
Contents
What is a breast lump
A breast lump is a growth of tissue that develops within your breast. If you feel a lump in your breast, you should always get it checked by a doctor. Most breast lumps are harmless but some can be breast cancer. It is also important crucial that women are aware that a lump is not the only symptom of breast cancer. If you are worried about any breast symptoms, the best thing to do is to get it checked by a doctor as soon as possible. Around one in six women (17 per cent) diagnosed with breast cancer go to their doctor with a symptom other than a breast lump – the most commonly reported breast cancer symptom – according to new research presented at the 2016 National Cancer Research Institute 1.
Breast lumps in men is often due to gynecomastia, however men can also develop breast cancer. The diagnosis for breast lumps in men is the same as in women, that is mammogram, ultrasound and fine needle aspiration cytology (FNAC) or biopsy (taking a tissue sample for lab analysis).
Clinical breast exam and breast self-exam
Research has not shown a clear benefit of regular physical breast exams done by either a health professional (clinical breast exams) or by yourself (breast self-exams). There is very little evidence that these tests help find breast cancer early when women also get screening mammograms 2. Most often when breast cancer is detected because of symptoms (such as a lump), a woman discovers the symptom during usual activities such as bathing or dressing. Women should be familiar with how their breasts normally look and feel and report any changes to a health care provider right away.
See a doctor if you notice:
- a lump in your breast or armpit
- any other unusual changes in your breasts – such as the nipple turning inwards, dimpled skin or bloodstained nipple discharge
- the lump feels firm or fixed
- the lump persists beyond four to six weeks
- you notice skin changes on your breast, such as redness, crusting, dimpling or puckering
- you have discharge, possibly bloody, from your nipple
- your nipple is turned inward and isn’t normally positioned that way
- you can feel enlarging lumps in your armpit
Don’t try to self-diagnose the cause of your lump – always see a doctor. Changes in the breasts can be a sign of breast cancer. This is easier to treat if it’s found early. Finding breast cancer early and getting state-of-the-art cancer treatment are the most important strategies to prevent deaths from breast cancer. Breast cancer that’s found early, when it’s small and has not spread, is easier to treat successfully. Getting regular screening tests is the most reliable way to find breast cancer early.
What happens at the breast clinic
At the hospital or breast clinic, you may have a:
- breast examination
- scan – usually a breast X-ray (mammogram) or ultrasound
- biopsy – where a needle is inserted into the lump to remove some cells for testing
These tests are often done during the same visit. You’ll usually be told the results on the same day, although biopsy results take longer – you should get them within a week.
Treatment for a lump depends on the cause. Most are harmless and may go away on their own without treatment.
Figure 1. Normal breast (female)
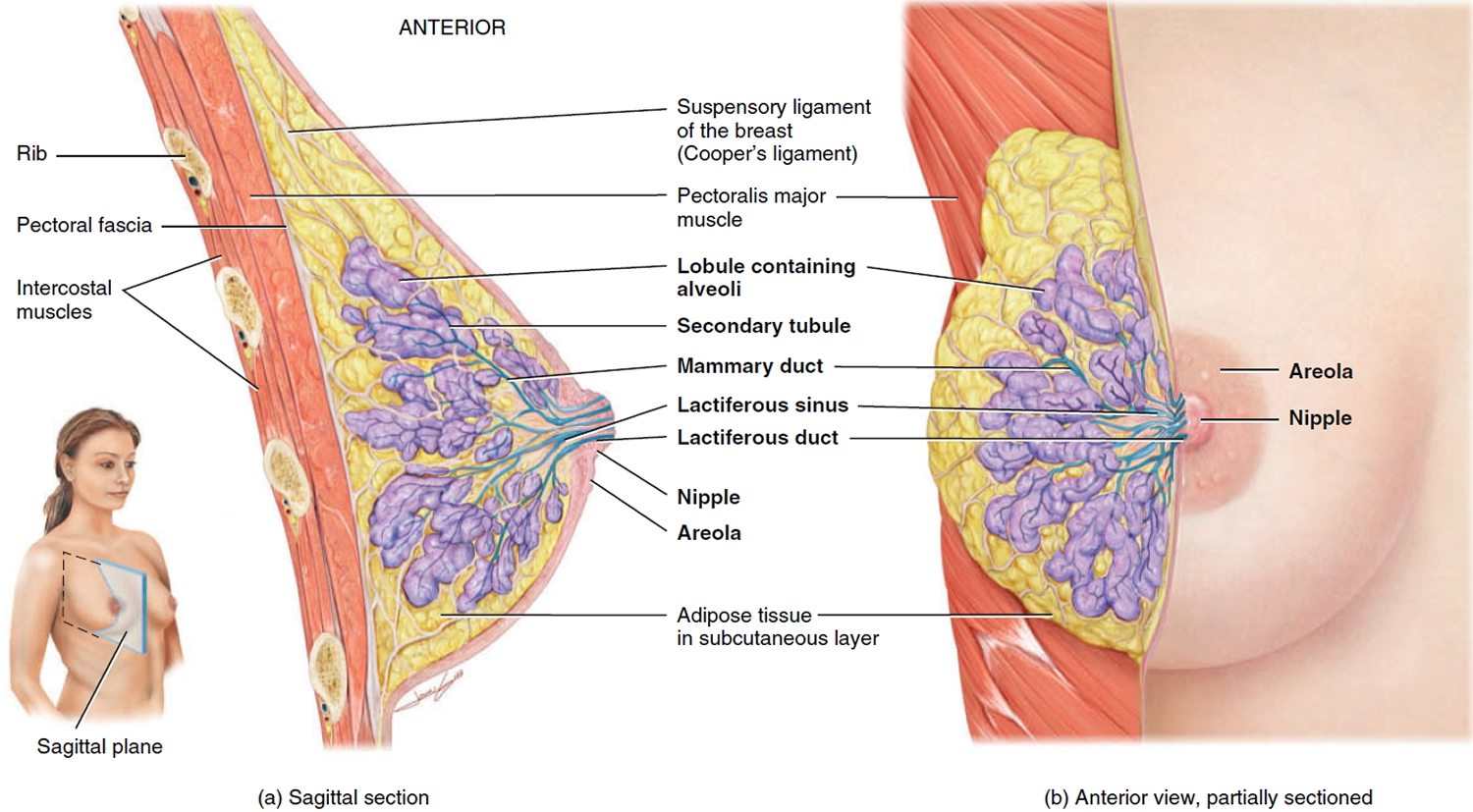
Types of breast lumps
Different types of breast lumps can vary in the way they look and feel. You may perceive a lump as a mass, growth, swelling, thickness or fullness.
You might notice:
- A distinct lump with definite borders
- A firm, hard area within your breast
- A thickened, slightly more prominent area in your breast that’s different from surrounding breast tissue
- Other breast changes, such as redness, dimpling or pitting of the skin
- One breast that’s noticeably larger than the other
- Nipple changes, such as a nipple that’s pulled inward or spontaneous fluid discharge from your nipple
- Persistent breast pain or tenderness, which might increase during your menstrual period
Sometimes, a breast lump is a sign of breast cancer. That’s why you should seek prompt medical evaluation. Fortunately, however, most breast lumps result from noncancerous (benign) conditions.
What causes breast lumps
- Don’t try to self-diagnose the cause of your lump – always see a doctor.
Lumps in the breasts can have lots of different causes.
Most are due to something harmless, such as a non-cancerous tissue growth (fibroadenoma) or a build-up of fluid (breast cyst).
But sometimes they can be a sign of something serious, such as breast cancer.
Breast lumps can be caused by:
- Breast cancer
- Breast cysts (a fluid-filled sac in your breast that’s usually benign)
- Fibroadenoma (a solid, benign mass most common in young women)
- Fibrocystic breasts (lumpy or rope-like breast tissue)
- Injury or trauma to the breast
- Intraductal papilloma (a benign, wartlike growth in a milk duct)
- Lipoma (a slow-growing, doughy mass that’s usually harmless)
- Mastitis (an infection in breast tissue that most commonly affects women who are breast-feeding)
- Milk cyst (galactocele) — a milk-filled cyst that’s usually harmless
Breast cancer
Breast cancers can start from different parts of the breast. Most breast cancers begin in the ducts that carry milk to the nipple (ductal cancers). Some start in the glands that make breast milk (lobular cancers). There are also other types of breast cancer that are less common.
A small number of cancers start in other tissues in the breast. These cancers are called sarcomas and lymphomas and are not really thought of as breast cancers.
Although many types of breast cancer can cause a lump in the breast, not all do. Many breast cancers are found on screening mammograms which can detect cancers at an earlier stage, often before they can be felt, and before symptoms develop. There are other symptoms of breast cancer you should watch for and report to a health care provider.
It’s also important to understand that most breast lumps are benign and not cancer (malignant). Non-cancerous breast tumors are abnormal growths, but they do not spread outside of the breast and they are not life threatening. But some benign breast lumps can increase a woman’s risk of getting breast cancer. Any breast lump or change needs to be checked by a health care professional to determine if it is benign or malignant (cancer) and if it might affect your future cancer risk.
Breast cancer symptoms
Breast cancer is usually not painful in the early stages. But some things may be signs of breast cancer – or a non-cancerous lump. It is important to see your doctor very soon if you notice any of the following changes 3:
- One breast changes size or shape
- You can feel a lump in a breast or armpit
- There is a sunken dip (dimple) on the nipple or elsewhere on the breast
- Red or scaly skin on a breast that doesn’t go away
- A clear or bloody fluid comes out of a nipple
It is very important to see a doctor about these symptoms soon.
Abnormalities may also be discovered through breast cancer screening (a physical examination, ultrasound or mammography). If this is the case, further examinations can be done to take a closer look at the area.
Breast cancer causes and risk factors
Breast cancer can develop when the genetic material in cells changes (“mutates”) and causes them to start multiplying in an uncontrolled way. Lumps and nodules then form after some time. Why those changes come about, and how the cells develop, depends on many factors that can influence each other. The main factors include the woman’s age, hormones, and whether there is a higher risk of breast cancer in her family. But sometimes genetic mutations happen for no particular reason.
Breast cancer is more common in some families. If your mother or sister (a first-degree relative) develops the disease, that doubles your risk of getting it. If, on the other hand, a more distant relative has breast cancer, that hardly affects your risk.
About 5 to 10% of all breast cancer cases are known to be caused by gene mutations (changes) due to “hereditary breast cancer.” The mutations mainly affect the genes known as BRCA1 and BRCA2. The abbreviation “BRCA” stands for “breast cancer gene.” About 45 to 65% of women with these mutations develop breast cancer before the age of 69.
Some women worry that they might be partly to blame for getting cancer because of their lifestyle. But lifestyle only plays a small role overall. You may also hear theories that certain character traits can increase a person’s risk of getting cancer. These theories have never been proven, though, and are now considered to be outdated. Nobody is to blame for a serious disease like cancer. Anyone can get cancer, regardless of their lifestyle or character traits.
Breast cancer diagnosis
If you find a lump in your breast, notice changes in breast skin, find a swollen lymph node in your armpit or develop a nipple discharge. Your doctor is the first person to go to if you think you might have breast cancer. After discussing previous and/or current medical conditions (your medical history) with the doctor, he or she will perform a physical exam and you will need to have tests to find out if you have breast cancer. This may include the following:
- Diagnostic Mammography — Diagnostic mammograms focus on a specific area of the breast. A number of different views may be taken, including some that magnify the abnormality.
- Breast Ultrasound — Ultrasound, also called sonography, uses high-frequency sound waves to outline a part of the body. No radiation is involved in the procedure. Ultrasound is most often used to distinguish a solid mass from a cyst. It may also be used to guide a breast biopsy.
- Ductogram — This X-ray test can be helpful in finding the cause of a nipple discharge. A fine plastic tube is placed into the opening of the duct at the nipple. A small amount of contrast dye is injected, which outlines the shape of the duct when an X-ray image is taken.
- Magnetic Resonance Imaging (MRI) — Doctors are just starting to learn about how this imaging tool can be used to evaluate breast cancer. Your physician may recommend that you have a MRI of the breast, usually as part of a research study, to add to the information available from other tests.
- Nipple Discharge Examination — Some of the fluid may be collected and examined under a microscope to see if cancer cells are present. A red or red-brown discharge suggesting blood may be due to cancer. A clear or milky secretion is very unlikely to be cancer.
- Biopsy — A biopsy, a procedure in which a tissue sample is taken, must be performed to make sure that you have cancer. The diagnosis will be made by looking at the biopsy specimen under a microscope. There are several ways of performing biopsies, depending on where the suspicious area is located and whether it can be felt or seen with mammograms or ultrasound.
- Fine Needle Aspiration (FNA) Biopsy — In this procedure, a thin needle is guided into the abnormal area of the breast and a small amount of fluid or tissue is drawn out. To guide the needle, the physician will either palpate (feel) the lump, or use ultrasound.
- Core Needle Biopsy — This type of biopsy uses a larger needle than fine needle aspiration (FNA). It removes a small cylinder of tissue from the breast abnormality. If the lump can be felt, it is performed with local anesthesia in the doctor’s office. The needle is guided into position in the same way as for a FNA. If the abnormality cannot be felt, a stereotactic core biopsy is performed with computerized mammography.
- Surgical Biopsy — Surgery may be needed to remove all or part of a lump for examination. An excisional biopsy removes all of the lesion, and a surrounding margin of normal-appearing tissue. This is usually performed in a hospital outpatient department with local anesthesia and a sedative.
Sometimes the surgeon will have the radiologist mark the area right before surgery with a wire for localization. The area is numbed with local anesthetic and a thin hollow needle is placed with X-ray guidance in the suspicious area. Then a thin wire is inserted through the needle, with a small hook on the end to keep it in place. The needle is then removed and the wire is used to guide the surgeon to the area that must be removed.
If a breast tumor is detected, your doctor will also check whether the tumor has spread to the other breast or any other parts of the body. This can be done using an ultrasound examination or x-ray of the other breast, an x-ray of the chest (thorax), a bone scan (bone scintigraphy), an ultrasound of the liver, or a computed tomography (CT) scan. If anything abnormal is detected, that part of the body can be examined more closely.
After all the tests have been done, the breast cancer is then “classified.” A classification system is used to record the tumor size and information about whether the lymph nodes are also affected or whether there are any metastases (whether the cancer has spread). The doctors will also assess how rapidly the tumor cells are growing and whether that growth can be influenced by hormones or certain growth factors. This classification is important when it comes to choosing the most suitable treatment.
How breast cancer spreads
Breast cancer can spread when the cancer cells get into the blood or lymph system and are carried to other parts of the body.
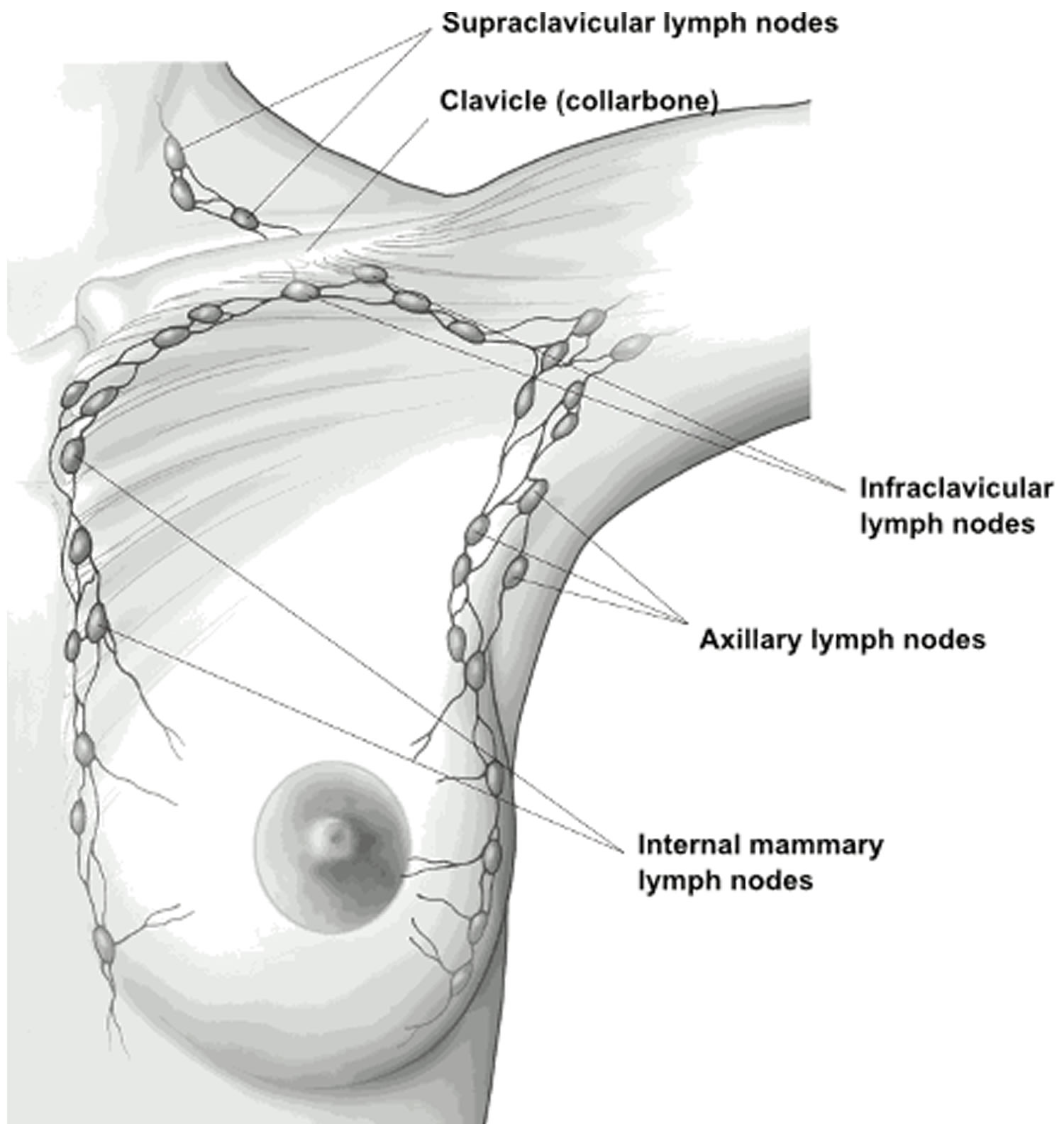
The lymph system is a network of lymph (or lymphatic) vessels found throughout the body that connects lymph nodes (small bean-shaped collections of immune system cells). The clear fluid inside the lymph vessels, called lymph, contains tissue by-products and waste material, as well as immune system cells. The lymph vessels carry lymph fluid away from the breast. In the case of breast cancer, cancer cells can enter those lymph vessels and start to grow in lymph nodes. Most of the lymph vessels of the breast drain into:
- Lymph nodes under the arm (axillary nodes)
- Lymph nodes around the collar bone (supraclavicular [above the collar bone] and infraclavicular [below the collar bone] lymph nodes)
- Lymph nodes inside the chest near the breast bone (internal mammary lymph nodes)
Figure 2. Lymph nodes around the breast
Breast cancer prognosis
The odds of successfully treating breast cancer depend on many factors. These factors include:
- the size of the tumor,
- whether the tumor is confined to breast tissue and where exactly it is located in the breast,
- whether the tumor growth is affected by hormones,
- whether the cancer cells have growth factor receptors (HER2 receptors) on them,
- how much the cancer cells have changed,
- the number of cancerous growths,
- whether the cancer cells have spread through the lymph vessels in the skin (inflammatory breast cancer),
- whether all of the tumor tissue can be removed,
- whether it has already spread to distant parts of the body, and
- whether the woman has already had breast cancer in the past.
Sometimes breast cancer is first diagnosed after it has already reached an advanced stage. In this case the cancer is often no longer only found in the breast and surrounding tissue. It may already have led to the growth of other tumors (metastatic tumors), for instance in bones or lymph nodes. But even if this happens the disease can still be treated.
If a tumor can be completely removed and there are no distant metastases, full recovery is possible. This is also true for breast cancer that returns after going away, known as recurrent breast cancer.
Breast cancer screening
American Cancer Society screenings recommendations for women at average breast cancer risk
The goal of screening tests for breast cancer is to find it before it causes symptoms (like a lump that can be felt). Screening refers to tests and exams used to find a disease in people who don’t have any symptoms. Early detection means finding and diagnosing a disease earlier than if you’d waited for symptoms to start.
Breast cancers found during screening exams are more likely to be smaller and still confined to the breast. The size of a breast cancer and how far it has spread are some of the most important factors in predicting the prognosis (outlook) of a woman with this disease.
American Cancer Society screenings recommendations for women at average breast cancer risk
These guidelines are for women at average risk for breast cancer. For screening purposes, a woman is considered to be at average risk if she doesn’t have a personal history of breast cancer, a strong family history of breast cancer, or a genetic mutation known to increase risk of breast cancer (such as in a BRCA gene), and has not had chest radiation therapy before the age of 30. (See below for guidelines for women at high risk.)
- Women between 40 and 44 have the option to start screening with a mammogram every year.
- Women 45 to 54 should get mammograms every year.
- Women 55 and older can switch to a mammogram every other year, or they can choose to continue yearly mammograms. Screening should continue as long as a woman is in good health and is expected to live 10 more years or longer.
All women should understand what to expect when getting a mammogram for breast cancer screening – what the test can and cannot do.
Mammograms
Regular mammograms can help find breast cancer at an early stage, when treatment is most successful. A mammogram can find breast changes that could be cancer years before physical symptoms develop. Results from many decades of research clearly show that women who have regular mammograms are more likely to have breast cancer found early, are less likely to need aggressive treatment like surgery to remove the breast (mastectomy) and chemotherapy, and are more likely to be cured.
Mammograms are not perfect. They miss some cancers. And sometimes a woman will need more tests to find out if something found on a mammogram is or is not cancer. There’s also a small possibility of being diagnosed with a cancer that never would have caused any problems had it not been found during screening. It’s important that women getting mammograms know what to expect and understand the benefits and limitations of screening.
American Cancer Society screening recommendations for women at high risk
Women who are at high risk for breast cancer based on certain factors should get an MRI and a mammogram every year, typically starting at age 30. This includes women who:
- Have a lifetime risk of breast cancer of about 20% to 25% or greater, according to risk assessment tools that are based mainly on family history (see below)
- Have a known BRCA1 or BRCA2 gene mutation (based on having had genetic testing)
- Have a first-degree relative (parent, brother, sister, or child) with a BRCA1 or BRCA2 gene mutation, and have not had genetic testing themselves
- Had radiation therapy to the chest when they were between the ages of 10 and 30 years
- Have Li-Fraumeni syndrome, Cowden syndrome, or Bannayan-Riley-Ruvalcaba syndrome, or have first-degree relatives with one of these syndromes
The American Cancer Society recommends against MRI screening for women whose lifetime risk of breast cancer is less than 15%.
There’s not enough evidence to make a recommendation for or against yearly MRI screening for women who have a higher lifetime risk based on certain factors , such as:
- Having a personal history of breast cancer, ductal carcinoma in situ (DCIS), lobular carcinoma in situ (LCIS), atypical ductal hyperplasia (ADH), or atypical lobular hyperplasia (ALH)
- Having “extremely” or “heterogeneously” dense breasts as seen on a mammogram
If MRI is used, it should be in addition to, not instead of, a screening mammogram. This is because although an MRI is more likely to detect cancer than a mammogram, it may still miss some cancers that a mammogram would detect.
Most women at high risk should begin screening with MRI and mammograms when they are 30 and continue for as long as they are in good health. But a woman at high risk should make the decision to start with her health care providers, taking into account her personal circumstances and preferences.
Tools used to assess breast cancer risk
Several risk assessment tools are available to help health professionals estimate a woman’s breast cancer risk. These tools give approximate, rather than precise, estimates of breast cancer risk based on different combinations of risk factors and different data sets.
Because the different tools use different factors to estimate risk, they may give different risk estimates for the same woman. Two models could easily give different estimates for the same person.
Risk assessment tools that include family history in first-degree relatives (parents, siblings, and children) and second-degree relatives (such as aunts and cousins) on both sides of the family should be used with the American Cancer Society guidelines to decide if a woman should have MRI screening. The use of any of the risk assessment tools and its results should be discussed by a woman with her health care provider.
Breast cancer treatment
The treatment options always depend on the type and size of the tumor, where it has spread to (if it has spread), the patient’s general health, as well as their personal preferences. Breast cancer can be treated with surgery, radiation and medication. Different treatment approaches are often combined.
The standard treatment is to try to surgically remove as much of the tumor as possible. Neighboring lymph nodes are sometimes also removed. If the tumor is small, women are often faced with a decision: Should they keep the breast or have it completely removed? Nowadays many women can have surgery that allows them to keep the breast (breast-conserving surgery). But sometimes the entire breast needs to be removed (mastectomy) to make sure that all of the tumor tissue has gone.
Chemotherapy (treatment with medication) is sometimes used to shrink larger tumors before surgery and make it easier to operate on them. This kind of treatment is called “neoadjuvant chemotherapy.”
Chemotherapy is sometimes used after surgery too. Women who have a hormone-sensitive tumor may have anti-hormonal therapy. This aims to slow down tumor growth.
After breast-conserving surgery the surrounding tissue is exposed to radiation, if possible, so that any remaining tumor cells can be destroyed. This is sometimes necessary after a mastectomy as well. Radiotherapy is also commonly used if the tumor cannot be surgically removed.
The different types of treatment can be very difficult to go through and sometimes have very severe side effects or cause other medical problems. The side effects vary depending on the kind of treatment, but they are often easy to treat. The treatment of side effects is part of what is known as supportive care.
Before deciding on whether to have a particular treatment, there is usually enough time to get information from your doctor about the possible benefits and the expected side effects, and to talk with your family or other people who are close to you. You have the right to seek a second opinion from another doctor or to decide not to have a treatment.
- Typical and atypical symptoms in women with breast cancer: Evidence of variation in diagnostic intervals from a national audit of cancer diagnosis. http://abstracts.ncri.org.uk/abstract/typical-and-atypical-symptoms-in-women-with-breast-cancer-evidence-of-variation-in-diagnostic-intervals-from-a-national-audit-of-cancer-diagnosis[↩]
- American Cancer Society Recommendations for the Early Detection of Breast Cancer. https://www.cancer.org/cancer/breast-cancer/screening-tests-and-early-detection/american-cancer-society-recommendations-for-the-early-detection-of-breast-cancer.html[↩]
- Breast cancer: Overview. https://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0072606/[↩]


{kind=link}