Contents
What is Schilling test
The Schilling test is performed to evaluate vitamin B12 absorption. In a Schilling test, you first ingest a tiny amount of radioactive vitamin B-12. Then your blood is checked to see if your body absorbed the vitamin B-12. After that, you ingest a combination of radioactive vitamin B-12 and intrinsic factor. If the radioactive B-12 is absorbed only when taken with intrinsic factor, it confirms that you lack your own intrinsic factor.
The Schilling test is done to diagnose pernicious anemia, which is a form of anemia that is caused by vitamin B12 deficiency. Without sufficient vitamin B12, your body can’t make enough healthy red blood cells. Vitamin B12 is also important for nerve health, to maintain the central nervous system, and is important for metabolism and a vitamin B12 deficiency can lead to varying degrees of neuropathy, nerve damage that can cause tingling and numbness in the affected person’s hands and feet.
Normally, ingested vitamin B12 also known as cobalamin, combines with intrinsic factor, which is produced by the parietal cells in the stomach. Intrinsic factor is necessary for vitamin B12 to be absorbed in the small intestine. Certain diseases, such as pernicious anemia, can result when absorption of vitamin B12 is inadequate.
Vitamin B12 is converted into adenosylcobalamin, which converts L-methylmalonic acid to succinyl coenzyme A; hence, a decrease in vitamin B12 absorption in the intestine can cause an excess of methylmalonic acid (MMA) within the body.
The Schilling test is rarely, if ever, done today. Currently, Schilling test is not readily available in most countries as a means of diagnosis for vitamin B12 deficiency. The level of serum vitamin B12 is now a test of choice in many hospitals 1. Patients with >300 pg/mL are normal, 200 to 300 pg/mL borderline and less than 200 pg/mL classified as deficient in vitamin B12. The levels of homocysteine and methylmalonic acid (MMA) are also usually investigated and elevated in those patients.
Patients with low levels of cobalamin are tested for autoantibodies to intrinsic factor with an immunoassay. Pernicious anemia is usually caused by the presence of autoantibodies against parietal cells that make intrinsic factors and presence of those autoantibodies are considered as a confirmatory test 2. The immunoassay has low sensitivity and specificity 3, and if the physician suspects pernicious anemia and has a negative immunoassay, it is advised to measure gastrin levels. Since parietal cells are also responsible for the production of gastrin level, patients with pernicious anemia will have a low level of gastrin also.
A group of tests is often required to establish the correct diagnosis as determination of vitamin B12 in serum does not detect all cases of vitamin B12 deficiency.
- The most sensitive test for vitamin B12 deficiency at the cellular level is the assay for methylmalonic acid (MMA).
- Nearly half of the cases of pernicious anemia can be unambiguously identified if the serum test for intrinsic factor blocking antibody is positive (this is a simpler and less expensive test than the MMA).
- Serum gastrin is usually markedly increased in pernicious anemia (as a result of gastric atrophy) and this test can be used as a substitute for the more complicated and more expensive Schilling test of intestinal absorption of vitamin B12.
- Normal vitamin B12 levels = 300-914 ng/L
- If vitamin B12 is <150 ng/L, then intrinsic factor blocking antibody is performed. If intrinsic factor blocking antibody is negative or indeterminate, then gastrin is performed.
- If vitamin B12 is 150 to 400 ng/L, then methylmalonic acid (MMA) is performed. If methylmalonic acid is >0.40 nmol/mL, then intrinsic factor blocking antibody is performed.
The substitution of the serum gastrin assay for the Schilling test offers 3 advantages:
- It is an in vitro test that does not require administration of radioisotopes to patients
- It can be performed on mailed-in specimens
- It is much less expensive
Figure 1. Vitamin B-12 evaluation algorithm
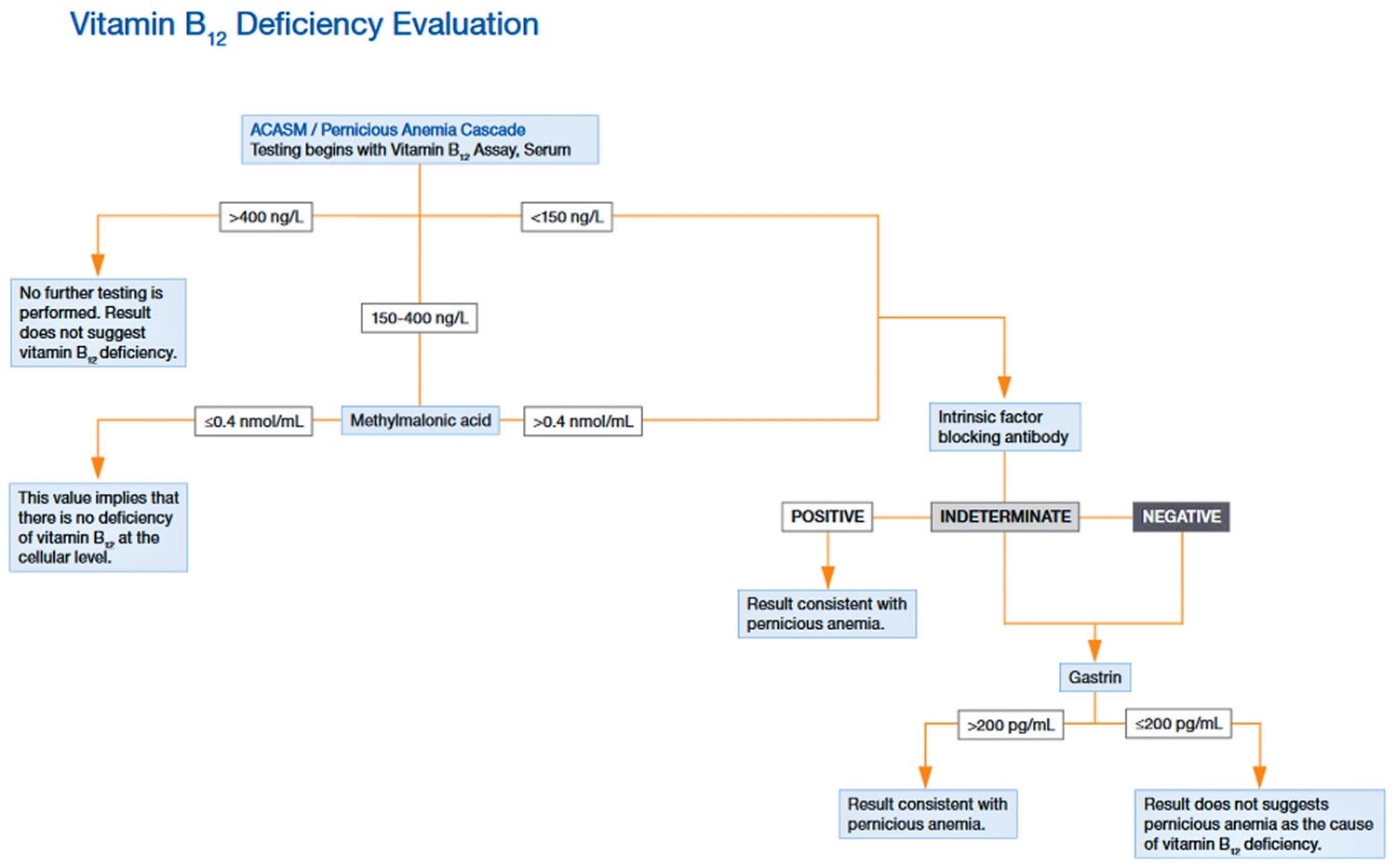 Table 1. Vitamin B12 Test Results Interpretation
Table 1. Vitamin B12 Test Results Interpretation| Vitamin B12 >400 ng/L | Results do not suggest B12 deficiency-no further testing. |
| Vitamin B12 150 to 400 ng/L | Borderline vitamin B12 level-methylmalonic acid (MMA) is performed. If methylmalonic acid (MMA) is >0.40 nmol/mL, then intrinsic factor blocking antibody (IFBA) is performed. |
| Vitamin B12 <150 ng/L | Vitamin B12 deficiency-intrinsic factor blocking antibody is performed. If intrinsic factor blocking antibody is negative or indeterminate, then gastrin is performed. |
| Methylmalonic acid (MMA) < or =0.40 nmol/mL | This value implies that there is no vitamin B12 deficiency at the cellular level. |
| Intrinsic factor blocking antibody positive | Consistent with pernicious anemia, Graves disease, or Hashimoto thyroiditis. |
| Gastrin >200 pg/mL | Result consistent with pernicious anemia. |
| Gastrin <200 pg/mL | Result does not suggest pernicious anemia. |
What is pernicious anemia?
Pernicious anemia is a type of vitamin B12 anemia. Vitamin B12 anemia can result from:
- an inability to absorb vitamin B12; or
- an inadequate dietary intake of vitamin B12.
Vitamin B12 deficiency may present with any combination of the following: macrocytic anemia, glossitis (painful inflammation of the tongue), peripheral neuropathy, weakness, hyperreflexia, ataxia, loss of proprioception, poor coordination, and affective behavioral changes. These manifestations may occur in any combination; many patients present with neurologic symptoms without macrocytic anemia.
Problems absorbing vitamin B12
Pernicious anemia is vitamin B12 deficiency anemia that is caused by a lack of a special substance known as ‘intrinsic factor’ that is needed to absorb vitamin B12. Lack of intrinsic factor is the most common cause of vitamin B12 deficiency.
Intrinsic factor is made by cells called parietal cells in the stomach, and is necessary for vitamin B12 to be to be absorbed in the small bowel. In some people, intrinsic factor is not produced in sufficient amounts, and even with a good diet they cannot absorb enough vitamin B12.
Lack of intrinsic factor can be caused by:
- an auto-immune illness, where the immune system attacks the cells in the stomach that produce intrinsic factor (parietal cells);
- having all or part of the stomach (where intrinsic factor is made) removed; or
- a rare, inherited condition known as congenital pernicious anemia.
Vitamin B12 deficiency may also be due to:
- problems with absorption of vitamin B12 in the small intestine due to part or all of the small intestine being surgically removed or affected by disease (such as Crohn’s disease, coeliac disease or infection); or
- a side effect from certain medicines, such as some type 2 diabetes and seizure medicines and some medicines used to treat gastro-oesophageal reflux, which can interfere with vitamin B12 absorption.
Problems with vitamin B12 intake
An inadequate intake of foods that contain vitamin B12, such as meat, seafood, dairy products, mushrooms, eggs and foods fortified with vitamin B12 can lead to vitamin B12 deficiency anemia. Vegans and people with a poor diet may be at risk.
Vitamin B-12 deficiency including pernicious anemia treatment
For milder cases of vitamin B-12 deficiency, treatment may involve changes to your diet and vitamin B-12 supplements in pill form or as a nasal spray. Your doctor may suggest vitamin B-12 injections, particularly if your vitamin B-12 deficiency is severe. At first, you may receive the shots as often as every other day. Eventually, you’ll need injections just once a month, which may continue for life, depending on your situation.
Schilling test procedure
The Schilling Test is divided into 2 main stages 1.
The physician should make sure that the patient has no allergy to the radiolabeled cobalamin administered.
Stage 1
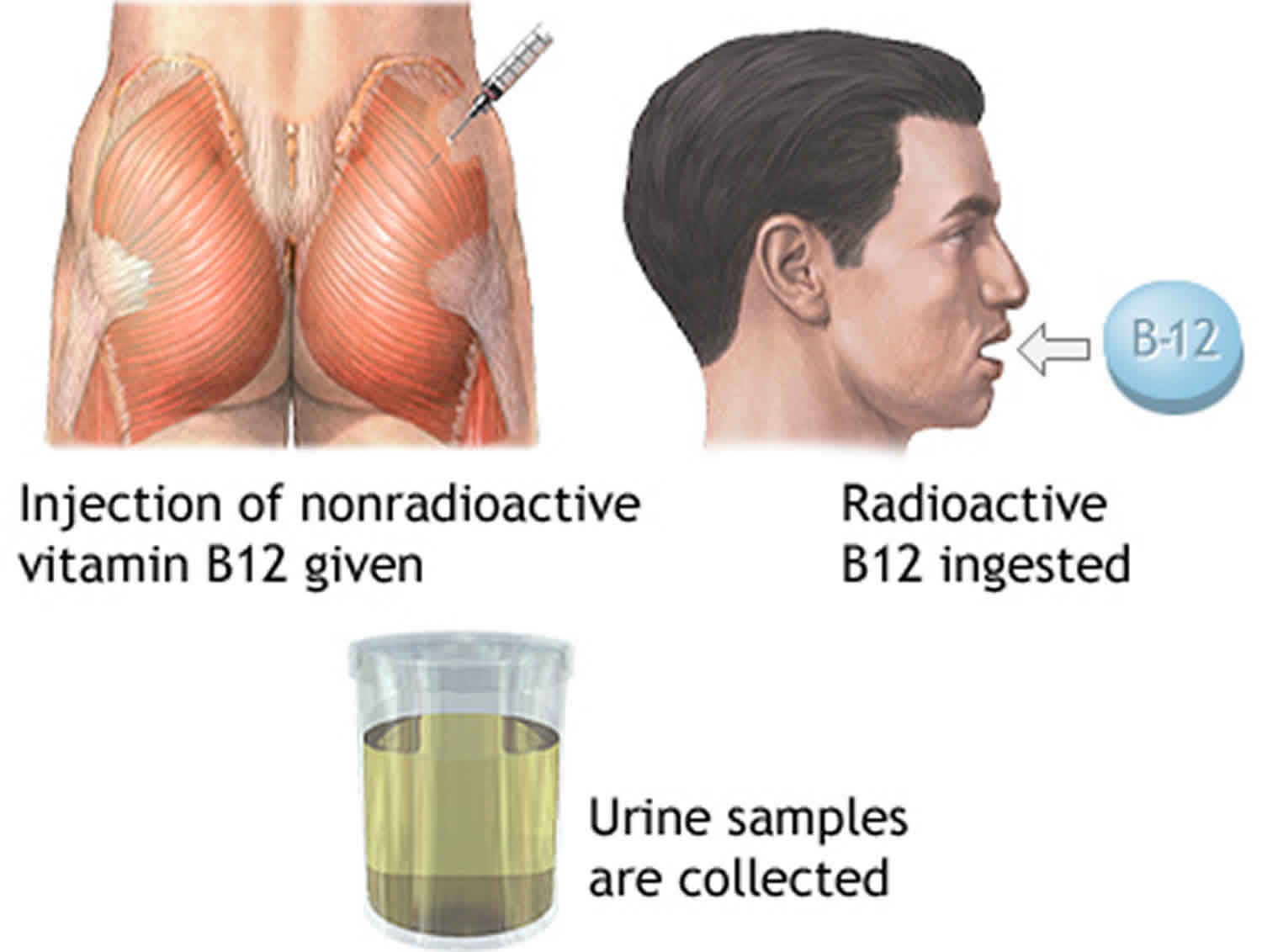
- The patient is given radiolabeled vitamin B12 orally, following an intramuscular (IM) dose of unlabeled vitamin B12 one hour later. The injection is given to ensure that none of the radioactive B12 binds to any vitamin B12 depleted tissues, for example, the liver. A 24-hour urine collection monitors the absorption and the excretion.
If stage 1 is abnormal, stage 2 may be done 3 to 7 days later.
Stage 2
- If the previous stage provides an abnormal result, stage 2 can be done to assess whether there is a deficiency of intrinsic factor. Stage 1 is repeated along with an oral dose of intrinsic factor. A 24-hour urine collection is carried out to assess the level of vitamin B12.
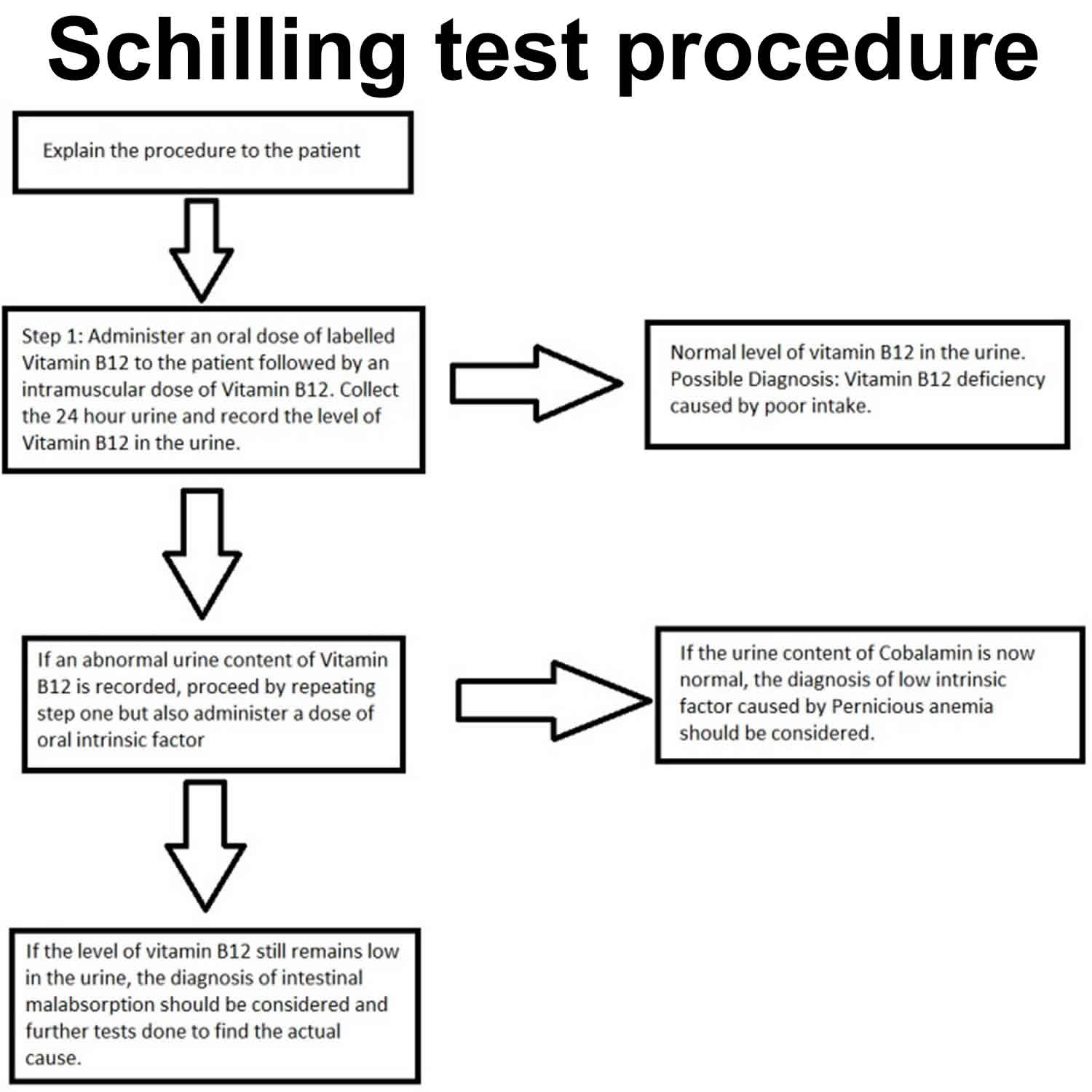
During Stage 1, a healthy person will be able to absorb the administered radioactive B12 in their terminal ileum. It will then be excreted in the urine. If there are any defects with the cubam receptor at the terminal ileum, the result will show a low level of labeled cobalamin in urine as it will remain in the intestines and is likely to be excreted in feces. A defect associated with low levels of an intrinsic factor will also produce a similar abnormal result.
Patients with an abnormally low level of cobalamin in the urine in stage 1 usually undergo stage 2. If stage 2 shows a normal level of excreted vitamin B12, it means that the patient has low levels of intrinsic factor and one possible cause is pernicious anemia. If the test still indicates a low level of vitamin B12 in the urine, it means that the patient has a poor intestinal absorption of cobalamin. Further tests should be done to assess the cause of malabsorption that can include Crohn’s disease, small bowel bacterial overgrowth syndrome, and infection by Diphyllobothrium latum.
Figure 2. Schilling test procedure
Normal and Critical Findings
Stage 1
A normal patient will show a normal level of cobalamin in urine upon administration of the oral dose. If the urine level is abnormal, it can be from either an absorption defect in the terminal ileum or a lack of intrinsic factor.
Excreting 8% to 40% of the radioactive vitamin B12 in the urine within 24 hours is considered a normal finding. The values, however, may fluctuate between laboratories.
Stage 2
If the abnormal result of stage 1 improves with administration of Intrinsic factor, it means that the patient has intrinsic factor deficiency. If the patient still has a low urine level of cobalamin, it means that there is an absorption defect in the terminal ileum and further tests should be done to investigate.
- Ramphul K, Mejias SG. Schilling Test. [Updated 2018 Oct 27]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK507784[↩][↩]
- Green R. Vitamin B12 deficiency from the perspective of a practicing hematologist. Blood. 2017 May 11;129(19):2603-2611.[↩]
- Carmel R. Reassessment of the relative prevalences of antibodies to gastric parietal cell and to intrinsic factor in patients with pernicious anaemia: influence of patient age and race. Clin. Exp. Immunol. 1992 Jul;89(1):74-7.[↩]





{kind=link}