Contents
- What is tubal ligation
- How tubal ligation works
- Advantages and disadvantages of tubal ligation
- Noncontraceptive Benefits of Tubal Ligation
- Does tubal ligation protect against sexually transmitted infections (STIs)?
- Will tubal ligation affect my sex life?
- Will my periods be the same after tubal ligation?
- What if I decide I want to get pregnant after I had tubal ligation?
- What are the alternatives to tubal ligation?
- Tubal ligation failure
- What is fallopian tube
- Tubal ligation procedure
- Pregnancy after tubal ligation
- Tubal ligation side effects
- Tubal ligation reversal
- Vasectomy vs Tubal ligation
What is tubal ligation
Tubal ligation also known as getting your “tubes tied” or “tubal sterilization”, is a type of surgery where the fallopian tubes are clipped, cut and tied or sealed shut. This blocks the path between the ovaries and the uterus. The sperm cannot reach the egg to fertilize it, and the egg cannot reach the uterus. Tubal ligation prevents a woman from getting pregnant. Tubal ligation is a permanent form of birth control, and is effective right away. This means that it protects against pregnancy forever. Only adult women who do not want any children, or do not want any more, or cannot carry a pregnancy because of a medical condition should use tubal ligation as a method of contraception. With tubal ligation, very tiny cuts (called incisions) are made in your abdomen or belly. Tubal ligation prevents pregnancy immediately.
Also known as laparoscopic sterilization, tubal ligation is very effective. Fewer than 1 woman in every 100 who has a tubal ligation will become pregnant later.
You get the tubal ligation surgery in a hospital or outpatient surgical center. Tubal ligation usually takes about 30 minutes. Almost all women go home the same day. They can return to most normal activities within a few days.
Tubal ligation can be done:
- Following a vaginal birth using a small incision under the belly button (mini-laparotomy)
- During a C-section
- Anytime as an outpatient procedure using a laparoscope and short-acting general anesthesia (interval tubal ligation)
The fallopian tubes (see Figures 1 to 3 below) is where an egg and sperm meet, and where the egg becomes fertilized before it moves to the uterus. By closing off the tubes, sperm can’t get to the egg which means that pregnancy can’t happen.
Tubal ligation isn’t right for everyone, however. Your doctor or health care provider will make sure you fully understand the risks and benefits of the procedure.
Your doctor may also talk to you about other options, including long-acting reversible contraceptives such as an intrauterine device (IUD) or a birth control device that’s implanted in your arm. An alternative permanent option is hysteroscopic sterilization, this procedure is called the “Essure”, in which your doctor places a small coil or other insert into the fallopian tubes. The insert causes scar tissue to form and seal off the tubes.
Another option for permanent birth control is male sterilization (vasectomy).
Tubal ligation key facts
- tubal ligation is more than 99% effective at preventing pregnancy
- Tubal ligation is a safe and effective form of permanent birth control. But it doesn’t work for everyone. Fewer than 1 out of 100 women will get pregnant in the first year after the procedure. The younger you are at the time it’s done, the more likely it is to fail.
- you don’t have to think about protecting yourself against pregnancy every time you have sex, so it doesn’t interrupt your sex life
- it doesn’t affect your hormone levels and you’ll still have periods
- you’ll need to use contraception up until you have the operation, and until your next period or for 3 months after the operation (depending on the type of sterilization)
- as with any surgery, there’s a small risk of complications, such as internal bleeding, infection or damage to other organs
- there’s a small risk that the tubal ligation operation won’t work – blocked tubes can rejoin immediately or years later
- if the tubal ligation operation fails, this may increase the risk of a fertilized egg implanting outside the womb (ectopic pregnancy). An ectopic pregnancy requires immediate medical treatment. The pregnancy cannot continue to birth. If you think you’re pregnant at any time after a tubal ligation, contact your health care provider immediately.
- tubal ligation is very difficult to reverse, so you need to be sure it’s right for you
- tubal ligation doesn’t protect against sexually transmitted infections, so you may need to use condoms as well
Tubal ligation risks
Tubal ligation is an operation that involves making incisions in your abdomen. It requires anesthesia. Risks associated with tubal ligation include:
- Damage to the bowel, bladder or major blood vessels
- Reaction to anesthesia
- Improper wound healing or infection
- Continued pelvic or abdominal pain
- Failure of the procedure, resulting in a future unwanted pregnancy
Things that make you more likely to have complications from tubal ligation include:
- History of pelvic or abdominal surgery
- Obesity/Overweight
- Diabetes
- Pelvic inflammatory disease
- Lung disease
You may have other risks, depending on your specific health condition. Be sure to discuss any concerns with your healthcare provider before the procedure.
How tubal ligation works
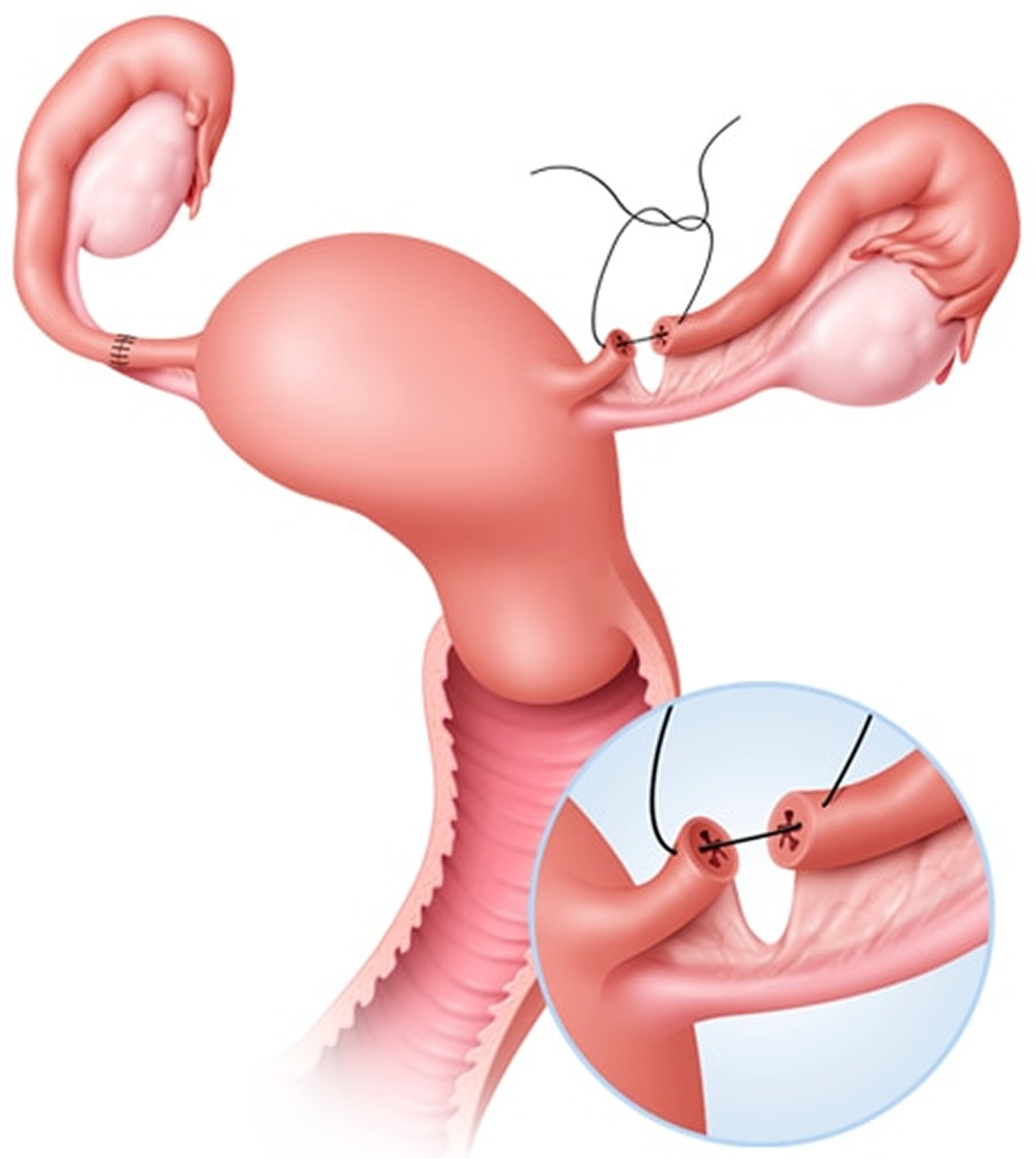
Female sterilization or tubal ligation works by preventing eggs from travelling down the fallopian tubes, which link the ovaries to the womb (uterus). This means a woman’s eggs cannot meet sperm, so fertilisation cannot happen.
Eggs will still be released from the ovaries as normal, but they’ll be absorbed naturally into the woman’s body.
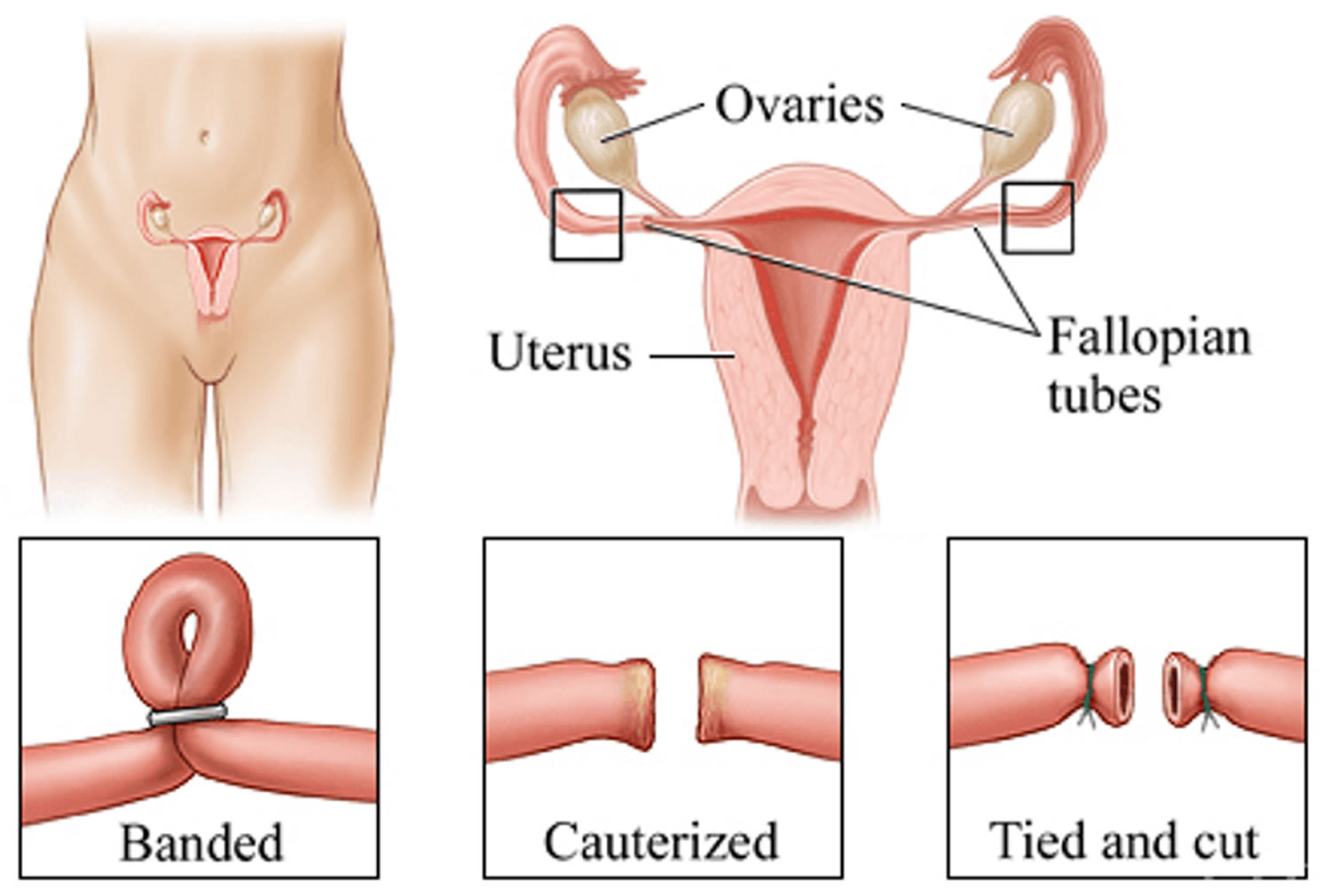
The surgeon will block your fallopian tubes (tubal occlusion) by either:
- applying clips – plastic or titanium clamps are closed over the fallopian tubes
- applying rings – a small loop of the fallopian tube is pulled through a silicone ring, then clamped shut
- tying, cutting and removing a small piece of the fallopian tube
This is a fairly minor operation, and many women return home the same day.
Figure 1. Tubal ligation
Advantages and disadvantages of tubal ligation
Tubal ligation advantages:
- more than 99% effective at preventing pregnancy
- blocking the fallopian tubes and removal of the tubes should be effective immediately – but use contraception until your next period
- tubal ligation won’t affect your sex drive or interfere with sex
- tubal ligation won’t affect your hormone levels
Tubal ligation disadvantages
- tubal ligation doesn’t protect against STIs, so you may need to use condoms
- tubal ligation can’t be easily reversed
- tubal ligation can fail – the fallopian tubes can rejoin and make you fertile again, although this is rare
- there’s a very small risk of complications, including internal bleeding, infection or damage to other organs
- tubal ligation you get pregnant after the operation, there’s an increased risk that it will be an ectopic pregnancy
Noncontraceptive Benefits of Tubal Ligation
Tubal ligation has been found to confer noncontraceptive health benefits. A number of case control and cohort studies in the United States and other countries report a protective effect of sterilization against ovarian cancer 1), 2), 3). While tubal ligation does not protect against sexually transmitted diseases (STDs), several case control and cohort studies have reported that pelvic inflammatory disease is less common in sterilized women 4), 5).
Although retrospective studies have reported both improvement and deterioration of sexuality after sterilization, most prospective cohort studies have shown either no change or improvement in sexual function, sexual desire, sexual satisfaction, coital frequency, and self-perceived femininity 6). Some women have reported that tubal ligation positively affected sexual spontaneity and satisfaction because they felt less anxious about the possibility of unplanned pregnancy 7).
Does tubal ligation protect against sexually transmitted infections (STIs)?
NO. Female sterilization does not protect against sexually transmitted infections. Using condoms every time you have sex is recommended and greatly lowers the risk of getting an STI.
Will tubal ligation affect my sex life?
No. Female tubal ligation will not change anything such as your sexual performance or your ability to have orgasms. In fact, some women feel more relaxed during sex because they’re not worried about becoming pregnant. Neither you nor your partner will be able to feel the clips or rings that may have been used to seal off your fallopian tubes.
Will my periods be the same after tubal ligation?
Your periods will likely be the same. Medical studies have shown that women who are sterilized may in fact have fewer days of bleeding with their menstrual cycle, have a lighter flow and less menstrual cramps. A very small number of women may complain of irregular periods and menstrual cramping after tubal ligation.
If you have any of the following symptoms, call your health care provider:
- Late or missed menstrual period
- Severe lower abdominal (belly) pain
- Nausea – feeling like you want to throw up
- Breast tenderness
What if I decide I want to get pregnant after I had tubal ligation?
If you change your mind after your fallopian tubes have been closed off you may be able to have your tubes rejoined, however reversing tubal ligation is a major operation and only about 50-70% successful. Less than 1% of women get their tubes rejoined, because they are almost always sure that they do not want any more children at the time of the tubal ligation procedure. Medical insurance does not pay to have a woman’s tubes “untied” or tubal ligation reversed.
The risk of ectopic pregnancy after a tubal ligation reversal also increases.
So if you’re thinking about a tubal ligation, talk about the risks and benefits with your partner and your doctor. This is meant to be permanent, although it doesn’t stop you having in vitro fertilization (IVF) and other forms of assisted reproduction later.
You should have a tubal ligation only if you’re absolutely sure you don’t want any more children, and not regret the decision later.
What are the alternatives to tubal ligation?
There are many alternatives to permanent tubal ligation, including:
- permanent male sterilization – vasectomy
- long-acting reversible contraception such as intrauterine devices (IUDs) and contraceptive implants in the skin of the arm
- short-acting reversible types of contraception – birth control pills, patches or vaginal rings, condoms, the diaphragm, a cervical cap or regular contraceptive injections
Tubal ligation failure
While tubal ligation is intended to permanently prevent pregnancy, failures do occur. Reasons for failure include undetected luteal pregnancy, occlusion of an incorrect structure (most commonly the round ligament), incomplete or inadequate occlusion, slippage of a mechanical device, development of a tuboperitoneal fistula, and spontaneous re-anastomosis or recanalization of the cut ends 8).
The U.S. Collaborative Review of Sterilization is the landmark prospective, multicenter, observational study 9) on the use of sterilization in this country. The U.S. Collaborative Review of Sterilization study was conducted by the Centers for Disease Control and Prevention (CDC) with support from the National Institute for Child Health and Human Development. The U.S. Collaborative Review of Sterilization recently reported a 10-year (1978 to 1987) cumulative failure rate for sterilization of 1.85 percent in 10,685 women 10). The U.S. Collaborative Review of Sterilization, which reports failure rates that are higher than previously expected, is the largest body of data, thus far, for this length of follow-up.
The U.S. Collaborative Review of Sterilization study found a higher-than-expected failure rate (i.e., 2.01 per 100 women over 10 years) for interval minilaparotomy sterilization, an office-based procedure 11). Most likely, this was a consequence of the low numbers of minilaparotomy cases (i.e., 425 women among a total of 10,685). The higher failure rate also might be caused by the fact that in the United States, interval minilaparotomy often is performed in surgically challenging circumstances, such as when severe pelvic adhesions are present and laparoscopy is deemed inappropriate 12).
The risk of tubal ligation failure persisted throughout the study period 13). This finding contradicts the widely held but inaccurate belief that if pregnancies are to occur after tubal ligation procedures, they will do so within one to two years after the operation. Although the U.S. Collaborative Review of Sterilization study revealed cumulative 10-year failure rates higher than previously thought, the study confirms that tubal ligation, when performed with appropriate technique by an experienced clinician, continues to be an extremely effective long-term contraceptive. Contraceptive candidates can be reassured that long-term risk of failure is low and that only the intrauterine device (IUD) and levonorgestrel (Norplant) implant system have comparable, long-term failure rates 14), 15).
The U.S. Collaborative Review of Sterilization study did not include data on the Filshie clip, which was unavailable in the United States at the time of study enrollment. A 10-year cumulative failure rate of 0.5 percent for 200 women was recently reported for the Filshie clip 16).
By preventing pregnancy, female tubal ligation has an overall protective effect on the risk of ectopic pregnancy. However, when pregnancy does occur it is likely to be ectopic pregnancy. Of the 143 pregnancies reported in the U.S. Collaborative Review of Sterilization study, one third were ectopic pregnancies 17).
Regret after tubal ligation
The two most common factors associated with regret are young age and unpredictable life events, such as change in marital status or death of a child 18). Regret also has been shown to correlate with external pressure by the clinician, spouse, relatives, or others 19). Interestingly, marital status at the time of the operation, level of education, and the absence of children do not, in many studies, correlate with regret 20).
Regret is difficult to measure because it encompasses a complex spectrum of feelings that can change over time. This helps to explain that while some studies have shown “regret” on the part of 26 percent of women, fewer than 20 percent seek reversal and fewer than 10 percent actually undergo the reversal procedure 21).
Depending on such factors as the technique used for tubal ligation, the resulting length and portion of undamaged fallopian tube remaining, the woman’s age, and the surgeon’s skill, success rates for reversal range from 47 to 90 percent 22). Women who are ambivalent about the permanence of the tubal ligation procedure should be counseled to strongly consider another contraceptive method.
What is fallopian tube
The fallopian tubes (uterine tubes or oviducts) open near the ovaries (Figure 2 and 3). Each fallopian tube is about 10 centimeters long and 0.7 centimeters in diameter, the middle and longest part of the fallopian tube is the ampulla and the segment near the uterus is a narrower isthmus – which passes medially to the uterus, penetrates its wall and opens into the uterine cavity. Near each ovary, a fallopian tube expands, forming a funnel-shaped infundibulum, which partially encircles the ovary. Fingerlike extensions called fimbriae fringe the infundibulum margin. Although the infundibulum generally does not touch the ovary, one of the larger fimbriae connects directly to the ovary.
The fallopian tube is enclosed in the mesosalpinx, which is the superior margin of the broad ligament.
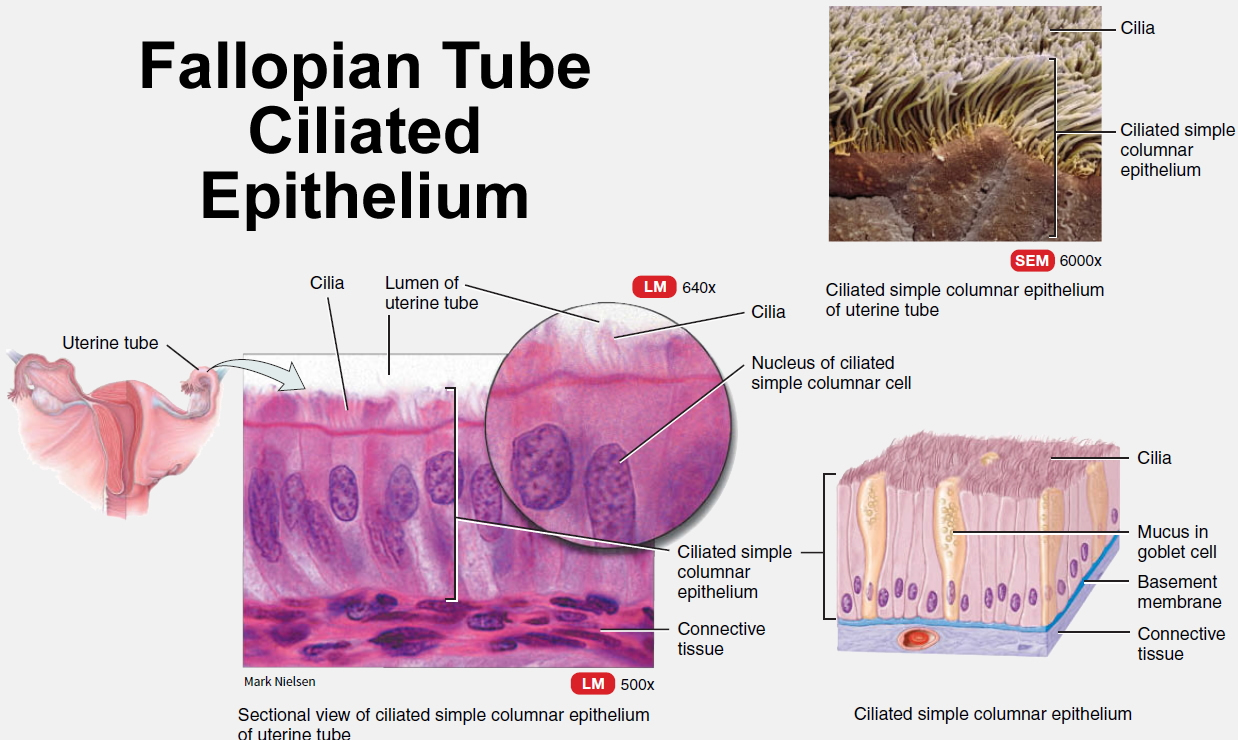
Simple columnar epithelial cells, some ciliated, line the fallopian tube. The epithelium secretes mucus, and the cilia beat toward the uterus. These actions help draw the secondary oocyte (an immature egg cell of the female ovary) and expelled follicular fluid into the infundibulum following ovulation. Ciliary action and peristaltic contractions of the fallopian tube’s smooth muscle layer aid transport of the oocyte down the uterine tube. Fertilization usually occurs in the fallopian tube.
Figure 2. Fallopian tube
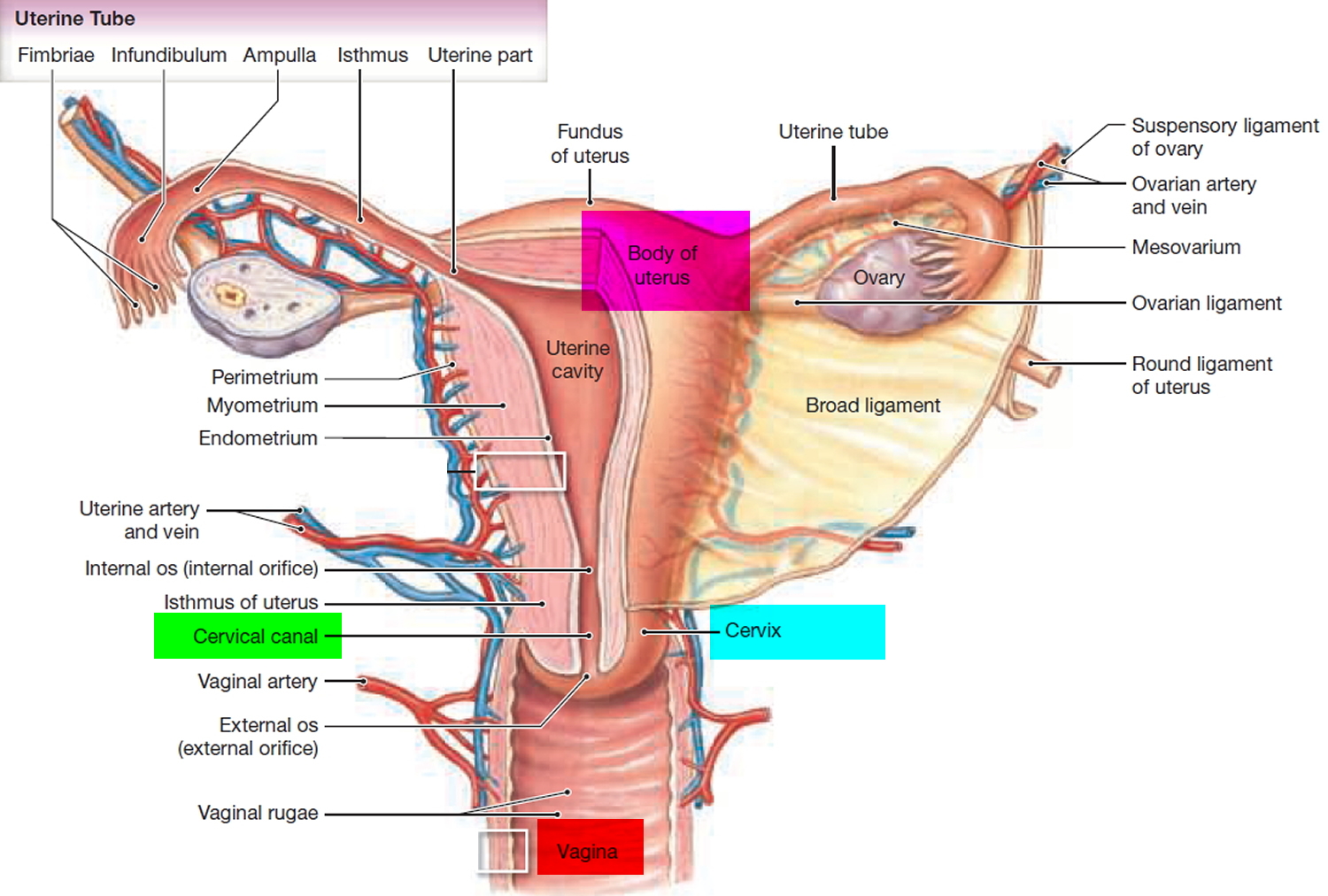
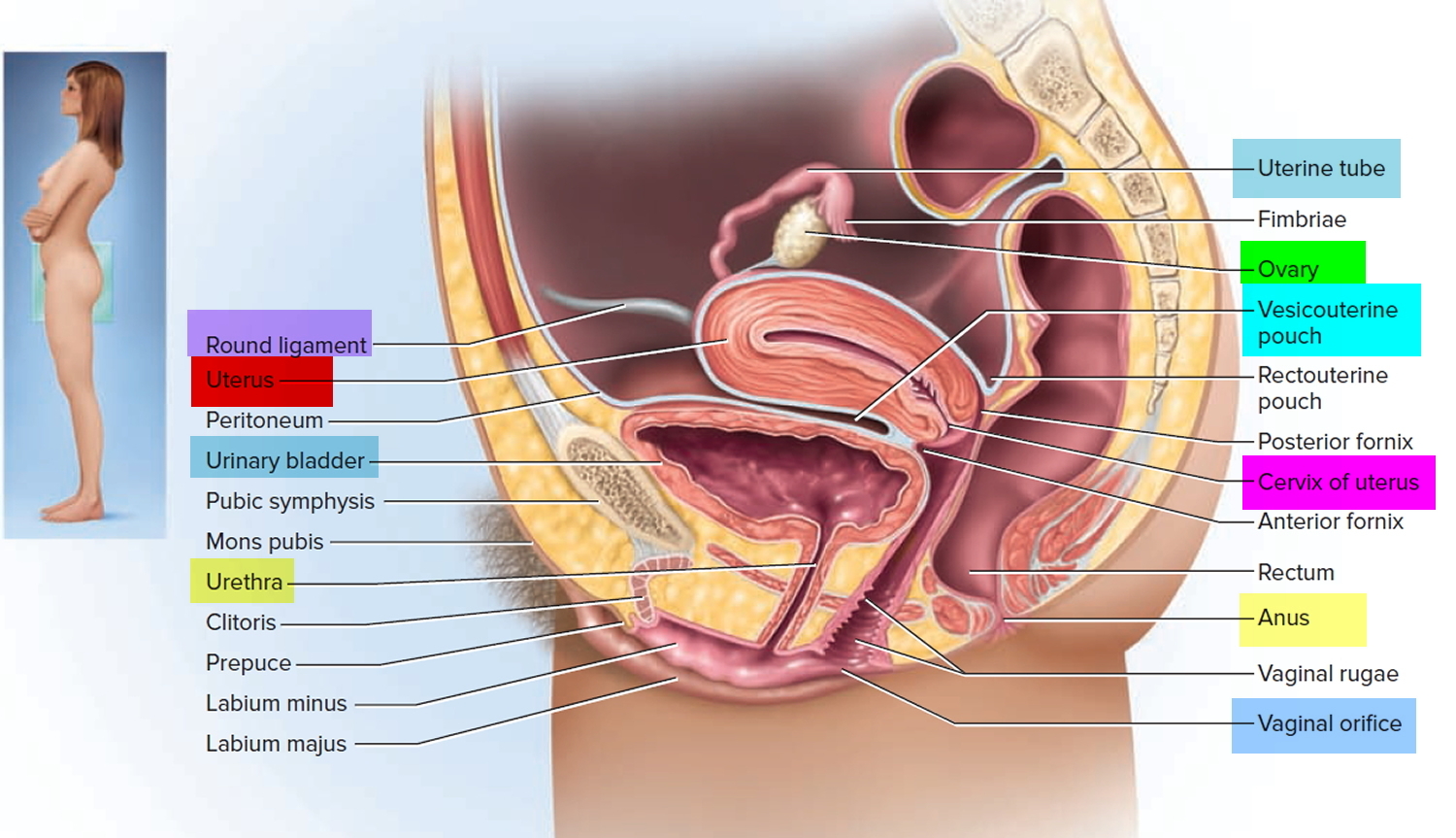
Figure 3. Fallopian tube location
Fallopian tube function
The normal epithelium of the fallopian tube is comprised of two cell types: ciliated and secretory. The ciliated cells of the fallopian tube play a major role in the transport of the ovum, the sperm cells, and the zygote (a fertilized ovum). The human ovary usually releases one egg (oocyte) per month, around day 14 of a typical 28-day ovarian cycle. This egg is swept into the fallopian (uterine) tube by the beating of cilia on the fallopian tube’s epithelial cells and begins a 3-day trip down the fallopian tube toward the uterus. If the egg is not fertilized, it dies within 24 hours and gets no more than one-third of the way to the uterus. Therefore, if a sperm is to fertilize an egg, it must migrate up the fallopian tube to meet it. The vast majority of sperm never make it. Although a typical ejaculation may contain 200 million sperm, many of these are destroyed by vaginal acid or drain out of the vagina; others fail to get through the cervical canal into the uterus; still more are destroyed by leukocytes in the uterus; and half of the survivors of all these ordeals are likely to go up the wrong fallopian tube tube. Only about 200 (1 in a million) reach the general vicinity of the egg.
The fallopian tube secretory cells secrete mucus that slows the progression of the spermatozoa through the fallopian tube, preserves their viability and facilitates their appropriate capacitation (functional maturation of the spermatozoon and is required to render them competent to fertilize an oocyte) and activation 23).
Figure 4. Fallopian tube ciliated epithelium
Tubal ligation procedure
You may be asked to take a pregnancy test to make sure you’re not pregnant.
If you have a tubal ligation, you will have a general anesthetic. The operation is usually done via keyhole surgery known as laparoscopy. Gas may be pumped into your belly to inflate it. This gives your surgeon a better view and more room to work. It is normally a day procedure, although an overnight stay in hospital is possible.
One or two tiny incisions are made in the lower abdomen and a small camera (laparoscope) is inserted so that the fallopian tubes can be seen. The tubes are then closed off by clips or sealed by heat.
After surgery is done, the surgeon will close the incisions in the skin, probably using 1 to 2 stitches. He or she will cover the area with small dressings.
Some women might need another form of operation known as a laparotomy, which involves a larger incision in the abdomen and several days’ stay in hospital.
How tubal ligation is done
Options for tubal ligation include laparoscopy or minilaparotomy. A laparoscopy is usually used because it’s faster, but a mini-laparotomy may be recommended for women who:
- have had recent abdominal or pelvic surgery
- are obese
- have a history of pelvic inflammatory disease, a bacterial infection that can affect the womb and fallopian tubes
Female tubal ligation can be done in an operating room or in a medical office depending on the type of procedure. It can be done while you are sleeping or while you are awake. If awake, you will be given numbing medicine so you don’t feel too uncomfortable. Depending on the type of method you choose to have, you could either have a small incision or cut in your abdomen (belly) or the procedure can be done vaginally (without any incisions or cuts).
A. Laparoscopic tubal ligation: A small cut is made in the abdomen (belly) and then an instrument with a tiny camera (called a laparoscope) is placed inside the belly near the navel (belly button). The fallopian tubes (the tubes that carry eggs from the ovaries to the uterus) are then closed shut with another instrument. This procedure is done in an operating room under general anesthesia (while sleeping) at any time during a woman’s cycle except immediately after she delivers a baby.
The fallopian tubes are cut and tied, removed, stitched with suture material, or burned. The fallopian tubes can also be entirely removed.
If blocking the fallopian tubes hasn’t worked, the tubes may be completely removed. This is called a salpingectomy.
- Sterilization using electrical current: An electrical current is used to burn and destroy the fallopian tubes after they have been cut. Sterilization done with an electrical current cannot be reversed.
- Silicone band (tubal ring): Through the laparoscope, the surgeon will insert a special tool that stretches a plastic band, picks up a small loop of the fallopian tube, and places the plastic band over the loop. The tube is then clamped shut.
- Spring clips: There are two types of clips that are used to clamp off the fallopian tubes. One, shaped like a clothespin, is placed over the fallopian tube and is held closed by its spring clip. The other type is a rounded clamp, which is closed over the fallopian tubes. The clamp’s plastic liner gets bigger to keep the tube closed as the tube flattens.
B. Minilaparotomy tubal ligation: This procedure is also done in an operating room with general or local anesthesia (numbing medicine) usually within 1-2 days after a woman has a baby.
C. Hysteroscopic tubal ligation: This procedure is called the “Essure” method and is done in an operating or office setting using local anesthesia (numbing medicine) about 7-10 days after a woman’s period. While the women is awake, the doctor inserts a thin instrument with a camera at the end, into the vagina, which is then passed through the cervix, uterus and finally to the fallopian tube where a tiny coil is placed. Scar tissue then grows which seals the tube shut. Since this takes time to happen, another form of birth control must be used for the first 3 months.
A follow-up test called the Essure Confirmation Test is done within 3 months after the procedure. This is similar to an x-ray which allows your doctor to see that your tubes are closed off. If the tubes are tightly sealed at this point, your health care provider will likely tell you that you can stop other forms of birth control. However, you should always use condoms to prevent sexually transmitted infections (STIs). Essure can usually be done anytime except immediately after a woman gives birth.
What should I expect if I have the hysteroscopic sterilization or “Essure” procedure?
Before you sign the consent to have the procedure, your health care provider should talk to you about the possible risks that include; infection, pelvic pain, incomplete blockage of the tubes, and the rare possibility of causing a hole in the uterus or fallopian tubes.
You may be given medicine before the procedure to help you relax and prevent spasms of the tubes. The procedure itself is usually takes about 30-45 minutes. You will be able to go home shortly after the procedure and go back to your normal activities later in the day.
You may have:
- Dizziness
- Cramps
- Bleeding or spotting
- Abdominal (belly) pain
Tubal ligation recovery
After your laparoscopic procedure, you will stay in the recovery room until you are wide awake and able to eat and drink light foods such as crackers and ginger ale. Most women go home within 2-4 hours on the same day. You’ll need someone to bring you to the hospital and take you home. Most women need a few days to recover from the anesthetic. Some women have pain in their shoulders, and some have minor abdominal discomfort immediately after the operation for a few days. If any of the symptoms below last longer than a couple of days, call your health care provider. Most women can go back to school or work within 1 week of having the tubal ligation procedure, but everyone is different so be sure to listen to what your health care provider tells you.
- Dizziness
- Shoulder pain
- Cramps
- Bloated or gassy feeling
A few women get injuries to the bowel, bladder or blood vessels due to accidental perforation.
There is still a small chance you can get pregnant, even years later. If this does happen, there is an increased risk of the pregnancy being ectopic, or outside the uterus, which can be dangerous.
Caring for your wound
If you had tubal occlusion, you’ll have a wound with stitches where the surgeon made the cut. The stitches would need to be removed at a follow-up appointment unless dissolvable ones were used.
If there’s a dressing over your wound, you can normally remove this the day after your operation. After this, you’ll be able to have a bath or shower.
Follow these self-care steps after your procedure:
- Keep your incision areas clean, dry, and covered. Change your dressings (bandages) as your health care provider told you to.
- DO NOT take baths, soak in a hot tub, or go swimming until your skin has healed.
- Avoid heavy exercise for several days after the procedure. Try not to lift anything heavier than 10 pounds (about a gallon, 5 kg, jug of milk).
- You can have sexual intercourse as soon as you feel ready. For most women, this is usually within a week.
- You may be able to return to work within a few days.
- You may eat your normal foods. If you feel sick to your stomach, try dry toast or crackers with tea.
Call your doctor if you have:
- Severe belly pain, or the pain you are having is getting worse and does not get better with pain medicines
- Heavy bleeding from your vagina on the first day, or your bleeding does not lessen after the first day
- Fever higher than 100.5 °F (38 °C) or chills
- Pain, shortness of breath, feeling faint
- Nausea or vomiting
Also call your doctor if your incisions are red or swollen, become painful, or there is a discharge coming from them.
Having sex
Your sex drive and sex life shouldn’t be affected. You can have sex as soon as it’s comfortable to do so after the operation.
If you had tubal occlusion, use additional contraception until your first period to protect yourself from pregnancy.
Sterilisation doesn’t protect against sexually transmitted infections (STIs), so you may need to use condoms.
Pregnancy after tubal ligation
Can you get pregnant with your tubes tied?
While tubal ligation is intended to permanently prevent pregnancy, failures do occur. Reasons for failure include undetected luteal pregnancy, occlusion of an incorrect structure (most commonly the round ligament), incomplete or inadequate occlusion, slippage of a mechanical device, development of a tuboperitoneal fistula, and spontaneous re-anastomosis or recanalization of the cut ends 24).
The U.S. Collaborative Review of Sterilization is the landmark prospective, multicenter, observational study 25) on the use of sterilization in this country. The U.S. Collaborative Review of Sterilization study was conducted by the Centers for Disease Control and Prevention (CDC) with support from the National Institute for Child Health and Human Development. The U.S. Collaborative Review of Sterilization recently reported a 10-year (1978 to 1987) cumulative failure rate for sterilization of 1.85 percent in 10,685 women 26). The U.S. Collaborative Review of Sterilization, which reports failure rates that are higher than previously expected, is the largest body of data, thus far, for this length of follow-up.
The U.S. Collaborative Review of Sterilization study found a higher-than-expected failure rate (i.e., 2.01 per 100 women over 10 years) for interval minilaparotomy sterilization, an office-based procedure 27). Most likely, this was a consequence of the low numbers of minilaparotomy cases (i.e., 425 women among a total of 10,685). The higher failure rate also might be caused by the fact that in the United States, interval minilaparotomy often is performed in surgically challenging circumstances, such as when severe pelvic adhesions are present and laparoscopy is deemed inappropriate 28).
The risk of tubal ligation failure persisted throughout the study period 29). This finding contradicts the widely held but inaccurate belief that if pregnancies are to occur after tubal ligation procedures, they will do so within one to two years after the operation. Although the U.S. Collaborative Review of Sterilization study revealed cumulative 10-year failure rates higher than previously thought, the study confirms that tubal ligation, when performed with appropriate technique by an experienced clinician, continues to be an extremely effective long-term contraceptive. Contraceptive candidates can be reassured that long-term risk of failure is low and that only the intrauterine device (IUD) and levonorgestrel (Norplant) implant system have comparable, long-term failure rates 30), 31).
The U.S. Collaborative Review of Sterilization study did not include data on the Filshie clip, which was unavailable in the United States at the time of study enrollment. A 10-year cumulative failure rate of 0.5 percent for 200 women was recently reported for the Filshie clip 32).
By preventing pregnancy, female tubal ligation has an overall protective effect on the risk of ectopic pregnancy. However, when pregnancy does occur it is likely to be ectopic pregnancy. Of the 143 pregnancies reported in the U.S. Collaborative Review of Sterilization study, one third were ectopic pregnancies 33).
Tubal ligation side effects
Overall, major complications of tubal ligation are rare, occurring in fewer than 0.5 percent of cases 34). Complications are influenced by factors such as choice of anesthetic, patient characteristics, positioning, technique, and operator experience 35).
Short-term complications (e.g., anesthetic difficulties and hemorrhage) occur in the operating room and manifest immediately or in the first several weeks after surgery. Trauma to organs such as the bowel, bladder, ureter, uterus, and cervix can result from cautery, occlusion, and sharp and blunt traumas. Death, a rare outcome of tubal ligation, occurs in only one or two of every 100,000 cases in the United States 36). Currently, the U.S. death rate secondary to complications of pregnancy is seven per 100,000 live births 37). The 29 sterilization-associated deaths reported in the United States between 1977 and 1981 were associated with complications of anesthesia (11 women), sepsis (seven women), hemorrhage (four women), myocardial infarction (three women), and “other causes” (four women) 38).
Women may fear long-term complications of tubal ligation, such as future risk of hysterectomy and changes in menstrual pattern. Although hysterectomy rates are higher among U.S. women who were sterilized before the age of 30, a plausible biologic effect of tubal ligation on hysterectomy risk is unlikely 39), 40). Increased risk of hysterectomy is a finding unique to the United States. Studies from other countries, where hysterectomy is less common, consistently do not report an increased risk 41). Recent studies also show no association between tubal ligation and menstrual cycle change 42).
Post tubal ligation syndrome
The term post tubal ligation syndrome was first reported in the early 1950s based on the results of a study in which the effect of menstrual disorders on some of somatic and psychological symptoms were evaluated 43). Post tubal ligation syndrome has been described, variously, as encompassing symptoms such as abnormal bleeding and/or pain, changes in sexual behavior and emotional health, exacerbation of premenstrual symptoms, and menstrual symptoms necessitating hysterectomy or tubal reanastomosis 44). Although based on the conjecture, it has been postulated that the destruction of the fallopian tube and, in some cases, portions of the mesosalpinx, alters the blood supply to the ovary, with consequent impairment of follicular growth and corpus luteum function, leading to altered gonadotropin signal and ovarian hormone levels, resulting in menstrual disorders 45). Abnormalities reports associated with tubal ligation surgery include the entire spectrum of menstrual disorders, such as: more frequent menstrual periods, irregular menstrual cycles, menorrhagia, metrorrhagia, spotting, dysmenorrhea and oligomenorrhea 46). However, some studies 47), 48) showed no increase in menstrual disorders in women undergoing tubal ligation as compared with a control group.
This study 49) indicated that sterilized women (tubal ligation) were more likely to experience an increase in polymenorrhea, hypermenorrhea, menorrhagia, and menometrorrhagia and to have an irregular menstrual cycle when compared with the other group.
Some studies showed a significant increase in incidence of menstrual disorder in women undergoing tubal ligation when compared with a control group 50). Increased duration (hypermenorrhea) and amount of bleeding (menorrhagia) have been reported by Shain et al. 51). Tubal ligation has been considered as the cause of menstrual abnormalities by damaging the ovary 52), including acute increase in pressure in the utero-ovarianarterial loop 53).
Peterson et al. 54) found women who have undergone tubal ligation are no more likely than other women to have menstrual abnormalities. Futhermore, Shobeiri and Atashkhoii 55) concluded that tubal ligation does not cause menstrual disorders. Several other studies concluded that the duration of bleeding, volume of menstrual flow, menstrual cycle length and cycle irregularity are similar in women with and without tubal legation 56). Although it has been hypothesized that menstrual disorders are caused by the damaging effect of tubal ligation on ovarian function through an increase in pressure within the utero-ovarian arterial circulation or disruption of the ovarian blood supply, some researchers have not observed an alteration in ovarian function 57). In addition, laboratory studies comparing women before and after tubal ligation have found no constant abnormalities in ovarian function 58), indicating no difference in luteinizing hormone (LH), follicle stimulating hormone (FSH) and estradiol (E2) levels in women undergoing tubal ligation when compared with a non-tubal ligation group 59).
Menorrhagia is identified as the most common bleeding disorders 60). Several studies showed that there was no significantly difference regarding menorrhagia between the case and control groups 61). In another study by Wilcox et al. 62), they reported heavy menstrual flow (41%) after 5 years following tubal ligation. However, we need more evidence based on cohort studies to confirm the results of the present study.
Tubal ligation reversal
Tubal ligation reversal or tuboplasty is a surgery done to allow a woman who has had her tubes tied (tubal ligation) to become pregnant again 63). The fallopian tubes are reconnected in this reversal surgery. A tubal ligation cannot always be reversed if there is too little tube left or if it is damaged.
Tubal ligation reversal surgery is done to allow a woman who has had her tubes tied to become pregnant. However, the surgery is rarely done any more. This is because the success rates with in vitro fertilization (IVF) have risen. Women who wish to become pregnant after having tubal ligation, are most often counselled to try in vitro fertilization (IVF) instead of surgical reversal.
Insurance plans often do not pay for tubal ligation reversal surgery surgery.
Figure 4. Tubal ligation reversal
Tubal ligation reversal risks
Risks for anesthesia and surgery are:
- Bleeding or infection
- Damage to other organs (bowel or urinary systems) may need more surgery to repair
- Allergic reactions to medicines
- Breathing problems or pneumonia
- Heart problems
Risks for tubal ligation reversal are:
- Even when surgery reconnects the tubes, the woman may not become pregnant.
- A 2% to 7% chance of a tubal (ectopic) pregnancy.
- Injury to nearby organs or tissues from surgical instruments.
Before the tubal ligation reversal procedure
Always tell your health care provider what medicines you are taking, even medicines, herbs, or supplements you bought without a prescription.
During the days before your tubal ligation reversal surgery:
- You may be asked to stop taking aspirin, ibuprofen (Advil, Motrin), warfarin (Coumadin), and any other medicines that make it hard for your blood to clot.
- Ask your healthcare provider which medicines you should still take on the day of your surgery.
- If you smoke, try to stop. Ask provider for help quitting.
On the day of your tubal ligation reversal surgery
- You will most often be asked not to drink or eat anything after midnight the night before your surgery, or 8 hours before the time of your surgery.
- Take the medicines your provider told you to take with a small sip of water.
- Your healthcare provider will tell you when to arrive at the hospital or clinic.
After the tubal ligation reversal procedure
You will probably go home the same day you have the tubal ligation reversal procedure. Some women may need to stay in the hospital overnight. You will need a ride home.
It may take a week or more to recover from tubal ligation reversal surgery. You will have some tenderness and pain. Your provider will give you a prescription for pain medicine or tell you which over-the-counter pain medicine you can take.
Many women will have shoulder pain for a few days. This is caused by the gas used in the abdomen to help the surgeon see better during the procedure. You can relieve the gas by lying down.
You may shower 48 hours after the procedure. Pat the incision dry with a towel. DO NOT rub the incision or strain for 1 week. The stitches will dissolve over time.
Your healthcare provider will tell you how long to avoid heavy lifting and sex after the surgery. Return to normal activities slowly as you feel better. See the surgeon 1 week after surgery to make sure healing is going well.
Tubal ligation reversal outlook (prognosis)
Most women have no problems with the tubal ligation reversal surgery itself.
A range from 30% to 50% up to 70% to 80% of women may become pregnant. Whether a woman becomes pregnant after this surgery may depend on 64):
- Her age
- The presence of scar tissue in the pelvis
- The method used when tubal ligation was done
- The length of the fallopian tube that is rejoined
- The skill of the surgeon
Most pregnancies after tubal ligation reversal procedure occur within 1 to 2 years.
Vasectomy vs Tubal ligation
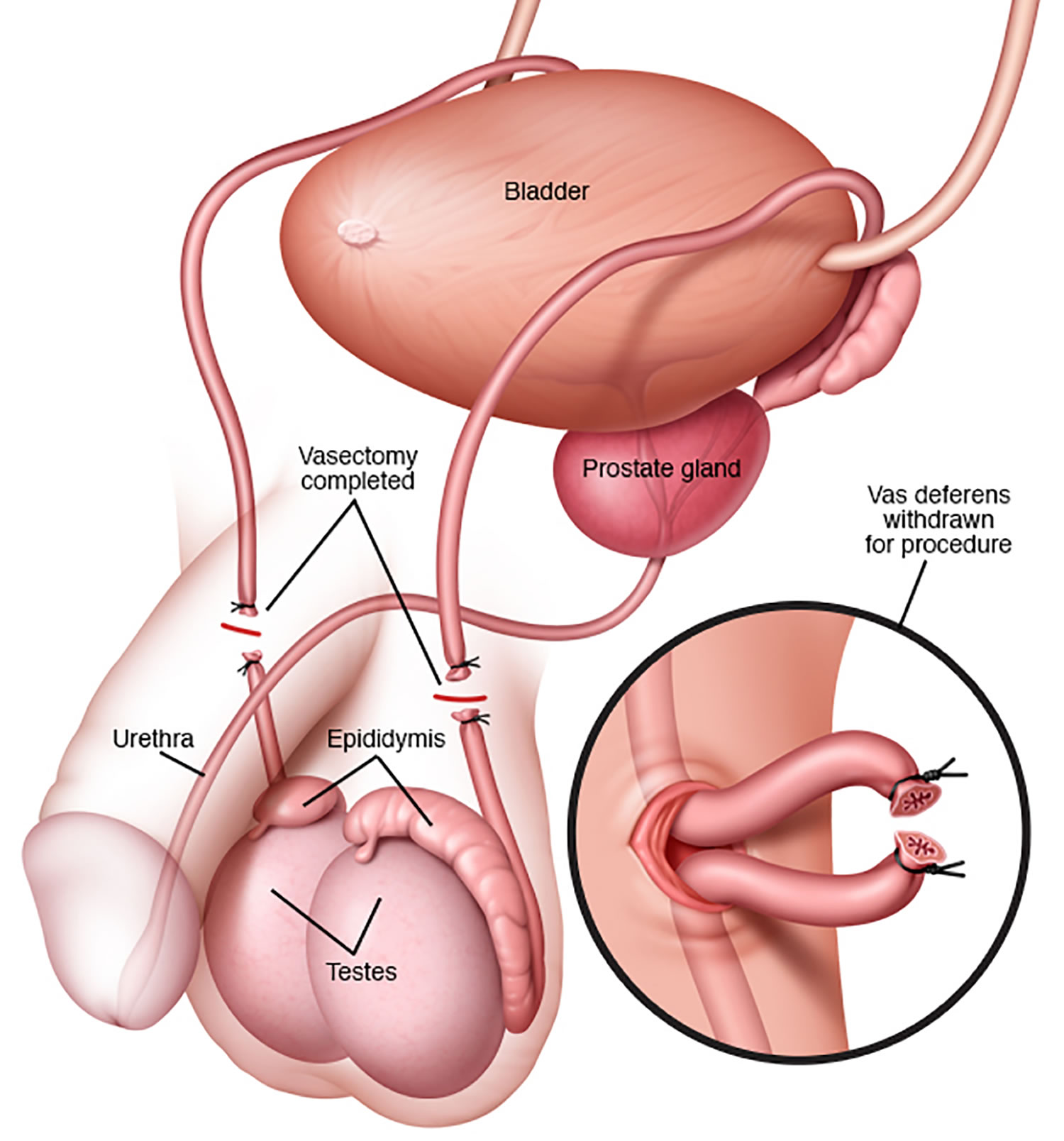
Vasectomy or ‘male sterilization’ is a minor surgical procedure to cut or seal the tubes (vas deferens) that carry a man’s sperm to permanently prevent pregnancy. Vasectomy procedure is done to keep a man’s sperm from going to his penis, so his ejaculate never has any sperm in it that can fertilize an egg. Although sperm continue to be produced, they can no longer exit the body and are phagocytized in the epididymis. Vasectomy is a simple procedure that is done at an outpatient surgical center and reliable method of contraception. Vasectomy is usually considered permanent and is therefore a big decision that should be fully discussed with your doctor beforehand. Although most men who undergo contraceptive sterilization do not regret having had the procedure, the permanence of the vasectomy method is an important consideration, as regret has been documented in studies. Men who have vasectomy before age 30 are the group most likely to want a vasectomy reversal in the future 65).
A vasectomy is a quick and relatively painless surgical procedure. Vasectomy is usually done under local anesthetic, where you’re awake but don’t feel any pain, and takes about 15 to 30 minutes. You can go home the same day. In rare cases, you may have a general anesthetic, where you’re asleep during the operation. Recovery time is less than one week. Patients should refrain from ejaculation for approximately one week after vasectomy. After the operation, you need to visit your doctor for tests to count your sperm and to make sure the sperm count has dropped to zero; this takes about 12 to 16 weeks. Another form of birth control should be used until the your sperm count has dropped to zero.
Vasectomy is the most common non-diagnostic operation performed by urologists in the United States. Data from the National Study of Family Growth in which only married couples were polled indicate a range from 175,000 to 354,000 66). In a physician survey, an estimated 526,501 vasectomies were performed in the US in 2002 67). This number seems to have been approximately stable for the previous decade. More than 75% of vasectomies in the US are done by urologists, and about 90% of urology practices in the US perform vasectomy 68).
In 2002, data collected in the US show that vasectomy was used by 5.7% of men ages 15-44 and that this represents the fourth most commonly-used contraceptive method. The first three were condoms, used by 29.5% of men, oral contraceptives for women used by 25.6% of couples and tubal ligation used by 8.1% of couples 69). Compared to tubal ligation , which is also a method of permanent contraception, vasectomy is equally effective in preventing pregnancy; however, vasectomy is simpler, faster, safer and less expensive. Vasectomy is one of the most cost-effective of all methods of contraception; its cost is about one-fourth of the cost of tuba lligation 70). Vasectomy requires less time off work, requires only local rather than general anesthesia and is usually performed in a doctor’s office or clinic. The potential complications of vasectomy are less serious than those of tubal ligation.
Despite the clear advantages of vasectomy, prevalence data for 1998-2002 show that tubal ligation (female sterilization) was performed about two to three times more often than vasectomy 71). Among all women in 2002, married and unmarried, ages 15 to 44 years in the United States, only 5.7% relied on vasectomy for contraception compared to 16.7% who relied on tubal ligation 72). Even among married women and married men who desire permanent contraception, in the US the prevalence of tubal ligation has exceeded the prevalence of vasectomy 73).
Worldwide, the discrepancy between vasectomy and tubal ligation is even more marked than in the US. Data compiled in 2008 by the Population Division of the Department of Economic and Social Affairs of the United Nations show that 33 million married women ages 15-49 relied on vasectomy for contraception compared to 225 million who relied on tubal ligation 74). There are only eight nations in which vasectomy use is equal to or more frequent than tubal ligation for contraception – Korea, Canada, the United Kingdom, New Zealand, Bhutan, the Netherlands, Denmark and Austria ()World Contraceptive Use 2011. http://www.un.org/esa/population/publications/contraceptive2011/wallchart_front.pdf)).
Given that vasectomy and tubal ligation have equivalent contraceptive effectiveness and that vasectomy enjoys advantages compared to tubal sterilization of lower cost, less pain, greater safety and faster recovery, vasectomy should be considered for permanent contraception much more frequently than is the current practice in the United States and most nations of the world.
When considering a vasectomy, it’s important to understand that failures can occur. The U.S. Centers for Disease Control and Prevention research has estimated there is a probability of 11 failures per 1,000 procedures over 2 years; half of the failures occurred in the first three months after the vasectomy, and no failures occurred after 72 weeks 75). The U.S. Centers for Disease Control and Prevention research also examined regret among women whose partner underwent a vasectomy 76). In interviews with female partners of men who received vasectomies, the U.S. Centers for Disease Control and Prevention found that while most women did not regret their husband’s vasectomies, the probability of regret over 5 years was about 6%. This is why it is important to know facts about vasectomy and other permanent forms of birth control before making a decision.
Vasectomy key facts
- A vasectomy is more than 99% effective.
- Vasectomy does not produce immediate sterility. Following vasectomy, another form of contraception is required until vas occlusion is confirmed by post- vasectomy semen analysis. You’ll need to use contraception for at least 8 to 16 weeks after the vasectomy operation, because sperm will still be in the tubes leading to the penis.
- Eight to sixteen weeks after vasectomy is the appropriate time range for the first post- vasectomy semen analysis. The choice of time to do the first post- vasectomy semen analysis should be left to the judgment of the surgeon.
- Up to 2 semen tests are done after the vasectomy operation to make sure that all the sperm have gone.
- Vasectomy should be considered a failure if any motile sperm are seen on post- vasectomy semen analysis at six months after vasectomy, in which case repeat vasectomy should be considered.
- If > 100,000 non-motile sperm/mL persist beyond six months after vasectomy, then trends of serial post- vasectomy semen analyses and clinical judgment should be used to decide whether the vasectomy is a failure and whether repeat vasectomy should be considered 77).
- Even after vas deferens occlusion is confirmed, vasectomy is not 100% reliable in preventing pregnancy. The risk of failure depends on a number of factors. For example, some surgical techniques are more likely to fail than others 78). Additionally, there is a very small risk that the two ends of the vas deferens will grow back together. If this happens, sperm may be able to enter the semen and make pregnancy possible 79).
- The risk of pregnancy after vasectomy is approximately 1 or 2 out of 1,000 couples get pregnant the first year after a vasectomy even after post-vasectomy azoospermia (absence of sperm during microscopic exam of at least 50 Hpfs in a single well mixed, uncentrifuged semen specimen) or post- vasectomy semen analysis showing rare non-motile sperm.
- Vasectomy is considered permanent, so once it’s done you don’t have to think about contraception again.
- Vasectomy doesn’t affect your sex drive or ability to enjoy sex. You’ll still have erections and ejaculate, but your semen won’t contain sperm.
- Your ball sack (scrotum) may become bruised, swollen or painful – some men have ongoing pain in their testicles. Chronic scrotal pain associated with negative impact on quality of life occurs after vasectomy in about 1-2% of men. Few of these men require additional surgery.
- As with any surgery, there’s a small risk of infection.
- Vasectomy is very difficult to reverse, so be sure it’s right for you.
- A vasectomy doesn’t protect against sexually transmitted infections (STIs), so you will need to use condoms as well.
- Vasectomy is intended to be a permanent form of contraception.
- Repeat vasectomy is necessary in ≤1% of vasectomies, provided that a technique for vas occlusion known to have a low occlusive failure rate has been used.
- Options for fertility after vasectomy include vasectomy reversal and sperm retrieval with in vitro fertilization (IVF). These options are not always successful, and they may be expensive.
- The rates of surgical complications such as symptomatic hematoma and infection are 1-2%. These rates vary with the surgeon’s experience and the criteria used to diagnose these conditions.
- Other permanent and non-permanent alternatives to vasectomy are available.
Before you decide to have a vasectomy
Your doctor will ask about your circumstances, provide information, and may recommend counseling before agreeing to the procedure.
You should only have a vasectomy if you’re certain you don’t want any more children or don’t want children at all.
If you have a partner, discuss it with them before you decide. If possible, you should both agree to the procedure, but it’s not a legal requirement to get your partner’s permission.
Once you have had a vasectomy, it’s very difficult to reverse it, so consider all options and use another method of contraception until you’re completely sure.
You may be more likely to be accepted for a vasectomy if you’re over 30 and have had children.
But your doctor can refuse to carry out the procedure, or refuse to refer you, if they don’t believe it’s in your best interests.
How vasectomy works
A vasectomy works by stopping sperm getting into a man’s semen, the fluid that he ejaculates.
The tubes (vas deferens) that carry sperm from a man’s testicles to the penis are cut, blocked or sealed with heat.
This means that when a man ejaculates, the semen has no sperm in it and a woman’s egg can’t be fertilized.
Who can have a vasectomy?
You should only have a vasectomy if you’re sure that you don’t want more, or any, children. Vasectomy should always be seen as permanent.
This is because although vasectomy reversal is sometimes possible, it may not be successful. Even with a successful operation, it may still not be possible to father a child.
Can I have the vasectomy operation if I’m single?
Yes. But if you’re under 30, you’ll find many surgeons are reluctant to do it in case your circumstances change and you regret it later.
Will vasectomy affect my sex drive?
No. After a successful vasectomy, your testicles will continue to produce the male hormone (testosterone) just as they did before the procedure.
Your sex drive, sensation and ability to have an erection won’t be affected. The only difference is that there’ll be no sperm in your semen. Your body still produces sperm, but they’re absorbed back into your body without harm.
Could being sterile affect me emotionally?
It’s a big decision to have a vasectomy, so you should think it over carefully. If you’re sure about your decision, you may feel relieved that you don’t need to think about contraception and the possibility of pregnancy again.
But if you feel anxious or uncomfortable about the procedure, or you think you would find it hard to accept being infertile, it may not be suitable for you.
See a doctor or a professional at a contraception or sexual health clinic to talk about all of your options.
Is there any risk of vasectomy causing cancer?
Although prostate cancer and testicular cancer can occur in men who have had a vasectomy, research suggests that a vasectomy doesn’t increase your risk of cancer.
Can I use IVF to father a child?
If you have a vasectomy and later decide that you want a child, you may be able to use IVF. To do this, a surgeon would retrieve sperm from your testicles and use this to fertilize your partner’s egg.
But IVF:
- isn’t always successful
- can be expensive if done privately
Can I store sperm in a sperm bank, just in case?
You could, but as with IVF, sperm stored in a sperm bank can’t be relied on to bring about a pregnancy. It can also be expensive.
Advantages and disadvantages of a vasectomy
Vasectomy advantages
- a vasectomy is more than 99% effective at preventing pregnancy
- long-term effects on your health are rare
- it doesn’t affect your hormone levels, sex drive or interfere with sex
- it may be chosen as a simpler and safer alternative to female tubal ligation
Vasectomy disadvantages
- vasectomy doesn’t protect against STIs, so you may need to use condoms as well
- a vasectomy can’t be easily reversed
- you need to keep using contraception after the operation until tests show your semen is free of sperm
- possible complications include a collection of blood inside the scrotum (hematoma), hard lumps called sperm granulomas (caused by sperm leaking from the tubes), an infection, or long-term testicle pain (you may need further surgery)
- the vas deferens tubes can reconnect, but this is very rare
Figure 5. Vasectomy
How a vasectomy is performed
A vasectomy is a quick and relatively painless surgical procedure. In most cases, you’ll be able to return home the same day.
There are 2 types of vasectomy:
- a conventional vasectomy using a scalpel (surgical knife)
- a no-scalpel vasectomy
The doctor doing your vasectomy will discuss which option is best for you.
Conventional vasectomy
The doctor first numbs your scrotum with a local anesthetic. They then make 2 small cuts in the skin on each side of your scrotum to reach the tubes (vas deferens) that carry sperm out of your testicles.
Each tube (vas deferens) is cut and a small section removed. The ends of the vas deferens tubes are then closed, either by tying them or sealing them using heat.
The cuts are stitched, usually using dissolvable stitches that go away on their own within about a week.
No-scalpel vasectomy
The doctor first numbs your scrotum with local anesthetic. They then make a tiny puncture hole in the skin of your scrotum to reach the tubes. This means they don’t need to cut the skin with a scalpel.
The vas deferens tubes are then closed in the same way as a conventional vasectomy, either by being tied or sealed.
There’s little bleeding and no stitches with this procedure. It’s thought to be less painful and less likely to cause complications than a conventional vasectomy.
Recovering after the vasectomy operation
It’s common to have some mild discomfort, swelling and bruising of your scrotum for a few days after the vasectomy.
You can take painkillers, such as paracetamol, to help. See a doctor if it’s still painful after taking painkillers.
It’s common to have blood in your semen in the first few ejaculations after a vasectomy. This isn’t harmful.
Underwear
Wear tight-fitting underwear or athletic support day and night for the first few days to help support your scrotum and ease any discomfort or swelling. Make sure you change your underwear every day.
Hygiene
It’s usually safe for you to have a bath or shower after your operation – check with your doctor what’s suitable for you. Make sure you dry your genital area gently and thoroughly.
Returning to work
You can usually return to work 1 or 2 days after a vasectomy, but should avoid sport and heavy lifting for at least a week after the procedure to prevent complications. See a doctor if you still have symptoms after a few days.
Having sex
You can have sex again as soon as it’s comfortable to do so. You’ll need to use another method of contraception for at least the first 8 to 12 weeks, as it can take this long to clear the remaining sperm in your tubes.
How long this takes varies from man to man. There’s still a risk of pregnancy during this time.
How will I know if my vasectomy has worked?
About 12 weeks after the procedure, you’ll need to produce a sample of semen, which will be tested for sperm.
Once tests have confirmed that your semen is sperm-free, the vasectomy is considered successful and you can stop using additional contraception.
Some men may need 2 tests. But until it’s been confirmed that your semen is free of sperm, continue to use another form of contraception.
A few men will continue to have small numbers of sperm in their system, but these sperm don’t move and are less likely to make your partner pregnant.
If you’re one of these men, your doctor will discuss your options with you.
The test also helps to identify the rare cases in which the tubes naturally rejoin themselves.
Is vasectomy reversal possible?
It’s possible to have a vasectomy reversed. But the procedure isn’t always successful. You have a better chance if it’s done soon after the vasectomy.
If a reversal is carried out within 10 years of your vasectomy, the success rate is about 55%. This falls to 25% if your reversal is carried out more than 10 years after.
Even if a surgeon manages to join up the vas deferens tubes again, pregnancy may still not be possible, so you should be certain before going ahead with the vasectomy.
References [ + ]





{kind=link}