
Contents
What is dysphonia
Dysphonia commonly known as hoarseness, is any impairment of the voice or difficulties in speaking arising from physical disorders of the mouth or vocal cords 1. The terms hoarseness and dysphonia are often used interchangeably, although hoarseness is a symptom of altered voice quality and dysphonia is a diagnosis 1. Dysphonia may be broadly defined as altered vocal quality, pitch, loudness or vocal effort that impairs social and professional communication 2. In contrast, hoarseness is a coarse or rough quality to the voice 1.
Nearly one-third of the population has impaired voice production at some point in their lives 3. Dysphonia is more prevalent in certain groups, such as teachers and older adults, but all age groups and both genders can be affected 3. In addition to the impact on health and quality of life 4, dysphonia leads to frequent health care visits. The economic burden of dysphonia is substantial. An estimated 7.2% of the general population misses work for at least 1 day because of voice problems; this represents approximately $2.5 billion in annual work productivity lost in the United States 5. Therefore, dysphonia may be considered a public health challenge.
Dysphonia is often caused by benign or self-limited conditions, but may also be the presenting symptom of a more serious or progressive condition requiring prompt diagnosis and management.
Dysphonia is an important but under recognized adverse effect of numerous medications, with a lifetime prevalence of 29.9% in adults aged 65 years or younger 6. Women are more frequently affected than men (female to male ratio, 3:2) 7. The prevalence of dysphonia (hoarseness) is higher in individuals who use their voice extensively in their profession; for example, 31% of telemarketers 8, aerobics instructors (44%) 9 and 58% of teachers are affected 10.
Dysphonia has significant public health implications. Patients suffer social isolation, depression, and reduced disease-specific and general quality of life 3. For example, patients with dysphonia caused by neurologic disorders (Parkinson’s disease, spasmodic dysphonia, vocal tremor, or vocal fold paralysis) reported severe levels of voice handicap and reduced general health-related quality of life, comparable to impairments observed in patients with congestive heart failure,
angina, and chronic obstructive pulmonary disease 4.
Conditions leading to suspicion of a “serious underlying cause”
- Hoarseness with a history of tobacco or alcohol use
- Hoarseness with concomitant discovery of a neck mass
- Hoarseness after trauma
- Hoarseness associated with coughing up blood (hemoptysis), difficulty swallowing (dysphagia), painful swallowing (odynophagia), ear pain (otalgia) or airway compromise
- Hoarseness with accompanying neurologic symptoms
- Hoarseness with unexplained weight loss
- Hoarseness that is worsening
- Hoarseness in an immunocompromised host
- Hoarseness and possible aspiration of a foreign body
- Hoarseness in a baby
- Unresolving hoarseness after surgery (intubation or neck surgery)
Spasmodic dysphonia
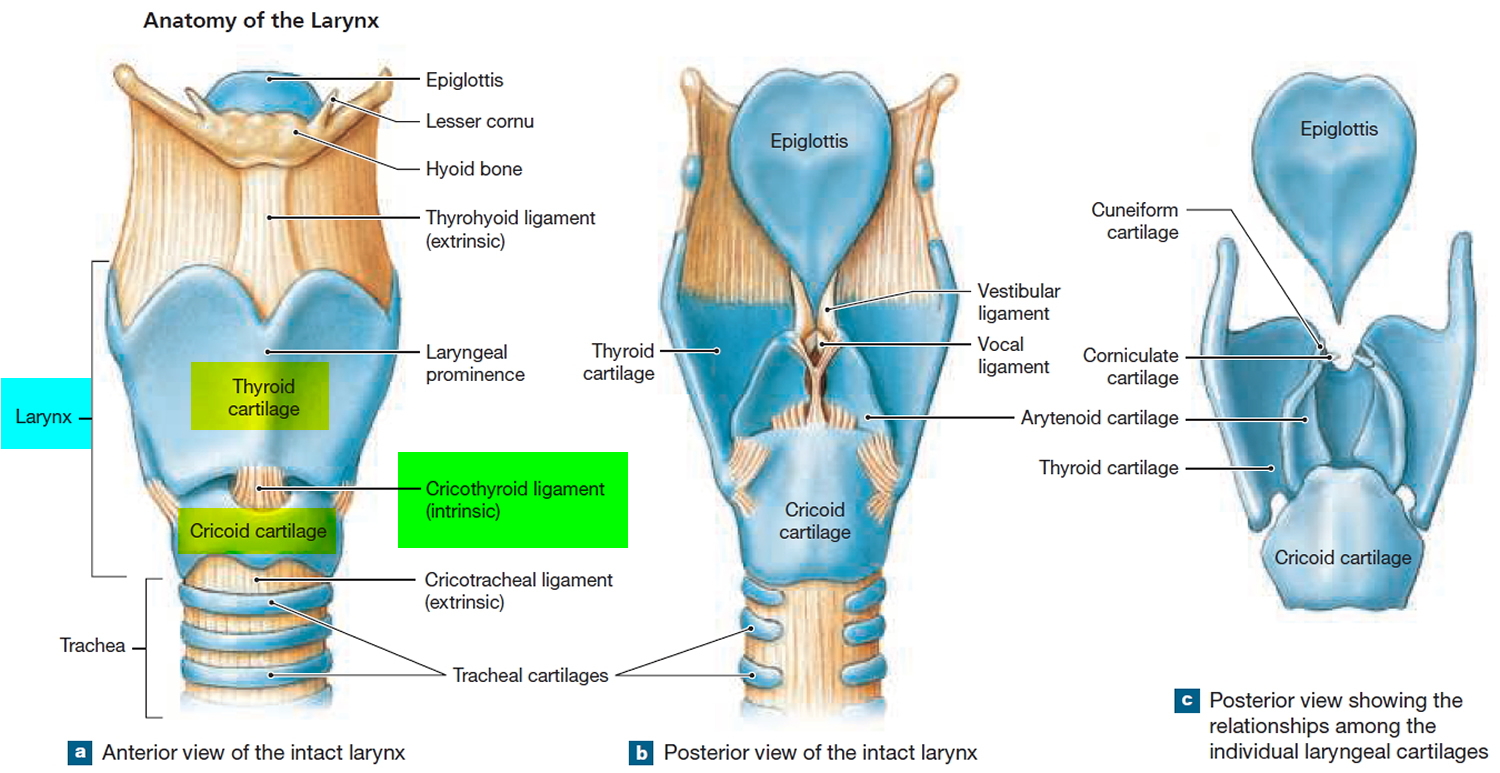
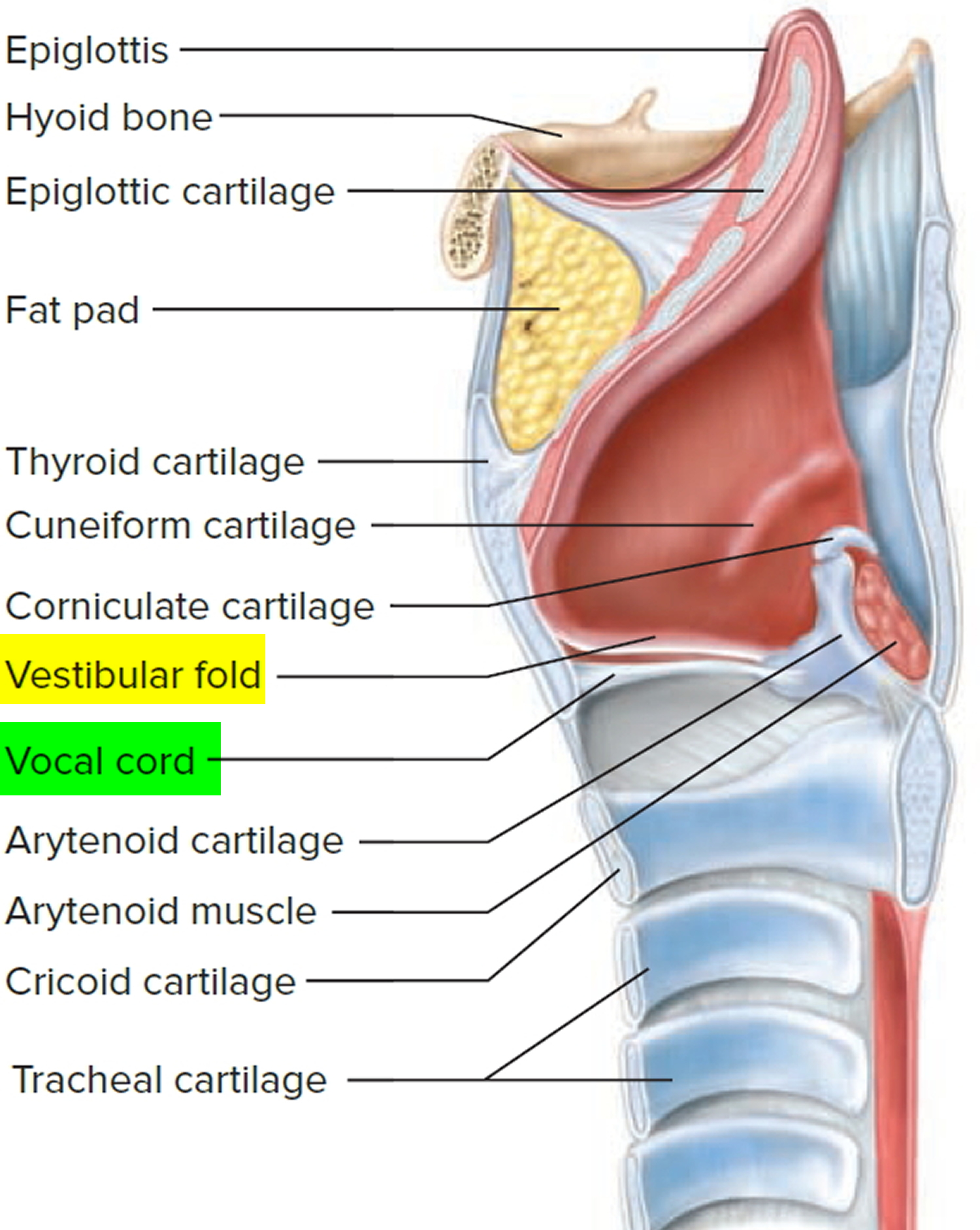
Spasmodic dysphonia is an uncommon voice disorder caused by a neurological disorder affecting the voice muscles in the larynx (laryngeal muscles and vocal cords) or voice box. When you speak, air from the lungs is pushed between two elastic structures—called vocal folds or vocal cords—with sufficient pressure to cause them to vibrate, producing voice (see Figures 1 and 2). In spasmodic dysphonia, the muscles inside the vocal folds experience sudden involuntary movements—called spasms—which interfere with the ability of the folds to vibrate and produce voice. Spasmodic dysphonia is also known as laryngeal dystonia.
The term spasmodic describes sudden and intermittent jerking movements of muscles and, as such, spasmodic dysphonia is characterised by poor vocal motor control during speech due to intermittent and involuntary spasms of the laryngeal muscles. spasmodic dysphonia is a task-specific disorder, which means that symptoms are only experienced while performing a specific task – in this case, speech. Emotive expressions such as screaming, crying and laughing are not affected and so spasmodic dysphonia is purely a speech disorder. Speech while whispering, shouting or singing appears to be less affected by the muscle contractions, and people may use one or more of these sensory “tricks” to try to alleviate the problem (e.g. speaking with a sing-song intonation or adopting an accent).
Spasmodic dysphonia causes voice breaks and can give the voice a tight, strained quality. People with spasmodic dysphonia may have occasional breaks in their voice that occur once every few sentences. Usually, however, the disorder is more severe and spasms may occur on every other word, making a person’s speech very difficult for others to understand. At first, symptoms may be mild and occur only occasionally, but they may worsen and become more frequent over time. Spasmodic dysphonia is a chronic condition that continues throughout a person’s life.
Spasmodic dysphonia can affect anyone. Spasmodic dysphonia is a rare disorder, occurring in roughly one to four people per 100,000 people. The first signs of spasmodic dysphonia are found most often in people between 30 and 50 years of age, but the average age that the condition is diagnosed is 39 years. Spasmodic dysphonia affects women more than men. Women make up around 60–80% of both subtypes of people with spasmodic dysphonia.
People with spasmodic dysphonia exert significant effort and strain to speak. There are two types of spasmodic dysphonia which display markedly different vocal symptoms. Very rarely, a person may experience both forms of spasmodic dysphonia.
Figure 1. Larynx and pharynx anatomy
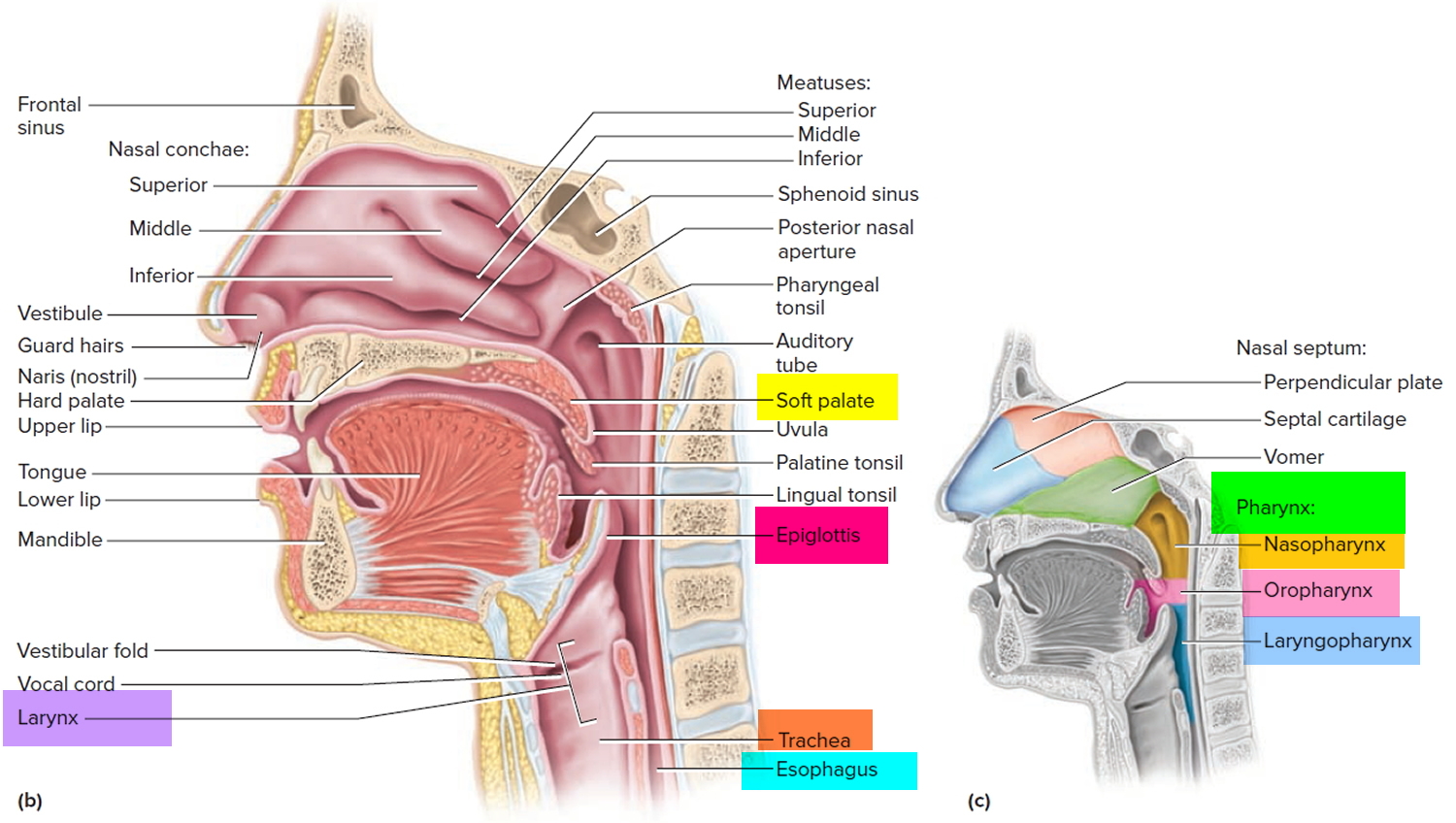
Figure 2. Larynx anatomy
Types of spasmodic dysphonia
- Adductor spasmodic dysphonia is the most common form of spasmodic dysphonia. It is characterized by spasms that cause the vocal folds to slam together and stiffen. These spasms make it difficult for the vocal folds to vibrate and produce sounds. Words are often cut off or are difficult to start because of muscle spasms. Therefore, speech may be choppy. The voice of someone with adductor spasmodic dysphonia is commonly described as strained or strangled and full of effort. The spasms are usually absent—and the voice sounds normal—while laughing, crying, or shouting. Stress often makes the muscle spasms more severe.
- Abductor spasmodic dysphonia is characterized by spasms that cause the vocal folds to open. The vocal folds cannot vibrate when they are open too far. The open position also allows air to escape from the lungs during speech. As a result, the voice often sounds weak and breathy. As with adductor spasmodic dysphonia, the spasms are often absent during activities such as laughing, crying, or shouting.
- Mixed spasmodic dysphonia, a combination of the above two types, is very rare. Because both the muscles that open and the muscles that close the vocal folds are not working properly, it has features of both adductor and abductor spasmodic dysphonia.
Spasmodic dysphonia causes
The cause of spasmodic dysphonia is unknown. Because the voice can sound normal or near normal at times, spasmodic dysphonia was once thought to be psychogenic, or originating in a person’s mind, rather than from a physical cause. In rare cases, psychogenic forms of spasmodic dysphonia do exist; however, in most instances, the muscle spasms are caused by abnormalities in the central nervous system (the brain).
A disorder that involves involuntary muscle contractions is also called a dystonia; therefore, another name for spasmodic dysphonia is laryngeal dystonia. Spasmodic dysphonia is considered a form of focal dystonia, a neurological disorder that affects muscle tone in one part of the body. Writer’s cramp is another type of focal dystonia. Other dystonias can affect multiple regions of the body or the entire body.
Spasmodic dysphonia may co-occur with other dystonias that cause involuntary and repetitious movement of such muscles as the eyes; face, body, arms, and legs; jaws, lips, and tongue; or neck.
Spasmodic dysphonia is thought to be caused by abnormal functioning in an area of the brain called the basal ganglia. The basal ganglia consist of several clusters of nerve cells deep inside the brain. They help coordinate movements of the muscles throughout the body. Recent research has found abnormalities in other regions of the brain, including the brainstem, the stalk-like part of the brain that connects to the spinal cord.
Symptoms of spasmodic dysphonia generally develop gradually and with no obvious explanation. Some people with spasmodic dysphonia also have vocal tremor, a shaking of the larynx and vocal folds that causes the voice to shake. Although the risk factors for spasmodic dysphonia have not been identified, the voice symptoms can begin following an upper respiratory infection, injury to the larynx, voice overuse, or stress.
In some cases, spasmodic dysphonia may run in families. Although 14 genes have been recently associated with various dystonias, only mutations in one gene, named THAP1, have been associated with forms of whole body dystonia that begin in childhood and that appear with spasmodic dysphonia. However, this genetic defect does not seem to be associated with the more usual form of focal spasmodic dysphonia that begins in adults.
Risk factors for developing spasmodic dysphonia
Unlike other dystonias, there have been no genes identified for spasmodic dysphonia, although this may be because the condition is so rare that family studies are difficult to conduct.
Spasmodic dysphonia occurs due to irregular inhibition (obstruction) of the laryngeal muscles. The mechanism for this inhibition is not clear. Post-mortem studies have determined that people with spasmodic dysphonia show decreased axonal and myelin density and increased numbers of inflammatory cells in areas of the brain that control laryngeal behavior.
The following have not been confirmed as risk factors for spasmodic dysphonia, but have been associated with the condition at the time of diagnosis:
- Major life stress;
- Upper respiratory tract infection;
- Autoimmune disorders;
- Antihistamine use; and
- Thyroid disorders.
Like other dystonias, stress and fatigue appear to make spasmodic dysphonia symptoms worse and could be a trigger for contracting the condition, but whether they are causes is still unknown.
How is spasmodic dysphonia diagnosed?
Diagnosis of spasmodic dysphonia is sometimes difficult because individuals with spasmodic dysphonia often have symptoms similar to other voice disorders. The diagnosis of spasmodic dysphonia usually is made following careful examination by a team that includes an otolaryngologist, a doctor who specializes in diseases of the ear, nose, throat, head, and neck; a speech-language pathologist, a health professional trained to evaluate and treat speech, language, and voice disorders; and a neurologist, a doctor who specializes in nervous system disorders.
The otolaryngologist examines the vocal folds for other possible causes of the voice disorder. A small lighted tube is passed through the nose and into the back of the throat—a procedure called fiberoptic nasolaryngoscopy—allowing the otolaryngologist to evaluate vocal fold structure and movement during speech and other activities. The speech-language pathologist evaluates the types of voice symptoms to see if they are characteristic of spasmodic dysphonia or other voice disorders and voice quality. The neurologist evaluates the patient for signs of other muscle movement disorders.
Spasmodic dysphonia treatment
There is currently no cure for spasmodic dysphonia; therefore, treatment can only help reduce its symptoms.
Firstly, it is important to develop coping and management skills, as spasmodic dysphonia symptoms worsen during stress and fatigue. Therefore people are taught ways to relax and respond to stress in a more positive manner, which may decrease the intensity of the laryngeal spasms.
In terms of physical treatments, destroying the nerve endings (denervation) in laryngeal muscles is the most successful treatment for spasmodic dysphonia. This is most commonly achieved temporarily with botulinum toxin.
Botulinum toxin (BoNT; Botox) injection
The most common treatment for spasmodic dysphonia is the injection of very small amounts of botulinum toxin directly into the affected muscles of the larynx. Botulinum toxin is produced by Clostridium botulinum, the same bacterium that occurs in improperly canned foods and honey. The toxin weakens muscles by blocking the nerve impulse to the muscle. Botulinum toxin injections generally improve the voice for a period of three to four months, after which the voice symptoms gradually return. Different people will respond differently to the treatment. Botulinum toxin injection will work better for some people than others, and some people will require repeat injections sooner than others. Reinjections after 3–6 months are necessary to maintain a good speaking voice. Initial side effects, including a temporary weak, breathy voice and occasional swallowing difficulties, usually subside after a few days to a few weeks. Botulinum toxin will relieve symptoms of most cases of adductor spasmodic dysphonia and is helpful in many cases of abductor spasmodic dysphonia.
Behavioral therapy (voice therapy) is another form of treatment that may work to reduce symptoms in mild cases. Other people may benefit from psychological counseling to help them accept and live with their voice problem.
In some cases, augmentative and alternative devices can help people with spasmodic dysphonia to communicate more easily. For example, some devices can help amplify a person’s voice in person or over the phone. Special software can be added to a computer or handheld device such as a personal digital assistant or cell phone to translate text into synthetic speech.
When more conventional measures have failed, surgery on the larynx may be performed. Long-term benefits and effects of this procedure are unknown.
Behavioral therapy (voice therapy)
Voice therapy is the treatment of choice for muscle tension dysphonia and there is evidence to support its utility in these cases 11. In complex disorders such as paradoxical vocal fold motion, voice therapy prevents long-term costs of treatment by helping reduce expensive emergency room visits and hospitalizations 12. Voice therapy techniques have been shown to improve voice in individuals without voice disorders, suggesting a role for therapy in the prevention of voice disorders 13.
Benign vocal fold lesions are a common cause of dysphonia 14. Many studies document excellent outcome after voice therapy in patients with a variety of benign lesions 15, 16. In cases in which surgery is necessary, pre- and post-operative voice therapy may shorten the postoperative recovery time, allowing faster return to work and limiting scar and permanent dysphonia 17.
Many laryngologists consider voice therapy essential for patients with unilateral vocal fold paralysis, as definitive treatment or as adjunctive to surgery 18. Evidence suggests that preoperative voice therapy improves voice outcomes for greater than 50% of patients with unilateral vocal fold paralysis and may render surgery unnecessary 19. In other neurological-based dysphonia such as Parkinsons disease, voice therapy has yielded significant improvement in overall communication 20.
In conclusion, research data and expert clinical experience support the use of voice therapy in the management of patients with acute and chronic voice disorders. Voice therapy contributes to increased effectiveness and efficiency in the treatment of voice disorders. When surgery is necessary, adjuvant voice therapy can improve surgical outcomes, prevent additional injury, and limit additional treatment costs.
Surgical treatment
Surgical treatment provides permanent structural changes to the larynx, and should only be considered for people who respond well to botulinum toxin injection and desire longer term management for their condition.
The aim of the procedure is to denervate the larynx to better control the muscle spasms. There is a risk of producing aphonia (an inability to speak), breathiness and swallowing difficulties after denervation. The risk of these adverse events must be weighed against the potential benefits.
Radiofrequency ablation
Radiofrequency ablation involves the use of a high frequency alternating current to destroy damaged or dysfunctional tissue. In the case of spasmodic dysphonia, the tissue destroyed is the dystonic laryngeal muscles. This is an advantageous procedure, as it is less invasive than surgery and does not require anaesthesia.
Radiofrequency ablation has been found to improve scores in acoustics and voice handicap two months after the operation. Radiofrequency also does not leave a scar on the neck. Some people will require further ablation or botulinum toxin injection one year after radiofrequency ablation.
Spasmodic dysphonia prognosis
Spasmodic dysphonia is a chronic disorder that develops suddenly and often in the third decade. Once developed, people tend to experience a gradual worsening of symptoms. If left untreated, the intensity of spasms is reduced over time in some people, indicating that eventually a change does occur in the muscles. However, very little is known in this area and it is not recommended to leave the condition untreated for this reason.
Dysphonia causes
Voice disorders are common in older adults and significantly affect the quality of life in these patients 21. Vocal fold atrophy with resulting hoarseness (dysphonia) is a common disorder of older adults and is frequently undiagnosed by primary care providers 22. Dysphonia resulting from neurologic disorders such as stroke and Parkinson disease is also more common in elderly patients 23. Multiple sclerosis can lead to dysphonia in patients of any age 24.
Chronic hoarseness (dysphonia) is quite common in young children and has an adverse impact on quality of life 25. Prevalence ranges from 15 percent to 24 percent of the population 26. In one study, 77 percent of hoarse children had vocal fold nodules 27. These may persist into adolescence if not properly treated 28. Craniofacial anomalies such as orofacial clefts are associated with abnormal voice 29, but these are frequently resonance disorders requiring very different therapies than for hoarse children with normal anatomical development.
Hoarseness or dysphonia in infants may be recognized only by an abnormal cry, and suspicion of such symptoms should prompt consultation with an otolaryngologist (ENT specialist) 30. When infants do present with hoarseness, underlying etiologies such as birth trauma, an intracranial process such as Arnold-Chiari malformation or posterior fossa mass, or mediastinal pathology should be considered 31.
Dysphonia (hoarseness) in tobacco smokers is associated with an increased frequency of polypoid vocal fold lesions and head and neck cancer 32. Accordingly, this requires an expedient assessment for malignancy as the potential cause of dysphonia. In addition, in patients treated with external beam radiation for glottic cancer, radiation treatment is associated with dysphonia in about 8 percent of cases 33.
Patients who use inhaled corticosteroids for the treatment of asthma or chronic obstructive pulmonary disease may present to a clinician with dysphonia that is a side effect of therapy either from direct irritation or from a fungal infection of the larynx 34.
Singers are also prone to develop microvascular ectasias that affect voice and require specific therapy 35. To a slightly lesser degree, individuals in a number of other occupations or avocations, such as teachers and clergy, depend on voice use. As an example, over 50 percent of teachers have dysphonia and vocal overuse is a common, but not exclusive, etiologic factor 36.
Medical conditions
Acute conditions
- Infection of the throat and/or larynx: viral, bacterial, fungal
- Foreign body in larynx, trachea, or esophagus
- Neck or laryngeal trauma
Chronic conditions
- Laryngeal cancer
- Lung cancer (or metastasis to the lung)
- Thyroid cancer
- Vocal fold nodules
- Vocal fold paralysis
- Vocal abuse
- Chemical laryngitis
- Chronic tobacco use
- Stroke
- Diabetes
- Parkinson’s disease
- Diseases from the Parkinson’s Plus family (progressive supranuclear palsy, etc)
- Myasthenia gravis
- Multiple sclerosis
- Amyotrophic lateral sclerosis (ALS)
- Testosterone deficiency
- Allergic rhinitis
- Chronic rhinitis
- Hypertension (because of certain medications used for this condition)
- Schizophrenia (because of anti-psychotics used for mental health problems)
- Osteoporosis (because of certain medications used for this condition)
- Asthma and chronic obstructive pulmonary disease (COPD) because of use of inhaled steroids
- Aneurysm of thoracic aorta (rare cause)
- Hypothyroidism and other endocrinopathies
- Sjögren syndrome
- Alcohol (moderate to heavy use or abuse)
Medications that may cause dysphonia
- Coumadin, thrombolytics, phosphodiesterase-5 inhibitors causing vocal fold hematoma 37
- Biphosphonates causing chemical laryngitis 38
- Angiotensin-converting enzyme (ACE) inhibitors causing cough 39
- Antihistamines, diuretics, anticholinergics causing drying effect on mucosa 40
- Danocrine, testosterone causing sex hormone production/utilization alteration 41
- Antipsychotics, atypical antipsychotics causing laryngeal dystonia 42
- Inhaled steroids causing dose-dependent mucosal irritation 43 and fungal laryngitis
Surgical and medical procedures
Surgery on the cervical spine via an anterior approach has been associated with a high incidence of voice problems. Recurrent laryngeal nerve paralysis has been reported to range from 1.27 percent to 2.7 percent 44. Assessment with laryngoscopy suggests an even higher incidence 45. The incidence of dysphonia immediately following anterior cervical spine surgery may be as high as 50 percent 46. Dysphonia resulting from anterior cervical spine surgery may or may not resolve over time 47.
Thyroid surgery has been associated with voice disorders. Patients with thyroid disease requiring surgery may have dysphonia and identifiable abnormalities on indirect laryngoscopy prior to surgery 48. Thyroidectomy may cause dysphonia as a result of recurrent laryngeal nerve paralysis in up to 2.1 percent of patients 49. Surgery in the anterior neck can also lead to injury to the superior laryngeal nerve with resulting voice alteration, although this is uncommon 50.
Carotid endarterectomy is frequently associated with postoperative voice problems 51 and may result in recurrent laryngeal nerve damage in up to 6 percent of patients 52.
Surgery to achieve an urgent airway or on the larynx directly may alter its structure, resulting in abnormal voice 53. Surgical procedures not involving the neck may also result in dysphonia. Dysphonia following cardiac surgery is a common problem, occurring in 17 percent to 31 percent of patients 54. Dysphonia may result from changes in position or manipulation of the endotracheal tube or from lengthy procedures 55. Recurrent laryngeal nerve injury occurs in about 1.4 percent of patients during cardiac surgery 55. The left recurrent laryngeal nerve is damaged more commonly than the right as it extends into the chest and loops under the arch of the aorta. Damage may result from direct physical injury to the nerve or hypothermic injury due to cold cardioplegia 56.
Surgery for esophageal cancer frequently results in damage to the recurrent laryngeal nerve with subsequent dysphonia. In one study, 51 of 141 patients undergoing esophagectomy for cancer had laryngeal nerve paralysis, with 30 of these patients having persistent paralysis one year following surgery 57. The implantation of vagal nerve stimulators for intractable seizures has been associated with dysphonia in as many as 28 percent of patients 58.
Prolonged endotracheal intubation has been associated with dysphonia. Direct laryngoscopy of patients intubated for more than four days (mean nine days) demonstrates that 94 percent of patients have laryngeal injury 59. The injury patterns seen in the patients with prolonged intubation include laryngeal edema and posterior and medial vocal fold ulceration. As many as 44 percent of patients with prolonged intubation may develop vocal fold granulomas within four weeks of being extubated. In this study, 18 percent of patients had prolonged true vocal fold immobility for at least four weeks after extubation 60. Another study following a large group of patients for several years found chronic phonatory dysfunction in many patients after long-term intubation 61.
Short-term intubation for general anesthesia may result in hoarseness and vocal fold pathology in over 50 percent of cases 62. While most symptoms resolved after five days, prolonged symptoms may result from vocal fold granuloma. If hoarseness persists, the remoteness of the index event may confound the evaluating clinician. Use of a laryngeal mask airway may reduce postsurgical complaints of discomfort, but does not objectively reduce hoarseness 63.
Long-term intubation of neonates may result in voice problems related to arytenoid and posterior commissure ulceration and cartilage erosion 64. Children with a history of prolonged intubation may have long-term complications of hoarseness and arytenoid dysfunction.
Dysphonia prevention
DO
- Adequately hydrate by drinking plenty of water daily.
- Use of amplification (microphone or megaphone) in large noisy spaces can help reduce shouting and voice strain.
- Rest your voice briefly to prevent voice fatigue, straining, and overuse.
- Provide indoor air humidification in dry, arid environments.
AVOID
- Smoking and second-hand smoke from cigarettes, cigars, and pipes that can irritate your airway, throat, nose, and mouth.
- Overusing or straining your voice by yelling, shouting, speaking over loud noises, and whispering.
- Excessive throat clearing and coughing.
- Alcohol (beer, wine, liquor) and caffeine beverages (coffee, soft drinks) as they can dry the throat resulting in mucous thickening.
- Use of drying medications (some antihistamines, diuretics).
- Clinical Practice Guideline: Hoarseness (Dysphonia). Otolaryngology–Head and Neck Surgery Vol 141, Issue 1_suppl, pp. 1 – 31. https://doi.org/10.1016/j.otohns.2009.06.744[↩][↩][↩]
- Galván CA, Guarderas JC. Practical Considerations for Dysphonia Caused by Inhaled Corticosteroids. Mayo Clinic Proceedings. 2012;87(9):901-904. doi:10.1016/j.mayocp.2012.06.022. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3496982/[↩]
- Roy N, Merrill RM, Gray SD, et al. Voice disorders in the general population: prevalence, risk factors, and occupational impact. Laryngoscope 2005;115:1988–95.[↩][↩][↩]
- Cohen SM, Dupont WD, Courey MS. Quality-of-life impact of non-neoplastic voice disorders: a meta-analysis. Ann Otol Rhinol Laryngol 2006;115:128–34.[↩][↩]
- Ramig L.O., Verdolini K. Treatment efficacy: voice disorders. J Speech Lang Hear Res. 1998;41(1):S101–S116.[↩]
- Roy N., Merrill R.M., Gray S.D., Smith E.M. Voice disorders in the general population: prevalence, risk factors, and occupational impact. Laryngoscope. 2005;115(11):1988–1995. https://www.ncbi.nlm.nih.gov/pubmed/16319611[↩]
- Titze I.R., Lemke J., Montequin D. Populations in the U.S. workforce who rely on voice as a primary tool of trade: a preliminary report. J Voice. 1997;11(3):254–259.[↩]
- Jones K, Sigmon J, Hock L, et al. Prevalence and risk factors for voice problems among telemarketers. Arch Otolaryngol Head Neck Surg 2002;128:571–7.[↩]
- Long J, Williford HN, Olson MS, et al. Voice problems and risk factors among aerobics instructors. J Voice 1998;12:197–207.[↩]
- Jones K., Sigmon J., Hock L., Nelson E., Sullivan M., Ogren F. Prevalence and risk factors for voice problems among telemarketers. Arch Otolaryngol Head Neck Surg. 2002;128(5):571–577.[↩]
- Speyer R, Wieneke GH, Dejonckere PH. Documentation of progress in voice therapy: perceptual, acoustic, and laryngostroboscopic findings pretherapy and posttherapy. J Voice;18: 325-40[↩]
- Martin RJ, Blager FB, Gay ML, Wood RP Paradoxic vocal cord motion in presumed asthmatics. Sem Respir Med. 1987; 8:332-337[↩]
- Stemple JC, Lee L, DAmico B, et al. Efficacy of vocal function exercises as a method of improving voice production. J Voice; 8: 270-8.[↩]
- Gould WJ, Rubin JS, & Yanagisawa E. (1995). Benign vocal fold pathology through the eyes of the laryngologist. In: JS Rubin, R Sataloff G Korovin, WJ Gould, eds. Diagnosis and Treatment of Voice Disorders. New York: Igaku-Shojin; 137-151.[↩]
- Lancer M, Syder D, Jones AS, et al.. The outcome of different management patterns for vocal cord nodules. J Laryngol and Otol; 102: 423-432.[↩]
- Smith S and Thyme K. (1976). Statistic research on changes in speech due to pedagologic treatment (the accent method). Folia Phoniatricia, 28, 98-103.[↩]
- Woo P, Casper J, Colton R, et al. Diagnosis and treatment of persistent dysphonia after laryngeal surgery: a retrospective analysis of 62 patients. Laryngoscope; 104:1084-1091.[↩]
- Anderson T, Sataloff RT. The power of voice therapy. Ear Nose Throat J;. 81:433-4. 39. Pedersen, M., Beranova, A., Moller, S. 2004.[↩]
- Heuer RJ, Sataloff RT, Emerich K, et al. Unilateral recurrent laryngeal nerve paralysis: the importance of “preoperative” voice therapy. J Voice; 11: 88-94.[↩]
- de Angelis EC, Mourao LF, Ferraz HB, Behlau MS, Pontes PA, & Andrade LA. (1997). Effect of voice rehabilitation on oral communication of Parkinson’s disease patients. Acta Neurologica Scandinavica, 96, 199-205.[↩]
- Golub JS, Chen PH, Otto KJ, et al. Prevalence of perceived dysphonia in a geriatric population. J Am Geriatr Soc 2006;54:1736–9.[↩]
- Kosztyła-Hojna B, Rogowski M, Pepin ́ski W. The evaluation of voice in elderly patients. Acta Otorhinolaryngol Belg 2003;57:107–12.[↩]
- Sewall GK, Jiang J, Ford CN. Clinical evaluation of Parkinson’s related dysphonia. Laryngoscope 2006;116:1740–4.[↩]
- Feijó AV, Parente MA, Behlau M, et al. Acoustic analysis of voice in multiple sclerosis patients. J Voice 2004;18:341–7.[↩]
- Connor NP, Cohen SB, Theis SM, et al. Attitudes of children with dysphonia. J Voice 2008;22:197–209.[↩]
- Sederholm E, McAllister A, Dalkvist J, et al. Aetiologic factors associated with hoarseness in ten-year-old children. Folia Phoniatr Logop 1995;47:262–78.[↩]
- Silverman EM. Incidence of chronic hoarseness among school-age children. J Speech Hear Disord 1975;40:211–5.[↩]
- De Bodt MS, Ketelslagers K, Peeters T, et al. Evolution of vocal fold nodules from childhood to adolescence. J Voice 2007;21:151–6.[↩]
- Hocevar-Boltezar I, Jarc A, Kozelj V. Ear, nose and voice problems in children with orofacial clefts. J Laryngol Otol 2006;120:276–81.[↩]
- Hirschberg J. Dysphonia in infants. Int J Pediatr Otorhinolaryngol 1999;49:S293–6.[↩]
- Shankargouda S, Krishnan U, Murali R, et al. Dysphonia: a frequently encountered symptom in the evaluation of infants with unobstructed supracardiac total anomalous pulmonary venous connection. Pediatr Cardiol 2000;21:458–60.[↩]
- Matsuo K, Kamimura M, Hirano M. Polypoid vocal folds. A 10-year review of 191 patients. Auris Nasus Larynx 1983;10:S37–45.[↩]
- Franchin G, Minatel E, Gobitti C, et al. Radiotherapy for patients with early-stage glottic carcinoma: univariate and multivariate analyses in a group of consecutive, unselected patients. Cancer 2003;98:765–72.[↩]
- Bernstein IL, Chervinsky P, Falliers CJ. Efficacy and safety of triamcinolone acetonide aerosol in chronic asthma. Results of a multicenter, short-term controlled and long-term open study. Chest 1982;81:20–6.[↩]
- Postma GN, Courey MS, Ossoff RH. Microvascular lesions of the true vocal fold. Ann Otol Rhinol Laryngol 1998;107:472–6.[↩]
- Preciado-López J, Pérez-Fernández C, Calzada-Uriondo M, et al. Epidemiological study of voice disorders among teaching professionals of La Rioja, Spain. J Voice 2008;22:489–508.[↩]
- Neely JL, Rosen C. Vocal fold hemorrhage associated with coumadin therapy in an opera singer. J Voice 2000;14:272–7.[↩]
- Bhutta MF, Rance M, Gillett D, et al. Alendronate-induced chemical laryngitis. J Laryngol Otol 2005;119:46–7.[↩]
- Dicpinigaitis PV. Angiotensin-converting enzyme inhibitor-induced cough: ACCP evidence-based clinical practice guidelines. Chest 2006;129:169S–73S.[↩]
- Abaza MM, Levy S, Hawkshaw MJ, et al. Effects of medications on the voice. Otolaryngol Clin North Am 2007;40:1081–90.[↩]
- Baker J. A report on alterations to the speaking and singing voices of four women following hormonal therapy with virilizing agents. J Voice 1999;13:496–507.[↩]
- Tsai CS, Lee Y, Chang YY, et al. Ziprasidone-induced tardive laryngeal dystonia: a case report. Gen Hosp Psychiatry 2008;30:277–9.[↩]
- Adams NP, Bestall JC, Lasserson TJ, Jones P, Cates CJ. Fluticasone versus placebo for chronic asthma in adults and children. Cochrane Database of Systematic Reviews 2008, Issue 4. Art. No.: CD003135. DOI: 10.1002/14651858.CD003135.pub4[↩]
- Kahraman S, Sirin S, Erdogan E, et al. Is dysphonia permanent or temporary after anterior cervical approach? Eur Spine J 2007;16:2092–5.[↩]
- Jung A, Schramm J, Lehnerdt K, et al. Recurrent laryngeal nerve palsy during anterior cervical spine surgery: a prospective study. J Neurosurg Spine 2005;2:123–7.[↩]
- Winslow CP, Winslow TJ, Wax MK. Dysphonia and dysphagia following the anterior approach to the cervical spine. Arch Otolaryngol Head Neck Surg 2001;127:51–5.[↩]
- Tervonen H, Niemelä M, Lauri ER, et al. Dysphonia and dysphagia after anterior cervical decompression. J Neurosurg Spine 2007;7: 124–30.[↩]
- Yeung P, Erskine C, Mathews P, et al. Voice changes and thyroid surgery: is pre-operative indirect laryngoscopy necessary? Aust N Z J Surg 1999;69:632–4.[↩]
- Moulton-Barrett R, Crumley R, Jalilie S, et al. Complications of thyroid surgery. Int Surg 1997;82:63–6.[↩]
- Bellantone R, Boscherini M, Lombardi CP, et al. Is the identification of the external branch of the superior laryngeal nerve mandatory in thyroid operation? Results of a prospective randomized study. Surgery 2001;130:1055–9.[↩]
- Zannetti S, Parente B, De Rango P, et al. Role of surgical techniques and operative findings in cranial and cervical nerve injuries during carotid endarterectomy. Eur J Vasc Endovasc Surg 1998;15:528–31.[↩]
- Espinoza FI, MacGregor FB, Doughty JC, et al. Vocal fold paralysis following carotid endarterectomy. J Laryngol Otol 1999;113:439–41.[↩]
- Schindler A, Favero E, Nudo S, et al. Voice after supracricoid laryngectomy: subjective, objective and self-assessment data. Logoped Phoniatr Vocol 2005;30:114–9.[↩]
- Kamalipour H, Mowla A, Saadi MH, et al. Determination of the incidence and severity of hoarseness after cardiac surgery. Med Sci Monit 2006;12:CR206–9.[↩]
- Inada T, Fujise K, Shingu K. Hoarseness after cardiac surgery. J Cardiovasc Surg (Torino) 1998;39:455–9.[↩][↩]
- Hamdan AL, Moukarbel RV, Farhat F, et al. Vocal cord paralysis after open-heart surgery. Eur J Cardiothorac Surg 2002;21:671–4.[↩]
- Baba M, Natsugoe S, Shimada M, et al. Does hoarseness of voice from recurrent nerve paralysis after esophagectomy for carcinoma influence patient quality of life? J Am Coll Surg 1999;188:231–6.[↩]
- Morris GL III, Mueller WM. Long-term treatment with vagus nerve stimulation in patients with refractory epilepsy. The Vagus Nerve Stimulation Study Group E01-E05. Neurology 1999;53:1731–5[↩]
- Colice GL, Stukel TA, Dain B. Laryngeal complications of prolonged intubation. Chest 1989;96:877–84.[↩]
- Santos PM, Afrassiabi A, Weymuller EA Jr. Risk factors associated with prolonged intubation and laryngeal injury. Otolaryngol Head Neck Surg 1994;111:453–9.[↩]
- Bastian RW, Richardson BE. Postintubation phonatory insufficiency: an elusive diagnosis. Otolaryngol Head Neck Surg 2001;124:625–33.[↩]
- Jones MW, Catling S, Evans E, et al. Hoarseness after tracheal intubation. Anaesthesia 1992;47:213–6.[↩]
- Zimmert M, Zwirner P, Kruse E, et al. Effects on vocal function and incidence of laryngeal disorder when using a laryngeal mask airway in comparison with an endotracheal tube. Eur J Anaesthesiol 1999; 16:511–5.[↩]
- Hengerer AS, Strome M, Jaffe BF. Injuries to the neonatal larynx from long-term endotracheal tube intubation and suggested tube modification for prevention. Ann Otol Rhinol Laryngol 1975;84:764–70.[↩]




{kind=link}