
Contents
What is trachoma
Trachoma is an eye infection caused by the bacterium Chlamydia trachomatis. If not treated, trachoma infection can cause eyelids to turn inwards, so that eyelashes scrape against a person’s eye with each blink and permanently scar the cornea. This condition is called trichiasis, and without immediate, corrective surgery, a person with trichiasis will slowly and painfully become blind. Repeated trachoma infections can cause blindness. Five hundred forty million people are at risk in 55 countries, and 84 million are already infected 1). The World Health Organization (WHO) reports trachoma is endemic to more than 50 countries, with most blinding trachoma in Africa. An estimated 21 million people are living with active trachoma and another 2.2 million people are blind or severely visually impaired. Furthermore, 7.3 million people suffer from trichiasis and are at risk for developing blindness.
Blindness from trachoma is due to recurrent episodes of active infection. The initial infection is confined to the conjunctival epithelium and triggers an immune response. Repeat infections with subsequent inflammatory responses results in tissue destruction, scarring, cicatricial entropion with trichiasis, and corneal opacification from lashes rubbing against the cornea.
Epidemiologic studies have shown active trachoma is most common in young children with the prevalence of active trachoma decreasing with age. Trachoma is particularly common in children who are less than five years of age and in the adults – mainly women – who care for them. In some rural communities, 60 – 90 percent of children are infected. The long-term sequelae of trachoma infection, including scarring, trichiasis and corneal opacification in adults relates to their exposure to active trachoma when they were young. The gender distrubtion of active trachoma is similar; however, scarring and trichiasis are more common in women than men because women are more likely to care for young children and have longer exposure to the trachoma eye disease.
Trachoma spreads quickly through close personal contact and often is more common in areas where people live close together. Often, whole communities can be affected. For these reasons, trachoma infections are often common in the poorest communities.
Trachoma Grading and Clinical Features
The World Health Organization (WHO) grading system 2):
| Trachomatous Follicular Inflammation (TF) | The presence of 5 or more follicles (>0.5 mm) in the upper tarsal conjunctiva |
| Trachomatous Intense Inflammation (TI) | Inflammatory thickening of the tarsal conjunctiva that obscures more than half of the deep normal vessels |
| Trachomatous Scarring (TS) | The presence of scarring in the tarsal conjunctiva |
| Trachomatous Trichiasis (TT) | At least one lash rubs on the eyeball |
| Corneal Opacity | Easily visible corneal opacity over the pupil |
The clinical manifestations of trachoma can be divided into findings associated with active trachoma eye disease and those associated with repeat infections.
Active Trachoma Eye Disease:
- Follicular Conjunctivitis: Follicles are dome-shaped collections of lympoid cells. The center of the follicle is avascular and has blood vessels that surround the round base. These appear as yellow-white elevations and are prominent on the everted upper eyelid in trachoma. Large conjunctival follicles located at the upper margin of the cornea may leave depressions known as ‘Herbert’s pits’ which are pathognomonic for trachoma.
- Papillary Hypertrophy: engorgement of small vessels with edema that can obscure deep tarsal vessels
- Corneal Pannus: vascularization of the upper cornea.
Repeat Infection and Inflammation:
- Conjunctival Scarring: White bands or lines that represent fibrosis
- Cicatricial Entropion and Trichiasis: Fibrotic scar tissue contraction causes the eyelid turning inward and lashes touching the eyeball.
- Corneal Opacification: secondary to repeat corneal irritation from inward turning eyelashes
Figure 1. Clinical features and grades of trachoma
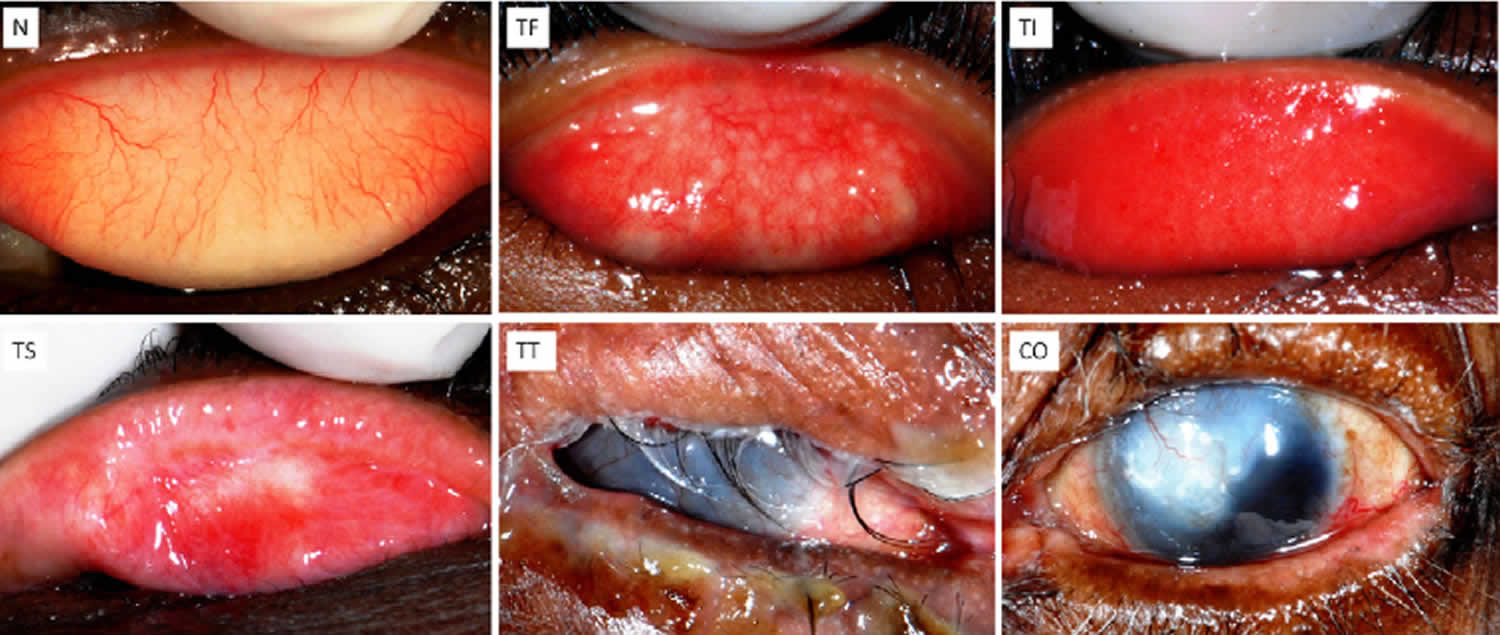
Abbreviations: N = normal; TF = Trachomatous follicular inflammation; TI = Trachomatous inflammation– intense; TS = trachomatous scarring; TT = trachomatous trichiasis; CO = corneal opacity.
[Source 3)]Figure 2. Trachomatous follicular inflammation
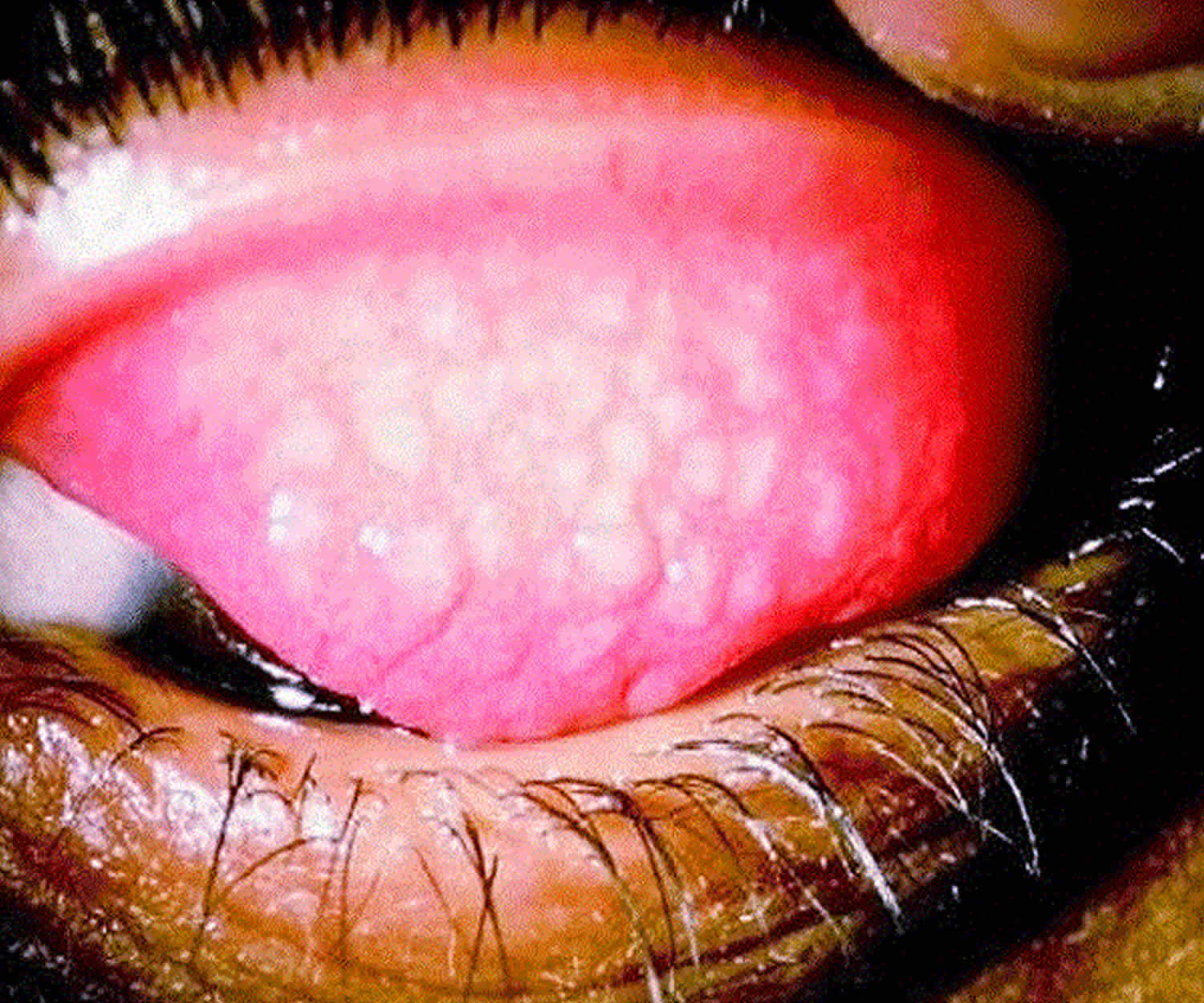
Footnote: Trachomatous follicular inflammation is 5 or more follicles in the central part of the upper tarsal conjunctiva. The follicles are round swellings that are pale compared to the rest of the conjunctiva. They must be at least 0.5 mm in diameter to be counted. If they are less than 5 follicles, then this is not trachomatous follicular inflammation and should not be graded as trachomatous follicular inflammation.
[Source 4)]Figure 3. Trachomatous intense inflammation
Footnote: Active trachoma eye disease is also seen as trachomatous intense inflammation, which stands for trachomatous inflammation intense. There is pronounced inflammatory swelling of the tarsal conjunctiva so that more than half of the deep, normal tarsal vessels are obscured by the swelling. Trachomatous follicular inflammation should also be diagnosed if 5 or more follicles are seen.
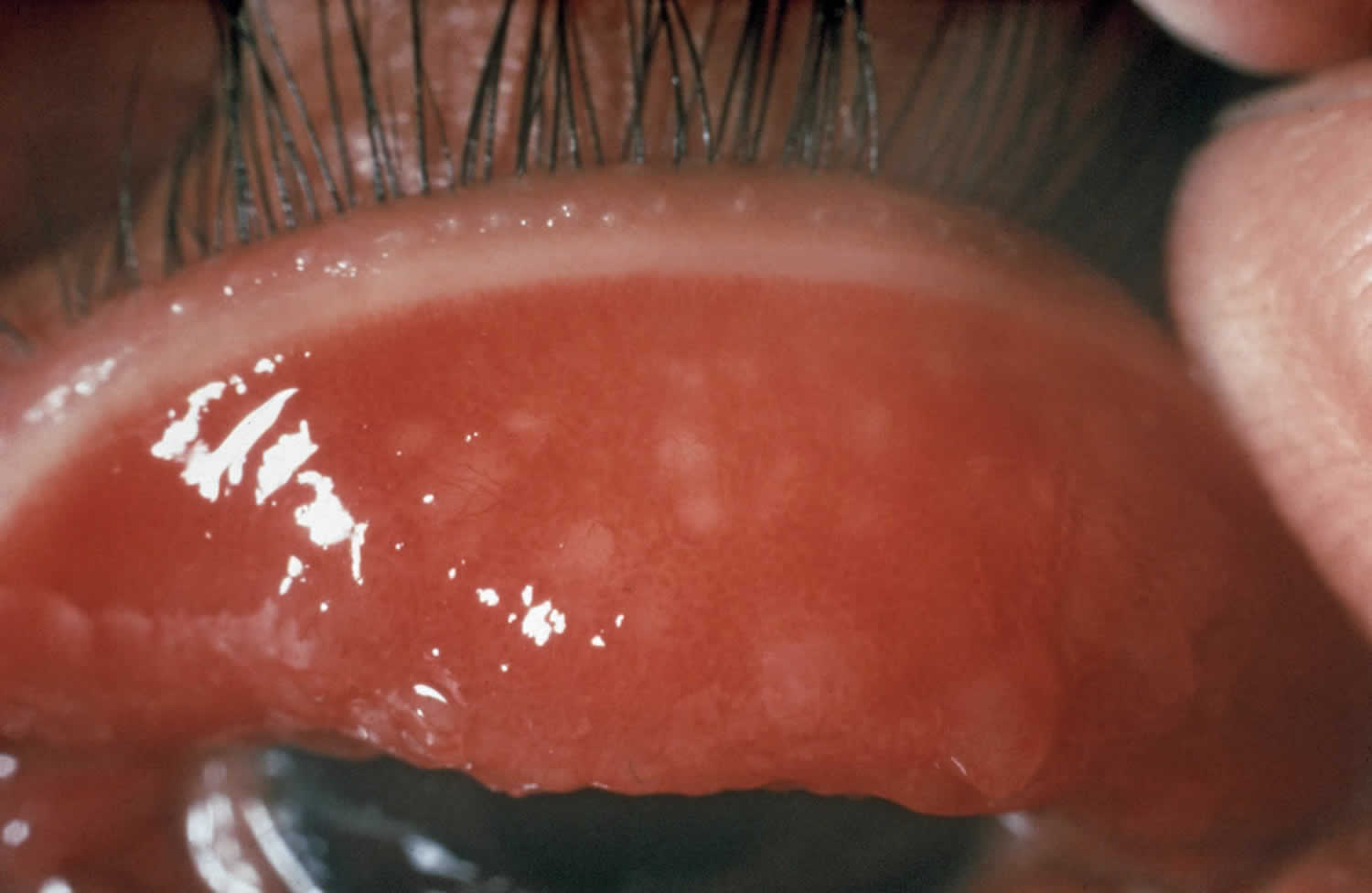
[Source 5)]Figure 4. Trachomatous conjunctival scarring

Footnote: Repeated episodes of inflammation results in trachomatous conjunctival scarring, which stands for trachoma scarring. The trachoma scarring is easily visible white lines, sheets or bands in the tarsal conjunctiva.
[Source 6)]Figure 5. Trachomatous trichiasis
Footnote: If the trachoma scarring is severe, it may result in trichiasis. At least one eyelash rubbing on the eyeball or evidence of eyelash removal.
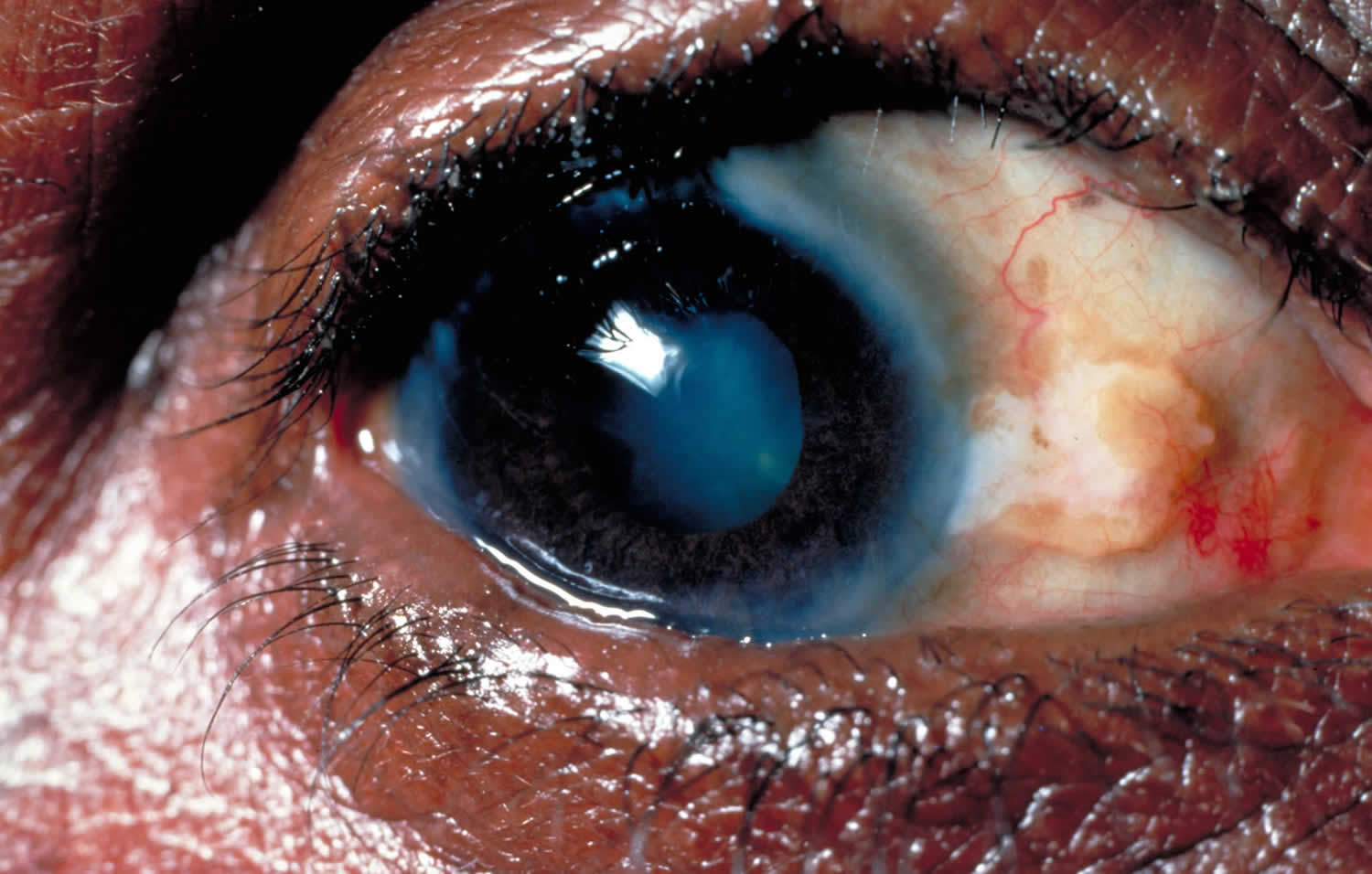
[Source 7)]Figure 6. Corneal opacity
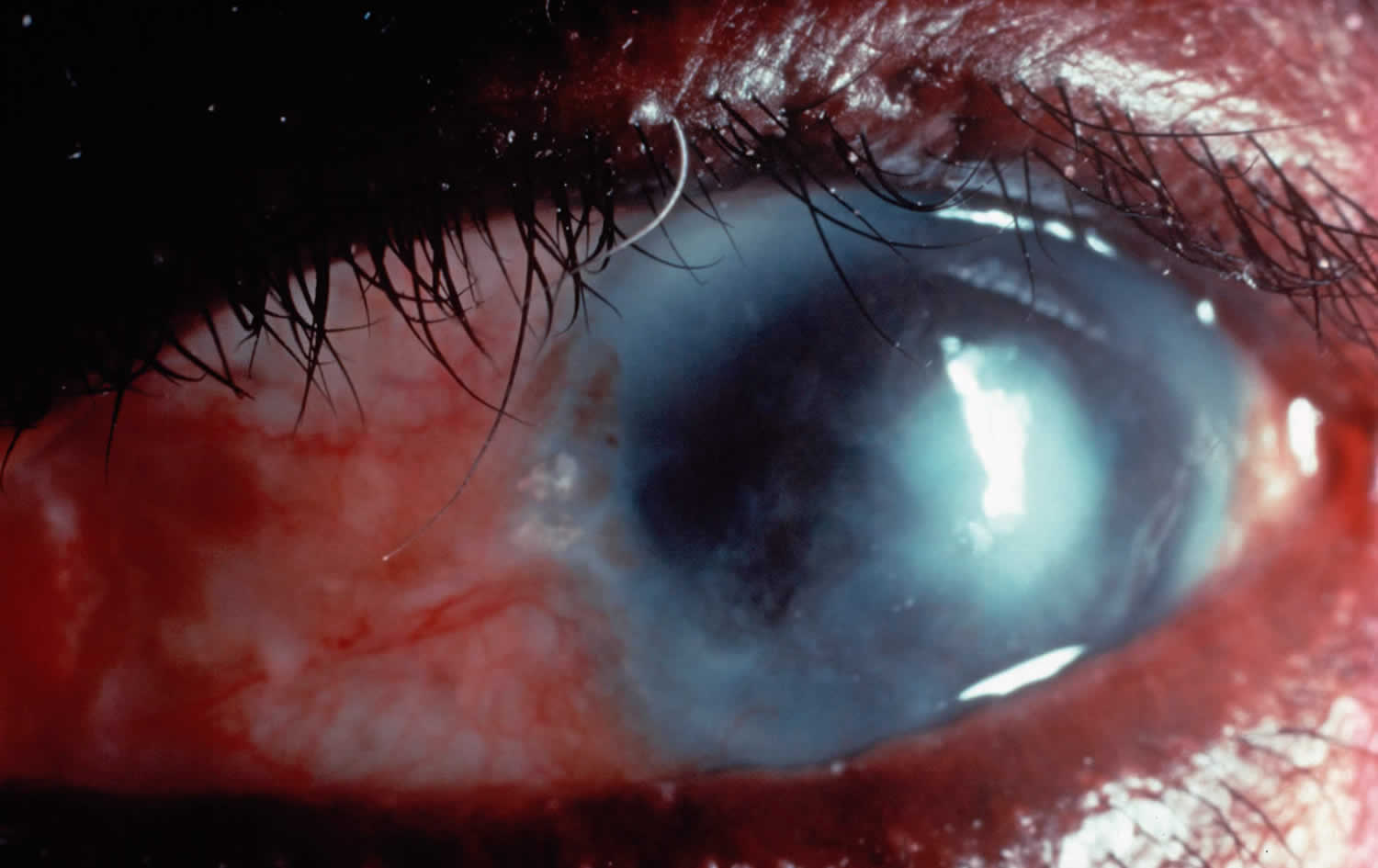
Footnote: If the trichiasis is not treated, it can cause corneal opacity and loss of vision.
[Source 8)]Trachoma eye disease complications
One episode of trachoma caused by Chlamydia trachomatis is easily treated with early detection and use of antibiotics. Repeated or secondary infections can lead to complications, including:
- Scarring of the inner eyelid
- Eyelid deformities, such as an inward folding eyelid (entropion) or ingrown eyelashes (trichiasis)
- Corneal scarring or cloudiness
- Partial or complete vision loss
Who is at risk for trachoma?
Trachoma is rare in the United States and Europe. It is commonly found in developing nations where poverty, crowded living conditions and poor sanitation help spread the trachoma eye disease. It is very contagious and is spread by direct contact with someone infected with the bacteria or with contaminated objects, such as towels.
The World Health Organization estimates that 41 million people worldwide, mostly women and children, have active trachoma infection.
Trachoma mainly exists in communities where extreme poverty has made it more difficult to improve environmental sanitation or to provide basic health education such as promoting hand and face washing.
People suffering from the advanced, blinding stage of trachoma experience severe pain and diminishing vision, preventing them from contributing to their families’ economic livelihood, or even taking care of themselves.
Women are twice as likely as men to go blind from repeated trachoma infections due to their role as traditional caretakers of children, who often are the primary hosts for the disease in their communities.
Tragically, in many cultures, a woman who cannot perform her household duties due to trachoma or another illness may be abandoned by her family, or an older daughter may be taken out of school to assume her mother’s responsibilities.
As a result, trachoma worsens an already challenging situation for communities living on the edge of survival, and decreases overall economic opportunities for women. Some estimates suggest trachoma can cost affected communities as much as US $2.9 billion per year in lost productivity.
Trachoma causes
Trachoma is caused by four ocular serotypes of Chalmydia trachomatis: A, B, Ba and C. Infection with genital serotypes D to K can cause isolated episodes of ophthalmia neonatorum in infants or inclusion conjunctivitis in adults and do not generally lead to blindness.
Chlamydia trachomatis bacteria that causes trachoma is spread through direct contact with fluid from the eyes and nose of infected people. The chlamydia trachomatis bacteria can also be on personal items such as facecloths. Flies that have been in contact with infected eyes can also carry the chlamydia trachomatis bacteria between people.
As trachoma is easily transmitted between children, the condition often starts in childhood, but anybody can get infected at any age. People who have repeated trachoma infections can go blind in their 30s.
Trachoma is more common in areas where there is:
- a lot of people living close together
- poor access to water
- poor toilet facilities
- poor hygiene
Risk factors for trachoma
Risk factors for trachoma include things that favor transmission of the organism. Examples include:
- Inadequate Water Supply: less water availabe to use for facial cleansing
- Poor Facial Hygiene: secretions around the eye attracts flies that are physical vectors for C. trachomatis tranmission
- Lack of latrines: Populations without access to working latrines — a type of communal toilet – leads to increased fecal contamination of the environment which provides a breeding environment for the fly and have a higher incidence of trachoma eye disease.
- Overcrowded Living Conditions: People living in close contact are at greater risk of spreading infection. Close contact, especially between children sleeping in same bed, enables exchange of secretions.
- Poverty. Trachoma is primarily a disease of extremely poor populations in developing countries.
- Poor sanitation. Poor sanitary conditions and lack of hygiene, such as unclean faces or hands, help spread the disease.
- Age. In areas where the disease is active, it’s most common in children ages 4 to 6.
- Sex. In some areas, women’s rate of contracting the disease is two to six times higher than that of men.
- Flies. People living in areas with problems controlling the fly population may be more susceptible to infection.
Trachoma prevention
Simple steps you can take to prevent the spread of trachoma infection. These include teaching children good hygiene (thorough face-washing and hand-washing) and making sure family members don’t share towels and facecloths.
If you’ve been treated for trachoma with antibiotics or surgery, reinfection is always a concern. For your protection and for the safety of others, be sure that family members or others you live with are screened and, if necessary, treated for trachoma.
Trachoma can occur worldwide but is more common in the Middle East, North Africa, sub-Saharan Africa, and areas of southern Asia and China. When in regions where trachoma is common, take extra care in practicing good hygiene, which can help prevent infection.
Proper hygiene practices include:
- Face washing and hand-washing. Keeping faces clean may help break the cycle of reinfection.
- Controlling flies. Reducing fly populations can help eliminate a major source of transmission.
- Proper waste management. Properly disposing of animal and human waste can reduce breeding grounds for flies.
- Improved access to water. Having a fresh water source nearby can help improve hygienic conditions.
No trachoma vaccine is available, but prevention is possible. The World Health Organization (WHO) has developed a strategy to prevent trachoma, with the goal of eliminating it by 2020. The strategy, titled SAFE, involves:
- Surgery to treat advanced forms of trachoma
- Antibiotics to treat and prevent the infection
- Facial cleanliness
- Environmental improvements, particularly in water, sanitation and fly control
Trachoma symptoms
Most individuals are asymptomatic or have mild symptoms depending on the level of inflammation. Symptoms, if present, are similar to those seen in any chronic conjunctivitis and include redness, discomfort, tearing, photophobia and muco-purulent discharge.
Infected eyes might feel sticky, itchy, or be painful and there might be a discharge from the nose. In later stages a person might feel as if they have sand in their eyes.
In its early stages, trachoma causes conjunctivitis (pink eye). Early symptoms, which begin to appear within five to 12 days of exposure to the bacterium, can include mild itching and irritation of the eyes and eyelids and a discharge from the eyes. As the infection progresses, it causes eye pain and blurred vision. If the infection is untreated, scarring occurs inside the eyelid. This leads to the eyelashes turning inward toward the eye, a condition called trichiasis. The eyelashes brush and scratch against the cornea, the clear covering at the front of the eye. This continual irritation turns the cornea cloudy and can lead to the development of corneal ulcers and vision loss.
Having one episode of trachoma rarely causes problems. It is thought that experiencing repeated infections is what leads to the scarring and blinding complications. Generally, it takes years before trachoma can cause vision loss.
Trachoma diagnosis
Health practitioners can diagnose trachoma using magnifiers and a flashlight. Trachoma is a clinical diagnosis based on the above mentioned clinical findings. They might also take photographs of the eyes.
PCR testing developed for urogenital infection is available but typically utilized for research purposes only.
Trachoma treatment
The World Health Organization recommends the ‘SAFE’ strategy for the management of trachoma. This strategy was developed in 1997 by The Alliance for the Global Elimination of Blinding Trachoma by the year 2020 and utilizes a 4 step approach 9):
- S: Surgery for Trichiasis – eyelid surgery corrects in-turning of eyelashes
- A: Antibiotics for Chlamydia trachomatis infection
- F: Facial cleanliness – to stop infection spreading to others, and reduce re-infection
- E: Environmental change to improve sanitation and increase access to clean water for households and communities.
Antibiotics. In the early stages of trachoma, treatment with antibiotics alone may be enough to eliminate the infection. Your doctor may prescribe tetracycline eye ointment or oral azithromycin (Zithromax). Azithromycin appears to be more effective than tetracycline, but it’s more expensive.
The World Health Organization (WHO) recommends giving antibiotics to an entire community when more than 10 percent of children have been affected by trachoma. The goal of this guideline is to treat anyone who has been exposed to trachoma and reduce the spread of trachoma.
More advanced cases of trachoma may require surgery to reposition eyelashes that are growing inward toward the eye. This surgery can help limit further scarring of the cornea and may help improve eyesight. Corneal transplants are another surgical option if the cornea has become so clouded that vision is seriously impaired.
Surgery
Treatment of later stages of trachoma — including painful eyelid deformities — may require surgery. WHO guidelines recommend surgery for people with the advanced stage of trachoma.
In eyelid rotation surgery (bilamellar tarsal rotation), your doctor makes an incision in your scarred lid and rotates your eyelashes away from your cornea. The procedure limits the progression of corneal scarring and may help prevent further loss of vision.
If your cornea has become clouded enough to seriously impair your vision, corneal transplantation may be an option that may improve vision. Frequently, however, with trachoma, this procedure doesn’t have good results.
You may have a procedure to remove eyelashes (epilation) in some cases. This procedure may need to be done repeatedly. Another temporary option, if surgery isn’t an available option, is to place an adhesive bandage over your eyelashes to keep them from touching your eye.
Good hygiene, such as hand washing and face washing, has been shown to decrease the spread of trachoma.
The “F” in the SAFE strategy refers to facial cleanliness. Because trachoma is transmitted through close personal contact, it tends to occur in clusters, often infecting entire families and communities. Children, who are more likely to touch their eyes and have unclean faces that attract eye-seeking flies, are especially vulnerable to infection, as are women 10), the traditional caretakers of the home. Therefore, the promotion of good hygiene practices, such as hand washing and the washing of children’s faces at least once a day with water, is a key step in breaking the cycle of trachoma transmission 11).
The “E” in the SAFE strategy refers to environmental change. Improvements in community and household sanitation, such as the provision of household latrines, help control fly populations and breeding grounds. Increased access to water facilitates good hygiene practices and is vital to achieving sustainable elimination of the disease 12). Separation of animal quarters from human living space, as well as safe handling of food and drinking water, are also important environmental measures that affected communities can take within a trachoma control program.
References [ + ]





{kind=link}