Contents
What is peripheral vision
Peripheral vision is a part of vision that occurs outside the very center of your gaze. The back part of your eye contains several special areas of the retina (Figure 1). The retina is a layer of tissue in the back of your eye that senses light and sends images to your brain. The retina provides the sharp, central vision needed for reading, driving, and seeing fine detail (see Figures 1 and 2). Lying precisely at your eye’s posterior pole is the macula lutea (“yellow spot”). At the center of the macula lutea is a tiny pit called the fovea centralis (“central pit”) which is central detailed vision. The fovea (your central vision) contains only cones and provides the sharpest vision and maximal visual acuity. Because the fovea lies directly in the anterior-posterior axis of the eye, you see things most clearly when you look straight at them. The macula contains mostly cones and the density of cones declines with increasing distance from the macula. For this reason, peripheral vision is not as sharp as central vision. The retinal membrane consists of millions of nerve cells; these cells gather together behind the eye to form a large nerve called the optic nerve. A few millimeters towards the center to the fovea is the optic disc (Figure 1), a circular elevation where the axons of ganglion cells converge to exit the eye as the optic nerve. The optic disc is called the blind spot because it lacks photoreceptors, and light focused on it cannot be seen.
The optic nerves from your two eyes join inside your brain. The brain uses information from each optic nerve to combine the vision from the two eyes allowing you to see one image. The overlapping gives you depth perception which is known as binocular vision. Depth perception allows you to judge distances and see the world around us in 3D. Some retinal nerve cells are only sensitive to color perception, while others are specifically sensitive to movement. Movement sensitive cells enable you to view things at the edge of your vision, known as peripheral vision. This helps with activities such as driving.
Your visual field refers to the total area in which objects can be seen in the peripheral vision as you focus your eyes on a central point.
Peripheral vision problems mean that you don’t have a normal, wide-angle field of vision, even though your central vision may be fine.
Moderate and severe cases of peripheral vision loss create the sensation of seeing through a narrow tube, a condition commonly referred to as “tunnel vision.”
Symptoms of peripheral vision loss also can include difficulty seeing in dim light and decreased ability to navigate while you are walking.
If you suspect you have lost peripheral vision, see your eye doctor for a comprehensive eye exam that includes visual field testing.
If you have a sudden decrease in peripheral vision, see your eye doctor immediately. Sudden loss of peripheral vision may indicate a detached retina, which is a medical emergency that must be treated as soon as possible to avoid permanent vision loss.
Figure 1. Human eye
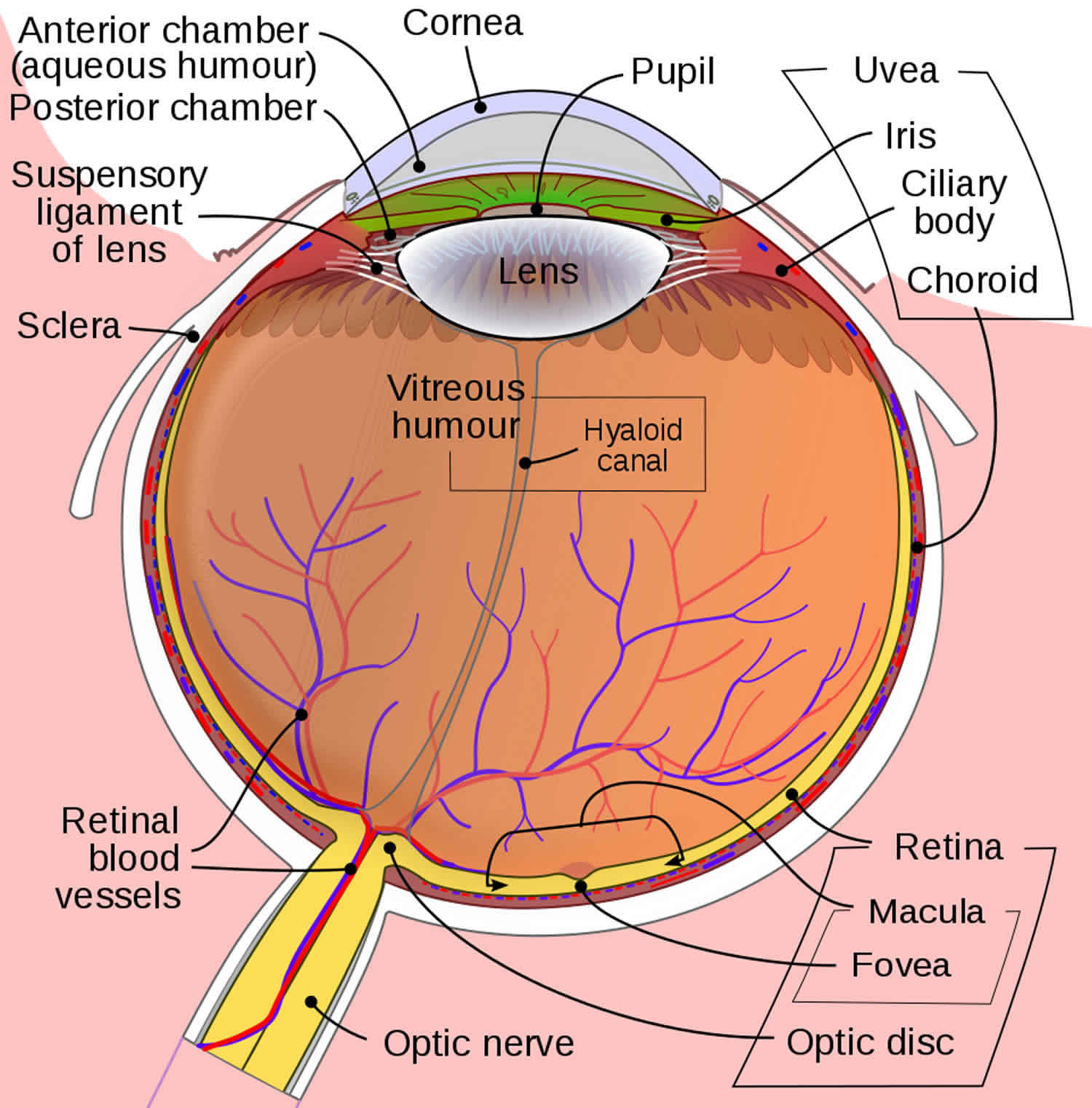
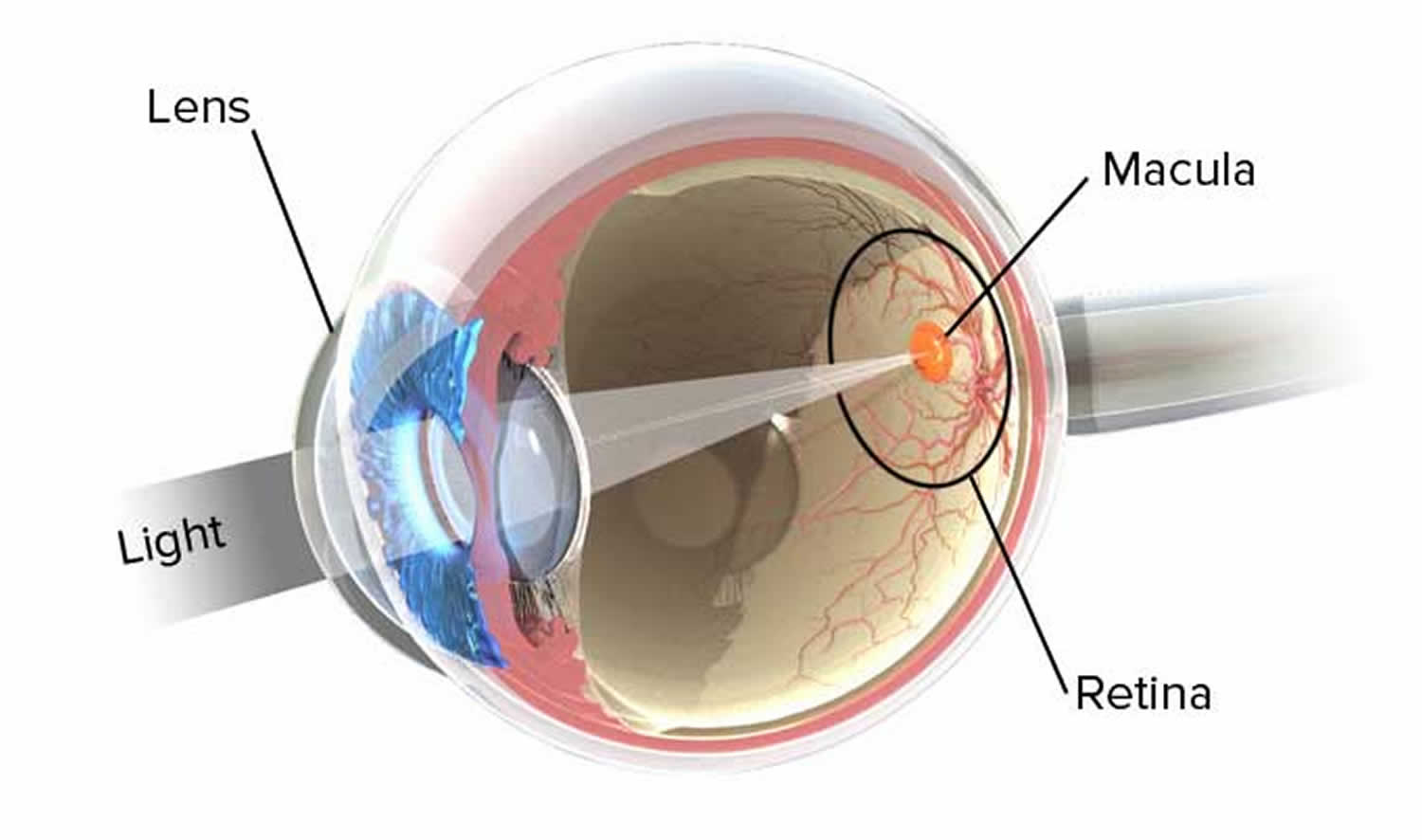 Figure 2. The retina
Figure 2. The retina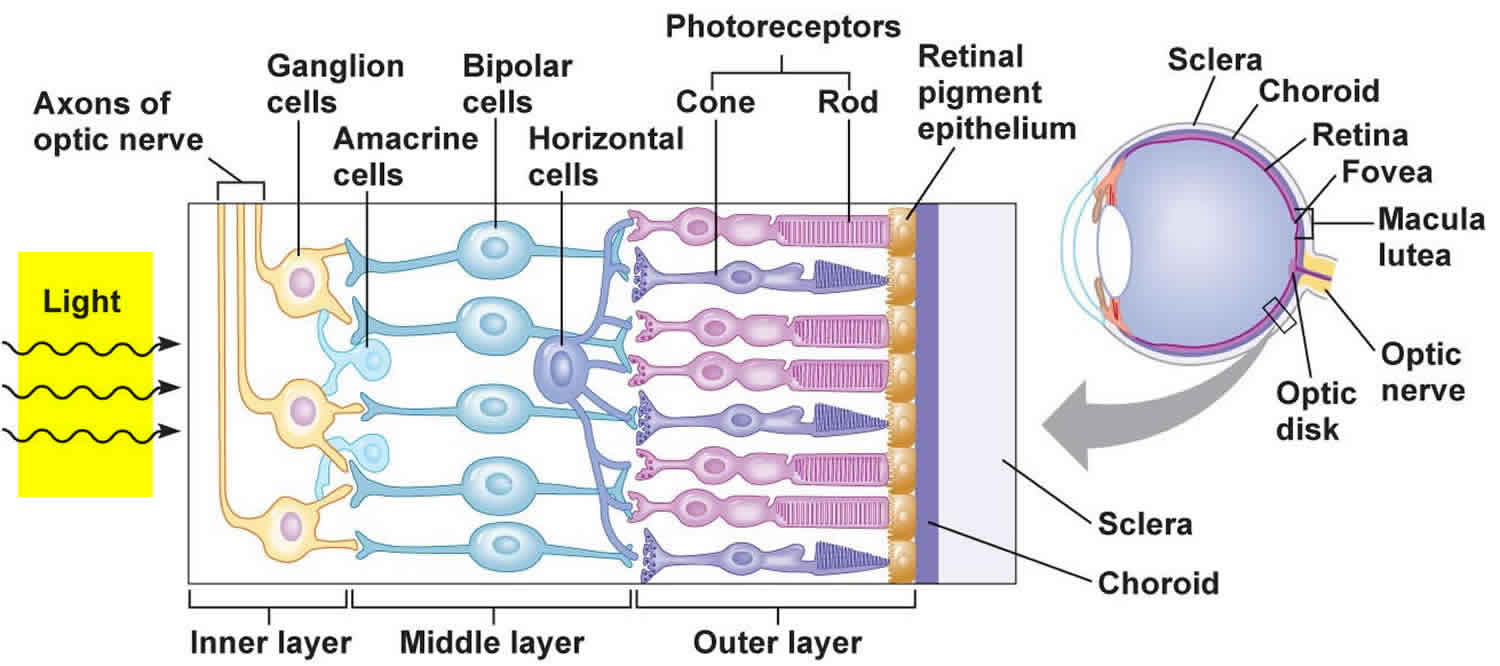
Loss of peripheral vision
There are many eye diseases and central nervous system (brain) disorders, such as tumors that damage or press on (compress) the parts of the brain that deal with vision. A stroke or injury also may damage portions of the brain where images are processed, leading to blind spots in the visual field.
Eye “strokes” (occlusions) that block normal blood flow to the eye’s internal structures, including the optic nerve, also can lead to loss of peripheral vision.
Other diseases that may affect your peripheral vision include:
- Brain damage from stroke, disease or injury
- Diabetes
- Compressed optic nerve head (papilledema)
- Concussions (head injuries)
- Glaucoma (increased eye pressure)
- High blood pressure
- Macular degeneration (eye disorder that slowly destroys sharp, central vision)
- Multiple sclerosis (disorder that affects the central nervous system)
- Neurological damage such as from optic neuritis
- Optic glioma (tumor of the optic nerve)
- Overactive thyroid (hyperthyroidism)
- Pituitary gland disorders
- Retinal detachment (separation of the retina in the back of the eye from its supporting layers)
- Retinitis pigmentosa
- Stroke
- Temporal arteritis (inflammation and damage to the blood vessels that supply blood to the head)
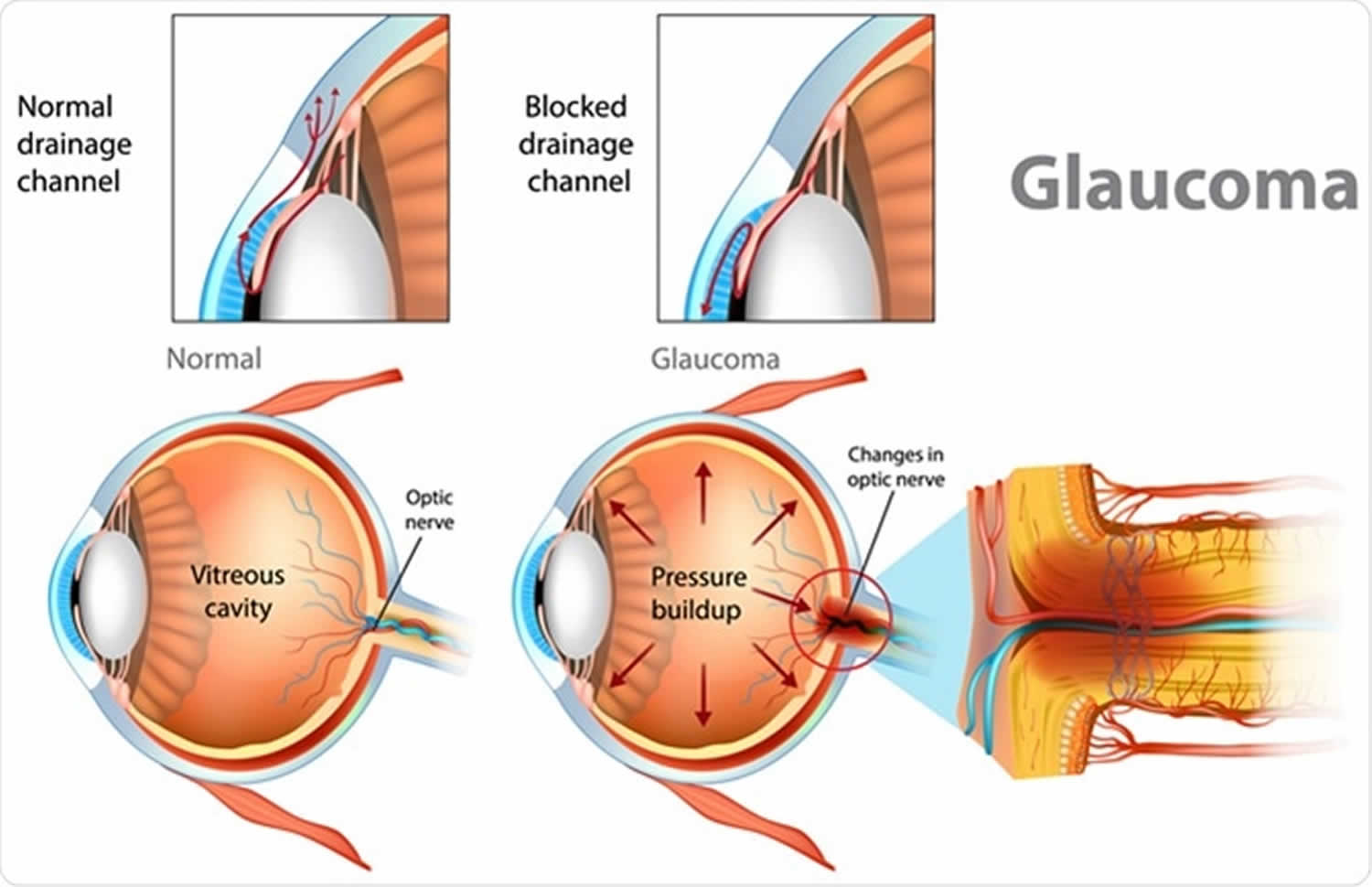
A common cause of loss of peripheral vision (also called a peripheral field defect) is optic nerve damage from glaucoma. Glaucoma is a group of eye conditions that can damage the optic nerve. Most often, optic nerve damage is caused by increased pressure in the eye. This is called intraocular pressure (IOP).
Glaucoma
Glaucoma is the second most common cause of blindness in the United States. There are four major types of glaucoma:
- Open-angle glaucoma
- Angle-closure glaucoma, also called closed-angle glaucoma
- Congenital glaucoma
- Secondary glaucoma
The front part of the eye is filled with a clear fluid called aqueous humor. This fluid is made in an area behind the colored part of the eye (iris). It leaves the eye through channels where the iris and cornea meet. This area is called the anterior chamber angle, or the angle. The cornea is the clear covering on the front of the eye that covers the iris, pupil, and angle.
Anything that slows or blocks the flow of this fluid will cause pressure to build up in the eye.
- In open-angle glaucoma, the increase in pressure is often small and slow.
- In closed-angle glaucoma, the increase is often high and sudden.
- Either type can damage the optic nerve.
Open-angle glaucoma is the most common type of glaucoma.
- The cause is unknown. The increase in eye pressure happens slowly over time. You cannot feel it.
- The increased pressure pushes on the optic nerve. Damage to the optic nerve causes blind spots in your vision.
- Open-angle glaucoma tends to run in families. Your risk is higher if you have a parent or grandparent with open-angle glaucoma. People of African descent are also at higher risk for this disease.
Closed-angle glaucoma occurs when the fluid is suddenly blocked and cannot flow out of the eye. This causes a quick, severe rise in eye pressure.
- Dilating eye drops and certain medicines may trigger an acute glaucoma attack.
- Closed-angle glaucoma is an emergency.
- If you have had acute glaucoma in one eye, you are at risk for it in the second eye. Your health care provider is likely to treat your second eye to prevent a first attack in that eye.
Secondary glaucoma occurs due to a known cause. Both open- and closed-angle glaucoma can be secondary when caused by something known. Causes include:
- Drugs such as corticosteroids
- Eye diseases, such as uveitis (an inflammation of the middle layer of the eye)
- Diseases such as diabetes
- Eye injury
Congenital glaucoma occurs in babies.
- It often runs in families.
- It is present at birth.
- It is caused when the eye does not develop normally.
Figure 3. Glaucoma
Glaucoma prevention
You cannot prevent open-angle glaucoma. Most people have no symptoms. But you can help prevent vision loss.
- A complete eye exam can help find open-angle glaucoma early, when it is easier to treat.
- All adults should have a complete eye exam by the age of 40.
- If you are at risk for glaucoma, you should have a complete eye exam sooner than age 40.
- You should have regular eye exams as recommended by your provider.
If you are at risk for closed-angle glaucoma, your provider may recommend treatment before you have an attack to help prevent eye damage and vision loss.
Glaucoma symptoms
Open-angle glaucoma
- Most people have no symptoms.
- Once you are aware of vision loss, the damage is already severe.
- Slow loss of side (peripheral) vision (also called tunnel vision).
- Advanced glaucoma can lead to blindness.
Angle-closure glaucoma
Symptoms may come and go at first, or steadily become worse. You may notice:
- Sudden, severe pain in one eye
- Decreased or cloudy vision, often called “steamy” vision
- Nausea and vomiting
- Rainbow-like halos around lights
- Red eye
- Eye feels swollen
Congenital glaucoma
Symptoms are most often noticed when the child is a few months old.
- Cloudiness of the front of the eye
- Enlargement of one eye or both eyes
- Red eye
- Sensitivity to light
- Tearing
Secondary glaucoma
- Symptoms are most often related to the underlying problem causing the glaucoma.
- Depending on the cause, symptoms may either be like open-angle glaucoma or angle-closure glaucoma.
Glaucoma diagnosis
The only way to diagnose glaucoma is by having a complete eye exam.
- You will be given a test to check your eye pressure. This is called tonometry.
- In most cases, you will be given eye drops to widen (dilate) your pupil.
- When your pupil is dilated, your eye doctor will look at the inside of your eye and the optic nerve.
Eye pressure is different at different times of the day. Eye pressure can even be normal in some people with glaucoma. So you will need other tests to confirm glaucoma. They may include:
- Using a special lens to look at the angle of the eye (gonioscopy).
- Photographs or laser scanning images of the inside of your eye (optic nerve imaging).
- Laser scanning images of the angle of the eye.
- Checking your retina — The retina is the light-sensitive tissue at the back of your eye.
- Checking how your pupil responds to light (pupillary reflex response).
- 3-D view of your eye (slit lamp examination).
- Testing the clearness of your vision (visual acuity).
- Testing your field of vision (visual field measurement).
Glaucoma treatment
The goal of treatment is to reduce your eye pressure. Treatment depends on the type of glaucoma that you have.
Open-angle glaucoma
- If you have open-angle glaucoma, you will probably be given eye drops.
- You may need more than one type. Most people can be treated with eye drops.
- Most of the eye drops used today have fewer side effects than those used in the past.
- You also may be given pills to lower pressure in the eye.
If drops alone do not work, you may need other treatment:
- Laser treatment uses a painless laser to open the channels where fluid flows out.
- If drops and laser treatment do not work, you may need surgery. The doctor will open a new channel so fluid can escape. This will help lower your pressure.
- Recently, new implants have been developed that can help treat glaucoma in people having cataract surgery.
Angle-closure glaucoma
An acute angle-closure attack is a medical emergency. You can become blind in a few days if you are not treated.
- You may be given drops, pills, and medicine given through a vein (by IV) to lower your eye pressure.
- Some people also need an emergency operation, called an iridotomy. The doctor uses a laser to open a new channel in the iris. Sometimes this is done with surgery. The new channel relieves the attack and will prevent another attack.
- To help prevent an attack in the other eye, the same procedure will often be performed on the other eye. This may be done even if it has never had an attack.
Congenital glaucoma
- Congenital glaucoma is almost always treated with surgery.
- This is done using general anesthesia. This means the child is asleep and feels no pain.
Secondary glaucoma
If you have secondary glaucoma, treating the cause may help your symptoms go away. Other treatments also may be needed.
Glaucoma prognosis
- Open-angle glaucoma cannot be cured. You can manage it and keep your sight by following your doctor’s directions.
- Closed-angle glaucoma is a medical emergency. You need treatment right away to save your vision.
- Babies with congenital glaucoma usually do well when surgery is done early.
- How you do with secondary glaucoma depends on what is causing the condition.
Flashes of light in peripheral vision
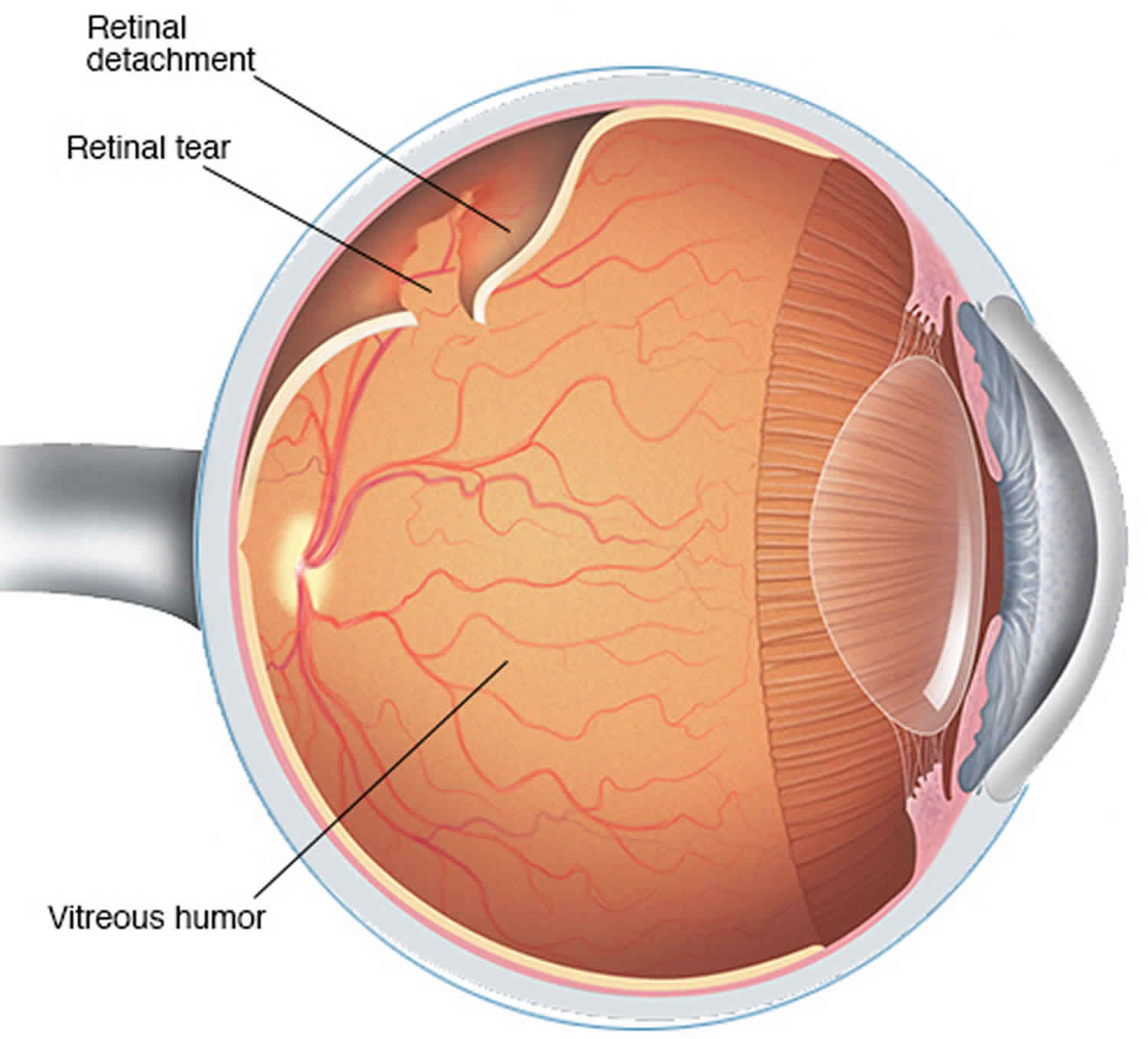
Retinal detachment refers to an eye condition in which the eye’s retina becomes detached from the vitreous fluid and layers of tissue that surround and support it. The retina is a layer of tissue in the back of your eye that senses light and sends images to your brain. It provides the sharp, central vision needed for reading, driving, and seeing fine detail. If your retina is damaged, you can lose you vision.
A retinal detachment can occur at any age, but it is more common in people over age 40. It affects men more than women and whites more than African Americans. A retinal detachment is also more likely to occur in people who:
- Are extremely nearsighted
- Have had a retinal detachment in the other eye
- Have a family history of retinal detachment
- Have had cataract surgery
- Have other eye diseases or disorders
- Have had an eye injury
Retinal detachment itself is painless. But warning signs almost always appear before it occurs or has advanced, such as:
- The sudden appearance of many floaters — tiny specks that seem to drift through your field of vision
- Flashes of light or “cobwebs” in one or both eyes
- Blurred vision
- Gradually reduced side (peripheral) vision
- A curtain-like shadow over your visual field
Symptoms include an increase in the number of floaters, which are little “cobwebs” or specks that float about in your field of vision, and/or light flashes in the eye. It may also seem like there is a “curtain” over your field of vision.
- A retinal detachment is a medical emergency. If not promptly treated, it can cause permanent vision loss. If you have any symptoms, see an eye care professional immediately. Treatment includes different types of surgery.
There are three different types of retinal detachment:
- Rhegmatogenous—A tear or break in the retina allows fluid to get under the retina and separate it from the retinal pigment epithelium (RPE), the pigmented cell layer that nourishes the retina. These types of retinal detachments are the most common.
- Tractional—In this type of detachment, scar tissue on the retina’s surface contracts and causes the retina to separate from the RPE. This type of detachment is less common.
- Exudative—Frequently caused by retinal diseases, including inflammatory disorders and injury/trauma to the eye. In this type, fluid leaks into the area underneath the retina, but there are no tears or breaks in the retina.
Get an urgent medical attention if:
- dots or lines (floaters) suddenly appear in your vision or suddenly increase in number
- you get flashes of light in your vision
- you have a dark “curtain” or shadow moving across your vision
These could be symptoms of a detached retina.
Retinal detachment is a medical emergency in which you can permanently lose your vision.
Figure 4. Retinal detachment
Retinal detachment causes
Retinal detachment can occur when the gel-like material (vitreous) leaks through a retinal hole or tear and collects underneath the retina.
Aging or retinal disorders can cause the retina to thin. Retinal detachment due to a tear in the retina typically develops when the vitreous collapses and tugs on the retina with enough force to create a tear.
Fluid inside the vitreous then finds its way through the tear and collects under the retina, peeling it away from the underlying tissues. These tissues contain a layer of blood vessels called the choroid. The areas where the retina is detached lose this blood supply and stop working, so you lose vision.
Aging-related retinal tears that lead to retinal detachment
As you age, your vitreous may change in consistency and shrink or become more liquid. Eventually, the vitreous may separate from the surface of the retina — a common condition called posterior vitreous detachment.
As the vitreous separates or peels off the retina, it may tug on the retina with enough force to create a retinal tear. Left untreated, fluid from the vitreous cavity can pass through the tear into the space behind the retina, causing the retina to become detached.
Posterior vitreous detachment can cause visual symptoms. You may see sudden new floaters or flashes of lights (photopsia). These may be visible even in daylight. The flashes may be more noticeable when your eyes are closed or you’re in a darkened room.
Who is at risk for retinal detachment?
A retinal detachment can occur at any age, but it is more common in people over age 40. It affects men more than women, and Whites more than African Americans.
A retinal detachment is also more likely to occur in people who:
- Are extremely nearsighted
- Have had a retinal detachment in the other eye
- Have a family history of retinal detachment
- Have had cataract surgery
- Have other eye diseases or disorders, such as retinoschisis, uveitis, degenerative myopia, or lattice degeneration
- Have had an eye injury
Retinal detachment prevention
Patients with known risk factors for retinal detachment should have serial dilated fundus examinations with scleral depression, often yearly. Protective eyewear is recommended for individuals with high myopia that participate in contact sports. Patients undergoing cataract surgery should be counseled about the importance of reporting symptoms of retinal tears and detachments.
Retinal detachment symptoms
Symptoms include a sudden or gradual increase in either the number of floaters, which are little “cobwebs” or specks that float about in your field of vision, and/or light flashes in the eye. Another symptom is the appearance of a curtain over the field of vision. A retinal detachment is a medical emergency. Anyone experiencing the symptoms of a retinal detachment should see an eye care professional immediately.
Retinal detachment itself is painless. But warning signs almost always appear before it occurs or has advanced, such as:
- The sudden appearance of many floaters — tiny specks that seem to drift through your field of vision
- Flashes of light or “cobwebs” in one or both eyes
- Blurred vision
- Gradually reduced side (peripheral) vision
- A curtain-like shadow over your visual field.
Retinal detachment diagnosis
Your doctor may use the following tests, instruments and procedures to diagnose retinal detachment:
- Retinal examination. The doctor may use an instrument with a bright light and a special lens (ophthalmoscope) to examine the back of your eye, including the retina. The ophthalmoscope provides a highly detailed view, allowing the doctor to see any retinal holes, tears or detachments.
- Ultrasound imaging. Your doctor may use this test if bleeding has occurred in the eye, making it difficult to see your retina.
Your doctor will likely examine both eyes even if you have symptoms in just one. If a tear is not identified at this visit, your doctor may ask you to return within a few weeks to confirm that your eye has not developed a delayed tear as a result of the same vitreous separation. Also, if you experience new symptoms, it’s important to return to your doctor right away.
Retinal detachment treatment
Retinal holes and tears can be treated in an eye specialist’s office with a laser surgery (photocoagulation) or a freeze treatment called cryopexy. During laser surgery tiny burns are made around the hole to “weld” the retina back into place. Cryopexy freezes the area around the hole and helps reattach the retina. However, retinal detachment usually requires surgery in an operating theater.
Surgery to re-attach the retina or fix a retinal tear may involve:
- Attaching a small synthetic band around outside of your eyeball to push the wall of your eye and retina closer together (scleral buckling).
- Removing and replacing the jelly inside your eye (vitrectomy). During a vitrectomy, the doctor makes a tiny incision in the sclera (white of the eye). Next, a small instrument is placed into the eye to remove the vitreous, a gel-like substance that fills the center of the eye and helps the eye maintain a round shape. Gas is often injected to into the eye to replace the vitreous and reattach the retina; the gas pushes the retina back against the wall of the eye. During the healing process, the eye makes fluid that gradually replaces the gas and fills the eye.
- Injecting a bubble of gas into your eye to push the retina against the back of your eye (pneumatic retinopexy)
- Sealing the tear in your retina with laser or freezing treatment (cryotherapy)
With all of these procedures, either laser (photocoagulation) or cryopexy is used to “weld” the retina back in place. It’s usually done with local anesthetic, so you’re awake but your eye is numbed. You don’t normally need to stay in hospital overnight.
After your procedure, you’ll likely be advised to avoid activities that might jar the eyes — such as running — for a couple of weeks or so.
Retinal detachment surgery
If your retina has detached, you’ll need surgery to repair it, preferably within days of a diagnosis. The type of surgery your surgeon recommends will depend on several factors, including how severe the detachment is.
- Injecting air or gas into your eye. In this procedure, called pneumatic retinopexy, the surgeon injects a bubble of air or gas into the center part of the eye (the vitreous cavity). If positioned properly, the bubble pushes the area of the retina containing the hole or holes against the wall of the eye, stopping flow of fluid into the space behind the retina. Your doctor also uses cryopexy during the procedure to repair the retinal break. Fluid that had collected under the retina is absorbed by itself, and the retina can then adhere to the wall of your eye. You may need to hold your head in a certain position for up to several days to keep the bubble in the proper position. The bubble eventually will reabsorb on its own.
- Indenting the surface of your eye. This procedure, called scleral buckling, involves the surgeon sewing (suturing) a piece of silicone material to the white of your eye (sclera) over the affected area. This procedure indents the wall of the eye and relieves some of the force caused by the vitreous tugging on the retina. If you have several tears or holes or an extensive detachment, your surgeon may create a scleral buckle that encircles your entire eye like a belt. The buckle is placed in a way that doesn’t block your vision, and it usually remains in place permanently.
- Draining and replacing the fluid in the eye. In this procedure, called vitrectomy, the surgeon removes the vitreous along with any tissue that is tugging on the retina. Air, gas or silicone oil is then injected into the vitreous space to help flatten the retina. Eventually the air, gas or liquid will be absorbed, and the vitreous space will refill with body fluid. If silicone oil was used, it may be surgically removed months later. Vitrectomy may be combined with a scleral buckling procedure.
These procedures are often done on an outpatient basis.
After surgery your vision may take several months to improve. You may need a second surgery for successful treatment. Some people never recover all of their lost vision.
Recovery time after surgery varies. But as a general guide, for 2 to 6 weeks after surgery:
- your vision may be blurry
- your eye may be sore and red – take paracetamol if you need to
- you may need to take time off work
- you may not be able to drive
- you may need to avoid flying (if you have had a bubble of gas put into your eye)
Over 90 percent of those with a retinal detachment can be successfully treated and most people are eventually able to return to all their normal activities. Although sometimes a second treatment is needed. However, the visual outcome is not always predictable. The final visual result may not be known for up to several months following surgery. Even under the best of circumstances, and even after multiple attempts at repair, treatment sometimes fails and vision may eventually be lost. Visual results are best if the retinal detachment is repaired before the macula (the center region of the retina responsible for fine, detailed vision) detaches. That is why it is important to contact an eye care professional immediately if you see a sudden or gradual increase in the number of floaters and/or light flashes, or a dark curtain over the field of vision.
Retinal detachment surgery complications
Proliferative retinopathy is the most common cause of repair failure and occurs in about 8–10% of patients undergoing primary retinal detachment repair 1. Risk factors for proliferative retinopathy include:
- Age
- Giant retinal tears
- Retinal detachments involving more than 2 quadrants
- Previous retinal detachment repair
- Use of cryotherapy
- Vitreous hemorrhage
- Choroidal detachment.
Proliferative retinopathy requires surgical intervention to release the traction caused by membranes and has a poor visual prognosis 2.
Peripheral vision loss treatment
Unfortunately, there are no easy vision correction options such as conventional eyeglasses or contact lenses that can correct permanent loss of peripheral vision. A type of lens known as a prism sometimes can be added to your eyeglasses prescription to expand your field of view if you have certain types of peripheral vision loss.
If you have glaucoma, the best “cure” for tunnel vision is prevention. If eye drops are prescribed, you absolutely must take your glaucoma medication regularly to control high eye pressure, or you risk permanent optic nerve damage and development of blind spots in your visual field. Left untreated, glaucoma can lead to permanent loss of peripheral vision and even blindness.
Therapy also may be available for blind spots created by brain damage. University of Rochester Eye Institute researchers in New York recently discovered that specific vision therapy techniques may help people regain at least some visual field loss linked to damage in the brain’s primary visual cortex 3.
Even if you have normal vision, you might use some techniques such as those taught by sports vision specialists to train yourself to see better in the peripheral parts of your field of view. These methods can be helpful particularly if you need to hone your peripheral vision skills for sports such as basketball and baseball.
If you have permanent loss of peripheral vision, you should consider visiting a low vision specialist who can advise you about special eyewear or optical devices that might help with mobility problems caused by tunnel vision.
Also, be aware that reduced peripheral vision may affect your ability to drive safely. A low vision specialist can tell you about the extent of your peripheral vision loss and whether your remaining vision meets the legal requirement for a valid driver’s license in your state.
- Brucker AJ, Hopkins TB. Retinal Detachment Surgery: The Latest in Current Management. Retina. 2006; 26: S28-S33.[↩]
- Girard P, Mimoun G, Karpouzas I, et al. Clinical risk factors for proliferative vitreoretinopathy after retinal detachment surgery. Retina. 1995; 14:417–424.[↩]
- Perceptual relearning of complex visual motion after V1 damage in humans. The Journal of Neuroscience. April 2009.[↩]





{kind=link}