
Skin rash
It is difficult to comprehensively review generalized skin rashes because the topic is so broad. Diagnostic errors involving generalized skin rashes are common 1, 2. However, accurate diagnosis is important because treatment varies depending on the cause and because some skin rashes can be life-threatening if not treated promptly. Some generalized skin rashes have distinctive features that allow immediate recognition, such as psoriasis (silvery white scale on the knees and elbows), pityriasis rosea (herald patch) and atopic dermatitis (lichenified skin in flexural areas). But these conditions, like many others, can present with similar appearances and can be mistaken for each other.
Skin rash causes
The causes of a generalized skin rash are numerous, but most patients have common diseases (Table 1). Many common skin rashes improve spontaneously or with simple measures, such as discontinuing a medication. Life-threatening skin rashes are rare in the United States, so they can be easily missed because they are not considered.
Table 1. Common Causes of Generalized Skin Rash
| Condition | Key clinical features | Tests |
|---|---|---|
Atopic dermatitis | Dry skin; pruritus; erythema; erythematous papules; excoriations; scaling; lichenification; accentuation of skin lines; keys to diagnosis are pruritus, eczematous appearance of lesions, and personal or family history of atopy | Skin biopsy is nonspecific and not often done* |
Contact dermatitis | Erythema; edema; vesicles; bullae in linear or geometric pattern; common causes include cosmetics, topical medications, metal, latex, poison ivy, textiles, dyes, sunscreens, cement, food, benzocaine, neomycin; keys to diagnosis are linear or geometric pattern and distribution of lesions | Skin biopsy is nonspecific and not often done,* but it can help exclude other conditions |
Drug eruption† | Many patterns, but most commonly maculopapular (95% of cases), common in patients taking allopurinol (Zyloprim), beta-lactam antibiotics, sulfonamides, anticonvulsants, angiotensin-converting enzyme inhibitors, nonsteroidal anti-inflammatory drugs, hypoglycemics, and thiazide diuretics, but can occur with almost any drug; usually appears within 1 to 4 weeks of initiating drug; key to diagnosis is timing of rash appearance in relation to drug use | Skin biopsy is usually nonspecific and not often done* |
Erythema multiforme | Round, dusky red lesions that evolve into target (iris) lesions over 48 hours; starts on backs of hands and feet and on extensor surfaces of arms and legs; symmetric; may involve palms, soles, oral mucous membranes, or lips; key to diagnosis is presence of target lesions | Skin biopsy is generally diagnostic and occasionally done; biopsy should be taken from the erythematous (not blistered) portion of the target |
Fifth disease (i.e., erythema infectiosum)† | “Slapped cheek” appearance with sparing of periorbital areas and nasal bridge; unique fishnet pattern; erythema on extremities, trunk, and buttocks; keys to diagnosis in children are slapped cheek appearance and net-like rash, and in adults are arthralgias and history of exposure to affected child | Parvovirus B19 serology; skin biopsy is nonspecific and rarely done* |
Folliculitis | Multiple small pustules localized to hair follicles on any body surface; key to diagnosis is hair follicle at center of each lesion | Skin biopsy is often diagnostic but not often done* |
Guttate psoriasis | Pinpoint to 1-cm scaling papules and plaques on trunk and extremities; often preceded by streptococcal pharyngitis 1 to 2 weeks before eruption; keys to diagnosis are scaling and history of streptococcal pharyngitis | Throat culture; antistreptolysin O titer; early skin biopsy may not be diagnostic and is not often done* |
Insect bites | Urticarial papules and plaques; keys to diagnosis are outdoor exposure (usually) and distribution of lesions where insects are likely to bite | Skin biopsy is nonspecific and not often done* |
Keratosis pilaris | Pinpoint follicular papules and pustules on posterolateral upper arms, cheeks, anterior thighs, or buttocks; keys to diagnosis are upper arm distribution, absence of comedones, and tiny palpable lesions | Skin biopsy can be diagnostic but is not often done* |
Lichen planus | Violaceous flat-topped papules and plaques; commonly on ankles and wrists; 5 P’s (pruritic, planar, polygonal, purple plaques); Wickham striae (reticular pattern of white lines on surface of lesions); lacy white buccal mucosal lesions; Koebner phenomenon (development of typical lesions at the site of trauma); keys to diagnosis are purple color and distribution of lesions | Skin biopsy is diagnostic and often done |
Miliaria rubra (i.e., prickly heat, heat rash) | Erythematous nonfollicular papules associated with heat exposure or fever; lesions on back, trunk, neck, or occluded areas; keys to diagnosis are history of heat exposure and distribution of lesions | Skin biopsy can be diagnostic but is not often done* |
Nummular eczema | Sharply defined, 2- to 10-cm, coin-shaped, erythematous, scaled plaques; lesions on dorsal hands and feet, extensor surfaces of arms and legs, flanks, and hips; key to diagnosis is sharply defined, round, erythematous, scaled lesions | Skin biopsy is nonspecific and not often done,* but it may help exclude other diagnoses |
Pityriasis rosea | Discrete, round to oval, salmon pink, 5- to 10-mm lesions; “Christmas tree” pattern on back; often (17 to 50%) preceded by solitary 2- to 10-cm oval, pink, scaly herald patch; keys to diagnosis are oval shape, orientation with skin lines, and distinctive scale | Skin biopsy is nonspecific and not often done,* but it may help exclude other diagnoses; rapid plasma reagin testing is optional to rule out secondary syphilis |
Psoriasis (plaque psoriasis) | Thick, sharply demarcated, round or oval, erythematous plaques with thick silvery white scale; lesions on extensor surfaces, elbows, knees, scalp, central trunk, umbilicus, genitalia, lower back, or gluteal cleft; positive Auspitz sign (removal of scale produces bleeding points); Koebner phenomenon; keys to diagnosis are distinctive scale and distribution of lesions | Skin biopsy can be diagnostic but is not often done* |
Roseola (i.e., exanthem subitum, sixth disease) | Sudden onset of high fever without rash or other symptoms in a child younger than 3 years; as fever subsides, pink, discrete, 2- to 3-mm blanching macules and papules suddenly appear on trunk and spread to neck and extremities; key to diagnosis is high fever followed by sudden appearance of rash as fever abruptly resolves | Skin biopsy is nonspecific and not often done* |
Scabies | Discrete, small burrows, vesicles, papules, and pinpoint erosions on fingers, finger webs, wrists, elbows, knees, groin, buttocks, penis, scrotum, axillae, belt line, ankles, and feet; keys to diagnosis are distribution of lesions, intense pruritus, and positive mineral oil mount | Mineral oil mount is routinely done to identify mites or eggs; skin biopsy is usually nonspecific and not often done* |
Seborrheic dermatitis | Erythematous patches with greasy scale; lesions behind ears or on scalp and scalp margins, external ear canals, base of eyelashes, eyebrows, nasolabial folds, central chest, axillae, inframammary folds, groin, and umbilicus; keys to diagnosis are greasy scale and distribution of lesions | Skin biopsy is nonspecific and not often done* |
Tinea corporis | Flat, red, scaly lesions progressing to annular lesions with central clearing or brown discoloration; keys to diagnosis are annular lesions with central clearing and positive KOH preparation | KOH preparation is routinely done; skin biopsy can be diagnostic but is not often done* |
Urticaria (i.e., hives) | Discrete and confluent, raised, edematous, round or oval, waxing and waning lesions with large variation in size; may have erythematous border (flare) and pale center (wheal); patient may have history of drug, food, or substance exposure; key to diagnosis is distinctive appearance of edematous lesions | Skin biopsy is nonspecific and not often done* |
Varicella† | Vesicles on erythematous papules (“dewdrop on rose petal” appearance); all stages (papules, vesicles, pustules, crusts) are present at the same time and in close proximity; keys to diagnosis are crops of lesions in different stages, systemic illness, and exposure to persons with the infection | Diagnosis is usually clinical, but real-time polymerase chain reaction assay of skin lesion or direct fluorescent antibody testing of skin scrapings could be done; skin biopsy is often diagnostic but cannot distinguish herpes zoster or herpes simplex, and is not often done* |
Viral exanthem, nonspecific | Blanchable, red, sometimes confluent macules and papules; may be indistinguishable from drug eruptions; keys to diagnosis are nonspecific generalized maculopapular rash in a child with systemic symptoms (fever, diarrhea, headache, fatigue) | Skin biopsy is nonspecific and not often done* |
KOH = potassium hydroxide.
*— Skin biopsy is often not performed because the histology is nonspecific or because a biopsy is usually not needed for diagnosis.
†— Rashes that can have serious consequences for the patient or pregnant contacts of the patient.
Table 2. Uncommon Causes of Generalized Skin Rash
| Condition | Key clinical features | Tests |
|---|---|---|
Bullous pemphigoid | Generalized bullae, especially on trunk and flexural areas; patient usually older than 60 years; Nikolsky sign (easy separation of epidermis from dermis with lateral pressure) usually negative | Skin biopsy with direct and indirect immunofluorescence is diagnostic and usually done |
Dermatitis herpetiformis | Symmetric, pruritic, urticarial papules and vesicles that are often excoriated and isolated or grouped on extensor surfaces (knees, elbows), buttocks, and posterior scalp; most patients have celiac disease, but it is often asymptomatic; diagnosis is often delayed | Skin biopsy with direct immunofluorescence is diagnostic and routinely done |
HIV acute exanthem* | Diffuse, nonspecific, erythematous, maculopapular, nonpruritic lesions; fever, fatigue, headache, lymphadenopathy, pharyngitis, myalgias, and gastrointestinal disturbances | Measurement of quantitative plasma HIV-1 RNA levels (viral load) by polymerase chain reaction; HIV serology (delay at least 1 month after acute illness); skin biopsy is nonspecific and not often done† |
Id reaction | Follicular papules or maculopapular or vesiculopapular rash involving forearms, thighs, legs, trunk, or face; associated with active dermatitis (e.g., stasis dermatitis) or fungal infection elsewhere | KOH preparation to diagnose dermatophyte infection; skin biopsy is nonspecific and not often done† |
Kawasaki disease* | Erythematous rash on hands and feet starting 3 to 5 days after onset of fever in children younger than 8 years (usually younger than 4 years); blanching macular exanthem on trunk, especially groin and diaper area; hyperemic oral mucosa and red, dry, cracked, bleeding lips | CBC to detect elevated white blood cell and platelet counts; measurement of C-reactive protein level and erythrocyte sedimentation rate; skin biopsy is nonspecific and not often done† |
Lupus (subacute cutaneous lupus erythematosus) | Papulosquamous or annular pattern, mainly on trunk and sun-exposed face and arms; can be drug induced | Antinuclear antibody testing; skin biopsy with direct immunofluorescence is diagnostic and often done |
Lyme disease* | Erythema migrans at site of tick bite, progressing to generalized macular lesions on proximal extremities, chest, and creases (median lesion size, 15 cm); history of outdoor activities; most common in northeastern U.S. seaboard, Minnesota, and Wisconsin | Serology; skin biopsy is nonspecific and not often done† |
Meningococcemia* | Nonblanching petechiae and palpable purpura, which may have gunmetal gray necrotic centers; usually spares palms and soles; may start as erythematous papules or pink macules | Positive cultures of blood, lesions, and cerebrospinal fluid; positive buffy coat Gram stain; skin biopsy is usually nonspecific and not often done† |
Mycosis fungoides (i.e., cutaneous T-cell lymphoma) | Flat erythematous macules evolving into red scaly plaques with indistinct edges and poikiloderma (atrophy, white and brown areas, telangiectasia); can present as erythroderma (Sézary syndrome); diagnosis is often delayed; often confused with eczema | Skin biopsy is diagnostic and routinely done |
Rocky Mountain spotted fever* | 2- to 6-mm macules that spread centrally from wrists and ankles and that progress to papules and petechiae; often involves palms and soles; fever, severe headache, photophobia, myalgias, abdominal pain, nausea, and vomiting; history of outdoor activities in endemic area (e.g., Oklahoma, Tennessee, Arkansas, southern Atlantic states) | Serology; skin biopsy with direct fluorescent antibody testing is diagnostic and often done, if available |
Scarlet fever* | Blanching sandpaper-like texture follows streptococcal pharyngitis or skin infection; Pastia lines (petechiae in antecubital and axillary folds); fever, vomiting, headache, and abdominal pain; most common in children | Antistreptolysin O titer; throat culture; skin biopsy is nonspecific and not often done† |
Secondary syphilis* | Variable morphology, but usually red-brown scaly papules with involvement of the palms and soles; oral and genital mucosa also commonly affected | Positive syphilis serology (usually done); skin biopsy can be nonspecific and is not often done† |
Staphylococcal scalded skin syndrome* | Starts with painful, tender sandpaper-like erythema favoring flexural areas, and progresses to large, flaccid bullae; positive Nikolsky sign; most common in children younger than 6 years | Skin biopsy is diagnostic and routinely done to distinguish from toxic epidermal necrolysis, which is rare in infancy and childhood; frozen section biopsy should be considered; eyes, nose, throat, and bullae should be cultured for Staphylococcus aureus |
Stevens-Johnson syndrome* Toxic epidermal necrolysis* | Stevens-Johnson syndrome: vesiculobullous lesions on the eyes, mouth, genitalia, palms, and soles; usually drug induced Toxic epidermal necrolysis: life-threatening condition with diffuse erythema, fever, and painful mucosal lesions; positive Nikolsky sign | Skin biopsy is diagnostic and routinely done for toxic epidermal necrolysis; frozen section biopsy should be considered |
Sweet syndrome (i.e., acute febrile neutrophilic dermatosis) | Red, tender papules that evolve into painful erythematous plaques and annular lesions on upper extremities, head, neck, backs of hands, and back; most common in middle-aged and older women | Skin biopsy is diagnostic and routinely done |
Toxic shock syndrome* | Diffuse erythema (resembling sunburn); fever, malaise, myalgia, nausea, vomiting, hypotension, diarrhea, and confusion; conjunctival injection, mucosal hyperemia (oral or genital); late desquamation, especially on palms and soles; most common in menstruating women or postoperative patients | CBC to detect thrombocytopenia; blood cultures; skin biopsy is nonspecific and not often done† |
CBC = complete blood count; HIV = human immunodeficiency virus; KOH = potassium hydroxide.
*— Rashes that can have serious consequences for the patient or pregnant contacts of the patient.
† — Skin biopsy is often not performed because the histology is nonspecific or because a biopsy is usually not needed for diagnosis.
Table 3. Rare Causes of Generalized Skin Rash
| Condition | Key clinical features | Tests |
|---|---|---|
Lichen nitidus | 1- to 3-mm, skin-colored, raised, flat-topped papules on trunk, flexor surfaces of extremities, dorsal hands, or genitalia | Skin biopsy is diagnostic and often done |
Pityriasis lichenoides | 2- to 10-mm, round or oval, red-brown papules progressing to hemorrhagic lesions on trunk, thighs, or upper arms | Skin biopsy is diagnostic and routinely done |
Pityriasis rubra pilaris | Red or orange follicular papules on fingers, elbows, knees, trunk, or scalp; often mistaken for psoriasis; characterized by “skip areas” of normal skin | Skin biopsy is occasionally nonspecific but can help exclude other conditions, and is routinely done |
Rickettsialpox | Initial lesion, which may not be noticed by patient, begins as papule and evolves to vesicle, then crusts; generalized maculopapular vesicular exanthem can involve palms and soles; most common in large cities | Serology (immunoglobulin G for Rickettsia rickettsii and Rickettsia akari); biopsy with direct fluorescent antibody testing may be diagnostic but is not often done* |
Rubella† | Round, pink macules and papules starting on forehead, neck, and face, then spreading to trunk and extremities, including palms and soles | Serology; skin biopsy is nonspecific and not often done* |
Rubeola | Maculopapular purple-red lesions that may become confluent; start on face and behind ears and at anterior hairline; Koplik spots (i.e., tiny red or white spots with red halo on buccal mucosa) | Serology; skin biopsy is usually nonspecific and not often done* |
*— Skin biopsy is often not performed because the histology is nonspecific or because a biopsy is usually not needed for diagnosis.
†— Rashes that can have serious consequences for the patient or pregnant contacts of the patient.
Table 4. Skin Rashes That Are Often Confused with Each Other
| Condition | Similar rashes (distinguishing features) |
|---|---|
Atopic dermatitis | Contact dermatitis (not associated with dry skin) |
Keratosis pilaris (nonpruritic, involves posterolateral upper arms) | |
Mycosis fungoides (lesion borders sharper, fixed size and shape) | |
Psoriasis (well-defined plaques, silvery white scale, involves extensor surfaces) | |
Scabies (involves genitalia, axillae, finger webs) | |
Seborrheic dermatitis (nonpruritic, greasy scale, characteristic distribution) | |
Contact dermatitis | Atopic dermatitis (symmetric distribution, history of hay fever or asthma, flexural areas, hyperlinear palms, family history, not limited to area of exposure, dry skin and itching precede skin lesions rather than follow them) |
Dermatitis herpetiformis (vesicles on extensor surfaces, enteropathy, burning pain) | |
Psoriasis (patches on knees, elbows, scalp, and gluteal cleft; pitted nails) | |
Seborrheic dermatitis (greasy scale on eyebrows, nasolabial folds, or scalp) | |
Drug eruption (morbilliform) | Erythema multiforme (target lesions) |
Viral exanthem (more common in children, less intense erythema and pruritus, less likely to be dusky red, more focal systemic symptoms, less likely to be polymorphic, less likely to be associated with eosinophilia) | |
Pityriasis rosea | Drug eruption (no scale, lesions coalesce) |
Erythema multiforme (target lesions) | |
Guttate psoriasis (thicker scale, history of streptococcal pharyngitis) | |
Lichen planus (violaceous, involves wrists and ankles) | |
Nummular eczema (larger round [not oval] lesions, do not follow skin lines) | |
Psoriasis (thick white scale, involves extensor surfaces) | |
Secondary syphilis (positive serology; involves palms and soles) | |
Tinea corporis (positive KOH preparation, scale at peripheral border of lesions rather than inside border) | |
Viral exanthem (no scale, lesions coalesce) | |
Psoriasis | Atopic dermatitis (atopic features, flexural areas, lichenification) |
Lichen planus (violaceous, minimal scale, involves wrists and ankles) | |
Mycosis fungoides (lesion borders less distinct) | |
Pityriasis rubra pilaris (islands of normal skin) | |
Seborrheic dermatitis (greasy scale, involves anterior face) | |
Secondary syphilis (red-brown lesions on palms and soles) | |
Tinea corporis (thinner peripheral scale, positive KOH preparation) | |
Seborrheic dermatitis | Atopic dermatitis (nongreasy scale, atopic history, pruritic) |
Psoriasis (silver scale, sharply demarcated lesions on extensor surfaces of extremities; involvement of scalp commonly extends onto forehead, whereas seborrheic dermatitis of scalp stops at scalp margin) |
KOH = potassium hydroxide.
How is skin rash diagnosed ?
Accurate diagnosis of the generalized skin rash can be difficult because of the nonspecific appearance of many rashes.
Patients with acute generalized maculopapular skin rashes and no systemic symptoms are often treated symptomatically without a definitive diagnosis. If the skin rash does not resolve spontaneously, skin biopsy and blood testing (e.g., serologies, complete blood count) may be indicated. There are no widely accepted guidelines that address indications for skin biopsy, but Table1, 2 and Table 3 include common clinical practices. The patient should be referred to a dermatologist if the skin rash is progressive or does not resolve with observation or empiric treatment. For example, mycosis fungoides (cutaneous T-cell lymphoma) mimics eczema in its early stages and is rarely diagnosed correctly at initial presentation 33. Reevaluation and possible referral are imperative in chronic eczematous conditions that do not respond to therapy.
It is important to look beyond the appearance of the skin rash itself and search for clues from the patient’s history, physical examination, laboratory tests, and skin biopsy.
Patient History
When the diagnosis of a generalized rash is not obvious, patients should be asked about recent travel, insect and plant exposure, drug exposure (including over-the-counter drugs, alternative medications, and illicit drugs), contact with persons who are ill, pets, hobbies, occupational exposures, chemical exposure, chronic illness, sexual history, and recent systemic symptoms, especially fever (Table 5). Patients should be asked about itchy skin, painful lesions, the initial site of involvement, and any personal or family history of atopy (e.g., asthma, allergic rhinitis, childhood eczema).
Table 5. Generalized Skin Rash: Conditions Suggested by Patient History
| Historical finding | Conditions |
|---|---|
Chemicals | Contact dermatitis |
Chronic illness | Dermatitis herpetiformis |
Seborrheic dermatitis | |
Contact with ill persons | Fifth disease (i.e., erythema infectiosum) |
Meningococcemia | |
Roseola (i.e., exanthem subitum, sixth disease) | |
Rubella | |
Rubeola | |
Scarlet fever | |
Varicella | |
Viral exanthem, nonspecific | |
Drug exposure | Lupus (subacute cutaneous lupus erythematosus) |
Drug eruption | |
Urticaria (i.e., hives) | |
Hobbies | Contact dermatitis |
Insect and arthropod exposure | Insect bites |
Lyme disease | |
Rickettsialpox | |
Rocky Mountain spotted fever | |
Scabies | |
Occupational exposures | Contact dermatitis |
Plant exposure | Contact dermatitis |
Recent systemic symptoms, fever | Fifth disease (i.e., erythema infectiosum) |
HIV acute exanthem | |
Kawasaki disease | |
Meningococcemia | |
Roseola (i.e., exanthem subitum, sixth disease) | |
Rubella | |
Rubeola | |
Scarlet fever | |
Varicella | |
Viral exanthem, nonspecific | |
Sexual history | HIV acute exanthem |
Secondary syphilis | |
Travel | Insect bites |
Lyme disease | |
Rickettsialpox | |
Rocky Mountain spotted fever |
HIV = human immunodeficiency virus.
The patient’s age may help narrow the possible diagnoses. For example, acute maculopapular rashes in children are usually caused by viral infections, whereas in adults they are usually caused by drug reactions 17. Some rashes are rare in children (e.g., nummular eczema, lichen planus, dermatitis herpetiformis), whereas others are rare in adults (e.g., roseola, Kawasaki disease, scarlet fever).
Patients should be asked about itchy skin, because some conditions routinely cause intense pruritus (e.g., scabies, urticaria, atopic dermatitis), whereas others are usually nonpruritic (e.g., seborrheic dermatitis, secondary syphilis, many viral exanthems; Table 6). Most generalized skin rashes are not painful, but Sweet syndrome, Kawasaki disease, and Stevens-Johnson syndrome are exceptions.
Table 6. Generalized Skin Rash: Conditions Associated with Itchy Skin
| Common | Variable | Absent or rare |
|---|---|---|
Atopic dermatitis | Drug eruption* | Fifth disease (i.e., erythema infectiosum)* |
Contact dermatitis | Erythema multiforme | HIV acute exanthem* |
Insect bites | Folliculitis | Keratosis pilaris |
Lichen planus | Guttate psoriasis | Lyme disease* |
Nummular eczema | Kawasaki disease* | Meningococcemia* |
Scabies | Pityriasis rosea | Miliaria rubra (i.e., prickly heat, heat rash) |
Urticaria (i.e., hives) | Psoriasis (plaque psoriasis) | Rocky Mountain spotted fever* |
Varicella* | Tinea corporis | Roseola (i.e., exanthem subitum, sixth disease) |
Toxic epidermal necrolysis* | Rubella* | |
Toxic shock syndrome (late)* | Scarlet fever* | |
Viral exanthem, nonspecific | Seborrheic dermatitis | |
Secondary syphilis* | ||
Staphylococcal scalded skin syndrome* | ||
Stevens-Johnson syndrome* |
Note: Table 6 includes all common skin rashes and all skin rashes that can have serious consequences for the patient or pregnant contacts of the patient (designated by *).
HIV = human immunodeficiency virus.
Systemic symptoms, especially fever, can help narrow the differential diagnosis 32. Skin rashes accompanied by fever are most commonly associated with infections, but drug eruptions and rheumatologic diseases can also cause fever. Although most maculopapular skin rashes that are associated with fever are caused by self-limited viral infections, empiric antibiotics and laboratory testing are indicated when the history, geography, demographics, and systemic manifestations suggest a more serious infection (e.g., meningococcemia, Lyme disease, Rocky Mountain spotted fever). Petechial skin rashes require immediate decisions about empiric antibiotics, but life-threatening infections characterized by petechiae (e.g., meningococcemia, Rocky Mountain spotted fever) can start as nonspecific maculopapular skin rashes 25.
Physical Examination
Characteristics of skin rash itself can help narrow the differential diagnosis. In dermatologic diagnosis, it is often helpful to focus on the clinical appearance of the rash after determining the patient’s primary symptom, but before taking a more focused history. The size of individual lesions can vary from pinpoint to total-body redness (i.e., erythroderma; Table 7). The shape of individual lesions and their tendency to cluster can also provide important clues. For example, linear patterns of erythema or vesicles are typical of poison ivy; oval lesions are typical of pityriasis rosea; round lesions are typical of nummular eczema; annular lesions are typical of tinea corporis; and geometric patterns may imply a contact component. The color of the lesions should also be noted. Although most generalized skin rashes are pink or red, lichen planus is characterized by violaceous lesions, and secondary syphilis by red-brown lesions.
Table 7. Generalized Skin Rash: Conditions Suggested by Size of Lesions
| Size of lesions | Conditions |
|---|---|
Pinpoint | Folliculitis |
Keratosis pilaris | |
Scarlet fever* | |
1 mm to 1 cm | Guttate psoriasis |
Insect bites† | |
Lichen planus | |
Miliaria rubra (i.e., prickly heat, heat rash) | |
Rocky Mountain spotted fever* | |
Roseola (i.e., exanthem subitum, sixth disease) | |
Rubella* | |
Scabies | |
Varicella* | |
1 to 25 cm | Lyme disease* |
Nummular eczema | |
Tinea corporis | |
Urticaria (i.e., hives) | |
Variable | Atopic dermatitis |
Contact dermatitis | |
Drug eruption* | |
Erythema multiforme | |
Fifth disease (i.e., erythema infectiosum)* | |
HIV acute exanthem* | |
Kawasaki disease* | |
Meningococcemia* | |
Pityriasis rosea | |
Psoriasis (plaque psoriasis) | |
Seborrheic dermatitis | |
Secondary syphilis* | |
Staphylococcal scalded skin syndrome* | |
Stevens-Johnson syndrome* | |
Toxic epidermal necrolysis* | |
Viral exanthem, nonspecific | |
Erythroderma possible | Atopic dermatitis |
Drug eruption* | |
Psoriasis (plaque psoriasis) | |
Sézary syndrome (i.e., chronic cutaneous T-cell lymphoma) | |
Toxic shock syndrome* |
note: Table includes all common rashes and all rashes that can have serious consequences for the patient or pregnant contacts of the patient (designated by *).
HIV = human immunodeficiency virus.
†—Some insect bites may be larger than 1 cm.
In addition to the rash itself, the physician should evaluate the patient’s lymph nodes, neurologic status, body temperature, and general appearance. Patients with fever and toxic appearance require prompt evaluation and possibly empiric treatment before reaching a definitive diagnosis.
Dermatologic Signs
Several dermatologic signs may help narrow the differential diagnosis. For example, the Koebner phenomenon (i.e., development of typical lesions at the site of trauma) is characteristic of psoriasis and lichen planus 35. The Nikolsky sign (i.e., easy separation of the epidermis from the dermis with lateral pressure) is associated with staphylococcal scalded skin syndrome and toxic epidermal necrolysis 36. The value of the Auspitz sign (i.e., the appearance of bleeding points when scale is removed from psoriatic lesions) in the diagnosis of patients with psoriasis has been questioned because of its low sensitivity and specificity 37. Blanching of erythematous lesions with brief downward pressure implies that the erythema is the result of vasodilation rather than dermal hemorrhage. Blanching is characteristic of drug eruptions, viral exanthems, Kawasaki disease, roseola, and scarlet fever, whereas the lesions of meningococcemia and the late petechial stage of Rocky Mountain spotted fever do not blanch. The physician should note the presence and quality of scale (e.g., psoriasis, tinea corporis, pityriasis rosea); whether the lesions are evanescent (e.g., urticaria) or stable (e.g., erythema multiforme); and whether lesions tend to become confluent (e.g., urticaria) or remain discrete (e.g., insect bites). When atopic dermatitis is considered, the physician should search for other signs of atopy, such as palmar hyper-linearity, infraorbital folds (Dennie-Morgan lines), dry skin, and lichenification 38.
Rash Location
Many rashes tend to avoid or favor certain regions of the body. Physicians should note whether the rash involves the palms, soles, mucous membranes, face, scalp, or extensor or flexor surfaces of extremities. For example, psoriasis usually does not involve the central face, and many generalized rashes avoid the palms and soles, whereas secondary syphilis, erythema multiforme, and rickettsial infections typically include the palms and soles (Table 8). Keratosis pilaris commonly involves the posterolateral upper arms. Scabies involves the fingers, finger webs, wrists, elbows, knees, groin, buttocks, penis, axillae, belt line, ankles, and feet. Seborrheic dermatitis most often involves the scalp margins, the area behind the ears, external ear canals, base of eyelashes, eyebrows, nasolabial folds, and central chest. Patients should be asked where the rash first appeared, because some rashes have a characteristic progression. For example, pityriasis rosea often starts with a relatively large herald patch on the trunk or proximal extremity several days before the smaller oval lesions appear. Rocky Mountain spotted fever often starts on the wrists and ankles before spreading centrally 25.
Table 8. Generalized Skin Rash: Involvement of Palms and Soles
| Common | Variable | Absent or rare |
|---|---|---|
Contact dermatitis Erythema multiforme Kawasaki disease* Rocky Mountain spotted fever* Rubella* Scabies (in infants) Secondary syphilis* Staphylococcal scalded skin syndrome* Stevens-Johnson syndrome* Tinea corporis Toxic epidermal necrolysis* Toxic shock syndrome* | Atopic dermatitis Drug eruption* HIV acute exanthem* Lichen planus Meningococcemia* Psoriasis (plaque psoriasis) Urticaria (i.e., hives) | Fifth disease (i.e., erythema infectiosum)* Folliculitis Guttate psoriasis Insect bites Keratosis pilaris Lyme disease* Miliaria rubra (i.e., prickly heat, heat rash) Nummular eczema Pityriasis rosea Roseola (i.e., exanthem subitum, sixth disease) Scarlet fever*† Seborrheic dermatitis Varicella* Viral exanthem, nonspecific |
Note: Table 8 includes all common skin rashes and all skin rashes that, if left untreated, can have serious consequences for the patient or pregnant contacts of the patient (designated by *).
HIV = human immunodeficiency virus.
†—Palms and soles can desquamate.
TESTS
Blood tests that may be helpful include a complete blood count to determine the presence of leukocytosis or thrombocytopenia, and serologic studies to identify various infectious causes. Mineral oil mounts and potassium hydroxide scrapings can be helpful when scabies or dermatophytes are considered. Skin biopsy, with or without direct or indirect immunofluorescence, is often helpful, especially to confirm lichen planus, dermatitis herpetiformis, mycosis fungoides, and staphylococcal scalded skin syndrome 13.
“Don’t-Miss” Skin Rashes
“Don’t-miss” skin rashes are those that can have serious consequences for the patient or pregnant contacts of the patient. These rashes include various infectious diseases, such as meningococcemia, Lyme disease, and Rocky Mountain spotted fever. Many of these rashes are associated with fever and manifest as petechiae or purpura 39. However, there are notable exceptions, such as Lyme disease, which is not petechial, and drug eruptions, which may not be associated with systemic symptoms. Don’t-miss skin rashes can usually be ruled out on the basis of clinical features and demographics, but sometimes further testing is indicated. Some patients should be treated immediately, before a diagnosis can be established. For example, toxic-appearing children and adults with petechiae should be treated immediately for presumed meningococcemia, before undergoing any further evaluation 40. Patients from Oklahoma, Tennessee, Arkansas, or the southern Atlantic states who present in the spring or summer with fever, myalgia, and headache—with or without a rash—should be strongly considered for antibiotic treatment of Rocky Mountain spotted fever while awaiting the results of serology or skin biopsy 41. If the physician cannot distinguish between meningococcemia and Rocky Mountain spotted fever on clinical grounds (a common occurrence), patients should be treated for both before undergoing diagnostic tests 42.
Baby skin rash
Skin rashes are extremely common in newborns and can be a significant source of parental concern. A baby’s skin may exhibit a variety of changes during the first four weeks of life. Most of these changes are benign and self-limited, but others require further work-up for infectious causes or underlying systemic disorders. Nearly all of these skin changes are concerning to parents and may result in visits to the physician or questions during routine newborn examinations.
Transient Vascular Phenomena
Newborn vascular physiology is responsible for two types of transient skin color changes: cutis marmorata and harlequin color change. These transient vascular phenomena represent normal newborn physiology rather than actual skin rashes, but they often cause parental concern.
Cutis Marmorata
Cutis marmorata is a reticulated mottling of the skin that symmetrically involves the trunk and extremities (Figure 1). I t is caused by a vascular response to cold and generally resolves when the skin is warmed. A tendency to cutis marmorata may persist for several weeks or months, or sometimes into early childhood.2No treatment is indicated.
Figure 1. Cutis marmorata, a normal reticulated mottling of the skin caused by vascular response to cold.
Harlequin color change
Harlequin color change occurs when the newborn lies on his or her side. It consists of erythema (redness) of the dependent side of the body with simultaneous blanching of the contralateral side. The color change develops suddenly and persists for 30 seconds to 20 minutes. It resolves with increased muscle activity or crying. This phenomenon affects up to 10 percent of full-term infants, but it often goes unnoticed because the infant is bundled. It occurs most commonly during the second to fifth day of life and may continue for up to three weeks. Harlequin color change is thought to be caused by immaturity of the hypothalamic center that controls the dilation of peripheral blood vessels.
Erythema Toxicum Neonatorum
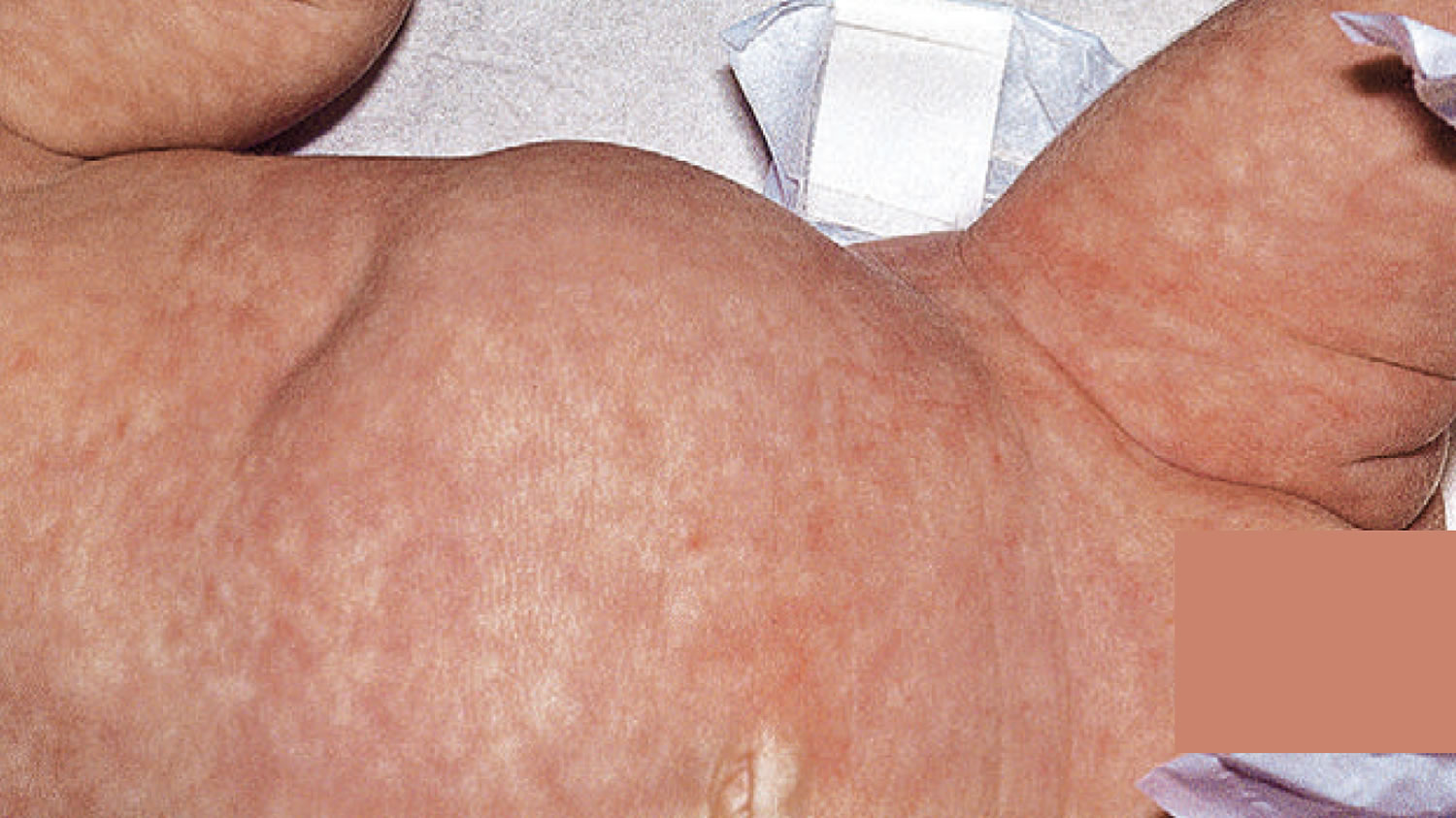
Erythema toxicum neonatorum is the most common pustular eruption in newborns. Estimates of incidence vary between 40 and 70 percent 43. It is most common in infants born at term and weighing more than 2,500 g (5.5 lb) 44. Erythema toxicum neonatorum may be present at birth but more often appears during the second or third day of life. Typical lesions consist of erythematous, 2- to 3-mm macules and papules that evolve into pustules (Figure 2) 45. Each pustule is surrounded by a blotchy area of erythema, leading to what is classically described as a “flea-bitten” appearance. Lesions usually occur on the face, trunk, and proximal extremities. Palms and soles are not involved.
The cause of erythema toxicum neonatorum is not known 46. Lesions generally fade over five to seven days, but they may recur for several weeks. No treatment is needed, and the condition is not associated with any systemic abnormality 46.
Figure 2. Erythema toxicum neonatorum

Several infections (e.g., herpes simplex, Candida, and Staphylococcus infections) also may present with vesicopustular rashes in the neonatal period (Table 9) 45, 47; infants who appear sick or who have an atypical rash should be tested for these infections 48. In healthy infants, the diagnosis of erythema toxicum neonatorum is made clinically and can be confirmed by cytologic examination of a pustular smear, which will show eosinophilia with Gram, Wright, or Giemsa staining. Peripheral eosinophilia may also be present 47.
Table 9. Infectious Causes of Vesicles or Pustules in the Newborn
| Class | Cause | Distinguishing features |
|---|---|---|
Bacterial | Group A or B Streptococcus Listeria monocytogenes Pseudomonas aeruginosa Staphylococcus aureus Other gram-negative organisms | Other signs of sepsis usually present Elevated band count, positive blood culture; Gram stain of intralesional contents shows polymorphic neutrophils |
Fungal | Candida | Presents within 24 hours after birth if congenital, after one week if acquired during delivery Thrush is common Potassium hydroxide preparation of intralesional contents shows pseudohyphae and spores |
Spirochetal | Syphilis | Rare Lesions on palms and soles Suspect if results of maternal rapid plasma reagin or venereal disease research laboratory test positive or unknown |
Viral | Cytomegalovirus Herpes simplex Varicella zoster | Crops of vesicles and pustules appear on erythematous base For herpes simplex and varicella zoster, Tzanck test of intralesional contents shows multinucleated giant cells |
[Source 46]
Transient Neonatal Pustular Melanosis
Transient neonatal pustular melanosis is a vesiculopustular rash that occurs in 5 percent of black newborns, but in less than 1 percent of white newborns 49. In contrast with erythema toxicum neonatorum, the lesions of transient neonatal pustular melanosis lack surrounding erythema (Figure 3). In addition, these lesions rupture easily, leaving a collarette of scale and a pigmented macule that fades over three to four weeks. All areas of the body may be affected, including palms and soles.
Clinical recognition of transient neonatal pustular melanosis can help physicians avoid unnecessary diagnostic testing and treatment for infectious etiologies. The pigmented macules within the vesicopustules are unique to this condition; these macules do not occur in any of the infectious rashes 49. Gram, Wright, or Giemsa staining of the pustular contents will show polymorphic neutrophils and, occasionally, eosinophils.
Figure 3. Transient neonatal pustular melanosis

Note: A baby with numerous discrete tiny pustules with hyperpigmented background, distributed over forehead, limbs, and trunk
Acne Neonatorum
Acne neonatorum occurs in up to 20 percent of newborns10 (Figure 4). It typically consists of closed comedones on the forehead, nose, and cheeks, although other locations are possible. Open comedones, inflammatory papules, and pustules can also develop.
Neonatal acne is thought to result from stimulation of sebaceous glands by maternal or infant androgens. Parents should be counseled that lesions usually resolve spontaneously within four months without scarring. Treatment generally is not indicated, but infants can be treated with a 2.5% benzoyl peroxide lotion if lesions are extensive and persist for several months 47. Parents should apply a small amount of benzoyl peroxide to the antecubital fossa to test for local reaction before widespread or facial application. Severe, unrelenting neonatal acne accompanied by other signs of hyperandrogenism should prompt an investigation for adrenal cortical hyperplasia, virilizing tumors, or underlying endocrinopathies 50.
Figure 4. Acne neonatorum

Milia
Milia are 1- to 2-mm pearly white or yellow papules caused by retention of keratin within the dermis. They occur in up to 50 percent of newborns 51. Milia occur most often on the forehead, cheeks, nose, and chin, but they may also occur on the upper trunk, limbs, penis, or mucous membranes. Milia disappear spontaneously, usually within the first month of life, although they may persist into the second or third month 51. Milia are a common source of parental concern, and simple reassurance about their benign, self-limited course is appropriate.
Figure 5. Milia

Miliaria
Miliaria results from sweat retention caused by partial closure of eccrine structures. Both milia and miliaria result from immaturity of skin structures, but they are clinically distinct entities. Miliaria affects up to 40 percent of infants and usually appears during the first month of life 52. Several clinically distinguishable subtypes exist; miliaria crystallina and miliaria rubra are the most common.
Miliaria crystallina is caused by superficial eccrine duct closure. It consists of 1- to 2-mm vesicles without surrounding erythema, most commonly on the head, neck, and trunk (Figure 6). Each vesicle evolves, with rupture followed by desquamation, and may persist for hours to days.
Figure 6. Miliaria crystallina

Miliaria rubra, also known as heat rash, is caused by a deeper level of sweat gland obstruction (Figure 7). Its lesions are small erythematous papules and vesicles, usually occurring on covered portions of the skin. Miliaria crystallina and miliaria rubra are benign. Avoidance of overheating, removal of excess clothing, cooling baths, and air conditioning are recommended for management and prevention of these disorders 45.
Figure 7. Miliaria rubra (heat rash)

Seborrheic Dermatitis
Seborrheic dermatitis is an extremely common rash characterized by erythema and greasy scales (Figures 8). Many parents know this rash as “cradle cap” because it occurs most commonly on the scalp. Other affected areas may include the face, ears, and neck. Erythema tends to predominate in the flexural folds and intertriginous areas, whereas scaling predominates on the scalp 53. Because seborrheic dermatitis often spreads to the diaper area, it is important to consider in the evaluation of diaper dermatitis 54.
Seborrheic dermatitis can be difficult to clinically distinguish from atopic dermatitis, but age at onset and the presence or absence of pruritus can be helpful (Table 10) 54. Psoriasis also has a clinical appearance similar to that of seborrheic dermatitis, but it is less common.
The exact etiology of seborrheic dermatitis is unknown. Some studies have implicated the yeast Malassezia furfur (previously known as Pityrosporum ovale) 55. Hormonal fluctuations may also be involved, which would explain why seborrheic dermatitis occurs most often in areas with a high density of sebaceous glands. Generalized seborrheic dermatitis accompanied by failure to thrive and diarrhea should prompt an evaluation for immunodeficiency 53.
Infantile seborrheic dermatitis is usually self-limited, resolving within several weeks to several months. In one prospective study, children with infantile seborrheic dermatitis were reexamined 10 years later 56. Overall, 85 percent of children were free of skin disease at follow-up. Seborrheic dermatitis persisted in 8 percent of children, but the link between infantile and adult seborrheic dermatitis remains unclear. In addition, 6 percent of children in this study later were diagnosed with atopic dermatitis, illustrating the difficulty in distinguishing these conditions during infancy.
Given the benign, self-limited nature of seborrheic dermatitis in infants, a conservative stepwise approach to treatment is warranted. Physicians should begin with reassurance and watchful waiting. If cosmesis is a concern, scales can often be removed with a soft brush after shampooing. An emollient, such as white petrolatum, may help soften the scales. Soaking the scalp overnight with vegetable oil and then shampooing in the morning is also effective.
If seborrheic dermatitis persists despite a period of watchful waiting, several treatment options exist (Table 11). Tar-containing shampoos can be recommended as first-line treatment 53. Selenium sulfide shampoos are probably safe, but rigorous safety data in infants is lacking. The use of salicylic acid is not recommended because of concerns about systemic absorption 53.
Evidence from small randomized controlled trials supports the use of topical antifungal creams or shampoos if treatment with tar-containing shampoo fails 57. Mild steroid creams are another commonly prescribed option. One meta-analysis found that topical ketoconazole (Nizoral, brand no longer available in the United States) and steroid creams are effective in the treatment of infantile seborrheic dermatitis, but ketoconazole may be better at preventing recurrences 57.
Figure 8. Seborrheic dermatitis

Table 10. Distinguishing Features of Seborrheic and Atopic Dermatitis in Infancy
| Feature | Seborrheic dermatitis | Atopic dermatitis |
|---|---|---|
Age at onset | Usually within first month | After three months of age |
Course | Self-limited, responds to treatment | Responds to treatment, but frequently relapses |
Distribution | Scalp, face, ears, neck, diaper area | Scalp, face, trunk, extremities, diaper area |
Pruritus (itchy skin) | Uncommon | Ubiquitous |
Table 11. Treatment Options for Infantile Seborrheic Dermatitis
| Medication | Directions | Notes |
|---|---|---|
White petrolatum | Apply daily | May soften scales, facilitating removal with soft brush |
Tar-containing shampoo | Use several times per week | Use when baby shampoo has failed Safe, but potentially irritating |
Ketoconazole (Nizoral, brand no longer available in the United States), 2% cream or 2% shampoo | Cream: apply to scalp three times weekly Shampoo: lather, leave on for three minutes, then rinse. Use three times weekly | Small trial showed no systemic drug levels or change in liver function after one month of use |
Hydrocortisone 1% cream | Apply every other day or daily | Limit surface area to reduce risk of systemic absorption and adrenal suppression |
May be especially effective for rash in flexural areas |
- Pariser RJ, Pariser DM. Primary care physicians’ errors in handling cutaneous disorders. A prospective survey. J Am Acad Dermatol. 1987;17(2 pt 1):239–245.[↩][↩]
- Norman GR, Rosenthal D, Brooks LR, Allen SW, Muzzin LJ. The development of expertise in dermatology. Arch Dermatol. 1989;125(8):1063–1068.[↩]
- Williams HC. Clinical practice. Atopic dermatitis. N Engl J Med. 2005;352(22):2314–2324.[↩]
- Zug KA, McGinley-Smith D, Warshaw EM, et al. Contact allergy in children referred for patch testing: North American Contact Dermatitis Group data, 2001–2004. Arch Dermatol. 2008;144(10):1329–1336.[↩]
- Bigby M. Rates of cutaneous reactions to drugs. Arch Dermatol. 2001;137(6):765–770.[↩]
- Brönnimann M, Yawalkar N. Histopathology of drug-induced exanthems: is there a role in diagnosis of drug allergy? Curr Opin Allergy Clin Immunol. 2005;5(4):317–321.[↩]
- Côté B, Wechsler J, Bastuji-Garin S, Assier H, Revuz J, Roujeau JC. Clini-copathologic correlation in erythema multiforme and Stevens-Johnson syndrome. Arch Dermatol. 1995;131(11):1268–1272.[↩]
- Telfer NR, Chalmers RJ, Whale K, Colman G. The role of streptococcal infection in the initiation of guttate psoriasis. Arch Dermatol. 1992;128(1):39–42.[↩]
- Marqueling AL, Gilliam AE, Prendiville J, et al. Keratosis pilaris rubra: a common but underrecognized condition. Arch Dermatol. 2006;142(12):1611–1616.[↩]
- Eisen D. The vulvovaginal-gingival syndrome of lichen planus. The clinical characteristics of 22 patients. Arch Dermatol. 1994;130(11):1379–1382.[↩]
- Tay YK, Goh CL. One-year review of pityriasis rosea at the National Skin Centre, Singapore. Ann Acad Med Singapore. 1999;28(6):829–831.[↩]
- Griffiths CE, Barker JN. Pathogenesis and clinical features of psoriasis. Lancet. 2007;370(9583):263–271.[↩]
- Boyd AS, Neldner KH. Lichen planus. J Am Acad Dermatol. 1991;25(4):593–619.[↩][↩]
- Asano Y, Yoshikawa T, Suga S, et al. Clinical features of infants with primary human herpesvirus 6 infection (exanthem subitum, roseola infantum). Pediatrics. 1994;93(1):104–108.[↩]
- Ziemer M, Seyfarth F, Elsner P, Hipler UC. Atypical manifestations of tinea corporis. Mycoses. 2007;50(suppl 2):31–35.[↩]
- Schmutzhard J, Merete Riedel H, Zweygberg Wirgart B, Grillner L. Detection of herpes simplex virus type 1, herpes simplex virus type 2 and varicella-zoster virus in skin lesions. Comparison of real-time PCR, nested PCR and virus isolation. J Clin Virol. 2004;29(2):120–126.[↩]
- Drago F, Rampini E, Rebora A. Atypical exanthems: morphology and laboratory investigations may lead to an aetiological diagnosis in about 70% of cases. Br J Dermatol. 2002;147(2):255–260.[↩][↩][↩]
- Joly P, Courville P, Lok C, et al., for the French Bullous Study Group. Clinical criteria for the diagnosis of bullous pemphigoid: a reevaluation according to immunoblot analysis of patient sera. Dermatology. 2004;208(1):16–20.[↩]
- George DE, Browning JC, Hsu S. Medical pearl: dermatitis herpeti-formis—potential for confusion with eczema. J Am Acad Dermatol. 2006;54(2):327–328.[↩]
- Lapins J, Lindbäck S, Lidbrink P, Biberfeld P, Emtestam L, Gaines H. Mucocutaneous manifestations in 22 consecutive cases of primary HIV-1 infection. Br J Dermatol. 1996;134(2):257–261.[↩]
- Perlmutter BL, Glaser JB, Oyugi SO. How to recognize and treat acute HIV syndrome [published correction appears in Am Fam Physician. 2000;61(2):308] Am Fam Physician. 1999;60(2):535–542.[↩]
- Newburger JW, Takahashi M, Gerber MA, et al., for the Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease, Council on Cardiovascular Disease in the Young, American Heart Association. Diagnosis, treatment, and long-term management of Kawasaki disease [published correction appears in Pediatrics. 2005;115(4):1118]. Pediatrics. 2004;114(6):1708–1733.[↩]
- Habif TP. Clinical Dermatology. 5th ed. New York, NY: Mosby; 2010:684.[↩]
- Centers for Disease Control and Prevention. Reported cases of lyme disease. United States, 2008. http://www.cdc.gov/ncidod/dvbid/lyme/ld_Incidence.htm[↩]
- Drage LA. Life-threatening rashes: dermatologic signs of four infectious diseases. Mayo Clin Proc. 1999;74(1):68–72.[↩][↩][↩]
- Zackheim HS, McCalmont TH. Mycosis fungoides: the great imitator. J Am Acad Dermatol. 2002;47(6):914–918.[↩]
- Walker DH, Burday MS, Folds JD. Laboratory diagnosis of Rocky Mountain spotted fever South Med J. 1980;73(11):1443–14461449.[↩]
- O’Connell NH, Mannix M, Philip RK, et al. Infant staphylococcal scalded skin syndrome, Ireland, 2007—preliminary outbreak report. Euro Surveill. 2007;12(24):pii=3220. http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=3220[↩]
- Rzany B, Hering O, Mockenhaupt M, et al. Histopathological and epidemiological characteristics of patients with erythema exudativum multiforme major, Stevens-Johnson syndrome and toxic epidermal necrolysis. Br J Dermatol. 1996;135(1):6–11.[↩]
- Kemmett D, Hunter JA. Sweet’s syndrome: a clinicopathologic review of twenty-nine cases. J Am Acad Dermatol. 1990;23(3 pt 1):503–507.[↩]
- Comer JA, Tzianabos T, Flynn C, Vlahov D, Childs JE. Serologic evidence of rickettsialpox (Rickettsia akari) infection among intravenous drug users in inner-city Baltimore, Maryland. Am J Trop Med Hyg. 1999;60(6):894–898.[↩]
- Aber C, Alvarez Connelly E, Schachner LA. Fever and rash in a child: when to worry? Pediatr Ann. 2007;36(1):30–38.[↩][↩]
- Pimpinelli N, Olsen EA, Santucci M, et al., for the International Society for Cutaneous Lymphoma. Defining early mycosis fungoides. J Am Acad Dermatol. 2005;53(6):1053–1063.[↩]
- The Generalized Rash: Part II. Diagnostic Approach. Am Fam Physician. 2010 Mar 15;81(6):735-739. http://www.aafp.org/afp/2010/0315/p735.html[↩][↩][↩][↩]
- Boyd AS, Neldner KH. The isomorphic response of Koebner. Int J Dermatol. 1990;29(6):401–410.[↩]
- O’Connell NH, Mannix M, Philip RK, et al. Infant staphylococcal scalded skin syndrome, Ireland, 2007—preliminary outbreak report. Euro Surveill. 2007;12(24): pii=3220. http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=3220[↩]
- Bernhard JD. Auspitz sign is not sensitive or specific for psoriasis. J Am Acad Dermatol. 1990;22(6 pt 1):1079–1081.[↩]
- Eichenfield LF, Hanifin JM, Luger TA, Stevens SR, Pride HB. Consensus conference on pediatric atopic dermatitis. J Am Acad Dermatol. 2003;49(6):1088–1095.[↩]
- Schlossberg D. Fever and rash. Infect Dis Clin North Am. 1996;10(1):101–110.[↩]
- Tunkel AR, Hartman BJ, Kaplan SL, et al. Practice guidelines for the management of bacterial meningitis. Clin Infect Dis. 2004;39(9):1267–1284.[↩]
- Chapman AS, Bakken JS, Folk SM, et al., for the Tickborne Rickettsial Diseases Working Group, CDC. Diagnosis and management of tickborne rickettsial diseases: Rocky Mountain spotted fever, ehrlichioses, and anaplasmosis—United States. MMWR Recomm Rep. 2006;55(RR-4):1–27.[↩]
- Centers for Disease Control and Prevention. Consequences of delayed diagnosis of Rocky Mountain spotted fever in children—West Virginia, Michigan, Tennessee, and Oklahoma, May–July 2000. MMWR Morb Mortal Wkly Rep. 2000;49(39):885–888.[↩]
- Liu C, Feng J, Qu R, et al. Epidemiologic study of the predisposing factors in erythema toxicum neonatorum. Dermatology. 2005;210(4):269–272.[↩]
- Carr JA, Hodgman JE, Freedman RI, Levan NE. Relationship between toxic erythema and infant maturity. Am J Dis Child. 1966;112(2):129–134.[↩]
- Schachner L, Press S. Vesicular, bullous and pustular disorders in infancy and childhood. Pediatr Clin North Am. 1983;30(4):609–629.[↩][↩][↩]
- Newborn Skin: Part I. Common Rashes. Am Fam Physician. 2008 Jan 1;77(1):47-52. http://www.aafp.org/afp/2008/0101/p47.html[↩][↩][↩][↩][↩]
- Van Praag MC, Van Rooij RW, Folkers E, Spritzer R, Menke HE, Oranje AP. Diagnosis and treatment of pustular disorders in the neonate. Pediatr Dermatol. 1997;14(2):131–143.[↩][↩][↩]
- Chang MW, Jiang SB, Orlow SJ. Atypical erythema toxicum neonatorum of delayed onset in a term infant. Pediatr Dermatol. 1999;16(2):137–141.[↩]
- Laude TA. Approach to dermatologic disorders in black children. Semin Dermatol. 1995;14(1):15–20.[↩][↩]
- Katsambas AD, Katoulis AC, Stavropoulos P. Acne neonatorum: a study of 22 cases. Int J Dermatol. 1999;38(2):128–130.[↩]
- Paller A, Mancini AJ, Hurwitz S. Hurwitz Clinical Pediatric Dermatology: A Textbook of Skin Disorders of Childhood and Adolescence. 3rd ed. Philadelphia, Pa.: Elsevier Saunders, 2006:737.[↩][↩]
- Feng E, Janniger CK. Miliaria. Cutis. 1995;55(4):213–216.[↩]
- Janniger CK. Infantile seborrheic dermatitis: an approach to cradle cap. Cutis. 1993;51(4):233–235.[↩][↩][↩][↩]
- Williams ML. Differential diagnosis of seborrheic dermatitis. Pediatr Rev. 1986;7(7):204–211.[↩][↩]
- Tollesson A, Frithz A, Stenlund K. Malassezia furfur in infantile seborrheic dermatitis. Pediatr Dermatol. 1997;14(6):423–425.[↩]
- Mimouni K, Mukamel M, Zeharia A, Mimouni M. Prognosis of infantile seborrheic dermatitis. J Pediatr. 1995;127(5):744–746.[↩]
- Taieb A, Legrain V, Palmier C, Lejean S, Six M, Maleville J. Topical ketoconazole for infantile seborrhoeic dermatitis. Dermatologica. 1990;181(1):26–32.[↩][↩]





{kind=link}