
Contents
- What is renal cell carcinoma
- About the kidneys
- Renal cell carcinoma symptoms
- Renal cell carcinoma causes
- Renal cell carcinoma prevention
- Renal cell carcinoma diagnosis
- Renal cell carcinoma staging
- Renal cell carcinoma prognosis
- Renal cell carcinoma treatment
- Treatment Choices by Stage for renal cell carcinoma
- Surgery for renal cell carcinoma
- Ablation and Other Local Therapy for renal cell carcinoma
- Active Surveillance for renal cell carcinoma
- Radiation Therapy for renal cell carcinoma
- Targeted Therapies for renal cell carcinoma
- Immunotherapy for renal cell carcinoma
- Chemotherapy for renal cell carcinoma
What is renal cell carcinoma
Renal cell carcinoma also known as renal cell cancer or renal cell adenocarcinoma, is by far the most common type of kidney cancer. About 9 out of 10 kidney cancers are renal cell carcinomas. Other types of kidney cancers include transitional cell carcinomas, Wilms tumors, and renal sarcomas.
Although renal cell carcinoma usually grows as a single tumor within a kidney, sometimes there are 2 or more tumors in one kidney or even tumors in both kidneys at the same time.
There are several subtypes of renal cell carcinoma, based mainly on how the cancer cells look under a microscope. Knowing the subtype of renal cell carcinoma can be a factor in deciding treatment and can also help your doctor determine if your cancer might be due to an inherited genetic syndrome.
Clear cell renal cell carcinoma: this is the most common form of renal cell carcinoma. About 7 out of 10 people with renal cell carcinoma have this kind of cancer. When seen under a microscope, the cells that make up clear cell renal cell carcinoma look very pale or clear.
Papillary renal cell carcinoma: this is the second most common subtype – about 1 in 10 renal cell carcinomas are of this type. These cancers form little finger-like projections (called papillae) in some, if not most, of the tumor. Some doctors call these cancers chromophilic because the cells take in certain dyes and look pink under the microscope.
Chromophobe renal cell carcinoma: this subtype accounts for about 5% (5 cases in 100) of renal cell carcinomas. The cells of these cancers are also pale, like the clear cells, but are much larger and have certain other features that can be recognized when looked at with a microscope .
Rare types of renal cell carcinoma: these subtypes are very rare, each making up less than 1% of renal cell carcinomas:
- Collecting duct renal cell carcinoma
- Multilocular cystic renal cell carcinoma
- Medullary carcinoma
- Mucinous tubular and spindle cell carcinoma
- Neuroblastoma-associated renal cell carcinoma
Unclassified renal cell carcinoma: rarely, renal cell cancers are labeled as unclassified because the way they look doesn’t fit into any of the other categories or because there is more than one type of cell present.
About the kidneys
To understand more about renal cell carcinoma, it helps to know about the kidneys and what they do.
The kidneys are a pair of bean-shaped organs, each about the size of a fist. They are attached to the upper back wall of the abdomen and protected by the lower rib cage. One kidney is just to the left and the other just to the right of the backbone.
Small glands called adrenal glands sit above each of the kidneys. Each kidney and adrenal gland is surrounded by fat and a thin, fibrous layer known as Gerota’s fascia.
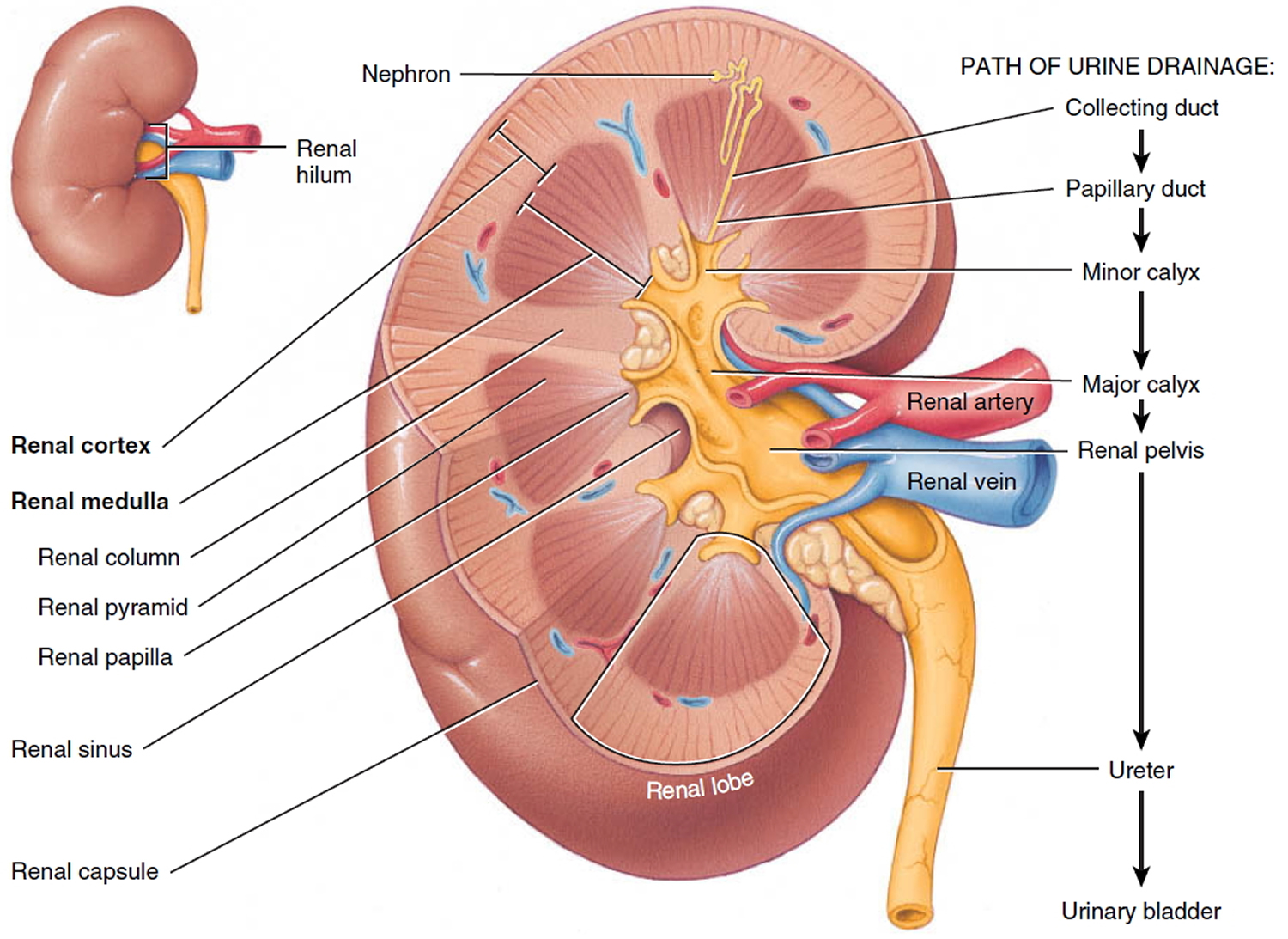
The kidneys’ main job is to filter the blood coming in from the renal arteries to remove excess water, salt, and waste products. These substances become urine. Urine leaves the kidneys through long slender tubes called ureters which connect to each kidney at an area called the renal pelvis. Urine travels down the ureters to the bladder, where it is stored until you urinate (pee).
The kidneys also have other jobs:
- They help control blood pressure by making a hormone called renin.
- They help make sure the body has enough red blood cells by making a hormone called erythropoietin (EPO). This hormone tells the bone marrow to make more red blood cells.
Your kidneys are important, but you can function with only one kidney. Many people in the United States are living normal, healthy lives with just one kidney.
Some people do not have any working kidneys at all, and survive with the help of a medical procedure called dialysis. The most common form of dialysis uses a specially designed machine that filters blood much like a real kidney would.
Figure 1. Kidney location
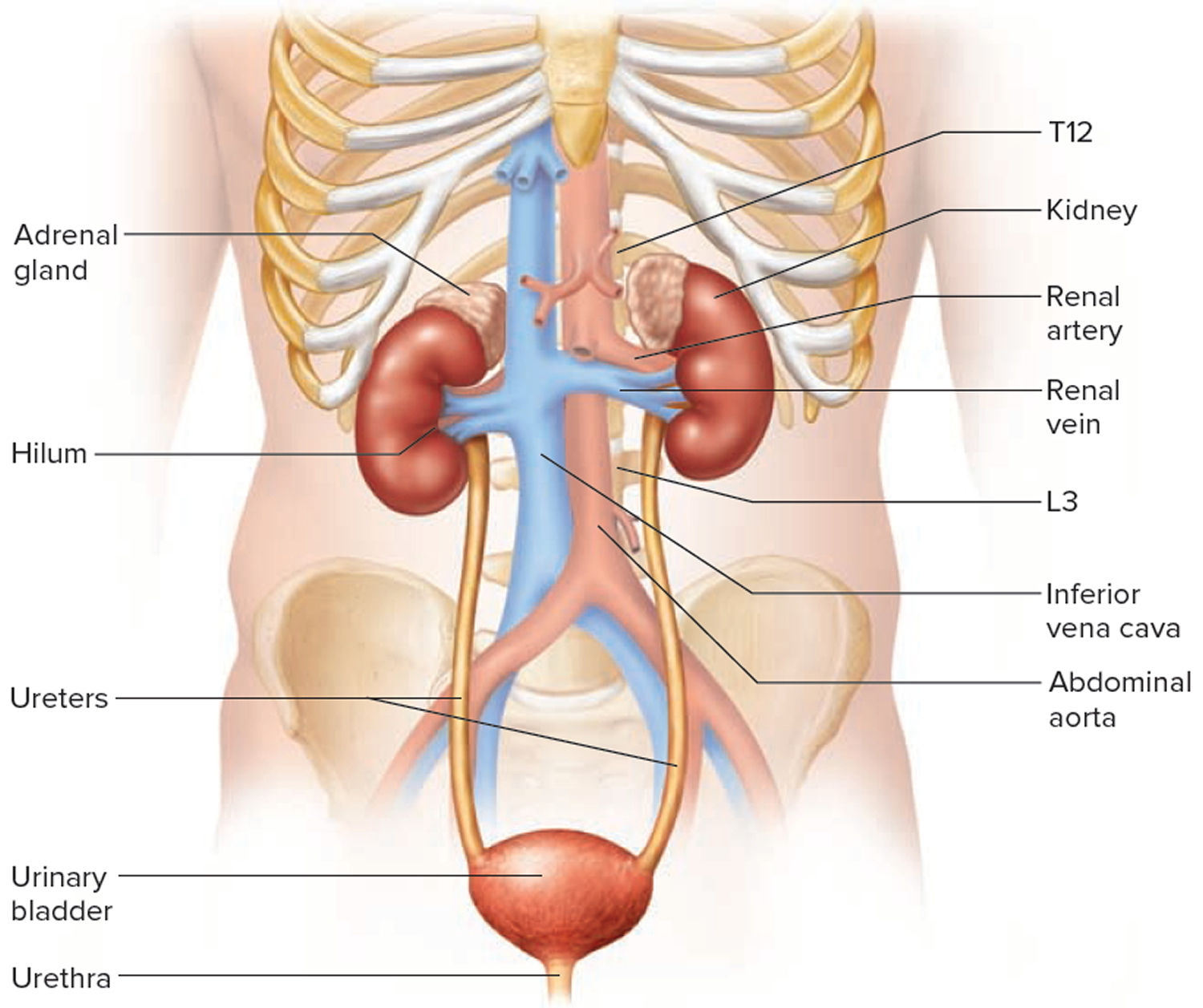
Figure 2. Kidney location (transverse section)
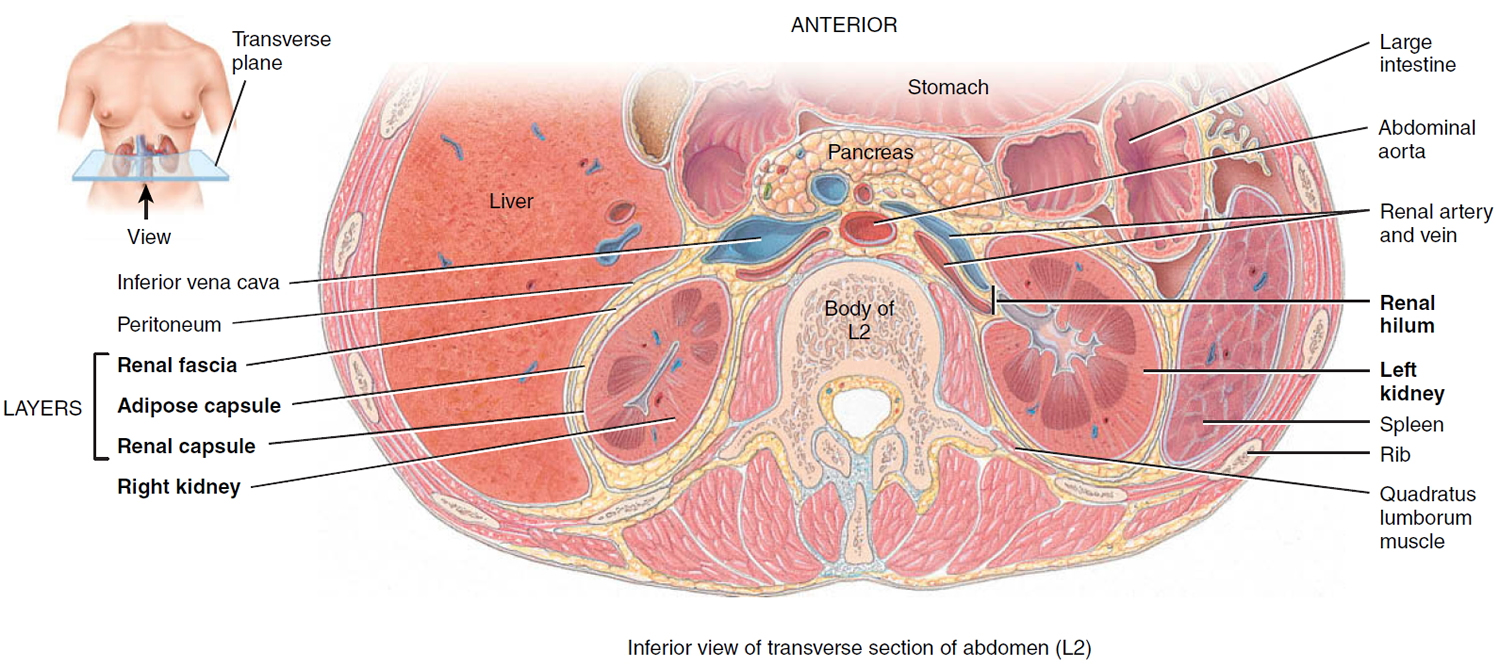
Figure 3. Kidney anatomy
Renal cell carcinoma symptoms
Early renal cell carcinoma do not usually cause any signs or symptoms, but larger ones might. Some possible signs and symptoms of kidney cancer include:
- Blood in the urine (hematuria)
- Low back pain on one side (not caused by injury)
- A mass (lump) on the side or lower back
- Fatigue (tiredness)
- Loss of appetite
- Weight loss not caused by dieting
- Fever that is not caused by an infection and that doesn’t go away
- Anemia (low red blood cell counts)
These signs and symptoms can be caused by renal cell carcinoma (or another type of cancer), but more often they are caused by other, benign, diseases. For example, blood in the urine is most often caused by a bladder or urinary tract infection or a kidney stone. Still, if you have any of these symptoms, see a doctor so that the cause can be found and treated, if needed.
Renal cell carcinoma causes
Although many risk factors can increase the chance of developing renal cell cancer, it is not yet clear how some of these risk factors cause kidney cells to become cancerous.
Changes (mutations) in genes
Cancer is caused by changes in the DNA inside our cells. DNA is the chemical in our cells that makes up our genes, which control how our cells function. DNA, which comes from both our parents, affects more than just how we look.
Some genes help control when our cells grow, divide into new cells, and die:
- Certain genes that help cells grow, divide, and stay alive are called oncogenes.
- Genes that help keep cell division under control or cause cells to die at the right time are called tumor suppressor genes.
Cancers can be caused by DNA mutations (changes) that turn on oncogenes or turn off tumor suppressor genes, resulting in cells growing out of control. Changes in many different genes are usually needed to cause kidney cancer.
Inherited gene mutations
Certain inherited DNA changes can lead to conditions running in some families that increase the risk of kidney cancer. These syndromes, which cause a small portion of all kidney cancers, were described in risk factors for renal cell carcinoma.
For example, VHL, the gene that causes von Hippel-Lindau (VHL) disease, is a tumor suppressor gene. It normally helps keep cells from growing out of control. Mutations (changes) in this gene can be inherited from parents. When the VHL gene is mutated, it is no longer able to control the abnormal growth, and kidney cancer is more likely to develop. The genes linked to hereditary leiomyoma (the FH gene), Birt-Hogg-Dube syndrome (the FLCN gene), and familial renal cancer (the SDHB and SDHD genes) are also tumor suppressor genes, and inherited changes in these genes lead to an increased risk of kidney cancer.
People with hereditary papillary renal cell carcinoma have inherited changes in the MET oncogene that cause it to be turned on all the time. This can lead to uncontrolled cell growth and makes the person more likely to develop papillary renal cell carcinoma.
Special genetic tests can detect some of the gene mutations associated with these inherited syndromes. If you have a family history of kidney cancer or other cancers linked to these syndromes, you may want to ask your doctor about genetic counseling and genetic testing.
Acquired gene mutations
Some gene mutations happen during a person’s lifetime and are not passed on. They affect only cells that come from the original mutated cell. These DNA changes are due to acquired mutations.
In most cases of kidney cancer, the DNA mutations that lead to cancer are acquired during a person’s life rather than having been inherited. Certain risk factors, such as exposure to cancer-causing chemicals (like those found in tobacco smoke), probably play a role in causing these acquired mutations, but so far it’s not known what causes most of them. Progress has been made in understanding how tobacco increases the risk for developing kidney cancer. Your lungs absorb many of the cancer-causing chemicals in tobacco smoke into the bloodstream. Because your kidneys filter this blood, many of these chemicals become concentrated in the kidneys. Several of these chemicals are known to damage kidney cells in ways that can cause the cells to become cancerous.
Obesity, another risk factor for this cancer, alters the balance of some of the body’s hormones. Researchers are now learning how certain hormones help control the growth (both normal and abnormal) of many different tissues in the body, including the kidneys.
Most people with sporadic (non-inherited) clear cell renal cell carcinoma have changes in the VHL gene in their tumor cells that have caused it to stop working properly. These changes are acquired during life rather than being inherited.
Other gene changes may also cause renal cell carcinomas. Researchers continue to look for these changes.
Risk factors for renal cell carcinoma
A risk factor is anything that affects your chance of getting a disease such as cancer. Different cancers have different risk factors. Some risk factors, like smoking, can be changed. Others, like your age or family history, can’t be changed.
But having a risk factor, or even several risk factors, does not mean that you will get the disease. And some people who get the disease may have few or no known risk factors. Even if a person with renal cell carcinoma has a risk factor, it is often very hard to know how much that risk factor contributed to the cancer.
Scientists have found several risk factors that could make you more likely to develop renal cell carcinoma.
Smoking
Smoking increases the risk of developing renal cell carcinoma. The increased risk seems to be related to how much you smoke. The risk drops if you stop smoking, but it takes many years to get to the risk level of someone who never smoked.
Obesity
People who are very overweight have a higher risk of developing renal cell carcinoma. Obesity may cause changes in certain hormones that can lead to renal cell carcinoma.
Workplace exposures
Many studies have suggested that workplace exposure to certain substances increases the risk for renal cell carcinoma. Some of these substances are cadmium (a type of metal), some herbicides, and organic solvents, particularly trichloroethylene.
Family history of renal cell carcinoma
People with a strong family history of renal cell cancer (without one of the known inherited conditions listed below) have a higher chance of developing this cancer. This risk is highest for people who have a brother or sister with the cancer. It’s not clear whether this is due to shared genes, something that both people were exposed to in the environment, or both.
High blood pressure
The risk of renal cell carcinoma is higher in people with high blood pressure. Some studies have suggested that certain medicines used to treat high blood pressure may raise the risk of renal cell carcinoma, but it is hard to tell if it’s the condition or the medicine (or both) that may be the cause of the increased risk.
Certain medicines
- Phenacetin: This drug used to be a popular non-prescription pain reliever and has been linked to renal cell carcinoma in the past. But it has not been available in the United States for over 30 years, so it no longer appears to be a major risk factor.
- Diuretics: Some studies have suggested that diuretics (water pills) may be linked to a small increase in the risk of renal cell carcinoma. It is not clear whether the cause is the drugs or the high blood pressure they treat. If you need to take diuretics, don’t avoid them to try to reduce the risk of renal cell carcinoma.
Advanced kidney disease
People with advanced kidney disease, especially those needing dialysis, have a higher risk of renal cell carcinoma. Dialysis is a treatment used to remove toxins from your body if the kidneys do not work properly.
Gender
Renal cell carcinoma is about twice as common in men as in women. Men are more likely to be smokers and are more likely to be exposed to cancer-causing chemicals at work, which may account for some of the difference.
Race
African Americans and American Indians/Alaska Natives have slightly higher rates of renal cell carcinoma than do whites. The reasons for this are not clear.
Genetic and hereditary risk factors
Some people inherit a tendency to develop certain types of cancer. The DNA in each of your cells that you get from your parents may have changes that give you this tendency. Some rare inherited conditions can cause renal cell carcinoma. It is important that people who have hereditary causes of renal cell carcinoma see their doctors often, especially if they have already been diagnosed with renal cell carcinoma. Some doctors recommend regular imaging tests (such as CT scans) to look for new kidney tumors in these people.
People who have the conditions listed here have a much higher risk for getting renal cell carcinoma, although they account for only a small portion of cases overall.
- von Hippel-Lindau disease: People with this condition often develop several kinds of tumors and cysts (fluid-filled sacs) in different parts of the body. They have an increased risk for developing clear cell renal cell carcinoma, especially at a younger age. They may also have benign tumors in their eyes, brain, spinal cord, pancreas, and other organs; and a type of adrenal gland tumor called pheochromocytoma. This condition is caused by mutations (changes) in the VHL gene.
- Hereditary papillary renal cell carcinoma: People with this condition have a tendency to develop one or more papillary renal cell carcinomas, but they do not have tumors in other parts of the body, as is the case with the other inherited conditions listed here. This disorder is usually linked to changes in the MET gene.
- Hereditary leiomyoma-renal cell carcinoma: People with this syndrome develop smooth muscle tumors called leiomyomas (fibroids) of the skin and uterus (in women) and have a higher risk for developing papillary renal cell carcinomas. It has been linked to changes in the FH gene.
- Birt-Hogg-Dube (BHD) syndrome: People with this syndrome develop many small benign skin tumors and have an increased risk of different kinds of kidney tumors, including renal cell carcinomas and oncocytomas. They may also have benign or malignant tumors of several other tissues. The gene linked to BHD is known as FLCN.
- Familial renal cancer: People with this condition develop tumors called paragangliomas of the head and neck region, as well as tumors known as pheochromocytomas of the adrenal glands and thyroid cancers. They also tend to get renal cell carcinoma in both kidneys before age 40. It is caused by defects in the genes SDHB and SDHD.
- Cowden syndrome: People with this syndrome have a high risk of breast, thyroid and renal cell carcinomas. It is linked to changes in the PTEN gene.
- Tuberous sclerosis: People with this syndrome develop many, usually benign (noncancerous) tumors in different parts of the body including the skin, brain, lungs, eyes, kidneys, and heart. Although the kidney tumors are most often benign, occasionally they can be clear cell renal cell carcinoma. It is caused by defects in the genes TSC1 and TSC2.
- Hereditary renal oncocytoma: Some people inherit the tendency to develop a kidney tumor called an oncocytoma, which is almost always benign (not cancer).
Renal cell carcinoma prevention
In many cases, the cause of renal cell carcinoma is not known. In some other cases (such as with inherited conditions that raise renal cell carcinoma risk), even when the cause is known it may not be preventable. But there are some ways you may be able to reduce your risk of this disease.
Cigarette smoking is responsible for a large percentage of cases, so stopping smoking may lower your risk.
Obesity and high blood pressure are also risk factors for renal cell cancer. Maintaining a healthy weight by exercising and choosing a diet high in fruits and vegetables, and getting treatment for high blood pressure may also reduce your chance of getting this disease.
Finally, avoiding workplace exposure to harmful substances such as cadmium and organic solvents may reduce your risk for renal cell cancer.
Renal cell carcinoma diagnosis
Kidney cancer might be found because of signs or symptoms a person is having, or it might be found because of lab tests or imaging tests a person is getting for another reason. If cancer is suspected, tests will be needed to confirm the diagnosis.
Medical history and physical exam
If you have any signs or symptoms that suggest you might have kidney cancer, your doctor will want to take a complete medical history to check for risk factors and to learn more about your symptoms.
A physical exam can provide information about signs of kidney cancer and other health problems. For example, the doctor may be able to feel an abnormal mass (lump) when he or she examines your abdomen (belly).
If symptoms or the results of the physical exam suggest you might have kidney cancer, more tests will probably be done. These might include lab tests and imaging tests.
Blood tests
Lab tests cannot show for sure if a person has kidney cancer, but they can sometimes give the first hint that there may be a kidney problem. If cancer has already been diagnosed, they are also done to get a sense of a person’s overall health and to help tell if the cancer might have spread to other areas. They also can help show if a person is healthy enough to have an operation.
Urinalysis (urine testing): This test may be done if your doctor suspects a kidney problem.
Microscopic and chemical tests are done on a urine sample to look for small amounts of blood and other substances not seen with the naked eye. About half of all patients with renal cell cancer will have blood in their urine. If the patient has transitional cell carcinoma (in the renal pelvis, the ureter, or the bladder), sometimes a special exam of the urine sample (called urine cytology) in the lab will show actual cancer cells in the urine.
Complete blood count (CBC): This is a test that measures the amounts of different cells in the blood. This test result is often abnormal in people with renal cell cancer. Anemia (having too few red blood cells) is very common. Less often, a person may have too many red blood cells (called polycythemia) because the kidney cancer cells make a hormone (erythropoietin) that causes the bone marrow to make more red blood cells. Blood counts are also important to make sure a person is healthy enough for surgery.
Blood chemistry tests: These tests are usually done in people who might have kidney cancer, because the cancer can affect the levels of certain chemicals in the blood. For example, high levels of liver enzymes are sometimes found. High blood calcium levels may indicate that cancer has spread to the bones, and may therefore prompt a doctor to order a bone scan. Blood chemistry tests also look at kidney function, which is especially important if certain imaging tests or if surgery is planned.
Imaging tests to look for kidney cancer
Imaging tests use x-rays, magnetic fields, sound waves, or radioactive substances to create pictures of the inside of your body. Imaging tests can be done for a number of reasons, such as:
- To look at suspicious areas that might be cancer
- To learn how far cancer has spread
- To help determine if treatment is working
Unlike most other cancers, doctors can often diagnose kidney cancer with fair certainty based on imaging tests without doing a biopsy (removing a sample of the tumor to be looked at under a microscope). In some patients, however, a biopsy may be needed.
Computed tomography (CT) scan
The CT scan uses x-rays to produce detailed cross-sectional images of your body. It is one of the most useful tests for finding and looking at a tumor in your kidney. It can provide precise information about the size, shape, and location of a tumor. It is also useful in checking to see if a cancer has spread to nearby lymph nodes or to organs and tissues outside the kidney. If a kidney biopsy is needed, this test can also be used to guide a biopsy needle into the mass (lump) to obtain a sample.
When a CT is done to look at the kidneys, an IV (intravenous) contrast dye is often needed to make certain areas stand out better on the scan. This CT contrast can damage the kidneys. This happens more often in patients whose kidneys are not working well in the first place. Because of this, your kidney function will be checked with a blood test before you get IV contrast.
Magnetic resonance imaging (MRI) scan
MRI scans are used less often than CT scans in people with kidney cancer. They may be done in cases where CT scans aren’t practical, such as if a person can’t have the CT contrast dye because they have an allergy to it or they don’t have good kidney function. MRI scans may also be done if there’s a chance that the cancer has grown into major blood vessels in the abdomen (like the inferior vena cava), because they provide a better picture of blood vessels than CT scans. Finally, they may be used to look at abnormal areas in the brain and spinal cord that might be due to cancer spread.
Ultrasound
Ultrasound can help find a kidney mass and show if it is solid or filled with fluid (kidney tumors are more likely to be solid). Different echo patterns also can help doctors tell some types of benign and malignant kidney tumors from one another.
If a kidney biopsy is needed, this test can also be used to guide a biopsy needle into the mass to obtain a sample.
Positron emission tomography (PET) scan
A PET scan uses a form of radioactive sugar that is put into the blood. Body cells take in different amounts of the sugar, depending on how fast they are growing. Cancer cells, which grow quickly, are more likely to take up larger amounts of the sugar than normal cells. A special camera is used to create a picture of areas of radioactivity in the body. The picture from a PET scan is not as detailed as a CT or MRI scan, but it provides helpful information about whether abnormal areas seen on these other tests are likely to be cancer or not. This scan can be useful in seeing if the cancer has spread to lymph nodes near the kidney. PET scans can also be useful if your doctor thinks the cancer may have spread but doesn’t know where.
Special machines can perform both a PET and CT scan at the same time (PET/CT scan). This lets the doctor compare areas of higher radioactivity (suggesting an area of cancer) on the PET scan with the more detailed picture of that area on the CT.
Still, PET and PET/CT scans are not a standard part of the work-up for kidney cancers.
Intravenous pyelogram
An intravenous pyelogram (IVP) is an x-ray of the urinary system taken after a special dye is injected into a vein. The kidneys remove the dye from the bloodstream and it then concentrates in the ureters and bladder. An IVP can help find abnormalities of the renal pelvis and ureter, such as cancer, but this test is not often used when kidney cancer is suspected.
Angiography
Angiography is an x-ray test for looking at blood vessels. A contrast dye is injected into the renal artery, and the dye outlines the blood vessels. X-rays are taken to identify and map the blood vessels that supply a kidney tumor. This type of contrast dye though, is not the same as the one used for an IVP.
This test can help in planning surgery for some patients. Angiography can also help diagnose renal cancers since the blood vessels usually have a special appearance with this test.
Angiography can often be done as a part of a CT or MRI scan, instead of as a separate x-ray test. This means less contrast dye is used, which is helpful since the dye can damage kidney function further if it is given to people whose kidneys aren’t working well.
Chest x-ray
An x-ray may be done after kidney cancer has been diagnosed to see if cancer has spread to the lungs.
Bone scan
A bone scan can help show if a cancer has spread to your bones. It might be done if there is reason to think the cancer might have spread to the bones (because of symptoms such as bone pain or blood test results showing an increased calcium level). PET scans can usually show the spread of cancer to bones as well, so if you’ve had a PET scan you might not need a bone scan.
Kidney biopsy
Unlike with most other types of cancer, biopsies are not often used to diagnose kidney tumors. Imaging tests usually provide enough information for a surgeon to decide if an operation is needed. The diagnosis is then confirmed when part of the kidney that was removed is looked at in the lab.
However, a biopsy is sometimes done to get a small sample of tissue from an area that may be cancer when the imaging tests are not clear enough to permit surgery. Biopsy may also be done to confirm cancer if a person might not be treated with surgery, such as with small tumors that will be watched and not treated, or when other treatments are being considered.
Fine needle aspiration (FNA) and needle core biopsy are 2 types of kidney biopsies that may be done.
In cases where the doctors think kidney cancer might have spread to other sites, they may take a biopsy of the metastatic site instead of the kidney.
Biopsy results
The biopsy samples are sent to a lab, where they are looked at by a pathologist, a doctor who specializes in diagnosing diseases with lab tests. If kidney cancer is found, an important feature that is evaluated is the grade, specifically called Fuhrman grade.
The Fuhrman grade is found by looking at kidney cancer cells (taken during a biopsy or during surgery) in a lab. Many doctors use it to describe how quickly the cancer is likely to grow and spread. The grade is based on how closely the cancer cells look like those of normal kidney cells. Renal cell cancers are usually graded on a scale of 1 through 4. Grade 1 renal cell cancers have cells that look a lot like normal kidney cells. These cancers usually grow and spread slowly and tend to have a good prognosis (outlook). At the other extreme, grade 4 renal cell cancer looks quite different from normal kidney cells. These cancers have a worse prognosis.
Although the cell type and grade can sometimes help predict prognosis (outlook), the cancer’s stage is by far the best predictor of survival. The stage describes the cancer’s size and how far it has spread beyond the kidney.
Renal cell carcinoma staging
After someone is diagnosed with kidney cancer, doctors will try to figure out whether it has spread, and if so, how far. This process is called staging. The stage of a cancer describes the extent of the cancer in the body. It helps determine how serious the cancer is and how best to treat it. The stage is one of the most important factors in deciding how to treat the cancer and determining how successful treatment might be.
To determine the cancer’s stage after a kidney cancer diagnosis, doctors try to answer these questions:
- How large has the cancer grown in the kidney?
- Has the cancer reached nearby structures, such as major blood vessels?
- Has the cancer spread to the nearby lymph nodes or to distant organs?
The stage of kidney cancer is based on the results of the physical exam, imaging tests (CT scan, chest x-ray, PET scan, etc.), and sometimes biopsies.
After looking at your test results, your doctor will tell you the stage of your cancer. The staging system most often used for kidney cancer is the American Joint Committee on Cancer (AJCC) TNM system. The TNM system is based on 3 key pieces of information:
- The size of the main (primary) tumor (T) and whether it has grown into nearby areas.
- If the cancer has spread to nearby (regional) lymph nodes (N). Lymph nodes are small bean-shaped collections of immune system cells to which cancers often spread first.
- If the cancer has spread (metastasized) to other organs (M). Kidney cancer can spread almost anywhere in the body, but common sites of spread are the bones, brain, and lungs.
Numbers or letters after T, N, and M provide more details about each of these factors. Higher numbers mean the cancer is more advanced. Once a person’s T, N, and M categories have been determined, usually after surgery, this information is combined in a process called stage grouping to assign an overall stage.
The earliest stage cancers are called stage 0 (carcinoma in situ), and then range from stages I (1) through IV (4). Some of the stages have sub-stages with the letters A, B, and C. The letter X means “cannot be assessed because the information is not available.”
As a rule, the lower the number, the less the cancer has spread. A higher number, such as stage IV, means a more advanced cancer. And within a stage, an earlier letter means a lower stage. Cancers with similar stages tend to have a similar outlook and are often treated in much the same way. Patients with lower stage numbers tend to have a better prognosis.
The staging system in the table below uses the pathologic stage. It is based on the results of physical exam, biopsy, imaging tests, and the results of surgery. This is likely to be more accurate than clinical staging, which only considers the tests done before surgery.
Kidney cancer staging can be complex. If you have any questions about your stage, please ask your doctor to explain it to you in a way you understand. (An explanation of the TNM system also follows the stage table below.)
Explaining the TNM system
T categories for kidney cancer
- TX: The primary tumor cannot be assessed (information not available).
- T0: No evidence of a primary tumor.
- T1: The tumor is only in the kidney and is no larger than 7 centimeters (cm), or a little less than 3 inches, across.
- T1a: The tumor is 4 cm (about 1½ inches) across or smaller and is only in the kidney.
- T1b: The tumor is larger than 4 cm but not larger than 7 cm across and is only in the kidney.
- T2: The tumor is larger than 7 cm across but is still only in the kidney.
- T2a: The tumor is more than 7 cm but not more than 10 cm (about 4 inches) across and is only in the kidney.
- T2b: The tumor is more than 10 cm across and is only in the kidney.
- T3: The tumor is growing into a major vein or into tissue around the kidney, but it is not growing into the adrenal gland (on top of the kidney) or beyond Gerota’s fascia (the fibrous layer that surrounds the kidney and nearby fatty tissue).
- T3a: The tumor is growing into the main vein leading out of the kidney (renal vein) or into fatty tissue around the kidney.
- T3b: The tumor is growing into the part of the large vein leading into the heart (vena cava) that is within the abdomen.
- T3c: The tumor has grown into the part of the vena cava that is within the chest or it is growing into the wall of the vena cava.
- T4: The tumor has spread beyond Gerota’s fascia (the fibrous layer that surrounds the kidney and nearby fatty tissue). The tumor may have grown into the adrenal gland (on top of the kidney).
N categories for kidney cancer
- NX: Regional (nearby) lymph nodes cannot be assessed (information not available).
- N0: No spread to nearby lymph nodes.
- N1: Tumor has spread to nearby lymph nodes.
M categories for kidney cancer
- M0: There is no spread to distant lymph nodes or other organs.
- M1: Distant metastasis is present; includes spread to distant lymph nodes and/or to other organs. Kidney cancer most often spreads to the lungs, bones, liver, or brain.
Table 1. Renal cell carcinoma TNM staging
| Stage | Stage grouping | Stage description |
| 1 | T1, N0, M0 | The tumor is 7 cm across or smaller and is only in the kidney (T1). There is no spread to lymph nodes (N0) or distant organs (M0). |
| 2 | T2, N0, M0 | The tumor is larger than 7 cm across but is still only in the kidney (T2). There is no spread to lymph nodes (N0) or distant organs (M0). |
|
3
| T3, N0, M0 | The tumor is growing into a major vein (like the renal vein or the vena cava) or into tissue around the kidney, but it is not growing into the adrenal gland or beyond Gerota’s fascia (T3). There is no spread to lymph nodes (N0) or distant organs (M0). |
| OR | ||
| T1 to T3, N1, M0 | The main tumor can be any size and may be outside the kidney, but it has not spread beyond Gerota’s fascia. The cancer has spread to nearby lymph nodes (N1) but has not spread to distant lymph nodes or other organs (M0). | |
| 4 | T4, Any N, M0 | The main tumor is growing beyond Gerota’s fascia and may be growing into the adrenal gland on top of the kidney (T4). It may or may not have spread to nearby lymph nodes (any N). It has not spread to distant lymph nodes or other organs (M0). |
| OR | ||
| Any T, Any N, M1 | The main tumor can be any size and may have grown outside the kidney (any T). It may or may not have spread to nearby lymph nodes (any N). It has spread to distant lymph nodes and/or other organs (M1). | |
[Source 1)]
Other staging and prognostic systems
The TNM staging system is useful, but some doctors have pointed out that there are factors other than the extent of the cancer that should be considered when determining prognosis and treatment.
University of California Los Angeles (UCLA) Integrated Staging System
This is a more complex system that came out in 2001. It was meant to improve upon the American Joint Committee on Cancer (AJCC) TNM staging that was then in place. Along with the stage of the cancer, it takes into account a person’s overall health and the Fuhrman grade of the tumor. These factors are combined to put people into low-, intermediate-, and high-risk groups. Ask your doctor if he or she uses this system and how it might apply to you.
Survival predictors
The stage of the cancer is an important predictor of survival, but other factors are also important. For example, researchers have linked certain factors with shorter survival times in people with kidney cancer that has spread outside the kidney. These include:
- High blood lactate dehydrogenase (LDH) level
- High blood calcium level
- Anemia (low red blood cell count)
- Cancer spread to 2 or more distant sites
- Less than a year from diagnosis to the need for systemic treatment (targeted therapy, immunotherapy, or chemotherapy)
- Poor performance status (a measure of how well a person can do normal daily activities)
People with none of the above factors are considered to have a good prognosis; 1 or 2 factors are considered intermediate prognosis, and 3 or more of these factors are considered to have a poor prognosis and may be less likely to benefit from certain treatments.
Renal cell carcinoma prognosis
Survival rates tell you what portion of people with the same type and stage of cancer are still alive a certain amount of time (usually 5 years) after they were diagnosed. They can’t tell you how long you will live, but they may help give you a better understanding about how likely it is that your treatment will be successful.
Survival rates are often based on previous outcomes of large numbers of people who had the disease, but they can’t predict what will happen in any particular person’s case. There are a few limitations to remember:
- The numbers below are among the most current available. But to get 5-year survival rates, doctors must look at people who were treated at least 5 years ago. As treatments are improving over time, people who are now being diagnosed with kidney cancer may have a better outlook than these statistics show.
- These statistics are based on the stage of the cancer when it was first diagnosed. They do not apply to cancers that later come back or spread, for example.
- The outlook for people with kidney cancer varies by the stage (extent) of the cancer – in general, the survival rates are better for people with earlier stage cancers. But many other factors can affect a person’s outlook, such as age and overall health, and how well the cancer responds to treatment. The outlook for each person is specific to his or her circumstances.
Your doctor can tell you how these numbers may apply to you, as he or she is familiar with your situation.
Survival rates by American Joint Committee on Cancer (AJCC) TNM stage
The numbers below come from the National Cancer Data Base and are based on patients first diagnosed in the years 2001 and 2002. These are observed survival rates. They include people diagnosed with kidney cancer who may have later died from other causes, such as heart disease. People with kidney cancer tend to be older and may have other serious health conditions. Therefore, the percentage of people surviving the cancer itself is likely to be higher.
| Stage | 5-Year Survival Rate |
| 1 | 81% |
| 2 | 74% |
| 3 | 53% |
| 4 | 8% |
Survival rates in the UCLA Integrated Staging System
Researchers at University of California Los Angeles (UCLA) have published a study evaluating their system in patients treated there from 1989 to 2005, looking at survival rates of the low-, intermediate- and high-risk groups. All of these patients at least had surgery to remove the tumor in the kidney. These numbers are disease-specific survival rates, meaning they only take into account people who died from their kidney cancer (and not other causes).
- For patients with localized kidney cancer (cancer that had not spread to the lymph nodes or distant organs), 5-year survival rates were 97% for the low-risk group, 81% for intermediate-risk group, and 62% for the high-risk group.
- For patients with kidney cancer that had spread to the lymph nodes or distant organs when it was first found, 5-year survival rates were 41% for the low-risk group, 18% for intermediate-risk group, and 8% for the high-risk group.
Renal cell carcinoma treatment
If you’ve been diagnosed with renal cell carcinoma, your cancer care team will discuss your treatment options with you. Think carefully about each of your choices. You will want to weigh the benefits of each treatment option against the possible risks and side effects.
Treatment Choices by Stage for renal cell carcinoma
The type of treatment(s) your doctor recommends will depend on the stage of the renal cell carcinoma and on your overall health. This section sums up the options usually considered for each stage of renal cell carcinoma.
Stages 1, 2, or 3 Renal Cell Carcinoma
Stage 1 and 2 cancers are still contained within the kidney. Stage 3 cancers have either grown into nearby large veins or have spread to nearby lymph nodes.
These cancers are usually removed with surgery when possible. There are two common approaches:
- Partial nephrectomy (removing part of the kidney). This is often the treatment of choice in tumors up to 7 cm (a little less than 3 inches) if it can be done.
- Radical nephrectomy (removing the entire kidney).
The lymph nodes near the kidney may be removed as well, especially if they are enlarged.
If the cancer has grown into nearby veins (as with some stage 3 cancers), your surgeon may need to cut open these veins to remove all of the cancer. This may require putting you on bypass (a heart-lung machine), so that the heart can be stopped for a short time to remove the cancer from the large vein leading to the heart.
After surgery, some people at high risk of the cancer returning might be helped by getting the targeted drug sunitinib (Sutent) for about a year, which can help lower this risk. Treatment given after surgery is known as adjuvant therapy. Sunitinib can have side effects, so it’s important to talk to your doctor about the benefits and risks. Clinical trials are also looking at other adjuvant treatments for kidney cancer. Ask your doctor if you are interested in learning more about adjuvant therapies being studied in clinical trials.
If you cannot have kidney surgery because of other serious medical problems, you might benefit from other local treatments such as cryotherapy, radiofrequency ablation, or arterial embolization. Radiation therapy may be another option. These treatments are generally only given when surgery can’t be done. Although these types of treatments can have similar outcomes to surgery as far as the chances of the cancer spreading to other parts of the body, some studies show the cancer might be more likely to come back in the same area.
Active surveillance is another option for some people with small kidney tumors. With active surveillance, the tumor is watched closely (with CTs or ultrasounds) and only treated if it grows.
Stage 4 Renal Cell Carcinoma
Stage 4 renal cell carcinoma means the cancer has grown outside of the kidney or has spread to other parts of the body such as distant lymph nodes or other organs.
Treatment of stage 4 kidney cancer depends on how extensive the cancer is and on the person’s general health. In some cases, surgery may still be a part of treatment.
In rare cases where the main tumor appears to be removable and the cancer has only spread to one other area (such as to one or a few spots in the lungs), surgery to remove both the kidney and the metastasis (the outside area of cancer spread) may be an option if a person is in good enough health. Otherwise, treatment with one of the targeted therapies is usually the first option.
If the main tumor is removable but the cancer has spread extensively elsewhere, removing the kidney may still be helpful. This would likely be followed by systemic therapy, which might consist of one of the targeted therapies or immunotherapy (interleukin-2). More often targeted therapy is used first. It’s not clear if any one of the targeted therapies or any particular sequence is better than another, although temsirolimus appears to be most helpful for people with kidney cancers that have a poorer prognosis (outlook).
For cancers that can’t be removed surgically (because of the extent of the tumor or the person’s health), first-line treatment is likely to be one of the targeted therapies or cytokine therapy.
Because advanced kidney cancer is very hard to cure, clinical trials of new combinations of targeted therapies, immunotherapy, or other new treatments are also options.
For some people, palliative treatments such as embolization or radiation therapy may be the best option. A special form of radiation therapy called stereotactic radiosurgery can be very effective in treating single brain metastases. Surgery or radiation therapy can also be used to help reduce pain or other symptoms of metastases in some other places, such as the bones.
Having your pain controlled can help you maintain your quality of life. Medicines to relieve pain do not interfere with your other treatments, and controlling pain will often help you be more active and continue your daily activities.
Recurrent cancer
Cancer is called recurrent when it come backs after treatment. Recurrence can be local (near the area of the initial tumor) or it may be in distant organs. Treatment of kidney cancer that comes back (recurs) after initial treatment depends on where it recurs and what treatments have been used, as well as a person’s health and wishes for further treatment.
Local recurrence
For renal cell carcinoma that recur after initial surgery, further surgery might be an option. Otherwise, treatment with targeted therapies or immunotherapy will probably be recommended. Clinical trials of new treatments are an option as well.
Distant recurrence
Kidney cancer that recurs in distant parts of the body is treated like a stage 4 cancer. Your options depend on which, if any, drugs you received before the cancer came back and how long ago you received them, as well as on your health.
For cancers that progress (continue to grow or spread) during treatment with targeted therapy or cytokine therapy, another type of targeted therapy or immunotherapy may be helpful. If these don’t work, chemotherapy may be tried, especially for people with non-clear cell types of renal cell cancer. Recurrent cancers can sometimes be hard to treat, so you might also want to ask your doctor about clinical trials of newer treatments.
For some people with recurrent kidney cancer, palliative treatments such as embolization or radiation therapy may be the best option. Controlling symptoms such as pain is an important part of treatment at any stage of the disease.
Surgery for renal cell carcinoma
Surgery is the main treatment for most renal cell carcinoma (over 56% of patients). The chances of surviving kidney cancer without having surgery are small.
The proportion of renal cell carcinoma patients having surgery to remove their primary tumor is strongly influenced by the renal cell carcinoma stage at diagnosis. Other factors are also important, such as whether the patient is generally well enough to tolerate the surgery, the patient’s age, and their own treatment preference.
Even people whose renal cell carcinoma has spread to other organs may benefit from surgery to take out the kidney tumor. Removing the kidney containing the cancer can help some people live longer, so a doctor may suggest surgery even if the cancer has spread beyond the kidney. Kidney removal can also be used to ease symptoms such as pain and bleeding.
Depending on the stage and location of the cancer and other factors, surgery might be done to remove either the cancer along with some of the surrounding kidney tissue (known as a partial nephrectomy), or the entire kidney (known as a radical nephrectomy). The adrenal gland (the small gland that sits on top of each kidney) and fatty tissue around the kidney is sometimes removed as well.
Radical nephrectomy
In this operation, the surgeon removes your whole kidney, the attached adrenal gland, nearby lymph nodes, and the fatty tissue around the kidney. Most people do just fine with only one working kidney.
The surgeon can make the incision in several places. The most common sites are the middle of the abdomen (belly), under the ribs on the same side as the cancer, or in the back, just behind the kidney. Each approach has its advantages in treating cancers of different sizes and in different parts of the kidney. Although removing the adrenal gland is a part of a standard radical nephrectomy, the surgeon may be able to leave it behind in some cases where the cancer is in the lower part of the kidney and is far away from the adrenal gland.
If the tumor has grown from the kidney through the renal vein (the vein leading away from the kidney) and into the inferior vena cava (the large vein that empties into the heart), the heart may need to be stopped for a short time in order to remove the tumor. The patient is put on cardiopulmonary bypass (a heart-lung machine) that circulates the blood while bypassing the heart. If you need this, a heart surgeon will work with your urologist during your operation.
Laparoscopic nephrectomy and robotic-assisted laparoscopic nephrectomy: These newer approaches to the operation are done through several small incisions instead of one large one. If a radical nephrectomy is needed, many doctors and patients now prefer these approaches when they can be used.
For a laparoscopic nephrectomy, special long instruments are inserted through the incisions, each of which is about 1/2-inch (1.27cm) long, to remove the kidney. One of the instruments, the laparoscope, is a long tube with a small video camera on the end. This lets the surgeon see inside the abdomen. Usually, one of the incisions has to be made longer in order to remove the kidney (although it’s not as long as the incision for a standard nephrectomy).
A newer approach is to do the laparoscopic surgery remotely using a robotic system. The surgeon sits at a panel near the operating table and controls robotic arms to perform the operation. For the surgeon, the robotic system may provide more maneuverability and more precision when moving the instruments than standard laparoscopic surgery. But the most important factor in the success of either type of laparoscopic surgery is the surgeon’s experience and skill. This is a difficult approach to learn. If you are considering this type of operation, be sure to find a surgeon with a lot of experience.
The laparoscopic approach can be used to treat most renal tumors that cannot be treated with nephron-sparing surgery (see below). In experienced hands, the technique is as effective as a standard (open) radical nephrectomy and usually results in a shorter hospital stay, a faster recovery, and less pain after surgery. This approach may not be an option for tumors larger than about 10 cm (4 inches) across or tumors that have grown into the renal vein or spread to lymph nodes around the kidney.
Partial nephrectomy (nephron-sparing surgery)
In this procedure, the surgeon removes only the part of the kidney that contains cancer, leaving the rest of the kidney behind. As with a radical nephrectomy, the surgeon can make the incision in several places, depending on factors like the location of the tumor.
Partial nephrectomy is now the preferred treatment for many people with early stage kidney cancer. It is often done to remove single small tumors (less than 4 cm across), and can also be done to remove larger tumors (up to 7 cm across). Studies have shown the long-term results to be about the same as when the whole kidney is removed. The obvious benefit is that the patient keeps more of their kidney function.
A partial nephrectomy might not be an option if the tumor is in the middle of the kidney or is very large, if there is more than one tumor in the same kidney, or if the cancer has spread to the lymph nodes or distant organs. Not all doctors can do this type of surgery. It should only be done by someone with a lot of experience.
Laparoscopic partial nephrectomy and robotic-assisted laparoscopic partial nephrectomy: Many doctors now do partial nephrectomies laparoscopically or using a robot (as described above). But again, this is a difficult operation, and it should only be done by a surgeon with a great deal of experience.
Regional lymphadenectomy (lymph node dissection)
This procedure removes nearby lymph nodes to see if they contain cancer. Some doctors do this when doing a radical nephrectomy The number of lymph nodes removed may be more extensive if the tumor has characteristics suggesting it has a high risk to spread.
Most doctors agree that the lymph nodes should be removed if they look enlarged on imaging tests or feel abnormal during the operation. Some doctors also remove these lymph nodes to check them for cancer spread even when they aren’t enlarged, in order to better stage the cancer. Before surgery, ask your doctor if they plan to remove the lymph nodes near the kidney.
Removal of an adrenal gland (adrenalectomy)
Although this is a standard part of a radical nephrectomy, if the cancer is in the lower part of the kidney (away from the adrenal gland) and imaging tests show the adrenal gland is not affected, it may not have to be removed. Just like with lymph node removal, this is decided on an individual basis and should be discussed with the doctor before surgery.
Removal of metastases
In about 1 in 4 people with kidney cancer, the cancer will already have spread (metastasized) to other parts of the body when it is diagnosed. The lungs, lymph nodes, bones, and liver are the most common sites of spread. For some people, surgery may still be helpful.
Attempts at curative surgery: In rare cases where there is only a single metastasis or if there are only a few that can be removed easily without causing serious side effects, surgery may lead to long-term survival in some people.
The metastasis may be removed at the same time as a radical nephrectomy or at a later time if the cancer recurs (comes back).
Surgery to relieve symptoms (palliative surgery): When other treatments aren’t helpful, surgically removing the metastases can sometimes relieve pain and other symptoms, although this usually does not help people live longer.
Risks and side effects of surgery
The short-term risks of any type of surgery include reactions to anesthesia, excess bleeding (which might require blood transfusions), blood clots, and infections. Most people will have at least some pain after the operation, which can usually be helped with pain medicines, if needed.
Other possible risks of surgery include:
- Damage to internal organs and blood vessels (such as the spleen, pancreas, aorta, vena cava, large or small bowel) during surgery
- Pneumothorax (unwanted air in the chest cavity)
- Incisional hernia (bulging of internal organs near the surgical incision due to problems with wound healing)
- Leakage of urine into the abdomen (after partial nephrectomy)
- Kidney failure (if the remaining kidney fails to function well)
Ablation and Other Local Therapy for renal cell carcinoma
For people who are too sick to have surgery, other approaches can sometimes be used to destroy renal cell carcinoma. They might be helpful for some people, but there is much less data on how well they work over time than there is for surgery, so they are not yet considered a standard treatment.
Cryotherapy (cryoablation)
This approach uses extreme cold to destroy the tumor. A hollow probe (needle) is inserted into the tumor either through the skin (percutaneously) or during laparoscopy. Very cold gases are passed through the probe, creating an ice ball at its tip that destroys the tumor. To be sure the tumor is destroyed without too much damage to nearby tissues, the doctor carefully watches images of the tumor during the procedure (with ultrasound) or measures tissue temperature.
The type of anesthesia used for cryotherapy depends on how the procedure is being done. Possible side effects include bleeding and damage to the kidneys or other nearby organs.
Radiofrequency ablation
This technique uses high-energy radio waves to heat the tumor. A thin, needle-like probe is placed through the skin and advanced until the end is in the tumor. Placement of the probe is guided by ultrasound or CT scans. Once it is in place, an electric current is passed through the tip of the probe, which heats the tumor and destroys the cancer cells.
Radiofrequency ablation is usually done as an outpatient procedure, using local anesthesia (numbing medicine) where the probe is inserted. You may be given medicine to help you relax as well.
Major complications are uncommon, but they can include bleeding and damage to the kidneys or other nearby organs.
Arterial embolization
This technique is used to block the artery that feeds the kidney that has the tumor. A small catheter (tube) is placed in an artery in the inner thigh and is moved up until it reaches the renal artery going from the aorta to the kidney. Material is then injected into the artery to block it, cutting off the kidney’s blood supply. This will cause the kidney (and the tumor in it) to die.
Although this procedure is not used very often, it is sometimes done before a radical nephrectomy to reduce bleeding during the operation or in patients who have persistent bleeding from the kidney tumor.
Active Surveillance for renal cell carcinoma
One option for some people with small renal cell carcinoma (less than 4 cm[about 1½ inches]), may be to give no treatment at first and watch the tumor carefully to see if it grows. The tumor is removed (or treated another way) if it grows quickly or gets larger than 4 cm.
This approach is most often used for elderly or frail patients as it avoids the risks of treatment, such as surgery or ablation. Often, a biopsy is done before deciding to watch the tumor to see if the growth is really cancer. Some of these small tumors turn out not to be cancers at all. Watching them closely for a time helps doctors decide which tumors are more likely to be cancer based on their growth.
Radiation Therapy for renal cell carcinoma
Radiation therapy uses high-energy radiation to kill cancer cells.
Renal cell carcinoma are not very sensitive to radiation, but it is sometimes used if a person is not healthy enough to have surgery. Sometimes other treatments will be tried first instead. When radiation therapy is used to treat kidney cancer, it is usually external beam therapy, which focuses radiation from a source outside the body on the cancer.
For people with kidney cancer, radiation therapy is more often used to palliate, or ease, cancer symptoms such as pain, bleeding, or problems caused by cancer spread (especially to the bones or brain).
Possible side effects
Side effects of radiation therapy depend on where it is aimed and can include skin changes (similar to sunburn) and hair loss where the radiation passes through the skin, nausea, diarrhea, or tiredness. Often these go away after a short while. Radiation may also make side effects from some other treatments worse.
Targeted Therapies for renal cell carcinoma
As researchers have learned more about the molecular and genetic changes in cells that cause cancer, they have developed newer drugs that target some of these changes. These targeted drugs are different from standard chemotherapy drugs. They sometimes work when standard chemo drugs don’t, and they often have different side effects.
Targeted drugs are proving to be especially important in renal cell carcinoma, where chemotherapy has not been shown to be very effective.
When might targeted drugs be used?
Treating advanced renal cell carcinoma
All of the targeted drugs below can be used as to treat advanced renal cell carcinomas. They can often shrink or slow the growth of the cancer for a time, but it doesn’t seem that any of these drugs can actually cure renal cell carcinoma.
Targeted drugs are most often used one at a time. If one doesn’t work, another can be tried. It’s not yet known if any one of these drugs is clearly better than the others, if combining them might be more helpful than giving them one at a time, or if one sequence is better than another. Studies are being done to help answer these questions.
Adjuvant therapy after surgery
Sunitinib (Sutent) can also be used after surgery is done to remove the cancer, to help lower the risk that the cancer will come back. This is known as adjuvant therapy.
Which targeted drugs are used to treat renal cell carcinoma?
The targeted drugs used to treat advanced renal cell carcinoma work by blocking angiogenesis (growth of the new blood vessels that nourish cancers) or important proteins in cancer cells (called tyrosine kinases) that help them grow and survive. Some targeted drugs affect both.
Sorafenib (Nexavar)
Sorafenib acts by blocking both angiogenesis and growth-stimulating proteins in the cancer cell itself. Sorafenib does this by blocking several tyrosine kinases that are important for cell growth and survival. It is taken as a pill twice a day.
The most common side effects seen with this drug include fatigue, rash, diarrhea, increases in blood pressure, and redness, pain, swelling, or blisters on the palms of the hands or soles of the feet (hand-foot syndrome).
Sunitinib (Sutent)
Sunitinib also blocks several tyrosine kinases, similar to the ones blocked by sorafenib. It attacks both blood vessel growth and other targets that help cancer cells grow. This drug is taken as a pill.
The most common side effects are nausea, diarrhea, changes in skin or hair color, mouth sores, weakness, and low white and red blood cell counts. Other possible effects include tiredness, high blood pressure, congestive heart failure, bleeding, hand-foot syndrome, and low thyroid hormone levels.
Temsirolimus (Torisel)
Temsirolimus works by blocking a protein known as mTOR, which normally helps cells grow and divide. This drug has been shown to be helpful against advanced renal cell carcinomas that have a poorer prognosis because of certain factors. It is given as an intravenous (IV) infusion, typically once a week.
The most common side effects of this drug include skin rash, weakness, mouth sores, nausea, loss of appetite, fluid buildup in the face or legs, and increases in blood sugar and cholesterol levels. Rarely, more serious side effects have been reported.
Everolimus (Afinitor)
Everolimus also blocks the mTOR protein. It is used to treat advanced renal cell carcinomas after other drugs such as sorafenib or sunitinib have been tried. Everolimus is taken as a pill once a day.
Common side effects of this drug include mouth sores, an increased risk of infections, nausea, loss of appetite, diarrhea, skin rash, feeling tired or weak, fluid buildup (usually in the legs), and increases in blood sugar and cholesterol levels. A less common but serious side effect is lung damage, which can cause shortness of breath or other problems.
Bevacizumab (Avastin)
Bevacizumab is an IV drug that works by slowing the growth of new blood vessels. It may help some people with renal cell carcinoma when used with interferon-alfa.
More common side effects include high blood pressure, tiredness, and headaches. Less common but possibly serious side effects include bleeding, blood clots, holes forming in the intestines, heart problems, and slow wound healing.
Pazopanib (Votrient)
Pazopanib is another drug that blocks several tyrosine kinases involved in cancer cell growth and the formation of new blood vessels in the tumor. It is taken as a pill once a day.
Common side effects include high blood pressure, nausea, diarrhea, headaches, low blood cell counts, and liver problems. It can cause lab test results of liver function to become abnormal, but it rarely leads to severe liver damage that could be life threatening. Problems with bleeding, clotting, and wound healing can occur, as well. In rare cases it can also cause a problem with the heart rhythm or even a heart attack. If you are taking this drug, your doctor will monitor your heart with EKGs as well as check your blood tests to check for liver or other problems.
Axitinib (Inlyta)
Axitinib also inhibits several tyrosine kinases involved in the formation of new blood vessels. It is typically used after at least one other treatment has been tried. Axitinib is taken as a pill twice a day.
Common side effects include high blood pressure, fatigue, nausea and vomiting, diarrhea, poor appetite and weight loss, voice changes, hand-foot syndrome, and constipation. High blood pressure requiring treatment is fairly common, but in a small number of patients it can get high enough to be life-threatening. It can also cause problems with bleeding, clotting, and wound healing. In some patients, lab test results of liver function can become abnormal. Axitinib may also cause the thyroid gland to become underactive, so your doctor will watch your blood levels of thyroid hormone while you are on this drug.
Cabozantinib (Cabometyx)
Cabozantinib is another drug that blocks several tyrosine kinases, including some that help form new blood vessels. It is taken as a pill once a day.
Common side effects include diarrhea, fatigue, nausea and vomiting, poor appetite and weight loss, high blood pressure, hand-foot syndrome, and constipation. Less common but more serious side effects can include serious bleeding, blood clots, very high blood pressure, severe diarrhea, and holes forming in the intestines.
Lenvatinib (Lenvima)
Lenvatinib (Lenvima) is another kinase inhibitor that helps block tumors from forming new blood vessels, as well as targeting some of the proteins in cancer cells that normally help them grow. It is typically used along with everolimus after at least one other treatment has been tried. Lenvatinib is taken as capsules once a day.
Common side effects include diarrhea, fatigue, joint or muscle pain, loss of appetite, nausea and vomiting, mouth sores, weight loss, high blood pressure, and swelling in the arms or legs. Less common but more serious side effects can include serious bleeding, blood clots, very high blood pressure, severe diarrhea, holes forming in the intestines, and kidney, liver, or heart failure.
Immunotherapy for renal cell carcinoma
The goal of immunotherapy (sometimes called biologic therapy) is to boost the body’s immune system to help fight off or destroy cancer cells.
Cytokines
Cytokines are man-made versions of natural proteins that activate the immune system. The cytokines used most often to treat renal cell carcinoma are interleukin-2 (IL-2) and interferon-alpha. Both cytokines can cause renal cell carcinomas to shrink in a small percentage of patients.
Interleukin-2 (IL-2)
In the past, IL-2 was commonly used as first-line therapy for advanced renal cell carcinoma, and it may still be helpful for some people. But it can cause serious side effects, so many doctors only use it for people who are healthy enough to withstand the side effects, or for cancers that aren’t responding to targeted drugs.
Although only a small percentage of patients respond to IL-2, it is the only therapy that appears to result in long-lasting responses. Doctors are now looking to see if certain patient and cancer characteristics can help predict if IL-2 will be helpful.
Giving high doses of IL-2 seems to offer the best chance of shrinking the cancer, but this can cause serious side effects, so it is not used in people who are in poor overall health to begin with. Special care is needed to recognize and treat these side effects. Because of this, high-dose IL-2 is only given in the hospital at certain centers that are experienced with giving this type of treatment. IL-2 is given through a vein (IV).
The possible side effects of high-dose IL-2 include:
- Extreme fatigue
- Low blood pressure
- Fluid buildup in the lungs
- Trouble breathing
- Kidney damage
- Heart attacks
- Intestinal bleeding
- Diarrhea or abdominal pain
- High fever and chills
- Rapid heart beat
- Mental changes
These side effects are often severe and, rarely, can be fatal. Only doctors experienced in the use of these cytokines should give this treatment.
Interferon-alfa
Interferon has less serious side effects than IL-2, but it does not seem to be as effective when used by itself. It is more often used in combination with the targeted drug bevacizumab (Avastin). Interferon is given as a subcutaneous injection (under the skin) usually three times a week.
Common side effects of interferon include flu-like symptoms (fever, chills, muscle aches), fatigue, and nausea.
Immune checkpoint inhibitors
An important part of the immune system is its ability to keep itself from attacking normal cells in the body. To do this, it uses “checkpoints,” which are molecules on immune cells that need to be turned on (or off) to start an immune response. Cancer cells sometimes use these checkpoints to avoid being attacked by the immune system. But newer drugs that target these checkpoints hold a lot of promise as cancer treatments.
Nivolumab (Opdivo) is a drug that targets PD-1, a protein on immune system cells called T cells that normally helps keep these cells from attacking other cells in the body. By blocking PD-1, this drug boosts the immune response against cancer cells. This can shrink some tumors or slow their growth.
This drug can be used for people whose renal cell carcinoma starts growing again after other drug treatments.
For patients with intermediate or poor risk advanced renal cell carcinoma who have not received any treatment, nivolumab can be given with ipilimumab (a CTLA-4 inhibitor) for 4 doses followed by nivolumab alone. This drug combination has been shown to shrink the tumor significantly as well as help people live longer.
Nivolumab is given as an intravenous (IV) infusion, typically every 2 weeks.
Possible side effects
Side effects of immune checkpoint inhibitors can include fatigue, cough, nausea, itching, skin rash, loss of appetite, constipation, joint pain, and diarrhea.
Other, more serious side effects occur less often. These drugs work by basically removing the brakes on the body’s immune system. Sometimes the immune system starts attacking other parts of the body, which can cause serious or even life-threatening problems in the lungs, intestines, liver, hormone-making glands (like the thyroid), kidneys, or other organs.
It’s very important to report any new side effects to your health care team promptly. If serious side effects do occur, treatment may need to be stopped and you may get high doses of steroids to suppress your immune system and treat the side effects.
CTLA-4 inhibitors
Ipilimumab (Yervoy) is another drug that boosts the immune response, but it has a different target. It blocks CTLA-4, another protein on T cells that normally helps keep them in check.
For patients with intermediate or poor risk advanced renal cell carcinoma who have not received any treatment, ipilimumab can be given with nivolumab (an immune checkpoint inihibitor) for 4 doses followed by nivolumab alone. This drug combination has been shown to shrink the tumor significantly as well as help people live longer.
Ipilimumab is given as an intravenous (IV) infusion, usually once every 3 weeks for 4 treatments.
The most common side effects from Ipilimumab include fatigue, diarrhea, skin rash, and itching.
Like the PD-1 inhibitors, this drug can cause the immune system to attack other parts of the body, which can lead to serious problems in the intestines, liver, hormone-making glands, nerves, skin, eyes, or other organs. In some people these side effects can be life threatening.
It’s very important to report any new side effects during or after treatment to your health care team promptly. If serious side effects do occur, you may need to stop treatment and take high doses of corticosteroids to suppress your immune system.
Chemotherapy for renal cell carcinoma
Chemotherapy (chemo) uses anti-cancer drugs that are given into a vein (IV) or taken by mouth (as pills). These drugs enter your blood and reach nearly all areas of the body, which makes this treatment potentially useful for cancer that has spread (metastasized) to organs beyond the kidney.
Unfortunately, renal cell carcinoma cells usually do not respond well to chemo, so chemo is not a standard treatment for renal cell carcinoma. Some chemo drugs, such as vinblastine, floxuridine, 5-fluorouracil (5-FU), capecitabine, and gemcitabine have been shown to help a small number of patients. Still, chemo is often only used for renal cell carcinoma after targeted drugs and/or immunotherapy have already been tried.
Doctors give chemotherapy in cycles, with each period of treatment followed by a rest period to allow the body time to recover. Chemo cycles generally last a few weeks.
Possible side effects of chemotherapy
Chemo drugs attack cells that are dividing quickly, which is why they often work against cancer cells. But other cells in the body, such as those in the bone marrow (where new blood cells are made), the lining of the mouth and intestines, and the hair follicles, also divide quickly. These cells are also likely to be affected by chemo, which can lead to certain side effects.
The side effects of chemo depend on the type of drugs, the amount taken, and the length of treatment. Possible side effects can include:
- Hair loss
- Mouth sores
- Loss of appetite
- Nausea and vomiting
- Diarrhea or constipation
- Increased chance of infections (due to low white blood cell counts)
- Easy bruising or bleeding (due to low blood platelet counts)
- Fatigue (due to low red blood cell counts)
These side effects usually go away after treatment is finished. There are often ways to prevent or lessen them. For example, drugs can be given to help prevent or reduce nausea and vomiting. Specific chemo drugs may each cause specific side effects. Ask your health care team about the side effects your chemo drugs may cause.
References [ + ]





{kind=link}