Contents
- Ubiquinone
- Ubiquinone Food sources
- Ubiquinone mechanism of action
- Ubiquinone vs Ubiquinol
- Coenzyme Q10 deficiency
- Ubiquinone supplement benefits
- Ubiquinone for cancer
- Reversal of statin-induced myopathy
- Neurological disorders
- Aging
- Blood lipids
- Atherosclerosis
- Cardiovascular risk factors
- Congestive heart failure
- Ischemia-reperfusion injury
- Periprocedural myocardial injury
- Angina pectoris
- High blood pressure
- Diabetes mellitus
- Athletic performance
- Other uses
- Ubiquinone dosage
- Ubiquinone Contraindications
- Ubiquinone side effects
Ubiquinone
Ubiquinone also called coenzyme Q10 (CoQ10), ubidecarenone or vitamin Q10 is a benzoquinone compound (a fat-soluble vitamin K-like molecule) that is naturally present in the human body in most body tissues, with the highest levels in your heart, liver, kidneys, and pancreas 1, 2. The lowest amounts are found in your lungs 3. In Coenzyme Q10, the letter Q refers to the quinone ring which is the active catalytic site of the coenzyme (a molecule that binds to an enzyme and is essential for its activity but is not permanently altered by the reaction); the number 10 refers to the 10 isoprene units (a volatile organic compound with the chemical formula C5H8) that make up the long tail of the Coenzyme Q10 molecule. The name Ubiquinone refers to the ubiquitous presence of these compounds in living organisms and their chemical structure, which contains a functional group known as a benzoquinone (a compound related to benzene but having two hydrogen atoms replaced by oxygen with the formula C₆H₄O₂). Ubiquinones are fat-soluble molecules with anywhere from 1 to 12 isoprene (5-carbon) units. The ubiquinone found in humans, ubidecaquinone or coenzyme Q10, has a “tail” of 10 isoprene units (a total of 50 carbon atoms) attached to its benzoquinone “head” (Figures 1 and 2) 4. All humans, including animals, can synthesize ubiquinones, hence, coenzyme Q10 is not considered a vitamin despite Ubiquinone (Coenzyme Q10) being somewhat similar in structure to vitamin K 4.
The largest percentage coenzyme Q10 (CoQ10) is synthetized in the cell (4-hydroxybenzoate is the precursor of a quinone ring, while an isoprenoid tail is derived from the mevalonate pathway), although the pathways involved are not yet completely known 5. The biosynthesis of coenzyme Q10 (CoQ10) from the amino acid tyrosine is a complex multistage process (governed by at least 13 genes) requiring at least eight vitamins and several trace elements and a deficiency of any of which can adversely affect the normal coenzyme Q10 (CoQ10) production 6, 7, 8. Furthermore, coenzyme Q10 (CoQ10) can be derived from your diet, about 5 mg/day for a Mediterranean diet 5. In particular coenzyme Q10 (CoQ10) is present in fatty fishes, soja, nuts, and spinach 9, however, coenzyme Q10 (CoQ10) intake may not be sufficient to counteract physiological or pathological deficiencies 10. Meat has the highest amount of coenzyme Q10 (CoQ10), followed by dairy, eggs, and plant-based food sources (oils and legumes). Coenzyme Q10 (CoQ10) extracted from living tissues is more expensive than produced in the laboratory by fermentation, yielding consistent quality and cheaper supplements 11. Furthermore, with the widespread consumption of nutrient-deficient fast foods and highly processed foods and the fact that nutritional content of our commercial food supply has been steadily declining since the end of World War II, due to the use of toxic chemicals, artificial fertilizers and other destructive farming practices, it is easy to see why many people have nutritional deficiencies that hinder the body’s ability to synthesize coenzyme Q10. For this reason, nutritional supplementation with coenzyme Q10 (CoQ10) could help to maintain adequate levels within your body.
The first ubiquinone was isolated in 1957 by a biochemist Fred Crane from the University of Wisconsin, who isolated a yellowish substance from beef hearts. He sent samples to a colleague, biochemist Dr. Karl Folkers who worked at the pharmaceutical company Merck, Sharpe and Dohme 8. In 1958, Dr. Folkers successfully determined the chemical structure of coenzyme Q10 and conducted some preliminary studies, which led him to believe that coenzyme Q10 had enormous potential as a cardiovascular drug. At the time, Merck executives were not interested in developing a new cardiovascular drug. Consequently, the patent rights to coenzyme Q10 were sold to a company in Japan. Since that time, ubiquinones have been studied extensively in Japan, Russia, and Europe, with research in the United States beginning more recently. In 1978, a British biochemist Peter Mitchell was awarded the Nobel Prize in Chemistry for discovering the key role Coenzyme Q10 plays in the electron transport chain in mitochondrial membranes, which results in the generation of cellular energy in the form of adenosine triphosphate (ATP) 12. Specifically, coenzyme Q10 facilitates the production of adenosine triphosphate (ATP), carrying the electrons from complexes I and II to complex III of the mitochondrial respiratory chain 13, 14. In addition, coenzyme Q10 is the major lipid-soluble antioxidant and it protects cell membranes and lipoproteins from oxidative damage 13. The antioxidant activity of coenzyme Q10 is linked to its reduced form, Ubiquinol, ability to reduce oxidative stress, lipid peroxidation, and regenerate also vitamins C and E back to their active fully reduced forms 15. Last but not least, some test tube studies have shown the ability of coenzyme Q10 to reduce the inflammatory markers, suggesting that coenzyme Q10 might have anti-inflammatory action through the regulation of gene expression 16, 17. However, some factors, such as aging, drugs (e.g., statins), genetic factors, neurodegenerative diseases, and degenerative muscle disorders, are well-known to be associated with reduced plasma concentrations of coenzyme Q10 (CoQ10), resulting in worsening of oxidative stress and inflammatory processes 15. This takes place through the upregulation of nuclear factor kappa-light-chain-enhancer of activated B (NF-κB) gene expression and chronic activation of immune inflammatory responses 18.
In the 1970s, Dr. Folkers and his colleague, Dr. Gian-Paolo Littarru of Italy published data they had collected with tissue biopsies from 200 patients, which revealed that patients with heart disease and patients undergoing heart surgery had blood and tissue Coenzyme Q10 levels significantly below normal levels 19. Due to Dr. Folkers’ early work along with Peter Mitchell’s Nobel prize dramatically increased scientific interest in coenzyme Q10 (CoQ10) around the world. Popular press accounts claim that roughly 12 million Japanese people use ubiquinones as the medication of choice for management of cardiovascular diseases, supplied via more than 250 commercially available preparations. Ubiquinone is touted as an effective treatment for congestive heart failure, heart arrhythmias, high blood pressure, and in reducing hypoxic injury to the myocardium. Other claims include increases in exercise tolerance, stimulation of the immune system, and counteraction of the aging process. Ubiquinone has not been approved by the United States Food and Drug Administration (FDA) for treating any medical condition or therapeutic use; however, it is available as a food supplement 1, 2. While not approved by the FDA for these indications, ubiquinone (coenzyme Q10) has been used for heart attack (acute myocardial infarction), AIDS, Alzheimer’s disease, angina (chest pain or discomfort caused by a lack of blood and oxygen flow to the heart muscle, most commonly due to coronary artery disease), breast cancer, cardiomyopathy (heart muscle disease that weakens the heart’s ability to pump blood throughout the body, leading to potential heart failure), heart protection during surgery, congestive heart failure, exercise performance, high blood pressure, migraine, mitochondrial disease, Kearns-Sayre syndrome, muscular dystrophy, Parkinson’s disease, periodontal disease (an infection of the gums and supporting bone that is caused by plaque), and kidney failure.
Ubiquinone, the oxidized form of coenzyme Q10, is soluble in lipids (fats) and is found in virtually all cell membranes, including mitochondrial membranes. The ability of the benzoquinone head group of coenzyme Q10 to accept and donate electrons is a critical feature to its function. Ubiquinone (oxidized form of coenzyme Q10) plays an essential role in the mitochondrial oxidative phosphorylation as an electron shuttle between complexes I and II of the respiratory chain, and complex III and the production of adenosine triphosphate (ATP). Ubiquinone, the oxidized form of coenzyme Q10, is required for energy production in the mitochondria of all cells except the red blood cells. Specifically, Ubiquinone is required in several steps of the electron transport chain in mitochondrial inner membranes, which is where cellular energy, known as adenosine triphosphate (ATP), is produced. This is the work that earned Peter Mitchell his 1978 Nobel Prize 12. Ubiquinone also functions as a cofactor of other dehydrogenases, a modulator of the permeability transition pore and an essential antioxidant in cell membranes and lipoproteins. While normally synthesized in the body in adequate amounts, coenzyme Q10 is used as a nutritional supplement for conditions highly dependent upon its actions, some of which are associated with low serum levels of the coenzyme.
A coenzyme Q10 deficiency occurs with age; ubiquinone decreases in the body as people get older due to increased requirements, decreased production or insufficient intake of the chemical precursors needed for coenzyme Q10 synthesis 3, 20. Furthermore, certain drugs can cause depletion of coenzyme Q10 levels, particularly hydroxy-methylglutaryl-coenzyme A (HMG-CoA) reductase inhibitors, or statins 21. Statins are prescribed to reduce cholesterol levels and work by inhibiting HMG-CoA reductase and the mevalonate metabolic pathway 22. Mevalonate is used to synthesize cholesterol as well as coenzyme Q10 23, therefore, when statin drugs lower cholesterol levels they simultaneously lower coenzyme Q10 levels. Statins are known to block coenzyme Q10 biosynthesis and reduce serum concentrations of coenzyme Q10 by up to 40% 24. Statin use is often associated with a variety of muscle-related symptoms or myopathies. Research has suggested that coenzyme Q10 supplementation may decrease muscle pain associated with statin treatment 25.
Your body uses coenzyme Q10 to make energy needed for the cells to grow and stay healthy. Your body also uses Coenzyme Q10 as an antioxidant 26, 27, 28, 29, 30. An antioxidant is a substance that protects cells from free radicals, which are highly reactive chemicals, often containing oxygen atoms, capable of damaging important cellular components such as DNA and lipids. In addition, the plasma level of coenzyme Q10 has been used in studies as a measure of oxidative stress 31, 32. Conditions such as fibromyalgia, diabetes, cancer, heart failure, and neurodegenerative, mitochondrial, and muscular diseases are associated with decreased circulating levels of Coenzyme Q10 (CoQ10) 33, 34, 35, 36, 37, 38. Several studies have been conducted to determine whether increasing systemic coenzyme Q10 levels would enhance bodily function 39, 40, 41.
Coenzyme Q10 is sold in the United States as a dietary supplement. Supplementary oral administration of coenzyme Q10 has been shown to increase coenzyme Q10 levels in plasma, platelets, and white blood cells 42. Because CoQ10 has important functions in the body and because people with some diseases have reduced levels of this substance, researchers have been interested in finding out whether CoQ10 supplements might have health benefits. Studies suggest that CoQ10 deficiency may be associated with a multitude of diseases as diverse as coronary artery disease and congestive heart failure, Parkinson’s disease, diabetes, and breast cancer, as well as the risk factor, hypertension 42. It has been suggested that Coenzyme Q10 has the potential to lower blood pressure without significant adverse events in hypertensive patients 43.
There are also a number of ways that coenzyme Q10 could act favorably to reduce blood pressure. Coenzyme Q10 could act directly on vascular endothelium and decrease total peripheral resistance by acting as an antagonist of vascular superoxide, by either scavenging it, or suppressing its synthesis 44. Further to this, a recent meta-analysis has associated CoQ10 supplementation with a significant improvement in arterial endothelial function in patients with and without cardiovascular disease 45. Coenzyme Q10’s antioxidant properties may also result in the quenching of free radicals that cause inactivation of endothelium-derived relaxing factor or fibrosis of arteriolar smooth muscle, or both 46. In addition, CoQ10 has been found to decrease blood viscosity and improve blood flow to cardiac muscle in patients with ischemic heart disease; therefore it may reduce blood pressure 47.
Dietary supplementation with coenzyme Q10 results in increased levels of Ubiquinol (the reduced form of coenzyme Q10) within circulating lipoproteins. In its reduced form the coenzyme Q10 molecule acts as a powerful intracellular antioxidant due to its ability to hold electrons rather loosely, and will quite easily give up one or both electrons. The antioxidant and free radical scavenger effects of coenzyme Q10 can therefore help to prevent lipid peroxidation and thus the progression of atherosclerosis 24. Furthermore, coenzyme Q10 has also been found to modulate the amount of ß-integrin levels on the surface of blood monocytes, strongly suggesting that the anti-atherogenic effects of coenzyme Q10 are mediated by other mechanisms beside its antioxidant properties 48.
According to 2022 American College of Cardiology/American Heart Association/The Heart Failure Society of America guidelines for the Management of Heart Failure recommended supplementation with coenzyme Q10 effectively reduced vascular mortality, all-cause mortality, and hospital stays for heart failure at 2 years 49. However, long-term supplementation is needed 49.
A recently published systematic review showed that supplementation with coenzyme Q10, in addition to standard therapy in patients with moderate-to-severe heart failure, is associated with symptom reduction and reduction of major adverse cardiovascular events 40, 50. CoQ10 may improve functional capacity, endothelial function, and left ventricle contractility in congestive heart failure patients 40, 51.
Coenzyme Q10 supplementation shows promising results in improving endothelial function in several subsets of patients. CoQ10 can improve endothelial function in patients with ischemic left ventricular systolic dysfunction and heart failure 52, 53. Likewise, compared with placebo, CoQ10 improves endothelial function in the peripheral circulation of patients with type 2 diabetes and hyperlipidemia 54. However, routine use of CoQ10 in patients with coronary artery disease apart from congestive heart failure is still inconclusive 52, 55.
There is also evidence that combined with selenium, CoQ10 supplementation in healthy older patients and older patients with diabetes, hypertension, and ischemic heart disease may decrease cardiovascular mortality risk 56. Data are conflicting on whether CoQ10 may play a role in treating high blood pressure 57. Coenzyme Q10 shows the potential to decrease pain, fatigue, and morning tiredness compared to a placebo in patients with fibromyalgia 58, 59. Some data suggest that supplementation with moderate-to-high dose coenzyme Q10 may influence bicycle exercise aerobic capacity in patients with mitochondrial disorders 60.
Supplementation with coenzyme Q10 300 mg daily for 24 weeks in men with Peyronie disease may decrease penile plaque size, reduce penile curvature, and improve erectile function 61. Statin drugs inhibit the production of an intermediate in the mevalonate pathway—a biochemical route leading to CoQ10 synthesis 62. Therefore, many researchers theorize that statin drugs may contribute to coenzyme Q10 depletion in the body. Given that muscle pain and cramping are frequent side effects of statins, they attribute these symptoms to the diminished levels of coenzyme Q10 63.
Although most studies have used patients with preexisting medical conditions, one study of healthy participants did show that oral coenzyme Q10 supplementation improved fatigue and physical performance during bicycle exercise routines 64.
Coenzyme Q10 has also shown promise in migraine prevention 35. A cohort study of 1550 children and adolescents with headaches found that this population has low coenzyme Q10 levels 65. Coenzyme Q10 supplementation appeared to decrease headache frequency 35 A recent study indicated that CoQ10 is beneficial for the prophylactic treatment of migraine headaches in children without significant adverse effects 66. A double-blind, randomized controlled trial showed Coenzyme Q10 300 mg daily to be safe and superior to a placebo for migraine prevention 67. Another randomized, double-blind, placebo-controlled trial in adult women showed that Coenzyme Q10 400 mg of supplementation decreased migraine frequency, severity, and duration 35. One study showed that only Coenzyme Q10 100 mg daily reduced the severity of headaches and the number of headaches per month in migraine sufferers 68.
Interestingly, CoQ10 levels may be decreased in those with acute influenza infection 69. However, studies on coenzyme Q10 supplementation in patients with acute influenza have yet to be done.
Coenzyme Q10 supplemented alongside standard psychiatric medical therapy appears to lessen symptoms of depression in patients with bipolar disorder 70. In patients with polycystic ovary syndrome (PCOS), Coenzyme Q10 supplementation may improve fasting blood glucose, insulin levels, and total testosterone levels 71.
Figure 1. Coenzyme Q10
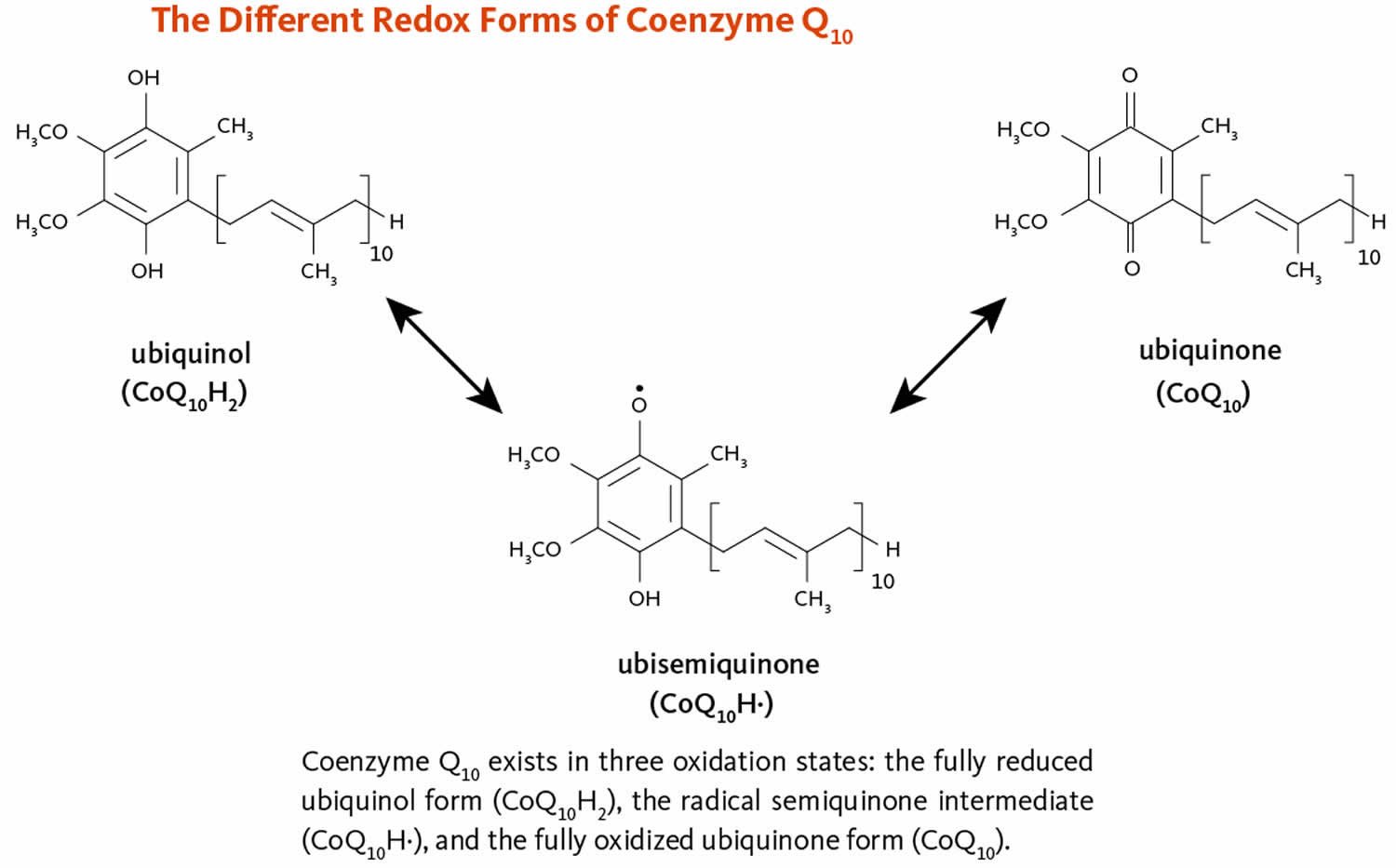
Footnotes: Coenzyme Q10 exists in 3 oxidation states. The fully oxidized form of coenzyme-Q10 called Ubiquinone. The fully reduced form of coenzyme-Q10 called Ubiquinol. And the intermediate form of oenzyme-Q10 is called Ubisemiquinone. Ubiquinone (oxidized form of coenzyme-Q10) is mainly acknowledged as the key cofactor for mitochondrial enzyme complexes and Ubiquinol (reduced form of coenzyme-Q10) is a potent antioxidant and both functions make coenzyme Q10 especially attractive for healthcare providers 8. Ubiquinone and ubiquinol are a redox pair (oxidation-reduction) that can be rapidly converted from one form to the other in cells, lymph or blood depending on the demand for their various functions. When ubiquinone is taken orally, it is converted to ubiquinol during absorption and remains in its reduced form in the lymph and in blood. Ubiquinone is not needed to produce energy when it is circulating in the lymph or blood. This conversion takes place so that reduced ubiquinol form of coenzyme-Q10 can provide antioxidant protection as it is being circulated throughout the body.
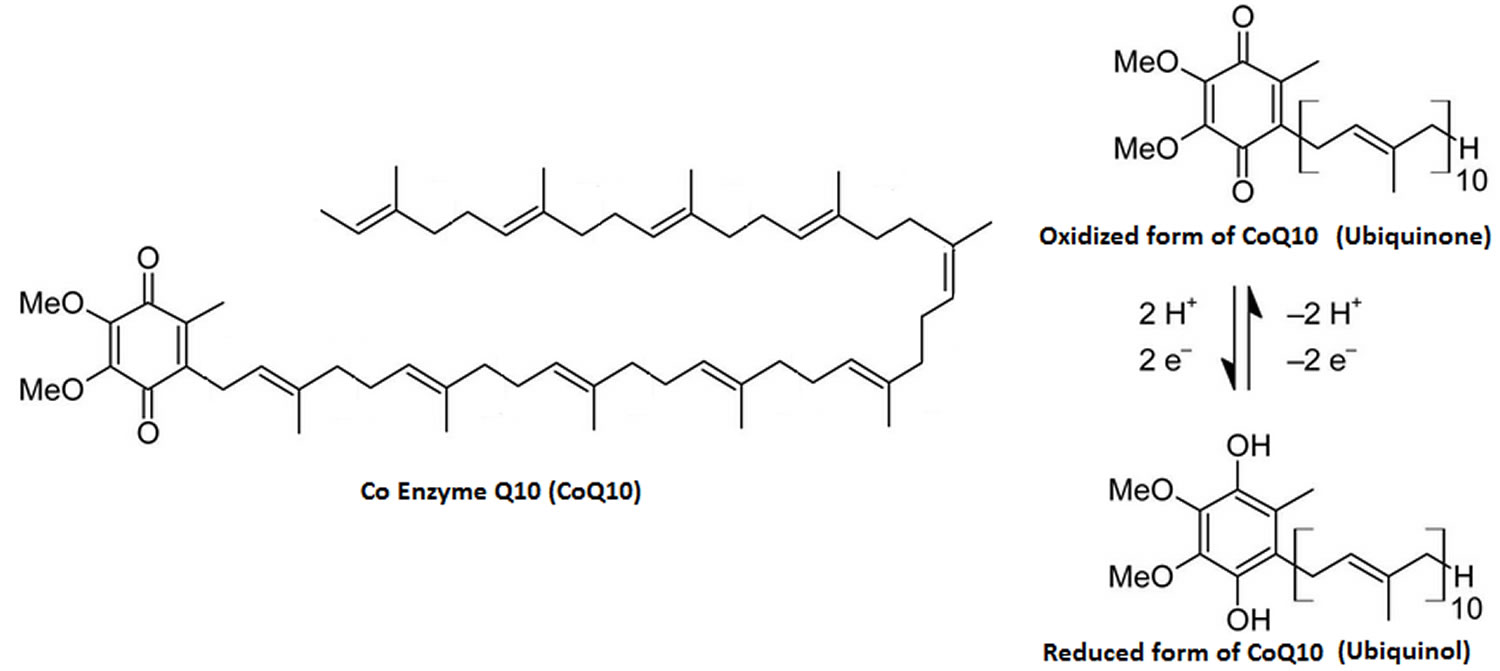
[Source 72 ]Figure 2. Ubiquinone (oxidized form of Coenzyme Q10)
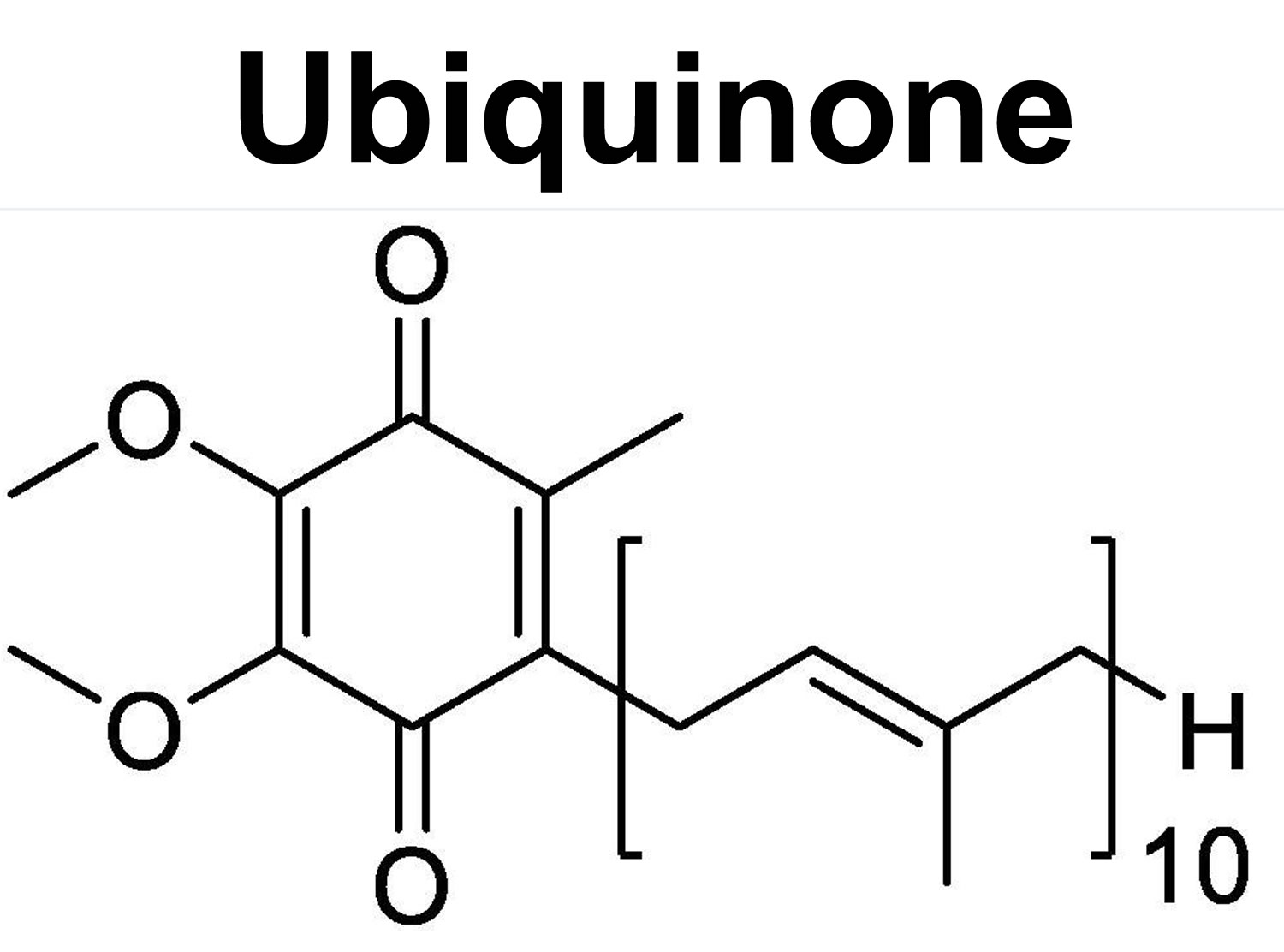
Figure 3. Ubiquinol (reduced form of Coenzyme Q10)

Figure 4. The role of coenzyme Q10 (CoQ10) in mitochondrial electron transport chain (ETC)
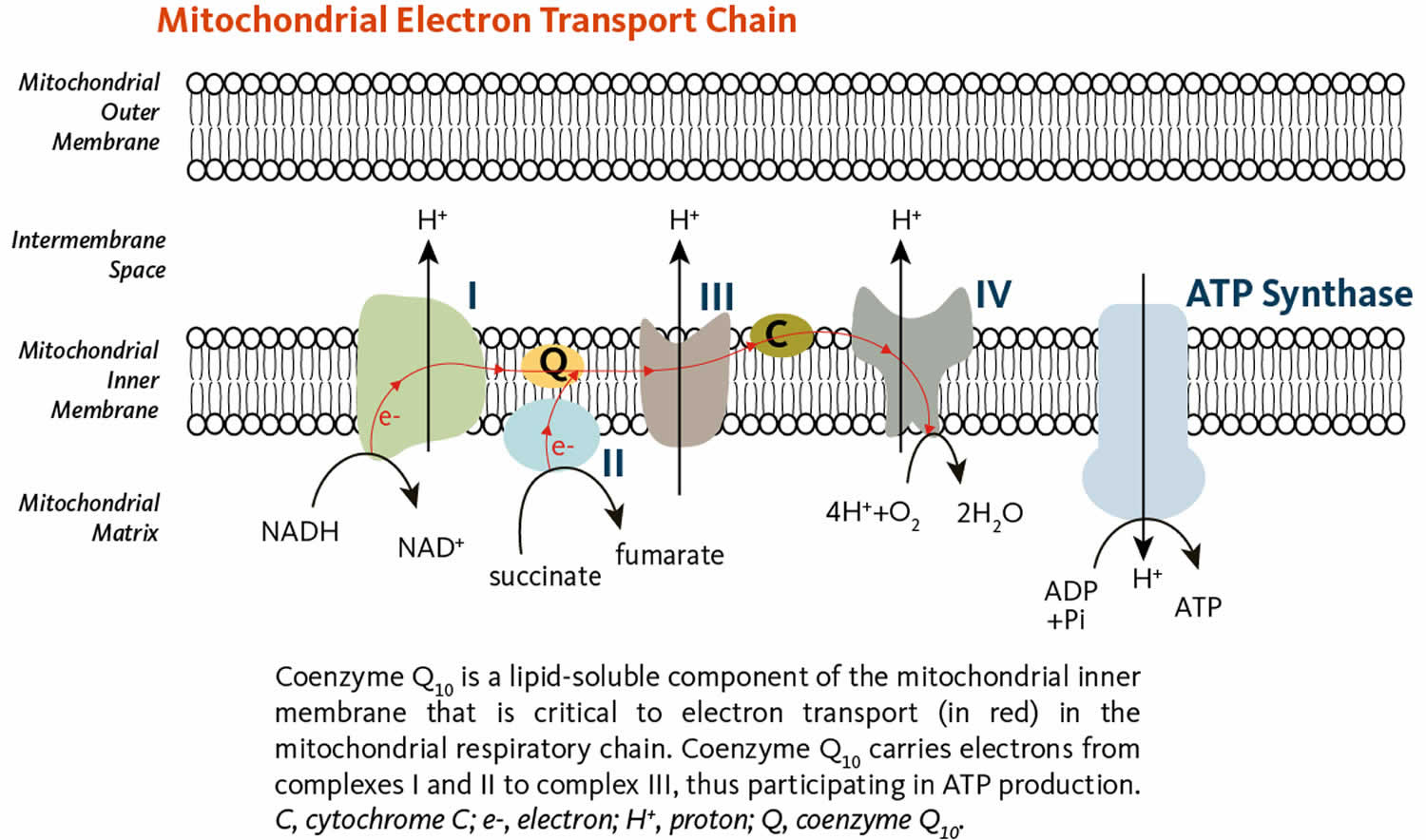
Table 1. Ubiquinone and Ubiquinol distribution in human tissues
| Organ | Ubiquinone Concentration (µg/g) | Ubiquinol Concentration (µg/g) |
|---|---|---|
| Heart | 132 | 61 |
| Kidneys | 77 | 75 |
| Liver | 63.6 | 95 |
| Muscle | 39.7 | 65 |
| Brain | 13.4 | 23 |
| Pancreas | 32.7 | |
| Spleen | 24.6 | |
| Lung | 7.9 | 25 |
| Thyroid | 24.7 | |
| Testis | 10.5 | |
| Intestine | 11.5 | 95 |
| Colon | 10.7 | |
| Ventricle | 11.8 | |
| Plasma (µmol/mL) | 1.1 | 96 |
Coenzyme Q10 (CoQ10) key facts
- Coenzyme Q10 (CoQ10) is made naturally by the human body. Coenzyme Q10 is present in most tissues, but the highest concentrations are found in the following organs 3:
- Heart
- Liver
- Kidneys
- Pancreas
- The lowest coenzyme Q10 concentration is found in the lungs 3. Tissue levels of coenzyme Q10 decrease as people age, due to increased requirements, decreased production, or insufficient intake of the chemical precursors needed for synthesis 3, 20. In humans, normal blood levels of coenzyme Q10 have been defined variably, with reported normal values ranging from 0.30 to 3.84 µg/mL 74, 75, 32, 76.
- Coenzyme Q10 helps cells to produce energy (adenosine triphosphate [ATP]), and it acts as an antioxidant 74, 77, 78, 79, 80, 81.
- Coenzyme Q10 (CoQ10) is marketed in the United States as a dietary supplement. In human studies, coenzyme Q10 supplementation doses and administration schedules have varied, but usually have been in the range of 90 to 390 mg/day. In humans, coenzyme Q10 is usually taken orally as a pill (gel bead or capsule), but intravenous infusions have been given 75. Coenzyme Q10 is absorbed best with fat; therefore, lipid preparations are better absorbed than the purified compound 75, 74.
- Coenzyme Q10 (CoQ10) has not been shown to be of value in treating cancer 82, 83.
- Low blood levels of coenzyme Q10 have been detected in patients with some types of cancer. However, no report of a randomized clinical trial of coenzyme Q10 as a treatment for cancer has been published in a peer-reviewed scientific journal 82, 83.
- Coenzyme Q10 has shown an ability to stimulate the immune system and to protect the heart from damage caused by certain chemotherapy drugs (anthracyclines family of chemotherapy drugs) 82. Coenzyme Q10 (CoQ10) may reduce the risk of heart damage caused by cancer chemotherapy drug doxorubicin 78, 27, 28, 29. It has been postulated that doxorubicin interferes with energy-generating biochemical reactions that involve coenzyme Q10 in heart muscle mitochondria and that this interference can be overcome by coenzyme Q10 supplementation 84. Studies with adults and children have confirmed the decrease in heart toxicity observed in animal studies 79, 74, 85, 80. A randomized trial of 20 patients tested the ability of coenzyme Q10 to reduce heart toxicity (cardiotoxicity) caused by chemotherapy drug doxorubicin 27, 28, 29.
- Coenzyme Q10 (CoQ10) supplements might be beneficial for treating congestive heart failure 40. The 2022 American College of Cardiology/American Heart Association/The Heart Failure Society of America guidelines for the Management of Heart Failure recommended supplementation with coenzyme Q10 effectively reduced vascular mortality, all-cause mortality, and hospital stays for heart failure at 2 years 49. However, long-term supplementation is needed 49.
- Although findings are mixed, Coenzyme Q10 (CoQ10) might help reduce blood pressure 57. Some research also suggests that when combined with other nutrients, CoQ10 might aid recovery in people who’ve had bypass and heart valve surgeries.
- Although more studies are needed, some research suggests that Coenzyme Q10 (CoQ10) may help reduce low-density lipoprotein (LDL) cholesterol and total cholesterol levels in people with diabetes, lowering their risk of heart disease.
- Some research suggests that Coenzyme Q10 (CoQ10) might help ease the muscle weakness and pain sometimes associated with taking statins. Supplementation with 50 mg twice daily has decreased statin-related mild-to-moderate myalgias, resulting in an increased ability to perform daily activities 63. The meta-analysis of randomized controlled trials indicated that CoQ10 supplementation (100 to 600 mg/day) decreased the Statin-Associated Muscle Symptoms (SAMS) 86.
- Recent research suggests that even high doses of Coenzyme Q10 (CoQ10) don’t seem to improve symptoms in people with Parkinson’s disease. A major study showed that coenzyme Q10, even in higher-than-usual doses, didn’t improve symptoms in patients with early Parkinson’s disease. A 2017 evaluation of this study and several other, smaller studies concluded that coenzyme Q10 is not helpful for Parkinson’s symptoms.
- Guidelines from the American Academy of Neurology and the American Headache Society say that cCoenzyme Q10 (CoQ10) is “possibly effective” in preventing migraines, but this conclusion is based on limited evidence. Some research suggests that CoQ10 might decrease the frequency of these headaches. A double-blind, randomized controlled trial showed Coenzyme Q10 300 mg daily to be safe and superior to a placebo for migraine prevention 67. Another randomized, double-blind, placebo-controlled trial in adult women showed that Coenzyme Q10 400 mg of supplementation decreased migraine frequency, severity, and duration 35. One study showed that only Coenzyme Q10 100 mg daily reduced the severity of headaches and the number of headaches per month in migraine sufferers 68.
- Because Coenzyme Q10 (CoQ10) is involved in energy production, it’s believed that this supplement might improve your physical performance. However, research in this area has produced mixed results.
- Coenzyme Q10 (CoQ10) has also been studied for a variety of other conditions, including amyotrophic lateral sclerosis (Lou Gehrig’s disease), Down syndrome, Huntington’s disease, and male infertility, but the research is too limited for any conclusions to be drawn.
Ubiquinone Food sources
It has been estimated that dietary consumption contributes to about 25% of plasma coenzyme Q10, but there are currently no specific dietary intake recommendations for coenzyme Q10 from the US National Academy of Medicine or other agencies 87. The extent to which dietary coenzyme Q10 consumption contributes to tissue coenzyme Q10 concentrations is not clear.
Based on studies employing food frequency questionnaires, the average dietary intake of coenzyme Q10 is about 3 to 6 mg/day 88. Rich sources of dietary coenzyme Q10 include mainly meat, poultry, and fish. Other good sources include soybean, corn, olive, and canola oils; nuts; and seeds. Fruit, vegetables, eggs, and dairy products are moderate sources of coenzyme Q10 88. Some dietary sources are listed in Table 2.
Table 2. Ubiquinone Food sources
| Food | Serving | Coenzyme Q10 (mg) |
|---|---|---|
| Beef, fried | 3 ounces* | 2.6 |
| Herring, marinated | 3 ounces | 2.3 |
| Chicken, fried | 3 ounces | 1.4 |
| Soybean oil | 1 tablespoon | 1.3 |
| Canola oil | 1 tablespoon | 1.0 |
| Rainbow trout, steamed | 3 ounces | 0.9 |
| Peanuts, roasted | 1 ounce | 0.8 |
| Sesame seeds, roasted | 1 ounce | 0.7 |
| Pistachio nuts, roasted | 1 ounce | 0.6 |
| Broccoli, boiled | ½ cup, chopped | 0.5 |
| Cauliflower, boiled | ½ cup, chopped | 0.4 |
| Orange | 1 medium | 0.3 |
| Strawberries | ½ cup | 0.1 |
| Egg, boiled | 1 medium | 0.1 |
Footnotes: * A three-ounce serving of meat or fish is about the size of a deck of cards.
[Source 72 ]Ubiquinone mechanism of action
Ubiquinone also called coenzyme Q10 (CoQ10) is a lipid-soluble benzoquinone that has 10 isoprenyl units in its side chain and is a key component of the mitochondrial respiratory chain for adenosine triphosphate (ATP) synthesis by acting as an electron carrier in mitochondria and as a co-enzyme for mitochondrial enzymes 89, 90. In cell membranes, coenzyme Q10 acts as an antioxidant, protecting cells from damage caused by unstable oxygen-containing molecules (free radicals), which are byproducts of energy production. Studies have indicated that coenzyme Q10 (CoQ10) is also an intracellular antioxidant that can protects membrane phospholipids, mitochondrial membrane protein, and low density lipoprotein-cholesterol (LDL-C) from free radical-induced oxidative damage 91. Coenzyme Q10 can potentially increase the production of vital antioxidants, such as superoxide dismutase, an enzyme that effectively reduces vascular oxidative stress in individuals with high blood pressure 92. In addition, coenzyme Q10 (CoQ10) lowers lipid peroxidation levels by diminishing pro-oxidative compounds 93. Furthermore, coenzyme Q10 can improve blood flow and safeguard blood vessels by preserving nitric oxide.
Coenzyme Q10 is used by cells of your body in a process known variously as 84:
- Aerobic respiration: A chemical process in which oxygen is used to make energy from carbohydrates (sugars). Also called aerobic metabolism, cell respiration, and oxidative metabolism.
- Aerobic metabolism: A chemical process in which oxygen is used to make energy from carbohydrates (sugars). Also called aerobic respiration, cell respiration, and oxidative metabolism.
- Oxidative metabolism: A chemical process in which oxygen is used to make energy from carbohydrates (sugars). Also called aerobic metabolism, aerobic respiration, and cell respiration
- Cell respiration: A chemical process in which oxygen is used to make energy from carbohydrates (sugars). Also called aerobic metabolism, aerobic respiration, and oxidative metabolism.
The “Q” and the “10” in Coenzyme Q10 refer to the quinone chemical group and the 10 isoprenyl subunits that are part of this compound’s structure 84. The term “coenzyme” denotes it as an organic (meaning it contains carbon atoms) nonprotein molecule necessary for the proper functioning of its protein partner (an enzyme or an enzyme complex) 84.
Ubiquinones participate in oxidation-reduction reactions in the mitochondrial respiratory chain. Ubiquinones also have properties of hydrogen carriers, providing a coupling of proton translocation to respiration by means of a chemiosmotic mechanism. Ubiquinol (the reduced form of ubiquinone), present in all cellular membranes, is a recognized antioxidant that can reduce oxidized tocopherol and ascorbate after free radicals have been removed. Other membrane-related functions have been identified for coenzyme Q10, including the activation of the sodium/hydrogen ion antiporter, apoptosis control, and nicotinamide adenine dinucleotide/nicotinamide/adenine dinucleotide hydrogen ratio control. Reviews of the actions of coenzymes have been published 2, 94.
Test tube and animal studies have demonstrated that coenzyme Q10 (CoQ10) not only plays an antioxidant, but also has anti-inflammation effects by modulating the expression of cyclooxygenase-2 and nuclear factor-κB (NF-κB) in the liver tissue of rats with hepatocellular carcinoma 95, 96.
Mitochondrial ATP synthesis
Coenzyme Q10 (CoQ10) is crucial for efficiently transferring electrons within the mitochondrial oxidative respiratory chain and producing adenosine triphosphate (ATP), which is a packet of energy for cell growth and maintenance 97, 26, 27, 98, 99. The conversion of energy from carbohydrates and fats to adenosine triphosphate (ATP), the form of energy used by cells, requires the presence of coenzyme Q10 (CoQ10) in the inner mitochondrial membrane 72. As part of the mitochondrial electron transport chain (ETC), coenzyme Q10 accepts electrons from reducing equivalents generated during fatty acid and glucose metabolism and then transfers them to electron acceptors 72. At the same time, coenzyme Q10 contributes to transfer protons (H+) from the mitochondrial matrix to the intermembrane space, creating a proton gradient across the inner mitochondrial membrane 72. The energy released when the protons flow back into the mitochondrial interior is used to form ATP (Figure 4) 100. In addition to coenzyme Q10 (CoQ10) role in ATP synthesis, mitochondrial coenzyme Q10 mediates the oxidation of dihydroorotate to orotate in the pyrimidine synthesis, which are building blocks of DNA, its chemical cousin RNA, and molecules such as ATP and GTP that serve as energy sources in the cell 72.
Lysosomal function
Lysosomes are organelles within cells that are specialized for the digestion of cellular debris. The digestive enzymes within lysosomes function optimally at an acidic pH, meaning they require a permanent supply of protons. The lysosomal membranes that separate those digestive enzymes from the rest of the cell contain relatively high concentrations of coenzyme Q10. Research suggests that coenzyme Q10 plays an important role in the transport of protons across lysosomal membranes to maintain the optimal pH 101, 102.
Antioxidant functions
Antioxidants protect cells from the damaging effects of free radicals, which are molecules that contain an unshared electron. Free radicals damage cells and might contribute to the development of cardiovascular disease and cancer 103. Unshared electrons are highly energetic and react rapidly with oxygen to form reactive oxygen species (ROS). Your body forms reactive oxygen species (ROS) endogenously when it converts food to energy, and antioxidants might protect cells from the damaging effects of reactive oxygen species (ROS). Your body is also exposed to free radicals from environmental exposures, such as cigarette smoke, air pollution, and ultraviolet radiation from the sun. Reactive oxygen species (ROS) are part of signaling mechanisms among cells.
Ubiquinol, a fully reduced form of coenzyme Q10, is an effective fat-soluble antioxidant that protects cell membranes and lipoproteins from oxidation 72. The presence of a significant amount of ubiquinol in cell membranes, along with enzymes capable of reducing oxidized coenzyme Q10 (ubiquinone) back to ubiquinol (i.e., NAD(P)H oxidoreductases), supports the idea that ubiquinol is an important cellular antioxidant 104. Ubiquinol (reduced form of coenzyme Q10) has been found to inhibit lipid peroxidation when cell membranes and low-density lipoproteins (LDL) are exposed to oxidizing conditions. When LDL is oxidized, Ubiquinol is the first antioxidant consumed. In isolated mitochondria, coenzyme Q10 can protect membrane proteins and mitochondrial DNA from the oxidative damage that accompanies lipid peroxidation 81. Furthermore, when present, Ubiquinol was found to limit the formation of oxidized lipids and the consumption of alpha-tocopherol (a form of vitamin E with antioxidant properties) 105. In addition to neutralizing free radicals directly, Ubiquinol is capable of regenerating antioxidants like alpha-tocopherol and ascorbate (vitamin C) 104. Finally, the role of coenzyme Q10 as an antioxidant is also exemplified by recent evidence showing that mitochondrial coenzyme Q10 deficiency causes an increased production of mitochondrial superoxide radical anion (O2–) which might be driving insulin resistance in fatty (adipose) and muscle tissues 106.
Pharmacokinetics
Absorption: Coenzyme Q10 (CoQ10) is a lipophilic molecule (“fat-loving” meaning it can dissolve in or be attracted to lipids [fats]) with a high molecular weight; absorption of dietary coenzyme Q10 is slow but is improved in the presence of fatty meals. Solubilized coenzyme Q10 formulations provide improved bioavailability, with peak plasma concentrations typically ranging from 5.80 to 8.10 hours, depending on the specific formulation. Various formulations such as liposome, nanocapsule, and nanoemulsion are being explored to improve bioavailability. A second plasma peak may also be observed due to the enterohepatic recycling and redistribution from the liver to the circulation.
Distribution: Coenzyme Q10 (CoQ10) is primarily absorbed from the small intestine, and coenzyme Q10 is incorporated into chylomicrons and is redistributed via the bloodstream, primarily within VLDL, LDL, and HDL. Preclinical studies indicate that coenzyme Q10 in large doses is taken up by all tissues, including heart and brain mitochondria; consequently, a beneficial effect is observed in cardiovascular and neurodegenerative diseases. The highest levels of coenzyme Q10 in human tissues exist in the heart, liver, kidneys, and muscles (high energy requirements) 107.
Metabolism: Coenzyme Q10 (CoQ10) is metabolized (broken down) in all tissues, and the resulting metabolites are phosphorylated in the cells and transported through the plasma. Coenzyme Q10 is reduced to Ubiquinol during or after absorption in the small intestine, and the reduced form (Ubiquinol) represents approximately 95% of the circulating coenzyme Q10 in humans.
Elimination: The primary route of coenzyme Q10 elimination is biliary and fecal. A small fraction of coenzyme Q10 is eliminated in the urine 73.
Ubiquinone vs Ubiquinol
Coenzyme Q10 (CoQ10) is poorly absorbed because of its lipophilic nature (“fat-loving” or “fat-soluble” meaning it can dissolve in or be attracted to lipids [fats]) and its high molecular weight. In 2006, Kaneka Corporation in Japan began marketing the Ubiquinol (reduced form of coenzyme Q10) with claims that it was better absorbed than Ubiquinone (oxidized form of coenzyme-Q10) and hence, more effective. This has been a very successful marketing strategy for Kaneka, but actually, the claims are not scientifically accurate.
Ubiquinol products are substantially more expensive than Ubiquinone products. However, when ubiquinol is ingested, it is oxidized by gastric acid to ubiquinone before it is absorbed 8. Hence, people pay more for ubiquinol, but really do not get added benefit(s) 8. Research has shown that it is not necessary to take ubiquinol in order to significantly increase ubiquinol levels in plasma and in plasma lipoproteins. Taking a ubiquinone supplement will do the same 8.
Coenzyme Q10 deficiency
Coenzyme Q10 deficiency has not been described in the general population, so it is generally assumed that normal coenzyme Q10 biosynthesis, with or without a varied diet, provides sufficient coenzyme Q10 to sustain energy production in healthy individuals 75. Coenzyme Q10 concentrations have been found to decline gradually with age in a number of different tissues, but it is unclear whether this age-associated decline constitutes a coenzyme Q10 deficiency 81, 108, 109. Decreased plasma coenzyme Q10 concentrations have been observed in individuals with diabetes mellitus, cancer, and congestive heart failure. Lipid-lowering medications that inhibit the activity of 3-hydroxy-3-methylglutaryl (HMG)-coenzyme A (CoA) reductase (statins), a critical enzyme in both cholesterol and coenzyme Q10 biosynthesis, decrease plasma coenzyme Q10 concentrations, although it remains unproven that this has any clinical implications 72.
Coenzyme Q10 deficiency can be Primary coenzyme Q10 deficiency, a rare autosomal recessive disorder caused by COQ genes mutations involved in coenzyme Q10 biosynthesis. Or Secondary coenzyme Q10 deficiency that results from mutations or deletions in genes that are not directly related to coenzyme Q10 biosynthetic pathway 110, 72. Secondary coenzyme Q10 deficiency has been described in patients with mitochondrial DNA (mtDNA) mutations or deletions, with mitochondrial DNA depletion syndrome, Kearns-Sayre syndrome, or multiple acyl-CoA dehydrogenase deficiency (MADD) and in patients with mutations in APTX, ETFDH, BRAF, ACADVL or NPC genes 111, 112, 113, 114, 115, 116, 117, 118, 119.
Primary Coenzyme Q10 deficiency
Primary Coenzyme Q10 deficiency is a rare autosomal recessive disorder caused by COQ genes mutations that provide instructions for making proteins involved in the production (synthesis) of coenzyme Q10 with clinical features of steroid-resistant nephrotic syndrome (SRNS), optic atrophy, retinopathy, and encephalopathy 120, 121. To date, mutations in at least nine COQ genes have been identified 120. Most of the identified mutations have occurred in the COQ2, COQ4, COQ6, COQ8A, and COQ8B genes 122. Smaller numbers of mutations in other COQ genes have also been found to cause primary coenzyme Q10 deficiency 122. Coenzyme Q10 deficiency can also be caused by mutations in genes that are not directly related to the synthesis of coenzyme Q10. In these cases, the condition is referred to as secondary coenzyme Q10 deficiency. Secondary coenzyme Q10 deficiency is a common feature of certain other genetic conditions.
As noted above, coenzyme Q10 has several critical functions in cells throughout the body. In cell structures called mitochondria, coenzyme Q10 plays an essential role in a process called oxidative phosphorylation, which converts the energy from food into a form cells can use. Coenzyme Q10 is also involved in producing pyrimidines, which are building blocks of DNA, its chemical cousin RNA, and molecules such as ATP and GTP that serve as energy sources in the cell. In cell membranes, coenzyme Q10 acts as an antioxidant, protecting cells from damage caused by unstable oxygen-containing molecules (free radicals), which are byproducts of energy production.
Some mutations in the COQ genes greatly reduce or eliminate the production of the corresponding proteins; others change the structure of a protein, impairing its function. A lack of functional protein produced from any one of the COQ genes decreases the normal production of coenzyme Q10. Studies suggest that a deficiency of coenzyme Q10 impairs oxidative phosphorylation and increases the vulnerability of cells to damage from free radicals. A deficiency of coenzyme Q10 may also disrupt the production of pyrimidines. These changes can cause cells throughout the body to malfunction, which may help explain the variety of organs and tissues that can be affected by primary coenzyme Q10 deficiency.
As a result, primary coenzyme Q10 deficiency is a clinically heterogeneous disorder that includes five major clinical features 72:
- Severe infantile multi-systemic disease
- Encephalomyopathy
- Cerebellar ataxia
- Isolated myopathy
- Nephrotic syndrome (steroid-resistant nephrotic syndrome). Steroid-resistant nephrotic syndrome (SRNS), an unusual feature of mitochondrial disorders, is a hallmark of primary coenzyme Q10 deficiency. If not treated with supplementation of high-dose oral coenzyme Q10 (20 mg/kg), steroid-resistant nephrotic syndrome (SRNS) usually progresses to irreversible kidney failure (end-stage renal disease).
Primary coenzyme Q10 deficiency can affect many parts of the body, especially the brain, muscles, and kidneys. The severity, combination of signs and symptoms, and age of onset of primary coenzyme Q10 deficiency vary widely. In the most severe cases, the condition becomes apparent in infancy and causes severe brain dysfunction combined with muscle weakness (encephalomyopathy) and the failure of other body systems. These problems can be life-threatening. The mildest cases of primary coenzyme Q10 deficiency can begin as late as a person’s sixties and often cause cerebellar ataxia, which refers to problems with coordination and balance due to defects in the part of the brain that is involved in coordinating movement (cerebellum) 122. Other neurological abnormalities that can occur in primary coenzyme Q10 deficiency include seizures, intellectual disability, poor muscle tone (hypotonia), involuntary muscle contractions (dystonia), progressive muscle stiffness (spasticity), abnormal eye movements (nystagmus), vision loss caused by degeneration (atrophy) of the optic nerves or breakdown of the light-sensing tissue at the back of the eyes (retinopathy), and sensorineural hearing loss, which is caused by abnormalities in the inner ear 122. The neurological problems gradually get worse unless treated with coenzyme Q10 supplementation. Unlike other most mitochondrial diseases, oral coenzyme Q10 supplementation has been shown to improve muscular symptoms in some (yet not all) patients with primary coenzyme Q10 deficiency 111. Neurological symptoms in patients with cerebellar ataxia are only partially relieved by Ubiquinol supplementation 111.
A type of heart disease that enlarges and weakens the heart muscle (hypertrophic cardiomyopathy) can also occur in primary coenzyme Q10 deficiency.
A type of kidney dysfunction called nephrotic syndrome is another common feature of primary coenzyme Q10 deficiency 122. It can occur with or without neurological abnormalities. Nephrotic syndrome occurs when damage to the kidneys impairs their function, which allows protein from the blood to pass into the urine (proteinuria). Other signs and symptoms of nephrotic syndrome include increased cholesterol in the blood (hypercholesterolemia), an abnormal buildup of fluid in the abdominal cavity (ascites), and swelling (edema). Affected individuals may also have blood in the urine (hematuria), which can lead to a reduced number of red blood cells in the body (anemia), abnormal blood clotting, or reduced amounts of certain white blood cells. Low white blood cell counts can lead to a weakened immune system and frequent infections in people with nephrotic syndrome. If not treated with coenzyme Q10 supplementation, affected individuals eventually develop irreversible kidney failure (end-stage renal disease). Affected individuals often present initially with steroid-resistant nephrotic syndrome (SRNS) that leads to end-stage renal disease, followed by an encephalomyopathy with seizures and stroke-like episodes resulting in severe neurologic impairment and ultimately death 123, 124, 125. Some affected individuals manifest only steroid-resistant nephrotic syndrome (SRNS) with onset in the first or second decade of life and slow progression to end-stage renal disease without extrarenal manifestations 126. One of the two individuals in a family with COQ9 gene related primary coenzyme Q10 deficiency manifested tubulopathy within a few hours after birth 120.
No clinical practice guidelines for management of primary coenzyme Q10 (CoQ10) deficiency have been published. There is no cure for primary coenzyme Q10 deficiency, but coenzyme Q10 replacement therapy is indicated for primary coenzyme Q10 deficiency 127, 121. In patients with primary coenzyme Q10 deficiency, early treatment with high-dose coenzyme Q10 supplementation (ranging from 5 to 50 mg/kg/day) can limit disease progression 110, 127. High-dose coenzyme Q10 supplementation (ranging from 5 to 50 mg/kg/day) should be instituted as early as possible because it can limit disease progression and reverse some manifestations 128; however, established severe neurologic and/or kidney damage cannot be reversed 120.
A recent study of coenzyme Q10 supplementation (20 mg/kg) demonstrated promising results in patients with primary coenzyme Q10 deficiency with nephrotic syndrome and steroid-resistant nephrotic syndrome (SRNS) 127. Children with severe multisystem coenzyme Q10 deficiency respond poorly to treatment and generally die within the neonatal period or in the first year of life 127.
Data on the prognosis of primary coenzyme Q10 deficiency are limited due to the small number of affected individuals reported to date 127. It is a progressive disorder, with variable rates of progression and tissue involvement depending on the gene involved and the severity of the coenzyme Q10 deficiency 127.
Individuals with later-onset disease show better response to supplementation with high-dose oral coenzyme Q10 127. In many instances treatment can change the natural history of the disease by blocking progression of the kidney disease and preventing the onset of neurologic manifestations in persons with homozygous mutations in the COQ2, COQ6, COQ8B, or PDSS2 genes 129, 125, 128, 127.
Secondary Coenzyme Q10 deficiency
Secondary coenzyme Q10 deficiency results from mutations or deletions in genes that are not directly related to coenzyme Q10 biosynthetic pathway 110, 72. Secondary coenzyme Q10 deficiency has been described in patients with mitochondrial DNA (mtDNA) mutations or deletions, with mitochondrial DNA depletion syndrome, Kearns-Sayre syndrome, or multiple acyl-CoA dehydrogenase deficiency (MADD) and in patients with mutations in APTX, ETFDH, BRAF, ACADVL or NPC genes 111, 112, 113, 114, 115, 116, 117, 118, 119. Interestingly, coenzyme Q10 levels may be decreased in those with acute influenza infection 69.
Secondary coenzyme Q10 deficiency has also been identified in non-mitochondrial disorders, such as cardiofaciocutaneous syndrome and Niemann-Pick-type C disease 130. Secondary coenzyme Q10 deficiency can also be secondary to the inhibition of HMG-CoA reductase by statin drugs. A 2015 meta-analysis of six small, randomized controlled trials found no reduction in statin-induced muscle pain with 100 to 400 mg/day of supplemental coenzyme Q10 for one to three months 131. The trials failed to establish a diagnosis of relative coenzyme Q10 deficiency before the intervention started, hence limiting the conclusion of the meta-analysis. While statin therapy may not necessary lead to a reduction in circulating coenzyme Q10 concentrations, further research needs to examine whether secondary coenzyme Q10 deficiency might be predisposing patients to statin-induced myalgia 132.
It is not clear to what extent coenzyme Q10 supplementation might have therapeutic benefit in patients with inherited secondary Q10 deficiencies, because the therapeutic potential of supplemental coenzyme Q10 is limited to its capacity to restore electron transfer in a defective mitochondrial respiratory chain and/or to increase antioxidant defense 72. For example, multiple acyl-CoA dehydrogenase deficiency (MADD), caused by mutations in genes that impair the activity of enzymes involved in the transfer of electrons from acyl-CoA to coenzyme Q10, is usually responsive to riboflavin (vitamin B2) monotherapy yet patients with low coenzyme Q10 concentrations might also benefit from co-supplementation with coenzyme Q10 and riboflavin 133. Another study suggested clinical improvements in secondary coenzyme Q10 deficiency with supplemental coenzyme Q10 in patients presenting with ataxia 134. Because the cause of secondary coenzyme Q10 in inherited conditions is generally unknown, it is difficult to predict whether improving coenzyme Q10 status with supplemental coenzyme Q10 would lead to clinical benefits for the patients 72.
Ubiquinone supplement benefits
The U.S. Food and Drug Administration (FDA) does not approve dietary supplements as safe or effective. The company that makes the dietary supplements is responsible for making sure that they are safe and that the claims on the label are true and do not mislead the patient. The way that supplements are made is not regulated, so all batches and brands of coenzyme q10 supplements may not be the same.
Ubiquinone for cancer
There have been few clinical trials on the use of coenzyme Q10 to prevent side effects of cancer treatment, treat side effects of cancer treatment, and/or as a treatment for cancer 135, 84. A trial of 236 breast cancer patients were randomized to receive either Coenzyme q10 or placebo, each combined with vitamin E, for 24 weeks. The study found that levels of fatigue and quality of life were not improved in patients who received Coenzyme q10 compared to patients who received the placebo 135.
A randomized trial of 20 children treated for acute lymphoblastic leukemia or non-Hodgkin lymphoma looked at whether Coenzyme q10 would protect the heart from the damage caused by doxorubicin. The results reported that CoQ10 decreased the harmful effects of doxorubicin on the heart 135. It has been postulated that doxorubicin interferes with energy-generating biochemical reactions that involve coenzyme Q10 in heart muscle mitochondria and that this interference can be overcome by coenzyme Q10 supplementation 27, 98, 99. Studies with adults and children, including the aforementioned randomized trial, have confirmed the decrease in heart toxicity observed in animal studies 27, 29, 78, 28. A randomized trial 29 of 20 patients tested the ability of coenzyme Q10 to reduce cardiotoxicity caused by anthracycline drugs.
Anecdotal reports of coenzyme Q10 lengthening the survival of patients with pancreatic, lung, rectal, laryngeal, colon, and prostate cancers also exist in the peer-reviewed scientific literature 28. The patients described in these reports also received therapies other than coenzyme Q10, including chemotherapy, radiation therapy, and surgery.
A recent observational study conducted with 1,134 patients with breast cancer enrolled in an National Cancer Institute multi-institution clinical trial (SWOG S0221) suggested that the use of antioxidant supplements, including coenzyme Q10, prior to and during cancer treatment may be associated with increased recurrence rates and decreased survival 136.
Reversal of statin-induced myopathy
Statins (HMG-CoA reductase inhibitors) deplete circulating coenzyme Q10 levels by interfering with its biosynthesis 137. Most studies indicate a correlation between the decrease in serum coenzyme Q10 and decreases of total and low-density lipoprotein cholesterol levels. This effect may be particularly important in elderly patients, in whom coenzyme Q10 levels are already compromised, and is also associated with higher dosages (lower dosages do not seem to affect intramuscular levels of coenzyme Q10) 138. The use of ezetimibe alone or in combination with a statin does not offer protection against depletion of coenzyme Q10 138. No correlation has been established for decreased serum coenzyme Q10 and cardiovascular events 138. Supplemental coenzyme Q10 increased circulating levels of the compound. However, results from randomized clinical trials are inconsistent in showing an effect on statin-associated myopathy 139, 138.
Neurological disorders
The case for coenzyme Q10 as a treatment option in neurological (mitochondrial-related) disease is not as strong 140. The role of coenzyme Q10 in Parkinson, Alzheimer, and Huntington diseases; amyotrophic lateral sclerosis; and Friedreich ataxia is postulated but not established 141.
Studies in Friedreich and non-Friedreich ataxia have largely shown a continued worsening of disease, as measured by the International Cooperative Ataxia Group rating scale, irrespective of coenzyme q10 use (5 mg/kg/day) 142.
A link between mitochondrial dysfunction and Parkinson disease has been established, but the relationship with coenzyme Q10 has not 143. A multicenter clinical trial found a decrease in worsening of symptoms in patients with early Parkinson disease receiving coenzyme Q10 1,200 mg/day, but not at lower dosages 144. Effects were not apparent at 1 month, but were evident at 8 months. Changes in daily living factors were more pronounced than clinical disease progression changes 145. Increases in plasma coenzyme Q10 were recorded. A larger trial using higher dosages (coenzyme Q10 600 mg chewable wafers 4 times a day) found a mean change in total rating score high enough to warrant a phase 3 trial 146; however, the trial was not designed to evaluate efficacy 146. A multicenter trial of patients receiving anti-Parkinson medication found no difference in symptoms over placebo 147.
The role of mitochondrial stress in Alzheimer disease led to more studies of coenzyme Q10 142. Multicenter clinical trials using idebenone dosages of up to 360 mg 3 times a day found no effect on the rate of decline over placebo. Analyses using various rating scales showed some differences that were not considered clinically important, mirroring other older trials 148. Similarly, no slowing of decline was noted in Huntington disease 149.
Parkinson’s disease
Parkinson’s disease is a degenerative neurological disorder characterized by tremors, muscular rigidity, and slow movements. Parkinson’s disease is estimated to affect approximately 1% of Americans over the age of 65. Mitochondrial dysfunction and oxidative damage in a part of the brain called the substantia nigra may play a role in the development of the disease 150. Decreased ratios of reduced-to-oxidized coenzyme Q10 have been found in platelets of individuals with Parkinson’s disease 151, 152. One study also found higher concentrations of oxidized coenzyme Q10 in the cerebrospinal fluid of patients with untreated Parkinson’s disease compared to healthy controls 153. Additionally, a study in postmortem Parkinson’s disease patients found lower concentrations of total coenzyme Q10 in the cortex region of the brain compared to age-matched controls, but no differences were seen in other brain areas, including the striatum, substantia nigra, and cerebellum 154.
A 16-month randomized, placebo-controlled phase II clinical trial evaluated the safety and efficacy of 300, 600, or 1,200 mg/day of coenzyme Q10 in 80 people with early Parkinson’s disease 155. Coenzyme Q10 supplementation was well tolerated at all doses and resulted in a slower deterioration of function in Parkinson’s disease patients in the group taking 1,200 mg/day. A phase III clinical trial was then designed to further examine the effect of high-dose coenzyme Q10 (1,200-2,400 mg/day) and vitamin E (1,200 IU/day) supplementation on both motor and non-motor symptoms associated with Parkinson’s disease. This trial was prematurely terminated because it was unlikely that such a treatment was effective in treating Parkinson’s disease 156. A smaller placebo-controlled trial showed that oral administration of 300 mg/day of coenzyme Q10 for 48 to 96 months moderately improved motor symptoms in treated patients with Levodopa with re-emerging symptoms but not in patients at an early stage of Parkinson’s disease 157. Two recent meta-analyses of randomized, placebo-controlled trials found no evidence that coenzyme Q10 improved motor-related symptoms or delayed the progression of Parkinson’s disease when compared to placebo 158, 159.
Huntington’s disease
Huntington’s disease is an inherited neurodegenerative disorder characterized by selective degeneration of nerve cells known as striatal spiny neurons. Huntington’s disease symptoms, such as movement disorders and impaired cognitive function, typically develop in the fourth decade of life and progressively deteriorate over time. Animal models indicate that impaired mitochondrial function and glutamate-mediated neurotoxicity may be involved in the pathology of Huntington’s disease. Some, but not all, studies in mouse models of Huntington’s disease have suggested that coenzyme Q10 supplementation could improve motor performance, overall survival, and various hallmarks of Huntington’s disease, i.e., brain atrophy, ventricular enlargement, and striatal neuronal atrophy 160, 161. Interestingly, co-administration of coenzyme Q10 with remacemide (an NMDA receptor antagonist), the antibiotic minocycline, or creatine led to greater improvements in most biochemical and behavioral parameters 160, 161, 162.
To date, only two clinical trials have examined whether coenzyme Q10 might be efficacious in human patients with Huntington’s disease. A 30-month, randomized, placebo-controlled trial of coenzyme Q10 (600 mg/day), remacemide, or both in 347 patients with early Huntington’s disease found that neither coenzyme Q10 nor remacemide significantly altered the decline in total functional capacity, although coenzyme Q10 supplementation (with or without remacemide) resulted in a nonsignificant trend toward a slower decline 163. A 20-week pilot trial examined the safety and tolerability of increasing dosages of coenzyme Q10 (1,200 mg/day, 2,400 mg/day, and 3,600 mg/day) in eight healthy subjects and in 20 patients with Huntington’s disease; 22 of the subjects completed the study 164. All dosages were generally well tolerated, with gastrointestinal symptoms being the most frequently reported adverse effect. Blood concentrations of coenzyme Q10 at the end of the study were maximized with the daily dose of 2,400 mg 164. Coenzyme Q10 2,400 mg dose was tested in a multicenter phase III clinical trial in 609 participants with early-stage Huntington’s disease 165. Participants were randomized to receive either 2,400 mg/day of coenzyme Q10 or placebo for five years 165. The trial was prematurely halted because it appeared unlikely to demonstrate any health benefit in supplemented patients — about one-third of participants completed the trial at the time of study termination 165. Although coenzyme Q10 is generally well tolerated, there is no evidence that supplementation can improve functional and cognitive symptoms in Huntington’s disease patients.
Friedreich’s ataxia
Friedreich’s ataxia is an autosomal recessive neurodegenerative disease caused by mutations in the FXN gene that encodes for the mitochondrial protein, frataxin. Frataxin is needed for the making of iron-sulfur clusters (ISC). Iron-sulfur clusters-containing subunits are especially important for the mitochondrial respiratory chain and for the synthesis of heme-containing proteins 166. Frataxin deficiency is associated with imbalances in iron-sulfur containing proteins, mitochondrial respiratory chain dysfunction and lower ATP production, and accumulation of iron in the mitochondria, which increases oxidative stress and oxidative damage to macromolecules of the respiratory chain 167. Clinically, Friedreich’s ataxia is a progressive disease characterized by ataxia, areflexia, speech disturbance (dysarthria), sensory loss, motor dysfunction, cardiomyopathy, diabetes, and scoliosis 167. A pilot study administering coenzyme Q10 (200 mg/day) and vitamin E (2,100 IU/day) to 10 Friedreich’s ataxia patients found that energy metabolism of cardiac and skeletal muscle was improved after only three months of therapy 168. Follow-up assessments at 47 months indicated that cardiac and skeletal muscle improvements were maintained and that Friedreich’s ataxia patients showed significant increases in fractional shortening, a measure of cardiac function. Moreover, the therapy was effective at preventing the progressive decline of neurological function 169. Another study reported both coenzyme Q10 and vitamin E deficiencies among Friedreich’s ataxia patients and suggested that co-supplementation with both compounds, at doses as low as 30 mg/day of coenzyme Q10 and vitamin E 4 IU/day, might improve disease symptoms 170. Large-scale, randomized controlled trials are necessary to determine whether coenzyme Q10, in conjunction with vitamin E, has therapeutic benefit in Friedreich’s ataxia. At present, about one-half of patients use coenzyme Q10 and vitamin E supplements despite the lack of proven therapeutic benefit (77).
Spinocerebellar ataxias
Spinocerebellar ataxias are a group of rare autosomal dominant neurodegenerative diseases characterized by gait difficulty, loss of hand dexterity, dysarthria, and cognitive decline 171. To date, more than 40 distinct genetic spinocerebellar ataxias have been identified which are classified according to the genetic loci in order of identification. SCA1, 2, 3, and 6 are the most common spinocerebellar ataxias 172. In vitro coenzyme Q10 treatment of forearm skin fibroblasts isolated from patients with SCA2 was found to reduce oxidative stress and normalize complex I and II-III activity of the mitochondrial respiratory chain 173. A multicenter prospective cohort study that followed 319 patients with spinocerebellar ataxias (≥15 years) found no difference in the rate of disease progression over two years between those taking supplemental coenzyme Q10 (median dose, 600 mg/day) and nonusers 172.
Aging
According to the free radical and mitochondrial theories of aging, oxidative damage of cell structures by reactive oxygen species (ROS) plays an important role in the functional declines that accompany aging 174. Reactive oxygen species (ROS) are generated by mitochondria as a byproduct of ATP production. If not neutralized by antioxidants, reactive oxygen species (ROS) may damage mitochondria over time, causing them to function less efficiently and to generate more damaging reactive oxygen species (ROS) in a self-perpetuating cycle 72. Coenzyme Q10 plays an important role in mitochondrial ATP synthesis and functions as an antioxidant in mitochondrial membranes. One of the hallmarks of aging is a decline in energy metabolism in many tissues, especially liver, heart, and skeletal muscle. Tissue concentrations of coenzyme Q10 have been found to decline with age, thereby accompanying age-related declines in energy metabolism 108. Early animal studies have not been able to demonstrate an effect of lifelong dietary supplementation with coenzyme Q10 on the lifespan of rats or mice 175, 176, 177. Nonetheless, more recent studies have suggested that supplemental coenzyme Q10 could promote mitochondrial biogenesis and respiration and delay senescence in transgenic mice 178, 179. At the present time, there is limited scientific evidence to suggest that coenzyme Q10 supplementation prolongs life or prevents age-related functional declines in humans. In a small randomized controlled trial, elderly individuals (>70 years) who received a combination of selenium (100 µg/day) and coenzyme Q10 (200 mg/day) for four years reported an improvement in vitality, physical performance, and quality of life 180. Furthermore, a 12-year follow-up of these participants showed a reduction in cardiovascular mortality with supplemental selenium and coenzyme Q10 compared to placebo 56.
Blood lipids
Elevated plasma lipoprotein-A concentration is an independent risk factor for cardiovascular disease. A meta-analysis of six controlled trials of which five were randomized in 409 participants found a reduction in plasma lipoprotein-A concentration with coenzyme Q10 supplementation 100-300 mg/day for 4 to 12 weeks 181. Other effects of coenzyme Q10 on blood lipids have not been reported 181, 182, 183.
A therapeutic approach combining coenzyme Q10 with other antioxidants might prove to be more effective to target co-existing metabolic disorders in individuals at risk for cardiovascular disease 184.
Atherosclerosis
Oxidative modification of low-density lipoproteins (LDL), also known as “bad” cholesterol, in arterial walls is thought to represent an early event leading to the development of atherosclerosis. Ubiquinol or reduced coenzyme Q10 inhibits the oxidation of LDL in the test tube (in vitro) and works together with alpha-tocopherol (active form of vitamin E) to inhibit LDL oxidation by regenerating tocopheroxyl radical (oxidized form of vitamin E) back to alpha-tocopherol (reduced form of vitamin E) 185. In the absence of a co-antioxidant, such as ubiquinol or vitamin C, tocopheroxyl radical (oxidized form of vitamin E) can, under certain conditions, promote the oxidation of LDL in test tube study 105. Supplementation with coenzyme Q10 increases the concentration of ubiquinol (reduced coenzyme Q10) in human LDL 186. Studies in apolipoprotein E-deficient mice, an animal model of atherosclerosis, found that coenzyme Q10 supplementation with supra-pharmacological amounts of coenzyme Q10 inhibited lipoprotein oxidation in the blood vessel wall and the formation of atherosclerotic lesions 187. Interestingly, co-supplementation of these mice with alpha-tocopherol (vitamin E) and coenzyme Q10 was more effective in inhibiting atherosclerosis than supplementation with either alpha-tocopherol (vitamin E) or coenzyme Q10 alone 188.
Another important step in the development of atherosclerosis is the recruitment of immune cells known as monocytes into the blood vessel walls. This recruitment is dependent in part on monocyte expression of cell adhesion molecules (integrins). Supplementation of 10 healthy men and women with 200 mg/day of coenzyme Q10 for 10 weeks resulted in significant decreases in monocyte expression of integrins, suggesting another potential mechanism for the inhibition of atherosclerosis by coenzyme Q10 189. Although coenzyme Q10 supplementation shows promise as an inhibitor of LDL oxidation and atherosclerosis, more research is needed to determine whether coenzyme Q10 supplementation can inhibit the development or progression of atherosclerosis in humans.
Cardiovascular risk factors
Normally functioning vascular endothelium promotes blood vessel relaxation (vasodilation) when needed (for example, during exercise) and inhibits the formation of blood clots. Atherosclerosis is associated with impairment of vascular endothelial function, thereby compromising vasodilation and normal blood flow. Endothelium-dependent vasodilation is impaired in individuals with elevated serum cholesterol concentrations, as well as in patients with coronary heart disease or diabetes mellitus. A 2012 meta-analysis examining the results of five small randomized controlled trials in 194 subjects in total found that supplemental coenzyme Q10 with 150-300 mg/day for 4 to 12 weeks resulted in a clinically significant, 1.7% increase in flow-dependent endothelial-mediated dilation 190. Evidence from larger studies is needed to further establish the effect of coenzyme Q10 on endothelium-dependent vasodilation.
Several small randomized controlled trials in patients at increased cardiovascular disease risk or with established cardiovascular disease have examined the effect of supplemental coenzyme Q10 for ≤3 months on circulating inflammation markers i.e., C-reactive protein (CRP), interleukin-6 (IL-6) and/or tumor necrosis factor alpha (TNF-α). Recently published pooled analyses of these trials have given mixed results 191, 182, 192. Larger studies are needed to examine the effect of coenzyme Q10 supplementation on low-grade inflammation.
Congestive heart failure
Impairment of the heart’s ability to pump enough blood for all of the body’s needs is known as congestive heart failure. In coronary heart disease (coronary artery disease), accumulation of atherosclerotic plaque in the coronary arteries may prevent parts of the heart muscle from getting adequate blood supply, ultimately resulting in heart damage and impaired pumping ability. Heart failure can also be caused by heart attack (myocardial infarction), high blood pressure (hypertension), diseases of the heart valves, cardiomyopathy (diseases of the heart muscle), and congenital heart diseases. Because physical exercise increases the demand on the weakened heart, measures of exercise tolerance are frequently used to monitor the severity of heart failure. Echocardiography is also used to determine the left ventricular ejection fraction, an objective measure of the heart’s pumping ability 193.
A study of 1,191 heart failure patients found that low plasma coenzyme Q10 concentration was a good biomarker of advanced heart disease 194. A number of small intervention trials that administered supplemental coenzyme Q10 to congestive heart failure patients have been conducted. A recently published systematic review showed that supplementation with coenzyme Q10, in addition to standard therapy in patients with moderate-to-severe heart failure, is associated with symptom reduction and reduction of major adverse cardiovascular events 40, 50. Another meta-analysis of 14 randomized, placebo-controlled trials in 2,149 participants with heart failure found that coenzyme Q10 supplementation (30-300 mg/day) resulted in a 39% reduction in mortality (seven studies), improved exercise capacity (four studies), but had no effect on left ventricular ejection fraction (nine studies) compared to placebo 195. Coenzyme Q10 may improve functional capacity, endothelial function, and left ventricle contractility in congestive heart failure patients 40, 51.
Coenzyme Q10 cupplementation shows promising results in improving endothelial function in several subsets of patients. Coenzyme Q10 can improve endothelial function in patients with ischemic left ventricular systolic dysfunction and heart failure 52, 53. Likewise, compared with placebo, coenzyme Q10 improves endothelial function in the peripheral circulation of patients with type 2 diabetes mellitus and hyperlipidemia 54. Routine use of coenzyme Q10 in patients with coronary artery disease apart from congestive heart failure is still inconclusive 55, 52.
There is also evidence that combined with selenium, coenzyme Q10 supplementation in healthy older patients and older patients with diabetes, hypertension, and ischemic heart disease may decrease cardiovascular mortality risk 56.
A trial is presently being conducted to assess the value of supplemental coenzyme Q10 and/or D-ribose in the treatment of congestive heart failure in patients with normal left ventricular ejection fraction 196.
A 2021 literature review identified 11 small randomized controlled trials involving 1573 participants examining the effect of coenzyme Q10 supplementation (60-200 mg/day for ≤3 months in most trials) in heart failure patients 197. The analyses show that based on currently available evidence it is not sufficient to draw robust conclusions about the safety and efficacy of coenzyme Q10 in heart failure 197.
According to the 2022 American College of Cardiology, American Heart Association and the Heart Failure Society of America guidelines, coenzyme Q10 supplementation effectively reduced vascular mortality, all-cause mortality, and hospital stays for heart failure at 2 years 198. However, long-term supplementation is needed 49.
Ischemia-reperfusion injury
The heart muscle may become oxygen-deprived (ischemic) as the result of a heart attack (myocardial infarction) or during heart surgery. Increased generation of reactive oxygen species (ROS) when the heart muscle’s oxygen supply is restored (reperfusion) might be an important contributor to heart muscle damage occurring during ischemia-reperfusion 199. Pretreatment of animals with coenzyme Q10 has been found to preserve heart function following ischemia-reperfusion injury by increasing ATP concentration, enhancing antioxidant capacity and limiting oxidative damage, regulating autophagy, and reducing cardiomyocyte apoptosis 200. Another potential source of ischemia-reperfusion injury is aortic clamping during some types of cardiac surgery, such as coronary artery bypass graft (CABG) surgery. Early placebo-controlled trials found that coenzyme Q10 pretreatment with coenzyme Q10 60-300 mg/day for 7-14 days prior to surgery provided some benefit in short-term outcome measures after coronary artery bypass graft (CABG) surgery 201, 202. In a small randomized controlled trial in 30 patients, oral administration of coenzyme Q10 for 7 to 10 days before coronary artery bypass graft (CABG) surgery reduced the need for mediastinal drainage, platelet transfusion, and positive inotropic drugs (e.g. dopamine) and the risk of arrhythmia within 24 hours post-surgery 203. In one trial that did not find preoperative coenzyme Q10 supplementation to be of benefit, patients were treated with 600 mg of coenzyme Q10 12 hours prior to surgery, suggesting that preoperative coenzyme Q10 treatment may need to commence at least one week prior to CABG surgery to improve surgical outcomes 204. The combined administration of coenzyme Q10, lipoic acid, omega-3 fatty acids, magnesium orotate, and selenium at least two weeks before CABG surgery and four weeks after was examined in a randomized, placebo-controlled trial in 117 patients with heart failure 205. The treatment resulted in lower concentration of troponin-I (a marker of heart muscle injury), shorter length of hospital stay, and reduced risk of postoperative transient cardiac dysfunction compared to placebo 205.
Although trials have included relatively few people and examined mostly short-term, post-surgical outcomes, the results are promising 196.
Periprocedural myocardial injury
Coronary angioplasty also called percutaneous coronary intervention (PCI) is a minimally invasive medical procedure for treating narrowed or blocked coronary arteries, including unstable angina pectoris, acute myocardial infarction, and multivessel coronary heart disease. Coronary angioplasty involves temporarily inserting a catheter with a balloon and inflating a tiny balloon into the blocked artery to help restore the blood flow to the heart and a stent is often inserted to keep the artery open. Periprocedural myocardial injury that occurs in up to one-third of patients undergoing otherwise uncomplicated angioplasty increases the risk of morbidity and mortality at follow-up.
A prospective cohort study followed 55 patients with acute ST segment elevation myocardial infarction (a type of heart attack characterized by the death of some myocardial tissue) who underwent coronary angioplasty 206. Plasma coenzyme Q10 concentration one month after angioplasty was positively correlated with less inflammation and oxidative stress and predicted favorable left ventricular end-systolic volume remodeling at six months 206. One randomized controlled trial has examined the effect of coenzyme Q10 supplementation on periprocedural myocardial injury in patients undergoing coronary angioplasty 207. The administration of 300 mg of coenzyme Q10 12 hours before the angioplasty to 50 patients reduced the concentration of C-reactive protein (CRP; a marker of inflammation) within 24 hours following the procedure compared to placebo. However, there was no difference in concentrations of two markers of myocardial injury (creatine kinase and troponin-I) or in the incidence of major adverse cardiac events one month after angioplasty between active treatment and placebo 207. Additional trials are needed to examine whether coenzyme Q10 therapy can improve clinical outcomes in patients undergoing coronary angioplasty.
Angina pectoris
Myocardial ischemia a condition where the heart muscle doesn’t get enough oxygen-rich blood, usually because a coronary artery is partially or completely blocked by plaque may also lead to chest pain known as angina pectoris. People with angina pectoris often experience symptoms when the demand for oxygen exceeds the capacity of the coronary circulation to deliver it to the heart muscle, e.g., during exercise. Five small placebo-controlled studies have examined the effects of oral coenzyme Q10 supplementation (60-600 mg/day) in addition to conventional medical therapy in patients with chronic stable angina 208. In most of the studies, coenzyme Q10 supplementation improved exercise tolerance and reduced or delayed electrocardiographic changes associated with myocardial ischemia compared to placebo. However, only two of the studies found significant decreases in symptom frequency and use of nitroglycerin with coenzyme Q10 supplementation. Presently, there is only limited evidence suggesting that coenzyme Q10 supplementation would be a useful adjunct to conventional angina therapy.
High blood pressure
Data are conflicting on whether coenzyme Q10 may play a role in treating high blood pressure 57. Very few high-quality trials have examined the potential therapeutic benefit of coenzyme Q10 supplementation in the treatment of primary hypertension or essential hypertension where high blood pressure without a single identifiable cause 209. A systematic review identified two small randomized, double-blind, placebo-controlled trials that found little evidence of a reduction in systolic or diastolic blood pressure following the administration of coenzyme Q10 (100-200 mg/day) for three months 209. In contrast, a meta-analysis that used less stringent selection criteria included 17 small trials and found evidence of a blood pressure-lowering effect of coenzyme Q10 in patients with cardiovascular disease or metabolic disorders 210. The effect of coenzyme Q10 on blood pressure needs to be examined in large, well-designed clinical trials.
Diabetes mellitus
Diabetes mellitus or diabetes, is a chronic condition characterized by high blood glucose (sugar) levels, resulting from the pancreas not producing enough insulin or the body being unable to use its insulin effectively. Symptoms include increased thirst and urination, fatigue, and blurred vision. It can be managed through a combination of lifestyle changes and medication, and common types include Type 1 diabetes, Type 2 diabetes, and gestational diabetes. Plasma concentrations of reduced coenzyme Q10 (Ubiquinol) have been found to be lower in diabetic patients than healthy controls after normalization to plasma cholesterol concentrations 211, 212. Tthe pathogenesis of type 2 diabetes mellitus involves the early onset of glucose intolerance and hyperinsulinemia associated with the progressive loss of tissue responsiveness to insulin. Recent experimental studies tied insulin resistance to a decrease in coenzyme Q10 expression and showed that supplementation with coenzyme Q10 could restore insulin sensitivity 106. Coenzyme Q10 supplementation might thus be a more useful tool for the primary prevention of type 2 diabetes rather than for its management.
Randomized controlled trials that examined the effect of coenzyme Q10 supplementation found little evidence of benefits on glycemic control in patients with diabetes mellitus. A meta-analysis of six trials in participants with type 2 diabetes and one trial in participants with type 1 diabetes found that 100 to 200 mg/day of coenzyme Q10 for three to six months lowered neither fasting plasma glucose nor levels of glycated hemoglobin ([HbA1c]; a measure of glycemic control). Maternally inherited diabetes mellitus-deafness syndrome is caused by a mutation in mitochondrial DNA, which is inherited exclusively from one’s mother. Maternally inherited diabetes mellitus-deafness syndrome accounts for less than 1% of all cases of diabetes. Some early evidence suggested that long-term coenzyme Q10 supplementation (150 mg/day) may improve insulin secretion and prevent progressive hearing loss in these patients 213, 214.
Athletic performance
There is little evidence that supplementation with coenzyme Q10 improves athletic performance in healthy individuals 215, 216, 217, 218, 219. A few placebo-controlled trials have examined the effects of 100 to 150 mg/day of supplemental coenzyme Q10 for three to eight weeks on physical performance in trained and untrained men. Most did not find significant differences between the group taking coenzyme Q10 and the group taking placebo with respect to measures of aerobic exercise performance, such as maximal oxygen consumption (VO2 max) and exercise time to exhaustion 215, 216, 217, 218, 219. One study found the maximal cycling workload to be slightly (4%) increased after eight weeks of coenzyme Q10 supplementation compared to placebo, although measures of aerobic power were not increased 220. Two studies actually found significantly greater improvement in measures of anaerobic and aerobic exercise performance with a placebo than with supplemental coenzyme Q10 215, 216. More recent studies have suggested that coenzyme Q10 could help reduce both muscle damage-associated oxidative stress and low-grade inflammation induced by strenuous exercise 221, 222, 223, 224. Studies on the effect of coenzyme Q10 supplementation on physical performance in women are lacking, but there is little reason to suspect a gender difference in the response to coenzyme Q10 supplementation.
Other uses
Coenzyme Q10 has also shown promise in migraine prophylaxis (prevention). Coenzyme Q10 has been evaluated in migraine versus placebo in small trials. A cohort study of 1550 children and adolescents with headaches found that this population has low coenzyme Q10 levels 65. Decreases in migraine attack frequency, days with headache, and days with nausea were found for a daily dose of 300 mg coenzyme Q10 (1 to 3 mg/kg per day) 67, 65. A recent study indicated that coenzyme Q10 (coenzyme Q10 30 mg for children <30 kg and coenzyme Q10 60 mg for children over 30 kg) is beneficial for the prophylactic (preventive) treatment of migraine headaches in children without significant adverse effects 66.
Coenzyme Q10 supplemented alongside standard psychiatric medical therapy appears to lessen symptoms of depression in patients with bipolar disorder 70. In patients with polycystic ovary syndrome (PCOS), coenzyme Q10 supplementation may improve fasting blood glucose, insulin levels, and total testosterone levels 71.
The coadministration of ubiquinone with tamoxifen mitigated the hyperlipidemia associated with tamoxifen, and tumor marker levels indicated an antiangiogenesis effect 225. An Agency for Healthcare Research and Quality review of clinical trials reported no evidence to support the use of ubiquinone in the prevention or treatment of cancer 226.
Deficiencies of coenzyme Q10 have been described, predominantly affecting children, in a spectrum of diseases including infantile-onset, multisystem diseases, as well as adult-onset cerebellar ataxia and pure myopathies 141. Lymphocyte and platelet coenzyme Q10 levels were lower in Down syndrome 227, while lowered serum levels are associated with phenylketonuria and mevalonic aciduria 228.
In infants with Prader-Willi syndrome, coenzyme Q10 had no effect on lean mass versus growth hormone 229.
Coenzyme Q10 cupplementation shows the potential to decrease pain, fatigue, and morning tiredness compared to a placebo in patients with fibromyalgia 58, 59. Some data suggest that supplementation with moderate-to-high dose coenzyme Q10 may influence bicycle exercise aerobic capacity in patients with mitochondrial disorders 60.
Although most coenzyme Q10 studies have used patients with preexisting medical conditions, one study of healthy participants did show that oral coenzyme Q10 supplementation improved fatigue and physical performance during bicycle exercise routines 64.
Supplementation with coenzyme Q10 in men with Peyronie disease may decrease penile plaque size, reduce penile curvature, and improve erectile function 61.
Statin drugs inhibit the production of an intermediate in the mevalonate pathway—a biochemical route leading to coenzyme Q10 synthesis 62. Therefore, many researchers theorize that statin drugs may contribute to coenzyme Q10 depletion in the body. Given that muscle pain and cramping are frequent adverse effects of statins, they attribute these symptoms to the diminished levels of coenzyme Q10 63.
Ubiquinone dosage
Several dosage forms exist, including compressed and chewable tablets, powder-filled and gel-filled capsules, liquid syrups, and newer solubilized formulations. The reduced form of coenzyme Q10, ubiquinol, is also commercially available. It may also be given by injection into a vein (IV).
Most human studies on coenzyme Q10 (CoQ10) have focused on its oral supplementation. Available in various forms, such as tablets, capsules, soft gels, and liquid formulations, these oral supplements range from 30 to 600 mg per unit and are easily accessible over the counter. While topical over-the-counter preparations applied to the skin are also available, research on this mode of administration is limited. For instance, one study explored the effectiveness of a topical coenzyme Q10 treatment for age-related skin oxidative damage 230.
Pharmacokinetic studies suggest split dosing is superior to single daily dosing; for tissue uptake and crossing the blood-brain barrier, plasma coenzyme Q10 levels should be higher than normal 231.
Coenzyme Q10 (CoQ10) is a fat-soluble nutrient and coenzyme Q10 dissolved in an oil matrix is more effective than the same amount of crystalline coenzyme Q10 in raising coenzyme Q10 serum levels 175. Coenzyme Q10 (CoQ10) supplements should be taken at a meal that contains some fat. This enhances the absorption of the coenzyme Q10 (CoQ10). Coenzyme Q10 (CoQ10) 200 mg in oil/soft gel formulation caused a larger increase in coenzyme Q10 serum levels than 100 mg 175. Because coenzyme Q10 is a large molecular weight, fat-soluble compound, its absorption is slow and limited. This explains why better blood levels are achieved with divided doses rather than taking a large single dose of coenzyme Q10. The following data was gathered from multiple human clinical trials. On average, participants’ pre-test coenzyme Q10 blood levels were 1.09 ug/ml. After ingestion of a single 100 mg dose of coenzyme Q10, blood levels increased to 2.33 ug/ml. However, when people ingested 200 mg of coenzyme Q10 in a single dose, the blood level only increased to 2.35 ug/ml, almost no different than the blood level following a 100 mg dose. However, when individuals took 100 mg of coenzyme Q10 in divided doses, twice daily, blood levels rose to 3.47 ug/ml. Divided dosages (2 x 100 mg) of coenzyme Q10 caused a larger increase in serum levels of coenzyme Q10 than a single dose of 200 mg 175.
Usual adult dose of coenzyme-Q10 is 30 to 200 mg/day oral.
Supplementation with coenzyme Q10 (CoQ10) 50 mg twice daily has decreased statin-related mild-to-moderate myalgias, resulting in an increased ability to perform daily activities 63. The meta-analysis of randomized controlled trials indicated that coenzyme Q10 supplementation (100 to 600 mg/day) decreased the Statin-Associated Muscle Symptoms 86.
Supplementation with coenzyme Q10 (CoQ10) 300 mg daily for 24 weeks in men with Peyronie disease may decrease penile plaque size, reduce penile curvature, and improve erectile function 61.
A double-blind, randomized controlled trial showed coenzyme Q10 300 mg daily to be safe and superior to a placebo for migraine prevention 67. Another randomized, double-blind, placebo-controlled trial in adult women showed that 400 mg of supplementation decreased migraine frequency, severity, and duration 35. One study showed that only 100 mg daily reduced the severity of headaches and the number of headaches per month in migraine sufferers 68.
In patients with primary coenzyme Q10 deficiency (a rare genetic disorder caused by mutations in COQ genes essential for coenzyme Q10 biosynthesis, leading to low coenzyme Q10 levels in the body), early treatment with high-dose coenzyme Q10 supplementation (ranging from 5 to 50 mg/kg/day) can limit disease progression 120. A recent study of coenzyme Q10 supplementation (20 mg/kg) demonstrated promising results in patients with primary coenzyme Q10 deficiency with steroid-resistant nephrotic syndrome and sensorineural hearing loss 121, 232.
In observational studies and clinical trials (12 studies, total of 362 patients) has shown that coenzyme Q10 supplementation reduces blood pressure 233. Dose of coenzyme Q10 ranged between 34 and 225 mg/day and duration of individual studies from one to 56 weeks.
Cardiovascular and neurologic trials predominately use coenzyme Q10 dosages of 300 mg/day or coenzyme Q10 dosages of 5 mg/kg/day.
Coenzyme Q10 supplementation is well tolerated up to 1200 mg/day 41. High-dose coenzyme Q10 (1,200 mg/day) was used in patients with early Parkinson disease 144, while dosages of 2,700 to 3,000 mg/day were used in amyotrophic lateral sclerosis trials 234. An open-label study that included children evaluated tolerability of high-dose coenzyme Q10. Daily dosages of 60 mg/kg given in 3 divided doses were used for 1 month 235.
Liver impairment
Coenzyme Q10 supplementation reduces systemic inflammation and biochemical parameters in nonalcoholic fatty liver disease (NAFLD). However, as mentioned in pharmacokinetics, CoQ10 is excreted in bile. Hence, the use is not advised in patients with biliary obstruction.[34]
Kidney impairment
According to a recent article on Kidney Disease Improving Global Outcomes (KDIGO 2022), coenzyme Q10 supplementation may benefit patients with nephrotic syndrome due to primary coenzyme Q10 deficiency 236. However, studies of coenzyme Q10 in patients with kidney impairment are lacking. Coenzyme Q10 supplements should be avoided in patients with kidney impairment and used only for the indications mentioned in Kidney Disease Improving Global Outcomes guidelines 236.
Pregnancy
According to the manufacturer, coenzyme Q10 is not advised during pregnancy. However, a recent meta-analysis demonstrated that supplementation with coenzyme Q10 may benefit clinical pregnancy rates in women using assisted reproductive technologies (ART) to get pregnant 237.
Breastfeeding
Coenzyme Q10 (ubiquinone) is a normal part of the diet, and is also endogenously synthesized. Coenzyme Q10 (ubiquinone) is a normal component of human milk, but milk levels are slightly low in the breastmilk of mothers with preterm infants 238. Coenzyme Q10 has no specific lactation-related uses and no data exist on the safety and efficacy of supplementation in nursing mothers or infants 238. Coenzyme Q10 supplements are usually well tolerated with only infrequent, minor side effects.
Milk levels of coenzyme Q10 have not been measured after exogenous administration in humans. Coenzyme Q10 is a normal component of human milk; however, values appear to vary depending on the country in which they are measured, possibly because of dietary, genetic or other population differences as well as assay differences 239.
Older patients
No specific dosing recommendations for older or pediatric patients are available.
Ubiquinone Contraindications
Patients receiving chemotherapeutic drugs should also avoid coenzyme Q10, as there is insufficient data on its interaction with these drugs. As coenzyme Q10 lowers fasting blood glucose in some patients, it should be used cautiously in those with diabetes and patients prone to hypoglycemic episodes 240. Researchers in one study sounded a cautionary note when they found that coadministration of coenzyme Q10 and radiation therapy decreased the effectiveness of the radiation therapy 241. In this study, mice inoculated with human small cell lung cancer cells (a xenograft study), and then given coenzyme Q10 and single-dose radiation therapy, showed substantially less inhibition of tumor growth than mice in the control group that were treated with radiation therapy alone 241. Since radiation leads to the production of free radicals, and since antioxidants protect against free radical damage, the effect in this study might be explained by coenzyme Q10 acting as an antioxidant.
Coenzyme Q10 is contraindicated in patients with known hypersensitivity reactions to coenzyme Q10 or excipients. Some supplements contain silicon dioxide, which may be responsible for hypersensitivity reactions 242.
Ubiquinone side effects
No serious toxicity associated with the use of coenzyme Q10 has been reported 74, 75, 243, 244. Doses of 100 mg/day or higher have caused mild insomnia or digestive upsets in some individuals 82. Liver enzyme elevation has been detected in patients taking doses of coenzyme Q10 300 mg/day for extended periods of time, but no liver toxicity has been reported 245. Researchers in one cardiovascular study reported that coenzyme Q10 caused rashes, nausea, and epigastric (upper abdominal) pain that required withdrawal of a small number of patients from the study 246. Other reported side effects have included dizziness, photophobia (abnormal visual sensitivity to light), irritability,[5] headache, heartburn, and fatigue 247.
Reported side effects from the use of Coenzyme-Q10 include the following:
- High levels of liver enzymes.
- Nausea.
- Heartburn.
- Headache.
- Pain in the upper part of the abdomen.
- Dizziness.
- Rashes.
- Unable to fall sleep or stay asleep.
- Feeling very tired.
- Feeling irritable.
- Sensitive to light.
In a prospective study that explored the association between supplement use and breast cancer outcomes (SWOG S0221), the use of any antioxidant supplement before and during treatment–including coenzyme Q10, vitamin A, vitamin C, vitamin E, and carotenoids was associated with a trend showing an increased hazard of recurrence 26.
Certain lipid-lowering drugs, such as the statins (lovastatin, pravastatin, and simvastatin) and gemfibrozil, as well as oral agents that lower blood sugar, such as glyburide and tolazamide, cause a decrease in serum levels of coenzyme Q10 and reduce the effects of coenzyme Q10 supplementation 248, 74, 249, 250. Beta-blockers (drugs that slow the heart rate and lower blood pressure) can inhibit coenzyme Q10-dependent enzyme reactions. The contractile force of the heart in patients with high blood pressure can be increased by coenzyme Q10 administration 74. Coenzyme Q10 can reduce the body’s response to the anticoagulant drug warfarin 248. Finally, coenzyme Q10 can decrease insulin requirements in individuals with diabetes.
It is important to check with your doctor to find out if coenzyme Q10 can be safely used with other drugs. Certain drugs, such as those that are used to lower cholesterol, blood pressure, or blood sugar levels, may decrease the effects of Coenzyme-Q10. CoQ10 may change the way the body uses warfarin (a drug that prevents the blood from clotting) and insulin.
Coenzyme-Q10 may interact with the anticoagulant (blood thinner) warfarin and the diabetes drug insulin, and it may not be compatible with some types of cancer treatment.
Coenzyme Q10 Overdose
Coenzyme-Q10 toxicity is unlikely up to a daily intake of 1200 mg/day, although typical dosages have been 100 to 200 mg/day 251. In preclinical studies, ubiquinol’s No-Observed-Adverse-Effect Level (NOAEL) is 300 to 600 mg/kg (Sprague Dawley rats).
The human supplementation dose of CoQ10 is generally 100 to 300 mg/day. Assuming the human dose is 300 mg/day (5 mg/kg body weight), the safety factor is 60 to -120 times. The study indicated that chronic use of ubiquinol as a dietary supplement in humans is safe 252.
What other drugs will affect Coenzyme Q10?
Do not take Coenzyme Q10 without medical advice if you are using any of the following medications:
- omega-3 fatty acids;
- vitamins (especially A, C, E, or K);
- blood pressure medicine;
- cancer medicine; or
- warfarin (Coumadin, Jantoven). Coenzyme Q10 is chemically similar to vitamin K, and some reports are available in the literature for potential warfarin and coenzyme Q10 interaction. There are chances of warfarin treatment failure when patients are taking coenzyme Q10 supplements with warfarin therapy. This interaction is reversible 253, 254, 255.
This list is not complete. Other drugs may affect Coenzyme Q10, including prescription and over-the-counter medicines, vitamins, and herbal products. Not all possible drug interactions are listed here.
Toxicology
A review of animal experiments and clinical trials has estimated an acceptable daily intake for coenzyme Q10 to be 12 mg/kg (ie, 720 mg/day for a 60 kg person) based on a no-observed-adverse-effect level in rats of 1,200 mg/kg/day. An observed safety level based on clinical data is given as 1,200 mg/day. No accumulation in plasma or tissue following cessation of coenzyme Q10 consumption was noted and endogenous biosynthesis was not affected 256.
- Sood B, Patel P, Keenaghan M. Coenzyme Q10. [Updated 2024 Jan 30]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK531491[↩][↩]
- Crane FL. Discovery of ubiquinone (coenzyme Q) and an overview of function. Mitochondrion. 2007 Jun;7 Suppl:S2-7. doi: 10.1016/j.mito.2007.02.011[↩][↩][↩]
- Ernster L, Forsmark-Andrée P. Ubiquinol: an endogenous antioxidant in aerobic organisms. Clin Investig. 1993;71(8 Suppl):S60-5. doi: 10.1007/BF00226842[↩][↩][↩][↩][↩]
- Acosta MJ, Vazquez Fonseca L, Desbats MA, Cerqua C, Zordan R, Trevisson E, Salviati L. Coenzyme Q biosynthesis in health and disease. Biochim Biophys Acta. 2016 Aug;1857(8):1079-1085. https://doi.org/10.1016/j.bbabio.2016.03.036[↩][↩]
- Testai L, Martelli A, Flori L, Cicero AFG, Colletti A. Coenzyme Q10: Clinical Applications beyond Cardiovascular Diseases. Nutrients. 2021 May 17;13(5):1697. doi: 10.3390/nu13051697[↩][↩][↩]
- Szkopińska A. Ubiquinone. Biosynthesis of quinone ring and its isoprenoid side chain. Intracellular localization. Acta Biochim. Pol. 2000;47:469–480. doi: 10.18388/abp.2000_4027[↩]
- Turunen M., Olsson J., Dallner G. Metabolism and function of coenzyme Q. Biochim. Biophys. Acta (BBA) Biomembr. 2004;1660:171–199. doi: 10.1016/j.bbamem.2003.11.012[↩]
- Pelton R. Coenzyme Q10: A Miracle Nutrient Advances in Understanding. Integr Med (Encinitas). 2020 Apr;19(2):16-20. https://pmc.ncbi.nlm.nih.gov/articles/PMC7482328[↩][↩][↩][↩][↩][↩]
- Weber C, Bysted A, Hłlmer G. The coenzyme Q10 content of the average Danish diet. Int J Vitam Nutr Res. 1997;67(2):123-9.[↩]
- Zhang Y, Aberg F, Appelkvist EL, Dallner G, Ernster L. Uptake of dietary coenzyme Q supplement is limited in rats. J Nutr. 1995 Mar;125(3):446-53. doi: 10.1093/jn/125.3.446[↩]
- Cluis CP, Burja AM, Martin VJ. Current prospects for the production of coenzyme Q10 in microbes. Trends Biotechnol. 2007 Nov;25(11):514-21. doi: 10.1016/j.tibtech.2007.08.008[↩]
- https://www.nobelprize.org/prizes/chemistry/1978/summary[↩][↩]
- Crane F.L. Biochemical Functions of Coenzyme Q10. J. Am. Coll. Nutr. 2001;20:591–598. doi: 10.1080/07315724.2001.10719063[↩][↩]
- Haas R.H. The evidence basis for coenzyme Q therapy in oxidative phosphorylation disease. Mitochondrion. 2007;7:S136–S145. doi: 10.1016/j.mito.2007.03.008[↩]
- Gutierrez-Mariscal F.M., Yubero-Serrano E.M., Villalba J.M., Lopez-Miranda J. Coenzyme Q10: From bench to clinic in aging diseases, a translational review. Crit. Rev. Food Sci. Nutr. 2019;59:2240–2257. doi: 10.1080/10408398.2018.1442316[↩][↩]
- Schmelzer C., Lindner I., Rimbach G., Niklowitz P., Menke T., Döring F. Functions of coenzyme Q10in inflammation and gene expression. BioFactors. 2008;32:179–183. doi: 10.1002/biof.5520320121[↩]
- Yubero-Serrano E.M., Gonzalez-Guardia L., Rangel-Zuñiga O., Delgado-Lista J., Gutierrez-Mariscal F.M., Perez-Martinez P., Delgado-Casado N., Cruz-Teno C., Tinahones F.J., Villalba J.M., et al. Mediterranean Diet Supplemented With Coenzyme Q10 Modifies the Expression of Proinflammatory and Endoplasmic Reticulum Stress-Related Genes in Elderly Men and Women. J. Gerontol. Ser. A Boil. Sci. Med. Sci. 2011;67:3–10. doi: 10.1093/gerona/glr167[↩]
- Shukla S., Dubey K.K. CoQ10 a super-vitamin: Review on application and biosynthesis. 3 Biotech. 2018;8:1–11. doi: 10.1007/s13205-018-1271-6[↩]
- Folkers K, Littarru GP, Ho L, Runge TM, Havanonda S, Cooley D. Evidence for a deficiency of coenzyme Q10 in human heart disease. Int Z Vitaminforsch. 1970;40(3):380-90.[↩]
- Folkers K. The potential of coenzyme Q 10 (NSC-140865) in cancer treatment. Cancer Chemother Rep 2. 1974 Dec;4(4):19-22.[↩][↩]
- Flowers N, Hartley L, Todkill D, Stranges S, Rees K. Co-enzyme Q10 supplementation for the primary prevention of cardiovascular disease. Cochrane Database of Systematic Reviews 2014, Issue 12. Art. No.: CD010405. DOI: 10.1002/14651858.CD010405.pub2. http://cochranelibrary-wiley.com/doi/10.1002/14651858.CD010405.pub2/full[↩]
- Folkers K, Langsjoen P, Willis R, Richardson P, Xia LJ, Ye CQ, et al. Lovastatin decreases coenzyme Q levels in humans. Proceedings of the National Academy of Sciences of the United States of America 1990;87:8931-4.[↩]
- Schaars CF, Stalenhoef AF. Effects of ubiquinone (coenzyme Q10) on myopathy in statin users. Current Opinion in Lipidology 2008;19:553-7.[↩]
- Kumar A, Kaur H, Devi P, Mohan V. Role of coenzyme Q10 (CoQ10) in cardiac disease, hypertension and Meniere-like syndrome. Pharmacology and Therapeutics 2009;124(3):259-68.[↩][↩]
- Caso G, Kelly P, McNurlan MA, Lawson WE. Effect of coenzyme q10 on myopathic symptoms in patients treated with statins. American Journal of Cardiology 2007;99(10):1409-12.[↩]
- Ambrosone CB, Zirpoli GR, Hutson AD, et al. Dietary Supplement Use During Chemotherapy and Survival Outcomes of Patients With Breast Cancer Enrolled in a Cooperative Group Clinical Trial (SWOG S0221). J Clin Oncol. 2020 Mar 10;38(8):804-814. doi: 10.1200/JCO.19.01203[↩][↩][↩]
- Cortes EP, Gupta M, Chou C, Amin VC, Folkers K. Adriamycin cardiotoxicity: early detection by systolic time interval and possible prevention by coenzyme Q10. Cancer Treat Rep. 1978 Jun;62(6):887-91.[↩][↩][↩][↩][↩][↩]
- Folkers K, Brown R, Judy WV, Morita M. Survival of cancer patients on therapy with coenzyme Q10. Biochem Biophys Res Commun. 1993 Apr 15;192(1):241-5. doi: 10.1006/bbrc.1993.1405[↩][↩][↩][↩][↩]
- Iarussi D, Auricchio U, Agretto A, Murano A, Giuliano M, Casale F, Indolfi P, Iacono A. Protective effect of coenzyme Q10 on anthracyclines cardiotoxicity: control study in children with acute lymphoblastic leukemia and non-Hodgkin lymphoma. Mol Aspects Med. 1994;15 Suppl:s207-12. doi: 10.1016/0098-2997(94)90030-2[↩][↩][↩][↩][↩]
- Lesser GJ, Case D, Stark N, Williford S, Giguere J, Garino LA, Naughton MJ, Vitolins MZ, Lively MO, Shaw EG; Wake Forest University Community Clinical Oncology Program Research Base. A randomized, double-blind, placebo-controlled study of oral coenzyme Q10 to relieve self-reported treatment-related fatigue in newly diagnosed patients with breast cancer. J Support Oncol. 2013 Mar;11(1):31-42. doi: 10.1016/j.suponc.2012.03.003[↩]
- Iwase S, Kawaguchi T, Yotsumoto D, Doi T, Miyara K, Odagiri H, Kitamura K, Ariyoshi K, Miyaji T, Ishiki H, Inoue K, Tsutsumi C, Sagara Y, Yamaguchi T. Efficacy and safety of an amino acid jelly containing coenzyme Q10 and L-carnitine in controlling fatigue in breast cancer patients receiving chemotherapy: a multi-institutional, randomized, exploratory trial (JORTC-CAM01). Support Care Cancer. 2016 Feb;24(2):637-646. doi: 10.1007/s00520-015-2824-4[↩]
- Folkers K, Osterborg A, Nylander M, Morita M, Mellstedt H. Activities of vitamin Q10 in animal models and a serious deficiency in patients with cancer. Biochem Biophys Res Commun. 1997 May 19;234(2):296-9. doi: 10.1006/bbrc.1997.6522[↩][↩]
- Du J, Wang T, Huang P, Cui S, Gao C, Lin Y, Fu R, Shen J, He Y, Tan Y, Chen S. Clinical correlates of decreased plasma coenzyme Q10 levels in patients with multiple system atrophy. Parkinsonism Relat Disord. 2018 Dec;57:58-62. doi: 10.1016/j.parkreldis.2018.07.017[↩]
- Chang PS, Chou HH, Lai TJ, Yen CH, Pan JC, Lin PT. Investigation of coenzyme Q10 status, serum amyloid-β, and tau protein in patients with dementia. Front Aging Neurosci. 2022 Jul 25;14:910289. doi: 10.3389/fnagi.2022.910289[↩]
- Dahri M, Tarighat-Esfanjani A, Asghari-Jafarabadi M, Hashemilar M. Oral coenzyme Q10 supplementation in patients with migraine: Effects on clinical features and inflammatory markers. Nutr Neurosci. 2019 Sep;22(9):607-615. doi: 10.1080/1028415X.2017.1421039[↩][↩][↩][↩][↩][↩]
- Al Saadi T, Assaf Y, Farwati M, Turkmani K, Al-Mouakeh A, Shebli B, Khoja M, Essali A, Madmani ME. Coenzyme Q10 for heart failure. Cochrane Database Syst Rev. 2021 Feb 3;(2)(2):CD008684. doi: 10.1002/14651858.CD008684.pub3[↩]
- Rauchová H. Coenzyme Q10 effects in neurological diseases. Physiol Res. 2021 Dec 30;70(Suppl4):S683-S714. doi: 10.33549/physiolres.934712[↩]
- Ho CC, Tseng CY, Chen HW, Chiu YW, Tsai MC, Chang PS, Lin PT. Coenzyme Q10 status, glucose parameters, and antioxidative capacity in college athletes. J Int Soc Sports Nutr. 2020 Jan 10;17(1):5. doi: 10.1186/s12970-020-0334-3[↩]
- Cordero MD, Santos-García R, Bermejo-Jover D, Sánchez-Domínguez B, Jaramillo-Santos MR, Bullón P. Coenzyme Q10 in salivary cells correlate with blood cells in Fibromyalgia: improvement in clinical and biochemical parameter after oral treatment. Clin Biochem. 2012 Apr;45(6):509-11. doi: 10.1016/j.clinbiochem.2012.02.001[↩]
- Jafari M, Mousavi SM, Asgharzadeh A, Yazdani N. Coenzyme Q10 in the treatment of heart failure: A systematic review of systematic reviews. Indian Heart J. 2018 Jul;70 Suppl 1(Suppl 1):S111-S117. doi: 10.1016/j.ihj.2018.01.031[↩][↩][↩][↩][↩][↩]
- Garrido-Maraver J, Cordero MD, Oropesa-Ávila M, Fernández Vega A, de la Mata M, Delgado Pavón A, de Miguel M, Pérez Calero C, Villanueva Paz M, Cotán D, Sánchez-Alcázar JA. Coenzyme q10 therapy. Mol Syndromol. 2014 Jul;5(3-4):187-97. doi: 10.1159/000360101[↩][↩]
- Niklowitz P, Sonnenschein A, Janetzky B, Andler W, Menke T. Enrichment of coenzyme Q10 in plasma and blood cells: defence against oxidative damage. International Journal of Biological Sciences 2007;3(4):257-62.[↩][↩]
- Rosenfeldt FL, Haas SJ, Krum H, Hadj A, Ng K, Leong J-Y, et al. Coenzyme Q10 in the treatment of hypertension: a meta-analysis of the clinical trials. Journal of Human Hypertension 2007;21:297–306.[↩]
- McCarty MF. Coenzyme Q versus hypertension: does CoQ decrease endothelial superoxide generation?. Medical Hypotheses 1999;53(4):300-4.[↩]
- Gao L, Mao Q, Cao J, Wang Y, Zhou X, Fan L. Effects of coenzyme Q10 on vascular endothelial function in humans: a meta-analysis of randomized controlled trials. Atherosclerosis 2012;221(2):311-6.[↩]
- Ignarro LJ. Biological actions and properties of endothelium-derived nitric oxide formed and released from artery and vein. Circulation Research 1989;65:1-21.[↩]
- Kato T, Yoneda S. Reduction in blood viscosity by treatment with coenzyme Q10 in patients with ischemic heart disease. International Journal of Clinical Pharmacology, Therapy and Toxicology 1990;28(3):123-6.[↩]
- Turunen M, Wehlin L, Sjoberg M, Lundahl J, Dallner G, Brismar K, et al. Beta2-Integrin and lipid modifications indicate a non-antioxidant mechanism for the anti-atherogenic effect of dietary coenzyme Q10. Biochemical and Biophysical Research Communications 2002;296:255-60.[↩]
- Correction to: 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2022 Sep 27;146(13):e185. doi: 10.1161/CIR.0000000000001097. Epub 2022 Sep 26. Erratum for: Circulation. 2022 May 3;145(18):e895-e1032. doi: 10.1161/CIR.0000000000001063[↩][↩][↩][↩][↩]
- Bhatt KN, Butler J. Myocardial Energetics and Heart Failure: a Review of Recent Therapeutic Trials. Curr Heart Fail Rep. 2018 Jun;15(3):191-197. doi: 10.1007/s11897-018-0386-8[↩][↩]
- Belardinelli R, Muçaj A, Lacalaprice F, Solenghi M, Seddaiu G, Principi F, Tiano L, Littarru GP. Coenzyme Q10 and exercise training in chronic heart failure. Eur Heart J. 2006 Nov;27(22):2675-81. doi: 10.1093/eurheartj/ehl158[↩][↩]
- Dai YL, Luk TH, Yiu KH, Wang M, Yip PM, Lee SW, Li SW, Tam S, Fong B, Lau CP, Siu CW, Tse HF. Reversal of mitochondrial dysfunction by coenzyme Q10 supplement improves endothelial function in patients with ischaemic left ventricular systolic dysfunction: a randomized controlled trial. Atherosclerosis. 2011 Jun;216(2):395-401. doi: 10.1016/j.atherosclerosis.2011.02.013[↩][↩][↩][↩]
- Zozina VI, Covantev S, Goroshko OA, Krasnykh LM, Kukes VG. Coenzyme Q10 in Cardiovascular and Metabolic Diseases: Current State of the Problem. Curr Cardiol Rev. 2018;14(3):164-174. doi: 10.2174/1573403X14666180416115428[↩][↩]
- Watts GF, Playford DA, Croft KD, Ward NC, Mori TA, Burke V. Coenzyme Q(10) improves endothelial dysfunction of the brachial artery in Type II diabetes mellitus. Diabetologia. 2002 Mar;45(3):420-6. doi: 10.1007/s00125-001-0760-y[↩][↩]
- Ayers J, Cook J, Koenig RA, Sisson EM, Dixon DL. Recent Developments in the Role of Coenzyme Q10 for Coronary Heart Disease: a Systematic Review. Curr Atheroscler Rep. 2018 May 16;20(6):29. doi: 10.1007/s11883-018-0730-1[↩][↩]
- Alehagen U, Aaseth J, Alexander J, Johansson P. Still reduced cardiovascular mortality 12 years after supplementation with selenium and coenzyme Q10 for four years: A validation of previous 10-year follow-up results of a prospective randomized double-blind placebo-controlled trial in elderly. PLoS One. 2018 Apr 11;13(4):e0193120. doi: 10.1371/journal.pone.0193120[↩][↩][↩]
- Wong AP, Kassab YW, Mohamed AL, Abdul Qader AM. Review: Beyond conventional therapies: Complementary and alternative medicine in the management of hypertension: An evidence-based review. Pak J Pharm Sci. 2018 Jan;31(1):237-244.[↩][↩][↩]
- Cordero MD, Alcocer-Gómez E, de Miguel M, Culic O, Carrión AM, Alvarez-Suarez JM, Bullón P, Battino M, Fernández-Rodríguez A, Sánchez-Alcazar JA. Can coenzyme q10 improve clinical and molecular parameters in fibromyalgia? Antioxid Redox Signal. 2013 Oct 20;19(12):1356-61. doi: 10.1089/ars.2013.5260[↩][↩]
- Cordero MD, Alcocer-Gómez E, de Miguel M, Cano-García FJ, Luque CM, Fernández-Riejo P, Fernández AM, Sánchez-Alcazar JA. Coenzyme Q(10): a novel therapeutic approach for Fibromyalgia? case series with 5 patients. Mitochondrion. 2011 Jul;11(4):623-5. doi: 10.1016/j.mito.2011.03.122[↩][↩]
- Glover EI, Martin J, Maher A, Thornhill RE, Moran GR, Tarnopolsky MA. A randomized trial of coenzyme Q10 in mitochondrial disorders. Muscle Nerve. 2010 Nov;42(5):739-48. doi: 10.1002/mus.21758[↩][↩]
- Safarinejad MR. Safety and efficacy of coenzyme Q10 supplementation in early chronic Peyronie’s disease: a double-blind, placebo-controlled randomized study. Int J Impot Res. 2010 Sep-Oct;22(5):298-309. doi: 10.1038/ijir.2010.20[↩][↩][↩]
- Zaleski AL, Taylor BA, Thompson PD. Coenzyme Q10 as Treatment for Statin-Associated Muscle Symptoms-A Good Idea, but…. Adv Nutr. 2018 Jul 1;9(4):519S-523S. doi: 10.1093/advances/nmy010[↩][↩]
- Skarlovnik A, Janić M, Lunder M, Turk M, Šabovič M. Coenzyme Q10 supplementation decreases statin-related mild-to-moderate muscle symptoms: a randomized clinical study. Med Sci Monit. 2014 Nov 6;20:2183-8. doi: 10.12659/MSM.890777[↩][↩][↩][↩]
- Mizuno K, Tanaka M, Nozaki S, Mizuma H, Ataka S, Tahara T, Sugino T, Shirai T, Kajimoto Y, Kuratsune H, Kajimoto O, Watanabe Y. Antifatigue effects of coenzyme Q10 during physical fatigue. Nutrition. 2008 Apr;24(4):293-9. doi: 10.1016/j.nut.2007.12.007. Epub 2008 Feb 13. Erratum in: Nutrition. 2008 Jun;24(6):616.[↩][↩]
- Hershey AD, Powers SW, Vockell AL, Lecates SL, Ellinor PL, Segers A, Burdine D, Manning P, Kabbouche MA. Coenzyme Q10 deficiency and response to supplementation in pediatric and adolescent migraine. Headache. 2007 Jan;47(1):73-80. doi: 10.1111/j.1526-4610.2007.00652.x[↩][↩][↩]
- Yaghini O, Hoseini N, Ghazavi MR, Mansouri V, Nasiri J, Moosavian T, Salehi MM. A Comparative Study on the Efficacy of Coenzyme Q10 and Amitriptyline in the Prophylactic Treatment of Migraine Headaches in Children: A Randomized Controlled Trial. Adv Biomed Res. 2022 May 30;11:43. doi: 10.4103/abr.abr_235_20[↩][↩]
- Sándor PS, Di Clemente L, Coppola G, Saenger U, Fumal A, Magis D, Seidel L, Agosti RM, Schoenen J. Efficacy of coenzyme Q10 in migraine prophylaxis: a randomized controlled trial. Neurology. 2005 Feb 22;64(4):713-5. doi: 10.1212/01.WNL.0000151975.03598.ED[↩][↩][↩][↩]
- Shoeibi A, Olfati N, Soltani Sabi M, Salehi M, Mali S, Akbari Oryani M. Effectiveness of coenzyme Q10 in prophylactic treatment of migraine headache: an open-label, add-on, controlled trial. Acta Neurol Belg. 2017 Mar;117(1):103-109. doi: 10.1007/s13760-016-0697-z[↩][↩][↩]
- Chase M, Cocchi MN, Liu X, Andersen LW, Holmberg MJ, Donnino MW. Coenzyme Q10 in acute influenza. Influenza Other Respir Viruses. 2019 Jan;13(1):64-70. doi: 10.1111/irv.12608[↩][↩]
- Mehrpooya M, Yasrebifar F, Haghighi M, Mohammadi Y, Jahangard L. Evaluating the Effect of Coenzyme Q10 Augmentation on Treatment of Bipolar Depression: A Double-Blind Controlled Clinical Trial. J Clin Psychopharmacol. 2018 Oct;38(5):460-466. doi: 10.1097/JCP.0000000000000938[↩][↩]
- Izadi A, Ebrahimi S, Shirazi S, Taghizadeh S, Parizad M, Farzadi L, Gargari BP. Hormonal and Metabolic Effects of Coenzyme Q10 and/or Vitamin E in Patients With Polycystic Ovary Syndrome. J Clin Endocrinol Metab. 2019 Feb 1;104(2):319-327. doi: 10.1210/jc.2018-01221[↩][↩]
- Coenzyme Q10. https://lpi.oregonstate.edu/mic/dietary-factors/coenzyme-Q10[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Campisi L, La Motta C. The Use of the Coenzyme Q10 as a Food Supplement in the Management of Fibromyalgia: A Critical Review. Antioxidants (Basel). 2022 Sep 30;11(10):1969. doi: 10.3390/antiox11101969[↩][↩][↩]
- Pepping J. Coenzyme Q10. Am J Health Syst Pharm. 1999 Mar 15;56(6):519-21. doi: 10.1093/ajhp/56.6.519[↩][↩][↩][↩][↩][↩][↩]
- Overvad K, Diamant B, Holm L, Holmer G, Mortensen SA, Stender S. Coenzyme Q10 in health and disease. Eur J Clin Nutr. 1999 Oct;53(10):764-70. doi: 10.1038/sj.ejcn.1600880[↩][↩][↩][↩][↩]
- Jolliet P, Simon N, Barré J, Pons JY, Boukef M, Paniel BJ, Tillement JP. Plasma coenzyme Q10 concentrations in breast cancer: prognosis and therapeutic consequences. Int J Clin Pharmacol Ther. 1998 Sep;36(9):506-9.[↩]
- Crane FL, Sun IL, Sun EE. The essential functions of coenzyme Q. Clin Investig. 1993;71(8 Suppl):S55-9. doi: 10.1007/BF00226841[↩]
- Folkers K, Wolaniuk A. Research on coenzyme Q10 in clinical medicine and in immunomodulation. Drugs Exp Clin Res. 1985;11(8):539-45.[↩][↩][↩]
- Beyer RE, Nordenbrand K, Ernster L: The role of coenzyme Q as a mitochondrial antioxidant: a short review. In: Folkers K, Yamamura Y, eds.: Biomedical and Clinical Aspects of Coenzyme Q. Vol 5. Elsevier Science Publishers B V (Biomedical Division), 1986, pp 17-24.[↩][↩]
- Gordon M. Dietary antioxidants in disease prevention. Nat Prod Rep. 1996 Aug;13(4):265-73. doi: 10.1039/np9961300265[↩][↩]
- Ernster L, Dallner G. Biochemical, physiological and medical aspects of ubiquinone function. Biochim Biophys Acta. 1995 May 24;1271(1):195-204. doi: 10.1016/0925-4439(95)00028-3[↩][↩][↩]
- PDQ Integrative, Alternative, and Complementary Therapies Editorial Board. Coenzyme Q10 (PDQ®): Health Professional Version. 2024 Oct 31. In: PDQ Cancer Information Summaries [Internet]. Bethesda (MD): National Cancer Institute (US); 2002-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK65890[↩][↩][↩][↩]
- Coulter I, Hardy M, Shekelle P, et al. Effect of the Supplemental Use of Antioxidants Vitamin C, Vitamin E, and Coenzyme Q10 for the Prevention and Treatment of Cancer. Rockville (MD): Agency for Healthcare Research and Quality (US); 2003 Aug. (Evidence Reports/Technology Assessments, No. 75.) Available from: https://www.ncbi.nlm.nih.gov/books/NBK36859[↩][↩]
- PDQ Integrative, Alternative, and Complementary Therapies Editorial Board. Coenzyme Q10 (PDQ®): Health Professional Version. 2024 Apr 5. In: PDQ Cancer Information Summaries [Internet]. Bethesda (MD): National Cancer Institute (US); 2002-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK65890[↩][↩][↩][↩][↩]
- Palazzoni G, Pucello D, Littarru GP, Nardone L, Marin AW, Romagnoli A. Coenzyme Q10 and colorectal neoplasms in aged patients. Rays. 1997 Jan-Mar;22(1 Suppl):73-6.[↩]
- Qu H, Guo M, Chai H, Wang WT, Gao ZY, Shi DZ. Effects of Coenzyme Q10 on Statin-Induced Myopathy: An Updated Meta-Analysis of Randomized Controlled Trials. J Am Heart Assoc. 2018 Oct 2;7(19):e009835. doi: 10.1161/JAHA.118.009835[↩][↩]
- Weber C. Dietary intake and absorption of coenzyme Q. In: Kagan VE, Quinn PJ, eds. Coenzyme Q: Molecular Mechanisms in Health and Disease. Boca Raton: CRC Press; 2001:209-215.[↩]
- Pravst I, Zmitek K, Zmitek J. Coenzyme Q10 contents in foods and fortification strategies. Crit Rev Food Sci Nutr. 2010 Apr;50(4):269-80. doi: 10.1080/10408390902773037[↩][↩]
- Niklowitz P, Sonnenschein A, Janetzky B, Andler W, Menke T. Enrichment of coenzyme Q10 in plasma and blood cells: defense against oxidative damage. International Journal of Biological Sciences 2007;3(4):257-62.[↩]
- Bhagavan H.N., Chopra R.K. Coenzyme Q10: Absorption, tissue uptake, metabolism and pharmacokinetics. Free Radic. Res. 2006;40:445–453. doi: 10.1080/10715760600617843[↩]
- Flowers N., Hartley L., Todkill D., Stranges S., Rees K. Co-enzyme Q10 supplementation for the primary prevention of cardiovascular disease. Cochrane Database Syst. Rev. 2014;12:CD010405 https://www.ncbi.nlm.nih.gov/pubmed/25474484[↩]
- Kędziora-Kornatowska K, Czuczejko J, Motyl J, Szewczyk-Golec K, Kozakiewicz M, Pawluk H, Kędziora J, Błaszczak R, Banach M, Rysz J. Effects of coenzyme Q10 supplementation on activities of selected antioxidative enzymes and lipid peroxidation in hypertensive patients treated with indapamide. A pilot study. Arch Med Sci. 2010 Aug 30;6(4):513-8. doi: 10.5114/aoms.2010.14461[↩]
- Cordero MD, Cano-García FJ, Alcocer-Gómez E, De Miguel M, Sánchez-Alcázar JA. Oxidative stress correlates with headache symptoms in fibromyalgia: coenzyme Q₁₀ effect on clinical improvement. PLoS One. 2012;7(4):e35677. doi: 10.1371/journal.pone.0035677[↩]
- Crane FL. The evolution of coenzyme Q. Biofactors. 2008;32(1-4):5-11. doi: 10.1002/biof.5520320102[↩]
- Yoneda T., Tomofuji T., Kawabata Y., Ekuni D., Azuma T., Kataoka K., Kunitomo M., Morita M. Application of coenzyme Q10 for accelerating soft tissue wound healing after tooth extraction in rats. Nutrients. 2014;6:5756–5769. doi: 10.3390/nu6125756[↩]
- Fouad A.A., Al-Mulhim A.S., Jresat I. Therapeutic effect of coenzyme Q10 against experimentally-induced hepatocellular carcinoma in rats. Environ. Toxicol. Pharmacol. 2013;35:100–108. doi: 10.1016/j.etap.2012.11.016[↩]
- Schniertshauer D, Müller S, Mayr T, Sonntag T, Gebhard D, Bergemann J. Accelerated Regeneration of ATP Level after Irradiation in Human Skin Fibroblasts by Coenzyme Q10. Photochem Photobiol. 2016 May;92(3):488-94. doi: 10.1111/php.12583[↩]
- Usui T, Ishikura H, Izumi Y, Konishi H, Dohmae N, Sawada H, Uchino H, Matsuda H, Konishi T. Possible prevention from the progression of cardiotoxicity in adriamycin-treated rabbits by coenzyme Q10. Toxicol Lett. 1982 Jun;12(1):75-82. doi: 10.1016/0378-4274(82)90201-6[↩][↩]
- Iwamoto Y, Hansen IL, Porter TH, Folkers K. Inhibition of coenzyme Q10-enzymes, succinoxidase and NADH-oxidase, by adriamycin and other quinones having antitumor activity. Biochem Biophys Res Commun. 1974 Jun 4;58(3):633-8. doi: 10.1016/s0006-291x(74)80465-1[↩][↩]
- Acosta MJ, Vazquez Fonseca L, Desbats MA, Cerqua C, Zordan R, Trevisson E, Salviati L. Coenzyme Q biosynthesis in health and disease. Biochim Biophys Acta. 2016 Aug;1857(8):1079-1085. doi: 10.1016/j.bbabio.2016.03.036[↩]
- Nohl H, Gille L. The role of coenzyme Q in lysosomes. In: Kagan VEQ, P. J., ed. Coenzyme Q: Molecular Mechanisms in Health and Disease. Boca Raton: CRC Press; 2001:99-106.[↩]
- Crane FL. Biochemical functions of coenzyme Q10. J Am Coll Nutr. 2001 Dec;20(6):591-8. doi: 10.1080/07315724.2001.10719063[↩]
- Verhagen H, Buijsse B, Jansen E, Bueno-de-Mesquita B. The state of antioxidant affairs. Nutr Today 2006;41:244-50.[↩]
- Navas P, Villalba JM, de Cabo R. The importance of plasma membrane coenzyme Q in aging and stress responses. Mitochondrion. 2007 Jun;7 Suppl:S34-40. doi: 10.1016/j.mito.2007.02.010[↩][↩]
- Thomas SR, Stocker R. Mechanisms of antioxidant action of ubiquinol-10 for low-density lipoprotein. In: Kagan VE, Quinn PJ, eds. Coenzyme Q: Molecular Mechanisms in Health and Disease. Boca Raton: CRC Press; 2001:131-150.[↩][↩]
- Fazakerley DJ, Chaudhuri R, Yang P, et al. Mitochondrial CoQ deficiency is a common driver of mitochondrial oxidants and insulin resistance. Elife. 2018 Feb 6;7:e32111. doi: 10.7554/eLife.32111[↩][↩]
- Bhagavan HN, Chopra RK. Coenzyme Q10: absorption, tissue uptake, metabolism and pharmacokinetics. Free Radic Res. 2006 May;40(5):445-53. doi: 10.1080/10715760600617843[↩]
- Kalén A, Appelkvist EL, Dallner G. Age-related changes in the lipid compositions of rat and human tissues. Lipids. 1989 Jul;24(7):579-84. doi: 10.1007/BF02535072[↩][↩]
- Hernández-Camacho JD, Bernier M, López-Lluch G, Navas P. Coenzyme Q10 Supplementation in Aging and Disease. Front Physiol. 2018 Feb 5;9:44. doi: 10.3389/fphys.2018.00044[↩]
- Desbats MA, Lunardi G, Doimo M, Trevisson E, Salviati L. Genetic bases and clinical manifestations of coenzyme Q10 (CoQ 10) deficiency. J Inherit Metab Dis. 2015 Jan;38(1):145-56. doi: 10.1007/s10545-014-9749-9[↩][↩][↩]
- Hargreaves IP. Coenzyme Q10 as a therapy for mitochondrial disease. Int J Biochem Cell Biol. 2014 Apr;49:105-11. doi: 10.1016/j.biocel.2014.01.020[↩][↩][↩][↩]
- Matsuoka T, Maeda H, Goto Y, Nonaka I. Muscle coenzyme Q10 in mitochondrial encephalomyopathies. Neuromuscul Disord. 1991;1:443–447. doi: 10.1016/0960-8966(91)90007-F[↩][↩]
- Sacconi S, Trevisson E, Salviati L, Aymé S, Rigal O, Redondo AG, et al. Coenzyme Q10 is frequently reduced in muscle of patients with mitochondrial myopathy. Neuromuscul Disord. 2010;20:44–48. doi: 10.1016/j.nmd.2009.10.014[↩][↩]
- Montero R, Grazina M, López-Gallardo E, Montoya J, Briones P, Navarro-Sastre A, et al. Coenzyme Q10 deficiency in mitochondrial DNA depletion syndromes. Mitochondrion. 2013;13:337–341. doi: 10.1016/j.mito.2013.04.001[↩][↩]
- Quinzii CM, Kattah AG, Naini A, Akman HO, Mootha VK, DiMauro S, et al. Coenzyme Q deficiency and cerebellar ataxia associated with an aprataxin mutation. Neurology. 2005;64:539–541. doi: 10.1212/01.WNL.0000150588.75281.58[↩][↩]
- Gempel K, Topaloglu H, Talim B, Schneiderat P, Schoser BG, Hans VH, et al. The myopathic form of coenzyme Q10 deficiency is caused by mutations in the electron-transferring-flavoprotein dehydrogenase (ETFDH) gene. Brain. 2007;130:2037–2044. doi: 10.1093/brain/awm054[↩][↩]
- Liang WC, Ohkuma A, Hayashi YK, López LC, Hirano M, Nonaka I, et al. ETFDH mutations, CoQ10 levels, and respiratory chain activities in patients with riboflavin-responsive multiple acyl-CoA dehydrogenase deficiency. Neuromuscul Disord. 2009;19:212–216. doi: 10.1016/j.nmd.2009.01.008[↩][↩]
- Aeby A, Sznajer Y, Cavé H, Rebuffat E, Van Coster R, Rigal O, et al. Cardiofaciocutaneous (CFC) syndrome associated with muscular coenzyme Q10 deficiency. J Inherit Metab Dis. 2007;30:827. doi: 10.1007/s10545-007-0612-0[↩][↩]
- Buján N, Arias A, Montero R, García-Villoria J, Lissens W, Seneca S, et al. Characterization of CoQ10 biosynthesis in fibroblasts of patients with primary and secondary CoQ10 deficiency. J Inherit Metab Dis. 2014;37:53–62. doi: 10.1007/s10545-013-9620-4[↩][↩]
- Salviati L, Trevisson E, Agosto C, et al. Primary Coenzyme Q10 Deficiency Overview. 2017 Jan 26 [Updated 2023 Jun 8]. In: Adam MP, Feldman J, Mirzaa GM, et al., editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2025. Available from: https://www.ncbi.nlm.nih.gov/books/NBK410087[↩][↩][↩][↩][↩]
- Yuruk Yildirim Z, Toksoy G, Uyguner O, Nayir A, Yavuz S, Altunoglu U, Turkkan ON, Sevinc B, Gokcay G, Kurkcu Gunes D, Kiyak A, Yilmaz A. Primary coenzyme Q10 Deficiency-6 (COQ10D6): Two siblings with variable expressivity of the renal phenotype. Eur J Med Genet. 2020 Jan;63(1):103621. doi: 10.1016/j.ejmg.2019.01.011[↩][↩][↩]
- Primary coenzyme Q10 deficiency. https://medlineplus.gov/genetics/condition/primary-coenzyme-q10-deficiency[↩][↩][↩][↩][↩]
- Rötig A, Appelkvist EL, Geromel V, Chretien D, Kadhom N, Edery P, Lebideau M, Dallner G, Munnich A, Ernster L, Rustin P. Quinone-responsive multiple respiratory-chain dysfunction due to widespread coenzyme Q10 deficiency. Lancet. 2000 Jul 29;356(9227):391-5. doi: 10.1016/S0140-6736(00)02531-9[↩]
- Salviati L, Sacconi S, Murer L, Zacchello G, Franceschini L, Laverda AM, Basso G, Quinzii C, Angelini C, Hirano M, Naini AB, Navas P, DiMauro S, Montini G. Infantile encephalomyopathy and nephropathy with CoQ10 deficiency: a CoQ10-responsive condition. Neurology. 2005 Aug 23;65(4):606-8. doi: 10.1212/01.wnl.0000172859.55579.a7[↩]
- Heeringa SF, Chernin G, Chaki M, et al. COQ6 mutations in human patients produce nephrotic syndrome with sensorineural deafness. J Clin Invest. 2011 May;121(5):2013-24. doi: 10.1172/JCI45693[↩][↩]
- Gigante M, Diella S, Santangelo L, Trevisson E, Acosta MJ, Amatruda M, Finzi G, Caridi G, Murer L, Accetturo M, Ranieri E, Ghiggeri GM, Giordano M, Grandaliano G, Salviati L, Gesualdo L. Further phenotypic heterogeneity of CoQ10 deficiency associated with steroid resistant nephrotic syndrome and novel COQ2 and COQ6 variants. Clin Genet. 2017 Aug;92(2):224-226. doi: 10.1111/cge.12960[↩]
- Salviati L, Trevisson E, Agosto C, et al. Primary Coenzyme Q10 Deficiency Overview. 2017 Jan 26 [Updated 2023 Jun 8]. In: Adam MP, Feldman J, Mirzaa GM, et al., editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2024. Available from: https://www.ncbi.nlm.nih.gov/books/NBK410087[↩][↩][↩][↩][↩][↩][↩][↩]
- Montini G, Malaventura C, Salviati L. Early coenzyme Q10 supplementation in primary coenzyme Q10 deficiency. N Engl J Med. 2008 Jun 26;358(26):2849-50. doi: 10.1056/NEJMc0800582[↩][↩]
- Ashraf S, Gee HY, Woerner S, et al. ADCK4 mutations promote steroid-resistant nephrotic syndrome through CoQ10 biosynthesis disruption. J Clin Invest. 2013 Dec;123(12):5179-89. doi: 10.1172/JCI69000[↩]
- Fragaki K, Chaussenot A, Benoist JF, Ait-El-Mkadem S, Bannwarth S, Rouzier C, Cochaud C, Paquis-Flucklinger V. Coenzyme Q10 defects may be associated with a deficiency of Q10-independent mitochondrial respiratory chain complexes. Biol Res. 2016 Jan 8;49:4. doi: 10.1186/s40659-015-0065-0[↩]
- Banach M, Serban C, Sahebkar A, Ursoniu S, Rysz J, Muntner P, Toth PP, Jones SR, Rizzo M, Glasser SP, Lip GY, Dragan S, Mikhailidis DP; Lipid and Blood Pressure Meta-analysis Collaboration Group. Effects of coenzyme Q10 on statin-induced myopathy: a meta-analysis of randomized controlled trials. Mayo Clin Proc. 2015 Jan;90(1):24-34. doi: 10.1016/j.mayocp.2014.08.021[↩]
- Potgieter M, Pretorius E, Pepper MS. Primary and secondary coenzyme Q10 deficiency: the role of therapeutic supplementation. Nutr Rev. 2013 Mar;71(3):180-8. doi: 10.1111/nure.12011[↩]
- Gempel K, Topaloglu H, Talim B, Schneiderat P, Schoser BG, Hans VH, Pálmafy B, Kale G, Tokatli A, Quinzii C, Hirano M, Naini A, DiMauro S, Prokisch H, Lochmüller H, Horvath R. The myopathic form of coenzyme Q10 deficiency is caused by mutations in the electron-transferring-flavoprotein dehydrogenase (ETFDH) gene. Brain. 2007 Aug;130(Pt 8):2037-44. doi: 10.1093/brain/awm054[↩]
- Pineda M, Montero R, Aracil A, O’Callaghan MM, Mas A, Espinos C, Martinez-Rubio D, Palau F, Navas P, Briones P, Artuch R. Coenzyme Q(10)-responsive ataxia: 2-year-treatment follow-up. Mov Disord. 2010 Jul 15;25(9):1262-8. doi: 10.1002/mds.23129[↩]
- PDQ Integrative, Alternative, and Complementary Therapies Editorial Board. Coenzyme Q10 (PDQ®): Patient Version. 2024 May 28. In: PDQ Cancer Information Summaries [Internet]. Bethesda (MD): National Cancer Institute (US); 2002-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK65828[↩][↩][↩]
- Ambrosone CB, Zirpoli GR, Hutson AD, McCann WE, McCann SE, Barlow WE, Kelly KM, Cannioto R, Sucheston-Campbell LE, Hershman DL, Unger JM, Moore HCF, Stewart JA, Isaacs C, Hobday TJ, Salim M, Hortobagyi GN, Gralow JR, Budd GT, Albain KS. Dietary Supplement Use During Chemotherapy and Survival Outcomes of Patients With Breast Cancer Enrolled in a Cooperative Group Clinical Trial (SWOG S0221). J Clin Oncol. 2020 Mar 10;38(8):804-814. doi: 10.1200/JCO.19.01203[↩]
- Littarru GP, Tiano L. Clinical aspects of coenzyme Q10: an update. Curr Opin Clin Nutr Metab Care . 2005;8(6):641-646.[↩]
- Marcoff L, Thompson PD. The role of coenzyme Q10 in statin-associated myopathy: a systematic review. J Am Coll Cardiol . 2007;49(23):2231-2237.[↩][↩][↩][↩]
- Caso G, Kelly P, McNurlan MA, Lawson WE. Effect of coenzyme q10 on myopathic symptoms in patients treated with statins. Am J Cardiol . 2007;99(10):1409-1412.[↩]
- Marriage B, Clandinin MT, Glerum DM. Nutritional cofactor treatment in mitochondrial disorders. J Am Diet Assoc . 2003;103(8):1029-1038.[↩]
- Quinzii CM, López LC, Naini A, DiMauro S, Hirano M. Human CoQ10 deficiencies. Biofactors . 2008;32(1-4):113-118.[↩][↩]
- Schapira AH. Mitochondrial disease. Lancet . 2006;368(9529):70-82.[↩][↩]
- Schapira AH, Olanow CW. Neuroprotection in Parkinson disease: mysteries, myths, and misconceptions. JAMA . 2004;291(3):358-364.[↩]
- Shults CW, Oakes D, Kieburtz K, et al; Parkinson Study Group. Effects of coenzyme Q10 in early Parkinson disease: evidence of slowing of the functional decline. Arch Neurol . 2002;59(10):1541-1550.[↩][↩]
- LeWitt PA. Clinical trials of neuroprotection for Parkinson’s disease. Neurology . 2004;63(7 suppl 2):S23-S31.[↩]
- NINDS NET-PD Investigators. A randomized clinical trial of coenzyme Q10 and GPI-1485 in early Parkinson disease. Neurology . 2007;68(1):20-28.[↩][↩]
- Storch A, Jost WH, Vieregge P, et al; German Coenzyme Q(10) Study Group. Randomized, double-blind, placebo-controlled trial on symptomatic effects of coenzyme Q(10) in Parkinson disease. Arch Neurol . 2007;64(7):938-944.[↩]
- Steele PE, Tang PH, DeGrauw AJ, Miles MV. Clinical laboratory monitoring of coenzyme Q10 use in neurologic and muscular diseases. Am J Clin Pathol . 2004;121(suppl):S113-S120.[↩]
- Thal LJ, Grundman M, Berg J, et al. Idebenone treatment fails to slow cognitive decline in Alzheimer’s disease. Neurology . 2003;61(11):1498-1502.[↩]
- Henchcliffe C, Beal MF. Mitochondrial biology and oxidative stress in Parkinson disease pathogenesis. Nat Clin Pract Neurol. 2008 Nov;4(11):600-9. doi: 10.1038/ncpneuro0924[↩]
- Götz ME, Gerstner A, Harth R, Dirr A, Janetzky B, Kuhn W, Riederer P, Gerlach M. Altered redox state of platelet coenzyme Q10 in Parkinson’s disease. J Neural Transm (Vienna). 2000;107(1):41-8. doi: 10.1007/s007020050003[↩]
- Shults CW, Haas RH, Passov D, Beal MF. Coenzyme Q10 levels correlate with the activities of complexes I and II/III in mitochondria from parkinsonian and nonparkinsonian subjects. Ann Neurol. 1997 Aug;42(2):261-4. doi: 10.1002/ana.410420221[↩]
- Isobe C, Abe T, Terayama Y. Levels of reduced and oxidized coenzyme Q-10 and 8-hydroxy-2′-deoxyguanosine in the cerebrospinal fluid of patients with living Parkinson’s disease demonstrate that mitochondrial oxidative damage and/or oxidative DNA damage contributes to the neurodegenerative process. Neurosci Lett. 2010 Jan 18;469(1):159-63. doi: 10.1016/j.neulet.2009.11.065[↩]
- Hargreaves IP, Lane A, Sleiman PM. The coenzyme Q10 status of the brain regions of Parkinson’s disease patients. Neurosci Lett. 2008 Dec 5;447(1):17-9. doi: 10.1016/j.neulet.2008.09.069[↩]
- Shults CW, Oakes D, Kieburtz K, Beal MF, Haas R, Plumb S, Juncos JL, Nutt J, Shoulson I, Carter J, Kompoliti K, Perlmutter JS, Reich S, Stern M, Watts RL, Kurlan R, Molho E, Harrison M, Lew M; Parkinson Study Group. Effects of coenzyme Q10 in early Parkinson disease: evidence of slowing of the functional decline. Arch Neurol. 2002 Oct;59(10):1541-50. doi: 10.1001/archneur.59.10.1541[↩]
- Parkinson Study Group QE3 Investigators; Beal MF, Oakes D, Shoulson I, et al. A randomized clinical trial of high-dosage coenzyme Q10 in early Parkinson disease: no evidence of benefit. JAMA Neurol. 2014 May;71(5):543-52. doi: 10.1001/jamaneurol.2014.131[↩]
- Yoritaka A, Kawajiri S, Yamamoto Y, Nakahara T, Ando M, Hashimoto K, Nagase M, Saito Y, Hattori N. Randomized, double-blind, placebo-controlled pilot trial of reduced coenzyme Q10 for Parkinson’s disease. Parkinsonism Relat Disord. 2015 Aug;21(8):911-6. doi: 10.1016/j.parkreldis.2015.05.022[↩]
- Negida A, Menshawy A, El Ashal G, Elfouly Y, Hani Y, Hegazy Y, El Ghonimy S, Fouda S, Rashad Y. Coenzyme Q10 for Patients with Parkinson’s Disease: A Systematic Review and Meta-Analysis. CNS Neurol Disord Drug Targets. 2016;15(1):45-53. doi: 10.2174/1871527314666150821103306[↩]
- Zhu ZG, Sun MX, Zhang WL, Wang WW, Jin YM, Xie CL. The efficacy and safety of coenzyme Q10 in Parkinson’s disease: a meta-analysis of randomized controlled trials. Neurol Sci. 2017 Feb;38(2):215-224. doi: 10.1007/s10072-016-2757-9[↩]
- Ferrante RJ, Andreassen OA, Dedeoglu A, Ferrante KL, Jenkins BG, Hersch SM, Beal MF. Therapeutic effects of coenzyme Q10 and remacemide in transgenic mouse models of Huntington’s disease. J Neurosci. 2002 Mar 1;22(5):1592-9. doi: 10.1523/JNEUROSCI.22-05-01592.2002[↩][↩]
- Stack EC, Smith KM, Ryu H, Cormier K, Chen M, Hagerty SW, Del Signore SJ, Cudkowicz ME, Friedlander RM, Ferrante RJ. Combination therapy using minocycline and coenzyme Q10 in R6/2 transgenic Huntington’s disease mice. Biochim Biophys Acta. 2006 Mar;1762(3):373-80. doi: 10.1016/j.bbadis.2005.11.002[↩][↩]
- Yang L, Calingasan NY, Wille EJ, Cormier K, Smith K, Ferrante RJ, Beal MF. Combination therapy with coenzyme Q10 and creatine produces additive neuroprotective effects in models of Parkinson’s and Huntington’s diseases. J Neurochem. 2009 Jun;109(5):1427-39. doi: 10.1111/j.1471-4159.2009.06074.x[↩]
- Huntington Study Group. A randomized, placebo-controlled trial of coenzyme Q10 and remacemide in Huntington’s disease. Neurology. 2001 Aug 14;57(3):397-404. doi: 10.1212/wnl.57.3.397[↩]
- Huntington Study Group Pre2CARE Investigators; Hyson HC, Kieburtz K, Shoulson I, et al. Safety and tolerability of high-dosage coenzyme Q10 in Huntington’s disease and healthy subjects. Mov Disord. 2010 Sep 15;25(12):1924-8. doi: 10.1002/mds.22408[↩][↩]
- McGarry A, McDermott M, Kieburtz K, et al. Huntington Study Group 2CARE Investigators and Coordinators. A randomized, double-blind, placebo-controlled trial of coenzyme Q10 in Huntington disease. Neurology. 2017 Jan 10;88(2):152-159. doi: 10.1212/WNL.0000000000003478[↩][↩][↩]
- Bürk K. Friedreich Ataxia: current status and future prospects. Cerebellum Ataxias. 2017 Apr 7;4:4. doi: 10.1186/s40673-017-0062-x[↩]
- Strawser C, Schadt K, Hauser L, McCormick A, Wells M, Larkindale J, Lin H, Lynch DR. Pharmacological therapeutics in Friedreich ataxia: the present state. Expert Rev Neurother. 2017 Sep;17(9):895-907. doi: 10.1080/14737175.2017.1356721[↩][↩]
- Lodi R, Hart PE, Rajagopalan B, Taylor DJ, Crilley JG, Bradley JL, Blamire AM, Manners D, Styles P, Schapira AH, Cooper JM. Antioxidant treatment improves in vivo cardiac and skeletal muscle bioenergetics in patients with Friedreich’s ataxia. Ann Neurol. 2001 May;49(5):590-6. https://doi.org/10.1002/ana.1001[↩]
- Hart PE, Lodi R, Rajagopalan B, Bradley JL, Crilley JG, Turner C, Blamire AM, Manners D, Styles P, Schapira AH, Cooper JM. Antioxidant treatment of patients with Friedreich ataxia: four-year follow-up. Arch Neurol. 2005 Apr;62(4):621-6. doi: 10.1001/archneur.62.4.621[↩]
- Cooper JM, Korlipara LV, Hart PE, Bradley JL, Schapira AH. Coenzyme Q10 and vitamin E deficiency in Friedreich’s ataxia: predictor of efficacy of vitamin E and coenzyme Q10 therapy. Eur J Neurol. 2008 Dec;15(12):1371-9. doi: 10.1111/j.1468-1331.2008.02318.x[↩]
- Bhandari J, Thada PK, Samanta D. Spinocerebellar Ataxia. [Updated 2023 Sep 15]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK557816[↩]
- Lo RY, Figueroa KP, Pulst SM, Lin CY, Perlman S, Wilmot G, Gomez C, Schmahmann J, Paulson H, Shakkottai VG, Ying S, Zesiewicz T, Bushara K, Geschwind M, Xia G, Subramony SH, Ashizawa T, Kuo SH. Coenzyme Q10 and spinocerebellar ataxias. Mov Disord. 2015 Feb;30(2):214-20. doi: 10.1002/mds.26088[↩][↩]
- Cornelius N, Wardman JH, Hargreaves IP, Neergheen V, Bie AS, Tümer Z, Nielsen JE, Nielsen TT. Evidence of oxidative stress and mitochondrial dysfunction in spinocerebellar ataxia type 2 (SCA2) patient fibroblasts: Effect of coenzyme Q10 supplementation on these parameters. Mitochondrion. 2017 May;34:103-114. doi: 10.1016/j.mito.2017.03.001[↩]
- Beckman KB, Ames BN. Mitochondrial aging: open questions. Ann N Y Acad Sci. 1998 Nov 20;854:118-27. doi: 10.1111/j.1749-6632.1998.tb09897.x[↩]
- Singh RB, Niaz MA, Kumar A, Sindberg CD, Moesgaard S, Littarru GP. Effect on absorption and oxidative stress of different oral Coenzyme Q10 dosages and intake strategy in healthy men. Biofactors. 2005;25(1-4):219-24. doi: 10.1002/biof.5520250127[↩][↩][↩][↩]
- Sohal RS, Kamzalov S, Sumien N, Ferguson M, Rebrin I, Heinrich KR, Forster MJ. Effect of coenzyme Q10 intake on endogenous coenzyme Q content, mitochondrial electron transport chain, antioxidative defenses, and life span of mice. Free Radic Biol Med. 2006 Feb 1;40(3):480-7. doi: 10.1016/j.freeradbiomed.2005.08.037[↩]
- Lapointe J, Hekimi S. Early mitochondrial dysfunction in long-lived Mclk1+/- mice. J Biol Chem. 2008 Sep 19;283(38):26217-27. doi: 10.1074/jbc.M803287200[↩]
- Schmelzer C, Kubo H, Mori M, Sawashita J, Kitano M, Hosoe K, Boomgaarden I, Döring F, Higuchi K. Supplementation with the reduced form of Coenzyme Q10 decelerates phenotypic characteristics of senescence and induces a peroxisome proliferator-activated receptor-alpha gene expression signature in SAMP1 mice. Mol Nutr Food Res. 2010 Jun;54(6):805-15. doi: 10.1002/mnfr.200900155[↩]
- Tian G, Sawashita J, Kubo H, Nishio SY, Hashimoto S, Suzuki N, Yoshimura H, Tsuruoka M, Wang Y, Liu Y, Luo H, Xu Z, Mori M, Kitano M, Hosoe K, Takeda T, Usami S, Higuchi K. Ubiquinol-10 supplementation activates mitochondria functions to decelerate senescence in senescence-accelerated mice. Antioxid Redox Signal. 2014 Jun 1;20(16):2606-20. doi: 10.1089/ars.2013.5406[↩]
- Johansson P, Dahlström Ö, Dahlström U, Alehagen U. Improved Health-Related Quality of Life, and More Days out of Hospital with Supplementation with Selenium and Coenzyme Q10 Combined. Results from a Double Blind, Placebo-Controlled Prospective Study. J Nutr Health Aging. 2015 Nov;19(9):870-7. doi: 10.1007/s12603-015-0509-9[↩]
- Sahebkar A, Simental-Mendía LE, Stefanutti C, Pirro M. Supplementation with coenzyme Q10 reduces plasma lipoprotein(a) concentrations but not other lipid indices: A systematic review and meta-analysis. Pharmacol Res. 2016 Mar;105:198-209. doi: 10.1016/j.phrs.2016.01.030[↩][↩]
- Mazidi M, Kengne AP, Banach M; Lipid and Blood Pressure Meta-analysis Collaboration Group. Effects of coenzyme Q10 supplementation on plasma C-reactive protein concentrations: A systematic review and meta-analysis of randomized controlled trials. Pharmacol Res. 2018 Feb;128:130-136. doi: 10.1016/j.phrs.2017.08.011[↩][↩]
- Suksomboon N, Poolsup N, Juanak N. Effects of coenzyme Q10 supplementation on metabolic profile in diabetes: a systematic review and meta-analysis. J Clin Pharm Ther. 2015 Aug;40(4):413-8. doi: 10.1111/jcpt.12280[↩]
- Shargorodsky M, Debby O, Matas Z, Zimlichman R. Effect of long-term treatment with antioxidants (vitamin C, vitamin E, coenzyme Q10 and selenium) on arterial compliance, humoral factors and inflammatory markers in patients with multiple cardiovascular risk factors. Nutr Metab (Lond). 2010 Jul 6;7:55. doi: 10.1186/1743-7075-7-55[↩]
- Traber MG. Vitamin E. In: Shils ME, Shike M, Ross AC, Caballero B, Cousins R, eds. Modern Nutrition in Health and Disease. 10th ed. Baltimore, MD: Lippincott Williams & Wilkins, 2006;396-411.[↩]
- Mohr D, Bowry VW, Stocker R. Dietary supplementation with coenzyme Q10 results in increased levels of ubiquinol-10 within circulating lipoproteins and increased resistance of human low-density lipoprotein to the initiation of lipid peroxidation. Biochim Biophys Acta. 1992 Jun 26;1126(3):247-54. doi: 10.1016/0005-2760(92)90237-p[↩]
- Witting PK, Pettersson K, Letters J, Stocker R. Anti-atherogenic effect of coenzyme Q10 in apolipoprotein E gene knockout mice. Free Radic Biol Med. 2000 Aug;29(3-4):295-305. doi: 10.1016/s0891-5849(00)00311-7[↩]
- Thomas SR, Leichtweis SB, Pettersson K, Croft KD, Mori TA, Brown AJ, Stocker R. Dietary cosupplementation with vitamin E and coenzyme Q(10) inhibits atherosclerosis in apolipoprotein E gene knockout mice. Arterioscler Thromb Vasc Biol. 2001 Apr;21(4):585-93. doi: 10.1161/01.atv.21.4.585[↩]
- Turunen M, Wehlin L, Sjöberg M, Lundahl J, Dallner G, Brismar K, Sindelar PJ. beta2-Integrin and lipid modifications indicate a non-antioxidant mechanism for the anti-atherogenic effect of dietary coenzyme Q10. Biochem Biophys Res Commun. 2002 Aug 16;296(2):255-60. doi: 10.1016/s0006-291x(02)00871-9[↩]
- Gao L, Mao Q, Cao J, Wang Y, Zhou X, Fan L. Effects of coenzyme Q10 on vascular endothelial function in humans: a meta-analysis of randomized controlled trials. Atherosclerosis. 2012 Apr;221(2):311-6. doi: 10.1016/j.atherosclerosis.2011.10.027[↩]
- Fan L, Feng Y, Chen GC, Qin LQ, Fu CL, Chen LH. Effects of coenzyme Q10 supplementation on inflammatory markers: A systematic review and meta-analysis of randomized controlled trials. Pharmacol Res. 2017 May;119:128-136. doi: 10.1016/j.phrs.2017.01.032[↩]
- Zhai J, Bo Y, Lu Y, Liu C, Zhang L. Effects of Coenzyme Q10 on Markers of Inflammation: A Systematic Review and Meta-Analysis. PLoS One. 2017 Jan 26;12(1):e0170172. doi: 10.1371/journal.pone.0170172[↩]
- Trupp RJ, Abraham WT. Congestive heart failure. In: Rakel RE, Bope ET, eds. Rakel: Conn’s Current Therapy 2002. 54th ed. New York: W. B. Saunders Company; 2002:306-313.[↩]
- McMurray JJ, Dunselman P, Wedel H, Cleland JG, Lindberg M, Hjalmarson A, Kjekshus J, Waagstein F, Apetrei E, Barrios V, Böhm M, Kamenský G, Komajda M, Mareev V, Wikstrand J; CORONA Study Group. Coenzyme Q10, rosuvastatin, and clinical outcomes in heart failure: a pre-specified substudy of CORONA (controlled rosuvastatin multinational study in heart failure). J Am Coll Cardiol. 2010 Oct 5;56(15):1196-204. doi: 10.1016/j.jacc.2010.02.075[↩]
- Lei L, Liu Y. Efficacy of coenzyme Q10 in patients with cardiac failure: a meta-analysis of clinical trials. BMC Cardiovasc Disord. 2017 Jul 24;17(1):196. doi: 10.1186/s12872-017-0628-9[↩]
- Celik T, Iyisoy A. Coenzyme Q10 and coronary artery bypass surgery: what we have learned from clinical trials. J Cardiothorac Vasc Anesth. 2009 Dec;23(6):935-6. doi: 10.1053/j.jvca.2009.01.009[↩][↩]
- Al Saadi T, Assaf Y, Farwati M, Turkmani K, Al-Mouakeh A, Shebli B, Khoja M, Essali A, Madmani ME. Coenzyme Q10 for heart failure. Cochrane Database of Systematic Reviews 2021, Issue 2. Art. No.: CD008684. DOI: 10.1002/14651858.CD008684.pub3[↩][↩]
- Correction to: 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2022 Sep 27;146(13):e185. https://doi.org/10.1161/CIR.0000000000001097 Erratum for: Circulation. 2022 May 3;145(18):e895-e1032. doi: 10.1161/CIR.0000000000001063[↩]
- Milei J, Forcada P, Fraga CG, Grana DR, Iannelli G, Chiariello M, Tritto I, Ambrosio G. Relationship between oxidative stress, lipid peroxidation, and ultrastructural damage in patients with coronary artery disease undergoing cardioplegic arrest/reperfusion. Cardiovasc Res. 2007 Mar 1;73(4):710-9. doi: 10.1016/j.cardiores.2006.12.007[↩]
- Liang S, Ping Z, Ge J. Coenzyme Q10 Regulates Antioxidative Stress and Autophagy in Acute Myocardial Ischemia-Reperfusion Injury. Oxid Med Cell Longev. 2017;2017:9863181. doi: 10.1155/2017/9863181[↩]
- Rosenfeldt FL, Pepe S, Linnane A, Nagley P, Rowland M, Ou R, Marasco S, Lyon W. The effects of ageing on the response to cardiac surgery: protective strategies for the ageing myocardium. Biogerontology. 2002;3(1-2):37-40. doi: 10.1023/a:1015299127969[↩]
- Langsjoen PH, Langsjoen AM. Overview of the use of CoQ10 in cardiovascular disease. Biofactors. 1999;9(2-4):273-84. doi: 10.1002/biof.5520090224[↩]
- Makhija N, Sendasgupta C, Kiran U, Lakshmy R, Hote MP, Choudhary SK, Airan B, Abraham R. The role of oral coenzyme Q10 in patients undergoing coronary artery bypass graft surgery. J Cardiothorac Vasc Anesth. 2008 Dec;22(6):832-9. doi: 10.1053/j.jvca.2008.03.007[↩]
- Taggart DP, Jenkins M, Hooper J, Hadjinikolas L, Kemp M, Hue D, Bennett G. Effects of short-term supplementation with coenzyme Q10 on myocardial protection during cardiac operations. Ann Thorac Surg. 1996 Mar;61(3):829-33. doi: 10.1016/0003-4975(95)01120-X[↩]
- Leong JY, van der Merwe J, Pepe S, Bailey M, Perkins A, Lymbury R, Esmore D, Marasco S, Rosenfeldt F. Perioperative metabolic therapy improves redox status and outcomes in cardiac surgery patients: a randomised trial. Heart Lung Circ. 2010 Oct;19(10):584-91. doi: 10.1016/j.hlc.2010.06.659[↩][↩]
- Huang CH, Kuo CL, Huang CS, Tseng WM, Lian IB, Chang CC, Liu CS. High plasma coenzyme Q10 concentration is correlated with good left ventricular performance after primary angioplasty in patients with acute myocardial infarction. Medicine (Baltimore). 2016 Aug;95(31):e4501. doi: 10.1097/MD.0000000000004501[↩][↩]
- Aslanabadi N, Safaie N, Asgharzadeh Y, Houshmand F, Ghaffari S, Garjani A, Dousti S, Hamishehkar H, Entezari-Maleki T. The randomized clinical trial of coenzyme Q10 for the prevention of periprocedural myocardial injury following elective percutaneous coronary intervention. Cardiovasc Ther. 2016 Aug;34(4):254-60. doi: 10.1111/1755-5922.12195[↩][↩]
- Tran MT, Mitchell TM, Kennedy DT, Giles JT. Role of coenzyme Q10 in chronic heart failure, angina, and hypertension. Pharmacotherapy. 2001 Jul;21(7):797-806. doi: 10.1592/phco.21.9.797.34564[↩]
- Ho MJ, Li EC, Wright JM. Blood pressure lowering efficacy of coenzyme Q10 for primary hypertension. Cochrane Database Syst Rev. 2016 Mar 3;3(3):CD007435. doi: 10.1002/14651858.CD007435.pub3[↩][↩]
- Tabrizi R, Akbari M, Sharifi N, Lankarani KB, Moosazadeh M, Kolahdooz F, Taghizadeh M, Asemi Z. The Effects of Coenzyme Q10 Supplementation on Blood Pressures Among Patients with Metabolic Diseases: A Systematic Review and Meta-analysis of Randomized Controlled Trials. High Blood Press Cardiovasc Prev. 2018 Mar;25(1):41-50. doi: 10.1007/s40292-018-0247-2[↩]
- McDonnell MG, Archbold GP. Plasma ubiquinol/cholesterol ratios in patients with hyperlipidaemia, those with diabetes mellitus and in patients requiring dialysis. Clin Chim Acta. 1996 Sep 30;253(1-2):117-26. doi: 10.1016/0009-8981(96)06357-7[↩]
- Lim SC, Tan HH, Goh SK, Subramaniam T, Sum CF, Tan IK, Lee BL, Ong CN. Oxidative burden in prediabetic and diabetic individuals: evidence from plasma coenzyme Q(10). Diabet Med. 2006 Dec;23(12):1344-9. doi: 10.1111/j.1464-5491.2006.01996.x[↩]
- Alcolado JC, Laji K, Gill-Randall R. Maternal transmission of diabetes. Diabet Med. 2002 Feb;19(2):89-98. doi: 10.1046/j.1464-5491.2002.00675.x[↩]
- Suzuki S, Hinokio Y, Ohtomo M, Hirai M, Hirai A, Chiba M, Kasuga S, Satoh Y, Akai H, Toyota T. The effects of coenzyme Q10 treatment on maternally inherited diabetes mellitus and deafness, and mitochondrial DNA 3243 (A to G) mutation. Diabetologia. 1998 May;41(5):584-8. doi: 10.1007/s001250050950[↩]
- Laaksonen R, Fogelholm M, Himberg JJ, Laakso J, Salorinne Y. Ubiquinone supplementation and exercise capacity in trained young and older men. Eur J Appl Physiol Occup Physiol. 1995;72(1-2):95-100. doi: 10.1007/BF00964121[↩][↩][↩]
- Malm C, Svensson M, Ekblom B, Sjödin B. Effects of ubiquinone-10 supplementation and high intensity training on physical performance in humans. Acta Physiol Scand. 1997 Nov;161(3):379-84. doi: 10.1046/j.1365-201X.1997.00198.x[↩][↩][↩]
- Weston SB, Zhou S, Weatherby RP, Robson SJ. Does exogenous coenzyme Q10 affect aerobic capacity in endurance athletes? Int J Sport Nutr. 1997 Sep;7(3):197-206. doi: 10.1123/ijsn.7.3.197[↩][↩]
- Porter DA, Costill DL, Zachwieja JJ, Krzeminski K, Fink WJ, Wagner E, Folkers K. The effect of oral coenzyme Q10 on the exercise tolerance of middle-aged, untrained men. Int J Sports Med. 1995 Oct;16(7):421-7. doi: 10.1055/s-2007-973031[↩][↩]
- Braun B, Clarkson PM, Freedson PS, Kohl RL. Effects of coenzyme Q10 supplementation on exercise performance, VO2max, and lipid peroxidation in trained cyclists. Int J Sport Nutr. 1991 Dec;1(4):353-65. doi: 10.1123/ijsn.1.4.353[↩][↩]
- Bonetti A, Solito F, Carmosino G, Bargossi AM, Fiorella PL. Effect of ubidecarenone oral treatment on aerobic power in middle-aged trained subjects. J Sports Med Phys Fitness. 2000 Mar;40(1):51-7.[↩]
- Abdizadeh L, Jafari A, Armanfar M. Effects of short-term coenzyme Q10 supplementation on markers of oxidative stress and inflammation after downhill running in male mountaineers. Science & Sports. 2015;30(6):328-334.[↩]
- Leelarungrayub D, Rawattikanon A, Klaphajone J, Pothong-sunan P, Bloomer RJ. Coenzyme Q10 supplementation decreases oxidative stress and improves physical performance in young swimmers Open Sports Med J 2010;4(1):1-8.[↩]
- Díaz-Castro J, Guisado R, Kajarabille N, García C, Guisado IM, de Teresa C, Ochoa JJ. Coenzyme Q(10) supplementation ameliorates inflammatory signaling and oxidative stress associated with strenuous exercise. Eur J Nutr. 2012 Oct;51(7):791-9. doi: 10.1007/s00394-011-0257-5[↩]
- Ostman B, Sjödin A, Michaëlsson K, Byberg L. Coenzyme Q10 supplementation and exercise-induced oxidative stress in humans. Nutrition. 2012 Apr;28(4):403-17. doi: 10.1016/j.nut.2011.07.010[↩]
- Sachdanandam P. Antiangiogenic and hypolipidemic activity of coenzyme Q10 supplementation to breast cancer patients undergoing tamoxifen therapy. Biofactors . 2008;32(1-4):151-159.[↩]
- Coulter I, Hardy M, Shekelle P, et al. Effect of the Supplemental Use of Antioxidants Vitamin C, Vitamin E, and Coenzyme Q10 for the Prevention and Treatment of Cancer . Evidence Report/Technology Assessment Number 75 (Prepared by Southern California Evidence-based Practice Center under Contract No. 290-97-0001). AHRQ Publication No. 03-E047. Rockville, MD[↩]
- Tiano L, Padella L, Carnevali P, et al. Coenzyme Q10 and oxidative imbalance in Down syndrome: biochemical and clinical aspects. Biofactors . 2008;32(1-4):161-167.[↩]
- Hargreaves IP. Coenzyme Q10 in phenylketonuria and mevalonic aciduria. Mitochondrion . 2007;7(suppl 1):S175-S180.[↩]
- Eiholzer U, L’allemand D, Schlumpf M, Rousson V, Gasser T, Fusch C. Growth hormone and body composition in children younger than 2 years with Prader-Willi syndrome. J Pediatr . 2004;144(6):753-758.[↩]
- Knott A, Achterberg V, Smuda C, et al. Topical treatment with coenzyme Q10-containing formulas improves skin’s Q10 level and provides antioxidative effects. Biofactors. 2015 Nov-Dec;41(6):383-90. doi: 10.1002/biof.1239[↩]
- Bhagavan HN, Chopra RK. Potential role of ubiquinone (coenzyme Q10) in pediatric cardiomyopathy. Clin Nutr . 2005;24(3):331-338.[↩]
- Wang Y, Hekimi S. The efficacy of coenzyme Q10 treatment in alleviating the symptoms of primary coenzyme Q10 deficiency: A systematic review. J Cell Mol Med. 2022 Sep;26(17):4635-4644. doi: 10.1111/jcmm.17488[↩]
- Rosenfeldt FL, Haas SJ, Krum H, Hadj A, Ng K, Leong J-Y, et al. Coenzyme Q10 in the treatment of hypertension: a meta-analysis of the clinical trials. Journal of Human Hypertension 2007;21:297-306.[↩]
- Levy G, Kaufmann P, Buchsbaum R, et al. A two-stage design for a phase II clinical trial of coenzyme Q10 in ALS. Neurology . 2006;66(5):660-663.[↩]
- Di Prospero NA, Sumner CJ, Penzak SR, Ravina B, Fischbeck KH, Taylor JP. Safety, tolerability, and pharmacokinetics of high-dose idebenone in patients with Friedreich ataxia. Arch Neurol . 2007;64(6):803-808.[↩]
- KDIGO Conference Participants. Genetics in chronic kidney disease: conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference. Kidney Int. 2022 Jun;101(6):1126-1141. doi: 10.1016/j.kint.2022.03.019[↩][↩]
- Florou P, Anagnostis P, Theocharis P, Chourdakis M, Goulis DG. Does coenzyme Q10 supplementation improve fertility outcomes in women undergoing assisted reproductive technology procedures? A systematic review and meta-analysis of randomized-controlled trials. J Assist Reprod Genet. 2020 Oct;37(10):2377-2387. doi: 10.1007/s10815-020-01906-3[↩]
- Drugs and Lactation Database (LactMed®) [Internet]. Bethesda (MD): National Institute of Child Health and Human Development; 2006-. Coenzyme Q10. [Updated 2021 May 17]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK501788[↩][↩]
- Tang PH, Miles MV, Steele P, Davidson BS, Geraghty SR, Morrow AL. Determination of coenzyme Q10 in human breast milk by high-performance liquid chromatography. Biomed Chromatogr. 2006 Dec;20(12):1336-43. doi: 10.1002/bmc.702[↩]
- Sood B, Patel P, Keenaghan M. Coenzyme Q10. [Updated 2024 Jan 30]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK531491[↩]
- Lund EL, Quistorff B, Spang-Thomsen M, Kristjansen PE. Effect of radiation therapy on small-cell lung cancer is reduced by ubiquinone intake. Folia Microbiol (Praha). 1998;43(5):505-6. doi: 10.1007/BF02820805[↩][↩]
- Ben Fredj N, Ben Fadhel N, Chaabane A, Chadly Z, Ben Romdhane H, Boughattas A, Aouam K. Colloidal silica-induced hypersensitivity: myth or reality. Int J Clin Pharm. 2016 Feb;38(1):7-9. doi: 10.1007/s11096-015-0225-x[↩]
- Hodges S, Hertz N, Lockwood K, Lister R. CoQ10: could it have a role in cancer management? Biofactors. 1999;9(2-4):365-70. doi: 10.1002/biof.5520090237[↩]
- Heller JH. Disease, the host defense, and Q-10. Perspect Biol Med. 1973 Winter;16(2):181-7. doi: 10.1353/pbm.1973.0062[↩]
- LiverTox: Clinical and Research Information on Drug-Induced Liver Injury [Internet]. Bethesda (MD): National Institute of Diabetes and Digestive and Kidney Diseases; 2012-. Coenzyme Q10. [Updated 2024 Apr 20]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK603562[↩]
- Baggio E, Gandini R, Plancher AC, Passeri M, Carmosino G. Italian multicenter study on the safety and efficacy of coenzyme Q10 as adjunctive therapy in heart failure. CoQ10 Drug Surveillance Investigators. Mol Aspects Med. 1994;15 Suppl:s287-94. doi: 10.1016/0098-2997(94)90040-x[↩]
- Feigin A, Kieburtz K, Como P, Hickey C, Claude K, Abwender D, Zimmerman C, Steinberg K, Shoulson I. Assessment of coenzyme Q10 tolerability in Huntington’s disease. Mov Disord. 1996 May;11(3):321-3. doi: 10.1002/mds.870110317[↩]
- Coenzyme Q10. In: Jellin JM, Hitchens K, eds.: Natural Medicines Comprehensive Database. Therapeutic Research Faculty, 1999, pp 241-42.[↩][↩]
- Kaikkonen J, Nyyssönen K, Tuomainen TP, Ristonmaa U, Salonen JT. Determinants of plasma coenzyme Q10 in humans. FEBS Lett. 1999 Jan 25;443(2):163-6. doi: 10.1016/s0014-5793(98)01712-8[↩]
- Thibault A, Samid D, Tompkins AC, Figg WD, Cooper MR, Hohl RJ, Trepel J, Liang B, Patronas N, Venzon DJ, Reed E, Myers CE. Phase I study of lovastatin, an inhibitor of the mevalonate pathway, in patients with cancer. Clin Cancer Res. 1996 Mar;2(3):483-91.[↩]
- Hidaka T, Fujii K, Funahashi I, Fukutomi N, Hosoe K. Safety assessment of coenzyme Q10 (CoQ10). Biofactors. 2008;32(1-4):199-208. doi: 10.1002/biof.5520320124[↩]
- Deshmukh G, Venkataramaiah SB, Doreswamy CM, Umesh MC, Subbanna RB, Pradhan BK, Seekallu S, Sekar R, Prabhu K, Sadagopan S, Arumugam SN, Sharma S, Gavara G, Balaraman S, Sambasivam G, Chandrappa RK, Flynn S, Shivarudraiah P. Safety Assessment of Ubiquinol Acetate: Subchronic Toxicity and Genotoxicity Studies. J Toxicol. 2019 Apr 1;2019:3680757. doi: 10.1155/2019/3680757[↩]
- Landbo C, Almdal TP. Interaktion mellem warfarin og coenzym Q10 [Interaction between warfarin and coenzyme Q10]. Ugeskr Laeger. 1998 May 25;160(22):3226-7. Danish.[↩]
- Engelsen J, Nielsen JD, Hansen KF. Effekten af Coenzym Q10 og Ginkgo biloba på warfarindosis hos patienter i laengerevarende warfarinbehandling. Et randomiseret, dobbeltblindt, placebokontrolleret overkrydsningsforsøg [Effect of Coenzyme Q10 and Ginkgo biloba on warfarin dosage in patients on long-term warfarin treatment. A randomized, double-blind, placebo-controlled cross-over trial]. Ugeskr Laeger. 2003 Apr 28;165(18):1868-71. Danish.[↩]
- Engelsen J, Nielsen JD, Winther K. Effect of coenzyme Q10 and Ginkgo biloba on warfarin dosage in stable, long-term warfarin treated outpatients. A randomised, double blind, placebo-crossover trial. Thromb Haemost. 2002 Jun;87(6):1075-6.[↩]
- Hidaka T, Fujii K, Funahashi I, Fukutomi N, Hosoe K. Safety assessment of coenzyme Q10 (CoQ10). Biofactors . 2008;32(1-4):199-208.[↩]




{kind=link}