Contents
What is cardioversion
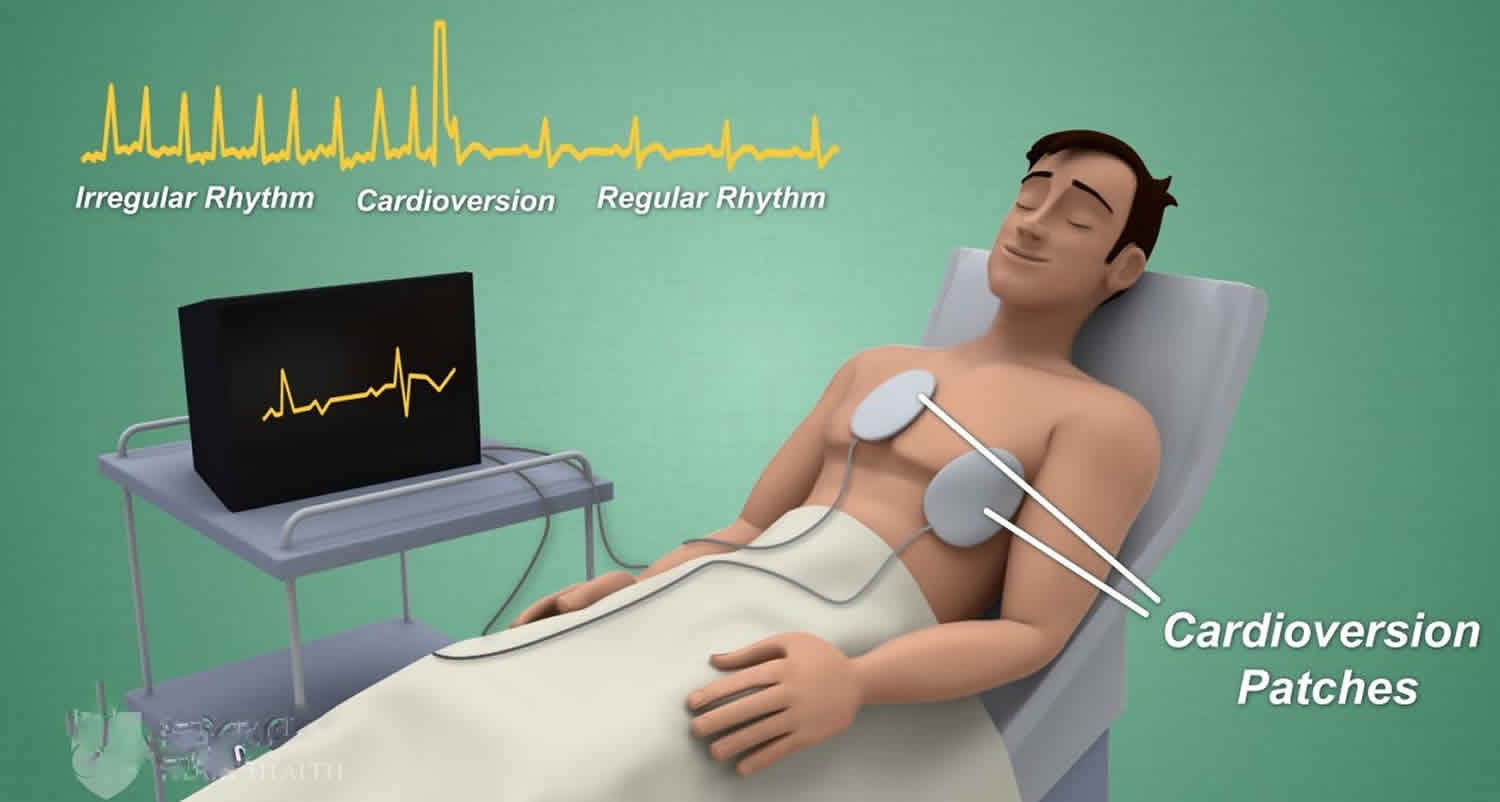
Cardioversion is a procedure that uses external electric shocks to get your abnormal heart rhythm (arrhythmia) back to a normal rhythm (sinus rhythm). Cardioversion is done by sending electric signals to your heart through electrodes placed on the chest. Cardioversion is called defibrillation when it is done in an emergency to prevent death due to potentially fatal ventricular arrhythmias that can result in sudden cardiac arrest. Alternatively, your doctor can schedule cardioversion as a way to treat arrhythmias (abnormal heart rhythms) in the upper chambers of your heart called atrial fibrillation (A Fib). If untreated, atrial fibrillation can increase your risk for stroke and heart failure. Most elective or “non-emergency” cardioversions are performed to treat atrial fibrillation (A Fib) or atrial flutter (AFL), non-life threatening abnormal rhythms in the top of the heart.
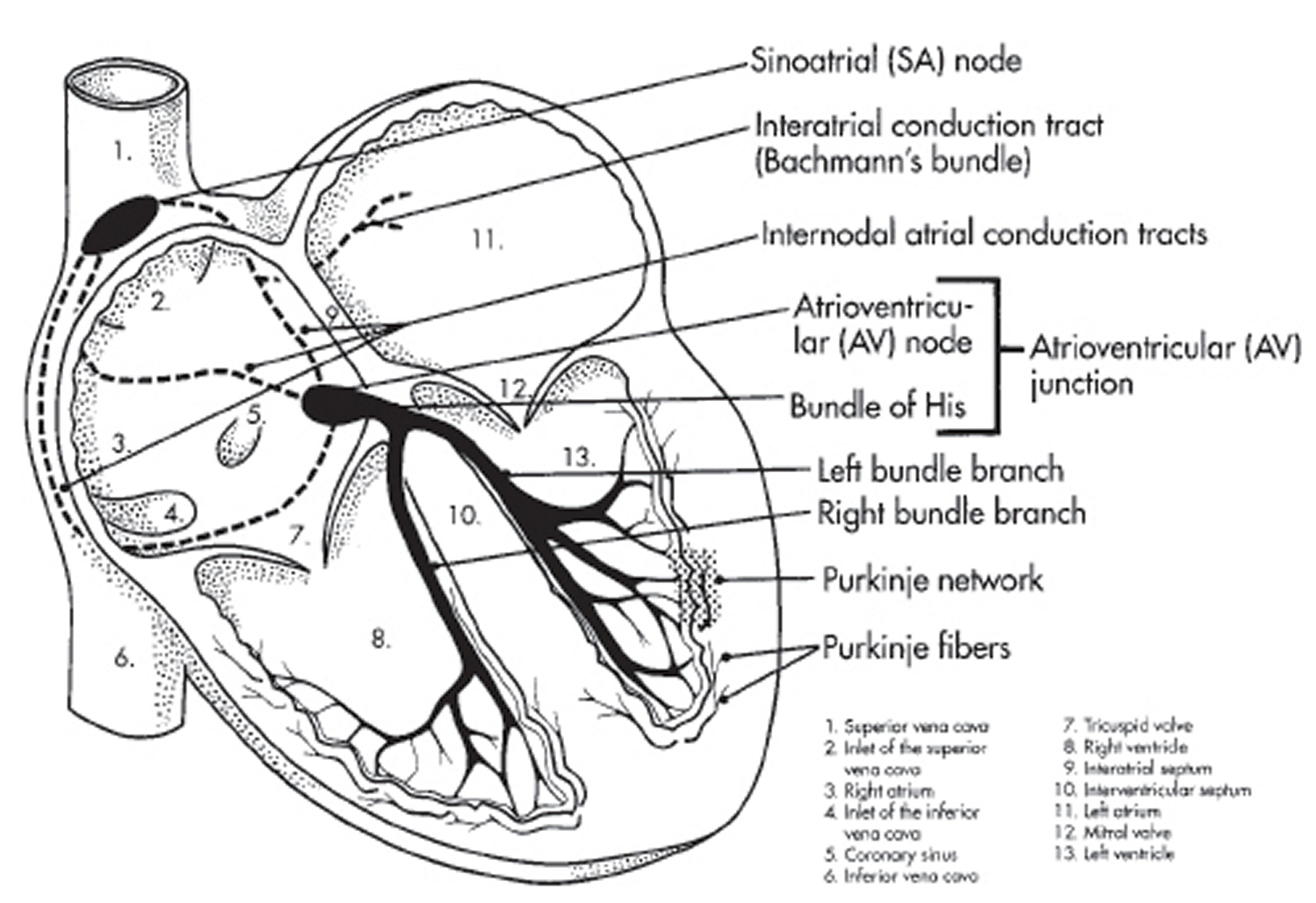
Each normal heartbeat starts in an area of the heart known as the sinus node, located in the upper right chamber of the heart (right atrium). The sinus node sends organized electrical signals through the heart resulting in a perfectly timed, rhythmic heartbeat. In people with atrial fibrillation however, this electrical signal is chaotic, causing the atria to fibrillate (or “quiver”). This typically results in a fast and irregular heartbeat. While some people have no symptoms, others may experience shortness of breath, lightheadedness and fatigue. Depending on your specific medical history and symptoms, your doctor may recommend a cardioversion to return your heart to normal sinus rhythm.
Scheduled cardioversion procedures may be done in a hospital or other health care facility by cardiologists, or doctors who specialize in the heart. While the procedure takes only a few minutes, it requires that you arrive a few hours before the procedure. To prepare, you will be given anesthesia through an intravenous (IV) line in your arm to make you fall asleep, and you will have electrodes placed on your chest and possibly your back. These electrodes will be attached to the cardioversion machine. The machine will record your heart’s electrical activity and send the shocks to your heart. When ready, the doctor will send one or more brief, low-energy shocks to your heart to restore a normal rhythm. You will not feel any pain from the shocks.
You will need to stay for a few hours after your procedure. During this time, your health care team will monitor your heart rhythm and blood pressure closely and watch for complications. You will need a ride home because of the medicines or anesthesia you received. You may have some redness or soreness where the electrodes were placed. You also may have slight bruising where the IV line was inserted in your arm.
Watch the below video to find out what to expect.
Figure 1. The heart’s electrical system

Reasons for having a cardioversion
Cardioversion can correct a heartbeat that’s too fast (tachycardia) or irregular (fibrillation). Cardioversion is usually used to treat people who have atrial fibrillation or atrial flutter. These conditions occur when the electrical signals that normally make your heart beat at a regular rate don’t travel properly through the upper chambers of your heart.
Cardioversion is performed when your heart is beating ineffectively. It’s usually scheduled in advance but is sometimes also done in emergency situations.
Cardioversion is usually done with electric shocks, administered through electrodes attached to your chest, while you’re sedated. Electric cardioversion takes less time than cardioversion done solely with medications, and your doctor can instantly see if the procedure has restored a normal heartbeat.
If your doctor recommends cardioversion with medications to restore your heart’s rhythm, you won’t receive electric shocks to your heart.
Cardioversion is different from defibrillation, an emergency procedure that’s performed when your heart stops or quivers uselessly. Defibrillation delivers more powerful shocks to the heart to correct its rhythm.
Types of cardioversion
Chemical cardioversion
Antiarrhythmic medications can be used to restore the heart’s normal rhythm. Antiarrhythmic medications work by altering the flow of electricity through the heart. Depending on severity of symptoms, underlying heart disease and the specific medication to be used, the chemical conversion may be done as an outpatient, or in the hospital under monitoring.
Cardioversion using drugs is most often used for people with atrial fibrillation that comes and goes. However, you will need to be closely followed-up by a cardiologist.
You may be given blood thinning medicines to prevent blood clots from forming and leaving the heart (which can cause a stroke).
Electrical cardioversion
Electric cardioversion, is done with a device that gives off an electrical shock to the heart to change the rhythm back to normal. Electric cardioversion is also known as “direct-current” or DC cardioversion, a synchronized (perfectly timed) electrical shock is delivered through the chest wall to the heart through special electrodes or paddles that are applied to the skin of the chest and back. The goal of the procedure is to disrupt the abnormal electrical circuit(s) in the heart and thereby to reset the heart to normal rhythm. This split second interruption of the abnormal beat allows the heart’s electrical system to regain control and restore a normal heartbeat. Electrical cardioversion is performed in a hospital setting where oxygen levels, blood pressure and heart rhythm are closely monitored.
Normal sinus rhythm can be restored more than 90 percent of the time, however atrial fibrillation or other abnormal rhythms may recur in over time. Your doctor may prescribe medications or recommend catheter ablation to reduce the risk of atrial fibrillation recurrence.
Electric cardioversion will be used when the abnormal heart rhythm cannot be controlled with medicine.
- Some people may need to start blood thinners beforehand to prevent small blood clots.
- You will be given medicine to help you relax before the procedure.
- After the procedure, you may be given medicines to prevent blood clots or to help prevent the arrhythmia from coming back.
An implantable cardioverter-defibrillator (ICD) is a device that is placed inside your body. It is most often used in people who are at risk for sudden death because their heart function is so poor, or they have had dangerous heart rhythms before.
- The implantable cardioverter-defibrillator (ICD) is implanted underneath the skin of your upper chest or abdomen.
- Wires are attached that go into or near the heart.
- If the device detects a dangerous heartbeat, it sends an electrical shock to the heart to change the rhythm back to normal.
Synchronized cardioversion
Synchronized cardioversion is a procedure similar to electrical defibrillation (direct-current cardioversion), in that a transthoracic electrical current is applied to the anterior chest to terminate a life-threatening or unstable tachycardic arrhythmia 1. Unlike defibrillation, which is used in cardiac arrest patients, synchronized cardioversion is performed on patients that still have a pulse but are hemodynamically unstable. It is used to treat both hemodynamically unstable ventricular and supraventricular rhythms.
Each year almost 350,000 Americans die from heart disease. Half of these will die suddenly, outside of a hospital because of the sudden cessation of spontaneous, organized cardiac function. The most common cause of sudden cardiac arrest in adults is pulseless ventricular tachycardia (VT) or ventricular fibrillation (VF). Ventricular tachycardia (VT) can also occur in the presence of a pulse; often it is the precursor to ventricular fibrillation (VF). Ventricular tachycardia (VT) is characterized by rapid, wide (greater than 0.12 seconds) QRS complexes.
Supraventricular tachycardia (SVT) refers to a cardiac rhythm greater than 100 beats per minute, which originates above the bundle of His. Supraventricular tachycardia (SVT) is characterized by rapid, narrow (less than 0.12 seconds wide) QRS complexes. Any tachycardic rhythm that does not originate in the ventricles is referred to as SVT. This includes sinus tachycardia, junctional tachycardia, reentrant tachycardias, multiple atrial tachycardia, atrial fibrillation, and atrial flutter. Although various supraventricular rhythms can cause supraventricular tachycardia (SVT), clinically, they are treated with the same approach.
Indications for synchronized cardioversion
Ventricular tachycardia (VT) can be caused by coronary artery disease, hypertension, valvular heart disease, and cardiomyopathy. It can also be induced by a blow to the chest (Commotio Cordis).
Supraventricular tachycardia (SVT) is usually caused by the repetitive “re-entry“ of the electrical impulse proximally, instead of propagating distally through the cardiac conduction system, due to blockages in the heart’s electrical conduction system. It can also be seen as the result of premature atrial or ventricular beats, cardiac stimulants, thyroid conditions, valvular and coronary artery disease, and as the result of digoxin toxicity.
Contraindications for synchronized cardioversion
There are no contraindications to synchronized cardioversion. The presence of a pacemaker or automated implanted cardiac defibrillator does not change the indication or performance of the procedure.
Synchronized cardioversion equipment
A monitor and defibrillator with synchronized function.
Synchronized cardioversion procedure
Under the American Heart Association’s advanced cardiovascular life support (ACLS) guidelines, the identification and treatment strategies for all tachycardic rhythms involve three simple, rapid decision points. First is the identification of the rhythm as tachycardic.
Next, the tachycardic rhythm is divided into one of two categories depending on the width of the QRS complex: (1) wide-complex tachycardia (QRS width greater than 0.12 seconds) or (2) narrow-complex tachycardia (QRS width less than 0.12 seconds). All narrow-complex tachycardias are considered to be supraventricular in origin and are referred to as supraventricular tachycardias (SVTs). Although wide-complex tachycardic rhythms can occur from sites above the ventricles (such as in supraventricular rhythms with a bundle branch block or other aberrant conduction), clinically, especially during emergent situations, wide-complex tachycardia is usually treated as ventricular in origin, as it is the most potentially life-threatening condition.
The treatment of all emergent tachycardic rhythms, whether narrow-complex or wide-complex depends on the third and final clinical determination: the presence or absence of a pulse. Pulseless rhythms are treated under the American Heart Association’s advanced cardiovascular life support (ACLS) cardiac arrest algorithms: a wide-complex tachycardia would be considered to be pulseless ventricular tachycardia, which is treated the same as VF, under the VF algorithm. A narrow-complex tachycardia would be considered to be a pulseless supraventricular tachycardia (SVT) and is treated under the PEA (Pulseless Electrical Activity) algorithm.
In the presence of a pulse, the specific treatment for all tachycardic rhythms depends on one final determination: whether the pulse being generated is allowing the patient to be considered stable or unstable. In stable patients, the treatment for the underlying arrhythmia is usually medication. For the unstable patient, the treatment of choice is electricity. All tachycardic rhythms, whether wide or narrow complex, are considered to be unstable if the patient also has chest pain, dyspnea, altered mental status, hypotension, pulmonary edema, or ischemic changes on the EKG. The treatment for all unstable tachycardic rhythms is synchronized cardioversion.
Like defibrillation, synchronized cardioversion delivers a shock across the chest, either by placing a pair of manual paddles on the chest or through the application of adhesive “hands-free” pads. Most current defibrillators utilize a biphasic waveform that allows for a lower energy level to be used to achieve effective cardioversion. Because of their greater ability to terminate ventricular dysrhythmias, defibrillators utilizing biphasic waveforms are preferred to those utilizing the older, monophasic waveform.
Synchronized cardioversion differs from defibrillation in two aspects: (1) the amount of energy needed to convert the rhythm is usually less than that required for defibrillation and (2) the shock is delivered in a different part of the cardiac cycle.
When a patient is defibrillated, the energy is released through the paddles or hands-free pads immediately when the defibrillation button/s are pressed. The shock is delivered at whatever point the cardiac cycle happens to be in at that moment. If an electrical shock is provided during the relative refractory period (corresponding to the latter part of the T wave), it is possible to induce VF (the so-called “R-on-T Phenomenon”). This would result in a patient who originally had a pulse being put into cardiac arrest.
To avoid inducing cardiac arrest in a patient with a pulse, synchronized cardioversion is performed instead of defibrillation when a patient is in an SVT with a pulse but is considered unstable according to the definition above. To perform synchronized cardioversion, the defibrillator is placed into the “synchronize” mode by pressing the appropriate button on the machine. This causes the monitor to track the R wave of each QRS complex that goes by. A synchronizing marker will appear above each QRS complex, indicating that the synchronize feature is active.
The appropriate energy level is then selected, and the discharge/shock button is pressed and held. The defibrillator does not release the shock immediately. Instead, it waits for the next R-wave to appear and delivers the shock at the time of the R-wave. This allows the shock to be provided safely away from the T wave, avoiding the R-on-T phenomenon.
The recommended energy levels used to perform synchronized cardioversion vary from 50 to 200 joules. Recalling the specific energy level for a particular sub-type of unstable tachycardia is difficult, especially in an emergent situation. The safest and easiest recommendation is to start at the lowest energy level (50 joules) and if the shock is unsuccessful, double the amount of energy used. In a refractory case, you will be at 200 joules after just three shocks.
Synchronized cardioversion complications
- If a patient with unstable supraventricular tachycardia (SVT) were to lose his or her pulse at any point, treatment would default to the American Heart Association’s advanced cardiovascular life support (ACLS) algorithm for PEA (Pulseless Electrical Activity).
- If a patient with unstable ventricular tachycardia (VT) with a pulse were to lose his or her pulse at any point, treatment would default to the American Heart Association’s advanced cardiovascular life support algorithm for ventricular fibrillation (VF).
- If a patient were to develop ventricular fibrillation (VF), the monitor/defibrillator needs to be taken out of the “synchronize” mode, as defibrillation will not be possible while the machine is searching for a QRS complex.
Cardioversion risks
Although uncommon, cardioversion has some risks. It can cause or worsen life-threatening arrhythmias that will need to be treated. Cardioversion procedure can cause blood clots to break away and travel from the heart to other tissues or organs and cause a stroke or other problems. Taking anticlotting medicines before and after cardioversion can reduce this risk.
Major risks of cardioversion include:
- Dislodged blood clots. Some people who have irregular heartbeats have blood clots in their hearts. Electric cardioversion can cause these blood clots to move to other parts of your body. This can cause life-threatening complications, such as a stroke or a blood clot traveling to your lungs (pulmonary embolism). If necessary, your doctor may prescribe blood-thinning medications before the procedure or will check for blood clots in your heart before cardioversion.
- Abnormal heart rhythm. In rare cases, some people who undergo cardioversion end up with other heart rhythm problems during or after their procedure. This is a rare complication. If it happens, it usually shows up only minutes after your procedure, so your doctor can give you medications or additional shocks to correct the problem.
- Skin burns. Rarely, some people have minor burns on their skin where their electrodes were placed.
Pregnant women can have cardioversion, but it’s recommended that the baby’s heartbeat is monitored during the procedure.
Blood clots and anticoagulation
Because the upper chambers of the heart are fibrillating (quivering) rather than squeezing in people with atrial fibrillation, there is a risk that blood clots may form. The process of restoring a normal rhythm could dislodge a blood clot from the heart resulting in a stroke.
To help prevent blood clots and reduce the potential for stroke, the blood is thinned with medications called anticoagulants. Anticoagulant medications include aspirin, heparin, and warfarin.
In a patient with atrial fibrillation (A Fib) or atrial flutter (AFL) that has been present for more than 48 hours, the blood must be adequately thinned for at least 3-4 weeks prior to the procedure. Alternatively a transesophageal echocardiogram (TEE) can be performed to make sure there is no blood clot in the atrium. During a transesophageal echocardiogram, a special probe is placed in the esophagus which allows your doctor to directly visualize the atria. Because it takes many hours for blood clots to form, cardioversion can be safely performed without blood-thinning medication in patients who have been in an atrial arrhythmia for less than 48 hours.
Typically, anticoagulation is continued after the cardioversion for a minimum of 4 weeks, often longer.
Cardioversion complications
Complications aren’t common and if you experience any side effects after the cardioversion, they will usually be temporary.
Complications of cardioversion are uncommon, but may include:
- Allergic reactions from medicines used
- Blood clots that can cause a stroke or other organ damage
- Bruising, burning, or pain where the electrodes were used
- Worsening of the arrhythmia
- People who perform external cardioversion may be shocked if the procedure is not done correctly. This can cause heart rhythm problems, pain, and even death.
After your cardioversion, you may get headaches and dizziness from a drop in your blood pressure. You may also feel a small amount of discomfort in your chest where the shock was given. Feeling sick is also a common side effect of an anaesthetic.
Cardioversion success rate
Cardioversion doesn’t always restore normal heart rhythm. Sometimes electrical cardioversion is successful to start with, but then your abnormal heart rhythm could come back several days, weeks or even months later. If this happens, your doctor may want to repeat the electrical cardioversion or they may consider another treatment for you.
Normal sinus rhythm can be restored more than 90 percent of the time, however atrial fibrillation or other abnormal rhythms may recur in over time. Your doctor may prescribe medications or recommend catheter ablation to reduce the risk of atrial fibrillation recurrence.
To keep your heart healthy, you may need to make lifestyle changes that improve the overall health of your heart, especially to prevent or treat conditions that can cause arrhythmias, such as high blood pressure. Your doctor may suggest that you:
- Avoid or limit caffeine and alcohol.
- Use less salt (sodium), which can help lower blood pressure.
- Increase your physical activity.
- Quit smoking.
- Eat heart-healthy foods and maintain a healthy weight.
- Try to limit or manage stress and anger.
Cardioversion procedure
How you prepare
Cardioversion procedures are usually scheduled in advance, although if your symptoms are severe, you may need to have cardioversion in an emergency setting.
You typically can’t eat or drink anything for about 8 hours before your procedure. Your doctor will tell you whether you should take any of your regular medications before your procedure. If you do take medications before your procedure, sip only enough water to swallow your pills.
Before cardioversion, you may have a procedure called a transesophageal echocardiogram (TEE) to check for blood clots in your heart, which can be dislodged by cardioversion, causing life-threatening complications. Your cardiologist will decide if you need a transesophageal echocardiogram before cardioversion.
In a transesophageal echocardiogram, your throat is numbed and a flexible tube containing a transducer is guided down your throat and into your esophagus, which connects your mouth to your stomach. From there, the transducer can obtain more-detailed images of your heart so that your doctor can check for blood clots.
If your doctor finds blood clots, your cardioversion procedure will be delayed for three to four weeks while you take blood-thinning medications to reduce your risk of complications.
During the electrical cardioversion procedure
A nurse or technician will place several large patches called electrodes on your chest. The electrodes will be connected to a cardioversion machine (defibrillator) using wires.
The defibrillator will record your heart rhythm throughout the procedure and will deliver shocks to your heart to restore a normal heart rhythm. This machine can also correct your heart’s rhythm if it beats too slowly after cardioversion.
Before the shocks are delivered, a nurse or technician will insert an intravenous (IV) line in your arm. The IV line is used to give you medications that will make you sleep during the procedure so that you won’t feel any pain from the shocks. Your doctor may also use the IV line to give you additional medications that can help restore your heart rhythm.
Once you’re sedated, electric cardioversion usually only lasts about 10 minutes.
During electrical cardioversion procedure:
- you’ll be given a short-acting general anaesthetic or heavy sedation so you will be asleep throughout
- a doctor or nurse will put electrodes, stuck to large sticky pads, on your chest
- the electrodes are connected to a defibrillator machine and will give you one or more controlled electric shocks to your chest wall
- the defibrillator monitors your heart rhythm throughout the procedure so the medical staff can see straight away if the cardioversion was successful.
After the electrical cardioversion procedure
Electric cardioversion is done on an outpatient basis, meaning you can go home the same day your procedure is done. You’ll spend an hour or so in a recovery room being closely monitored for complications.
Because you’ll be asleep for the procedure, your awareness of your surroundings may be affected afterward. You’ll need someone to drive you home, and your ability to make decisions may be affected for several hours after your procedure.
Even if no clots were found in your heart before your procedure, you’ll take blood-thinning medications for at least several weeks after your procedure to prevent new clots from forming.
Cardioversion recovery
You should be able to return to normal activities after about 2 days.
Do not drink alcohol or caffeine.
Regular exercise should improve your long-term health. Before you start exercising, ask the healthcare team or your doctor for advice.
- Sciammarella JC, Bhimji SS. Cardioversion, Synchronized Electrical. [Updated 2018 Oct 27]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2018 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482173[↩]





{kind=link}