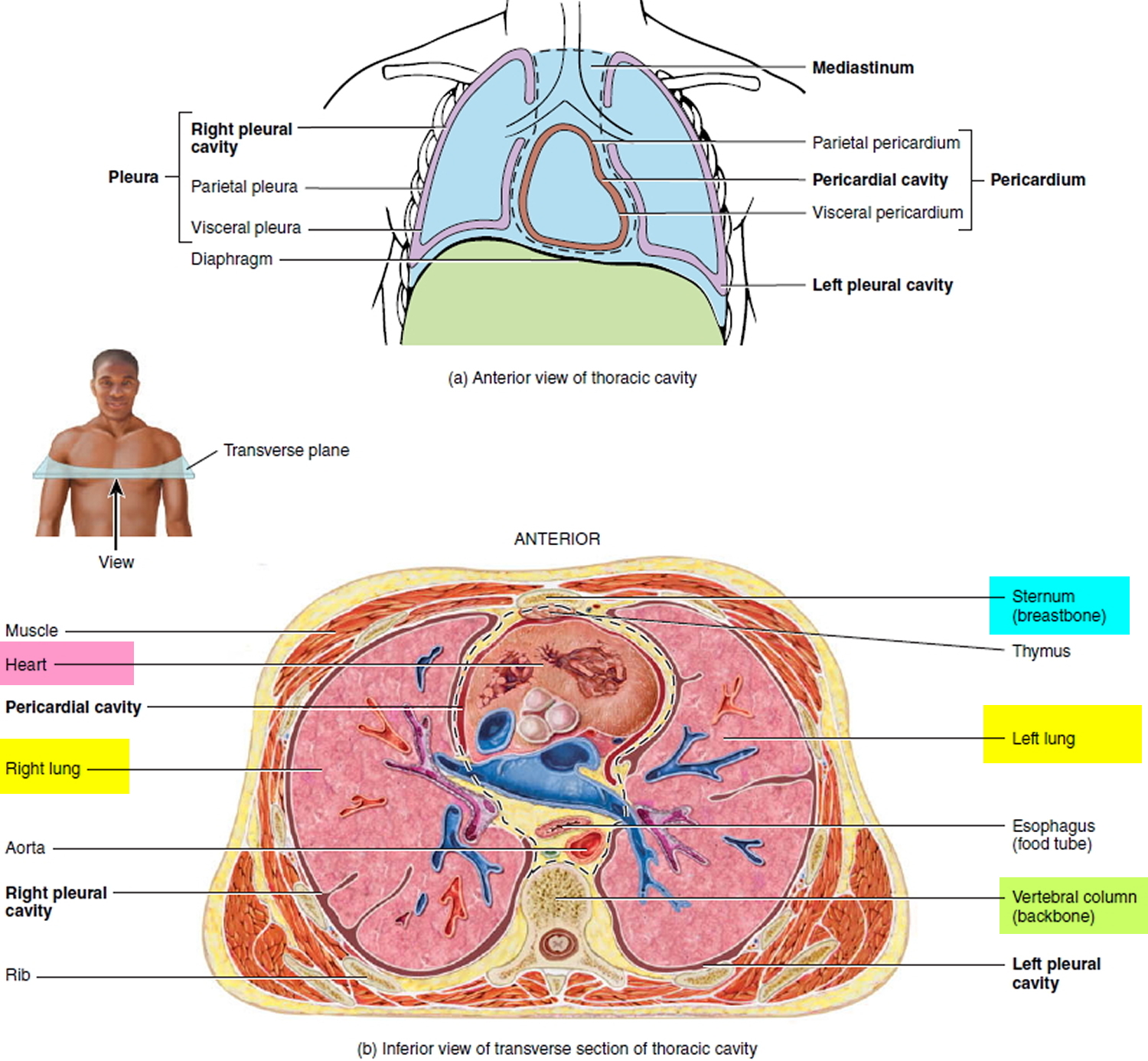
Figure 4. Pectus carinatum brace

Pectus carinatum causes
The pathophysiology of pectus carinatum is not well established. About 25% of patients with pectus carinatum have a family history of some type of chest wall defect 7. Various diseases such as scoliosis, Marfan syndrome, osteogenesis imperfecta, Noonan syndrome, as well as some types of congenital heart disease have been associated with pectus carinatum 8.
Pectus carinatum causes may include:
- Congenital pectus carinatum (present at birth)
- Trisomy 18
- Trisomy 21
- Homocystinuria
- Marfan syndrome
- Morquio syndrome
- Multiple lentigines syndrome
- Osteogenesis imperfecta
Nakaoka et al. 9 have reported that, in patients with asymmetric pectus excavatum, the lengths of the ribs and costal cartilages in the more depressed side were not longer than those in the contralateral side. They had hypothesized that, if overgrowth of the costal cartilage was the cause of pectus excavatum, the costal cartilage lengths on the more depressed side would be longer than those on the opposite side. Their findings suggest, however, that overgrowth of the costal cartilage might not be the aetiology of that asymmetric chest deformity. A study by Park et al 1 demonstrated that neither the rib length nor the cartilage lengths were different between the more protruded side and the opposite side in these patients. Based on these findings, it was concluded that overgrowth of the costal cartilage might not be the responsible factor in pectus carinatum. These findings suggest that overgrowth of costal cartilage cannot explain the asymmetric protrusion of anterior chest wall and may not be the main cause of pectus carinatum.
Pectus carinatum diagnosis
The provider will perform a physical exam and ask questions about the child’s medical history and symptoms. Questions may include:
- When did you first notice this? Was it present at birth, or did it develop as the child grew?
- Is it getting better, worse, or staying the same?
- What other symptoms are present?
Tests that may be done include:
- Lung function testing to measure how well the heart and lungs are performing
- Lab tests such as chromosome studies, enzyme assays, x-rays, or metabolic studies
A brace may be used to treat children and young adolescents. Surgery is sometimes done. Some people have gained improved exercise ability and better lung function after surgery.
Pectus carinatum treatment
It is estimated that the optimal timing for non-surgical therapy of pectus carinatum is between 10 and 15 years old, because of greater chest wall malleability, and enough time available to execute the bracing protocols and minimize recurrence 3.
Younger patients have a lower pressure of correction (major thoracic flexibility) than older patients and better final results are seen in pectus carinatum patients with lower pressure of corrections. Unfortunately, it is still frequent to receive patients older than this, because the severity of the pectus carinatum or the associated signs or psychological impact have been overlooked or underestimated.
Pectus carinatum surgery
Surgical repair is indicated in cases of symmetric carinatum that are not suitable for bracing; asymmetrical chest wall deformities; and combined excavatum and carinatum deformities.
Simple external compression of pectus carinatum seems to have its limitations, particularly the repair of asymmetric pectus carinatum or excavatum/carinatum complex. Compression of the chest wall protrusion by using a pectus bar was introduced by Abramson 10, but simple external compression was not successful in asymmetric pectus carinatum or excavatum/carinatum complex. Therefore, the “press-mold” by sandwiching two bars inside and outside of the chest wall was introduced for remodeling the entire anterior chest wall for cases of carinatum or combined type (excavatum/carinatum) chest wall deformities 11. Dr. Park et al 11 had an excellent result in a case of extreme pectus excavatum/carinatum complex (Figure 5), they were convinced that the sandwich approach is the ideal method of correcting all types of chest wall protrusions. The researchers applied this technique to a total of 58 patients including those with pectus carinatum and mixed deformities of excavatum and carinatum. The morphological features of the patients were five (8.6%) symmetric pectus carinatum, 11 (18.9%) asymmetric pectus carinatum, and 42 (72.4%) pectus carinatum/excavatum complex cases. The length of follow-up of the patients was: 3 months to 9 years (median, 48 months) for the sandwich technique; 3 to 52 months (median, 37 months) for the flare-buster; and 3 to 9 months (median, 5 months) for the magic string technique.
The result of repair was near complete resolution of carinatum in 50 patients (96.2%), but in two patients, the carinatum was not effectively compressed by the sandwich 1 technique due to its rigidity 11. The sandwich 2 technique achieved an almost symmetric configuration with no residual carinatum in all six cases 11. No serious complications related to the procedure were observed, except for one pleural effusion and one wound hematoma. Thirty-three patients (56.9%) had pectus bar removal, and their results were favorable.
This approach was extended to relieve the lower costal flare, the flare-buster, in 2013 11. The lower costal flare invariably accompanied with the pectus excavatum due to the unique feature of the pectus excavatum deformity: the scaphoid costal cartilage configuration. It has no physiological significance but often causes cosmetic dissatisfaction. The simple maneuver adapted from the sandwich technique using heavy strings created an effective relief of the flares. For this purpose, instead of the external pectus bar, heavy strings are used to compress the costal protrusions.
The flare-buster was applied to 426 patients of pectus excavatum. The mean age of the patients was 7.8 years (range, 3 to 50 years) 11. Seventy six percent of the patients was male. The morphological features of the chest wall deformity were: symmetric in 307 (72.1%) patients, eccentric in 92 (21.6%), and unbalanced in 24 (5.6%).
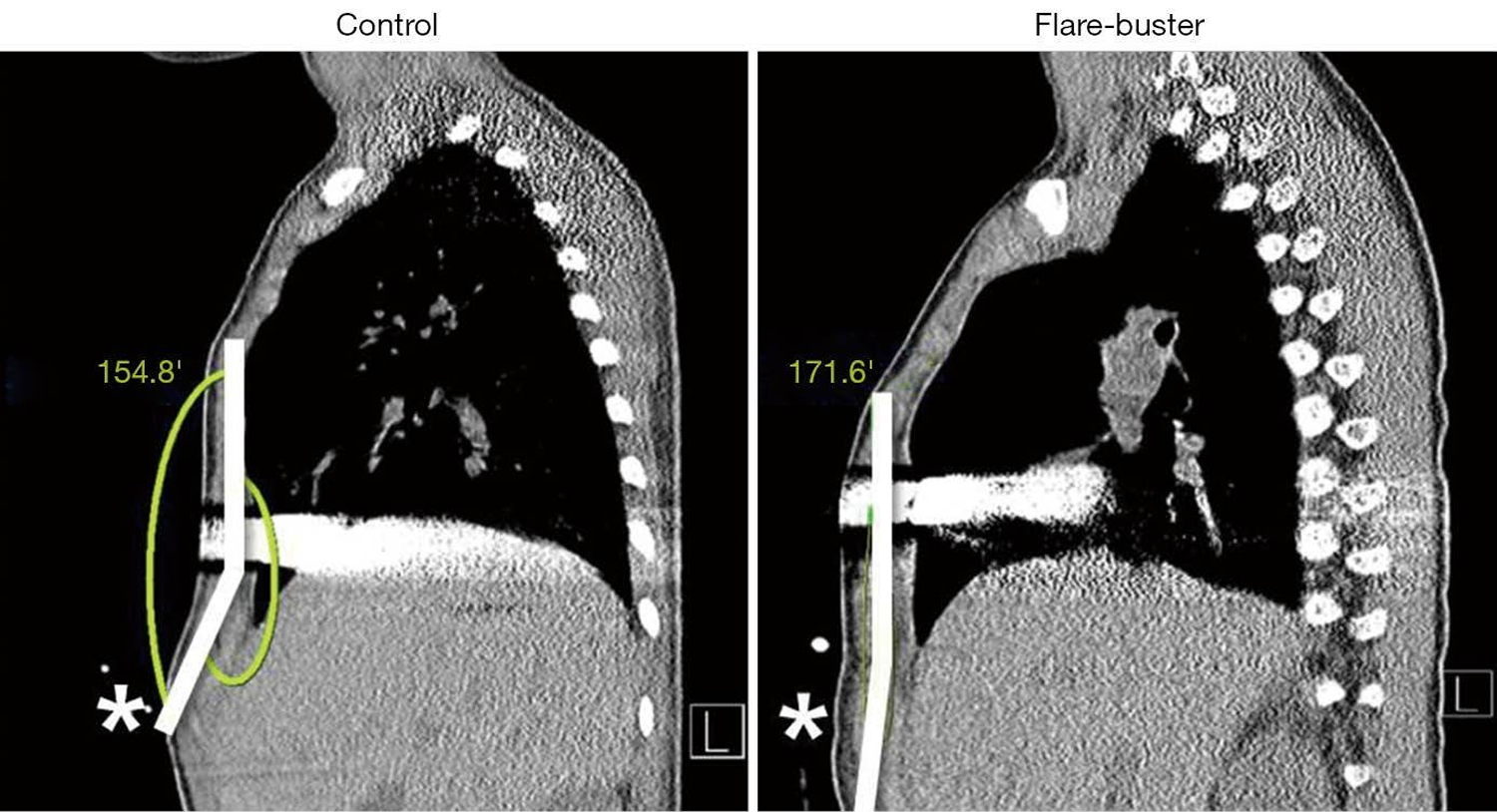
The efficacy of the flare-buster was verified using measurements of flare angles before and after repair (see Figure 9). There was a significant difference in flare angles between the control and the flare-buster group: 163.04±4.58 degrees in the control group versus 174.97±2.31 degrees in the flare-buster group 11.
The magic string was applied to 39 patients with pectus excavatum 11. The mean age was 9.03 years (range, 3 to 26 years). Thirty patients (76.9%) were male. The morphological features of the chest wall deformities were: symmetric in 24 (66.7%) patients, eccentric in four (10.3%), and unbalanced in eight (20.5%). The magic string relieved focal protrusions and was assessed to be effective according to the operator’s judgment.
There were no complications related to the flare-buster or the magic string procedure 11.
The sandwich technique, flare-buster, and the magic string were initially thought to be possible only in pediatric patients, but their use continues to extend to all age groups. Young adult patients have a resistant costal cage, but with the aid of the Omni crane compression system, the carinatum can be molded to a greater degree 12.
Figure 5. Pectus carinatum surgery

The researchers found that the sandwich technique is indicated for the following chest wall deformities: pectus carinatum, symmetric (Figure 6) or asymmetric (Figure 7); pectus excavatum/carinatum complex (Figure 8); pectus excavatum with focal protrusions; and lower costal flare relief. The flare angle is defined as the angle between the sternal line and flare line (Figure 9).
Figure 6. Repair of symmetric pectus carinatum: press-molding the anterior chest wall by sandwiching between the external bar (white) and the internal bar (gray). (A) pre-repair; (B) post-repair.
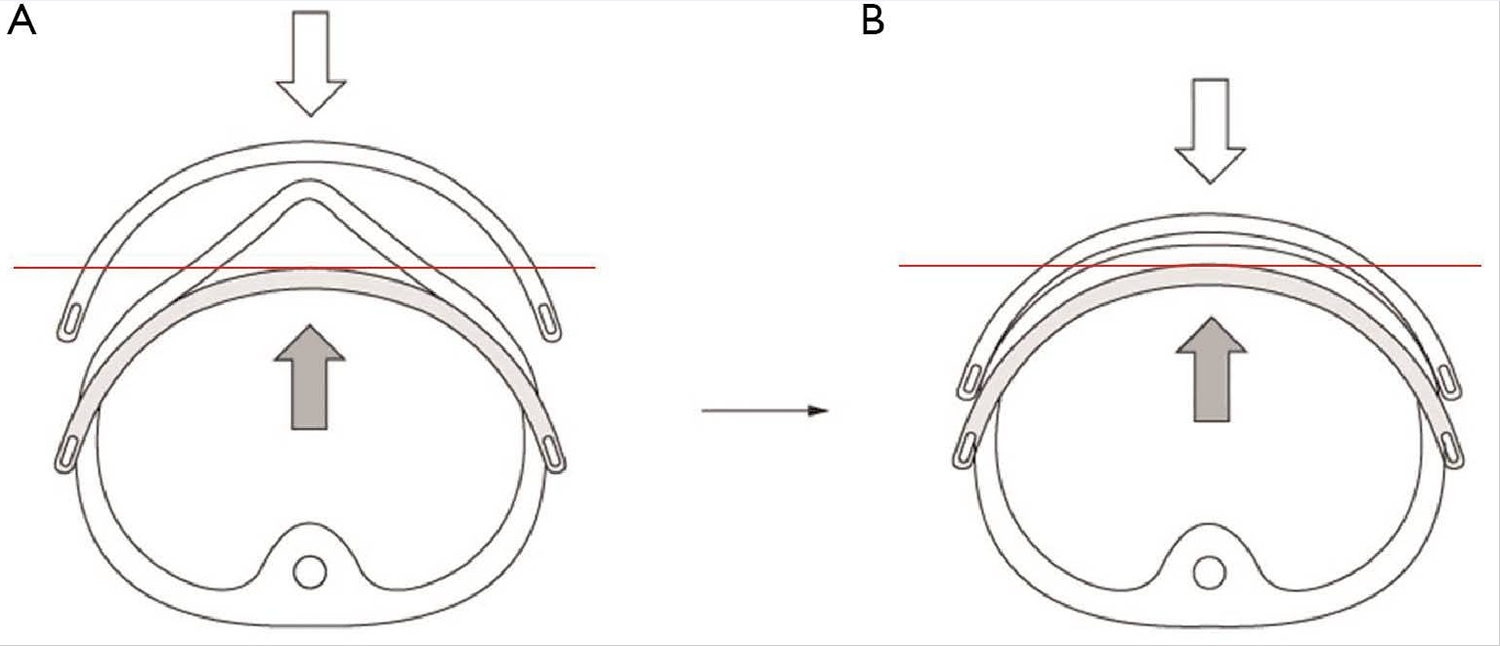
Figure 7. Repair of asymmetric (eccentric) pectus carinatum: press-molding the anterior chest wall by sandwiching between the external bar (white) and the internal bar (gray). (A) pre-repair; (B) post-repair.
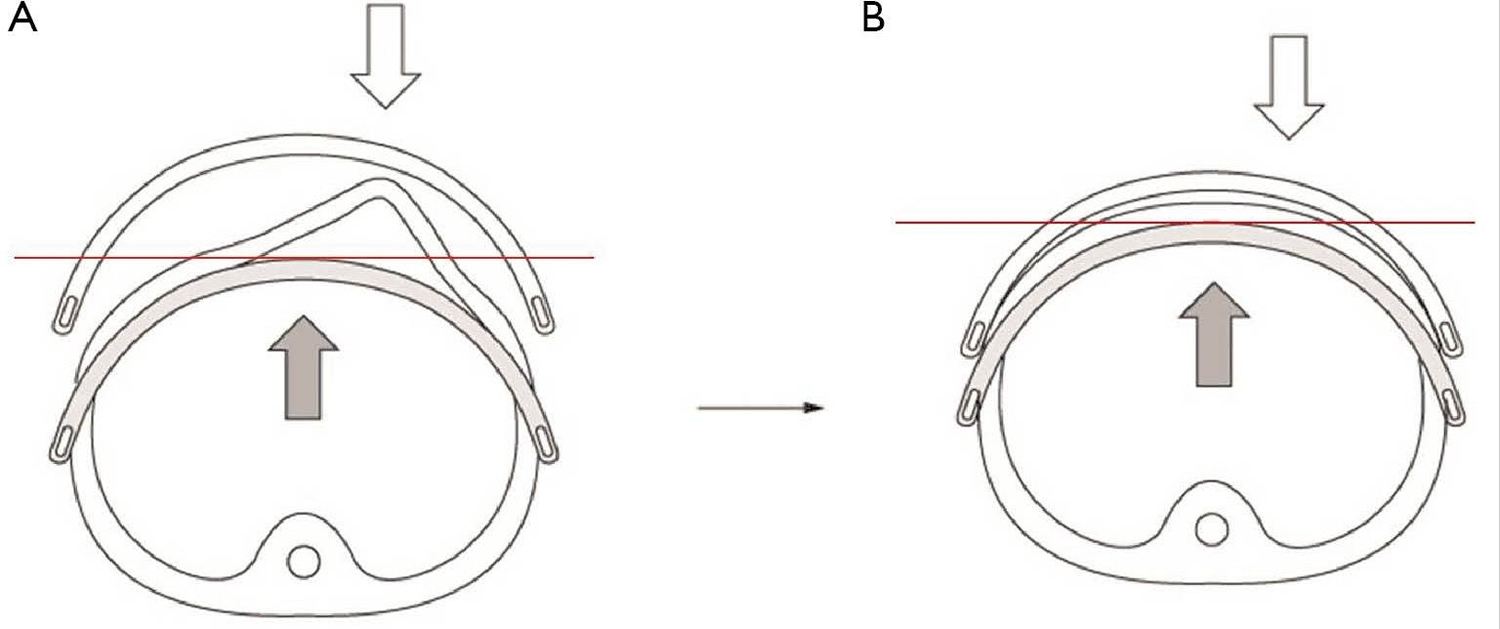
Figure 8. Repair of pectus carinatum/excavatum complex: press-molding the anterior chest wall by sandwiching between the external bar (white) and the internal bar (gray). (A) pre-repair; (B) post-repair.
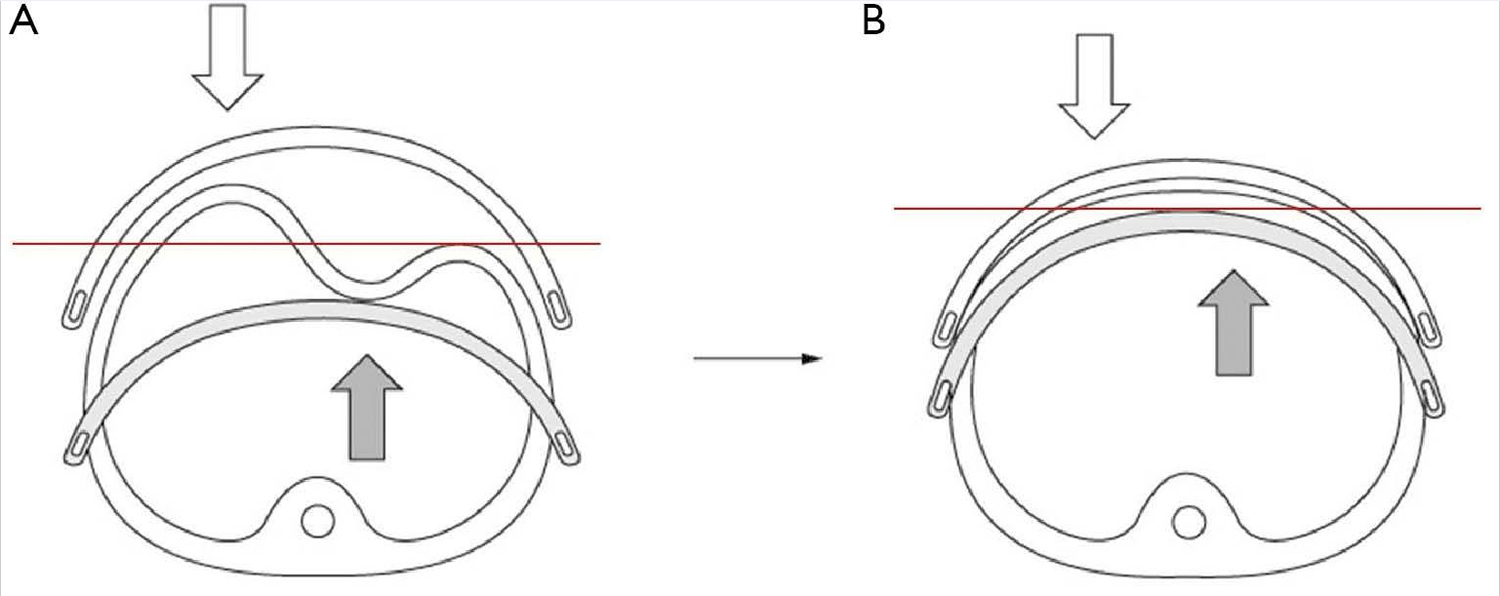
Figure 9. Comparison of the flare angles between the control group (without flare-buster) and the flare-buster group. The flare angle is defined as the angle between sternal line and flare line (the white bold lines). *, lower costal flare.
Pectus carinatum brace
Several non-surgical approaches have been proposed for pectus carinatum patients 13, 14 and during the mid 2000s, when non-operative approaches began to consolidate, major surgery was the only option.
Pectus carinatum brace comprises the following elements:
- A custom-fitted, expandable, low-profile, cushioned, ultra-light aluminum brace that is adjustable to any thoracic shape or size and has a locking system on one side to keep it in place;
- An adaptable compression plate to be placed against the chest wall protrusion.
- A pressure measuring device which can be docked to the brace’s compression plate and measures the pressure exerted to the patient in pounds per square inches (PSI) (Figure 11);
- A portable plate bender to curve the aluminum segments according to the patient’s initial chest size and shape and throughout the continuous re-shaping process.
The pectus carinatum brace corrects pectus carinatum gradually by using the continuous anterior-posterior compression to widen and remodel the entire chest and cartilages, which accommodate, grow and finally ossify in the correct position.
Two measurements were defined and must be collected:
- Pressure of correction (PC): an indirect parameter of the chest wall’s flexibility. It is defined as the pressure applied to the patient, in the most protruding area of the chest, needed to accomplish a proper shape of the thorax.
- Pressure of treatment (PT): is the pressure required to treat the patient. It should be measured before and after adjusting the pectus carinatum brace.
It is recommended that for adequate measurement of the pressure of correction (PC) two persons are involved. One person will be holding the pressure measuring device and pressing it onto the most protruding area of the thorax until the thorax seems leveled. The other person will observe the patient’s thorax from the side (profile) and will let the person holding the pressure measuring device know when the thorax seems leveled, so that the pressure of correction (PC) is measured.
Figure 10. Pectus carinatum brace (an aluminum brace with cushioned interior lining, side lock, adjustable shoulder straps and central compression plate)

Figure 11. Pectus carinatum brace pressure measuring device

Initial fitting of the pectus carinatum brace and patient training
Once the brace is fitted (http://www.asvide.com/article/view/6656), the pressure of treatment (PT) needs to be adjusted, never higher than 2.5 PSI. If higher, the brace will be loosened by using the different adjustment positions and the pressure of treatment (PT) will be measured again until satisfactory values are obtained.
When fitting the brace on the patient, ensure that the space between the sides of the chest and the brace allows one finger to fit. It is very important that enough space is available to allow for lateral expansion of the thorax as remodeling occurs. When enough pressure to correct the pectus carinatum is applied on the chest wall, lateral expansion of the thorax naturally occurs, as can be seen in.
Initially, patients will be classified into one of four groups following the treatment guidelines shown in Table 1.
Note: Although Table 1 is a general guideline, treatment can be customized for each patient considering individual tolerance, characteristic of the defect, skin status and age.
Table 1. Recommended use table of the Pectus carinatum brace (FMF® Dynamic Compressor System)
| Parameter | Group 1 | Group 2 | Group 3 | Group 4 |
|---|---|---|---|---|
| PC | 1–4 | 4–6 | 6–8 | >8 |
| PT | 2.5 | 2 | 1.5 | 1 |
| Use [hours/day] | 24 | 12–24 | 6–12 (day or night) | 3–6 (day or night) |
| Duration of treatment (approx.) | 2 months | 4 months | 8 months | 1–2 years |
Both pressures are measured in PSI. Values are estimates and for guidance only. DCS, Dynamic Compressor System; PC, pressure of correction; PT, pressure of treatment.
Note: Always check the PT during maximal inspiration. Values of 2.5 PSI or more must be avoided because skin lesions due to pressure necrosis can happen or the patient may not tolerate the device well enough, leading to non-compliance.
Group 1 and 2 patients are instructed to wear the FMF® DCS Pectus carinatum brace every day, overnight and as much as possible during the day, depending on their activities 3. They are only allowed to remove the device during sports and while having a shower/bath. We ensure that they understand that the more they wear the device, the faster they will correct the defect.
Patients belonging to group 3 and 4, will begin to wear the system less hours per day, at lower pressure of treatments (PTs), to indirectly increase the flexibility of the thoracic cage, enhance compliance and prevent skin lesions. We are careful to advise these patients about the complications of overusing the brace and the need to strictly follow medical indications.
The pressure of correction (PC) and the duration of treatment result very useful in helping patients understand what to expect throughout the treatment stages.
Patients with sensitive skin, age lower than 4 years old, stiff chests or reporting pain will have their brace set at pressure of treatments (PTs) ranging from 1 to 2.4 PSI.
- A pressure of treatment higher than that obtained at the last evaluation, can mean that the patient either has not worn the brace as indicated, or has grown up. This can be clarified by checking the patient’s records of height and weight and by verifying if the brace seems too tight. Be sure to keep these records updated.
- Pay attention to comfort to avoid non-compliance and complications:
- Different compression plates exist, adaptable to distinctive sternal protrusions, independently of their locations, sizes and shapes. Compression pads can also be adhered to the compression plate to cushion the defect, prevent skin lesions, increase pressure of treatment in girls with breast development, etc.;
- Patients with extremely sensitive skin can experience relief by using a tight cotton shirt below the brace, or by placing a DuoDerm® Extra Thin patch at the site of the defect for protection.
- Since the end of the correction phase is defined as the impression of full resolution of the deformity by the patient, the family and the interdisciplinary team several methods can be used to evaluate this. It is important to discuss which criteria will be used. Some examples are pre and post treatment photographs, a scoring system ranging from 1 to 10, etc.
Correction phase
The patient has to return for follow up monthly. During each visit, the pressure of treatment (PT) is measured with the brace setting as is, the skin status is evaluated, together with the habits of use of the brace and the practice of complementary activities. The pressure of correction (PC) is also measured and the brace is adjusted to set a new pressure of treatment (PT) and usage pattern as described in Table 1.
Once the patient’s pressure of correction (PC) lowers to the pressure of correction (PC) range of the previous group, he/she is re-classified and time of usage is adjusted accordingly.
The correction phase ends when the interdisciplinary team, patient, and/or family agree that the deformity has been fully repaired.
Weaning phase
Once the defect is reverted (pressure of correction equal to zero), the pectus carinatum brace is gradually withdrawn to avoid eventual partial recurrences. Pectus carinatum may return mildly, in approximately 10% of cured patients, particularly if they have been treated before pubertal growth spurts or in case they have cured very rapidly.
During the weaning phase, patients wear the brace as a “retainer” during the day or overnight (they generally prefer the latter), every day for the first month, every 2 days for the second month and every 3–4 days for the next months (range, 2–6 months).
The faster the patient gets cured, the longer the weaning phase should be. Pressure of treatment (PT) will remain fixed during the post-correction period. The weaning period is not contemplated in the calculation of the duration of treatment.
Follow-up phase
Provisory treatment interruption is indicated when the weaning period ends. Patients are controlled every 6 months until they are 18 years old. In adults, treatment finishes when the defect is corrected. Nonetheless, they are all instructed to return if any partial recurrence is observed so that it can be corrected with a few more months of treatment with the brace.
Physiotherapist
The role of physiotherapy is central to the non-surgical therapy of pectus carinatum. Daily physical therapy exercises can be indicated, to improve elongation, posture, etc. Swimming, playing wind instruments, inflating balloons and other similar respiratory exercises are indicated and encouraged as accessory activities to complement the non-operative treatment, especially to treat the costal flares.
- Park CH, Kim TH, Haam SJ, Lee S. Does overgrowth of costal cartilage cause pectus carinatum? A three-dimensional computed tomography evaluation of rib length and costal cartilage length in patients with asymmetric pectus carinatum. Interactive Cardiovascular and Thoracic Surgery. 2013;17(5):757-763. doi:10.1093/icvts/ivt321. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3805208/[↩][↩]
- Fokin AA, Steuerwald NM, Ahrens WA, Allen KE. Anatomical, histologic, and genetic characteristics of congenital chest wall deformities. Semin Thorac Cardiovasc Surg. 2009;21:44–57. https://www.ncbi.nlm.nih.gov/pubmed/19632563[↩]
- Martinez-Ferro M, Bellia Munzon G, Fraire C, et al. Non-surgical treatment of pectus carinatum with the FMF® Dynamic Compressor System. Journal of Visualized Surgery. 2016;2:57. doi:10.21037/jovs.2016.02.20. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5638266/[↩][↩][↩][↩][↩]
- Coelho Mde S, Guimaraes Pde S. Pectus carinatum. J Bras Pneumol. 2007;33:463–74. https://www.ncbi.nlm.nih.gov/pubmed/17982540[↩]
- Goretsky MJ, Kelly RE, Jr, Croitoru D, Nuss D. Chest wall anomalies: pectus excavatum and pectus carinatum. Adolesc Med Clin. 2004;15:455–71. https://www.ncbi.nlm.nih.gov/pubmed/15625987[↩]
- Pectus excavatum and pectus carinatum patients suffer from lower quality of life and impaired body image: a control group comparison of psychological characteristics prior to surgical correction. Steinmann C, Krille S, Mueller A, Weber P, Reingruber B, Martin A. Eur J Cardiothorac Surg. 2011 Nov; 40(5):1138-45. https://www.ncbi.nlm.nih.gov/pubmed/21440452/[↩]
- Goretsky MJ, Kelly RE, Jr, Croitoru D, Nuss D. Chest wall anomalies: pectus excavatum and pectus carinatum. Adolesc Med Clin. 2004;15:455–71 https://www.ncbi.nlm.nih.gov/pubmed/15625987[↩]
- Robicsek F, Watts LT. Pectus carinatum. Thorac Surg Clin. 2010;20:563–74. https://www.ncbi.nlm.nih.gov/pubmed/20974441[↩]
- Nakaoka T, Uemura S, Yano T, Nakagawa Y, Tanimoto T, Suehiro S. Does overgrowth of costal cartilage cause pectus excavatum? A study on the lengths of ribs and costal cartilages in asymmetric patients. J Pediatr Surg. 2009;44:1333–6. https://www.ncbi.nlm.nih.gov/pubmed/19573657[↩]
- Abramson H, D’Agostino J, Wuscovi S. A 5-year experience with a minimally invasive technique for pectus carinatum repair. J Pediatr Surg 2009;44:118-23; discussion 123-4. 10.1016/j.jpedsurg.2008.10.020 https://www.ncbi.nlm.nih.gov/pubmed/19159728[↩]
- Park HJ, Kim KS. The sandwich technique for repair of pectus carinatum and excavatum/carinatum complex. Annals of Cardiothoracic Surgery. 2016;5(5):434-439. doi:10.21037/acs.2016.08.04. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5056943/[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Park HJ, Kim KS, Lee S, et al. A next-generation pectus excavatum repair technique: new devices make a difference. Ann Thorac Surg 2015;99:455-61. 10.1016/j.athoracsur.2014.08.026 https://www.ncbi.nlm.nih.gov/pubmed/25488621[↩]
- Stephenson JT, Du Bois J. Compressive orthotic bracing in the treatment of pectus carinatum: the use of radiographic markers to predict success. J Pediatr Surg 2008;43:1776-80. 10.1016/j.jpedsurg.2008.03.049 https://www.ncbi.nlm.nih.gov/pubmed/18926206[↩]
- Lee SY, Lee SJ, Jeon CW, et al. Effect of the compressive brace in pectus carinatum. Eur J Cardiothorac Surg 2008;34:146-9. 10.1016/j.ejcts.2008.04.012 https://www.ncbi.nlm.nih.gov/pubmed/18479931[↩]





{kind=link}