Ulnar nerve
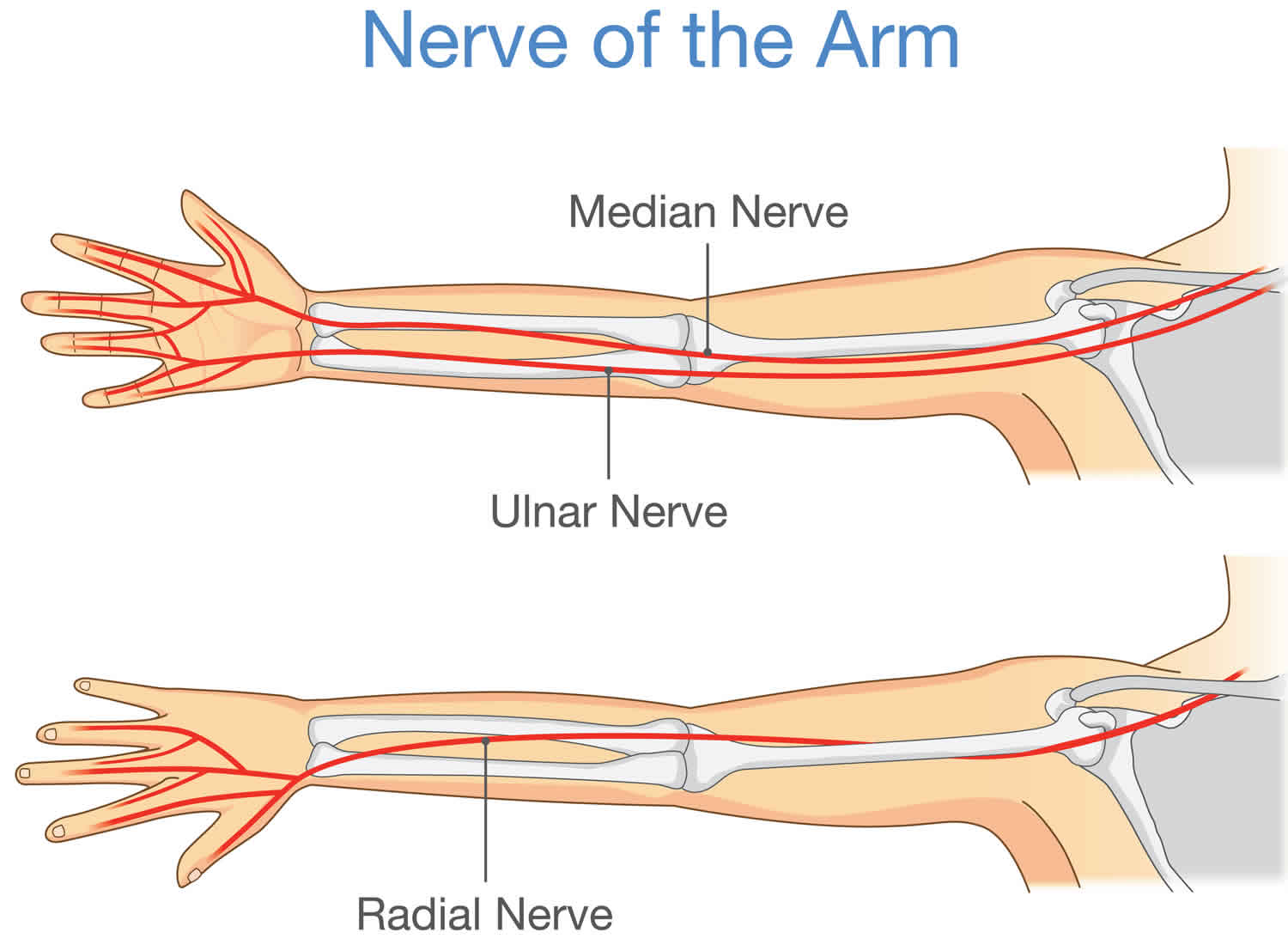
The ulnar nerve originates from C8-T1 and is a terminal branch of the brachial plexus. The C8 and T1 nerve roots merge to form the lower trunk of the brachial plexus which continues as the medial cord to give rise to the ulnar nerve (see Figure 1). The ulnar nerve is one of the three main nerves in your arm (the other nerves are median and radial nerves). Ulnar nerve travels from your neck down into your hand, and can be constricted in several places along the way, such as beneath the collarbone, wrist, forearm, and upper arm. The most common place for entrapment of the nerve is behind the inside part of the elbow. Ulnar nerve entrapment at the elbow is called “cubital tunnel syndrome.”
In the upper arm, the ulnar nerve courses posterior and medial to the brachial artery, and heads for the posterior aspect of the elbow, piercing the medial intermuscular septum at the arcade of Struthers. The nerve pierces the medial intermuscular septum approximately 8 cm proximal to the medial epicondyle 1.
At the elbow, the ulnar nerve enters the cubital tunnel posterior to the medial epicondyle and enters the forearm by piercing between the two heads of the flexor carpi ulnaris muscle. The spot where the ulnar nerve runs posterior to the medial epicondyle is commonly referred to as the “funny bone.” At the medial epicondyle the ulnar nerve is close to your skin, and bumping it causes a shock-like feeling, which for some reason is commonly referred to as the funny bone, even though this event is anything but funny. The ulnar nerve may be palpated by rolling a finger over the skin surface above the posterior surface of the medial epicondyle.
Beyond the elbow, the ulnar nerve travels under muscles on the inside of your forearm and into your hand on the side of the palm with the little finger. As the ulnar nerve enters the hand, it travels through another tunnel (Guyon’s canal). Guyon’s canal is a unique location where ulnar nerve is vulnerable to compressive injury. Guyon’s canal syndrome is a relatively rare peripheral ulnar neuropathy which involves injury to the distal portion of the ulnar nerve as it travels through a narrow anatomic corridor at the wrist 2.
The ulnar nerve gives feeling to the little finger and half of the ring finger. It also controls most of the little muscles in the hand that help with fine movements, and some of the bigger muscles in the forearm that help you make a strong grip.
The ulnar nerve enters the arm with the median nerve and axillary artery. It passes through proximal regions medial to the axillary artery. In the middle of the arm, the ulnar nerve penetrates the medial intermuscular septum and enters the posterior compartment where it lies anterior to the medial head of the triceps brachii muscle. It passes posterior to the medial epicondyle of the humerus and then into the anterior compartment of the forearm.
The ulnar nerve has no major branches in the arm.
Figure 1. Ulnar nerve
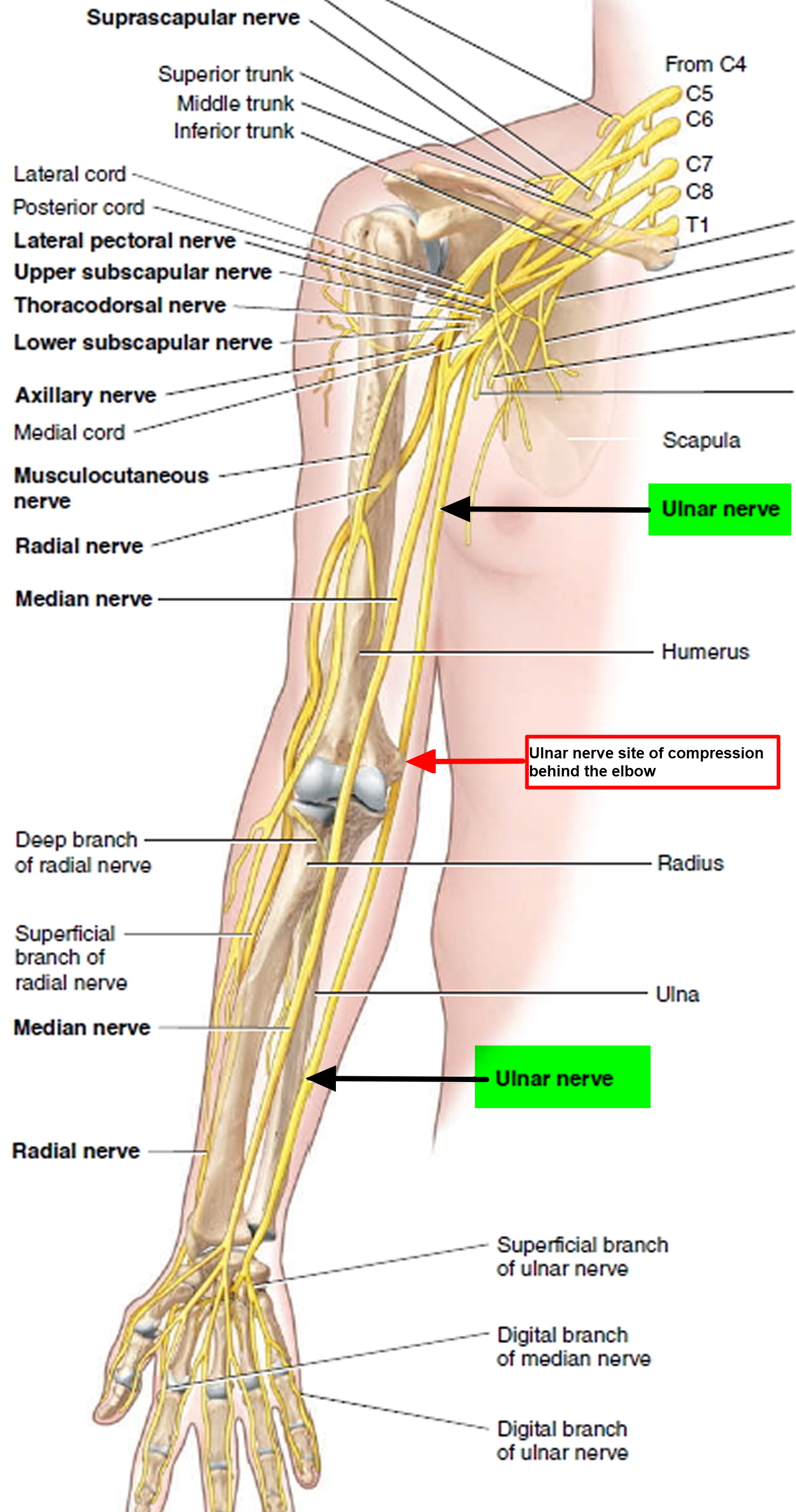
Figure 2. The ulnar nerve runs behind the medial epicondyle of the humerus on the inside of the elbow.
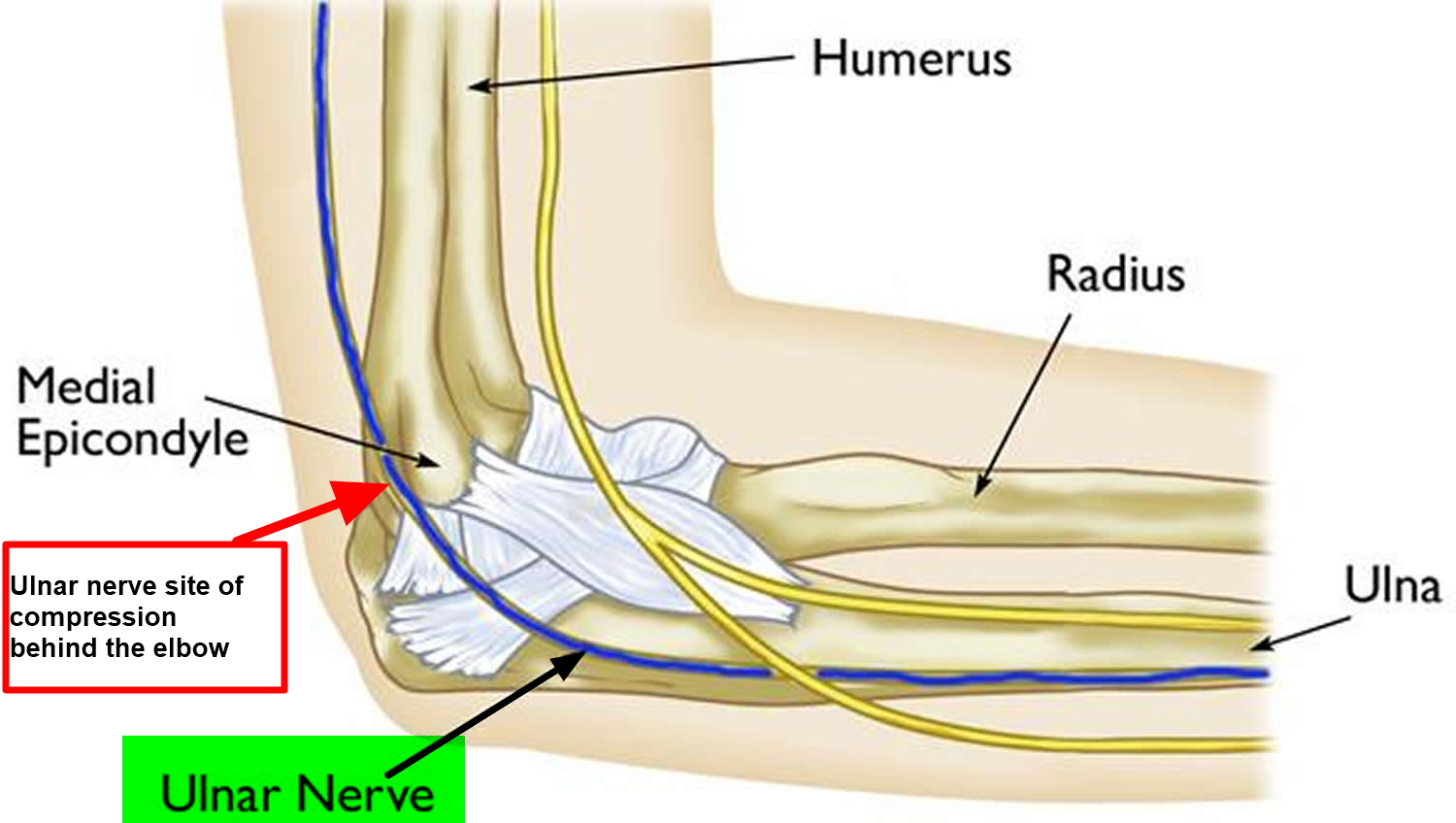
Figure 3. The ulnar nerve gives sensation (feeling) to the little finger and to half of the ring finger on both the palm and back side of the hand.
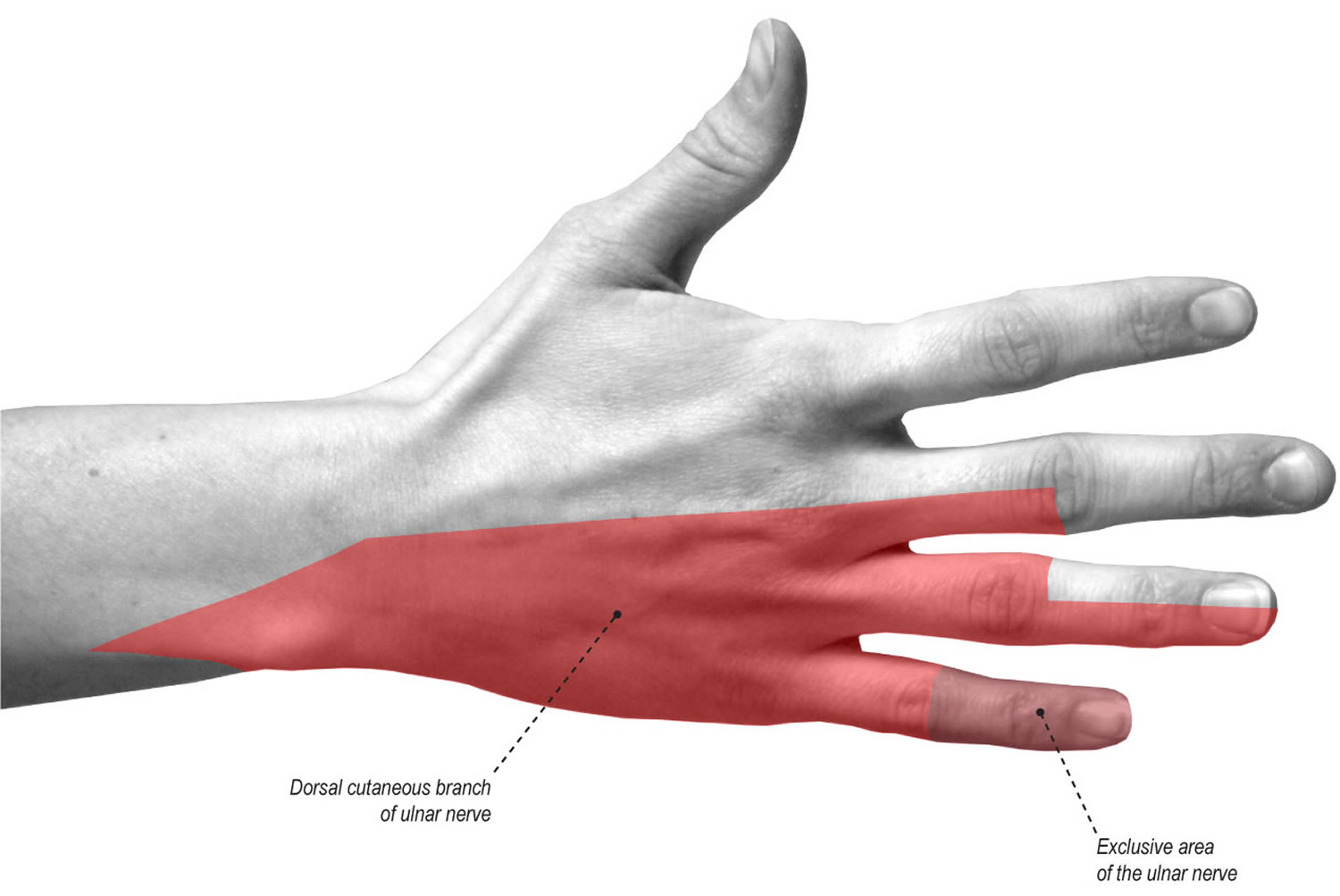
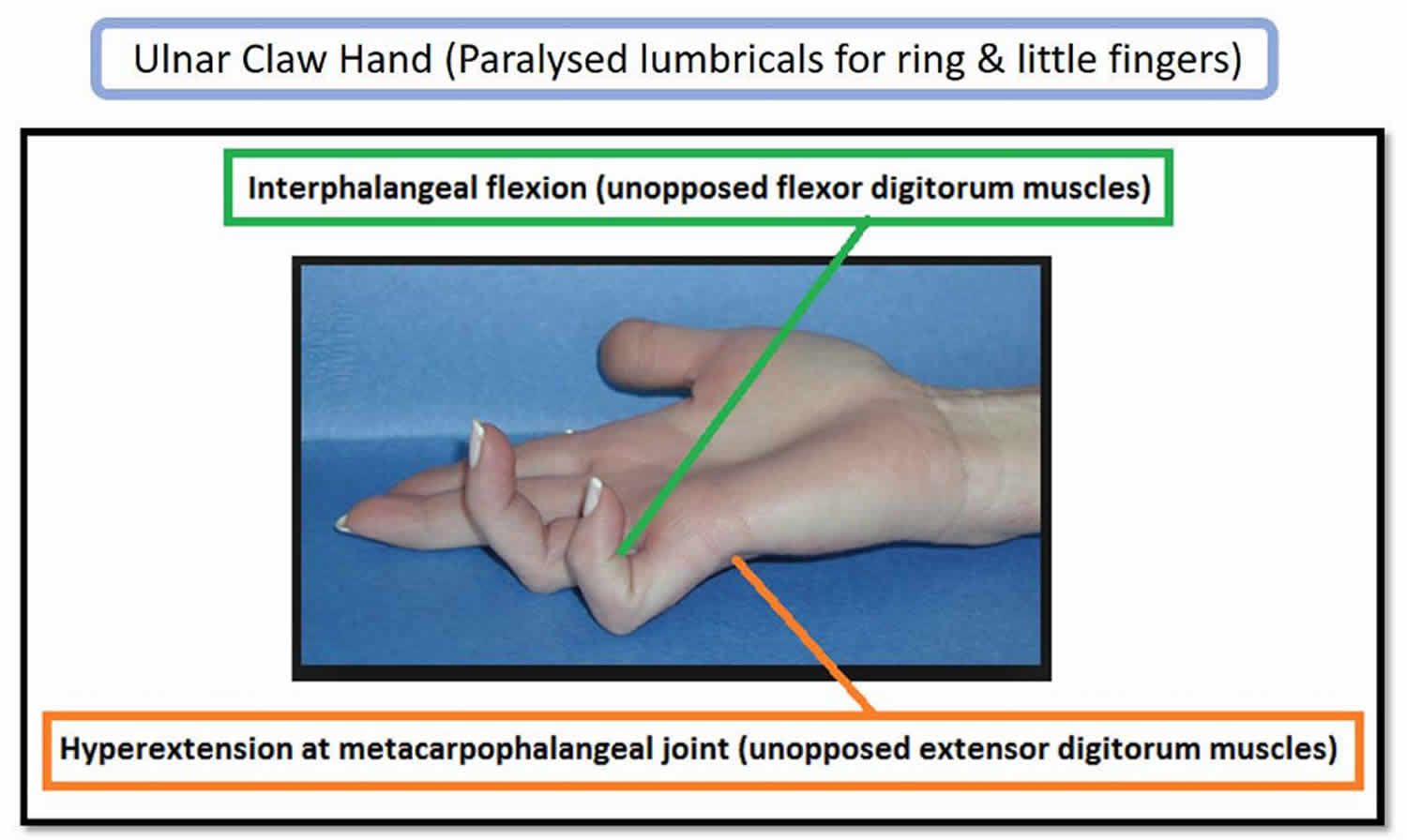
Figure 4. Ulnar claw hand
Ulnar nerve innervation
The ulnar nerve supplies the anteromedial muscles of the forearm and most of the muscles of the hand.
Injury to the ulnar nerve may result in ulnar nerve palsy, which is indicated by an inability to abduct or adduct the fingers, atrophy of the interosseous muscles of the hand, hyperextension of the metacarpophalangeal joints, and flexion of the interphalangeal joints, a condition called clawhand (Figure 4). There is also loss of sensation over the little finger.
Ulnar nerve injury
The second most common upper extremity entrapment neuropathy is ulnar neuropathy at the elbow 3. At the elbow, the ulnar nerve lacks protective cover in the ulnar groove. This causes its susceptibility to external compression. Repetitive elbow flexion and extension, arthritic changes, and valgus deformities at the elbow increase its vulnerability to injury. In some individuals, the ulnar nerve may be subluxed out of the retroepicondylar groove medially over the medial epicondyle during elbow flexion. In a study investigating patients with ulnar neuropathy at the elbow, the pressures recorded between the ulnar nerve and overlying arcade increased up to above 200 mm Hg in elbow flexion or during isometric contraction of the flexor carpi ulnaris muscle. In contrast, the pressure was less than 19 at elbow extension 4.
Repetitive movement that exerts pressure on the ulnar wrist and hypothenar eminence predisposes the ulnar nerve to develop neuropathy. Wrist fractures and compressive mass lesions may also cause ulnar neuropathy at the wrist.
Neurapraxia of the ulnar nerve is often seen with mild injury. However, moderate-to-severe injuries of the nerve will present as axonotmesis, or in severe cases, neurotmesis.
Symptoms of ulnar neuropathy at the elbow usually start slowly unless it is associated with trauma. The patient may have numbness and paresthesia, radiating distally to the ulnar aspect of the hand, the fifth digit and the ulnar aspect of the fourth digit. It is usually associated with elbow flexion, particularly at night. Unless it is associated with an acute injury to the elbow, pain is not a dominant feature; however, some patients may complain of pain due to overuse of the forearm flexors such as the flexor carpi ulnaris.
Sensory symptoms involving the fifth digit and medial half of the fourth digit may indicate an ulnar neuropathy at the wrist. However, similar findings can be seen in ulnar neuropathy at the elbow. It is suggested that the fibers destined for the flexor carpi ulnaris, palmar ulnar cutaneous branch, and dorsal ulnar cutaneous lie in individual fascicles at the elbow in a deep dorsolateral position, rendering them less susceptible to damage 5. This renders them less susceptible to injury in ulnar neuropathy at the elbow, and may cause difficulty in distinguishing ulnar neuropathy at the elbow from ulnar neuropathy at the wrist. However, if there is an involvement of the entire ring finger or in contrast, total sparing, the diagnosis of cervical radiculopathy or brachial plexopathy should be taken into account.
When the disease gets worse, the symptom may progress to constant numbness and paresthesia and weakness of the innervated muscles. Weakness may start from clumsiness and loss of hand dexterity. This may then progress to a decrease in handgrip and pinch strength (Froment sign). In more severe cases, there may be atrophy of the hand intrinsic muscles and clawing of the fourth and the fifth digits, classically known as claw hand 6.
Ulnar neuropathy at the wrist and hand can range from pure sensory to pure motor deficits. The most common type of ulnar neuropathies at the wrist is compression of the deep palmar branch. Ulnar neuropathies of the wrist and hand are divided into 3 types. Type I is a lesion of the ulnar nerve just proximal to or within the Guyon canal involving deep and the superficial branches; this causes mixed motor and sensory deficits and subsequent weakness of all the ulnar hand muscles. Type II is a lesion involving the deep branch which causes a pure motor deficit with a varied pattern of weakness based on the compression site. Type III lesion is limited to the superficial branch, causing purely sensory deficits to the palmar aspect of the medial half of the fourth digit and the fifth digit. The sensory loss in type I and type III lesions spares the dorsal aspect of the hand and fingers and the hypothenar eminence due to the more proximal innervations from the dorsal ulnar cutaneous and the palmar ulnar cutaneous branch, respectively 7.
Ulnar nerve injury causes
Damage to one nerve group, such as the ulnar nerve, is called mononeuropathy. Mononeuropathy means there is damage to a single nerve. Diseases affecting the entire body (systemic disorders) can also cause isolated nerve damage.
Causes of ulnar nerve mononeuropathy include:
- An illness in the whole body that damages a single nerve
- Direct injury to the ulnar nerve
- Long-term pressure on the nerve
- Pressure on the nerve caused by swelling or injury of nearby body structures
Ulnar neuropathy is also common in those with diabetes.
Ulnar neuropathy occurs when there is damage to the ulnar nerve. This nerve travels down the arm to the wrist, hand, and ring and little fingers. It passes near the surface of the elbow. So, bumping the nerve there causes the pain and tingling of “hitting the funny bone.”
When the nerve compressed in the elbow, a problem called cubital tunnel syndrome may result.
When damage destroys the nerve covering (myelin sheath) or part of the nerve itself, nerve signaling is slowed or prevented.
Damage to the ulnar nerve can be caused by:
- Long-term pressure on the elbow or base of the palm
- An elbow fracture or dislocation
- Repeated elbow bending, such as with cigarette smoking
In some cases, no cause can be found.
Ulnar nerve injury symptoms
Ulnar nerve palsy symptoms may include any of the following:
- Abnormal sensations in the little finger and part of the ring finger, usually on the palm side
- Weakness, loss of coordination of the fingers
- Clawlike deformity of the hand and wrist
- Pain, numbness, decreased sensation, tingling, or burning sensation in the areas controlled by the nerve
Pain or numbness may awaken you from sleep. Activities such as tennis or golf may make the condition worse.
Ulnar nerve damage possible complications
Ulnar nerve damage complications may include:
- Deformity of the hand
- Partial or complete loss of sensation in the hand or fingers
- Partial or complete loss of wrist or hand movement
- Recurrent or unnoticed injury to the hand
Ulnar nerve injury diagnosis
Diagnosis traditionally relies on clinical history, physical examination, and electrodiagnostic studies. It has been suggested that combination of electromyography (EMG) and nerve conduction velocity tests can improve diagnostic accuracy by mapping out the location of pathological compression of the ulnar nerve, which would provide a relatively early diagnosis in patients who have symptoms suggestive of ulnar nerve lesions.
Ultrasound has also been suggested as a screening and follow-up imaging modality in patients with ulnar neuropathy at the elbow, as ultrasound can detect the morphologic changes and the extent of the ulnar nerve lesion at the elbow. A recent meta-analysis showed that in healthy participants, the ulnar nerve cross-sectional area at various locations at the elbow rarely exceeds 10 mm, and this can be considered a cutoff point for diagnosing ulnar nerve entrapment at the elbow region 8. Another study suggested that by measuring ulnar nerve cross-sectional area with MRI or ultrasound at 1-cm proximal to the medial epicondyle, patients with and without ulnar neuropathy at the elbow could be discriminated by using a cutoff threshold of 11.0 mm 9. It is also suggested that the ulnar nerve-swelling ratio can be a complementary tool for diagnosing ulnar neuropathy at the elbow, and other potential sonologic indicators include presence of intra-neural vascularity, increased flattening ratio, and enlarged intra-neural hypoechoic fraction, although further research is needed 10.
Ulnar nerve injury treatment
There are 2 main conservative treatments: reducing the frequency of external compression on the nerve and flexion of the elbow joint. This is expected to decrease the stress placed on the ulnar nerve. The use of elbow splints, elbow pads or sleeves, you may need to wear it all day and night or only at night and physical therapy have been suggested. Occupational therapy or counseling to suggest changes in the workplace may be needed. For patients with mild to moderate symptoms, conservative treatment can be administered. It was shown that in patients with mild symptoms, conservative treatments are proven to be beneficial in about 90% of the patients; however, only 38% of the patients with moderate symptoms respond well a non-operative method 11.
Injection procedures have also been proposed for the treatment of ulnar neuropathy at the elbow. However, studies with ultrasound-guided corticosteroid injections at the elbow have shown controversial results 12.
Surgical treatment becomes a consideration for patients with persistent symptoms, with accompanying sensory changes and muscle atrophy. Several surgical methods have been described, for example, decompression, anterior transposition techniques, and medial epicondylectomy. A systematic review showed that simple decompression and decompression with transposition are equally effective in idiopathic ulnar neuropathy at the elbow. However, the decompression surgery with transposition is associated with more wound infections than simple decompression 13.
Ulnar nerve damage prognosis
If the cause of the ulnar nerve damage can be found and successfully treated, there is a good chance of a full recovery. In some cases, there may be partial or complete loss of movement or sensation.
Ulnar nerve entrapment
Ulnar nerve entrapment at the elbow is called “cubital tunnel syndrome” 14.
At the elbow, the ulnar nerve travels through a tunnel of tissue (the cubital tunnel) that runs under a bump of bone at the inside of your elbow. This bony bump is called the medial epicondyle. The spot where the nerve runs under the medial epicondyle is commonly referred to as the “funny bone.” At the funny bone the nerve is close to your skin, and bumping it causes a shock-like feeling.
Numbness and tingling in the hand and fingers are common symptoms of ulnar nerve entrapment. In most cases, symptoms can be managed with conservative treatments like changes in activities and bracing. If conservative methods do not improve your symptoms, or if the nerve entrapment is causing muscle weakness or damage in your hand, your doctor may recommend surgery.
Ulnar nerve entrapment causes
In many cases of ulnar nerve entrapment, the exact cause is not known. The ulnar nerve is especially vulnerable to entrapment at the elbow because it must travel through a narrow space with very little soft tissue to protect it.
Common causes of ulnar nerve entrapment
There are several things that can cause pressure on the ulnar nerve at the elbow:
- When your bend your elbow, the ulnar nerve must stretch around the boney ridge of the medial epicondyle. Because this stretching can irritate the nerve, keeping your elbow bent for long periods or repeatedly bending your elbow can cause painful symptoms. For example, many people sleep with their elbows bent. This can aggravate symptoms of ulnar nerve entrapment and cause you to wake up at night with your fingers asleep.
- In some people, the nerve slides out from behind the medial epicondyle when the elbow is bent. Over time, this sliding back and forth may irritate the nerve.
- Leaning on your elbow for long periods of time can put pressure on the nerve.
- Fluid buildup in the elbow can cause swelling that may compress the nerve.
- A direct blow to the inside of the elbow can cause pain, electric shock sensation, and numbness in the little and ring fingers. This is commonly called “hitting your funny bone.”
Risk factors for ulnar nerve entrapment
Some factors put you more at risk for developing ulnar nerve entrapment (cubital tunnel syndrome). These include:
- Prior fracture or dislocations of the elbow
- Bone spurs/ arthritis of the elbow
- Swelling of the elbow joint
- Cysts near the elbow joint
- Repetitive or prolonged activities that require the elbow to be bent or flexed
Ulnar nerve entrapment symptoms
Ulnar nerve entrapment can cause an aching pain on the inside of the elbow. Most of the symptoms, however, occur in your hand.
- Numbness and tingling in the ring finger and little finger are common symptoms of ulnar nerve entrapment. Often, these symptoms come and go. They happen more often when the elbow is bent, such as when driving or holding the phone. Some people wake up at night because their fingers are numb.
- The feeling of “falling asleep” in the ring finger and little finger, especially when your elbow is bent. In some cases, it may be harder to move your fingers in and out, or to manipulate objects.
- Weakening of the grip and difficulty with finger coordination (such as typing or playing an instrument) may occur. These symptoms are usually seen in more severe cases of nerve entrapment.
- If the nerve is very compressed or has been compressed for a long time, muscle wasting in the hand can occur. Once this happens, muscle wasting cannot be reversed. For this reason, it is important to see your doctor if symptoms are severe or if they are less severe but have been present for more than 6 weeks.
Ulnar nerve entrapment diagnosis
Your doctor will discuss your medical history and general health. He or she may also ask about your work, your activities, and what medications you are taking.
After discussing your symptoms and medical history, your doctor will examine your arm and hand to determine which nerve is compressed and where it is compressed. Some of the physical examination tests your doctor may do include:
- Tap over the nerve at the funny bone. If the nerve is irritated, this can cause a shock into the little finger and ring finger — although this can happen when the nerve is normal as well.
- Check whether the ulnar nerve slides out of normal position when you bend your elbow.
- Move your neck, shoulder, elbow, and wrist to see if different positions cause symptoms.
- Check for feeling and strength in your hand and fingers.
Ulnar nerve entrapment test
X-rays. These imaging tests provide detailed pictures of dense structures, like bone. Most causes of entrapment of the ulnar nerve cannot be seen on an x-ray. However, your doctor may take x-rays of your elbow or wrist to look for bone spurs, arthritis, or other places that the bone may be compressing the nerve.
Nerve conduction studies. These tests can determine how well the nerve is working and help identify where it is being compressed.
Nerves are like “electrical cables” that travel through your body carrying messages between your brain and muscles. When a nerve is not working well, it takes too long for it to conduct.
During a nerve conduction test, the nerve is stimulated in one place and the time it takes for there to be a response is measured. Several places along the nerve will be tested and the area where the response takes too long is likely to be the place where the nerve is compressed.
Nerve conduction studies can also determine whether the entrapment is also causing muscle damage. During the test, small needles are put into some of the muscles that the ulnar nerve controls. Muscle damage is a sign of more severe nerve entrapment.
Ulnar nerve entrapment treatment
Unless your nerve entrapment has caused a lot of muscle wasting, your doctor will most likely first recommend nonsurgical treatment.
Nonsurgical Treatment
- Non-steroidal anti-inflammatory (NSAIDs) medicines. If your symptoms have just started, your doctor may recommend an anti-inflammatory medicine, such as ibuprofen, to help reduce swelling around the nerve.
Although steroids, such as cortisone, are very effective anti-inflammatory medicines, steroid injections are generally not used because there is a risk of damage to the nerve.
- Bracing or splinting. Your doctor may prescribe a padded brace or split to wear at night to keep your elbow in a straight position.
- Nerve gliding exercises. Some doctors think that exercises to help the ulnar nerve slide through the cubital tunnel at the elbow and the Guyon’s canal at the wrist can improve symptoms. These exercises may also help prevent stiffness in the arm and wrist.
Home remedies
There are many things you can do at home to help relieve symptoms. If your symptoms interfere with normal activities or last more than a few weeks, be sure to schedule an appointment with your doctor.
- Avoid activities that require you to keep your arm bent for long periods of time.
- If you use a computer frequently, make sure that your chair is not too low. Do not rest your elbow on the armrest.
- Avoid leaning on your elbow or putting pressure on the inside of your arm. For example, do not drive with your arm resting on the open window.
- Keep your elbow straight at night when you are sleeping. This can be done by wrapping a towel around your straight elbow or wearing an elbow pad backwards.
Ulnar nerve entrapment surgery
Your doctor may recommend surgery to take pressure off of the nerve if:
- Nonsurgical methods have not improved your condition
- The ulnar nerve is very compressed
- Nerve entrapment has caused muscle weakness or damage
There are a few surgical procedures that will relieve pressure on the ulnar nerve at the elbow. Your orthopedic surgeon will talk with you about the option that would be best for you.
These procedures are most often done on an outpatient basis, but some patients do best with an overnight stay at the hospital.
Cubital tunnel release. In this operation, the ligament “roof” of the cubital tunnel is cut and divided. This increases the size of the tunnel and decreases pressure on the nerve.
After the procedure, the ligament begins to heal and new tissue grows across the division. The new growth heals the ligament, and allows more space for the ulnar nerve to slide through.
Cubital tunnel release tends to work best when the nerve entrapment is mild or moderate and the nerve does not slide out from behind the bony ridge of the medial epicondyle when the elbow is bent.
Ulnar nerve anterior transposition. In many cases, the nerve is moved from its place behind the medial epicondyle to a new place in front of it. Moving the nerve to the front of the medial epicondyle prevents it from getting caught on the bony ridge and stretching when you bend your elbow. This procedure is called an anterior transposition of the ulnar nerve.
The nerve can be moved to lie under the skin and fat but on top of the muscle (subcutaneous transposition), or within the muscle (intermuscular transposition), or under the muscle (submuscular transposition).
Medial epicondylectomy. Another option to release the nerve is to remove part of the medial epicondyle. Like ulnar nerve transposition, this technique also prevents the nerve from getting caught on the boney ridge and stretching when your elbow is bent.
Surgical Recovery
Depending on the type of surgery you have, you may need to wear a splint for a few weeks after the operation. A submuscular transposition usually requires a longer time (3 to 6 weeks) in a splint.
Your surgeon may recommend physical therapy exercises to help you regain strength and motion in your arm. He or she will also talk with you about when it will be safe to return to all your normal activities.
Surgical Outcome
The results of surgery are generally good. Each method of surgery has a similar success rate for routine cases of nerve entrapment. If the nerve is very badly compressed or if there is muscle wasting, the nerve may not be able to return to normal and some symptoms may remain even after the surgery. Nerves recover slowly, and it may take a long time to know how well the nerve will do after surgery.
Ulnar nerve entrapment exercises
Nerve gliding exercises. Some doctors think that exercises to help the ulnar nerve slide through the cubital tunnel at the elbow and the Guyon’s canal at the wrist can improve symptoms. These exercises may also help prevent stiffness in the arm and wrist.
Figure 5. Ulnar nerve entrapment exercises

- Ramage JL, Varacallo M. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): Nov 27, 2018. Anatomy, Shoulder and Upper Limb, Hand Guyon Canal[↩]
- Aleksenko D, Varacallo M. Guyon Canal Syndrome. [Updated 2019 May 5]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK431063[↩]
- Lleva JMC, Chang KV. Ulnar Neuropathy. [Updated 2019 Jan 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK534226[↩]
- Werner CO, Ohlin P, Elmqvist D. Pressures recorded in ulnar neuropathy. Acta Orthop Scand. 1985 Oct;56(5):404-6[↩]
- Landau ME, Campbell WW. Clinical features and electrodiagnosis of ulnar neuropathies. Phys Med Rehabil Clin N Am. 2013 Feb;24(1):49-66.[↩]
- Idler RS. General principles of patient evaluation and nonoperative management of cubital syndrome. Hand Clin. 1996 May;12(2):397-403[↩]
- Shea JD, McClain EJ. Ulnar-nerve compression syndromes at and below the wrist. J Bone Joint Surg Am. 1969 Sep;51(6):1095-103.[↩]
- Chang KV, Wu WT, Han DS, Özçakar L. Ulnar Nerve Cross-Sectional Area for the Diagnosis of Cubital Tunnel Syndrome: A Meta-Analysis of Ultrasonographic Measurements. Arch Phys Med Rehabil. 2018 Apr;99(4):743-757[↩]
- Terayama Y, Uchiyama S, Ueda K, Iwakura N, Ikegami S, Kato Y, Kato H. Optimal Measurement Level and Ulnar Nerve Cross-Sectional Area Cutoff Threshold for Identifying Ulnar Neuropathy at the Elbow by MRI and Ultrasonography. J Hand Surg Am. 2018 Jun;43(6):529-536[↩]
- Chen IJ, Chang KV, Wu WT, Özçakar L. Ultrasound Parameters Other Than the Direct Measurement of Ulnar Nerve Size for Diagnosing Cubital Tunnel Syndrome: A Systemic Review and Meta-analysis. Arch Phys Med Rehabil. 2018 Jul 25[↩]
- Dellon AL, Hament W, Gittelshon A. Nonoperative management of cubital tunnel syndrome: an 8-year prospective study. Neurology. 1993 Sep;43(9):1673-7[↩]
- vanVeen KE, Alblas KC, Alons IM, Kerklaan JP, Siegersma MC, Wesstein M, Visser LH, Vankasteel V, Jellema K. Corticosteroid injection in patients with ulnar neuropathy at the elbow: A randomized, double-blind, placebo-controlled trial. Muscle Nerve. 2015 Sep;52(3):380-5[↩]
- Caliandro P, La Torre G, Padua R, Giannini F, Padua L. Treatment for ulnar neuropathy at the elbow. Cochrane Database Syst Rev. 2016 Nov 15;11:CD006839[↩]
- Natural history and conservative management of cubital tunnel syndrome. Szabo RM, Kwak C. Hand Clin. 2007 Aug; 23(3):311-8, v-vi.[↩]





{kind=link}