Contents
- What is platelet count
- When is platelet count ordered?
- What does the platelet count test result mean?
- Are there signs or symptoms of high or low platelet levels that I should pay attention to?
- My platelet count is low. How can I increase it?
- Is there anything else I should know?
- If my platelet count is abnormal, what follow-up tests might my doctor order?
- My report includes mean platelet volume (MPV) and platelet distribution width (PDW). What are they?
- My report mentions “giant platelets.” What are they?
- My complete blood count (CBC) report includes a result for immature platelet fraction (IPF). What is it?
- High platelet count
- Low platelet count
What is platelet count
Platelets, also called thrombocytes, are tiny fragments of cells that are essential for normal blood clotting. Platelets are formed from very large cells called megakaryocytes in the bone marrow and are released into the blood to circulate. The platelet count is a test that determines the number of platelets in a person’s sample of blood. A normal platelet count on a blood test is about 150,000 to 450,000 per microliter of blood. Normal clotting is still possible with a platelet count of 100,000. The risk of serious bleeding is very high when the platelet count goes below 20,000 per microliter of blood.
A platelet count is used to detect the number of platelets in the blood. The test is included in a complete blood count (CBC), a panel of tests often performed as part of a general health examination. A platelet count may be used to screen for or diagnose various diseases and conditions that can cause problems with clot formation. It may be used as part of the workup of a bleeding disorder, bone marrow disease, or excessive clotting disorder, to name just a few.
A platelet count test may be used as a monitoring tool for people with underlying conditions or undergoing treatment with drugs known to affect platelets. It may also be used to monitor those being treated for a platelet disorder to determine if therapy is effective.
A platelet count may be performed in conjunction with one or more platelet function tests, which assess the function of platelets, and other tests that evaluate coagulation such as Prothrombin Time (PT) and Partial Thromboplastin Time (PTT) . If results are not within the normal interval, a number of other tests may be performed to help give clues as to the cause. Sometimes a blood smear may be done in follow up to examine the platelets under a microscope. This would help to determine, for example, whether platelets might truly be low in number or have clumped together during testing.
You might recall your blood mainly consists of red blood cells, which carry oxygen from the lungs to the rest of your body, and plasma, the liquid component, the nutrient- and chemical-rich river in which red blood cells go tubing. You probably also remember white blood cells, which help you fight infection. The blood of a healthy, average person is about 45% red blood cells (RBCs), 55% plasma, and about 1% white blood cells (WBCs). Platelets are such a tiny percentage of your blood volume that you just count how many are in a microliter of blood. Platelets are actually tiny fragments of cells, all jagged and funky-looking, compared to those pretty, round, red blood cells that are five times bigger.
When there is an injury to a blood vessel or tissue and bleeding begins, platelets help stop bleeding in three ways. They:
- Adhere to the injury site
- Clump together (aggregate) with other platelets
- Release chemical compounds that stimulate further aggregation of other platelets
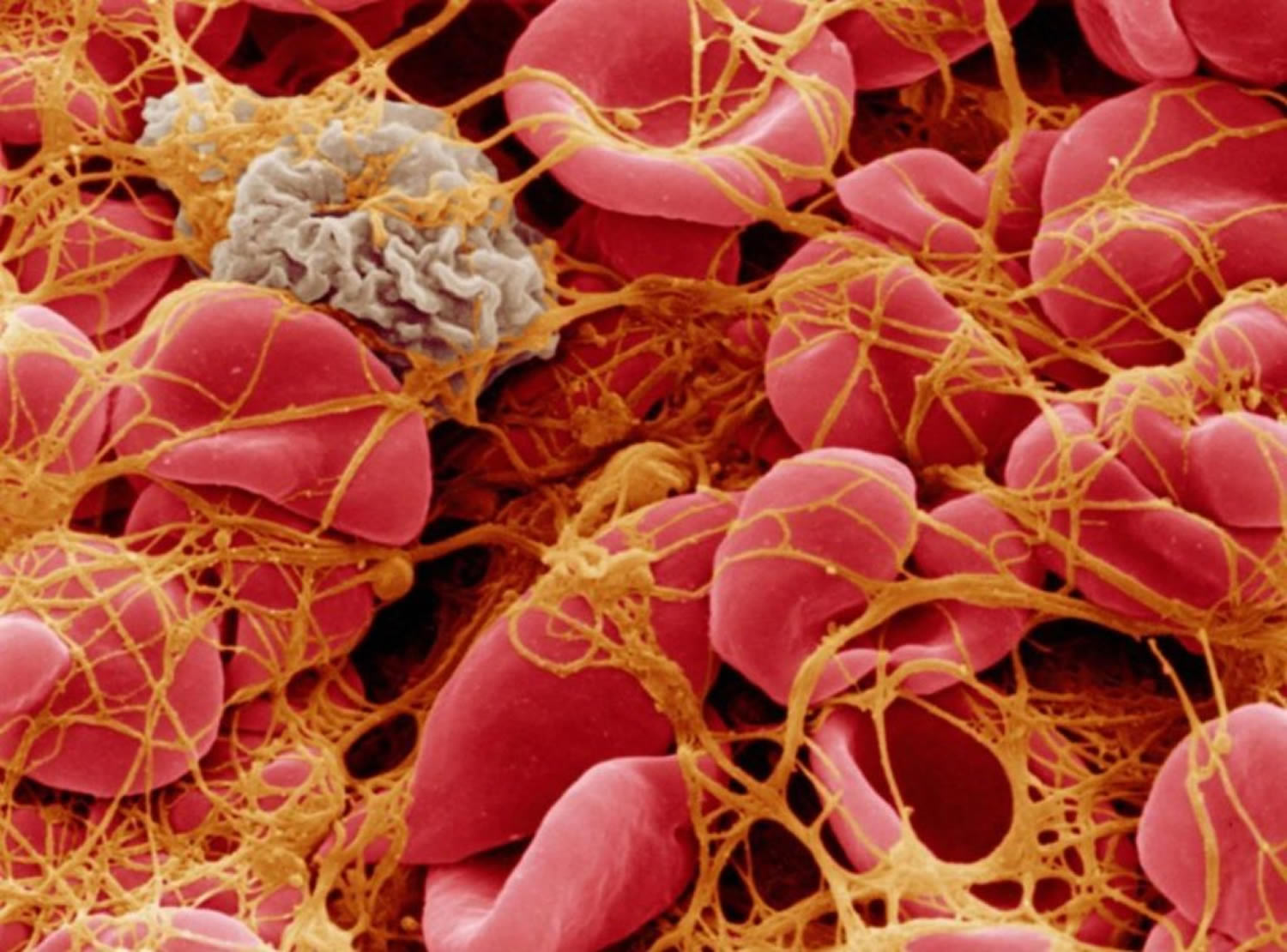
These steps result in the formation of a loose platelet plug at the site of the injury in a process called primary hemostasis. At the same time, activated platelets support the coagulation cascade, a series of steps that involves the sequential activation of proteins called clotting factors. This secondary hemostasis process results in the formation of strands of fibrin that weave through the loose platelet plug, form a fibrin net, and compress to form a stable clot that remains in place until the injury has healed. When the clot is no longer needed, other factors break the clot down and remove it.
Each component of primary and secondary hemostasis must be present, activated at the right time, and functioning properly for adequate clotting. If there are insufficient platelets, or if platelets are not functioning normally, a stable clot may not form and a person may be at an increased risk of excessive bleeding.
Platelets survive in the circulation about 8 to 10 days, and the bone marrow must continually produce new platelets to replace those that degrade, are used up, and/or are lost through bleeding. Determining the number of platelets in blood with a platelet count can help diagnose a range of disorders having to do with too few or too many platelets.
Figure 1. Platelets
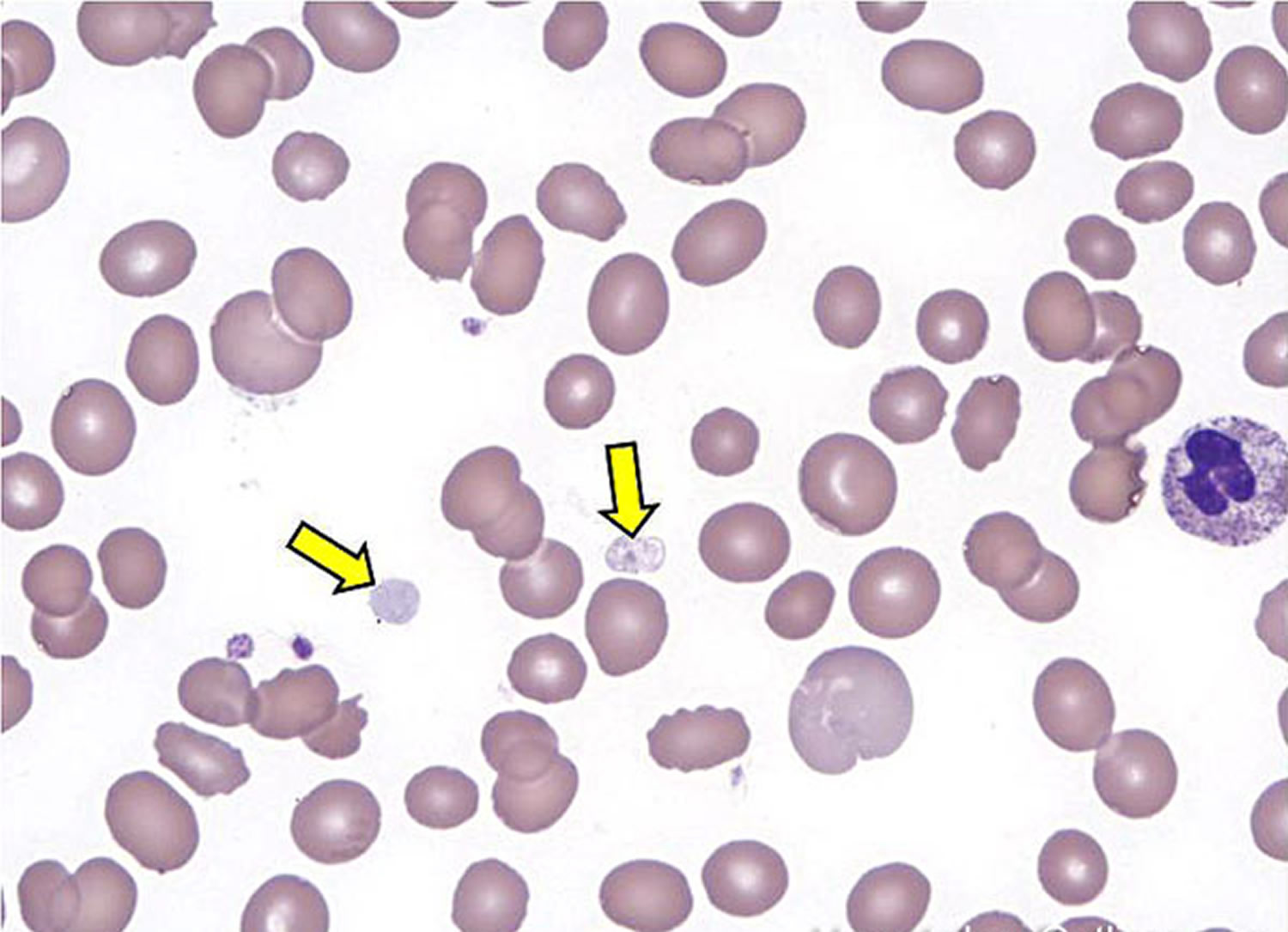
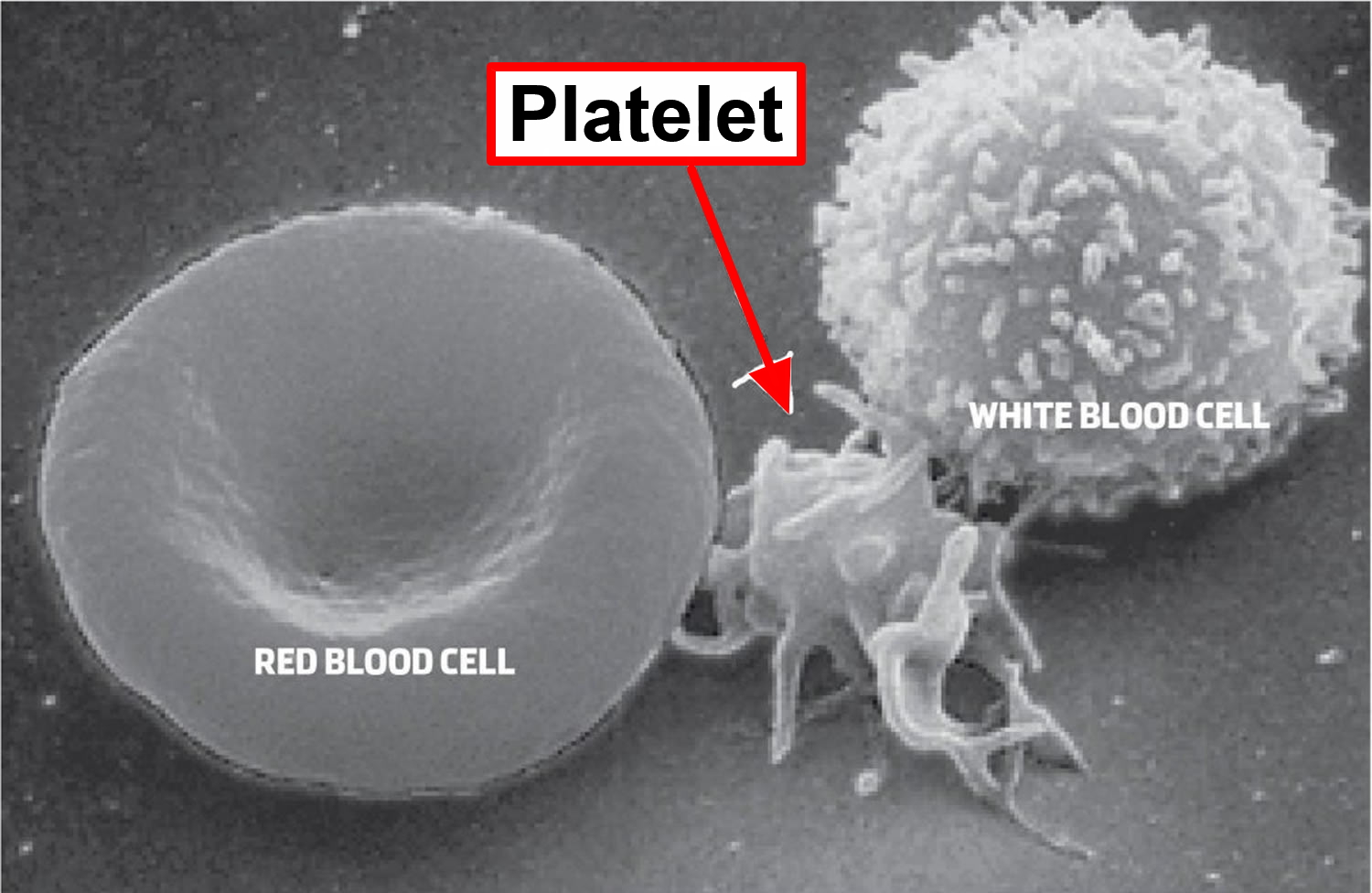
Figure 2. Blood composition


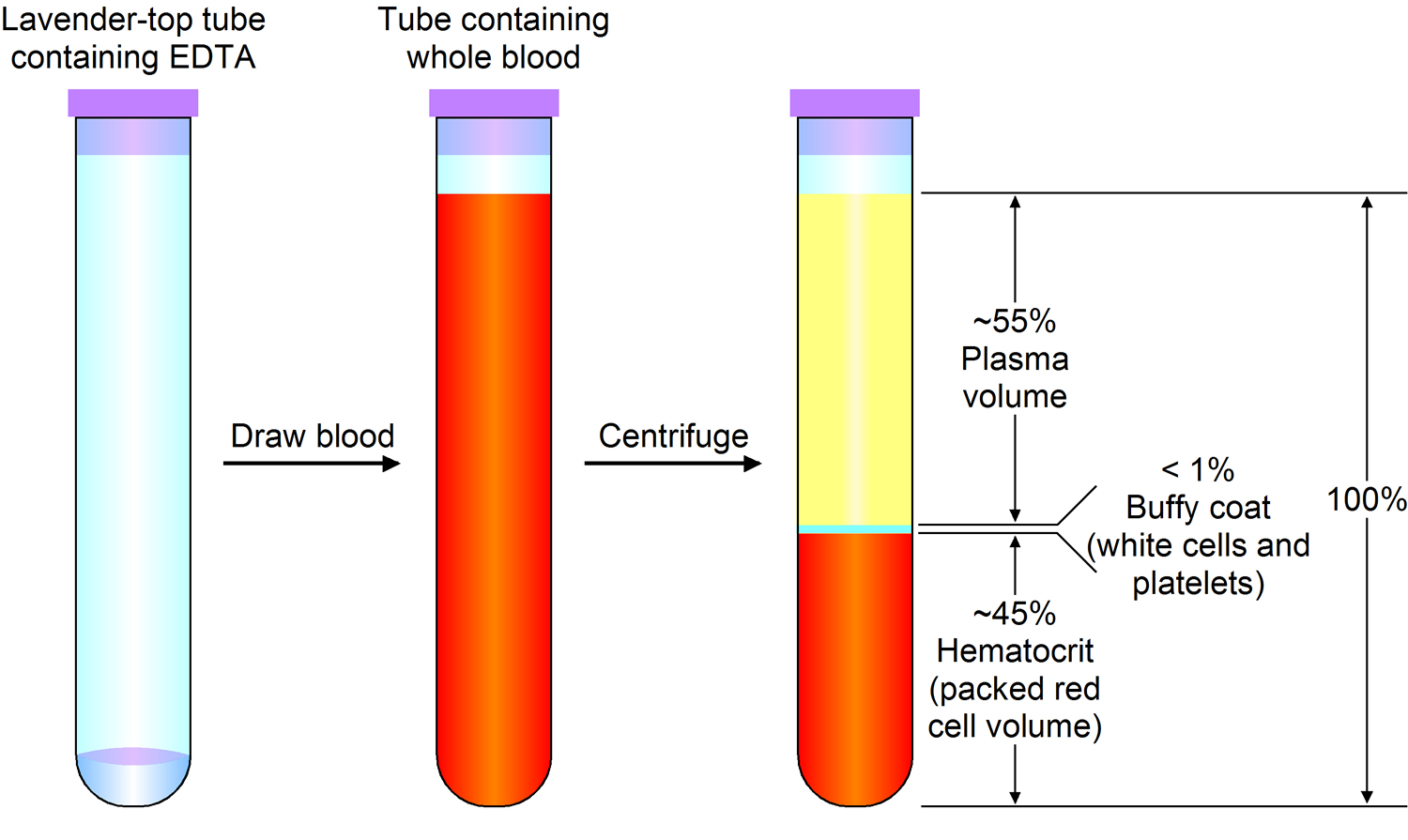
Note: Blood consists of a liquid portion called plasma and a solid portion (the formed elements) that includes red blood cells, white blood cells, and platelets. When blood components are separated by centrifugation, the white blood cells and platelets form a thin layer, called the “buffy coat,” between the plasma and the red blood cells, which accounts for about 1% of the total blood volume. Blood cells and platelets can be seen under a light microscope when a blood sample is smeared onto a glass slide.
Figure 3. Bone marrow anatomy

Figure 4. Blood cell development. A blood stem cell goes through several steps to become a red blood cell, platelet, or white blood cell

When is platelet count ordered?
A platelet count is often ordered as a part of a complete blood count (CBC), which may be done at the time of a routine health examination.
It may be ordered when a person has signs and symptoms associated with low platelets or a bleeding disorder, such as:
- Unexplained or easy bruising
- Prolonged bleeding from a small cut or wound
- Numerous nosebleeds
- Gastrointestinal bleeding (which can be detected in stool samples)
- Heavy menstrual bleeding
- Small red spots on the skin called petechiae—may sometimes look like a rash
- Small purplish spots on the skin called purpura, caused by bleeding under the skin
Testing may also be done when it is suspected that an individual has too many platelets. An excess of platelets can cause excessive clotting or sometimes bleeding if the platelets are not functioning properly. However, people with too many platelets often have no signs or symptoms, so the condition may be found only when a platelet count is done as part of a health check or for other reasons.
What does the platelet count test result mean?
A low platelet count, also called thrombocytopenia, and accompanying signs and symptoms may be caused by a number of conditions and factors. The causes typically fall into one of two general categories:
- Disorders in which the bone marrow cannot produce enough platelets
- Conditions in which platelets are used up (consumed) or destroyed faster than normal
Examples of conditions causing a low platelet count include:
- Idiopathic thrombocytopenia (ITP), also known as immune thrombocytopenic purpura, is the result of antibody production against platelets.
- Viral infections such as mononucleosis, hepatitis, HIV or measles
- Certain drugs, such as aspirin and ibuprofen, some antibiotics (including those containing sulfa), colchicine and indomethacin, H2-blocking agents, hydralazine, isoniazid, quinidine, thiazide diuretics, and tolbutamide, are just a few that have been associated with drug-induced decreased platelet counts.
- Heparin-induced thrombocytopenia (HIT) results in low platelets when a person who is on or received heparin therapy develops an antibody.
- Leukemia, lymphoma, or another cancer that has spread (metastasized) to the bone marrow—people with cancers often experience excessive bleeding due to a significantly decreased number of platelets. As the number of cancer cells increases in the bone marrow, normal bone marrow cells are crowded out, resulting in fewer platelet-producing cells.
- Aplastic anemia—a condition in which the production of all blood cells is significantly reduced
- Long-term bleeding problems (e.g., chronic bleeding from stomach ulcers)
- Sepsis, especially that caused by a serious bacterial infection with Gram-negative bacteria
- Cirrhosis
- Autoimmune disorders, such as lupus, where the body’s immune system produces antibodies that attack its own organs or tissues, causing increased destruction of platelets
- Chemotherapy or radiation therapy, which may affect the bone marrow’s ability to produce platelets
- Platelet consumption may be observed in various diseases and conditions. For example, disseminated intravascular coagulation (DIC), thrombocytopenic purpura (TTP) and hemolytic uremic syndrome (HUS) can result in fewer circulating platelets in the blood.
- Exposure to toxic chemicals, such as pesticides, arsenic, or benzene
If the platelet count falls below 20,000 per microliter, spontaneous bleeding may occur and is considered a life-threatening risk. A person with a very low count may be given platelets through a transfusion.
A high platelet count may be referred to as thrombocytosis. This is usually the result of an existing condition (also called secondary or reactive thrombocytosis) such as:
- Cancer, most commonly lung, gastrointestinal, ovarian, breast or lymphoma
- Anemia, in particular iron-deficiency anemia and hemolytic anemia
- Inflammatory conditions such as inflammatory bowel disease (IBD) or rheumatoid arthritis
- Infectious diseases such as tuberculosis
- If an individual has had their spleen removed surgically
- Use of birth control pills (oral contraceptives)
Some conditions may cause a temporary (transitory) increased platelet count. These may include:
- Recovery from significant blood loss such as from trauma or major surgery
- After physical activity or exertion
- Recovery from excess alcohol consumption and vitamin B12 and folate deficiency
Rarely, thrombocytosis is caused by a bone marrow disorder. An example is thrombocythemia, also called primary or essential thrombocythemia, a rare myeloproliferative disorder in which the bone marrow produces an extremely high number of platelets. Often there are no signs and symptoms and the condition is discovered when testing is done for a health check or for other reasons.
Individuals who have this condition may be at risk of excessive clotting (thrombosis) due to the excess platelets, but they may have bleeding problems, as the platelets may not function normally. This disorder is often associated with a mutation in the gene called JAK2. A test for this mutation should be performed if a health practitioner suspects that an individual has the disorder. More than half of the people with essential thrombocythemia have the JAK2 mutation. People with other myeloproliferative or myelodysplastic disorder, such as chronic myeloid leukemia, polycythemia vera or certain subtypes of myelodysplastic syndrome, may also have markedly higher platelet counts.
Are there signs or symptoms of high or low platelet levels that I should pay attention to?
Bruising for no apparent reason, bleeding from the nose, mouth, or rectum without obvious injury, excessive or prolonged menstrual periods, or the inability to stop a small wound from bleeding within a reasonable period of time may indicate a platelet deficiency.
My platelet count is low. How can I increase it?
Generally, there are no lifestyle changes that you can make that would increase your platelet count. Treatment for a low platelet count usually involves addressing the underlying condition that is causing it. If your condition is mild and your platelet count is only slightly low, you may not require any treatment. If it is caused by a drug, your healthcare provider may switch you to a different one. If it is due to an autoimmune disorder, your practitioner may prescribe a drug that helps to suppress the immune system. People with serious conditions and/or platelet counts that are significantly decreased may be at risk of excessive bleeding, so they may be transfused with platelets.
Is there anything else I should know?
Some people have platelets that tend to “pool” or collect (sequester) in their spleen, resulting in a low platelet count. However, these individuals typically do not experience any signs or symptoms related to this condition.
Living in high altitudes, strenuous exercise, and having recently delivered a baby (post partum) may cause increased platelet numbers. Drugs that may cause increased platelet counts include estrogen and birth control pills (oral contraceptives).
Mildly decreased platelet counts may be seen in women before menstruation. Up to 5% of pregnant women may have a lower platelet count at term.
Inherited disorders caused by genetic defects in platelets include Glanzmann’s Thrombasthenia, Bernard-Soulier disease, Chediak-Higashi syndrome, Wiskott-Aldrich syndrome, May-Hegglin syndrome, and Down syndrome. The occurrence of these genetic abnormalities, however, is relatively rare.
If my platelet count is abnormal, what follow-up tests might my doctor order?
If the cause of the abnormal result is not apparent and cannot be determined from your medical history and physical examination, your healthcare provider may choose to order additional tests. Depending on the suspected cause and results from a CBC and blood smear, various follow-up tests may be performed. A few examples include:
- Tests for inflammatory conditions such as CRP, ESR or tests for autoantibodies that target platelets
- Tests for infectious diseases including bacteria and viruses
- Tests for bleeding disorders such as PT, PTT, fibrinogen
- Tests for kidney failure
- Iron studies or vitamin B12 and folate levels
- Tests for liver disease
- In unexplained, serious cases, a bone marrow biopsy
My report includes mean platelet volume (MPV) and platelet distribution width (PDW). What are they?
Mean platelet volume (MPV) and platelet distribution width (PDW) are calculations performed by automated blood analyzers. Mean platelet volume (MPV) reflects the average size of platelets present in a person’s sample of blood while platelet distribution width (PDW) reflects how uniform the platelets are in size. These calculations can give the doctor additional information about platelets and/or about the cause of a high or low platelet count. Larger platelets are usually relatively young and more recently released from the bone marrow, while smaller platelets may be older and have been in circulation for a few days.
A high number of large platelets (high MPV) in a person with a low platelet count suggests the bone marrow is producing platelets and releasing them into circulation rapidly. Conversely, the mean platelet volume (MPV) may be low in people with low platelet counts due to a disorder affecting production by the bone marrow. A normal platelet distribution width (PDW) indicates platelets that are mostly the same size, while a high platelet distribution width (PDW) means that platelet size varies greatly, a clue that there may be a disorder affecting platelets.
Often, abnormal results will prompt additional testing. Under certain conditions, platelets may clump together and falsely appear to be low in number and/or large in size so a blood smear may be performed to examine platelets directly using a microscope.
My report mentions “giant platelets.” What are they?
“Giant platelet” is a term used to describe platelets that are abnormally large, i.e., as large as a normal red blood cell. These may be seen in certain disorders such as immune thrombocytopenic purpura (ITP) or in rare inherited disorders such as Bernard-Soulier disease. However, as mentioned in the previous question, a direct examination with a blood smear may be necessary to determine whether the platelets are truly giant or platelets have clumped together during testing. If platelets are clumping, repeat testing may be performed using a different collection tube containing a different anticoagulant that prevents or minimizes platelet clumping.
My complete blood count (CBC) report includes a result for immature platelet fraction (IPF). What is it?
Immature platelet fraction (IPF) is the relative number of immature platelets (also called reticulated platelets) in the blood. Platelets are produced in the bone marrow and are normally not released into the bloodstream until they have matured. When platelet numbers in the blood are low (thrombocytopenia), it stimulates the bone marrow to produce platelets faster. When the need is great and when production cannot keep up with “demand,” then an increased number of immature platelets will be released into the bloodstream.
This immature platelet fraction (IPF) test result would be one of the values reported when blood is evaluated using an automated hematology analyzer. The immature platelet fraction (IPF) may be used to help a healthcare provider determine the likely cause of a person’s thrombocytopenia, that is, decrease in production by the marrow (IPF is low) versus increased loss of platelets in the blood (IPF is higher). Lab test results including platelet count and IPF can also help determine if a person needs a platelet transfusion and help monitor bone marrow recovery, such as after a bone marrow transplant. Other uses are being studied and the test’s ultimate clinical utility has not yet been well determined.
High platelet count
A high platelet count or elevated platelet count is also called thrombocytosis or thrombocythemia, which is a disorder in which your body produces too many platelets (thrombocytes), which play an important role in blood clotting. The term “thrombocythemia” is preferred when the cause of a high platelet count isn’t known. Elevated platelet count condition is sometimes called primary or essential thrombocythemia. With primary thrombocythemia, a high platelet count may occur alone or with other blood cell disorders. This condition isn’t common. Primary thrombocythemia occurs if faulty cells in the bone marrow make too many platelets. Bone marrow is the sponge-like tissue inside the bones. It contains stem cells that develop into red blood cells, white blood cells, and platelets. What causes the bone marrow to make too many platelets often isn’t known.
When another disease or condition causes a high platelet count, the term “thrombocytosis” is preferred. This condition often is called secondary or reactive thrombocytosis. Secondary thrombocytosis is more common than primary thrombocythemia.
The high platelet count disorder is called reactive thrombocytosis or secondary thrombocythemia when it’s caused by an underlying condition, such as an infection.
Thrombocytosis (high platelet count) may also, less commonly, be caused by a blood and bone marrow disease. When caused by a bone marrow disorder, thrombocytosis is called autonomous, primary or essential thrombocytosis, or essential thrombocythemia.
Your doctor may detect thrombocytosis in routine blood test results that show a high platelet level. If your blood test indicates thrombocytosis, it’s important to determine whether it’s reactive thrombocytosis or if you have essential thrombocythemia, which is more likely to cause blood clots.
High platelet count signs and symptoms
People who have thrombocythemia or thrombocytosis may not have signs or symptoms. These conditions might be discovered only after routine blood tests.
However, people who have primary thrombocythemia are more likely than those who have secondary thrombocytosis to have serious signs and symptoms.
The signs and symptoms of a high platelet count are linked to blood clots and bleeding. They include weakness, bleeding, headache, dizziness, chest pain, and tingling in the hands and feet.
Reactive thrombocytosis rarely causes symptoms. More often, signs and symptoms relate to the underlying condition. If symptoms of reactive thrombocytosis do occur, they may include:
- Headache
- Dizziness or lightheadedness
- Chest pain
- Weakness
- Fainting
- Temporary vision changes
- Numbness or tingling of the hands and feet
Blood Clots
In primary thrombocythemia, blood clots most often develop in the brain, hands, and feet. But they can develop anywhere in the body, including in the heart and intestines.
Blood clots in the brain may cause symptoms such as chronic (ongoing) headache and dizziness. In extreme cases, stroke may occur.
Blood clots in the tiny blood vessels of the hands and feet leave them numb and red. This may lead to an intense burning and throbbing pain felt mainly on the palms of the hands and the soles of the feet.
Other signs and symptoms of blood clots may include:
- Changes in speech or awareness, ranging from confusion to passing out
- Seizures
- Upper body discomfort in one or both arms, the back, neck, jaw, or abdomen
- Shortness of breath and nausea (feeling sick to your stomach)
In pregnant women, blood clots in the placenta can cause miscarriage or problems with fetal growth and development.
Women who have primary thrombocythemia or secondary thrombocytosis and take birth control pills are at increased risk for blood clots.
Blood clots are related to other conditions and factors as well. Older age, prior blood clots, diabetes, high blood pressure, and smoking also increase your risk for blood clots.
Bleeding
If bleeding occurs, it most often affects people who have platelet counts higher than 1 million platelets per microliter of blood. Signs of bleeding include nosebleeds, bruising, bleeding from the mouth or gums, or blood in the stools.
Although bleeding usually is associated with a low platelet count, it also can occur in people who have high platelet counts. Blood clots that develop in thrombocythemia or thrombocytosis may use up your body’s platelets. This means that not enough platelets are left in your bloodstream to seal off cuts or breaks on the blood vessel walls.
Another cause of bleeding in people who have very high platelets counts is a condition called von Willebrand Disease. This condition affects the blood clotting process.
In rare cases of primary thrombocythemia, the faulty bone marrow cells will cause a form of leukemia (lu-KE-me-ah). Leukemia is a cancer of the blood cells.
High platelet count causes
Primary Thrombocythemia
In this condition, faulty stem cells in the bone marrow make too many platelets. What causes this to happen usually isn’t known. When this process occurs without other blood cell disorders, it’s called essential thrombocythemia. In essential thrombocythemia, there is a much higher risk of clotting or bleeding complications. Therefore, if your blood test results reveal a high platelet count, it’s important for your doctor to determine whether you have essential thrombocythemia or reactive thrombocytosis (secondary thrombocytosis).
A rare form of thrombocythemia is inherited. “Inherited” means the condition is passed from parents to children through the genes. In some cases, a genetic mutation may cause the condition.
In addition to the bone marrow making too many platelets, the platelets also are abnormal in primary thrombocythemia. They may form blood clots or, surprisingly, cause bleeding when they don’t work well.
Bleeding also can occur because of a condition that develops called von Willebrand disease. This condition affects the blood clotting process.
After many years, scarring of the bone marrow can occur.
Thrombocythemia isn’t common. The exact number of people who have the condition isn’t known. Some estimates suggest that 24 out of every 100,000 people have primary thrombocythemia.
Primary thrombocythemia is more common in people aged 50 to 70, but it can occur at any age. For unknown reasons, more women around the age of 30 have primary thrombocythemia than men of the same age.
Secondary Thrombocytosis
This condition occurs if another disease, condition, or outside factor causes the platelet count to rise. For example, 35 percent of people who have high platelet counts also have cancer—mostly lung, gastrointestinal, breast, ovarian, and lymphoma. Sometimes a high platelet count is the first sign of cancer.
Secondary thrombocytosis is more common than primary thrombocythemia. Studies have shown that most people who have platelet counts over 500,000 have secondary thrombocytosis.
Other conditions or factors that can cause a high platelet count are:
- Iron-deficiency anemia
- Hemolytic anemia — a type of anemia in which your body destroys red blood cells faster than it produces them, often due to certain blood diseases or autoimmune disorders
- Absence of a spleen (after surgery to remove the organ)
- Inflammatory diseases, such as rheumatoid arthritis, celiac disease, connective tissue disorders or inflammatory bowel disease
- Infections, including tuberculosis
- Reactions to medicine
Medications that can cause reactive thrombocytosis include:
- Epinephrine (AUVI-Q, EpiPen, others)
- Tretinoin (Retin-A, Renova, others)
- Vincristine Sulfate (Marqibo Kit)
- Heparin sodium
Some conditions can lead to a high platelet count that lasts for only a short time. Examples of such conditions include:
- Recovery from serious blood loss (acute bleeding and blood loss)
- Recovery from a very low platelet count caused by excessive alcohol use and lack of vitamin B12 or folate
- Acute (short-term) infection or inflammation
- Response to physical activity (exercise)
- Burns
- Coronary artery bypass
- Heart attack
- Major surgery
- Pancreatitis
- Removal of your spleen
- Trauma
- Vitamin deficiency
Although the platelet count is high in secondary thrombocytosis, the platelets are normal (unlike in primary thrombocythemia). Thus, people who have secondary thrombocytosis have a lower risk of blood clots and bleeding.
High platelet count prevention
You can’t prevent primary thrombocythemia. However, you can take steps to reduce your risk for complications. For example, you can control many of the risk factors for blood clots, such as high blood cholesterol, high blood pressure, diabetes, and smoking.
To reduce your risk, quit smoking, adopt healthy lifestyle habits, and work with your doctor to manage your risk factors.
It’s not always possible to prevent conditions that lead to secondary thrombocytosis. But, if you have routine medical care, your doctor may detect these conditions before you develop a high platelet count.
High platelet count diagnosis
Your doctor will diagnose thrombocythemia or thrombocytosis based on your medical history, a physical exam, and test results. A hematologist also may be involved in your care. This is a doctor who specializes in blood diseases and conditions.
Medical History
Your doctor may ask you about factors that can affect your platelets, such as:
- Any medical procedures or blood transfusions you’ve had
- Any recent infections or vaccines you’ve had
- The medicines you take, including over-the-counter medicines
- Your general eating habits, including the amount of alcohol you normally drink
- Any family history of high platelet counts
Physical Exam
Your doctor will do a physical exam to look for signs and symptoms of blood clots and bleeding. He or she also will check for signs of conditions that can cause secondary thrombocytosis, such as an infection.
Primary thrombocythemia is diagnosed only after all possible causes of a high platelet count are ruled out. For example, your doctor may recommend tests to check for early, undiagnosed cancer. If another disease, condition, or factor is causing a high platelet count, the diagnosis is secondary thrombocytosis.
Diagnostic Tests
Your doctor may recommend one or more of the following tests to help diagnose a high platelet count.
Complete Blood Count
A complete blood count (CBC) measures the levels of red blood cells, white blood cells, and platelets in your blood. For this test, a small amount of blood is drawn from a blood vessel, usually in your arm.
If you have thrombocythemia or thrombocytosis, the CBC results will show that your platelet count is high.
Blood Smear
A blood smear is used to check the condition of your platelets. For this test, a small amount of blood is drawn from a blood vessel, usually in your arm. Some of your blood is put on a glass slide. A microscope is then used to look at your platelets.
Bone Marrow Tests
Bone marrow tests check whether your bone marrow is healthy. Blood cells, including platelets, are made in the bone marrow. The two bone marrow tests are aspiration and biopsy.
Bone marrow aspiration might be done to find out whether your bone marrow is making too many platelets. For this test, your doctor removes a sample of fluid bone marrow through a needle. He or she examines the sample under a microscope to check for faulty cells.
A bone marrow biopsy often is done right after an aspiration. For this test, your doctor removes a small amount of bone marrow tissue through a needle. He or she examines the tissue to check the number and types of cells in the bone marrow.
With thrombocythemia and thrombocytosis, the bone marrow has a higher than normal number of the very large cells that make platelets.
Other Tests
Your doctor may recommend other blood tests to look for genetic factors that can cause a high platelet count.
High platelet count treatment
Primary Thrombocythemia
This condition is considered less harmful today than in the past, and its outlook often is good. People who have no signs or symptoms don’t need treatment, as long as the condition remains stable.
Taking aspirin may help people who are at risk for blood clots (aspirin thins the blood). However, talk with your doctor about using aspirin because it can cause bleeding.
Doctors prescribe aspirin to most pregnant women who have primary thrombocythemia. This is because it doesn’t have a high risk of side effects for the fetus.
Some people who have primary thrombocythemia may need medicines or medical procedures to lower their platelet counts.
Medicines To Lower Platelet Counts
You may need medicines to lower your platelet count if you:
- Have a history of blood clots or bleeding
- Have risk factors for heart disease, such as high blood cholesterol, high blood pressure, or diabetes
- Are older than 60
- Have a platelet count over 1 million
You’ll need to take these medicines throughout your life.
Hydroxyurea. This platelet-lowering medicine is used to treat cancers and other life-threatening diseases. Hydroxyurea most often is given under the care of doctors who specialize in cancer or blood diseases. Patients on hydroxyurea are closely monitored.
Currently, hydroxyurea plus aspirin is the standard treatment for people who have primary thrombocythemia and are at high risk for blood clots.
Anagrelide. This medicine also has been used to lower platelet counts in people who have thrombocythemia. However, research shows that when compared with hydroxyurea, anagrelide has worse outcomes. Anagrelide also has side effects, such as fluid retention, palpitations arrhythmias, heart failure, and headaches.
Interferon alfa. This medicine lowers platelet counts, but 20 percent of patients can’t handle its side effects. Side effects include a flu-like feeling, decreased appetite, nausea (feeling sick to the stomach), diarrhea, seizures, irritability, and sleepiness.
Doctors may prescribe this medicine to pregnant women who have primary thrombocythemia because it’s safer for a fetus than hydroxyurea and anagrelide.
Plateletpheresis
Plateletpheresis is a procedure used to rapidly lower your platelet count. This procedure is used only for emergencies. For example, if you’re having a stroke due to primary thrombocythemia, you may need plateletpheresis.
An intravenous (IV) needle that’s connected to a tube is placed in one of your blood vessels to remove blood. The blood goes through a machine that removes platelets from the blood. The remaining blood is then put back into you through an IV line in one of your blood vessels.
One or two procedures might be enough to reduce your platelet count to a safe level.
Secondary Thrombocytosis
Secondary thrombocytosis is treated by addressing the condition that’s causing it.
People who have secondary thrombocytosis usually don’t need platelet-lowering medicines or procedures. This is because their platelets usually are normal (unlike in primary thrombocythemia).
Also, secondary thrombocytosis is less likely than primary thrombocythemia to cause serious problems related to blood clots and bleeding.
Living with high platelet count
If you have thrombocythemia or thrombocytosis:
- See your doctor for ongoing medical care.
- Control risk factors for blood clots—for example, quit smoking and work to manage risk factors such as high blood cholesterol, high blood pressure, and diabetes.
- Watch for signs and symptoms of blood clots and bleeding and report them to your doctor right away.
- Take all medicines as prescribed.
If you’re taking medicines to lower your platelet count, tell your doctor or dentist about them before any surgical or dental procedures. These medicines thin your blood and may increase bleeding during these procedures.
Medicines that thin the blood also may cause internal bleeding. Signs of internal bleeding include bruises, bloody or tarry-looking stools, pink or bloody urine, increased menstrual bleeding, bleeding gums, and nosebleeds. Contact your doctor right away if you have any of these signs.
Avoid over-the-counter pain medicines such as ibuprofen (except Tylenol or acetaminophen/paracetamol). These medicines may raise your risk of bleeding in the stomach or intestines and may limit the effect of aspirin. Be aware that cold and pain medicines and other over-the-counter products may contain ibuprofen.
Low platelet count
Thrombocytopenia is a condition in which you have a low blood platelet count. Platelets (thrombocytes) are colorless blood cells that help blood clot. Platelets stop bleeding by clumping and forming plugs in blood vessel injuries. Platelets are made in your bone marrow along with other kinds of blood cells. They travel through your blood vessels and stick together (clot) to stop any bleeding that may happen if a blood vessel is damaged. Platelets also are called thrombocytes because a clot also is called a thrombus.
When your blood has too few platelets, mild to serious bleeding can occur. Bleeding can occur inside your body (internal bleeding) or underneath your skin or from the surface of your skin (external bleeding). Low blood platelet count (thrombocytopenia) can be fatal, especially if the bleeding is severe or occurs in the brain. However, the overall outlook for people who have low blood platelet count (thrombocytopenia) is good, especially if the cause of the low platelet count is found and treated.
A normal platelet count in adults ranges from 150,000 to 450,000 platelets per microliter of blood. A platelet count of less than 150,000 platelets per microliter is lower than normal. If your blood platelet count falls below normal, you have thrombocytopenia.
However, the risk for serious bleeding doesn’t occur until the count becomes very low—less than 10,000 or 20,000 platelets per microliter. Mild bleeding sometimes occurs when the count is less than 50,000 platelets per microliter.
Many factors can cause a low platelet count, such as:
- The body’s bone marrow doesn’t make enough platelets.
- The bone marrow makes enough platelets, but the body destroys them or uses them up.
- The spleen holds on to too many platelets. The spleen is an organ that normally stores about one-third of the body’s platelets. It also helps your body fight infection and remove unwanted cell material.
- A combination of the above factors.
Low blood platelet count (thrombocytopenia) often occurs as a result of a separate disorder, such as leukemia or an immune system problem. Or it can be a side effect of taking certain medications. Low blood platelet count (thrombocytopenia) affects both children and adults.
How long low blood platelet count (thrombocytopenia) lasts depends on its cause. It can last from days to years.
The treatment for long low blood platelet count (thrombocytopenia) also depends on its cause and severity. Mild long low blood platelet count (thrombocytopenia) often doesn’t require treatment. If long low blood platelet count (thrombocytopenia) causes or puts you at risk for serious bleeding, you may need medicines or blood or platelet transfusions. Rarely, the spleen may need to be removed.
Low platelet count symptoms
Mild to serious bleeding causes the main signs and symptoms of thrombocytopenia. Bleeding can occur inside your body (internal bleeding) or underneath your skin or from the surface of your skin (external bleeding).
Signs and symptoms can appear suddenly or over time. Mild thrombocytopenia often has no signs or symptoms. Many times, it’s found during a routine blood test.
Check with your doctor if you have any signs of bleeding. Severe thrombocytopenia can cause bleeding in almost any part of the body. Bleeding can lead to a medical emergency and should be treated right away.
External bleeding usually is the first sign of a low platelet count. External bleeding may cause purpura or petechiae. Purpura are purple, brown, and red bruises. This bruising may happen easily and often. Petechiae are small red or purple dots on your skin.
Figure 5. Purpura


Figure 6. Petechiae

Other signs of external bleeding include:
- Prolonged bleeding, even from minor cuts
- Bleeding or oozing from the mouth or nose, especially nosebleeds or bleeding from brushing your teeth
- Abnormal vaginal bleeding (especially heavy menstrual flow)
A lot of bleeding after surgery or dental work also might suggest a bleeding problem.
Heavy bleeding into the intestines or the brain (internal bleeding) is serious and can be fatal. Signs and symptoms include:
- Blood in the urine or stool or bleeding from the rectum. Blood in the stool can appear as red blood or as a dark, tarry color. (Taking iron supplements also can cause dark, tarry stools.)
- Headaches and other neurological symptoms. These problems are very rare, but you should discuss them with your doctor.
Low platelet count causes
Many factors can cause thrombocytopenia (a low platelet count). The condition can be inherited or acquired. “Inherited” means your parents pass the gene for the condition to you. “Acquired” means you aren’t born with the condition, but you develop it. Sometimes the cause of thrombocytopenia isn’t known.
In general, a low platelet count occurs because:
- The body’s bone marrow doesn’t make enough platelets.
- The bone marrow makes enough platelets, but the body destroys them or uses them up.
- The spleen holds on to too many platelets.
A combination of the above factors also may cause a low platelet count.
What causes a low platelet count
The Bone Marrow Doesn’t Make Enough Platelets
Bone marrow is the sponge-like tissue inside the bones. It contains stem cells that develop into red blood cells, white blood cells, and platelets. When stem cells are damaged, they don’t grow into healthy blood cells.
Many conditions and factors can damage stem cells.
- Cancer
Cancer, such as leukemia or lymphoma, can damage the bone marrow and destroy blood stem cells. Cancer treatments, such as radiation and chemotherapy, also destroy the stem cells.
- Aplastic Anemia
Aplastic anemia is a rare, serious blood disorder in which the bone marrow stops making enough new blood cells. This lowers the number of platelets in your blood.
- Toxic Chemicals
Exposure to toxic chemicals—such as pesticides, arsenic, and benzene—can slow the production of platelets.
- Medicines
Some medicines, such as diuretics and chloramphenicol, can slow the production of platelets. Chloramphenicol (an antibiotic) rarely is used in the United States.
Common over-the-counter medicines, such as aspirin or ibuprofen, also can affect platelets.
- Alcohol
Alcohol also slows the production of platelets. A temporary drop in the platelet count is common among heavy drinkers, especially if they’re eating foods that are low in iron, vitamin B12, or folate.
- Viruses
Chickenpox, mumps, rubella, Epstein-Barr virus, or parvovirus can decrease your platelet count for a while. People who have AIDS often develop thrombocytopenia.
- Genetic Conditions
Some genetic conditions can cause low numbers of platelets in the blood. Examples include Wiskott-Aldrich and May-Hegglin syndromes.
The Body Destroys Its Own Platelets
A low platelet count can occur even if the bone marrow makes enough platelets. The body may destroy its own platelets due to autoimmune diseases, certain medicines, infections, surgery, pregnancy, and some conditions that cause too much blood clotting.
- Autoimmune Diseases
Autoimmune diseases occur if the body’s immune system mistakenly attacks healthy cells in the body. If an autoimmune disease destroys the body’s platelets, thrombocytopenia can occur.
One example of this type of autoimmune disease is immune thrombocytopenia (ITP). Immune thrombocytopenia is a bleeding disorder in which the blood doesn’t clot as it should. An autoimmune response is thought to cause most cases of immune thrombocytopenia (ITP).
Normally, your immune system helps your body fight off infections and diseases. But if you have immune thrombocytopenia (ITP), your immune system attacks and destroys its own platelets. Why this happens isn’t known. (ITP also may occur if the immune system attacks your bone marrow, which makes platelets.)
Other autoimmune diseases that destroy platelets include lupus and rheumatoid arthritis.
- Medicines
A reaction to medicine can confuse your body and cause it to destroy its platelets. Examples of medicines that may cause this to happen include quinine; antibiotics that contain sulfa; and some medicines for seizures, such as Dilantin,® vancomycin, and rifampin. (Quinine is a substance often found in tonic water and nutritional health products.)
Heparin is a medicine commonly used to prevent blood clots. But an immune reaction may trigger the medicine to cause blood clots and thrombocytopenia. This condition is called heparin-induced thrombocytopenia (HIT). Heparin-induced thrombocytopenia rarely occurs outside of a hospital.
In heparin-induced thrombocytopenia, the body’s immune system attacks a substance formed by heparin and a protein on the surface of the platelets. This attack activates the platelets and they start to form blood clots.
Blood clots can form deep in the legs (deep vein thrombosis), or they can break loose and travel to the lungs (pulmonary embolism).
- Infection
A low platelet count can occur after blood poisoning from a widespread bacterial infection. A virus, such as mononucleosis or cytomegalovirus, also can cause a low platelet count.
- Surgery
Platelets can be destroyed when they pass through man-made heart valves, blood vessel grafts, or machines and tubing used for blood transfusions or bypass surgery.
- Pregnancy
About 5 percent of pregnant women develop mild thrombocytopenia when they’re close to delivery. The exact cause isn’t known for sure.
- Rare and Serious Conditions That Cause Blood Clots
Some rare and serious conditions can cause a low platelet count. Two examples are thrombotic thrombocytopenic purpura (TTP) and disseminated intravascular coagulation (DIC).
Thrombotic thrombocytopenic purpura (TTP) is a rare blood condition. It causes blood clots to form in the body’s small blood vessels, including vessels in the brains, kidneys, and heart.
Disseminated intravascular coagulation (DIC) is a rare complication of pregnancy, severe infections, or severe trauma. Tiny blood clots form suddenly throughout the body.
In both conditions, the blood clots use up many of the blood’s platelets.
The Spleen Holds On to Too Many Platelets
Usually, one-third of the body’s platelets are held in the spleen. If the spleen is enlarged, it will hold on to too many platelets. This means that not enough platelets will circulate in the blood.
An enlarged spleen often is due to cancer or severe liver disease, such as cirrhosis. Cirrhosis is a disease in which the liver is scarred. This prevents it from working well.
An enlarged spleen also might be due to a bone marrow condition, such as myelofibrosis. With this condition, the bone marrow is scarred and isn’t able to make blood cells.
Low platelet count risk factors
People who are at highest risk for low blood platelet count (thrombocytopenia) are those affected by one of the conditions or factors described above.
This includes people who:
- Have certain types of cancer, aplastic anemia, or autoimmune diseases
- Are exposed to certain toxic chemicals
- Have a reaction to certain medicines
- Have certain viruses
- Have certain genetic conditions
People at highest risk also include heavy alcohol drinkers and pregnant women.
Low blood platelet count prevention
Whether you can prevent low blood platelet count (thrombocytopenia) depends on its specific cause. Usually the condition can’t be prevented. However, you can take steps to prevent health problems associated with thrombocytopenia. For example:
- Avoid heavy drinking. Alcohol slows the production of platelets.
- Try to avoid contact with toxic chemicals. Chemicals such as pesticides, arsenic, and benzene can slow the production of platelets.
- Avoid medicines that you know have decreased your platelet count in the past.
- Be aware of medicines that may affect your platelets and raise your risk of bleeding. Two examples of such medicines are aspirin and ibuprofen. These medicines may thin your blood too much.
- Talk with your doctor about getting vaccinated for viruses that can affect your platelets. You may need vaccines for mumps, measles, rubella, and chickenpox. You may want to have your child vaccinated for these viruses as well. Talk with your child’s doctor about these vaccines.
Low blood platelet count diagnosis
Your doctor will diagnose low blood platelet count (thrombocytopenia) based on your medical history, a physical exam, and test results. A hematologist also may be involved in your care. This is a doctor who specializes in diagnosing and treating blood diseases and conditions.
Once low blood platelet count (thrombocytopenia) is diagnosed, your doctor will begin looking for its cause.
Medical History
Your doctor may ask about factors that can affect your platelets, such as:
- The medicines you take, including over-the-counter medicines and herbal remedies, and whether you drink beverages that contain quinine. Quinine is a substance often found in tonic water and nutritional health products.
- Your general eating habits, including the amount of alcohol you normally drink.
- Your risk for AIDS, including questions about blood transfusions, sexual partners, intravenous (IV) drugs, and exposure to infectious blood or bodily fluids at work.
- Any family history of low platelet counts.
Physical Exam
Your doctor will do a physical exam to look for signs and symptoms of bleeding, such as bruises or spots on the skin. He or she will check your abdomen for signs of an enlarged spleen or liver. You also will be checked for signs of infection, such as a fever.
Diagnostic Tests
Your doctor may recommend one or more of the following tests to help diagnose a low platelet count.
- Complete Blood Count
A complete blood count (CBC) measures the levels of red blood cells, white blood cells, and platelets in your blood. For this test, a small amount of blood is drawn from a blood vessel, usually in your arm.
If you have thrombocytopenia, the results of this test will show that your platelet count is low.
- Blood Smear
A blood smear is used to check the appearance of your platelets under a microscope. For this test, a small amount of blood is drawn from a blood vessel, usually in your arm.
- Bone Marrow Tests
Bone marrow tests check whether your bone marrow is healthy. Blood cells, including platelets, are made in your bone marrow. The two bone marrow tests are aspiration and biopsy.
Bone marrow aspiration might be done to find out why your bone marrow isn’t making enough blood cells. For this test, your doctor removes a sample of fluid bone marrow through a needle. He or she examines the sample under a microscope to check for faulty cells.
A bone marrow biopsy often is done right after an aspiration. For this test, your doctor removes a sample of bone marrow tissue through a needle. He or she examines the tissue to check the number and types of cells in the bone marrow.
- Other Tests
If a bleeding problem is suspected, you may need other blood tests as well. For example, your doctor may recommend Prothrombin Time (PT) and Partial Thromboplastin Time (PTT) tests to see whether your blood is clotting properly.
Your doctor also may suggest an ultrasound to check your spleen. An ultrasound uses sound waves to create pictures of your spleen. This will allow your doctor to see whether your spleen is enlarged.
Low platelet count treatment
Treatment for thrombocytopenia depends on its cause and severity. The main goal of treatment is to prevent death and disability caused by bleeding.
If your condition is mild, you may not need treatment. A fully normal platelet count isn’t necessary to prevent bleeding, even with severe cuts or accidents.
Thrombocytopenia often improves when its underlying cause is treated. People who inherit the condition usually don’t need treatment.
If a reaction to a medicine is causing a low platelet count, your doctor may prescribe another medicine. Most people recover after the initial medicine has been stopped. For heparin-induced thrombocytopenia (HIT), stopping the heparin isn’t enough. Often, you’ll need another medicine to prevent blood clotting.
If your immune system is causing a low platelet count, your doctor may prescribe medicines to suppress the immune system.
Severe Thrombocytopenia
If your thrombocytopenia is severe, your doctor may prescribe treatments such as medicines, blood or platelet transfusions, or splenectomy.
Treating the underlying cause of thrombocytopenia
If your doctor can identify a condition or a medication that’s causing your thrombocytopenia, addressing that cause may clear up your thrombocytopenia
For example, if you have heparin-induced thrombocytopenia, your doctor will direct you to stop using heparin and prescribe a different blood-thinning drug. Your thrombocytopenia may persist for a week or more despite stopping all heparin therapy.
Medicines
Your doctor may prescribe corticosteroids, also called steroids for short. Steroids may slow platelet destruction. These medicines can be given through a vein or by mouth. One example of this type of medicine is prednisone.
The steroids used to treat thrombocytopenia are different from illegal steroids taken by some athletes to enhance performance.
Your doctor may prescribe immunoglobulins or medicines like rituximab to block your immune system. These medicines are given through a vein. He or she also may prescribe other medicines, such as eltrombopag or romiplostim, to help your body make more platelets. The former comes as a tablet to take by mouth and the latter is given as an injection under the skin.
Blood or Platelet Transfusions
Blood or platelet transfusions are used to treat people who have active bleeding or are at a high risk of bleeding. During this procedure, a needle is used to insert an intravenous (IV) line into one of your blood vessels. Through this line, you receive healthy blood or platelets.
For more information about this procedure, go to the Blood Transfusion article.
Splenectomy
A splenectomy is surgery to remove the spleen. This surgery may be used if treatment with medicines doesn’t work. This surgery mostly is used for adults who have immune thrombocytopenia (ITP). However, medicines often are the first course of treatment.
Plasma exchange
Thrombotic thrombocytopenic purpura (TTP) can result in a medical emergency requiring plasma exchange.
Living with Low platelet count
If you have low blood platelet count (thrombocytopenia), watch for any signs and symptoms of bleeding. Report these signs and symptoms to your doctor right away.
Symptoms can appear suddenly or over time. Severe low blood platelet count (thrombocytopenia) can cause bleeding in almost any part of the body. Bleeding can lead to a medical emergency and should be treated right away.
You can take steps to avoid health problems associated with low blood platelet count (thrombocytopenia). Be aware of the medicines you’re taking, avoid injuries, and contact your doctor if you have a fever or other signs or symptoms of an infection.
Medicines
Avoid medicines that may affect your platelets and raise your risk of bleeding. Two examples of such medicines are aspirin and ibuprofen. These medicines may thin your blood too much. Be careful when using over-the-counter medicines—many contain aspirin or ibuprofen.
Tell your doctor about all of the medicines you take, including over-the-counter medicines, vitamins, supplements, and herbal remedies.
Injuries
Avoid injuries that can cause bruising and bleeding. Don’t take part in contact sports such as boxing, football, or karate. These sports are likely to lead to injuries that can cause bleeding.
Other sports, such as skiing or horseback riding, also put you at risk for injuries that can cause bleeding. Ask your doctor about physical activities that are safe for you.
Take safety precautions, such as using a seatbelt while riding in a car and wearing gloves when working with knives and other tools.
If your child has low blood platelet count (thrombocytopenia), try to protect him or her from injuries, especially head injuries that can cause bleeding in the brain. Ask your child’s doctor whether you need to restrict your child’s activities.
Infection
If you’ve had your spleen removed, you may be more likely to become ill from certain types of infection. Watch for fever or other signs of infection and report them to your doctor promptly. People who have had their spleens removed may need vaccines to prevent certain infections.





{kind=link}