
Contents
What is Poland syndrome
Poland syndrome is a rare condition that is evident at birth (congenital). Poland syndrome is characterized by an underdeveloped or absent chest muscle on one side of the body, absence of the breastbone portion (sternal) of the chest muscle, and webbing of the fingers of the hand on the same side 1). The cause of Poland syndrome is not known. Poland syndrome is nearly always sporadic. Poland syndrome tends to occur on the right side and is more common in boys than girls 2). Treatment typically involves surgical correction of the chest wall deformities 3).
Poland syndrome is thought to be under-reported and under-diagnosed, making the exact incidence of the condition difficult to determine. Some men remain undiagnosed unless they seek treatment for associated hand abnormalities when present; other individuals may not realize they have features of the condition until puberty 4). It has been estimated that the incidence of Poland syndrome is about 1 in 30,000 5). However, it has also been reported that the incidence ranges from 1 in 7,000 to 1 in 100,000, depending on the severity of the condition and the patient population 6).
A current search of the available literature does not yield reliable statistics specific to the incidence or prevalence of Poland syndrome in the United States. If the estimated incidence of 1 in 30,000 were applied to the U.S. population size, over 10,000 people in the U.S. would have Poland syndrome. However, data confirming these statistics in the U.S. are not currently available.
Management of Poland syndrome may include surgical correction of the chest wall deformities 7). Surgical options are available to improve appearance in both males and females 8). In females, breast reconstruction is typically performed at the time of normal full breast development and can be planned in conjunction with or following reconstruction of the chest wall 9). In males reconstruction of the chest may not be necessary if there is no underlying chest wall deformity. The optimal surgical approach will vary from patient to patient. Surgical options should be discussed with a surgeon familiar with reconstructive surgery in people with Poland syndrome 10).
Figure 1. Poland syndrome breast

Figure 2. Poland syndrome hand
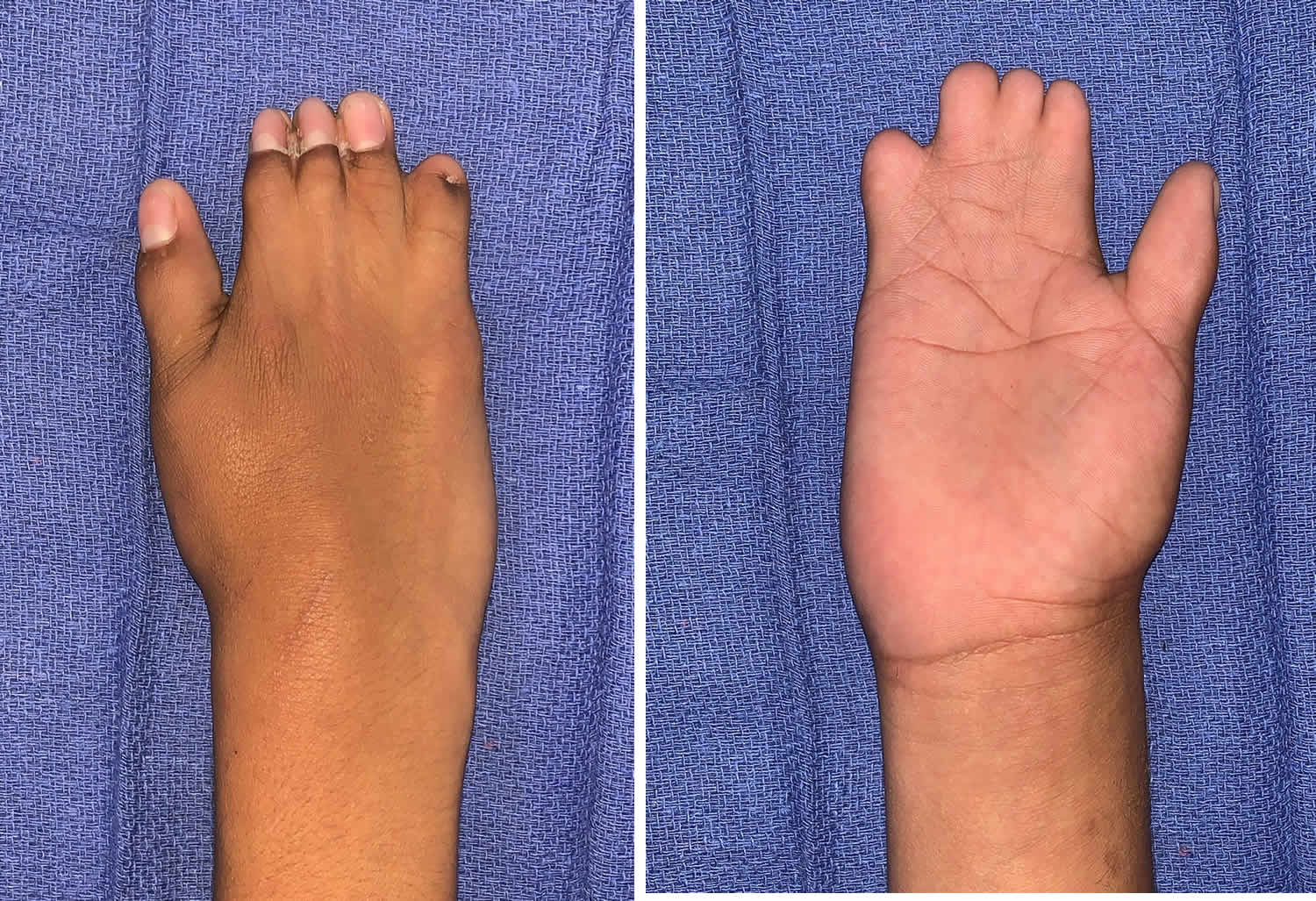
Figure 3. Poland syndrome female
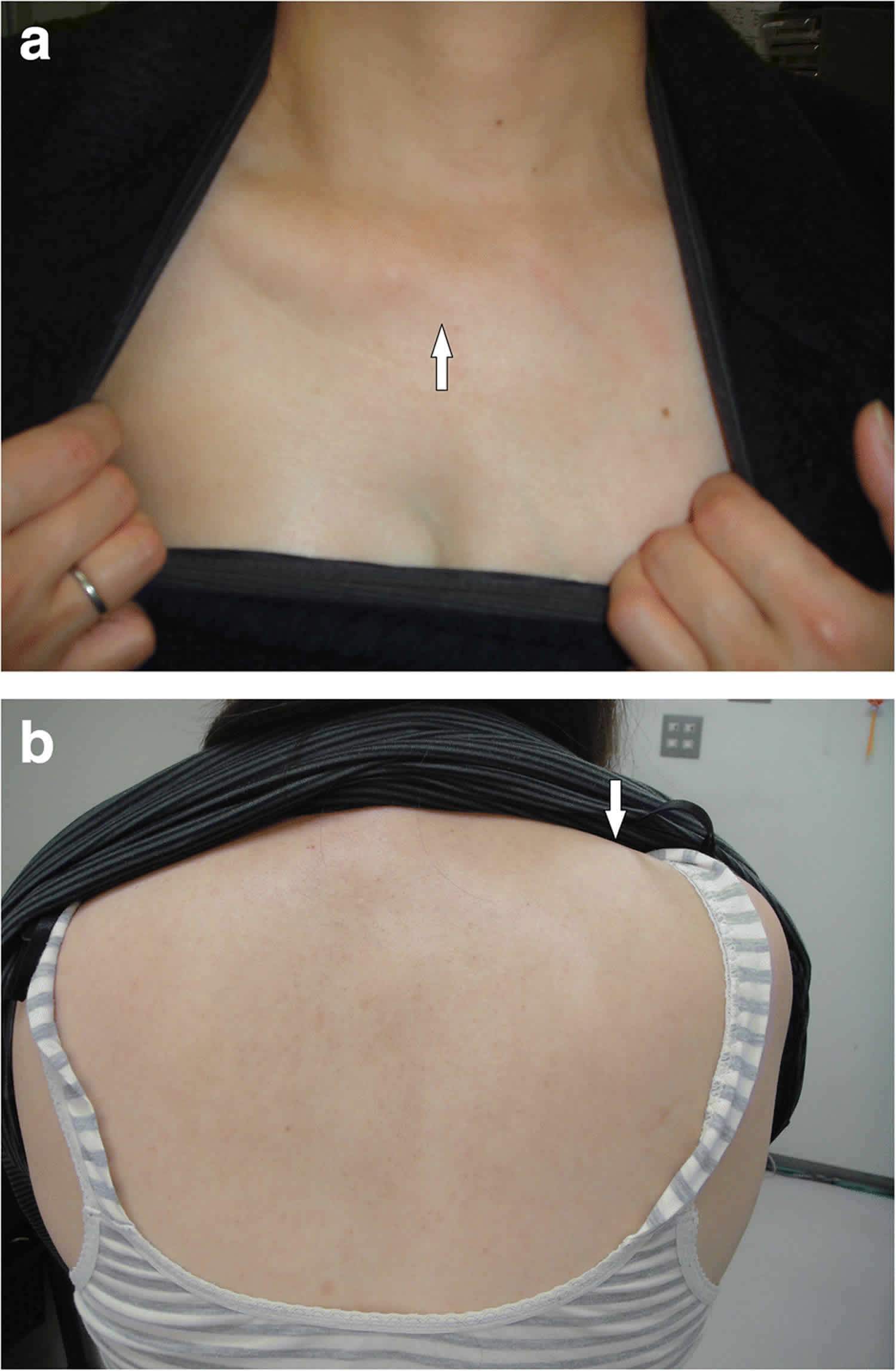
Footnote: (a) Absence of the sternal head of the pectoralis major (white arrow); (b) Protrusion of the right scapula (white arrow). A 45-year-old Japanese woman, an out-patient, underwent an emergency examination for intense left lower abdominal pain. Computed tomography images revealed a hydronephrotic left kidney and dilatation of the left ureter. No ureteral calculus or neoplasm was found. In addition, no abnormalities connected to her left abdominal pain were found. Nephritis was diagnosed based on the results of urine analysis, and a course of antibiotics was administered. Computed tomography images also revealed a history of breast reconstruction with a custom-made silicone implant in her right breast. The present case showed symptoms of Poland syndrome, which were absence of the sternal head of the right pectoralis major and asymmetrical malformation of the chest wall due to hypoplasia of the right rib cage. In addition to typical Poland syndrome symptoms, she had hypoplasia of her right kidney, hypoplasia of the right gluteus minimus muscle, right-sided pelvic hypoplasia, spinal curvature to the right, and a cystic mass in her right ovary.
[Source 11) ]Poland syndrome causes
The cause of Poland syndrome is unknown. According to reports in the medical literature, an overwhelming majority of cases appear to occur randomly for unknown reasons (sporadically) in the absence of a family history. Researchers have suggested that it may result from a disruption of blood flow during development before birth. This disruption is thought to occur at about the sixth week of embryonic development and affect blood vessels that will become the subclavian and vertebral arteries on each side of the body. The arteries normally supply blood to embryonic tissues that give rise to the chest wall and hand on their respective sides. Variations in the site and extent of the disruption may explain the range of signs and symptoms that occur in Poland syndrome. Abnormality of an embryonic structure called the apical ectodermal ridge, which helps direct early limb development, may also be involved in Poland syndrome.
Rare cases of Poland syndrome are thought to be caused by a genetic change that can be passed down in families, but no related genes have been identified. Some researchers suggest that apparently familial cases may result from inherited susceptibility to a certain event or anomaly (such as early interruption of blood flow) that may predispose to the syndrome (see directly below).
Poland syndrome is sometimes referred to as Poland sequence. A “sequence” (or anomalad) refers to a pattern of malformations derived from a single anomaly. According to some investigators, the primary defect in Poland Syndrome may be impaired development of a certain artery or other mechanical factors that may result in diminished or interrupted blood flow during early embryonic growth. The term “Subclavian Artery Supply Disruption Sequence” (SASDS) 12) has been suggested for a group of conditions that may occur due to disruption of blood flow through particular arteries (i.e., subclavian artery, vertebral artery, and/or their branches) at or around the sixth week of embryonic development. Such conditions include Poland Syndrome, Moebius Syndrome 13), Klippel-Feil Syndrome, and Sprengel deformity 14). The specific pattern of defects that results is thought to depend on the particular site and degree of the diminished blood flow.
Poland syndrome inheritance pattern
Most cases of Poland syndrome are sporadic, which means they are not inherited and occur in people with no history of the disorder in their families. Rarely, this condition is passed through generations in families. In these families the condition appears to be inherited in an autosomal dominant pattern, which means one copy of an altered gene in each cell is sufficient to cause the disorder, although no associated genes have been found.
Poland syndrome symptoms
Poland syndrome associated symptoms and features are extremely variable from case to case, including in rare cases in which more than one family member has been affected. For example, in some reported cases, one sibling has had all major features of the condition, while the other sibling has had only absence of pectoral muscle or hand involvement. However, Poland syndrome is most commonly characterized by absence (aplasia) of chest wall muscles on one side of the body (unilateral) and abnormally short, webbed fingers (symbrachydactyly) of the hand on the same side (ipsilateral). In approximately 75 percent of cases, such abnormalities affect the right side of the body.
In most affected individuals with Poland syndrome, there is typically unilateral absence of the pectoralis minor and the sternal or breastbone portion of the pectoralis major. The pectoralis major, a large fanlike muscle of the upper chest wall, arises from the breastbone (sternum), the collarbone (clavicle), and cartilages of the second to the sixth ribs; it acts on the joint of the shoulder, functioning to move the arm across the body. The pectoralis minor is a thin, triangular muscle beneath the pectoralis major. This muscle arises from the third to fifth ribs and functions to rotate the shoulder blade (scapula) and move it forward and down.
In some individuals with Poland Syndrome, there may also be unilateral absence of other regional muscles, such as certain large muscles of the back (latissimus dorsi) and/or a thin muscle of the chest wall that extends from ribs under the arm to the scapula (serratus anterior).
Affected individuals may have variable associated features, such as underdevelopment or absence of one nipple (including the darkened area around the nipple [areola]) and/or patchy absence of hair growth under the arm (axilla). In females, there may be underdevelopment or absence (aplasia) of one breast and underlying (subcutaneous) tissues.
In some cases, associated skeletal abnormalities may also be present, such as underdevelopment or absence of certain upper ribs and the bars of cartilage (costal cartilages) by which the ribs are attached to the sternum. In addition, in some cases, there may be abnormal elevation and/or underdevelopment of the shoulder blade (scapula) and the development of a lump at the base of the neck due to elevation of the scapula, a condition known as Sprengel deformity.
As noted above, most individuals with Poland Syndrome also have involvement of the hand on the affected side of the body. Certain bones of the fingers (phalanges) are underdeveloped or absent, resulting in abnormally short fingers (brachydactyly). In addition, in most cases, there is webbing (syndactyly) of certain fingers, particularly the index and middle fingers. In addition, in some cases, affected individuals may have abnormal shortening of the arm, with underdevelopment of the forearm bones on the thumb and pinky sides of the forearm (i.e., radius and ulna) on the affected side.
Poland syndrome diagnosis
The severity of Poland syndrome differs from person to person. As a result it is not often diagnosed or reported. Sometimes, a person does not realize they have the condition until puberty, when lopsided (asymmetrical) growth makes it more obvious 15). The diagnosis of Poland syndrome is usually made at birth based upon characteristic physical findings, a thorough clinical evaluation, and a variety of specialized tests. During the examination, the stage of breast development and of the latissimus dorsi muscle (one of the largest muscle of the back) should be noted. Other exams may be needed to rule out other problems such as Moebius syndrome 16).
Imaging Tests
Tests may include advanced imaging techniques, such as a CT scan that can determine the extent to which the muscles may be affected. During CT scanning, a computer and X-rays are used to create a film showing cross-sectional images particular organs or structures within the body. X-ray studies may be used to help identify and characterize specific abnormalities in the hands, forearms, ribs, and/or shoulder blades.
Poland syndrome treatment
The treatment of Poland syndrome is directed toward the specific symptoms that are apparent in each individual. Treatment may require the coordinated efforts of a team of specialists. Plastic surgery may be performed to rebuild the chest wall and to graft ribs into their proper places. In females, plastic surgery may also be performed to construct a breast mound. In some cases, surgery may also be performed to help correct skeletal abnormalities affecting other areas of the body such as the hands. Physical therapy may also be prescribed to help improve any limitations of motion.
Genetic counseling will be of benefit for affected individuals and their families. Other treatment for Poland syndrome is symptomatic and supportive.
Poland syndrome surgery
In female teenagers, abnormal breast development can influence the patient’s psychological growth. However, if the reconstruction is performed too early, asymmetry may result with continued growth of the breasts. In this case, a secondary revision procedure may be required once breast development is completed, but this compromises the overall result. When the young female patient experiences intense anxiety associated with the breast deformity, one may consider early treatment with a temporary expander, planning for additional reconstruction once breast development has been completed.
During adolescence, a subcutaneous tissue expander can be placed in the affected side. The expander is placed in the subcutaneous plane, since the pectoralis muscle is absent. This expander can be inflated at intervals to rival or match the development of the unaffected breast. This expanded breast does not exactly match the uninvolved side but may help the patient look more symmetrical. Placement of the expander during breast development allows for expansion of the skin to accommodate the eventual permanent implant and latissimus muscle. Moreover, this expansion of the breast skin may enlarge the hypoplastic nipple-areola complex often present in these patients. Tissue expansion also can correct the eccentric and elevated NAC observed in patients with Poland syndrome through strategic expander placement to lower it 17). Tissue expansion can be performed with a pure temporary tissue expander that is eventually replaced with a permanent implant or with an permanent implant expander.
If the patient has mild breast asymmetry, breast reconstruction with an implant expander can be considered in a one-stage procedure. As described above, an implant expander is a permanent implant with a removable remote port. The implant expander can be incrementally expanded postoperatively until the desired size is achieved to match the other breast. Then, the port of the expander can be removed through a separate incision while the permanent implant is left in place. The most popular implant expander is the Becker implant, which contains silicone gel and saline. The saline component of this implant allows for adjustable expansion.
Occasionally, with long periods of implant inactivity between expansions, a capsule contracture may develop, which can restrict expansion. An open capsulotomy may be required to release the capsule and allow for further tissue expansion and or implant repositioning. Finally, upon completion of breast development (when the patient is aged 18-19 years), the tissue expander can be removed and the breast can be reconstructed with the latissimus muscle transposed over a permanent implant.
The latissimus muscle can be used to correct the absence of the axillary line, correct infraclavicular flattening, and provide subcutaneous filler to cover the edge of the implant, thus preventing or minimizing rippling. Occasionally, a de-epithelialized skin paddle may be required with the latissimus muscle to reconstruct the axillary line. If the nipple is absent the skin paddle of the latissimus muscle can be used to reconstruct a nipple, and the areola can be reconstructed with tattooing.
The latissimus muscle is harvested through a small axillary incision and a transverse incision in the back, which can be concealed in the bra line. The muscle is transposed anteriorly over the breast implant and sutured to the pectoralis fascia superiorly, medially, and inferiorly. The use of the latissimus is saved until the completion of breast development and tissue expansion; if used earlier over the tissue expander, the muscle is attenuated with expansion. If skin is required with muscle harvest, the back incision can be modified to recruit as much skin as needed, making sure to still be able to close the back primarily.
When striving to achieve breast symmetry at the final operation, treatment of the contralateral breast by reduction, mastopexy, or augmentation may be indicated. Furthermore, over time, the patient may develop a unilateral contracture to the breast prosthesis, resulting in loss of symmetry. Accordingly, long-term symmetry may be optimized by placement of an implant in the unaffected breast, as well. If the unaffected breast is excessively large, it may require a reduction or mastopexy as an adjunct to implant insertion.
If tissue expansion does not correct nipple-areola asymmetry, additional procedures may be needed to correct nipple and areolar size and location. Consider nipple-sharing composite grafts if the unaffected nipple is of adequate size, or consider nipple reconstruction with local flaps. Areolar discrepancies can be corrected with crescent excisions, strategic tattooing, or relocation by transposing through a new skin opening and skin closure of old location. These nipple-areolar reconstruction procedures are usually performed at a separate stage after the maturation from the initial reconstructive procedure.
If the latissimus is absent as part of the Poland syndrome complex, other options for reconstruction include free latissimus muscle from the unaffected side, the transverse rectus abdominus muscle (TRAM) flap, Rubens flap, gluteus maximus flap, thigh flap, or free perforator transverse rectus abdominus muscle (TRAM) or gluteus flaps. Because thoracic vascular anomalies also can be encountered in patients with Poland syndrome, assessment of recipient vessels with duplex or angiogram is required 18). Another described reconstructive option is a customized prosthetic implant for the chest wall placed under the breast implant 19).
The transverse rectus abdominus muscle (TRAM) flap should not be considered for those who intend to become pregnant. The gluteus and Rubens flaps have short pedicles, often requiring grafts for microanastomoses, and result in significant donor site asymmetry. In general, these other reconstructive options provide less aesthetically acceptable results than the latissimus muscle for coverage over the implant; however, treatment must be individualized.
For male patients with Poland syndrome who have an intact latissimus muscle, consider reconstruction when they are aged 12-13 years. The ipsilateral latissimus muscle is harvested through a small incision in the back and axilla and transposed to fill the void of the absent pectoralis major muscle. The latissimus is folded along the sternal and inferior borders to resemble the contour of the pectoralis major muscle. The humeral insertion of the latissimus muscle must be detached, anteriorly transposed, and sutured to the bicipital groove of the humerus. Reconstruction with prosthesis also has been described for males but with disappointing results. If the latissimus is absent on the affected side, the contralateral latissimus can be used as a free flap to the axillary or internal mammary vessels after appropriate evaluation for recipient vessels with duplex or angiogram.
Insertion of the tissue expander or single-stage implant expander is usually performed on an outpatient basis. The patient’s follow-up care is initially for wound evaluation. Then, patients return at 2 weeks for possible suture removal and the initial expansion, if wound healing is suitable. Tissue expansion then is performed at weekly to biweekly intervals until the affected breast matches the contralateral side. The affected breast is expanded further as the unaffected breast grows.
Patients with moderate to severe abnormalities may require 2-stage reconstruction with the latissimus muscle over the permanent implant. The second procedure, involving expander exchange to permanent implant and latissimus muscle reconstruction, involves placement of drains in the donor site and breast pocket. An elastic wrap (eg, Ace) is used to minimize potential space at the donor site and risk of hematoma or seroma. Drain care can be performed at home. These drains are removed when outputs are less than 25 mL over 24 hours. Expansion exercises of the implants can usually be initiated at 1-4 weeks to minimize risk for capsule contracture.
A study by Manzano Surroca et al. 20) indicated that the use of free autologous fat grafts a year or more after breast implant surgery may improve reconstructive results in females with Poland syndrome. In the study, 6 females with the syndrome underwent free autologous fat grafting 11-18 months after receiving breast implants, with the contralateral breast also treated in order to improve symmetry and volume. The investigators concluded that fat grafting permits correction of the anterior axillary fold and improves the projection and symmetry of the breasts.
Surgical complications
Any of the complications described for breast reconstruction with implants and autogenous tissue can be experienced in the reconstruction of patients with Poland syndrome, including seroma 21) or hematoma around the implant, implant displacement, implant deflation, implant defect, implant infection, implant exposure, requirement for removal of implant, contracture, breast asymmetry immediate or late, progressive change in symmetry, drooping of the breasts, loss of feeling of the breast or nipple, need for displacement mammography, difficulty with breast cancer surveillance, galactorrhea, symmastia, difficulty with breast feeding, nipple asymmetry, rippling, contour abnormalities, inability to guarantee bra size, painful unattractive scarring, flap loss, muscle atrophy, latissimus donor site seroma and hematoma, back asymmetry from latissimustransposition, and need for additional revisions 22).
Poland syndrome surgery contraindications
Breast implants and expanders should not be placed in patients who are too young to maturely accept the responsibility of a foreign body and to have the ability to deal with the potential complications. Patients must be able to tolerate occasional expansion procedures. Remote port tissue expanders may be preferred for younger patients. Integrated port tissue expanders can be used in young patients with an increased risk of deflation because the actual implant can be punctured in attempting to access the port in a moving target.
Poland syndrome prognosis
With appropriate timing, procedure selection, preoperative evaluation, and preoperative discussion to give appropriate expectations, excellent results and high patient satisfaction can be achieved in the treatment of chest and breast deformities resulting from Poland syndrome. Through the early use of tissue expansion, breast growth can be achieved to rival or match the normal development on the unaffected side. Tissue expansion prepares the breast envelope for the autogenous reconstruction and permanent implant and can sometimes improve nipple and areolar irregularities as well. Finally, upon completion of breast development, the latissimus muscle can be used to reconstruct the axillary line, reconstruct the infraclavicular hollow, and provide implant coverage.
References [ + ]





{kind=link}