
Contents
- What is pelvic pain
- Pelvic pain in women
- Pelvic pain during pregnancy
- Pelvic pain in men
What is pelvic pain
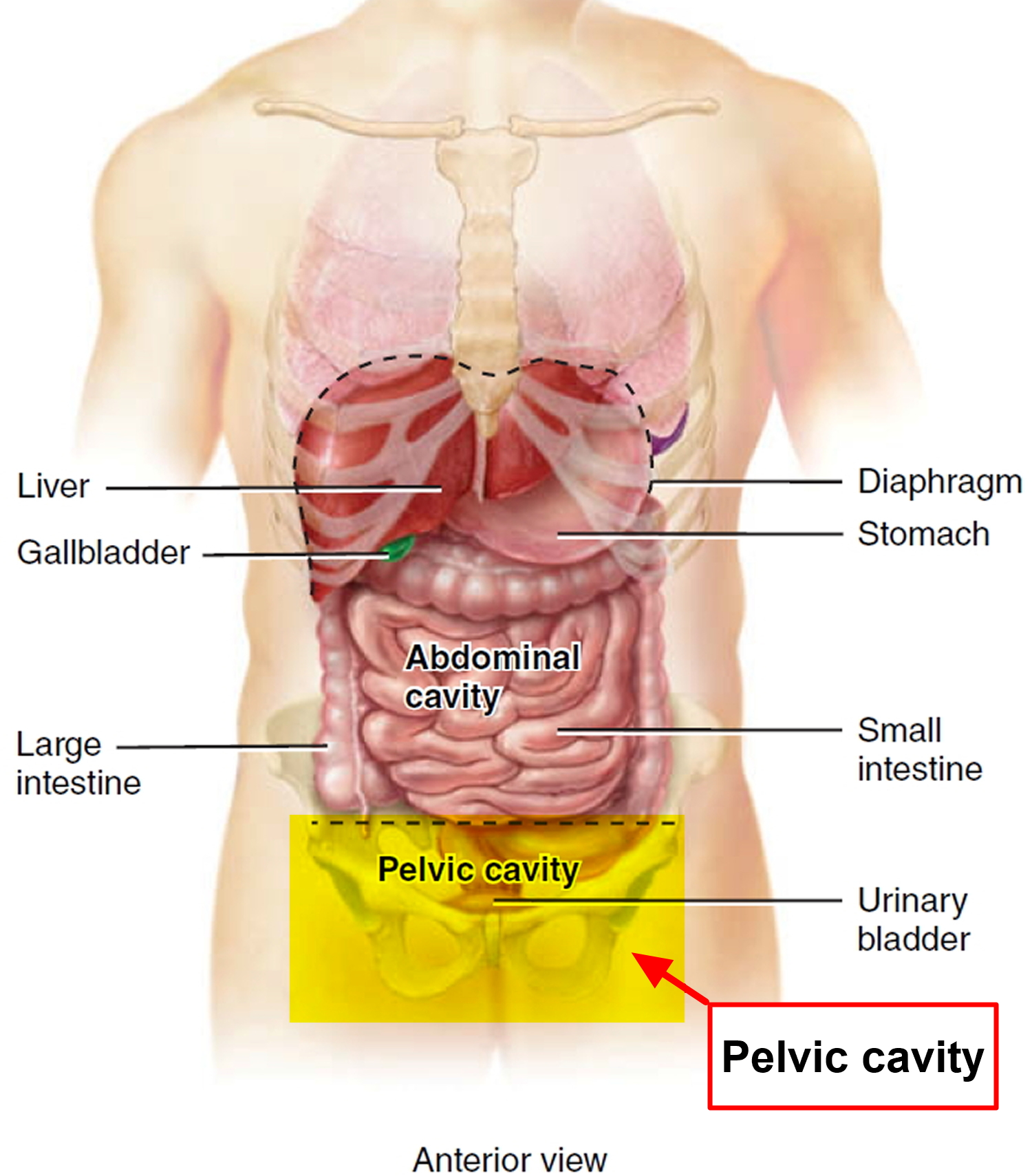
Pelvic pain is a general term used to describe pain that occurs mostly or only in the region below a woman’s belly button. The pelvic region includes the lower stomach, lower back, buttocks, and genital area 1). Depending on its source, pelvic pain can be dull or sharp; it might be constant or off and on (intermittent); and it might be mild, moderate or severe. Pelvic pain can sometimes radiate to your lower back, buttocks or thighs. Sometimes, you might notice pelvic pain only at certain times, such as when you urinate or during sexual activity.
Pelvic pain can occur suddenly, sharply and briefly (acute) or over the long term (chronic). Chronic pelvic pain refers to any constant or intermittent pelvic pain that has been present for six months or more.
Several types of diseases and conditions can cause acute pelvic pain. Chronic pelvic pain can also result from more than one condition.
Pelvic pain can arise from your digestive, reproductive or urinary system. Recently, doctors have recognized that some pelvic pain, particularly chronic pelvic pain, can also arise from muscles and connective tissue (ligaments) in the structures of the pelvic floor. Occasionally, pelvic pain might be caused by irritation of nerves in the pelvis.
Figure 1. Pelvic cavity
Pelvic pain in women
Pelvic pain is a common reason why women seek medical care 2). One study estimated that up to 39% of reproductive-aged women who presented to their primary care physician had symptoms related to pelvic pain, and one in seven women has acute or chronic pelvic pain at some point 3). Severe pain can interfere with daily living and quality of life. Pelvic pain is chronic if it lasts for more than 6 months and affects a woman’s quality of life 4).
Researchers are not sure exactly how many women in the United States have chronic pelvic pain.
Because pelvic pain is often linked to other disorders, such as endometriosis or vulvodynia, chronic pelvic pain may be misdiagnosed as another condition, making it difficult to estimate reliable prevalence rates for pelvic pain 5). According to one study, about 15% of women of childbearing age in the United States reported having pelvic pain that lasted at least 6 months 6). Worldwide, the rates of chronic pelvic pain for women of childbearing age range from 14% to 32% 7). Between 13% and 32% of these women have pain that is severe enough to cause them to miss work 8).
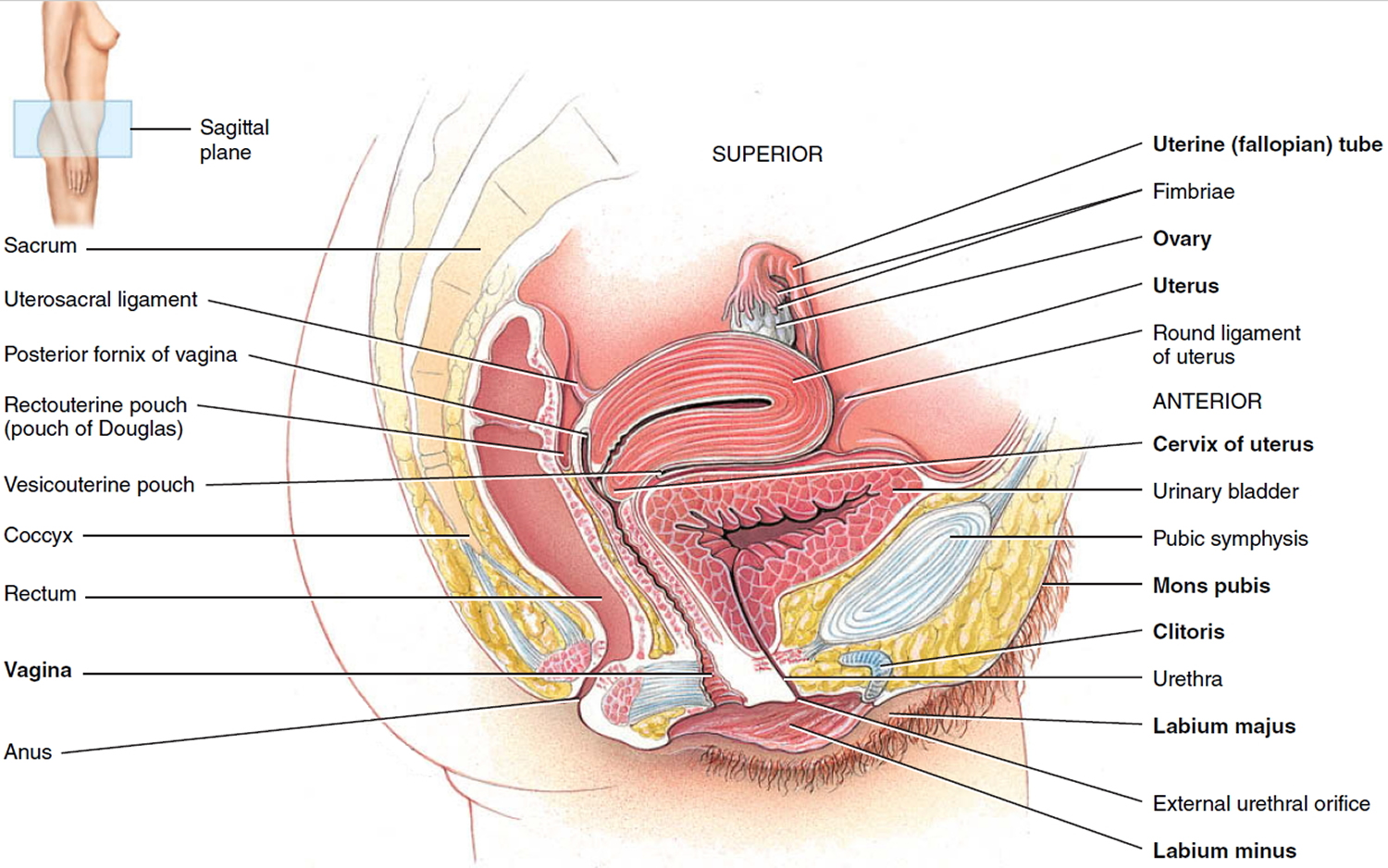
Figure 2. Female reproductive system
Pelvic pain symptoms
Although pain is the core symptom of pelvic pain, the specifics of that pain and other symptoms vary from woman to woman. Pelvic pain can be severe enough that it interferes with normal activities, such as going to work, exercising, or having sex.
Women describe pelvic pain in many ways. Pelvic pain can be steady, or it can come and go. It can be a sharp and stabbing pain felt in a specific spot, or a dull pain that is spread out. Some women have pain that occurs only during their menstrual periods. Some women feel pain when they need to use the bathroom, and some feel pain when lifting something heavy. Some women have pain in the vulva (the external genitals), which is called vulvodynia, during sex or when inserting a tampon 9).
Pelvic pain causes
There are many possible causes of pelvic pain and it may be difficult to figure out the specific cause or causes 10). A woman’s pain may result from multiple causes occurring all at the same time. And a woman with one chronic pain condition is at increased risk for other types of chronic pain.
In many cases, pelvic pain indicates a problem with one or more of the organs in the pelvic area, such as the uterus, vagina, intestine, or bladder. Problems may include infection, inflammation, or conditions such as endometriosis.
The intensity of a woman’s pelvic pain may not relate to the severity of the problem or condition causing the pain. For example, a woman with only small areas of endometriosis may experience intense pain.
The following health problems can cause or contribute to pelvic pain:
Table 1. Conditions Causing Acute Pelvic Pain in Different Populations
| Patient category | Common diagnoses | Less common diagnoses | Rare diagnoses |
|---|---|---|---|
Reproductive age (not pregnant) | Endometriosis (ruptured endometrioma) | Adenomyosis | Endosalpingiosis |
Idiopathic (no cause identified) | Dysmenorrhea | Round ligament mass (lipoma, teratoma) | |
Ovarian cyst, ruptured | Endometritis (postprocedure) | Transverse vaginal septum | |
Ovarian torsion | Imperforate hymen | ||
PID, tubo-ovarian abscess | Intrauterine device perforation | ||
Leiomyoma (degenerating) | |||
Mittelschmerz | |||
Reproductive age (pregnancy related) | Corpus luteum cyst | Leiomyoma (degenerating) | Incarcerated gravid uterus |
Ectopic pregnancy | Pubic symphysis separation | Ovarian vein thrombosis | |
Endometritis (postpartum) | Subchorionic hemorrhage | PID (rare after first trimester) | |
Normal labor | Uterine rupture | ||
Ovarian torsion | |||
PID (first trimester) | |||
Placental abruption | |||
Preterm labor | |||
Spontaneous abortion | |||
Reproductive age (undergoing fertility treatment) | Ectopic pregnancy | — | Heterotopic pregnancy |
Ovarian follicular cyst | |||
Ovarian hyperstimulation syndrome | |||
Ovarian torsion | |||
Postmenopausal | Malignancy | Ischemic colitis | Endometriosis |
PID, tubo-ovarian abscess | |||
Retained intrauterine device | |||
All groups | Appendicitis | Bowel obstruction | Mesenteric adenitis |
Diverticulitis | Inguinal hernia | ||
Inflammatory bowel disease | Interstitial cystitis | ||
Irritable bowel syndrome | Pelvic adhesive disease (postoperative scarring) | ||
Musculoskeletal (abdominal wall) pain | Perirectal abscess | ||
Urinary tract infection | Urethral diverticulum | ||
Urolithiasis | Urinary retention | ||
PID = pelvic inflammatory disease.
Gynecologic Causes
Pelvic Adhesions
Adhesions are bands of scar tissue that form between internal tissues and organs 12). They can form as a result of surgery or infections, such as pelvic inflammatory disease or by pelvic or abdominal surgery, or by endometriosis. There is disagreement about whether adhesions can cause pelvic pain. It has been proposed that pelvic pain may occur when adhesions prevent normal movement of internal organs, such as the bowel 13). Pelvic adhesions can be difficult to diagnose, but in some cases the uterus and ovaries feel bound together on pelvic examination. A definitive diagnosis of pelvic adhesions is usually made during surgical exploration, frequently via laparoscopy. Symptoms from pelvic adhesions include generalized pelvic discomfort or localized pain. Surgery to cut bands of scar tissue can relieve pain. However, sometimes the adhesions re-form.
Endometriosis
Endometriosis occurs when tissues that normally grow inside the uterus grow somewhere else in the body, usually in other parts of the pelvis, such as on the outside of the uterus, ovaries, or fallopian tubes. The two most common symptoms of endometriosis are pelvic pain and infertility. Endometriosis may cause pelvic pain, especially during menstruation. Hormones of the menstrual cycle cause the endometriosis to bleed each month. This can be painful and result in the formation of pelvic adhesions, also known as scar tissue. Blood trapped in the ovary can build up into a cyst. This is called an endometrioma.
Uterine fibroids
Uterine fibroids consist of an overgrowth of muscle cells within the wall of the uterus. These noncancerous tumors may cause heavy, irregular, or painful periods and local pressure symptoms, including frequent urination, trouble defecating, and lower back pain.
Vulvodynia
Vulvodynia involves pain or discomfort of the vulva (the external female genitalia)), especially during intercourse. The pain may range from sharp pain to burning to itching. The cause is unknown. It’s thought that the nerves, muscles and tissues in the area are inflamed, so treatment is focused on addressing these factors. Women with this condition may find it painful to insert a tampon, have sexual intercourse or even wear tight pants. Symptoms include burning, stinging, stabbing, irritation and rawness. The pain may be constant or intermittent, localized or diffuse.
Although the vulvar pain is outside the pelvis, health care providers who see patients with pelvic pain may also care for patients with this disorder.
Other gynecologic causes of pelvic pain in women
- Adenomyosis
- Ectopic pregnancy (or other pregnancy-related conditions). An ectopic pregnancy is when a fertilized egg implants itself outside of the womb, usually in one of the fallopian tubes. Unfortunately, it’s not possible to save the pregnancy. It usually has to be removed using medicine or an operation.
- Menstrual cramps (dysmenorrhea)
- Miscarriage (before the 20th week) or intrauterine fetal death
- Mittelschmerz (pain associated with ovulation)
- Ovarian cancer
- Ovarian cysts
- Pelvic inflammatory disease (PID) — infection of the female reproductive organs
Non-Gynecologic Causes
Non-gynecologic problems can also cause pelvic pain. The most common are:
Interstitial cystitis/painful bladder syndrome
Interstitial cystitis (painful bladder syndrome) is associated with pain in the region of the bladder as well as the need to urinate frequently and urgently. This pain may be a burning or sharp pain in the bladder or at the opening where urine leaves the body (urethra), and it is often relieved by emptying the bladder 14).
Irritable bowel syndrome
Irritable bowel syndrome (IBS) is a digestive problem that can cause pelvic pain, bloating, constipation, or diarrhea. Researchers have yet to find a specific cause for irritable bowel syndrome but stress or certain foods can trigger symptoms in some people 15).
Pelvic floor disorders
Pelvic floor disorders occur when the muscles and connective tissues that hold the pelvic organs in place weaken or are injured, such as may occur during childbirth. These organs include the uterus, bladder, and rectum. Pelvic floor disorders can cause discomfort as well as functional problems, such as the uncontrolled loss of urine (urinary incontinence) or stool (fecal incontinence). With pelvic floor disorders, pain may also be caused by spasms or an increase in pelvic floor muscle tone.
Musculoskeletal Causes
Musculoskeletal causes of pelvic pain are very common but are often overlooked. The muscles, joints and nerves in the pelvis can be injured just like any other part of your body. For instance, tissues can be overstretched, torn or cut in childbirth or surgery; muscles can weaken or tighten from disuse and injury; and habitual postures and movements can slowly stretch or compress structures in the pelvis, leading to pain and dysfunction. The pelvic muscles, joints and nerves may be the sole cause of pain or just a piece of the problem.
Chronic pain can be created by spasms of the muscles that line the pelvis, also known as the pelvic floor muscles. This “sling” of muscles, along with connective tissue called fascia, lift and support the pelvic organs including the bladder, uterus and rectum. Spasms in these muscles — known as pelvic floor tension myalgia or levator ani syndrome — may cause pain locally. Tight bands of muscle, known as trigger points, may be tender to the touch, and they may refer pain to other areas of the pelvis, abdomen and low back.
A thorough examination of the abdomen and pelvis can uncover these sources of pain, which can be treated with physical therapy and biofeedback.
Depression and Anxiety
Many women with chronic pain suffer from anxiety, depression, or both, which worsens pain. Recurring or chronic pain can cause some women to feel depressed. These feelings are normal. In other cases, pelvic pain can be a symptom of depression or anxiety. It’s essential to address depression or anxiety with therapy and medications as needed.
Other causes of pelvic pain in women
- Appendicitis
- Colon cancer
- Constipation
- Crohn’s disease (a type of inflammatory bowel disease)
- Diverticulitis
- Fibromyalgia
- Inguinal hernia
- Intestinal obstruction
- Kidney stones
- Past physical or sexual abuse
- Pelvic floor muscle spasms
- Ulcerative colitis (a type of inflammatory bowel disease)
- Urinary tract infection (UTI)
Sudden, unexpected pelvic pain
Pelvic pain that comes on suddenly for the first time is called acute pelvic pain.
See your doctor immediately if you have acute pelvic pain. They’ll be able to investigate the cause and arrange any necessary treatment.
Common causes of acute pelvic pain
The most common causes of acute pelvic pain in women who aren’t pregnant are:
- an ovarian cyst – a fluid-filled sac that develops on an ovary and causes pelvic pain when it bursts or becomes twisted
- acute pelvic inflammatory disease – a bacterial infection of the womb, fallopian tubes or ovaries, which often follows a chlamydia or gonorrhea infection and needs immediate treatment with antibiotics
- appendicitis – a painful swelling of the appendix (a finger-like pouch connected to the large intestine) which usually causes pain on the lower right-hand side of your abdomen (tummy)
- peritonitis – inflammation of the peritoneum (the thin layer of tissue that lines the inside of the abdomen); it causes sudden abdominal pain that gradually becomes more severe and requires immediate medical treatment
- a urinary tract infection – you’ll probably also have pain or a burning sensation when you urinate, and you may need to urinate more often
- constipation or bowel spasm – this may be brought on by changes in diet, medication, irritable bowel syndrome or, in rare cases, a bowel obstruction
Less common reasons for acute pelvic pain
Less common causes of acute pelvic pain include:
- a pelvic abscess – a collection of pus between the womb and vagina that needs urgent treatment in hospital
- endometriosis – a long-term condition where small pieces of womb lining are found outside the womb, such as on the ovaries, leading to painful periods
Chronic pelvic pain
If you’ve had pelvic pain for 6 months or more that either comes and goes or is continuous, it’s known as chronic pelvic pain.
Chronic pelvic pain is more intense than ordinary period pain and lasts longer. It affects around 1 in 6 women.
See your doctor if you have chronic pelvic pain. They’ll investigate the cause and arrange any necessary treatment.
Common causes of chronic pelvic pain
The most common causes of chronic pelvic pain are:
- endometriosis
- chronic pelvic inflammatory disease – a bacterial infection of the womb, fallopian tubes or ovaries, which often follows a chlamydia or gonorrhea infection and needs immediate treatment with antibiotics
- irritable bowel syndrome – a common long-term condition of the digestive system that can cause stomach cramps, bloating, diarrhea and constipation
Less common reasons for chronic pelvic pain
Less common causes of chronic pelvic pain include:
- recurrent ovarian cysts – fluid or blood-filled sacs that develop on the ovaries
- a recurrent urinary tract infection
- lower back pain
- prolapse of the womb – where the womb slips down from its normal position and usually causes a “dragging” pain
- adenomyosis – endometriosis that affects the muscle of the womb, causing painful, heavy periods
- uterine fibroids – non-cancerous tumors that grow in or around the womb; fibroids can be painful if they twist or deteriorate, but uncomplicated fibroids aren’t usually painful
- chronic interstitial cystitis – long-term inflammation of the bladder
- inflammatory bowel disease – a term used to describe two chronic conditions, ulcerative colitis and Crohn’s disease, which affect the gut
- a hernia – where an internal part of the body pushes through a weakness in the surrounding muscle or tissue wall
- trapped or damaged nerves in the pelvic area – these may cause sharp, stabbing or aching pain in a specific area, which often gets worse with certain movements
Can there be more than one reason for your pelvic pain?
Yes. Studies have found a good deal of overlap among pain conditions 16). For instance, a woman may have endometriosis, irritable bowel syndrome (IBS) and depression at the same time—each of which may contribute to the overall pain she feels.
Having more than one pain condition can complicate diagnosis and treatment. To be effective, treatment needs to address all the conditions that are contributing to a woman’s pain.
Can pelvic pain affect my ability to become pregnant?
Some pelvic conditions that are associated with pain also are associated with difficulty getting pregnant.
These include:
- Endometriosis. Up to 30% to 50% of women with endometriosis are not able to get pregnant, making this condition one of the top three causes of female infertility 17).
- Pelvic adhesions. Adhesions that form on the ovaries, fallopian tubes, or uterus can make it difficult or impossible to get pregnant 18).
- Uterine fibroids. Most women with fibroids do not have problems with fertility and can get pregnant. If a woman’s fibroid is located in the uterine cavity, she may face an increased risk of early pregnancy loss. Some women with fibroids may not be able to get pregnant naturally, but advances in treatments for infertility may help some of them get pregnant.
Some treatments for pelvic pain also can affect a woman’s ability to get pregnant. For example, hormonal birth control commonly is used to treat endometriosis. Hysterectomy, which is surgery to remove a woman’s uterus, may be an option for women who are not helped by other treatments, but it makes pregnancy impossible. However, a woman may still be able to become a mother through other means, such as a surrogate carrier.
Pelvic pain in women diagnosis
To find out the cause of a woman’s pain, her health care provider will 19):
- Ask questions about the woman’s pain and health history. How a woman describes her pain can help her health care provider figure out the pain type and what might be causing it.
- Perform a physical exam. The health care provider will examine the abdomen and pelvis, and check the woman’s organs, muscles, and tissues in the pelvic region for tenderness or abnormalities that suggest a pain disorder.
The information the doctor gathers from the questions and physical exam will help the doctor decide whether additional tests or procedures are needed to help diagnose the cause of the pelvic pain.
These tests or procedures may include:
- Lab tests, such as blood work or a urine test
- Pelvic ultrasound, a procedure that uses sound waves to look at organs and structures inside the pelvic region 20)
- Pelvic laparoscopy, a minor surgery in which the doctor inserts a viewing instrument called a laparoscope through a small cut in the skin below the belly button to look inside the pelvis 21)
- Pelvic MRI (magnetic resonance imaging) scan, an imaging test that uses powerful magnets and radio waves to create pictures of the pelvis 22)
- Cystoscopy, looking into the bladder by inserting a viewing instrument 23)
- Colonoscopy, looking into the bowel by inserting a viewing instrument 24)
Finding the cause of pelvic pain can be challenging and can take time. Some women must check with more than one doctor or with a specialist to get help for their pain. Sometimes, the cause of the pain is not found. But failure to locate the cause does not mean that the pain a woman feels is not real or that it cannot be treated. Understanding what triggers the pain also can be helpful.
Table 2. Historical Findings and Suggested Diagnoses and Subsequent Testing in Patients with Acute Pelvic Pain
| Finding | Suggested diagnoses | Further diagnostic considerations | |
|---|---|---|---|
History of intrauterine instrumentation, multiple cesarean deliveries, or other uterine surgeries | Adenomyosis (endometrial tissue grown into the uterine wall) | Magnetic resonance imaging | |
Pelvic adhesions | Consider nonurgent referral to gynecologist or general surgeon in absence of other findings | ||
Menstrual abnormalities | |||
Amenorrhea | Imperforate hymen | Pelvic examination | |
Transverse vaginal septum | Pelvic ultrasonography | ||
Dysmenorrhea | Endometriosis, ovarian cyst | Pelvic ultrasonography (to assess for ovarian cyst) | |
Nausea and vomiting | Appendicitis, ovarian torsion | If appendicitis is more likely: proceed with contrast CT | |
If ovarian torsion is more likely: proceed with pelvic ultrasonography with Doppler flow study | |||
Early urgent referral for surgical evaluation and treatment is recommended | |||
Pain symptoms | |||
Bilateral pain, particularly if associated with mucopurulent vaginal discharge | Pelvic inflammatory disease | Testing for sexually transmitted infections | |
Complete blood count to test for leukocytosis or left shift | |||
Dull, unilateral adnexal pain that is constant or intermittent | Ovarian torsion | Presence of risk factors (nausea, vomiting, pregnancy) | |
Pelvic ultrasonography with Doppler flow study | |||
Consider urgent referral for surgical evaluation and treatment | |||
Right lower quadrant pain | Acute appendicitis | Complete blood count demonstrating leukocytosis | |
Contrast CT of the abdomen and pelvis | |||
Ectopic pregnancy | Qualitative urine β-hCG can detect a pregnancy at four weeks’ gestation | ||
Quantitative serum β-hCG can determine if pregnancy is above the discriminatory level such that an intrauterine pregnancy should be visible on pelvic ultrasonography to rule out ectopic gestation | |||
Blood type to determine Rh status; if bleeding and pregnant, will need Rho(D) immune globulin (RhoGam) | |||
Pelvic ultrasonography | |||
Ovarian torsion | Pelvic ultrasonography with Doppler flow study | ||
Sexually active; pregnancy possible | Ectopic pregnancy, spontaneous abortion | Qualitative urine β-hCG can detect a pregnancy at four weeks’ gestation | |
Quantitative serum β-hCG can determine if pregnancy is above the discriminatory level such that an intrauterine pregnancy should be visible on pelvic ultrasonography to rule out ectopic gestation | |||
Blood type to determine Rh status; if bleeding and pregnant, will need Rho(D) immune globulin | |||
Pelvic ultrasonography | |||
Urinary symptoms | |||
Dysuria | Urinary tract infection | Urinalysis demonstrating white blood cells, bacteria, leukocyte esterase, or nitrites | |
Gross hematuria | Urolithiasis | Abdominal ultrasonography | |
β-hCG = beta human chorionic gonadotropin; CT = computed tomography.
Table 3. Physical Examination Findings and Suggested Diagnoses and Subsequent Testing in Patients with Acute Pelvic Pain
| Finding | Suggested diagnoses | Further diagnostic considerations |
|---|---|---|
Carnett sign (increased pain to palpation when the abdominal wall musculature is voluntarily contracted) | Musculoskeletal (abdominal wall) pain | No further testing needed in the absence of other historical or physical examination findings that might suggest intrapelvic or intra-abdominal conditions |
Cervical motion tenderness | Pelvic inflammatory disease | Consider testing for sexually transmitted infections |
Fever | Appendicitis | Ultrasonography or contrast CT of the abdomen and pelvis |
Complete blood count demonstrating leukocytosis | ||
Pelvic inflammatory disease | Consider testing for sexually transmitted infections | |
Pyelonephritis | Urinalysis demonstrating evidence of urinary tract infection (white blood cells, bacteria, leukocyte esterase, or nitrites) | |
Complete blood count demonstrating leukocytosis, left shift | ||
Tubo-ovarian abscess | Pelvic ultrasonography | |
Complete blood count demonstrating leukocytosis, left shift | ||
Pelvic mass | Ectopic pregnancy | See Table 2 |
Fibroid uterus | Pelvic ultrasonography | |
Ovarian cancer | Pelvic ultrasonography | |
Consider CT of the chest, abdomen, and pelvis if metastatic disease is suspected | ||
Ovarian cyst | Pelvic ultrasonography | |
Tubo-ovarian abscess | Pelvic ultrasonography | |
Rovsing sign (palpation in the left lower quadrant causes pain in the right lower quadrant) | Appendicitis | Contrast CT of the abdomen and pelvis |
Complete blood count demonstrating leukocytosis | ||
Tachycardia, hypotension | Ruptured ectopic pregnancy | Consider urgent referral to facility with immediate surgical |
Ruptured hemorrhagic cyst capability |
CT = computed tomography.
Pelvic pain in women treatment
Treatment depends on the cause of pelvic pain, how intense the pain is, and how often the pain occurs. No single treatment approach has been shown to be better than another in all cases 27).
Some treatment options include:
- Medicines. Many types of medicine are used to treat pelvic pain. These include pain relievers that are swallowed or injected, muscle relaxants, and antidepressants.
- Hormonal treatment. Hormones can help pain related to endometriosis and menstruation 28). These include hormones that are swallowed, injected, or placed in the uterus, such as birth control pills, gonadotropin-releasing hormone injections, or progestin-releasing intrauterine devices. Hormonal treatment for pelvic pain is not the same as hormone therapy that is sometimes used to treat the symptoms of menopause.
- Lifestyle changes. Some women’s pain is helped by changes in diet, improved posture, and regular physical activity.
- Nutrition and supplements — for instance, a diet rich in fruits, vegetables and grains is important. Avoiding foods that can increase inflammation and increasing foods that decrease inflammation can be useful.
- Physical therapy. Some types of pain, such as muscle and connective tissue pain, respond well to physical therapy. This type of therapy might involve massage, stretching, strengthening, or learning to relax or control pelvic muscles 29).
- Surgery. Some women may need surgery to remove adhesions 30), fibroids, and/or endometriosis. In some cases, the surgery might also reduce or relieve pelvic pain. Some women may have surgery to cut or destroy nerves to interrupt pain signals,1 but such pain surgeries often are not successful. Depending on the cause of the pain, a woman’s health care provider might recommend a hysterectomy, surgery to remove a woman’s uterus, to help relieve or reduce pelvic pain.
- Counseling. Counseling or “talk therapy” may help treat pain. In fact, talk therapy, when combined with medical treatment, appears to work better for improving some symptoms than does medical treatment alone 31).
Finding a treatment that works can take time. Some women want to try alternative therapies to relieve their pain. Learning healthy ways to cope with pain is an important aspect of any treatment approach.
Chronic pelvic pain
Chronic pelvic pain has many possible causes, and the symptoms may vary with what’s causing the pain.
Chronic pain is very difficult to deal with. It’s important to set reasonable goals and develop a treatment plan that addresses your unique health needs. It’s also important to attend to your emotional health, and to focus on what brings joy and meaning to your life.
Physical Therapy
Some studies show physical therapy helps 60 percent of women with chronic pelvic pain and levator ani syndrome. It helps to align bone or muscular imbalances, decrease abnormal muscle tension and soft tissue, and strengthen your core muscles to prevent further injury. A physical therapist can also help identify other factors that may contribute to your pain, such as poor posture, positioning and habits.
During a visit, your physical therapist will conduct a thorough musculoskeletal examination, identifying sources of pain and dysfunction. Sometimes alignment of the feet, hips, and back will affect the posture of the pelvis and perpetuate the pain cycle. A woman who has had chronic pelvic pain long-term may notice she has symptoms in other areas of her body. Patients may notice changes in the muscles, skin and tissue of the pelvis, back and abdomen.
Your physical therapist will examine the muscles of the pelvic floor as well as the abdomen, thighs and back. The therapist will work with you to develop a treatment plan to address your specific issues and goals.
Physical therapy techniques for disorders of the joints and soft tissues of the pelvis may include education, internal and external myofascial release, manual therapy, therapeutic exercise, and treatments such as electrical stimulation or biofeedback. You may also use tools for self treatment at home, such as dilators and a product called Crystal Wand. A home program is also a vital component of physical therapy, maintaining and improving the musculoskeletal changes doctors make in the clinic.
Pelvic pain during pregnancy
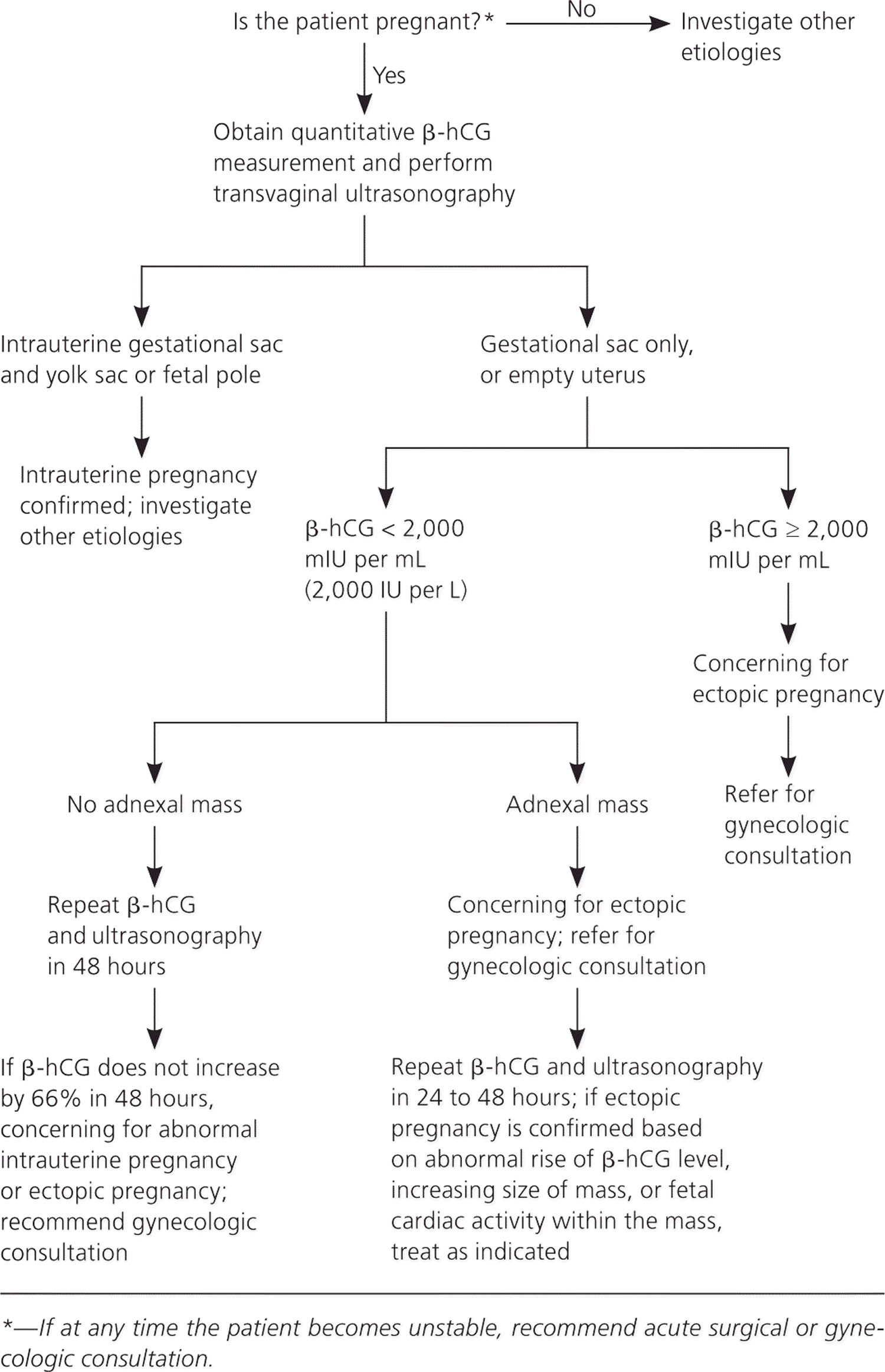
In early pregnancy, the most important consideration is to identify the location of the gestation to exclude ectopic pregnancy. Transvaginal ultrasonography is the imaging modality of choice, but results must be correlated with beta human chorionic gonadotropin (β-hCG) levels and, in particular, the discriminatory level (the β-hCG level at which the gestation should be visible on ultrasonography) 32). Figure 3 provides an algorithm for the evaluation and follow-up of patients with a positive β-hCG level and pelvic pain 33).
An ectopic pregnancy is when a fertilized egg implants itself outside of the womb, usually in one of the fallopian tubes. The fallopian tubes are the tubes connecting the ovaries to the womb. If an egg gets stuck in them, it won’t develop into a baby and your health may be at risk if the pregnancy continues.
Unfortunately, it’s not possible to save the pregnancy. It usually has to be removed using medicine or an operation.
What can cause an ectopic pregnancy?
In many cases, it’s not clear why a woman has an ectopic pregnancy. Sometimes it happens when there’s a problem with the fallopian tubes, such as them being narrow or blocked.
The following are all associated with an increased risk of ectopic pregnancy:
- pelvic inflammatory disease (PID) – inflammation of the female reproductive system, usually caused by a sexually transmitted infection (STI)
- previous ectopic pregnancy – the risk of having another ectopic pregnancy is around 10%
- previous surgery on your fallopian tubes – such as an unsuccessful female sterilisation procedure
- fertility treatment, such as IVF – taking medication to stimulate ovulation (the release of an egg) can increase the risk of ectopic pregnancy
- becoming pregnant while using an intrauterine device (IUD) or intrauterine system (IUS) for contraception – it’s rare to get pregnant while using these, but
- if you do you’re more likely to have an ectopic pregnancy
- smoking
- increasing age – the risk is highest for pregnant women aged 35 to 40
You can’t always prevent an ectopic pregnancy, but you can reduce your risk by using a condom when not trying for a baby to protect yourself against STIs, and by stopping smoking if you smoke.
Figure 3. Ultrasonography and Laboratory Evaluation of a Patient in Early Pregnancy with Acute Pelvic Pain
Ectopic pregnancy symptoms
An ectopic pregnancy doesn’t always cause symptoms and may only be detected during a routine pregnancy scan.
If you do have symptoms, they tend to develop between the 4th and 12th week of pregnancy.
Symptoms can include a combination of:
- a missed period and other signs of pregnancy
- a positive pregnancy test
- tummy pain low down on one side
- vaginal bleeding or a brown watery discharge
- pain in the tip of your shoulder
- discomfort when peeing or pooing
But these symptoms aren’t necessarily a sign of a serious problem. They can sometimes be caused by other problems, such as a stomach bug.
Vaginal bleeding
Vaginal bleeding tends to be a bit different to your regular period. It often starts and stops, and may be watery and dark brown in colour.
Some women mistake this bleeding for a regular period and don’t realize they’re pregnant.
Vaginal bleeding during pregnancy is relatively common and isn’t necessarily a sign of a serious problem, but you should seek medical advice if you experience it.
Tummy pain
You may experience tummy pain, typically low down on one side. It can develop suddenly or gradually, and may be persistent or come and go.
Tummy pain can have lots of causes, including stomach bugs and trapped wind, so it doesn’t necessarily mean you have an ectopic pregnancy.
But you should get medical advice if you have it and think you might be pregnant.
Shoulder tip pain
Shoulder tip pain is an unusual pain felt where your shoulder ends and your arm begins.
It’s not known exactly why it occurs, but it can be a sign of an ectopic pregnancy causing some internal bleeding, so you should get medical advice right away if you experience it.
Discomfort when going to the toilet
You may experience pain when going for a pee or poo. You may also have diarrhea.
Some changes to your normal bladder and bowel patterns are normal during pregnancy, and these symptoms can be caused by urinary tract infections and stomach bugs.
But it’s still a good idea to seek medical advice if you experience these symptoms and think you might be pregnant.
Symptoms of a ruptured ectopic pregnancy
In a few cases, an ectopic pregnancy can grow large enough to split open the fallopian tube. This is known as a rupture.
Ruptures are very serious, and surgery to repair the fallopian tube needs to be carried out as soon as possible.
Signs of a rupture include a combination of:
- a sharp, sudden and intense pain in your tummy
- feeling very dizzy or fainting
- feeling sick
- looking very pale
Call your local emergency number for an ambulance or go to your nearest accident and emergency department immediately if you experience these symptoms.
Ectopic pregnancy diagnosis
It can be difficult to diagnose an ectopic pregnancy from the symptoms alone, as they can be similar to other conditions.
- Your doctor may examine you and offer a pregnancy test.
- If you have the symptoms of an ectopic pregnancy and a positive pregnancy test, your doctor may do further testing.
Vaginal ultrasound
An ectopic pregnancy is usually diagnosed by carrying out a transvaginal ultrasound scan.
This involves inserting a small probe into your vagina. The probe is so small that it’s easy to insert and you won’t need a local anesthetic.
The probe emits sound waves that bounce back to create a close-up image of your reproductive system on a monitor.
This will often show whether a fertilized egg has become implanted in one of your fallopian tubes, although occasionally it may be very difficult to spot.
Blood tests
Blood tests to measure the pregnancy hormone human chorionic gonadotropin (hCG) may also be carried out twice, 48 hours apart, to see how the level changes over time.
This can be a useful way of identifying ectopic pregnancies that aren’t found during an ultrasound scan, as the level of hCG tends to be lower and rise more slowly over time than in a normal pregnancy.
The results of the test can also be useful in determining the best treatment for an ectopic pregnancy.
Keyhole surgery
If it’s still not clear whether you have an ectopic pregnancy or the location of the pregnancy is unknown, a laparoscopy may be carried out.
This is a type of keyhole surgery carried out under general anaesthetic (where you’re asleep) that involves making a small cut (incision) in your tummy and inserting a viewing tube called a laparoscope.
Your doctor uses the laparoscope to examine the womb and fallopian tubes directly.
If an ectopic pregnancy is found during the procedure, small surgical instruments may be used to remove it to avoid the possible need for a second operation later on.
Ectopic pregnancy treatment
Unfortunately, the baby cannot be saved in an ectopic pregnancy. Treatment is usually needed to remove the pregnancy before it grows too large.
The main treatment options are:
- expectant management – your condition is carefully monitored to see whether treatment is necessary
- medication – a medicine called methotrexate is used to stop the pregnancy growing
- surgery – surgery is used to remove the pregnancy, usually along with the affected fallopian tube
These options each have advantages and disadvantages that your doctor will discuss with you.
They’ll recommend what they think is the most suitable option for you, depending on factors such as your symptoms, the size of the pregnancy, and the level of pregnancy hormone (human chorionic gonadotropin, or hCG) in your blood.
Expectant management
If you have no symptoms or mild symptoms and the pregnancy is very small or can’t be found, you may only need to be closely monitored, as there’s a good chance the pregnancy will dissolve by itself.
This is known as expectant management.
The following is likely to happen:
- You’ll have regular blood tests to check that the level of hCG in your blood is going down – these will be needed until the hormone is no longer found.
- You may need further treatment if your hormone level doesn’t go down or it increases.
- You’ll usually have some vaginal bleeding – use sanitary pads or towels, rather than tampons, until this clears up.
- You may experience some tummy pain – take paracetamol to relieve this.
- You’ll be told what to do if you develop more severe symptoms.
The main advantage of monitoring is that you won’t experience any side effects of treatment.
A disadvantage is that there’s still a small risk of your fallopian tubes splitting open (rupturing) and you may eventually need treatment.
Medication
If an ectopic pregnancy is diagnosed early but active monitoring isn’t suitable, treatment with a medicine called methotrexate may be recommended.
This works by stopping the pregnancy from growing. It’s given as a single injection into your buttocks.
You won’t need to stay in hospital after treatment, but regular blood tests will be carried out to check if the treatment is working.
A second dose is sometimes needed and surgery may be necessary if it doesn’t work.
You need to use reliable contraception for at least 3 months after treatment.
This is because methotrexate can be harmful for a baby if you become pregnant during this time.
It’s also important to avoid alcohol until you’re told it’s safe, as drinking soon after receiving a dose of methotrexate can damage your liver.
Other side effects of methotrexate include:
- tummy pain – this is usually mild and should pass within a day or two
- dizziness
- feeling and being sick
- diarrhea
There’s also a chance of your fallopian tubes rupturing after treatment. You’ll be told what to look out for and what to do if you think this has happened.
Surgery
In most cases, keyhole surgery (laparoscopy) will be carried out to remove the pregnancy before it becomes too large.
During a laparoscopy:
- you’re given general anesthetic, so you’re asleep while it’s carried out
- small cuts (incisions) are made in your tummy
- a thin viewing tube (laparoscope) and small surgical instruments are inserted through the incisions
- the entire fallopian tube containing the pregnancy is removed if your other fallopian tube looks healthy – otherwise, removing the pregnancy without removing the whole tube may be attempted
Removing the affected fallopian tube is the most effective treatment and isn’t thought to reduce your chances of becoming pregnant again.
Your doctor will discuss this with you beforehand, and you’ll be asked whether you consent to having the tube removed.
Most women can leave hospital a few days after surgery, although it can take 4 to 6 weeks to fully recover.
If your fallopian tube has already ruptured, you’ll need emergency surgery.
The surgeon will make a larger incision in your tummy (laparotomy) to stop the bleeding and repair your fallopian tube, if that’s possible.
After either type of surgery, a treatment called anti-D rhesus prophylaxis will be given if your blood type is RhD negative.
This involves an injection of a medicine that helps to prevent rhesus disease in future pregnancies.
Pelvic girdle pain
Some women develop pelvic pain in pregnancy. This is sometimes called pregnancy-related pelvic girdle pain or symphysis pubis dysfunction.
It’s estimated that pregnancy-related pelvic girdle pain affects up to one in five pregnant women to some degree.
It’s not known exactly why pelvic pain affects some women, but it’s thought to be linked to a number of issues, including previous damage to the pelvis, pelvic joints moving unevenly, and the weight or position of the baby.
Factors that may make a woman more likely to develop pregnancy-related pelvic girdle pain include:
- a history of lower back or pelvic girdle pain
- previous injury to the pelvis – for example, from a fall or accident
- having pregnancy-related pelvic girdle pain in a previous pregnancy
- a physically demanding job
Pregnancy-related pelvic girdle pain is a collection of uncomfortable symptoms caused by a stiffness of your pelvic joints or the joints moving unevenly at either the back or front of your pelvis.
Pregnancy-related pelvic girdle pain is not harmful to your baby, but it can cause severe pain around your pelvic area and make it difficult for you to get around.
Different women have different symptoms, and pregnancy-related pelvic girdle pain is worse for some women than others.
Symptoms can include:
- pain over the pubic bone at the front in the center
- pain across one or both sides of your lower back
- pain in the area between your vagina and anus (perineum)
Pain can also radiate to your thighs, and some women feel or hear a clicking or grinding in the pelvic area.
The pain can be most noticeable when you are:
- walking
- going upstairs
- standing on one leg (for example, when you’re getting dressed or going upstairs)
- turning over in bed
It can also be difficult to move your legs apart – for example, when you get out of a car.
There is treatment to help, and techniques to manage the pain and discomfort. If you get the right advice and treatment early on, pregnancy-related pelvic girdle pain can usually be managed and the symptoms minimized. Occasionally, the symptoms even clear up completely.
Most women with pregnancy-related pelvic girdle pain can have a normal vaginal birth.
Pelvic pain in pregnancy treatment
Physiotherapy aims to relieve or ease pain, improve muscle function and improve your pelvic joint position and stability. This may include:
- manual therapy to make sure the joints of your pelvis, hip and spine move normally
- exercises to strengthen your pelvic floor, stomach, back and hip muscles
- exercises in water
- advice and suggestions, including positions for labor and birth, looking after your baby and positions for sex
- pain relief, such as TENS
- equipment, if necessary, such as crutches or pelvic support belts
Labor and birth with pelvic pain
Many women with pelvic pain in pregnancy can have a normal vaginal birth. Plan ahead and talk about your birth plan with your birth partner and midwife.
Write in your birth plan that you have pregnancy-related pelvic girdle pain, so the people supporting you during labor and birth will be aware of your condition.
Think about birth positions that are the most comfortable for you, and write them in your birth plan. Being in water can take the weight off your joints and allow you to move more easily, so you might want to think about having a water birth. You can discuss this with your midwife.
Your ‘pain-free range of movement’
If you have pain when you open your legs, find out your pain-free range of movement.
To do this, lie on your back or sit on the edge of a chair and open your legs as far as you can without pain – your partner or midwife can measure the distance between your knees with a tape measure. This is your pain-free range.
To protect your joints, try not to open your legs wider than this during labor and birth. This is particularly important if you have an epidural for pain relief in labor, as you will not be feeling the pain that warns you that you are separating your legs too far.
If you have an epidural, make sure your midwife and birth partner are aware of your pain-free range of movement of your legs.
When pushing in the second stage of labor, you may find it beneficial to lie on one side. This prevents your legs from being separated too much. You can stay in this position for the birth of your baby, if you wish.
Sometimes, it might be necessary to open your legs wider than your pain-free range to deliver your baby safely, particularly if you have an assisted delivery (for example, with the vacuum or ventouse). Even in this case, it is possible to limit the separation of your legs. Make sure your midwife and doctor are aware that you have pregnancy-related pelvic girdle pain.
If you go beyond your pain-free range, your physiotherapist should assess you after the birth. Take extra care until they have assessed and advised you.
Coping with pelvic pain in pregnancy
Your physiotherapist may recommend a pelvic support belt to help ease your pain, or crutches to help you get around.
It can help to plan your day so that you avoid activities that cause you pain. For example, don’t go up or down stairs more often than you have to.
The Pelvic Obstetric & Gynaecological Physiotherapy network also offers this advice:
- Be as active as possible within your pain limits, and avoid activities that make the pain worse.
- Rest when you can.
- Get help with household chores from your partner, family and friends.
- Wear flat, supportive shoes.
- Sit down to get dressed – for example, don’t stand on one leg when putting on jeans.
- Keep your knees together when getting in and out of the car – a plastic bag on the seat can help you swivel.
- Sleep in a comfortable position – for example, on your side with a pillow between your legs.
- Try different ways of turning over in bed – for example, turning over with your knees together and squeezing your buttocks.
- Take the stairs one at a time, or go upstairs backwards or on your bottom.
- If you’re using crutches, have a small backpack to carry things in.
- If you want to have sex, consider different positions, such as kneeling on all fours.
Pelvic Obstetric & Gynaecological Physiotherapy network suggests that you AVOID:
- standing on one leg
- bending and twisting to lift, or carrying a baby on one hip
- crossing your legs
- sitting on the floor, or sitting twisted
- sitting or standing for long periods
- lifting heavy weights, such as shopping bags, wet washing or a toddler
- vacuuming
- pushing heavy objects, such as a supermarket trolley
- carrying anything in only one hand (try using a small backpack).
Pelvic pain in men
Men are rarely affected by pelvic pain.
Here is a list of possible causes of pelvic pain in men:
- Appendicitis
- Colon cancer
- Constipation
- Crohn’s disease (a type of inflammatory bowel disease)
- Diverticulitis
- Fibromyalgia
- Inguinal hernia
- Interstitial cystitis (also called painful bladder syndrome)
- Intestinal obstruction
- Irritable bowel syndrome
- Kidney stones
- Past physical or sexual abuse
- Pelvic floor muscle spasms
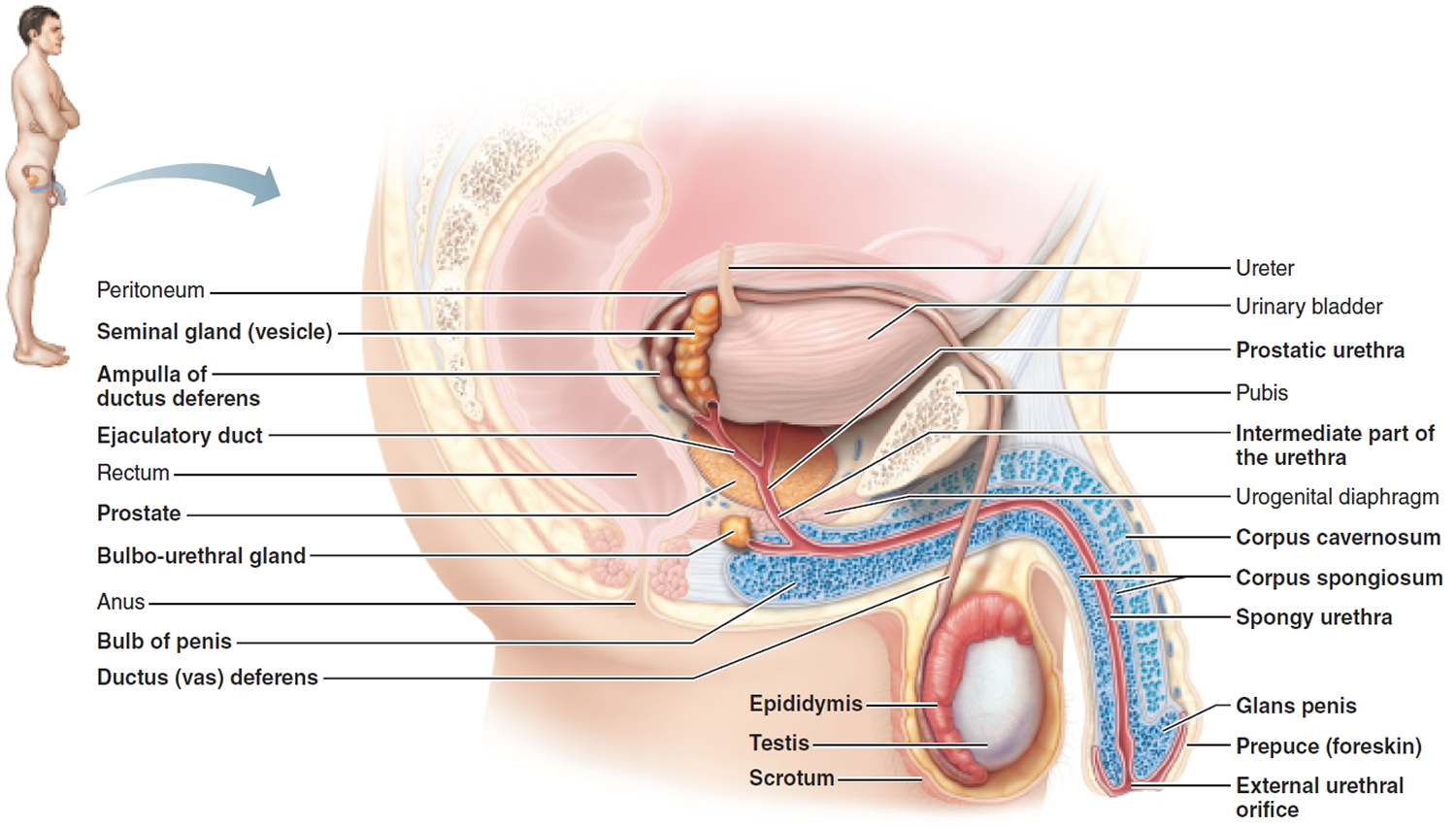
- Prostatitis (infection or inflammation of the prostate)
- Ulcerative colitis (a type of inflammatory bowel disease)
- Urinary tract infection (UTI)
Figure 4. Male reproductive system
References [ + ]





{kind=link}