Contents
What is vocal cord paralysis
Vocal cord paralysis occurs when the nerve impulses to your voice box (larynx) are disrupted. This results in paralysis of the vocal cord muscles.
Your vocal folds are inside your larynx, or voice box. When you talk, air moves from your lungs through the vocal folds to your mouth. The vocal folds vibrate to produce sound. Anything that makes it harder for the vocal folds to vibrate can cause a voice problem. Vocal fold paralysis happens when one or both vocal folds are not able to move. Vocal cord paralysis can affect your ability to speak, swallow and even breathe. That’s because your vocal cords, sometimes called vocal folds, do more than just produce sound. They also protect your airway by preventing food, drink and even your saliva from entering your windpipe (trachea) and causing you to choke.
There are different types of vocal fold paralysis. Bilateral vocal fold paralysis means that both vocal folds will not move. They become stuck halfway between open and closed. People with this condition often need a tracheotomy, which is an opening made in the neck. They breathe through this opening, and it keeps food from going into their lungs when they eat.
Unilateral vocal fold paralysis is when only one fold will not move or only moves a little bit. It is more common than bilateral paralysis. The paralyzed vocal fold does not vibrate with the other fold. The person’s voice will not sound clear or loud. They may run out of air when speaking.
Vocal fold movements are a result of the coordinated contraction of various muscles that are controlled by the brain through a specific set of nerves.
The superior laryngeal nerve (superior laryngeal nerve) carries signals to the cricothyroid muscle. Since this muscle adjusts the tension of the vocal fold for high notes during singing, superior laryngeal nerve paresis and paralysis result in abnormalities in voice pitch and the inability to sing with smooth change to each higher note. Sometimes patients with superior laryngeal nerve paresis/paralysis may have a normal speaking voice but an abnormal singing voice.
The recurrent laryngeal nerve (recurrent laryngeal nerve) carries signals to different voice box muscles responsible for opening vocal folds (as in breathing, coughing), closing the folds for vibration during voice use, and closing them during swallowing. The recurrent laryngeal nerve goes into the chest cavity and curves back into the neck until it reaches the larynx. Because the nerve is relatively long and takes a “detour” to the voice box, it is at greater risk for injury from different causesinfections and tumors of the brain, neck, chest, or voice box. It can also be damaged by complications during surgery in the head, neck, or chest, that directly injure, stretch, or compress the nerve. Consequently, the recurrent laryngeal nerve is involved in the majority of cases of vocal fold paresis/paralysis.
There are a number of causes of vocal cord paralysis including nerve damage during surgery, viral infections and certain cancers. Treatment for vocal cord paralysis usually involves surgery. Voice therapy can sometimes be an option.
Figure 1. Larynx and pharynx anatomy
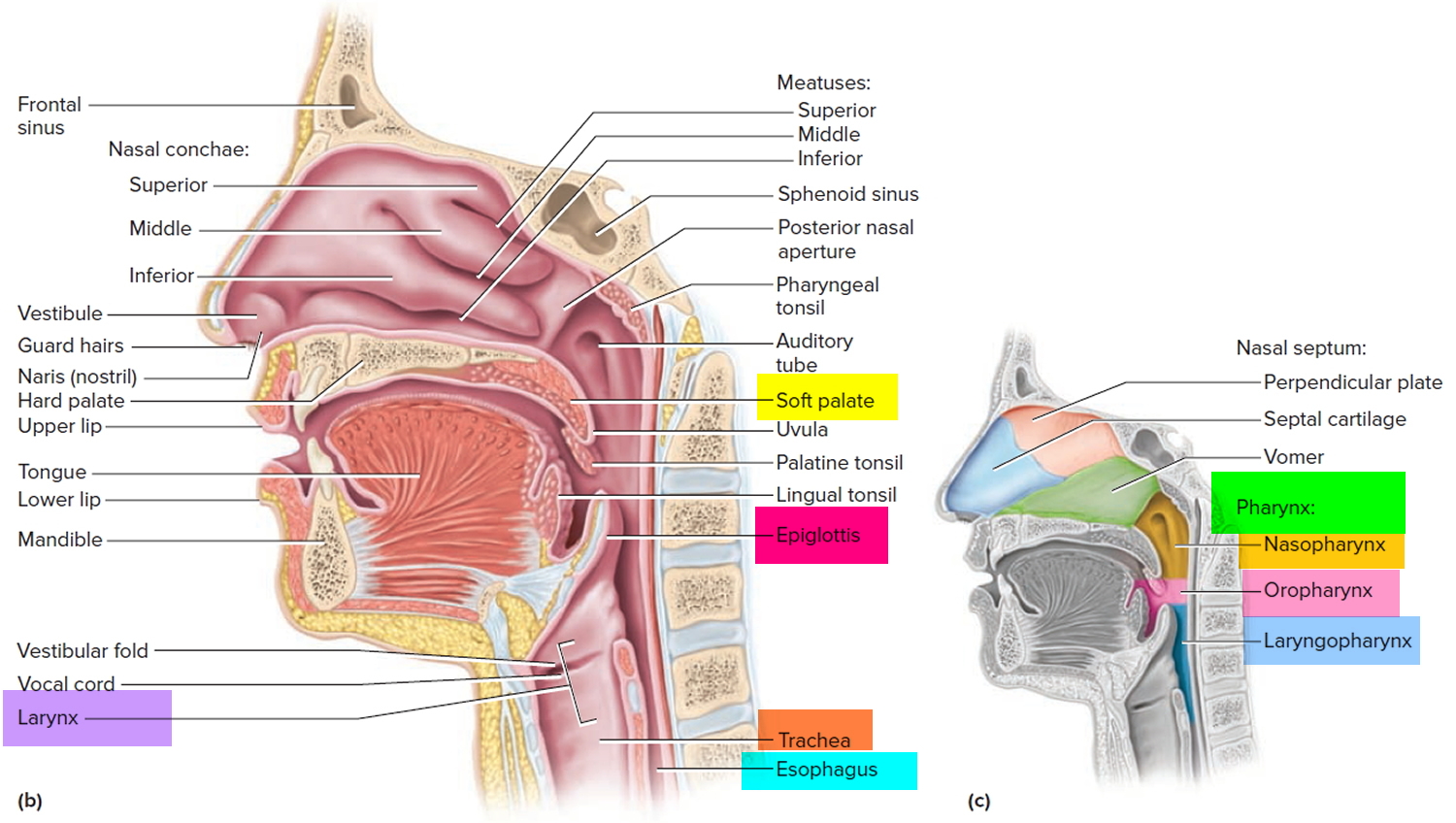
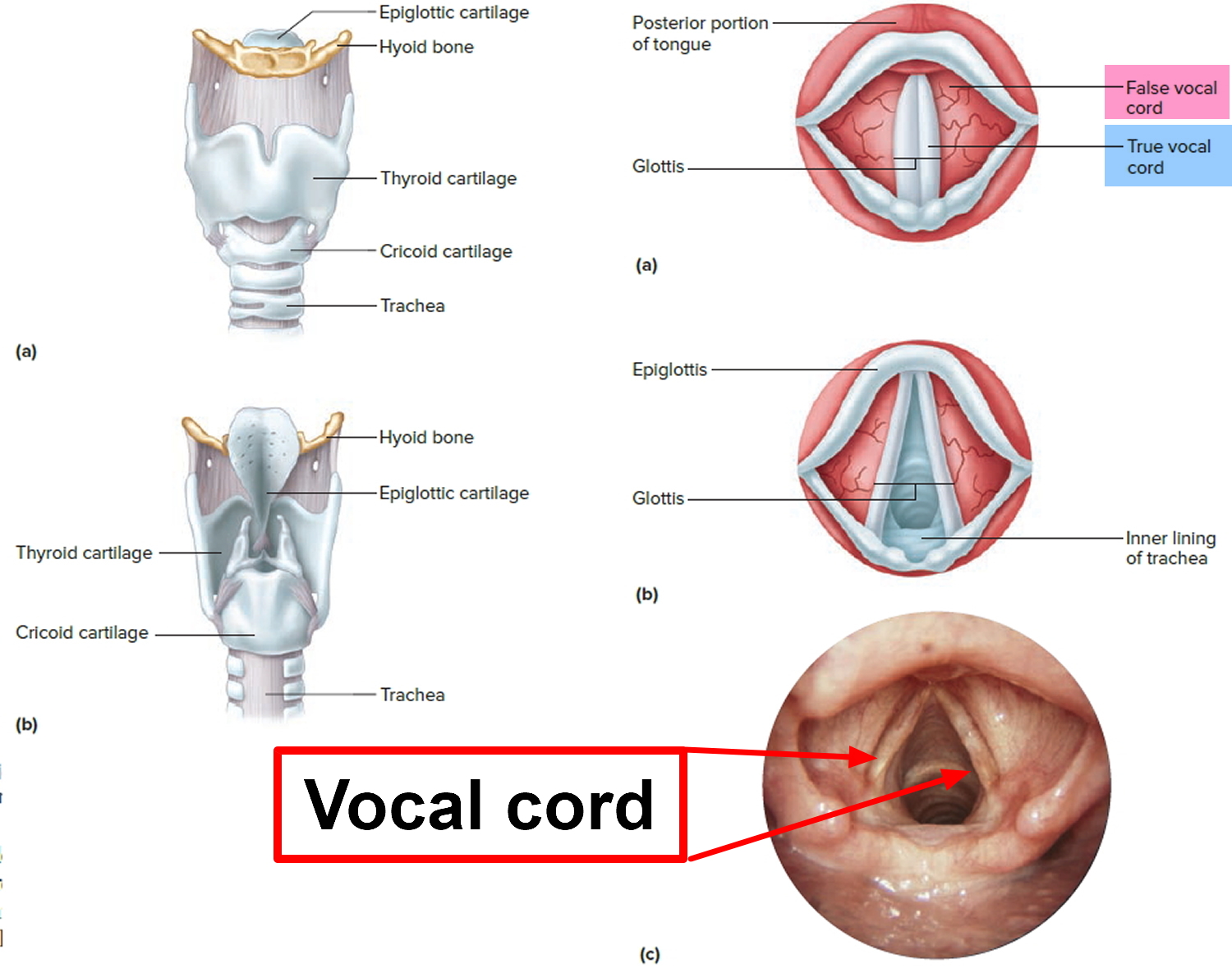
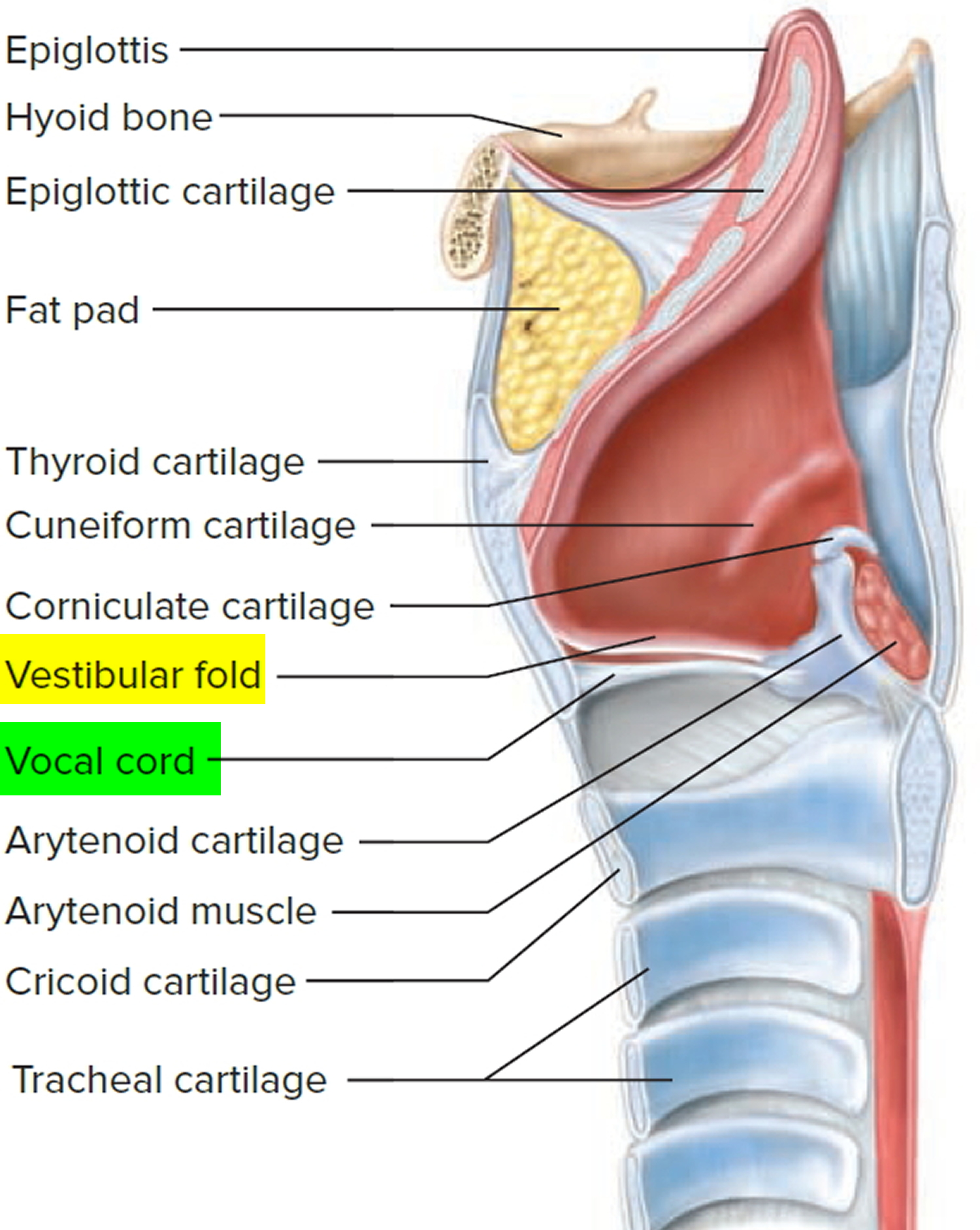
Figure 2. Larynx anatomy
Vocal cord paralysis causes
What causes vocal cord paralysis
In vocal cord paralysis, the nerve impulses to your voice box (larynx) are disrupted, resulting in paralysis of the muscle. The vagus nerve runs from the brainstem to the larynx. This nerve controls vocal fold movement. Anything that damages this nerve can cause paralysis. Despite advances in diagnostic technology, doctors are unable to detect the cause in about half of all vocal fold paralyses, referred to as idiopathic (due to unknown origins). In these cases, paralysis or paresis might be due to a viral infection affecting the voice box nerves (recurrent laryngeal nerve and superior laryngeal nerve), or the vagus nerve, but this cannot be proven in most cases. Known causes may include:
- Injury to the vocal cord during surgery. Surgery on or near your neck or upper chest can result in damage to the nerves that serve your voice box. Surgeries that carry a risk of damage include surgeries to the thyroid or parathyroid glands, esophagus, neck, and chest.
- Neck or chest injury. Trauma to your neck or chest may injure the nerves that serve your vocal cords or the voice box itself.
- Stroke. A stroke interrupts blood flow in your brain and may damage the part of your brain that sends messages to the voice box.
- Tumors of the skull base, neck, and chest: Tumors (both cancerous and non-cancerous) can grow around nerves and squeeze them, resulting in varying degrees of paresis or paralysis. Tumors can also grow in or around the muscles, cartilage or nerves controlling the function of your voice box and can cause vocal cord paralysis.
- Viral infections. Some viral infections, such as Lyme disease, Epstein-Barr and herpes, can cause inflammation and damage directly to the vagus nerve or its nerve branches to the voice box (recurrent laryngeal nerve and superior laryngeal nerve) in the larynx.
- Neurological conditions. If you have certain neurological conditions, such as multiple sclerosis or Parkinson’s disease, you may experience vocal cord paralysis.
Risk factors of developing vocal cord paralysis
Factors that may increase your risk of developing vocal cord paralysis include:
- Undergoing throat or chest surgery. Surgery in the neck (thyroid gland, carotid artery) or in the chest (lungs, esophagus, heart, or large blood vessels) may inadvertently result in recurrent laryngeal nerve paresis or paralysis. The superior laryngeal nerve may also be injured during head and neck surgery.
- Complication from endotracheal intubation: Injury to the recurrent laryngeal nerve may occur when breathing tubes are used for general anesthesia or assisted breathing. However, this type of injury is rare, given the large number of operations done under general anesthesia.
- Having a neurological condition. People with certain neurological conditions — such as Parkinson’s disease or multiple sclerosis — are more likely to develop vocal cord weakness or paralysis.
Vocal cord paralysis complications
Breathing problems associated with vocal cord paralysis may be so mild that you just have a hoarse-sounding voice, or they can be so serious that they’re life-threatening.
Because vocal cord paralysis keeps the opening to the airway from completely opening or closing, other complications may include choking on or actually inhaling (aspirating) food or liquid. Aspiration that leads to severe pneumonia is very serious and requires immediate medical care.
Vocal cord paralysis symptoms
Your vocal cords are two flexible bands of muscle tissue that sit at the entrance to the windpipe (trachea). When you speak, the bands come together and vibrate to make sound. The rest of the time, the vocal cords are relaxed in an open position, so you can breathe.
In most cases of vocal cord paralysis, only one vocal cord is paralyzed. If both of your vocal cords are affected, you may have vocal difficulties, as well as significant problems with breathing and swallowing.
Vocal fold paralysis can cause problems that are mild or severe. Some signs and symptoms of vocal cord paralysis may include:
- A breathy quality to the voice
- Hoarseness
- Noisy breathing
- Loss of vocal pitch and loudness
- Choking or coughing while swallowing food, drink or saliva
- Being able to produce voice for a very short time. The need to take frequent breaths while speaking
- Inability to speak loudly
- Loss of your gag reflex
- Ineffective coughing
- Frequent throat clearing
- Possible pneumonia if food and liquid get into the lungs. This may happen if the vocal folds cannot close to protect the airway while swallowing.
Vocal cord paralysis diagnosis
Your doctor will ask about your symptoms and lifestyle, listen to your voice, and ask you how long you’ve had voice problems. To further evaluate your voice problems, the following tests may be performed:
- Laryngoscopy. Your doctor will look at your vocal cords using a mirror or a thin, flexible tube (known as a laryngoscope or endoscope) or both. You may also have a test called videostrobolaryngoscopy that’s done using a special scope that contains a tiny camera at its tip or a larger camera connected to the scope’s viewing piece. These special high-magnification endoscopes allow your doctor to view your vocal cords directly or on a video monitor to determine the movement and position of the vocal cords and whether one or both vocal cords are affected.
- Laryngeal electromyography. This test measures the electric currents in your voice box muscles. To obtain these measurements, your doctor typically inserts small needles into your vocal cord muscles through the skin of the neck. This test doesn’t usually provide information that might change the course of treatment, but it may give your doctor information about how well you may recover. This test is most useful for predicting how you’ll recover when it’s done between six weeks and six months after your symptoms began.
- Blood tests and scans. Because a number of diseases may cause a nerve to be injured, you may need additional tests to identify the cause of the paralysis. Tests may include blood work, X-rays, MRI or CT scans.
Vocal cord paralysis treatment
Treatment of vocal cord paralysis depends on the cause, the severity of symptoms and the time from the onset of symptoms. Treatment may include voice therapy, bulk injections, surgery or a combination of treatments.
Voice therapy is normally the first treatment option. After voice therapy, the decision for surgery depends on the severity of the symptoms, vocal needs of the patient, position of paralyzed vocal folds, prognosis for recovery, and the cause of paresis/paralysis, if known.
In some instances, you may get better without surgical treatment. For this reason, your doctor may delay permanent surgery for at least a year from the beginning of your vocal cord paralysis.
However, surgical treatment with bulk injections containing collagen-like substances is often done within the first 3 months of voice loss.
During the waiting period for surgery, your doctor may suggest voice therapy to help keep you from using your voice improperly while the nerves heal.
Voice therapy
Voice therapy sessions involve exercises or other activities to strengthen your vocal cords, improve breath control during speech, prevent abnormal tension in other muscles around the paralyzed vocal cord or cords and protect your airway during swallowing. Occasionally, voice therapy may be the only treatment you need if your vocal cords were paralyzed in a location that doesn’t require additional bulk or repositioning.
Vocal cord paralysis can be frustrating and sometimes debilitating, especially because your voice affects your ability to communicate. A speech therapist can help you develop the skills you need to communicate.
Even if you’re not able to regain the voice you once had, voice therapy can help you learn effective ways to compensate. In addition, a speech-language pathologist can teach you efficient ways to use your voice without causing further damage to the vocal mechanism.
Vocal cord paralysis surgery
If your vocal cord paralysis symptoms don’t fully recover on their own, surgical treatments may be offered to improve your ability to speak and to swallow.
Surgical options include:
- Bulk injection. Paralysis of the nerve to your vocal cord will probably leave the vocal cord muscle thin and weak. To add bulk to a paralyzed vocal cord, a doctor who specializes in disorders of the larynx (laryngologist) may inject your vocal cord with a substance such as body fat, collagen or another approved filler substance. This added bulk brings the affected vocal cord closer to the middle of your voice box so that the opposite functioning and moving vocal cord can make closer contact with the paralyzed cord when you speak, swallow or cough.
- Structural implants. Instead of using a bulk injection, this procedure — known as thyroplasty, medialization laryngoplasty or laryngeal framework surgery — relies on the use of an implant in the larynx to reposition the vocal cord. Rarely, people who have this surgery may need to have a second surgery to reposition the implant.
- Vocal cord repositioning. In this procedure, a surgeon moves a window of your own tissue from the outside of your voice box inward, pushing the paralyzed vocal cord toward the middle of your voice box. This allows your unimpaired vocal cord to better vibrate against its paralyzed partner.
- Replacing the damaged nerve (reinnervation). In this surgery, a healthy nerve is moved from a different area of the neck to replace the damaged vocal cord. It can take as long as six to nine months before the voice improves. Some doctors combine this surgery with a bulk injection.
- Tracheotomy. If both of your vocal cords are paralyzed and positioned closely together, your airflow will be decreased. In this situation, you’ll have a lot of trouble breathing and require a surgical procedure called a tracheotomy. In a tracheotomy, an incision is made in the front of your neck and an opening created directly into the windpipe (trachea). A breathing tube is inserted, allowing air to bypass the immobilized vocal cords.
Emerging treatments
Linking the vocal cords to an alternative source of electrical stimulation — perhaps a nerve from another part of the body or a device similar to a cardiac pacemaker — may restore opening and closing of the vocal cords. Researchers continue to study this and other options.





{kind=link}