Contents
What is hepatorenal syndrome
Hepatorenal syndrome is a condition in which there is progressive kidney failure that occurs in individuals with end-stage liver disease (advanced chronic liver disease), occurring mainly in patients with advanced cirrhosis and ascites, who have marked circulatory dysfunction 1. Hepatorenal syndrome occurs in a person with cirrhosis of the liver. As many as 40% of individuals with cirrhosis and ascites will develop hepatorenal syndrome 2. Hepatorenal syndrome is a serious complication that can lead to death.
Hepatorenal syndrome symptoms may include fatigue, abdominal pain, and a general feeling of ill health (malaise). There are two distinct types of hepatorenal syndrome 3:
- Type I hepatorenal syndrome progresses quickly (within days) with doubling of serum creatinine in < 2 week, leading to kidney failure. Type I hepatorenal syndrome is characterized by acute onset and rapidly progressing kidney failure with a doubling of serum creatinine to > 2.5 mg/dL (corresponding to a 50% reduction in the creatinine clearance rate) in less than 2 week, usually associated with multiorgan damage. Individuals with type I typically have dramatically reduced urine output, edema, and jaundice, and often suffer from hepatic encephalopathy. No history of diuretic resistant ascites. The prognosis is poor with only 10% of patients surviving longer than 90 days 4. Type I hepatorenal syndrome can develop spontaneously but more often tends to follow a precipitating event, mostly spontaneous bacterial peritonitis or other infections like pneumonia, urinary tract infections or cellulitis 5. Other potential risk factors include viral, alcoholic, toxic or ischemic hepatitis (e.g., TIPS), gastrointestinal bleeding and surgical procedures.
- Type II hepatorenal syndrome progresses more slowly, over weeks or months, and the symptoms are less severe. Type II hepatorenal syndrome represents the final kidney response to hemodynamic impairments in cirrhosis. The increase in creatinine is gradual with mean values of 1.5-2.0 mg/dL. Type II hepatorenal syndrome predisposes patients to the development of type I hepatorenal syndrome after a precipitating event. The average survival rate is six to eight months after onset. Always ascites diuretic resistance.
According to Fede et al 6, approximately 20% of cirrhotic patients with diuretic-resistant ascites potentially develop hepatorenal syndrome, while a prospective study by Ginès et al 7 on 229 patients with cirrhosis found an 18% incidence of hepatorenal syndrome at one year, rising to 39% at five years after initial diagnosis.
Hepatorenal syndrome may also arise in patients with acute liver failure as shown in Akriviadis et al 8: They considered 101 patients with alcoholic hepatitis of whom 28 developed hepatorenal syndrome after a four-week follow-up. Planas et al 9, in a study enrolling 263 cirrhotic patients with a follow-up of 41 ± 3 months after the onset of ascites, found prevalence rates of 2.6% and 5% for hepatorenal syndrome types I and II respectively, with a cumulative probability of 11.4% at five years. The prevalence of hepatorenal syndrome increases with liver disease progression, Wong et al 10 reporting a rate of 48% in patients on the waiting list for liver transplant.
Despite discrepancies in literature data, the prevalence of hepatorenal syndrome has dropped in recent years, probably as a result of a better understanding of its pathophysiology and improved clinical management[19]. Nonetheless the long-term survival of hepatorenal syndrome patients remains poor and the only effective treatment for this condition is liver transplantation.
The cause of hepatorenal syndrome is unknown. A contributing factor seems to be a narrowing of the blood vessels that connect into the kidneys. This causes a decrease in blood flow to the kidneys, impairing their function. In some cases, triggers or precipitating factors (infections, blood loss from the gastrointestinal tract, low blood pressure) are involved. Treatment is aimed at helping the liver work better and maintaining kidney function. In many cases, a liver transplant is needed. In some cases, individuals also need a kidney transplant.
The goal of treatment is to help the liver work better and to make sure the heart is able to pump enough blood to the body.
Treatment is about the same as for kidney failure from any cause. It includes:
- Stopping all unnecessary medicines, especially ibuprofen and other NSAIDs, certain antibiotics, and diuretics (“water pills”)
- Having dialysis to improve symptoms
- Taking medicines to improve blood pressure and help your kidneys work better; infusion of albumin may also be helpful
- Placing a shunt (known as TIPS) to relieve the symptoms of ascites (this may also help kidney function, but the procedure can be risky)
- Surgery to place a shunt from the abdominal space to the jugular vein to relieve some symptoms of kidney failure (this procedure is risky and is rarely done)
Hepatorenal syndrome possible complications
Complications of hepatorenal syndrome may include:
- Bleeding
- Damage to, and failure of, many organ systems
- End-stage kidney disease
- Fluid overload and heart failure
- Coma caused by liver failure
- Secondary infections
Progressive liver failure, as manifested by worsening encephalopathy, jaundice, and coagulopathy, is a preterminal condition if liver transplantation is not performed.
Hepatorenal syndrome prognosis
The outcome is often poor. Death often occurs due to an infection or severe bleeding (hemorrhage). Renal failure increases mortality 7-fold, with 50% of patients dying within one month 11.
Hepatorenal syndrome life expectancy
Type 1 hepatorenal syndrome has a median survival of 2 weeks, with few patients surviving more than 10 weeks 12. Type 2 hepatorenal syndrome has a median survival of 3-6 months.
Hepatorenal syndrome symptoms
Symptoms include:
- Abdominal swelling due to fluid (called ascites, a symptom of liver disease)
- Mental confusion
- Muscle jerks
- Dark-colored urine (a symptom of liver disease)
- Decreased urine output
- Nausea and vomiting
- Weight gain
- Yellow skin (jaundice, a symptom of liver disease)
Individuals with hepatorenal syndrome will have a variety of nonspecific symptoms including fatigue, abdominal pain, and a general feeling of ill health (malaise). Affected individuals also have symptoms related to advanced liver disease including the accumulation of fluid in the abdomen (ascites), yellowing of the skin and the whites of the eyes (jaundice), an enlarged spleen (splenomegaly) and an enlarged, extremely tender liver (hepatomegaly).
Hepatorenal syndrome type I is characterized by a rapid decrease in kidney function. The kidneys act as a filtration system removing unwanted substances and excess fluid from the body. Symptoms of decreasing renal function include the accumulation of excess watery fluid in the spaces between the tissues and organs causing swelling of these areas (edema), dramatically decreased urination, and the presence of increased nitrogenous waste products such as creatinine and BUN in the blood (azotemia). Hepatorenal syndrome type I can progress to life-threatening renal failure within days.
Individuals with hepatorenal syndrome type I are more likely to suffer from hepatic encephalopathy, a condition that occurs when the liver fails to breakdown (metabolize) certain substances in the body. These substances travel through the bloodstream to the brain with toxic effects. Hepatic encephalopathy may cause confusion, drowsiness, recognizable changes in judgment and other intellectual processes, and other psychological alterations. It also is more likely to occur with acute liver failure due to any cause.
Hepatorenal syndrome type II causes renal dysfunction that generally progresses much slower than it does in type I. Affected individuals are less likely to develop jaundice and usually do not develop hepatic encephalopathy. Individuals with hepatorenal syndrome type II often develop accumulation of fluid in the abdomen (ascites) does not respond to treatment with diuretics, which are drugs that help remove excess fluid from the body. This finding is referred to as diuretic-resistant ascites. It can occur over weeks to months with a slow rise of BUN and Creatinine.
Hepatorenal syndrome causes
Hepatorenal syndrome occurs when the kidneys stop working well in people with serious liver problems. Less urine is removed from the body, so waste products that contain nitrogen build up in the bloodstream (azotemia).
The disorder occurs in up to 1 in 10 people who are in the hospital with liver failure. It leads to kidney failure in people with:
- Acute liver failure
- Alcoholic hepatitis
- Cirrhosis
- Infected abdominal fluid
Risk factors include:
- Blood pressure that falls when a person rises or suddenly changes position (orthostatic hypotension)
- Use of medicines called diuretics (“water pills”)
- Gastrointestinal bleeding
- Infection
- Recent abdominal fluid tap (paracentesis)
- Spontaneous bacterial peritonitis
- Large volume paracentesis (> 5 L) with inadequate albumin substitution
- NSAID and other nephrotoxic drugs, iv contrast
- Bleeding from esophageal varices
- Post transjugular intrahepatic portosystemic shunt syndrome
Hepatorenal syndrome pathogenesis
Hepatorenal syndrome can be considered the final stage of a pathophysiological condition characterized by decreased renal blood flow resulting from deteriorating liver function in patients with cirrhosis and ascites 13.
Hemodynamic changes associated with endothelial shear stress occur before the onset of ascites and are sustained by an increase in pro-angiogenic factors like the vascular endothelial growth factor and platelet-derived growth factor and vasodilators (carbon monoxide, endocannabinoids and nitric oxide) able to promote the formation of hepatic, splanchnic and portosystemic collateral vessels (Figure 1) 14.
The ensuing hemodynamic instability may give rise to many clinical events that further interfere with the compensatory mechanisms. These include the onset of spontaneous bacterial peritonitis, gastrointestinal bleeding and post-paracentesis circulatory dysfunction 15.
The renal impairment is worsened by a progressive cardiac dysfunction known as cirrhotic cardiomyopathy. The latter is characterized by diastolic impairment with septal ventricular hypertrophy, blunted ventricular response to stress, systolic and diastolic dysfunction, and electrophysiological abnormalities (prolongation of QT interval) 14. Systolic dysfunction is due to impairment of both β-adrenergic receptor and increasing in endogenous cannabinoids and cardiosuppressants such as nitric oxide and inflammatory cytokines and myocyte apoptosis. Furthermore it is possible that several intracellular signaling pathways are involved.
On the other hand the activation of renin-angiotensin system and salt retention play a role in diastolic disfunction. Recent studies have stated myocardial dysfunction in cirrhosis as a contributing, or even a precipitant factor, of hepatorenal syndrome 16.
Figure 1. Hepatorenal syndrome pathogenesis
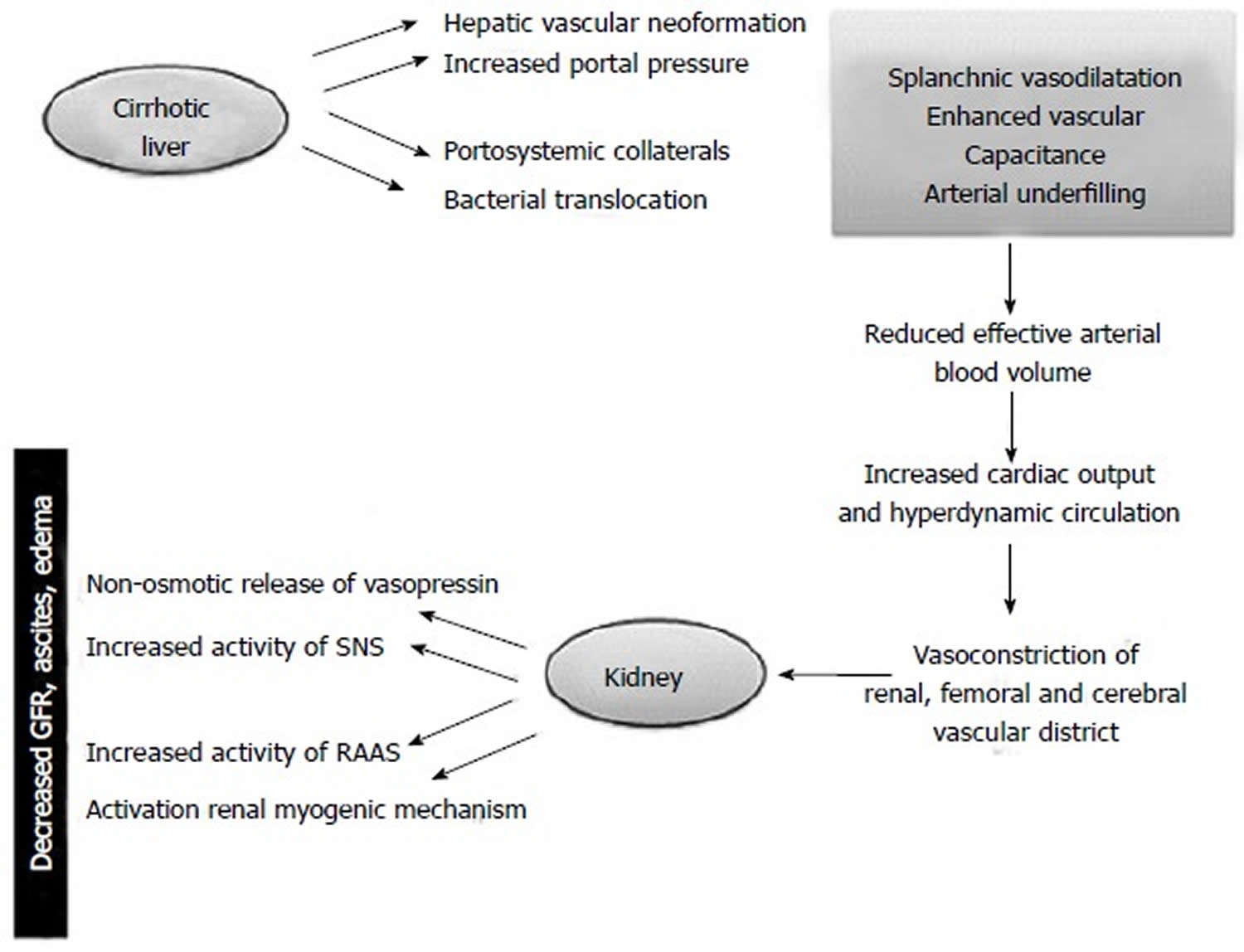
Footnote: In cirrhotic patients portal hypertension can lead to markedly dilated splanchnic arterial vessels. The bacterial translocation of intestinal germs, the gradual decrease in systemic vascular resistances, the hepatic vascular neoformation are potential risk factors. The fall in mean arterial pressure is compensated by increase in cardiac output and by activation of renin-angiotensin-aldosterone system (RAAS) and sympathetic nervous system (SNS) to improve systemic vascular resistence. The response mechanisms to the decreased effective circulating volume caused by Enhanced vascular capacitance (so-called “arterial underfilling”) include the non-osmotic release of vasopressin accounting for renal tubular sodium resorption and water retention leading to the onset of ascites, edema and hypervolemic hyponatremia. These compensatory mechanisms ultimately have repercussions on kidney function causing reduced glomerular filtration rate (GFR) and further water retention thereby worsening the water overload.
[Source 17]Hepatorenal syndrome prevention
Prevention of hepatorenal syndrome is important since it develops with a constant frequency in cases of spontaneous bacterial peritonitis and alcoholic hepatitis 18. It is possible to prevent hepatorenal syndrome if spontaneous bacterial peritonitis is urgently diagnosed and treated. Albumin infusion may help to prevent hepatorenal syndrome when spontaneous bacterial peritonitis develops. Albumin infusion is started together with antibiotics with an initial dose of 1.5 g/kg at the time of diagnosis of infection and albumin infusion is repeated after 48 hours with a dose of 1 g/kg 19. The incidence of renal dysfunction is decreased when compared to patients who are not treated with albumin (8% vs 31%) and mortality is also decreased (16% vs 35%) 20. Norfloxacin is recommended in selected patients with cirrhosis and ascites. 400 mg/day dose of oral norfloxacin in a one year time period was found to decrease spontaneous bacterial peritonitis development (7% vs 61%), decrease hepatorenal syndrome development (28% vs 41%) and improve survival at three months (94% vs 62%) and one year (60% vs 48%) 20. In a study investigating whether pentoxifylline is beneficial or not, significant benefit with 1200 mg/day pentoxifylline was observed when compared with placebo 21, but a meta-analysis revealed that pentoxifylline has no benefit in hepatorenal syndrome 22.
Hepatorenal syndrome diagnosis
As there are currently no specific tests to identify hepatorenal syndrome, diagnosis rests on the exclusion of other causes of kidney failure 17. It is important to establish the cause of acute kidney injury in order to institute the appropriate treatment.
- Hepatorenal syndrome is diagnosed after testing to rule out other causes of kidney failure.
A physical exam does not detect kidney failure directly. However, the exam will very often show signs of chronic liver disease, such as:
- Confusion (often due to hepatic encephalopathy)
- Excess fluid in the abdomen (ascites)
- Jaundice
- Other signs of liver failure
Other signs include:
- Abnormal reflexes
- Smaller testicles
- Dull sound in the belly area when tapped with the tips of the fingers
- Increased breast tissue (gynecomastia)
- Sores (lesions) on the skin
The following may be signs of kidney failure:
- Very little or no urine output
- Fluid retention in the abdomen or extremities
- Increased blood urea nitrogen (BUN) and creatinine blood levels
- Increased urine specific gravity and osmolality
- Low blood sodium
- Very low urine sodium concentration
The following may be signs of liver failure:
- Abnormal prothrombin time (PT)
- Increased blood ammonia level
- Low blood albumin
- Paracentesis shows ascites
- Signs of hepatic encephalopathy (an EEG may be done)
Table 1. Diagnostic criteria for hepatorenal syndrome
| Cirrhosis with ascites |
| Serum Creatinine > 1.5 mg/dL |
| Absence of shock |
| No improvement of serum creatinine (decrease to a level of 1.5 mg/dL or less) after at least 2 d of diuretic withdraw and volume expansion with albumin (The recommended dose of albumin is 1 g/kg of body weight per day up to a maximum of 100 g/d) |
| No current o recent exposure to nephrotoxic drugs |
| Absence of parenchymal disease as indicated by proteinuria > 500 mg/d, microscopic hematuria (50 red blood cells per high power field) and abnormal renal ultrasonography |
Hepatorenal syndrome treatment
Despite improvements in the clinical management of hepatorenal syndrome patients in the past twenty years, currently available treatments enhance patients’ short-term survival but offer little benefit in the longer term.
The main principle in the treatment of hepatorenal syndrome is to bring back renal function until the patients undergo liver transplantation.
Treatment is about the same as for kidney failure from any cause. It includes:
- Stopping all unnecessary medicines, especially ibuprofen and other NSAIDs, certain antibiotics, and diuretics (“water pills”)
- Having dialysis to improve symptoms
- Taking medicines to improve blood pressure and help your kidneys work better; infusion of albumin may also be helpful
- Placing a shunt (known as transjugular intrahepatic portosystemic shunt or TIPS) to relieve the symptoms of ascites (this may also help kidney function, but the procedure can be risky)
- Surgery to place a shunt from the abdominal space to the jugular vein to relieve some symptoms of kidney failure (this procedure is risky and is rarely done). Major complications associated with TIPS (transjugular intrahepatic portosystemic shunt) are hepatic encephalopathy which is a common and treatable condition, worsening of hepatic function, bleeding due to the procedure and acute kidney injury because of intravenous contrast injection during the procedure 24.
The only curative therapy for individuals with hepatorenal syndrome is a liver transplant, which corrects both the liver disease and associated impaired renal function. Even after successful liver transplantation, patients who had hepatorenal syndrome beforehand may not fully recover their kidney function. A small percentage may go on to permanent damage requiring dialysis. Much research is ongoing to determine which patients will recover and which may not. Those who may not recover may need a kidney transplant with their liver transplant. However, due to a limited amount of donors and long waiting lists, a liver transplant is not always feasible. For patients who develop hepatorenal syndrome with acute liver failure and not cirrhosis, recovery from hepatorenal syndrome can occur if the liver recovers. However, individuals with hepatorenal syndrome requiring dialysis or suffering from advanced kidney failure for 6-8 weeks before receiving a liver transplant, may require a kidney transplant with their liver transplant, as kidney function may not recover.
A recent literature review by Fabrizi et al 25 noted that pre-transplant kidney function is the most important predictor for patient survival after liver transplant. Pharmacological treatment and medical care serve as a “bridge” to transplant to improve the patient’s prognosis.
Individuals with liver disease and the hepatorenal syndrome who receive a liver transplant have a lower success rate than in individuals with liver disease and normal kidney function who receive a liver transplant. Three year survival after liver transplantation in patients with hepatorenal syndrome is 60%, while it is 70%-80% if it is performed before hepatorenal syndrome has developed 26. Therefore, many of the therapies used to treat hepatorenal syndrome are done to improve kidney function in individuals eligible for a liver transplant.
For individuals awaiting a transplant, several therapies to maintain kidney function may be used. Paracentesis is a surgical procedure that removes the excess fluid from the abdomen (ascites). Under carefully controlled conditions, this procedure may benefit some affected individuals. In addition, avoiding diuretics (which can worsen kidney function), maintaining electrolyte balance, and promptly treating infection may also be necessary.
- Mindikoglu AL, Weir MR. Current concepts in the diagnosis and classification of renal dysfunction in cirrhosis. Am J Nephrol. 2013;38:345–354.[↩]
- Hepatorenal Syndrome. https://emedicine.medscape.com/article/178208-overview[↩]
- Ascites and hepatorenal syndrome in cirrhosis: pathophysiological basis of therapy and current management. Arroyo V, Colmenero J. J Hepatol. 2003; 38 Suppl 1():S69-89. https://www.ncbi.nlm.nih.gov/pubmed/12591187/[↩]
- Hepatorenal syndrome. Ginès P, Guevara M, Arroyo V, Rodés J. Lancet. 2003 Nov 29; 362(9398):1819-27. https://www.ncbi.nlm.nih.gov/pubmed/14654322/[↩]
- Renal failure and bacterial infections in patients with cirrhosis: epidemiology and clinical features. Fasolato S, Angeli P, Dallagnese L, Maresio G, Zola E, Mazza E, Salinas F, Donà S, Fagiuoli S, Sticca A, Zanus G, Cillo U, Frasson I, Destro C, Gatta A. Hepatology. 2007 Jan; 45(1):223-9.[↩]
- Fede G, D’Amico G, Arvaniti V, Tsochatzis E, Germani G, Georgiadis D, Morabito A, Burroughs AK. Renal failure and cirrhosis: a systematic review of mortality and prognosis. J Hepatol. 2012;56:810–818[↩]
- Ginès P, Guevara M, Arroyo V, Rodés J. Hepatorenal syndrome. Lancet. 2003;362:1819–1827.[↩]
- Akriviadis E, Botla R, Briggs W, Han S, Reynolds T, Shakil O. Pentoxifylline improves short-term survival in severe acute alcoholic hepatitis: a double-blind, placebo-controlled trial. Gastroenterology. 2000;119:1637–1648.[↩]
- Planas R, Montoliu S, Ballesté B, Rivera M, Miquel M, Masnou H, Galeras JA, Giménez MD, Santos J, Cirera I, et al. Natural history of patients hospitalized for management of cirrhotic ascites. Clin Gastroenterol Hepatol. 2006;4:1385–1394.[↩]
- Wong LP, Blackley MP, Andreoni KA, Chin H, Falk RJ, Klemmer PJ. Survival of liver transplant candidates with acute renal failure receiving renal replacement therapy. Kidney Int. 2005;68:362–370.[↩]
- Renal failure and cirrhosis: A systematic review of mortality and prognosis. Fede, Giuseppe et al. Journal of Hepatology , Volume 56 , Issue 4 , 810 – 818 https://doi.org/10.1016/j.jhep.2011.10.016[↩]
- Appenrodt B, Zielinski J, Brensing KA, Heller J, Sauerbruch T, Schepke M. Degree of hepatic dysfunction and improvement of renal function predict survival in patients with HRS type I: a retrospective analysis. Eur J Gastroenterol Hepatol. 2009 Dec. 21(12):1428-32.[↩]
- Liangpunsakul S, Agarwal R. Renal failure in cirrhosis: is it time to change the diagnosis and classification? Am J Nephrol. 2013;38:342–344.[↩]
- Wadei HM. Hepatorenal syndrome: a critical update. Semin Respir Crit Care Med. 2012;33:55–69.[↩][↩]
- Fagundes C, Ginès P. Hepatorenal syndrome: a severe, but treatable, cause of kidney failure in cirrhosis. Am J Kidney Dis. 2012;59:874–885.[↩]
- Mocarzel L, Lanzieri P, Nascimento J, Peixoto C, Ribeiro M, Mesquita E. Hepatorenal syndrome with cirrhotic cardiomyopathy: case report and literature review. Case Reports Hepatol. 2015;2015:573513.[↩]
- Baraldi O, Valentini C, Donati G, et al. Hepatorenal syndrome: Update on diagnosis and treatment. World Journal of Nephrology. 2015;4(5):511-520. doi:10.5527/wjn.v4.i5.511. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4635371/[↩][↩]
- Dundar HZ, Yılmazlar T. Management of hepatorenal syndrome. World Journal of Nephrology. 2015;4(2):277-286. doi:10.5527/wjn.v4.i2.277. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4419138/[↩]
- Arroyo V, Fernández J. Management of hepatorenal syndrome in patients with cirrhosis. Nat Rev Nephrol. 2011;7:517–526.[↩]
- Salerno F, Navickis RJ, Wilkes MM. Albumin infusion improves outcomes of patients with spontaneous bacterial peritonitis: a meta-analysis of randomized trials. Clin Gastroenterol Hepatol. 2013;11:123–130.e1[↩][↩]
- Tyagi P, Sharma P, Sharma BC, Puri AS, Kumar A, Sarin SK. Prevention of hepatorenal syndrome in patients with cirrhosis and ascites: a pilot randomized control trial between pentoxifylline and placebo. Eur J Gastroenterol Hepatol. 2011;23:210–217[↩]
- Whitfield K, Rambaldi A, Wetterslev J, Gluud C. Pentoxifylline for alcoholic hepatitis. Cochrane Database Syst Rev. 2009;4:CD007339[↩]
- Baraldi O, Valentini C, Donati G, et al. Hepatorenal syndrome: Update on diagnosis and treatment. World Journal of Nephrology. 2015;4(5):511-520. doi:10.5527/wjn.v4.i5.511. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4635371[↩]
- TIPS for the treatment of refractory ascites, hepatorenal syndrome and hepatic hydrothorax: a critical update. Rössle M, Gerbes AL. Gut. 2010 Jul; 59(7):988-1000.[↩]
- Fabrizi F, Aghemo A, Messa P. Hepatorenal syndrome and novel advances in its management. Kidney Blood Press Res. 2013;37:588–601[↩]
- Continued influence of preoperative renal function on outcome of orthotopic liver transplant (OLTX) in the US: where will MELD lead us? Gonwa TA, McBride MA, Anderson K, Mai ML, Wadei H, Ahsan N. Am J Transplant. 2006 Nov; 6(11):2651-9.[↩]





{kind=link}