
Contents
- What is the kidney transplant process
- Considering a kidney transplant
- How does the evaluation process work?
- How long does a kidney transplant take?
- How long does a kidney transplant last?
- How much is a kidney transplant?
- Who can get a kidney transplant?
- What if I’m older or have other health problems?
- What is kidney transplant success rate?
- What should I eat or avoid eating with a kidney transplant?
- When was the first kidney transplant done?
- What is a “preemptive” or “early” transplant?
- Where do donated kidneys come from?
- Is it better to get a kidney from a living donor?
- Are there disadvantages to living donation?
- If I am a woman of child bearing age, can I become pregnant after kidney transplant?
- What are the financial costs to the living donor?
- What is Medicare?
- How can a person get Medicare for kidney failure?
- What health plans does Medicare offer?
- Where can a person enroll in Medicare?
- When does Medicare start for people with end-stage renal disease?
- When does Medicare end for people with end-stage renal disease?
- How does Medicare pay if a person has other health insurance?
- When does an employer or union group plan start to pay?
- What other federal programs can help?
- What state programs can help?
- What programs can help special populations?
- What private organizations can help?
- Kidney transplant surgery
- Kidney transplant procedure
- Kidney transplant recovery
- Kidney transplant survival rate
- Kidney transplant complications
- What are anti-rejection medications?
- Life after a kidney transplant
What is the kidney transplant process
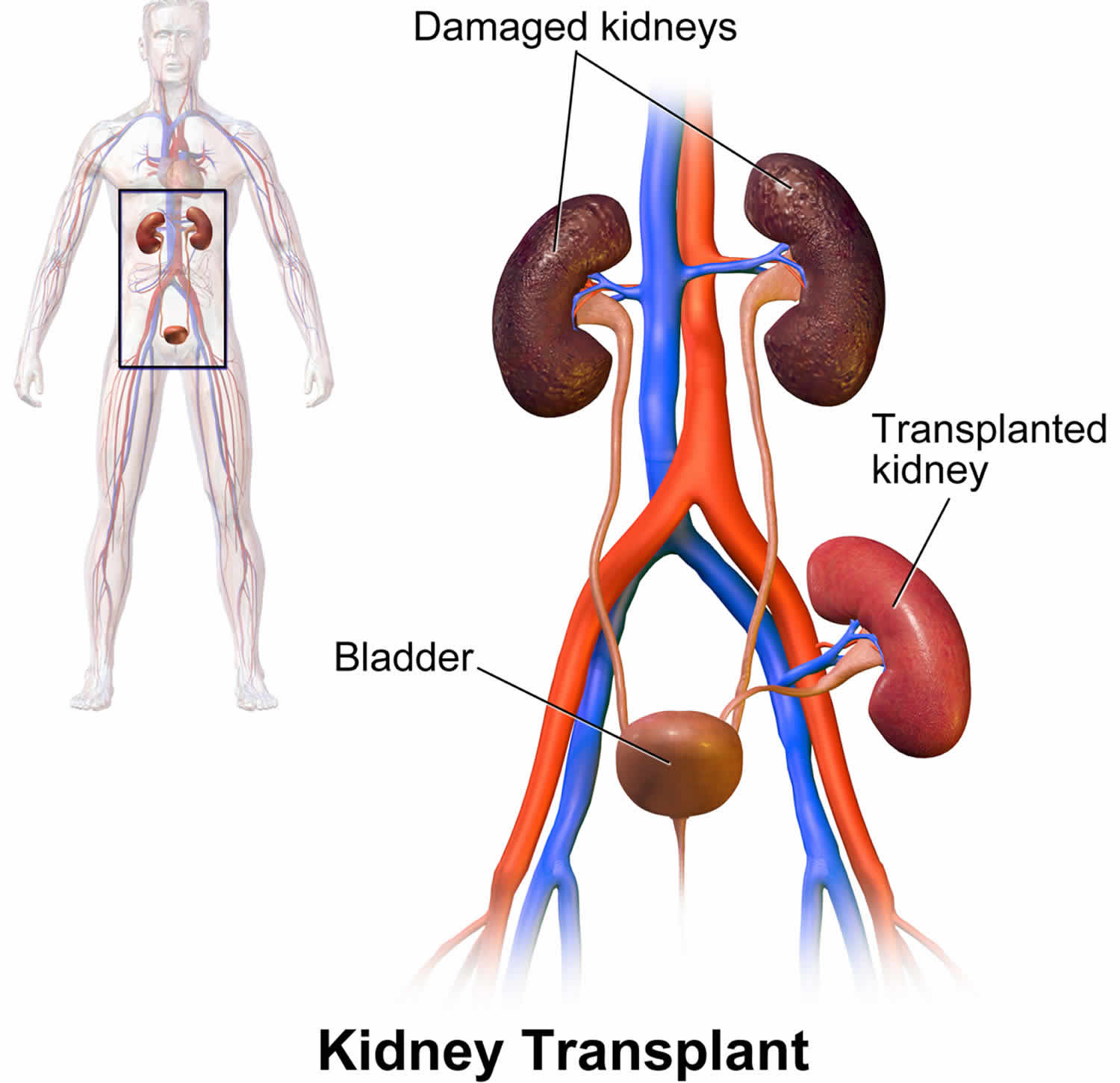
A kidney transplant is an operation to place a healthy donor kidney in a person whose two kidneys are no longer working properly. A kidney transplant is considered a long-term alternative to kidney dialysis. During a kidney transplant surgery, a healthy kidney from a donor is placed into your body. The new, donated kidney does the work that your two kidneys used to do. Many people feel that a kidney transplant offers more freedom and a better quality of life than kidney dialysis. In making a decision about whether kidney transplant is the best treatment for you, you may find it helpful to talk to people who already have a kidney transplant here (https://www.kidney.org/patients/peers). You also need to speak to your doctor, nurse and family members.
The donated kidney can come from someone you don’t know who has recently died (deceased donor), or from a living person—a relative, spouse, or friend. Due to the shortage of kidneys, patients on the waiting list for a deceased donor kidney may wait many years.
A kidney transplant is a treatment for kidney failure; a kidney transplant is not a cure. You will need to take medicines every day to make sure your immune system doesn’t reject the new kidney. You will also need to see your health care provider regularly.
A working transplanted kidney does a better job of filtering wastes and keeping you healthy than dialysis. However, a kidney transplant isn’t for everyone. Your doctor may tell you that you’re not healthy enough for transplant surgery.
On the plus side, there are fewer limits on what you can eat and drink, but you should follow a heart-healthy diet. Your health and energy should improve. In fact, a successful kidney transplant may allow you to live the kind of life you were living before you got kidney disease. Studies show that people with kidney transplants live longer than those who remain on dialysis.
On the minus side, there are the risks of surgery. You will also need to take anti-rejection medicines for as long as your new kidney is working, which can have side effects. You will have a higher risk for infections and certain types of cancer.
If you want a kidney transplant, the kidney transplant process includes these steps:
- Tell your doctor or nurse you want to have a kidney transplant.
- Your doctor will refer you to a transplant center for tests to see if you’re healthy enough to receive a kidney transplant. Living donors need to be tested to make sure they’re healthy enough to donate a kidney.
- If you don’t have a living donor, you’ll be placed on a waiting list to receive a kidney. You’ll have monthly blood tests while you wait for a kidney.
- You must go to the hospital to have your transplant as soon as you learn a kidney is available. If you have a living donor, you can schedule the transplant in advance.
Considering a kidney transplant
If you have serious (end-stage) kidney failure, a kidney transplant may be an option. A kidney transplant may offer you both a longer, dialysis-free life, and a better quality of life. Your healthcare team will assess whether you are medically suitable for a kidney transplant.
To decide whether you want a kidney transplant, it is important to understand your condition and the potential benefits and risks of the kidney transplant procedure. You also need to be willing to undertake the self-care that will be required – for the rest of your life – after the operation.
Talk with your doctor
The first step is to talk with your doctor to find out whether you’re a candidate for a transplant. If you’re on dialysis, your dialysis team will also be part of the process. If you and your doctor think a kidney transplant is right for you, your doctor will refer you to a transplant center.
Who is on my kidney transplant team?
A successful transplant involves working closely with your transplant team. Members of the team include:
- You—you are an important part of your transplant team.
- Your family members—this may include your spouse, parents, children or any other family member you would like to involve.
- Transplant surgeon—the doctor who places the kidney in your body.
- Nephrologist—a doctor who specializes in kidney health and may work closely with a nurse practitioner or a physician’s assistant.
- Transplant coordinator—a specially trained nurse who will be your point of contact, arrange your appointments, and teach you what to do before and after the transplant.
- Pharmacist—a person who tells you about all your medicines, fills your prescriptions, and helps you avoid unsafe medicine combinations and side effects.
- Social worker—a person trained to help you solve problems in your daily life and coordinate care needs after your transplant.
- Dietitian—an expert in food and nutrition who teaches you about the foods you should eat and avoid, and how to plan healthy meals.
Your kidney transplant team will be able to provide the support and encouragement you need throughout the transplant process.
How does the evaluation process work?
Medical professionals will give you a complete physical exam, review your health records, and order a series of tests and X-rays to learn about your overall health. Everything that can affect how well you can handle treatment will be checked. The evaluation process for a transplant is very thorough. Your healthcare team will need to know a lot about you to help them—and you—decide if a transplant is right for you. One thing you can do to speed the process is to get all the testing done as quickly as possible and stay in close contact with the transplant team. If you’re told you might not be right for a transplant, don’t be afraid to ask why—or if you might be eligible at some future time or at another center. Remember, being active in your own care is one of the best ways to stay healthy.
If someone you know would like to donate a kidney to you, that person will also need to go through a screening to find out if he or she is a match and healthy enough to donate.
If it’s your child who has kidney disease, you’ll want to give serious thought to getting a transplant evaluation for him or her. Because transplantation allows children and young adults to develop in as normal a way as possible in their formative years, it can be the best treatment for them.
If the evaluation process shows that a transplant is right for you or your child, the next step is getting a suitable kidney.
How to Find a Transplant Center
To find a transplant center in your area visit the Organ Procurement and Transplantation Network (OPTN) website (https://optn.transplant.hrsa.gov/members/member-directory/). Then follow these steps:
- Select “Transplant Centers by Organ” under Member Type
- Select “Kidney” for Organ Type
- Select your state or region
When you’re considering transplant centers, you may want to:
- Learn about the number and type of transplants the center performs each year
- Ask about the transplant center’s kidney transplant survival rates
- Compare transplant center statistics through the database maintained by the Scientific Registry of Transplant Recipients
- Find out if the center offers paired donation or donation chain programs that might increase your chances of receiving a living-donor kidney
- Understand the costs that will be incurred before, during and after your transplant. Costs will include tests, organ procurement, surgery, hospital stays, and transportation to and from the center for the procedure and follow-up appointments
- Consider additional services provided by the transplant center, such as coordinating support groups, assisting with travel arrangements, helping with local housing for your recovery period and offering referrals to other resources
- Assess the center’s commitment to keeping up with the latest transplant technology and techniques, which indicates that the program is growing
Get tested at a kidney transplant center
At the transplant center, you’ll meet members of your transplant team. You’ll have tests to make sure you’re a good candidate for transplant.
Tests will include blood tests and tests to check your heart and other organs—to make sure you’re healthy enough for surgery. Some conditions or illnesses could make a transplant less likely to succeed, such as cancer that is not in remission, or current substance abuse.
You’ll also have tests to check your mental and emotional health. The transplant team must be sure you’re prepared to care for a transplanted kidney. You’ll need to be able to understand and follow a schedule for taking the medicines you need after surgery.
In a process called cross-matching, the transplant team tests the donor’s blood against your blood to help predict whether your body’s immune system will accept or reject the new kidney.
If a family member or friend wants to donate a kidney and is a good match, that person will need a health exam to make sure he or she is healthy enough to be a donor. If you have a living donor, you don’t need to be on a waiting list for a kidney and can schedule the surgery when it’s best for you, your donor, and your surgeon.
Testing and evaluation at the transplant center may take several visits over weeks to months.
Get on the waiting list
If your tests show you can have a transplant, your transplant center will add your name to the waiting list. Wait times can range from a few months to years. Most transplant centers give preference to people who‘ve been on the waiting list the longest. Other factors, such as your age, where you live, and your blood type, may make your wait longer or shorter.
A transplant center can place you on the waiting list for a donor kidney if your kidney function is 20 or less—even if you aren’t on dialysis. While you wait for a kidney transplant, you may need to start dialysis.
Have monthly blood tests
While you wait for a kidney, you’ll need monthly blood tests. The center must have a recent sample of your blood to match with any kidney that becomes available.
How long does a kidney transplant take?
A kidney transplant surgery usually takes 3 or 4 hours.
How long does a kidney transplant last?
Although most transplants are successful and last for many years, how long they last can vary from one person to the next. Many people will need more than one kidney transplant during a lifetime.
How much is a kidney transplant?
Medicare, the Federal Government health insurance program, will pay for kidney transplant and care for 3 years after the transplant. Medicare will also pay for your donor’s surgery and his or her care.
The average cost to Medicare per person in 2011 1 was almost $33,000 for a kidney transplant. In comparison to almost $88,000 for hemodialysis and more than $71,000 for peritoneal dialysis 1.
Medicare and private insurance may help pay for your medicines too. Additionally, drug companies give discounts to people who can show that they can’t afford to pay for their prescriptions. Talk with your transplant social worker to find out what resources may be available to help you pay for your transplant.
Financial help is available from the Federal Government and other sources. In 1972, the U.S. Congress passed a law that allows most people with kidney failure coverage by Medicare. States and other sources may also help.
Health care providers often bill private health plans for additional costs. A person can live years with kidney failure, so getting help to pay for treatment is important.
Who can get a kidney transplant?
Kidney patients of all ages—from children to seniors—can get a transplant.
You must be healthy enough to have the operation. You must also be free from cancer and infection. Every person being considered for transplant will get a full medical and psychosocial evaluation to make sure they are a good candidate for transplant. The evaluation helps find any problems, so they can be corrected before transplant. For most people, getting a transplant can be a good treatment choice.
What if I’m older or have other health problems?
In many cases, people who are older or have other health conditions like diabetes can still have successful kidney transplants. Careful evaluation is needed to understand and deal with any special risks. You may be asked to do some things that can lessen certain risks and improve the chances of a successful transplant. For example, you may be asked to lose weight or quit smoking.
If you have diabetes, you may also be able to have a pancreas transplant. Ask your healthcare professional about getting a pancreas transplant along with a kidney transplant.
What is kidney transplant success rate?
According to the Organ Procurement and Transplantation Network:
- Failure of the transplanted kidney is reported in about 4 percent of deceased-donor kidney transplant recipients within one year after transplant and in 21 percent of cases five years after transplant.
- Among living-donor kidney transplant recipients, failure rates are about 3 percent at one year and 14 percent at five years after transplant.
Survival rates among kidney transplant recipients in U.S. transplant centers can be found online at the Scientific Registry of Transplant Recipients here (https://www.srtr.org/transplant-centers/?organ=kidney&recipientType=adult&query=).
If your new kidney fails, you can resume dialysis or consider a second transplant. You may also choose to discontinue treatment. This decision depends on your current health, your ability to withstand surgery and your expectations for maintaining a certain quality of life.
What should I eat or avoid eating with a kidney transplant?
You have more choices about what to eat after you receive a kidney transplant than you would if you were on dialysis. However, you will need to work with a dietitian to develop an eating plan that can change in response to your medicines, test results, weight, and blood pressure.
When was the first kidney transplant done?
In 1954, Dr. Joseph Murray and Dr. David Hume performed the first living-related kidney transplant at Brigham Hospital in Boston. Eight years later, in 1962, the same team of Dr. David Hume and Dr. Joseph Murray performed a successful transplant from a deceased donor.
What is a “preemptive” or “early” transplant?
Getting a transplant before you need to start dialysis is called a preemptive transplant. It allows you to avoid dialysis altogether. Getting a transplant not long after kidneys fail (but with some time on dialysis) is referred to as an early transplant. Both have benefits. Some research shows that a pre-emptive or early transplant, with little or no time spent on dialysis, can lead to better long-term health. It may also allow you to keep working, save time and money, and have a better quality of life.
Where do donated kidneys come from?
A donated kidney may come from someone who died and donated a healthy kidney. A person who has died and donated a kidney is called a deceased donor.
Donated kidneys also can come from a living donor. This person may be a blood relative (like a brother or sister) or non-blood relative (like a husband or wife). They can also come from a friend or even a stranger.
When a kidney is donated by a living person, the operations are done on the same day and can be scheduled at a convenient time for both the patient and the donor. A healthy person who donates a kidney can live a normal life with the one kidney that is left. But the operation is major surgery for the donor, as well as the recipient. As in any operation, there are some risks that you will need to consider.
Is it better to get a kidney from a living donor?
Kidneys from living or deceased donors both work well, but getting a kidney from a living donor can work faster and be better. A kidney from a living donor may last longer than one from a deceased donor.
To get a deceased donor kidney, you will be placed on a waiting list once you have been cleared for a transplant. It can take many years for a good donor kidney to be offered to you. From the time you go on the list until a kidney is found, you may have to be on some form of dialysis. While you’re waiting, you’ll need regular blood tests to make sure you are ready when a kidney is found. If you’re on dialysis, your center will make the arrangements for these tests. Your transplant center should know how to reach you at all times. Once a kidney become available, the surgery must be done as soon as possible.
Are there disadvantages to living donation?
A disadvantage of living donation is that a healthy person must undergo surgery to remove a healthy kidney. The donor will need some recovery time before returning to work and other activities. However, recent advances in surgery (often called minimally invasive or laparoroscopic surgery) allow for very small incisions. This means shorter hospital stays and recovery time, less pain, and a quicker return to usual activities. Living donors often experience positive feelings about their courageous gift.
If I am a woman of child bearing age, can I become pregnant after kidney transplant?
Women of child bearing age should consult with their transplant physician regarding pregnancy and/or contraception. If you are thinking about becoming pregnant, talk to your transplant team. Before becoming pregnant you should:
- Wait at least 1 year after your transplant
- Wait until your kidney function is stable
- See an obstetrician who specializes in high risk pregnancies
- Learn about the risks and benefits of breastfeeding. If you are interested in breastfeeding, it is very important to discuss the medications you are taking with your obstetrician. Some medicines can be passed on through your breast milk and can be harmful to your baby.
What are the financial costs to the living donor?
The surgery and evaluation is covered by Medicare or the recipient’s insurance. The living donor will not pay for anything related to the surgery. However, neither Medicare nor insurance covers time off from work, travel expenses, lodging, or other incidentals. The National Living Donor Assistance Program (https://www.livingdonorassistance.org/Home/default.aspx) or other programs may help cover travel and lodging costs.
Donors may be eligible for sick leave, state disability, and benefits under the federal Family Medical Leave Act. In addition, federal employees, some state employees, and certain other workers may be eligible for 30 days paid leave.
What is Medicare?
Medicare is a federal insurance program that pays health care costs for eligible people who are:
- age 65 or older
- under age 65 with certain disabilities
- of any age with end-stage renal disease (ESRD)
How can a person get Medicare for kidney failure?
To get Medicare for kidney failure, a person must meet two conditions:
- Be on dialysis or have a kidney transplant for end-stage renal disease
- Have paid enough taxes—or be the spouse or child of someone who has—through
- Social Security
- Railroad Retirement Board
- Government employment
What health plans does Medicare offer?
Three main types of Medicare health plans are available:
- Original Medicare has three parts:
- Part A (hospital) covers inpatient care, kidney transplantation, skilled nursing home residence, and hospice care. Part A has no premium for those who have paid enough Medicare taxes. A premium is an amount a person must pay periodically—monthly or quarterly—for Medicare, other health plan, or drug plan coverage. Part A does have a deductible, an amount a person must pay for health care or prescriptions before the health plan will pay. A person must pay a daily amount for hospital stays that last longer than 60 days.
- Part B (outpatient) covers most dialysis treatments and supplies, health care provider fees, and anti-rejection medications for transplant. Part B has a monthly premium based on a person’s income. Rates change each year. After a person pays the deductible each year, Part B pays 80 percent for most covered services as a primary payer. The billing staff of the service provider—hospital or clinic—can calculate how much a person will owe.
- Part D (medications) has a premium and covers some medications. Private insurance companies offer different Part D plans approved by Medicare. Costs and coverage vary by plan. A person who has few assets and earns less than 150 percent of the federal poverty level may qualify for extra help to pay Part D premiums and medication costs. The current-year guidelines can be found at (https://aspe.hhs.gov/poverty-guidelines). Information and applications for Part D plans can be found at (https://www.medicare.gov/). A person can also apply for Part D with an insurance company that sells one of these plans.
- Medicare Advantage plans, also called Part C, are sold by insurance companies. Medicare must approve Medicare Advantage plans. Each Medicare Advantage plan must cover Part A and Part B services and may cover other services, too. Medicare Advantage plans may have Part D medication coverage. If not, a person can buy a Part D plan separately. Medicare Advantage plans are not all the same. A person with failing kidneys who is thinking of choosing a Medicare Advantage plan should ask about the rules of the plan. The rules may specify which health care providers or hospitals a person may use. The plan may require a referral from a primary care provider to see a specialist. The plan may not cover medical expenses incurred during travel.
How much a person has to pay out-of-pocket each year will vary by plan. People who have a Medicare Advantage plan cannot have a Medigap plan to help pay out-of-pocket costs. See the section on Medigap (https://www.medicare.gov/supplements-other-insurance/whats-medicare-supplement-insurance-medigap).
- Four types of Medicare Advantage plans are available:
- health maintenance organizations (HMOs)
- preferred provider organizations (PPOs)
- private fee for service plans
- special needs plans for certain groups
- Those already on dialysis cannot join most Medicare Advantage plans. However, a person who had a Medicare Advantage plan before kidney failure can keep the plan. In some regions, special needs plans are designed for those on dialysis. More information can be found at (https://www.medicare.gov/) to learn if region-specific special needs plans are available for those on dialysis.
Other Medicare health plans are for certain groups, such as frail people living in the community, and people with multiple chronic illnesses and include hospital and medical coverage. Some pay for prescribed medications, too. Some are partially financed and administered by state health insurance programs—called Medicaid. The plans include the following:
- Medicare Cost Plans are HMOs, like the ones offered as Medicare Advantage plans, only out-of-network providers are paid as if the policy holder had original Medicare.
- Program of All-Inclusive Care for the Elderly (PACE) combines medical, social, and long-term care services for frail people who live and get health care in the community.
- Medicare Innovation Projects are special projects that test improvements in Medicare coverage, payment, and quality of care.
More information about Medicare Cost Plans and Demonstration or Pilot Programs can be found on the state Medicaid website at (https://www.medicaid.gov/). State Medicaid offices can provide more information about Program of All-Inclusive Care for the Elderly (PACE).
Where can a person enroll in Medicare?
A person can apply for Medicare online at a local Social Security office (https://www.ssa.gov/).
When does Medicare start for people with end-stage renal disease?
A person with end-stage renal disease can apply for Medicare at the start of dialysis or at the time of a kidney transplant. The Medicare start date depends on the type of treatment:
- Home dialysis, including peritoneal dialysis and hemodialysis at home. Medicare can start the first month of dialysis only if a person trains for home dialysis.
- Kidney transplant. Medicare can start the same month as the transplant. In some cases, Medicare could start up to 2 months earlier if the patient is admitted to the hospital and the transplant is delayed. For example, if a patient is admitted to the hospital for a transplant in March and the transplant is delayed until May, payment still begins in March. A transplant financial counselor can provide more information.
- In-center dialysis. Medicare will not start until the fourth month of in-center dialysis. For example, if a person starts dialysis in a clinic in July and does not train for home dialysis, Medicare will not start to pay until October 1.
When does Medicare end for people with end-stage renal disease?
Medicare continues for as long as a person is on dialysis and pays a premium, even for people who have jobs. Medicare will end for the following two reasons:
- Kidney failure is the only reason a person had Medicare and the person gets a kidney transplant. If the new kidney works and the person no longer needs dialysis, Medicare ends 3 years after the transplant surgery.
- A person’s kidneys get better and the person no longer needs dialysis. Medicare will end 12 months after a person stops dialysis, unless the person returns to dialysis or gets a transplant within those 12 months. Medicare will not end if the person is eligible because of age or disability.
How does Medicare pay if a person has other health insurance?
The rules for which plan pays first depend on which other health insurance a person has.
| Type of Insurance Plan | Who Pays First |
|---|---|
| Individual plan—not provided by an employer | Medicare always pays first. An individual plan always pays second. |
| Employer or union group plan | With kidney failure, the employer or union group plan pays first for 30 months* after a person is eligible for Medicare because of kidney failure. The 30-month clock starts whether the person enrolls in Medicare or not. However, the person will eventually have to enroll in Medicare. After the 30 months, Medicare pays first. The employer or union group plan may pay all or part of the rest. |
Footnote: *This time period is called the “Medicare secondary payer coordination period.”
Having Medicare Part B plus another health plan can limit what a person pays out-of-pocket for health care. In some cases, Medicare can limit how much a health care provider charges for services. If a person does not have Part B, the health care provider or dialysis clinic can bill the individual or group health plan and the person at a much higher rate. The person may have to pay what the plan does not pay.
In some situations, a person who has other insurance may be able to save money by not enrolling in Part B until the 30-month coordination period is over. The person would not have to pay the Part B premiums during that period.
Should a person with other insurance wait to start paying for Part B?
- YES, if: A person’s plan pays 100 percent of all health care costs during that time.
- If a person waits to enroll in both Part A and B, enrollment for both can happen at any time.
- If a person takes Part A—waiting to start Part B—the person can only enroll once a year from January 1 through March 31 and Part B will not start until July 1. A person should enroll in Part B in time to prevent a gap in coverage. For example, if the 30-month coordination period ends April 30, an employer or union group plan can stop paying first on May 1. If a person enrolled in Part B by March 31, Part B will not start paying first until July 1. The person will have large bills for May and June.
- NO, if: The person has to pay yearly deductibles, copays, or coinsurance, which are fees not covered by the insurance plan. Medicare may or may not pay those fees. However, having Medicare limits what a dialysis clinic can charge. The premium for Part B usually costs less than paying deductibles, copays, or coinsurance.
When does an employer or union group plan start to pay?
An employer or union group plan may help pay treatment and prescribed medication costs under the following circumstances:
- Before Medicare starts to pay for dialysis, the employer or union group plan may cover most or all costs.
- During the 30-month coordination period, the employer or union group plan pays the larger part of the costs first, and then Medicare pays its portion of the remaining costs.
- After the 30-month coordination period is over, Medicare pays the larger portion first, and then the employer or union group plan pays its portion of the remaining costs.
People with kidney failure should read their health insurance policy carefully to make sure it covers kidney failure treatment. If they have questions about their benefits, they should ask their insurance agent or employer benefits counselor.
What other federal programs can help?
The following federal programs can help cover the cost of kidney failure treatment:
- Social Security Disability Insurance (SSDI). Social Security Disability Insurance is a federal insurance plan that pays a monthly amount to people who cannot work. People earn Social Security Disability Insurance work credits when they pay Social Security taxes. A person must have enough credits based on age to qualify. Then, if an illness or injury prohibits a person from working for at least a year, Social Security Disability Insurance payments may be an option. A chart shows how many work credits a person needs at (https://www.ssa.gov/).
- Supplemental Security Income (SSI). Supplemental Security Income is a federal safety net program that pays a monthly amount to disabled children and adults who earn little and have few assets. A person who gets SSI may be able to get food stamps and Medicaid, too.
More information about both Social Security Disability Insurance (SSDI) and Supplemental Security Income (SSI) and how to apply can be found at (https://www.ssa.gov/)
What state programs can help?
State programs such as Medicaid, Medigap, and Medicare Savings Programs are funded in part by the Federal Government. However, states provide the services and decide who receives help.
Medicaid. Medicaid is a state program for those with low incomes and few assets. Each state runs its own program. The Federal Government requires that Medicaid programs cover a specific set of services; however, states can choose to cover more services in addition to the ones required. A person may have Medicaid alone or Medicare and Medicaid. If a person has both types of coverage, Medicare pays first and Medicaid pays second. Medicaid may pay for things Medicare does not. A person can apply for Medicaid at a city or county Department of Social Services office. A social worker can explain a state’s Medicaid program and help a person apply. More information about Medicaid can be found at (https://www.medicaid.gov/).
Medigap, also known as Medicare supplement. A Medigap plan can help pay what Original Medicare does not pay for covered services. Insurance companies sell Medigap coverage. People who have a Medicare Advantage plan cannot also have a Medigap plan.
For people who are 65 and older, federal law says that in the first 6 months a person has Part B, companies cannot deny an application or limit payment for anything Original Medicare covers based on the person’s health. Some states make insurance companies sell at least one Medigap coverage plan to those under 65 with Medicare. State insurance offices can explain the plans in their state. Local offices can be found by clicking on a map at (https://www.naic.org/).
Medicare Savings Programs. Some states may pay Medicare premiums, deductibles, and coinsurance if a person has low income and few assets. A city or county Department of Social Services can determine whether a person is eligible.
Kidney-specific state assistance programs. Some states use state funds to help pay for specific kidney-related costs. A dialysis or transplant clinic social worker or a social worker in a local Department of Social Services can help a person determine if a state has a kidney program.
State Health Insurance Assistance Program (SHIP). State Health Insurance Assistance Programs get money from the Federal Government to give free health insurance advice to those with Medicare. A person who needs more health insurance should talk with a State Health Insurance Assistance Program (SHIP) counselor or a social worker here (https://shipnpr.acl.gov/(X(1)S(x5lcbx45ep0c5a55spqfhejb))/Default.aspx).
What programs can help special populations?
Many programs can help specific populations such as U.S. veterans; military service members, retirees, and families; American Indians and Alaska Natives; children; people with disabilities; job seekers with kidney failure; kidney transplant recipients; and living organ donors.
U.S. Veterans
For U.S. veterans, the U.S. Department of Veterans Affairs (VA) can help pay some health costs. Veterans can see if they qualify and apply online at (https://www.va.gov/health-care/). A veteran can learn more at a local VA hospital. Some VA hospitals provide dialysis. Others contract with dialysis clinics to give veterans better access to treatment. The VA also has its own network of transplant centers.
Military Service Members, Retirees, and Families
A person may be able to get TRICARE—the health care program serving uniformed service members, retirees, and their families worldwide—if that person is:
- an active duty service member
- a military retiree
- a family member of an active duty service member or military retiree
- a member of the National Guard/Reserves on active duty for 30 days
- a family member of someone who is in the National Guard/Reserves on active duty for 30 days
TRICARE for Life is a specific TRICARE plan that offers secondary coverage for people who have Medicare Part A and Part B.
Information about TRICARE and phone numbers for its four regions can be found at (https://www.tricare.mil/).
American Indians and Alaska Natives
The Indian Health Service may help members of federally recognized American Indian or Alaska Native tribes. More information is available on the Indian Health Service website at (https://www.ihs.gov/). An American Indian or Alaska Native may also be eligible for help from public, private, and state programs.
Children
The Children’s Health Insurance Program (CHIP) gives free or low-cost Medicaid to children whose parents earn too much for Medicaid, though not enough to pay for a health plan. Children’s Health Insurance Program (CHIP) may also provide assistance to parents. Children’s Health Insurance Program (CHIP) is a federal and state program. More information can be found at (https://www.insurekidsnow.gov/).
People with Disabilities
A person can find state and local help for people with disabilities at (https://www.dol.gov/odep/topics/disability.htm). On this website, a person can learn more about civil rights, community life, education, emergency planning, work, health, housing, technology, and transportation. A social worker can refer a person to federal, state, and local resources.
Job Seekers with Kidney Failure
Laws such as the Americans with Disabilities Act protect people with certain disabilities, including kidney failure. A person with kidney failure may find job training and job seeking information through:
- state vocational rehabilitation programs
- private employment networks that contract with Social Security to help people with disabilities get jobs
More information about Social Security work incentives, the “Ticket to Work” program, and who can help, including vocational rehabilitation programs and employment networks, can be found at (https://yourtickettowork.ssa.gov/).
Kidney Transplant Recipients
The United Network for Organ Sharing (UNOS) has a website called Transplant Living at (https://transplantliving.org/financing-a-transplant/).
What private organizations can help?
Private organizations include charities and foundations. A few exist specifically to help people with kidney disease and kidney failure, such as the:
- American Kidney Fund. The American Kidney Fund gives small grants to U.S. dialysis and transplant patients based on need. The American Kidney Fund has grants to help pay health plan premiums. A social worker can help a person apply for assistance. The American Kidney Fund depends on donations, so there may be times when funds are low. More information can be found at (http://www.kidneyfund.org/).
- National Kidney Foundation. Local National Kidney Foundation offices may help with nutrition, transportation, medications, and scholarships. A social worker can help a person apply for assistance. The National Kidney Foundation depends on donations, so there may be times when funds are low. More information can be found at (https://www.kidney.org/).
Kidney transplant surgery
During kidney transplant surgery, a surgeon places a healthy kidney into your body. You’ll receive general anesthesia before the surgery. The surgery usually takes 3 or 4 hours. Unless your damaged kidneys cause infections or high blood pressure or are cancerous, your own kidneys generally aren’t taken out and they can stay in your body where they are. Surgeons usually transplant a kidney into the lower abdomen near the groin, where it’s easiest to connect it to your important blood vessels and bladder. Putting the new kidney in your abdomen also makes it easier to take care of any problems that might come up.
If you’re on a waiting list for a donor kidney, you must go to the hospital to have your transplant surgery as soon as you learn that a kidney is available.
If a family member or friend is donating the kidney, you’ll schedule the surgery in advance. Your surgical team will operate on you and your donor at the same time, usually in side-by-side rooms. One surgeon will remove the kidney from the donor, while another prepares you to receive the donated kidney.
You’ll be sore at first, but you should be out of bed in a day or so, and home within a week. If the kidney came from a living donor, it should start to work very quickly. A kidney from a deceased donor can take longer to start working—two to four weeks or more. If that happens, you may need dialysis until the kidney begins to work.
After surgery, you’ll be taught about the medicines you’ll have to take and their side effects. You’ll also learn about diet. If you’ve been on dialysis, you’ll find that there are fewer restrictions on what you can eat and drink, which is one of the benefits of a transplant.
Figure 1. Kidney transplant surgery
Kidney transplant procedure
Before the procedure
Finding a match
A kidney donor can be living or deceased, related or unrelated to you. Your transplant team will consider several factors when evaluating whether a donor kidney will be a good match for you.
Tests to determine whether a donated kidney may be suitable for you include:
- Blood typing. It’s preferable to get a kidney from a donor whose blood type matches or is compatible to your own. Blood-type incompatible transplants are also possible but require additional medical treatment before and after transplant to reduce the risk of organ rejection. These are known as ABO incompatible kidney transplants.
- Tissue typing. If your blood type is compatible, the next step is a tissue typing test called human leukocyte antigen (HLA) typing. This test compares genetic markers that increase the likelihood the transplanted kidney will last a long time. A good match means it’s less likely that your body will reject the organ.
- Crossmatch. The third and final matching test involves mixing a small sample of your blood with the donor’s blood in the lab. The test determines whether antibodies in your blood will react against specific antigens in the donor’s blood. A negative crossmatch means they are compatible and your body isn’t as likely to reject the donor kidney. Positive crossmatch kidney transplants are also possible but require additional medical treatment before and after the transplant to reduce the risk of your antibodies reacting to the donor organ.
Additional factors your transplant team may consider in finding the most appropriate donor kidney for you include matching age, kidney size and infection exposure.
During the procedure
Kidney transplants are performed with general anesthesia, so you’re not aware during the procedure. The surgical team monitors your heart rate, blood pressure and blood oxygen level throughout the procedure.
During the surgery:
- A kidney transplant usually takes 3 to 4 hours, with a couple of hours in recovery. The surgeon will make a cut in the lower part of your body and place the new kidney in position.
- The blood vessels of the new kidney are attached to blood vessels in the lower part of your abdomen, just above one of your legs.
- The new kidney’s ureter — the tube that links the kidney to the bladder — is connected to your bladder.
- Your old (diseased) kidneys are not usually removed unless they are causing complications such as high blood pressure, kidney stones, pain or infection.
- You will usually have a temporary tube to drain your urine (known as a catheter) for a few days.
- If your new kidney does not work right away, you may need dialysis for a short while until it does.
Your medical team will check if your kidney works and find any early signs of rejection by your body.
After the surgery, you will probably need to stay in hospital for a few weeks to recover.
After the procedure
After your kidney transplant, you can expect to:
- Spend several days to a week in the hospital. Doctors and nurses monitor your condition in the hospital’s transplant recovery area to watch for signs of complications. Your new kidney will make urine like your own kidneys did when they were healthy. Often this starts immediately. In other cases it may take several days. Expect soreness or pain around the incision site while you’re healing. Most kidney transplant recipients can return to work and other normal activities within three to eight weeks after transplant. No lifting objects weighing more than 10 pounds or exercise other than walking until the wound has healed (usually about six weeks after surgery).
- Have frequent checkups as you continue recovering. After you leave the hospital, close monitoring is necessary for a few weeks. You may need blood tests several times a week and have your medications adjusted in the weeks following your transplant. During this time, if you live in another town, you may need to make arrangements to stay near the transplant center.
- Take medications the rest of your life. You’ll take a number of medications after your kidney transplant. Drugs called immunosuppressants (anti-rejection medications) help keep your immune system from attacking and rejecting your new kidney. Additional drugs help reduce the risk of other complications, such as infection, after your transplant.
Kidney transplant recovery
Many people report feeling much better right after having kidney transplant surgery. For some people, it takes a few days for the new kidney to start working. You probably will need to stay in the hospital several days to recover from surgery—longer if you have any problems after the kidney transplant. You’ll have regular follow-up visits with your nephrologist after leaving the hospital.
If you have a living donor, the donor will probably also stay in the hospital for several days. However, a new technique for removing a kidney for donation that uses a smaller cut may make it possible for the donor to leave the hospital in 2 to 3 days.
Before you leave the hospital, you need to learn how to stay healthy and take care of your donor kidney. You will have to take one or more anti-rejection medicines—also called immunosuppressants. Without medicine, your immune system may treat your donor kidney as foreign, or not your own, and attack your new kidney. Anti-rejection medicines may have side effects.
You may also need to take other medicines—for example, antibiotics to protect against infections. Your transplant team will teach you what each medicine is for and when to take each one. Be sure you understand the instructions for taking your medicines before you leave the hospital.
When you’re taking anti-rejection medicines, you’re at a greater risk for infection. Anti-rejection medicines can dull symptoms of problems such as infection. Call your transplant center right away if you aren’t feeling well or have:
- a fever of more than 100 °F (37.8 °C)
- drainage from your surgical scar
- burning when you pass urine
- a cold or cough that won’t go away
How do I know my new kidney is working?
Blood tests help you know your donor kidney is working. Before you leave the hospital, you’ll schedule an appointment at the transplant center to test your blood. The tests show how well your kidneys are removing wastes from your blood.
At first, you’ll need regular checkups and blood tests at the transplant center or from your doctor. As time goes on, you’ll have fewer checkups.
Your blood tests may show that your kidney is not removing wastes from your blood as well as it should. You also may have other symptoms that your body is rejecting your donor kidney. If you have these problems, your transplant surgeon or nephrologist may order a kidney biopsy.
What happens after I go home?
Once you are home from the hospital, the most important work begins—the follow-up. For your kidney transplant to be successful, you will have regular checkups, especially during the first year. At first, you may need blood tests several times a week. After that, you’ll need fewer checkups, but enough to make sure that your kidney is working well and that you have the right amount of anti-rejection medication in your body. And because these anti-rejection medications make your body more vulnerable to infection, your doctor may also prescribe antibacterial, antiviral and antifungal medications.
Skin checkups with a dermatologist to screen for skin cancer and keeping your other cancer screening up to date is strongly advised.
What if my body tries to reject the new kidney?
One thing that you and your healthcare team will watch for is acute rejection, which means that your body is suddenly trying to reject the transplanted kidney. A rejection episode may not have any clear signs or symptoms. That is why it is so important to have regular blood tests to check how well your kidney is working. Things you might notice that can let you know you are having rejection are fevers, decreased urine output, swelling, weight gain, and pain over your kidney.
The chances of having a rejection episode are highest right after your surgery. The longer you have the kidney, the lower the chance that this will happen. Unfortunately, sometimes a rejection episode happens even if you’re doing everything you’re supposed to do. Sometimes the body just doesn’t accept the transplanted kidney. But even if a rejection episode happens, there are many ways to treat it so you do not lose your transplant. Letting your transplant team know right away that you think you have symptoms of rejection is very important.
When can I return to work?
How soon you can return to work depends on your recovery, the kind of work you do, and your other medical conditions. Many people can return to work eight weeks or more after their transplant. Your transplant team will help you decide when you can go back to work.
Will my sex life be affected?
People who have not had satisfactory sexual relations due to kidney disease may notice an improvement as they begin to feel better. In addition, fertility (the ability to conceive children) tends to increase. Men who have had a kidney transplant have fathered healthy children, and women with kidney transplants have had successful pregnancies. It’s best to talk to your healthcare practitioner when considering having a child.
Women should avoid becoming pregnant too soon after a transplant. Most centers want women to wait a year or more. All pregnancies must be planned. Certain medications that can harm a developing baby must be stopped six weeks before trying to get pregnant. Birth control counseling may be helpful. It’s important to protect yourself against sexually transmitted diseases (STDs). Be sure to use protection during sexual activity.
Will I need to follow a special diet?
In general, transplant recipients should eat a heart-healthy diet (low fat, low salt) and drink plenty of fluids. If you have diabetes or other health problems, you may still have some dietary restrictions. A dietitian can help you plan meals that are right for you.
Kidney transplant survival rate
According to the Organ Procurement and Transplantation Network:
- Failure of the transplanted kidney is reported in about 4 percent of deceased-donor kidney transplant recipients within one year after transplant and in 21 percent of cases five years after transplant.
- Among living-donor kidney transplant recipients, failure rates are about 3 percent at one year and 14 percent at five years after transplant.
Survival rates among kidney transplant recipients in U.S. transplant centers can be found online at the Scientific Registry of Transplant Recipients here (https://www.srtr.org/transplant-centers/?organ=kidney&recipientType=adult&query=).
Kidney transplant complications
The donated kidney may start working right away or may take up to a few weeks to make urine. If the new kidney doesn’t start working right away, you’ll need dialysis treatments to filter wastes and extra salt and fluid from your body until it starts working.
Transplant rejection is rare right after surgery and can take days or weeks to occur. Rejection is less common when the new kidney is from a living donor than when it’s from a deceased donor.
Complications of the kidney transplant procedure
Kidney transplant surgery carries a risk of significant complications, including:
- Blood clots
- Bleeding
- Leaking from or blockage of the tube (ureter) that links the kidney to the bladder
- Infection
- Failure of the donated kidney
- Rejection of the donated kidney
- An infection or cancer that can be transmitted with the donated kidney
- Death, heart attack and stroke
Anti-rejection medication side effects
After a kidney transplant, you’ll take medications to help prevent your body from rejecting the donor kidney. These medications can cause a variety of side effects, including:
- Acne
- Bone thinning (osteoporosis) and bone damage (osteonecrosis)
- Diabetes
- Excessive hair growth or hair loss
- High blood pressure
- High cholesterol
- Increased risk of cancer, particularly skin cancer and lymphoma
- Infection
- Puffiness (edema)
- Weight gain
Kidney transplant rejection
Rejection is the most common and important complication that may occur after receiving a transplant. Since you were not born with your transplanted kidney, your body will think this new tissue is “foreign” and will try to protect you by “attacking” it. Rejection is a normal response from your body after any transplant surgery. You must take anti-rejection medicine exactly as prescribed to prevent rejection.
There are two common types of rejection:
- Acute Rejection – Usually occurs anytime during the first year after transplant and can usually be treated successfully.
- Chronic Rejection – Usually occurs slowly over a long period of time. The causes are not well understood and treatment is often not successful.
Kidney transplant rejection symptoms
A rejection episode may not have any clear signs or symptoms. That is why it is so important to have regular blood tests to check how well your kidney is working. Things you might notice that can let you know you are having rejection are fevers, decreased urine output, swelling, weight gain, and pain over your kidney.
The routine blood tests that you have at the transplant center will reveal early signs of rejection. You may develop high blood pressure or notice swelling because your kidney isn’t getting rid of extra salt and fluid in your body.
Your health care provider will treat early signs of rejection by adjusting your medicines to help keep your body from rejecting your new kidney.
Transplant rejection is becoming less common. However, your body may still reject the donor kidney, even if you do everything you should. If that happens, you may need to go on dialysis and go back on the waiting list for another kidney. Some people are able to get a second kidney transplant.
How often do rejection episodes happen?
Rejections happen much less often nowadays. That’s because there have been many improvements in immunosuppressive medicines. However, the risk of rejection is different for every person. For most people, rejection can be stopped with special anti-rejection medicines. It’s very important to have regular checkups to see how well your kidney is working, and make sure you are not having rejection.
Infection
The anti-rejection medicines that help keep your body from rejecting your transplanted kidney also lower your immune system. Because your immune system is lowered, viral and other infections can be a problem.
What is the best way to stay healthy?
Finding and treating infections as early as possible is the best way to keep you and your transplanted kidney healthy. Exposure to diseases such as the flu or pneumonia can make you very sick. Receiving vaccines as determined by your transplant team can help you stay healthy. It is also important to frequently wash your hands or use an antimicrobial gel during cold and flu season.
What problems should I report to my doctor?
You should report any of the following problems to your doctor as soon as possible:
- Sores, wounds, or injuries; especially those that don’t heal
- Urinary tract infection symptoms such as frequent urge to urinate, pain or burning feeling when urinating, cloudy or reddish urine, or bad smelling urine
- Respiratory infection symptoms such as cough, nasal congestion, runny nose, sore or scratchy throat, or fever
How can I avoid getting infections?
To avoid getting infections you should:
- Wash your hands regularly
- Maintain good hygiene habits especially around pets
- Avoid close contact with people who have contagious illnesses
- Avoid close contact with children recently vaccinated with live vaccines (see section on Vaccines). Also, no one in the household should get the nasal influenza vaccine
- Practice safe food handling.
- Inform your doctor well in advance of any travel plans
Can a vaccine be harmful after kidney transplant?
Vaccines help your body protect you from infection. Some vaccines are not good for you when you have a transplant. For example, you should avoid all “live vaccines.” Check with your transplant team before receiving any vaccines or boosters.
What are some general rules for getting vaccines such as Hepatitis B, live vaccines, or a flu shot?
You should:
- Get Hepatitis B vaccine before transplant
- Avoid all live vaccines
- Avoid the nasal influenza vaccine
- Wait at least 3-6 months after transplant before getting a flu shot; then get a yearly booster (injection only)
What if someone I know receives a live vaccine?
You should avoid direct contact with anyone who has received a live vaccine. Examples include:
- Children who have received oral polio vaccine for 3 weeks
- Children who have received measles or mumps vaccines
- Adults who have received attenuated (a-TEN-yoo-ated) varicella vaccine to prevent zoster (attenuated means weaker strength)
- Children or adults who have received the nasal influenza vaccine
What if I travel to another country?
Contact your transplant physician if you plan to travel to another country. You may need to receive certain vaccines to prevent diseases that are common to the area.
Which vaccines are safe to get?
Always talk to your transplant coordinator before getting any vaccines or boosters. The following vaccines are recommended:
- Diphtheria-pertussis-tetanus
- Haemophilus influenzea B
- Hepatitis A (for travel or other risk)
- Hepatitis B (receive before transplant)
- Pneumovax (single booster at 5 years)
- Inactivated polio
- Influenza types A and B (booster every year)
- Meningococcus (if at high risk)
- Typhoid Vi
Which vaccines should you avoid?
You should NOT receive the following “live” vaccines:
- Varicella zoster
- Bacillus Calmette-Guerin (BCG)
- Smallpox
- Intranasal influenza
- Live oral typhoid Ty21a and other newer vaccines
- Measles (except during an outbreak)
- Mumps
- Rubella
- Oral polio
- Live Japanese B encephalitis vaccine
- Yellow fever
New-Onset Diabetes After Transplant
Even if you did not have diabetes before, you may develop diabetes after transplant. This type of diabetes is called new-onset diabetes after transplant or new-onset diabetes after transplant. This can occur as a side effect of the medications that you need to prevent rejection of your new kidney.
What are my chances of having new-onset diabetes after transplant?
- Your chances of having new-onset diabetes after transplant will be higher if you are obese. Your chances are also increased if others in your family have diabetes.
Why should I worry about diabetes?
- Having a high blood sugar level due to diabetes or due to new-onset diabetes after transplant can cause serious damage to your heart, blood vessels, eyes, feet, and nerves.
How can I find out about my blood sugar?
- Blood sugar levels will be closely watched while you are in the hospital after the transplant and in the outpatient clinic. If needed, your doctors will help you develop a plan to keep your blood sugar under control. If you are on corticosteroid medication (such as prednisone), your blood sugar levels will improve as the dose of this medication is decreased in the first 2 months after transplant.
If I have diabetes, how can I control my blood sugar?
Your transplant team will help you manage your blood sugar. High blood sugar is usually done with:
- A carbohydrate-controlled diet
- Exercise, as allowed by your doctor
- Diabetes medications
Heart Disease
People with kidney transplants are at greater risk for heart disease. There are many causes for heart disease including: smoking, diabetes, overweight, hypertension, high cholesterol and blood lipids, and number of years on dialysis.
How can I lower my chances of getting heart disease?
Here are some important things for you to do now to lower your chances for getting heart disease later (see information on each topic):
- Control high blood pressure
- Manage cholesterol and blood lipids
- Stop smoking
- Exercise, as allowed by your doctor
- Maintain a healthy weight by following a healthy diet
- If you have diabetes, work to keep it well controlled
Cancer
Your chances are greater than those without a transplant. The immune system is very important to keep your body from getting cancer. Anti-rejection (immunosuppressive) medications decrease your immune function and may decrease the body’s defenses for certain types of cancer. There are things that you can do to lower your chances of getting cancer.
How do I know if I am at increased risk for skin cancer?
- Skin cancer is the most common type of cancer and can cause death. If you have fair skin, live in a high sun exposure area or have a history of skin cancer you may have a higher chance for getting skin and lip cancer. There are also certain anti-rejection medication that may increase your risk more than others.
How can I lower my chances of getting skin cancer?
To lower your chances of getting skin cancer you should:
- Avoid direct sunlight
- Avoid tanning booths
- Wear UVA and UVB sunscreen protection
- Be aware of any changes in your skin. Preform self-examines of your skin and lips regularly. Tell your doctor if you notice a strange lump, bump, sore, ulcer, or colored area on the skin
- Follow the advice of your transplant team and kidney doctor for further skin care. Your doctor may recommend going to a dermatologist (skin doctor) for a yearly exam
What other cancer screening should I talk to my doctor about?
- Women – Discuss risk of cervical, breast and colon cancer with your doctor regularly and keep up with recommended exams
- Men – Discuss risk of prostate and colon cancer with your doctor regularly and keep up with recommended exams
Bone Disease
Bone disease (also known as chronic kidney disease-mineral and bone disorder) may continue even after your kidney transplant. Chronic kidney disease-mineral and bone disorder occurs due to medication side-effects, previous kidney disease, diabetes, smoking, lack of exercise, menopause, or number of years on dialysis.
Bone disease can cause weak and brittle bones and increase your chance for fractures.
How can I find out if I have bone disease?
- To check your bone health your doctor will test your blood levels of calcium, phosphorus, parathyroid hormone (PTH) and vitamin D.
How can I lower my chances of having bone disease?
- Weight bearing exercise such as walking, biking and using weights is a good way to increase bone and muscle strength. If your blood level of vitamin D is low your doctor may prescribe a vitamin D supplement.
Can I take bone density medications?
- Bone density medications are not commonly used after kidney transplant. If your doctor suggests this option a bone biopsy may be needed to check your bone health before starting this medication.
Anemia
Following a kidney transplant you may have anemia (low red blood cell count) due to the surgery, medication side-effects, infection, abnormal breakdown of red blood cells, or organ rejection. Blood pressure medication can cause your body to make fewer red blood cells.
Mild anemia can cause minor problems like feeling tired and having pale skin. If left untreated, anemia can cause a lack of oxygen to organs and lead to serious health problems such as heart failure.
What should I do if I have anemia?
- If you have anemia your doctor may prescribe an iron supplement or other medications. There are many choices for iron pills; if you do not tolerate one iron supplement, ask about other choices. Your doctor will work with you to decide on the best treatment. It is also important to eat a healthy diet.
Gout
Gout is a condition that occurs when high blood uric acid levels cause crystals to build up in the joints, causing painful swelling. Your body may have a hard time getting rid of uric acid (a normal waste product in blood) after your kidney transplant. This is often due to side-effects from medications, such as cyclosporine, leading to a high uric acid level in blood.
What do I do if I have high blood uric acid levels or gout?
Your doctor will help you manage high blood uric acid levels or gout. This is usually done with:
- Medication (avoid non-steroidal anti-inflammatory drugs (NSAIDS) whenever possible)
- A diet that limits certain foods and beverages including red meat, seafood, sugared soft drinks and alcohol (especially beer)
- Keeping a healthy weight
- Controlling high blood pressure, high blood lipid levels and diabetes, if present
High Blood Pressure
If you had high blood pressure before getting your new kidney, it may continue after your transplant. High blood pressure might also occur as a side-effect of anti-rejection medications, organ rejection and/or obesity (from weight gain after transplant).
Should I check my blood pressure?
- You should check your blood pressure as directed by your transplant team. The target blood pressure for people with a kidney transplant is less than 130/80.
How can I control my blood pressure?
Your doctor will help you manage your blood pressure. High blood pressure is usually controlled with:
- Weight control including regular exercise
- A low salt diet
- Blood pressure medication
High Cholesterol and Blood Lipids
Many people may have higher cholesterol and lipid levels in the blood after transplant due to medication side-effects , weight gain, poor diet, family history, or lack of exercise. Kidney-related issues that cause protein in the urine (proteinuria) can also increase blood lipids.
Why should I worry about high cholesterol and blood lipids?
- High blood lipids can lead to clogged blood vessels. When this occurs it increases risk of heart disease and stroke.
How can I control my cholesterol and blood lipids?
Your doctor will help you manage your cholesterol and blood lipids. Controlling high cholesterol and blood lipids is usually done with:
- A heart healthy diet
- More exercise as allowed by your doctor
- Lipid lowering medication
- Stop smoking. Smoking cigarettes significantly increases your risk for heart disease, cancer and lung disease. It may also decrease the amount of time your new kidney will work.
What are anti-rejection medications?
Anti–rejection (immunosuppressant) medications decrease the body’s natural immune response to a “foreign” substance (your transplanted kidney). They lower (suppress) your immune system and prevent your body from rejecting your new kidney.
There are 3 groups of anti-rejection (immunosuppressant) medications:
- Induction agent – Powerful anti-rejection medication used before the kidney transplant in the operating room, or immediately after the transplant surgery
- Maintenance agents – Anti-rejection medications you will take daily for as long as you have your transplanted kidney
- Rejection agents: Medications which are used for the treatment for rejection episodes
Why do I need to take anti-rejection medication?
Kidney rejection is hard to diagnose in its early stages. Rejection is often not reversible once it starts. You should never stop taking your anti-rejection medication no matter how good you feel and even if you think your transplanted kidney is working well. Stopping or missing them may cause a rejection to occur.
How should I take anti-rejection medication?
Here are some tips to help you take your anti-rejection (immunosuppressant) medication as directed:
- Make taking your medicine part of your daily routine
- Use digital alarms and alerts to remember when to take your medication. Be creative because it is easy to forget, especially once you are feeling wellKnow all of your medications by name and dose. Know the reason for taking each medication.
- Ask for and review all written instructions for any change in medication dose or frequency
- Tell your transplant team of problems and concerns about medications during every clinic visit
- If a doctor other than a member or your transplant team gives you a prescription, notify the transplant team before taking. Certain medications can interfere with your anti-rejection medications and keep them from working.
- Continue to take your anti-rejection medication no matter how great you feel, even if you think your transplanted kidney is working well. Stopping them may cause rejection to occur.
Anti-rejection medicines side effects
Some anti-rejection medicines may change your appearance. Your face may get fuller, you may gain weight, or you may develop acne or facial hair. Not all people have these side effects.
Anti-rejection medicines weaken your immune system, which can lead to infections. In some people over long periods of time, a weakened immune system can increase their risk of developing cancer. Some anti-rejection medicines cause cataracts, diabetes, extra stomach acid, high blood pressure, bone disease and increased your risk of some forms of cancer.
When used over time, these medicines may also cause liver or kidney damage in some people. Your transplant team will order regular tests to monitor the levels of anti-rejection medicines in your blood and to measure your liver and kidney function.
Life after a kidney transplant
After the operation, you will likely need to take medicine for the rest of your life to prevent your body from rejecting the new kidney. Your healthcare team will probably talk to you about your treatment plan, how to monitor your health and the self-care required. You will probably still need regular check-ups and you need to continue taking your medication as prescribed.
Since the anti-rejection medication weakens your immune system, you should try to avoid getting infections by:
- staying away from people who you know are sick, (e.g. with the flu or chickenpox)
- washing your hands well before eating
- covering any cuts or wounds.
Also, follow your healthcare team’s advice on living a healthy lifestyle, such as getting enough physical activity and eating healthily. For instance, avoid high-salt foods and drinking excessive amounts of alcohol because salt and alcohol can raise your blood pressure, which can damage your kidney.
Most people feel they have a better quality of life after a kidney transplant.
Gaining weight after kidney transplant
It is very likely that you will gain weight after your kidney transplant. Weight gain after transplant is common due to medication side-effects and a less strict diet (as compared to the diet for dialysis).
Why should I worry about gaining too much weight?
- Gaining too much weight can lead to having too much total body fat. This is known as obesity. Obesity increases the risk of heart disease and new-onset diabetes after transplant (NODAT).
How can I keep a healthy weight?
Your transplant team will include a dietitian. Your doctor and dietitian will help you develop a plan to keep a healthy weight. To control weight, work with your dietitian to reduce calories. Also, you should exercise regularly as allowed by your doctor
If I have Medicare, can I ask my doctor for a Medical Nutrition Therapy referral to see a registered dietitian?
Medicare covers Medical Nutrition Therapy services prescribed by a doctor for patients with diabetes or chronic kidney disease, and includes transplant patients. The services provided by a registered dietitian include:
- An initial assessment of your nutrition and lifestyle
- Nutrition counseling
- Information on managing lifestyle factors that affect your diet
- Follow-up visits to check progress on managing your diet
Healthy Lifestyle
A healthy lifestyle is important for many reasons. Many conditions such as new onset diabetes after transplant (NODAT), high cholesterol, and high blood pressure can be improved through living a healthy lifestyle. A healthy lifestyle also helps bring about a feeling of wellness.
Your transplant team will help you make the right choices to develop and live a healthy lifestyle. You should:
- Return to your normal routine, such as work, school or housework.
- Increase physical activity with regular exercise. Check with your doctor before you start an exercise program.
- Eat a proper diet. A dietitian can help you make the right heart healthy food choices for a healthy lifestyle.
- Lose weight, as needed, to reach and maintain a healthy weight. Consult with your dietitian and transplant team for a healthy weight loss diet. Fad diets should be avoided. Once you get to your healthy weight you will feel better.
How family and friends can help
Making the decision to have a kidney transplant, waiting for a donor organ, having the operation itself and getting used to life after the transplant can be stressful. The medication to prevent rejection can also affect your mood. However, family and friends can help in a number of ways, including:
- supporting you emotionally
- reminding you about taking your medications
- driving you to your appointments.



{kind=link}