Contents
What is the Epley maneuver
The Epley maneuver is used to treat benign paroxysmal positional vertigo (BPPV) by repositions the canalith from the semicircular canal into the vestibule 1. The success rate of the Epley maneuver is approximately 70% on the first attempt, and nearly 100% on successive maneuvers 2.
BPPV (benign paroxysmal positional vertigo) occurs when loose otoconia, known as canaliths, become dislodged and enter the semicircular canals, usually the posterior canal 3.
Inner ear anatomy
You rely on the inner ear, an intricate sensory organ, to hear and to maintain balance. The inner ear is a complex system of communicating chambers and tubes called a labyrinth. Each ear has two parts to the labyrinth—the bony (osseus) labyrinth and the membranous labyrinth (Figure 1). The bony labyrinth is a cavity within the temporal bone. The membranous labyrinth is a tube of similar shape that lies within the bony labyrinth. Between the bony and membranous labyrinths is a fluid called perilymph, which is secreted by cells in the wall of the bony labyrinth. The membranous labyrinth contains another fluid, called endolymph.
The parts of the labyrinths include three membranous semicircular ducts within three bony semicircular canals, and a cochlea. The semicircular canals and associated structures provide a sense of equilibrium (balance). The cochlea functions in hearing.
The vestibular system monitors the motion and position of the head in space by detecting angular and linear acceleration. The 3 semicircular canals in the inner ear detect angular acceleration and are positioned at near right angles to each other (Figure 2). Each canal is filled with endolymph and has a swelling at the base termed the “ampulla” (Figure 3). The ampulla contains the “cupula,” a gelatinous mass with the same density as endolymph, which in turn is attached to polarized hair cells. Movement of the cupula by endolymph can cause either a stimulatory or an inhibitory response, depending on the direction of motion and the particular semicircular canal. It should be noted that the cupula forms an impermeable barrier across the lumen of the ampulla, therefore particles within the semicircular canal may only enter and exit via the end with no ampulla 4.
Sense of Equilibrium
The sense of equilibrium (balance) is really two senses:
- Static equilibrium and
- Dynamic equilibrium—that come from different sensory organs.
The organs of static equilibrium sense the position of the head, maintaining balance, stability and posture when the head and body are still. When the head and body suddenly move or rotate, the organs of dynamic equilibrium detect such motion and aid in maintaining balance.
Figure 1. Inner ear anatomy

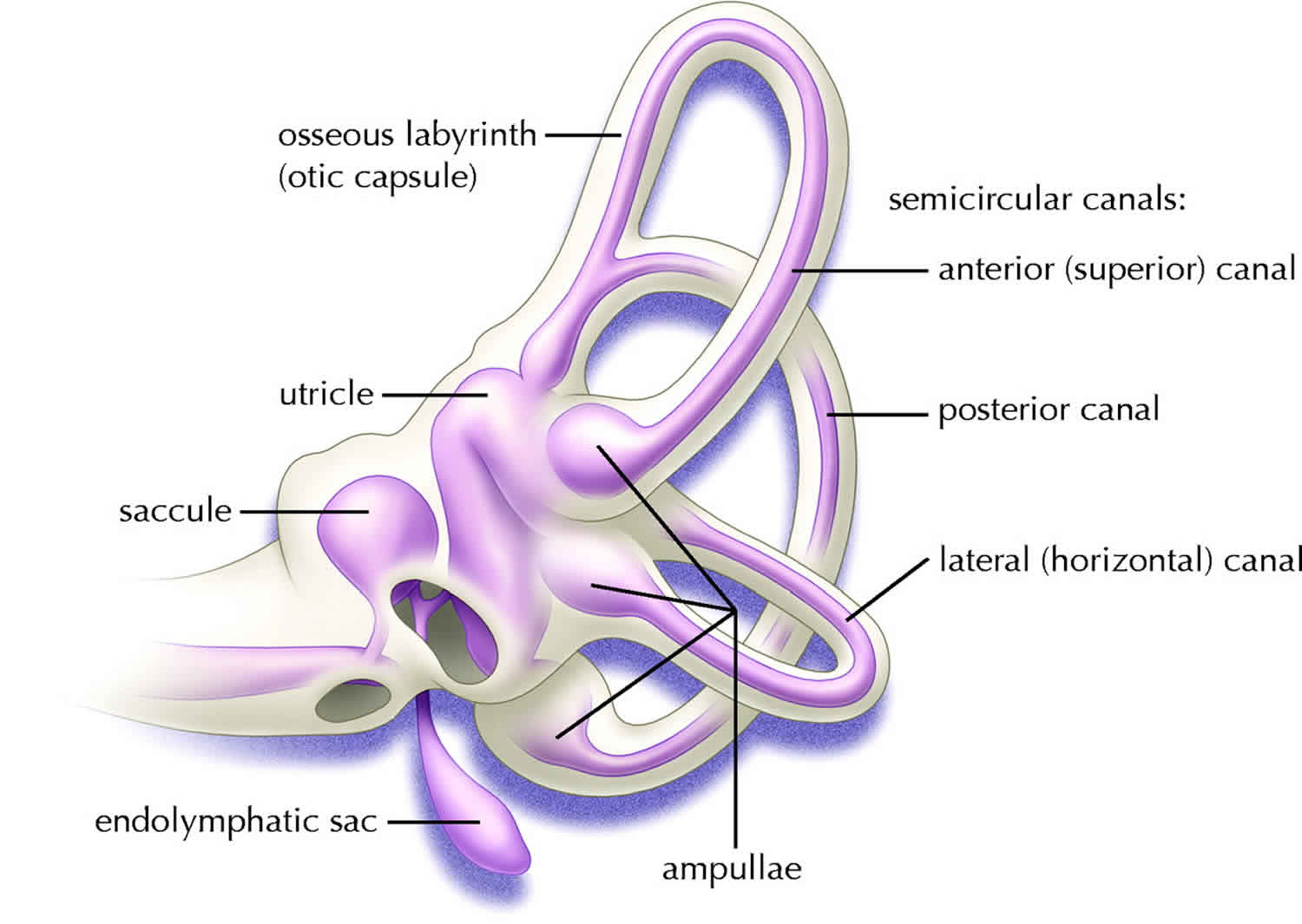
Figure 2. Parts of the inner ear
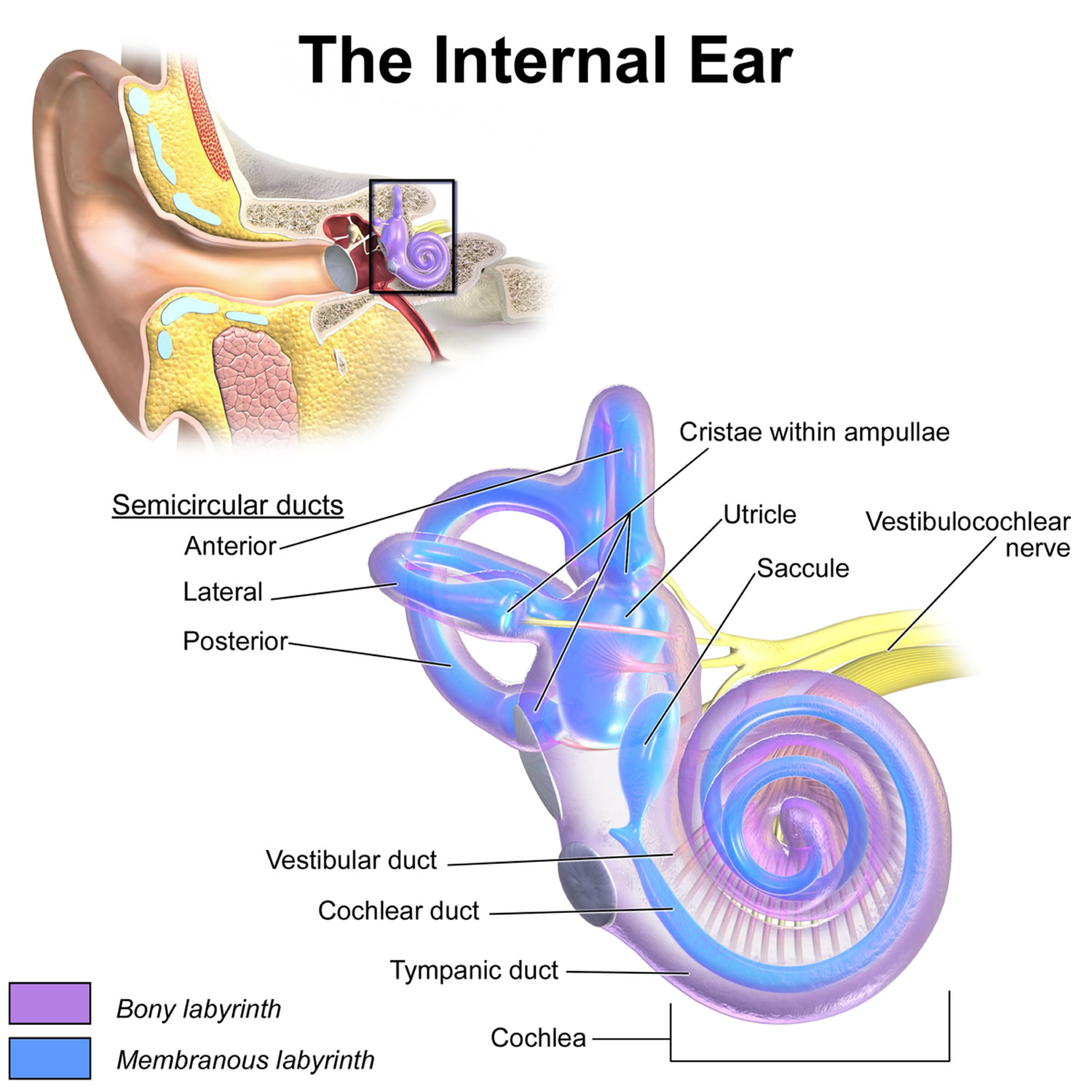
Figure 3. Semicircular canals
 Footnote: Osseous (grey/white) and membranous (lavender) labyrinth of the left inner ear. Perilymph fills the osseous labyrinth external to the membranous labyrinth, whereas endolymph fills the membranous labyrinth.
Footnote: Osseous (grey/white) and membranous (lavender) labyrinth of the left inner ear. Perilymph fills the osseous labyrinth external to the membranous labyrinth, whereas endolymph fills the membranous labyrinth.Dynamic Equilibrium
The organs of dynamic equilibrium are the three semicircular canals in the labyrinth. They detect motion of the head and aid in balancing the head and body during sudden movement. These semicircular canals lie at right angles to each other (see Figure 2).
Suspended in the perilymph of the bony portion of each semicircular canal is a membranous semicircular duct that ends in a swelling called an ampulla, which
houses the sensory organs of the semicircular canals. Each of these sensory organs, called a crista ampullaris, contains a number of sensory hair cells and supporting cells. Like the hairs of the maculae, the hair cells of the crista ampullaris extend upward into a dome-shaped, gelatinous mass called the cupula (Figure 4). When the head is stationary, the cupula of the crista ampullaris remains upright. When the head is moving rapidly, the cupula bends opposite the motion of the head, stimulating sensory receptors.
Rapid movement of the head or body stimulates the hair cells of the crista ampullaris (Figure 4). At such times, the semicircular canals move with the head or body, but the fluid inside the membranous ducts remains stationary. Imagine turning rapidly while holding a full glass of water. This action bends the cupula in one or more of the canals in a direction opposite that of the head or body movement, and the hairs embedded in it also bend. The stimulated hair cells signal their associated neurons, which conduct impulses to the brain. The brain interprets these impulses as a movement in a particular direction.
Parts of the cerebellum are particularly important in interpreting impulses from the semicircular canals. Analysis of such information allows the brain to predict the consequences of rapid body movements. By modifying signals to appropriate skeletal muscles, the cerebellum can maintain balance.
Other sensory structures aid in maintaining equilibrium. For example, certain mechanoreceptors (proprioceptors), particularly those associated with the joints of the neck, inform the brain about the position of body parts. In addition, the eyes detect changes in position that result from body movements. Such visual information is so important that even if the organs of equilibrium are damaged, a person may be able to maintain normal balance by keeping the eyes open and moving slowly.
The nausea, vomiting, dizziness, and headache of motion sickness arise from sensations that don’t make sense. The eyes of a person reading in a moving car, for example, signal the brain that the person is stationary, because the print doesn’t move. However, receptors in the skin detect bouncing, swaying, starting, and stopping as the inner ear detects movement. The contradiction triggers the symptoms. Similarly, in a passenger of an airplane flying through heavy turbulence, receptors in the skin and inner ear register the chaos outside, but the eyes focus on the immobile seats and surroundings.
To prevent or lessen the misery of motion sickness, focus on the horizon or an object in the distance ahead. Medications are available by pill (diphenhydramine and dimenhydrinate) and, for longer excursions, in a skin patch (scopolamine).
Figure 3. Dynamic inner ear balance organs (crista ampullaris) within the Semicricular canals
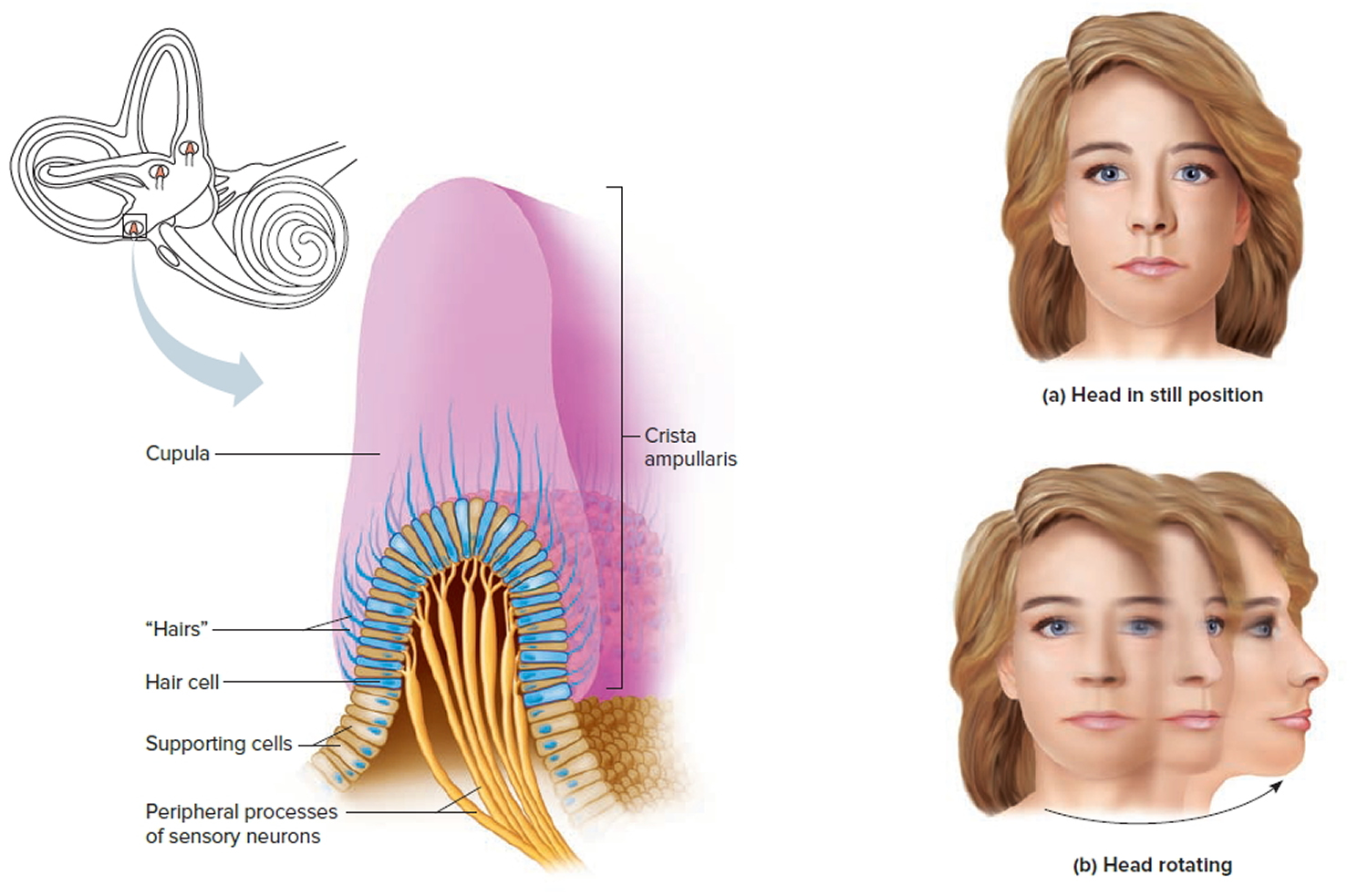
Figure 4. Spatial orientation of the semicircular canals
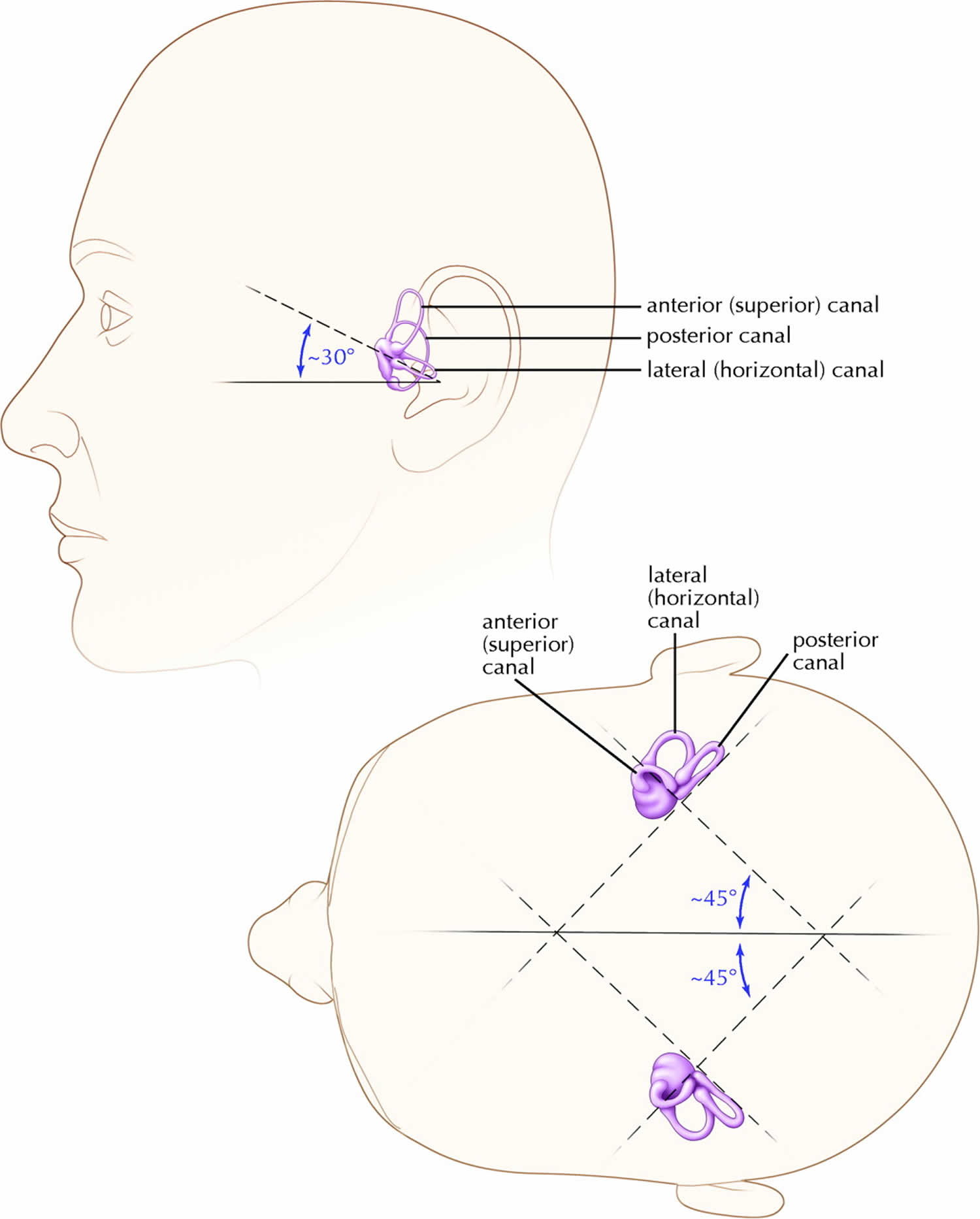
Footnote: Notice how the posterior canal on 1 side is in the same plane as the opposite side superior canal. Both lateral canals are in the same plane, 30 degrees above the horizontal.
[Source 5 ]What is benign paroxysmal positional vertigo (BPPV)?
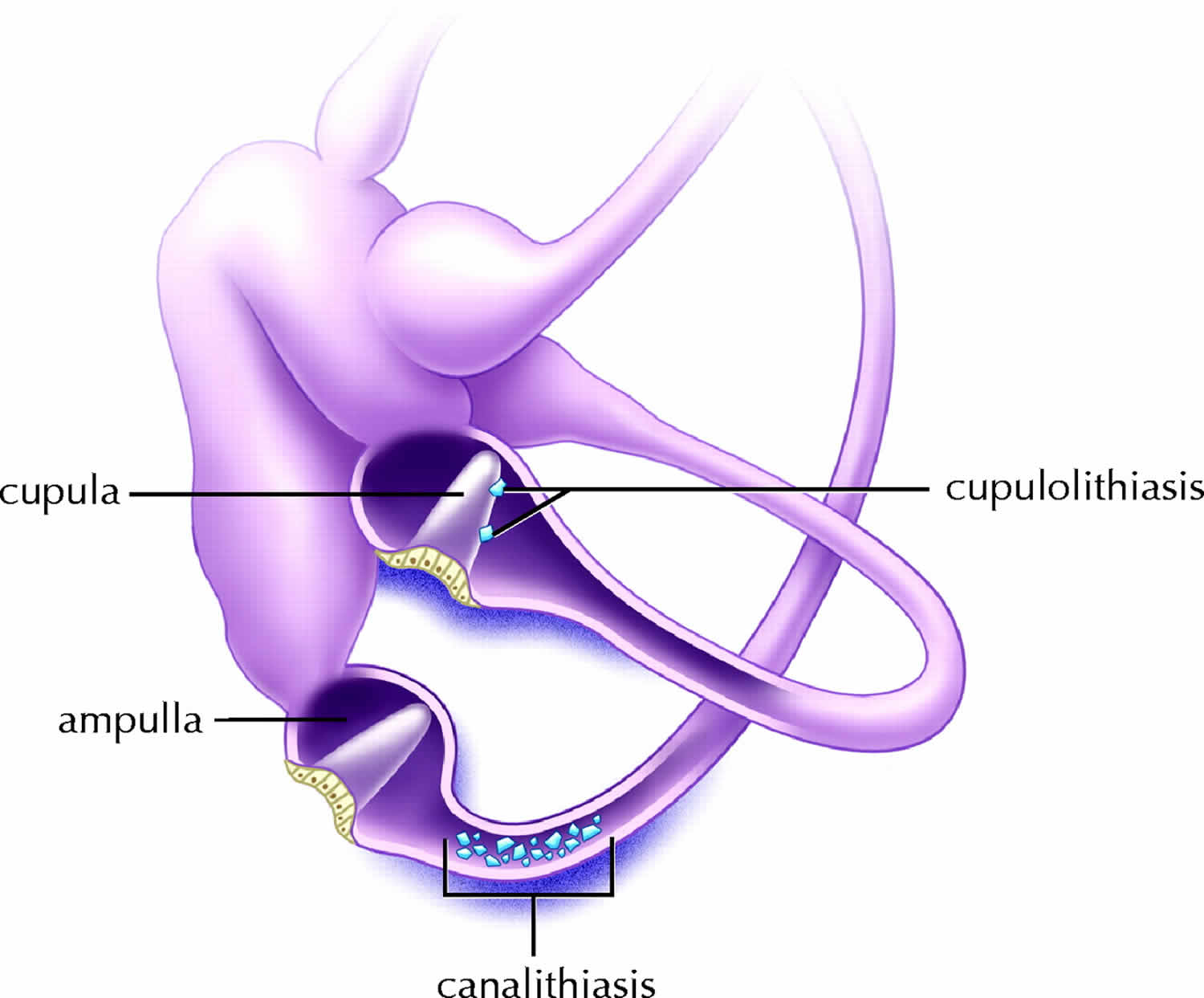
Benign paroxysmal positional vertigo (BPPV) can be caused by either canalithiasis or cupulolithiasis and can theoretically affect each of the 3 semicircular canals, although superior canal involvement is exceedingly rare 5. “Canalithiasis” describes free-floating particles within a semicircular canal (see Figure 5 below). The concept was first described in 1979 by Hall, Ruby and McClure 6 and the phenomenon was first demonstrated in vivo by Parnes and McClure in 1992 7. “Cupulolithiasis” describes particles adherent to the cupula of a semicircular canal (see Figure 5 below). This term was coined by Schuknecht in 1969 8. BPPV (benign paroxysmal positional vertigo) can occur at any age, but is most common between 50 and 70 years 9. No obvious cause is found in 50% to 70% of older patients, but head trauma is a possibility in younger persons 2.
Posterior canal BPPV
The vast majority of all BPPV cases are of the posterior canal variant 5. The pathophysiology that causes most posterior canal BPPV cases is thought to be canalithiasis. This is probably because most free-floating endolymph debris tends to gravitate to the posterior canal, being the most gravity-dependent part of the vestibular labyrinth in both the upright and supine positions. Once debris enters the posterior canal, the cupular barrier at the shorter, more dependent end of the canal blocks the exit of the debris. Therefore, the debris becomes “trapped” and can only exit at the end without the ampulla (the common crus) (Figure 5). Agrawal and Parnes 10 found obvious free-floating endolymph particles in 30% of ears operated on for posterior canal BPPV.
Figure 5. BPPV causes – Left inner ear. Depiction of canalithiasis of the posterior canal and cupulolithiasis of the lateral canal.
The mechanism by which canalithiasis causes nystagmus in the posterior semicircular canal was described by Epley 11. Particles must accumulate to a “critical mass” in the dependent portion of the posterior semicircular canal. The canalith mass moves to a more dependent position when the orientation of the semicircular canal is modified in the gravitational plane. The drag thus created must overcome the resistance of the endolymph in the semicircular canal and the elasticity of the cupular barrier in order to deflect the cupula. The time taken for this to occur plus the original inertia of the particles explains the latency seen during the Dix–Hallpike maneuver (a maneuver to diagnose BPPV).
In the head-hanging position, the canalith mass would move away from the cupula to induce ampullofugal cupular deflection. In the vertical canals, ampullofugal deflection produces an excitatory response. This would cause an abrupt onset of vertigo and the typical “torsional nystagmus” in the plane of the posterior canal. In the left head-hanging position (left posterior canal stimulation), the fast component of the nystagmus beats clockwise as viewed by the examiner. Conversely, the right head-hanging position (right posterior canal stimulation) results in a counter-clockwise nystagmus. These nystagmus profiles correlate with the known neuromuscular pathways that arise from stimulation of the posterior canal ampullary nerves in an animal model 12.
This nystagmus is of limited duration, because the endolymph drag ceases when the canalith mass reaches the limit of descent and the cupula returns to its neutral position. “Reversal nystagmus” occurs when the patient returns to the upright position; the mass moves in the opposite direction, thus creating a nystagmus in the same plane but the opposite direction. The response is fatiguable, because the particles become dispersed along the canal and become less effective in creating endolymph drag and cupular deflection.
Lateral (horizontal) canal BPPV
Although BPPV most commonly affects the posterior semicircular canal, 1 report suggests that up to 30% of BPPV may be of the horizontal canal variant 13. The posterior canal hangs inferiorly and has its cupular barrier at its shorter, more dependent end. Any debris entering the canal essentially becomes trapped within it. In contrast, the lateral canal slopes up and has its cupular barrier at the upper end. Therefore, free-floating debris in the lateral canal would tend to float back out into the utricle as a result of natural head movements.
In lateral canal canalithiasis, particles are most often in the long arm of the canal relatively far from the ampulla. If the patient performs a lateral head turn toward the affected ear, the particles will create an ampullopetal endolymph flow, which is stimulatory in the lateral canal. A geotropic nystagmus (fast phase toward the ground) will be present. If the patient turns away from the affected side, the particles will create an inhibitory, ampullofugal flow. Although the nystagmus will be in the opposite direction, it will still be a geotropic nystagmus, because the patient is now facing the opposite direction. Stimulation of a canal creates a greater response than the inhibition of a canal, therefore the direction of head turn that creates the strongest response (i.e., stimulatory response) represents the affected side in geotropic nystagmus.
Cupulolithiasis is thought to play a greater role in lateral canal BPPV than in the posterior canal variant. As particles are directly adherent to the cupula, the vertigo is often intense and persists while the head is in the provocative position. When the patient’s head is turned toward the affected side, the cupula will undergo an ampullofugal (inhibitory) deflection causing an apogeotropic nystagmus. A head turn to the opposite side will create an ampullopetal (stimulatory) deflection, resulting in a stronger apogeotropic nystagmus. Therefore, turning away from the affected side will create the strongest response. Apogeotropic nystagmus is present in about 27% of patients 13 who have lateral canal BPPV.
Epley maneuver instructions
The Epley maneuver is performed as follows:
- The patient begins in an upright sitting posture, with the legs fully extended and the head rotated 45 degrees towards the affected side.
- The patient is then quickly and passively forced down backwards into a laying down position with the head held approximately in a 20-30 degrees off the end of the examination table (20-30 degrees neck extension) (Dix-Hallpike position) where the affected ear faces the ground.
- The clinician observes the patient’s eyes for “primary stage” nystagmus. The patient remains in this position for approximately 30 seconds (takes about that long for the free-floating particles to settle into the new position).
- The patient’s head is then turned 90 degrees to the opposite direction so that the unaffected ear faces the ground, all while maintaining the 30 degree neck extension. The patient remains in this position for approximately 30 seconds.
- Keeping the head and neck in a fixed position relative to the body, the individual rolls onto their shoulder, rotating the head another 90 degrees in the direction that they are facing. The patient is now looking downwards at a 45 degree angle. The eyes should be immediately observed by the clinician for “secondary stage” nystagmus and this secondary stage nystagmus should beat in the same direction as the primary stage nystagmus. The patient remains in this position for approximately 30 seconds.
- Finally, the patient is slowly brought up to an upright sitting posture, while maintaining the 45 degree rotation of the head. The patient holds sitting position for up to 30 seconds.
The entire procedure may be repeated two more times for a total of three times. During every step of this procedure the patient may experience some dizziness.
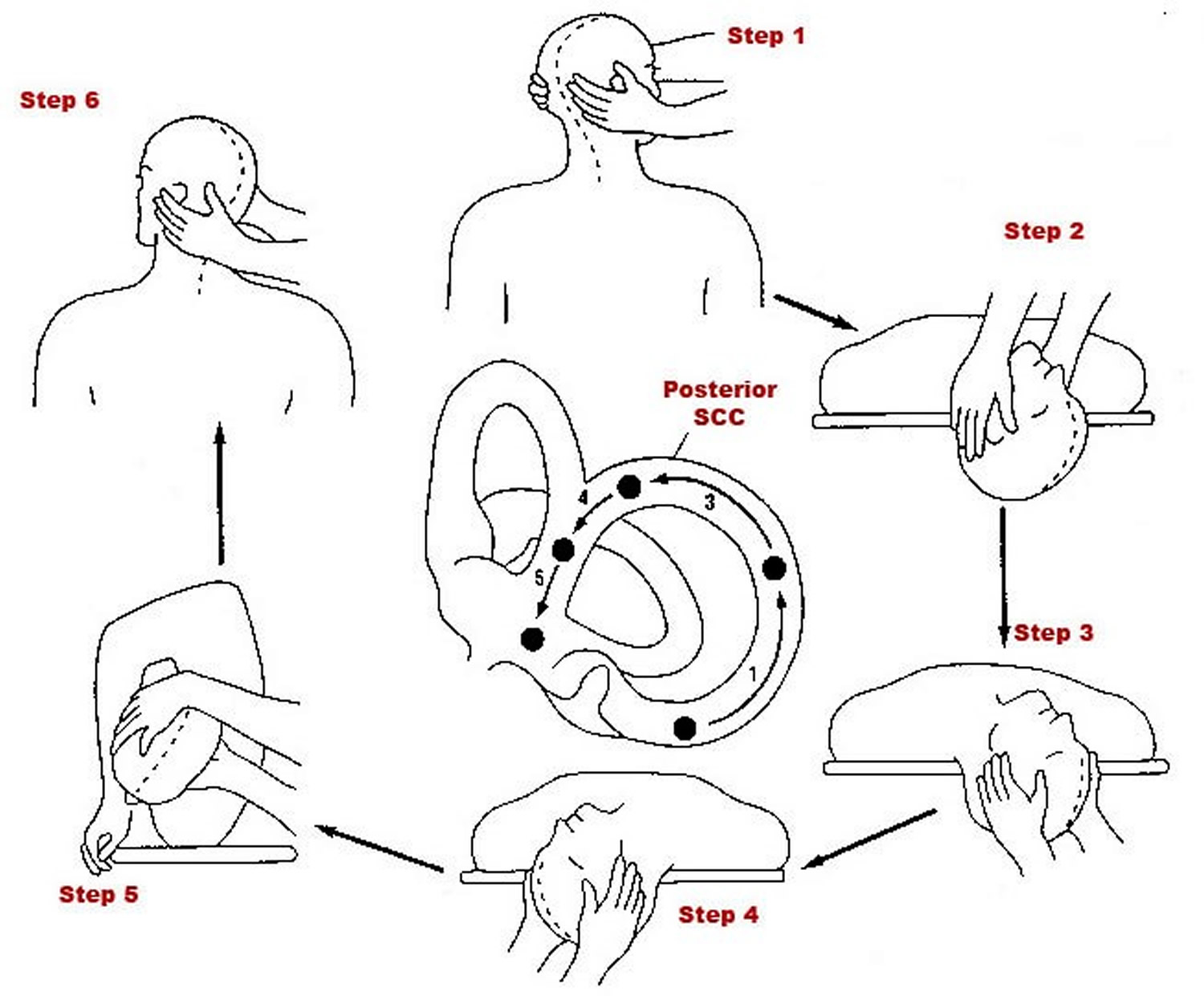
Figure 6. Epley maneuver steps
How to do the Epley maneuver – for Right side BPPV
- Step 1: The patient is placed in the upright position, with eyes open and head turned 45 degrees toward the affected ear (right side)
- Step 2: The patient is then laid back quickly to a position with the head extended below the shoulders, the head hanging 20 degrees off the end of the examination table. If benign paroxysmal positional vertigo (BPPV) is present, nystagmus ensues usually within seconds. The patient is held in the right head hanging 20 degrees off the end of the examination table for 30 seconds
- Step 3: The patient’s head is then turned 90 degrees toward the unaffected side (left side). The patient remains in this position for 30 seconds
- Step 4: The patient’s head is then turned an additional 90 degrees to the left while the patient rotates his or her body 90 degrees in the same direction, so that the head is nearly in the face-down position. The patient remains in this position for 30 seconds.
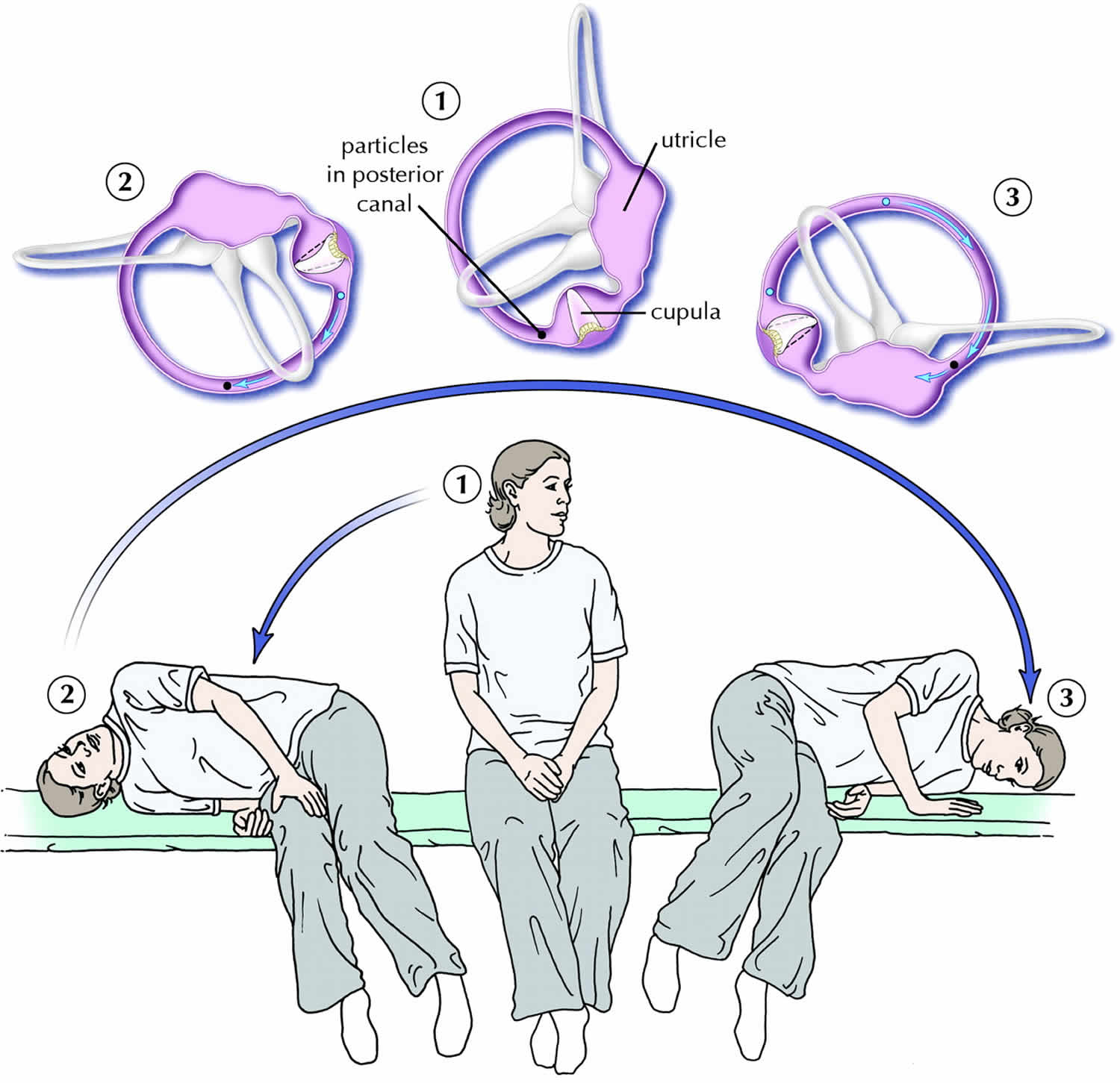
- Step 5: The patient then sits up on the left side of the examination table. The movement of the particles within the labyrinth is depicted with each step, showing how particles are moved from the semicircular canal to the vestibule.
The procedure may be repeated on either side until the patient experiences relief of symptoms.
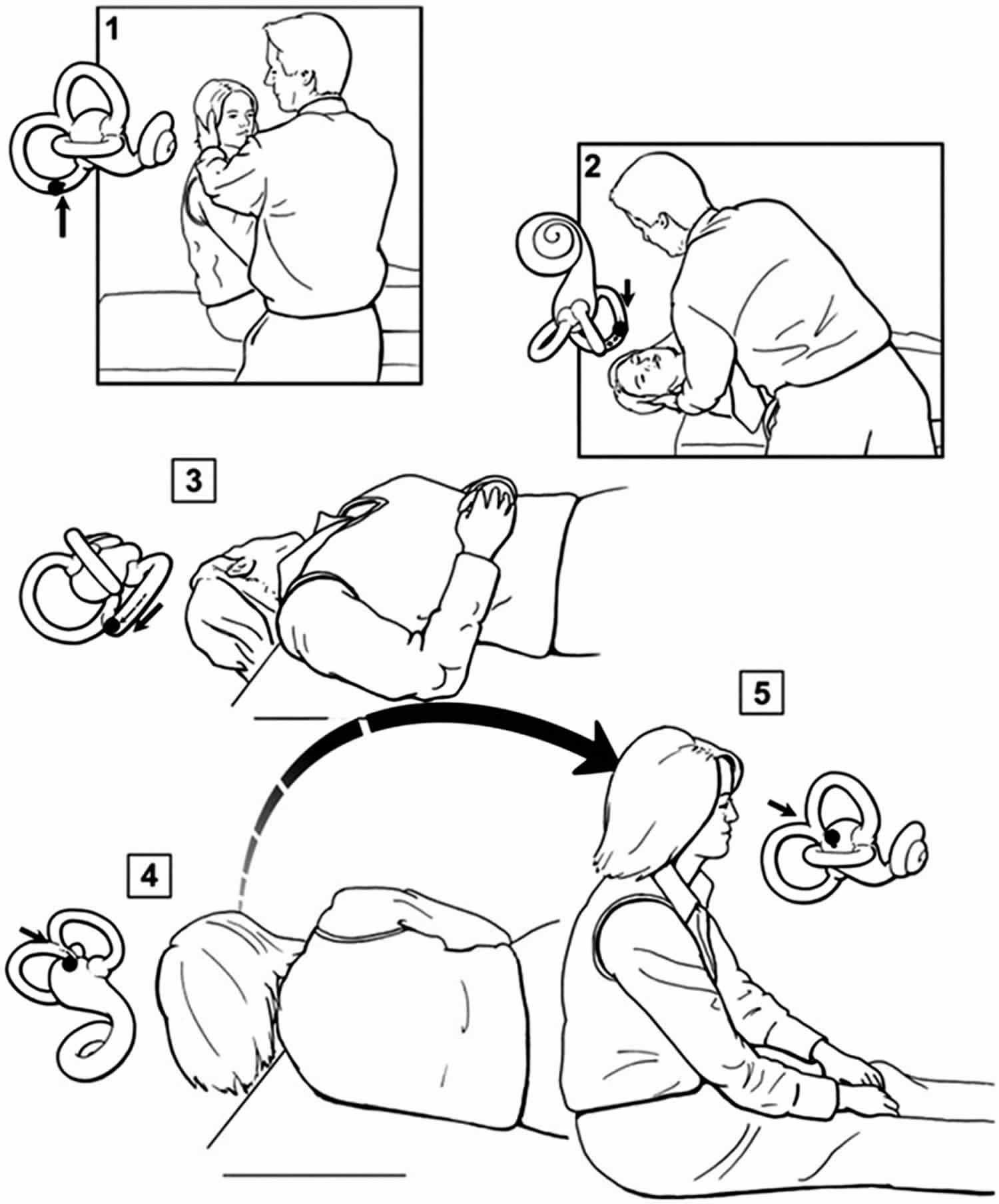
Figure 7. Epley maneuver for right-sided benign paroxysmal positional vertigo (BPPV)
How to do the Epley maneuver – for Left side BPPV
- Step 1: The patient is placed in the upright position, with eyes open and head turned 45 degrees toward the affected ear (left side)
- Step 2: The patient is then laid back quickly to a position with the head extended below the shoulders, the head hanging 20 degrees off the end of the examination table. If benign paroxysmal positional vertigo (BPPV) is present, nystagmus ensues usually within seconds. The patient is held in the left head hanging 20 degrees off the end of the examination table for 30 seconds
- Step 3: The patient’s head is then turned 90 degrees toward the unaffected side (right side). The patient remains in this position for 30 seconds
- Step 4: The patient’s head is then turned an additional 90 degrees to the right while the patient rotates his or her body 90 degrees in the same direction, so that the head is nearly in the face-down position. The patient remains in this position for 30 seconds.
- Step 5: The patient then sits up on the right side of the examination table.
The procedure may be repeated on either side until the patient experiences relief of symptoms.
Epley maneuver side effects
During the Epley maneuver procedure, you may experience:
- Intense vertigo symptoms
- Nausea
- Vomiting (less common)
In a few people, the canaliths may move into another canal in the inner ear and continue to cause vertigo.
Modified Epley maneuver
Particle repositioning maneuver
Although Epley had been teaching his technique for many years, it was not until 1992 that Epley 15 published his first report on the “canalith repositioning procedure” (Epley maneuver). This highly successful “Epley maneuver” is performed with the patient sedated. Mechanical skull vibration is routinely used and the patient’s head is moved sequentially through 5 separate positions. Epley postulated that the procedure enabled the otolithic debris to move under the influence of gravity from the posterior semicircular canal into the utricle. Most clinicians today are thought to use a modified version of the Epley maneuver.
One modified Epley maneuver is the “particle repositioning maneuver” which is a 3-position maneuver that eliminates the need for sedation and mastoid vibration (Figure 8) 16. With proper understanding of inner ear anatomy and the pathophysiology of BPPV, various appropriately trained health professionals, including family doctors and physiotherapists, should be able to successfully carry out the modified Epley maneuver (canalith repositioning procedure) in most straightforward cases. Atypical cases or cases that do not respond to this maneuver should be referred to a tertiary care dizziness clinic.
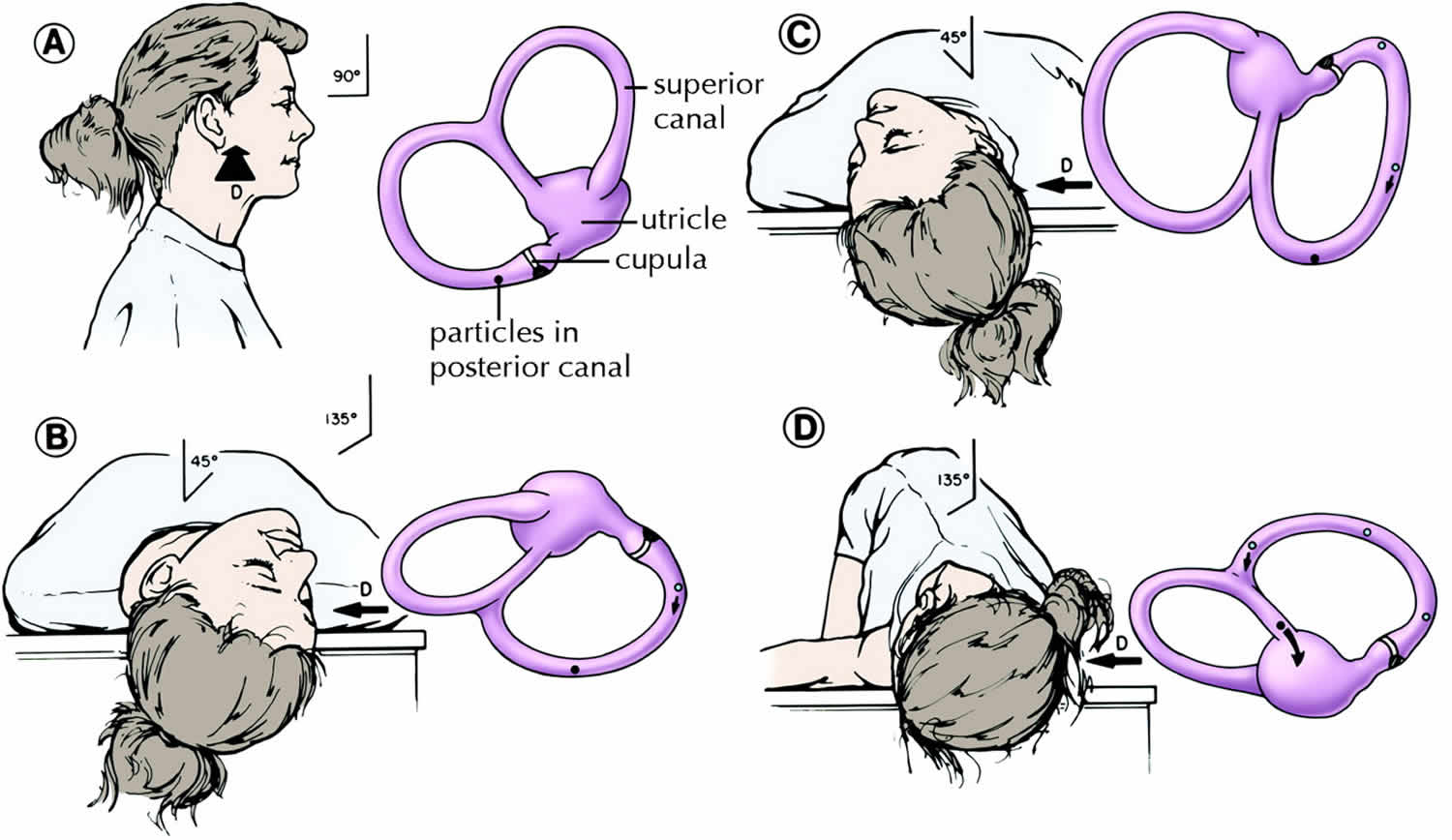
In the modified Epley maneuver (particle repositioning maneuver) 5:
- Place the patient in a sitting position
- Move the patient to the head-hanging Dix–Hallpike position of the affected ear
- Observe the eyes for “primary stage” nystagmus
- Maintain this position for 1–2 minutes (position B)
- The head is turned 90° to the opposite Dix–Hallpike position while keeping the neck in full extension (position C)
- Continue to roll the patient another 90° until his or her head is diagonally opposite the first Dix–Hallpike position (position D). The change from position B, through C, into D, should take no longer than 3–5 seconds
- The eyes should be immediately observed for “secondary stage” nystagmus. If the particles continue moving in the same ampullofugal direction, that is, through the common crus into the utricle, this secondary stage nystagmus should beat in the same direction as the primary stage nystagmus.
- This position is maintained for 30–60 seconds and then the patient is asked to sit up. With a successful manoeuvre, there should be no nystagmus or vertigo when the patient returns to the sitting position because the particles will have already been repositioned into the utricle 17.
Overall, the modified Epley maneuver (particle repositioning maneuver) should take less than 5 minutes to complete. Patients are then typically asked to remain upright for the next 24–48 hours in order to allow the otoliths to settle, so as to prevent a recurrence of the BPPV.
Figure 8. Modified Epley maneuver
Semont Maneuver
An alternative maneuver which may help posterior BPPV is called the Semont or “liberatory maneuver” demonstrated in the image below when the right ear is affected.
- Patient is made to sit on the examination table with legs hanging over the edge and head turned 45 degrees horizontally towards the unaffected ear.
- While maintaining head rotation patient’s upper body is swiftly moved to side lying position on the affected side with head resting on examination table and nose pointed upwards. Position is maintained for 3-5 minutes or till vertigo and nystagmus subsides. This step moves the debris to the apex.
- Patient is rapidly moved through the sitting position (Position 1) to lying on the opposite or unaffected side (maintaining same head rotation) with nose pointed to the ground. Position is again maintained for 3-10 minutes or till the vertigo and nystagmus subsides, before slowly being brought back to the sitting position. This maneuver moves the debris towards exit of the canal.
In their series of 711 patients, Semont and colleagues 18 found an 84% response rate after 1 procedure and a 93% response rate after a second procedure 1 week later. Several other case series have had response rates of 52%–90% 19, with recurrence rates of up to 29% 20. There has been no difference in efficacy shown between the liberatory manoeuvre and particle repositioning manoeuvre, which is described in the following section, in randomized studies by Herdman and colleagues 21 and Cohen and Jerabek 22. The liberatory maneuver of Semont is effective, but is cumbersome with elderly and obese patients, and shows no increased efficacy compared with the simple particle repositioning maneuver (modified Epley maneuver).
Figure 9. Liberatory maneuver of Semont
 [Source 5 ]
[Source 5 ] Foster Half-Somersault
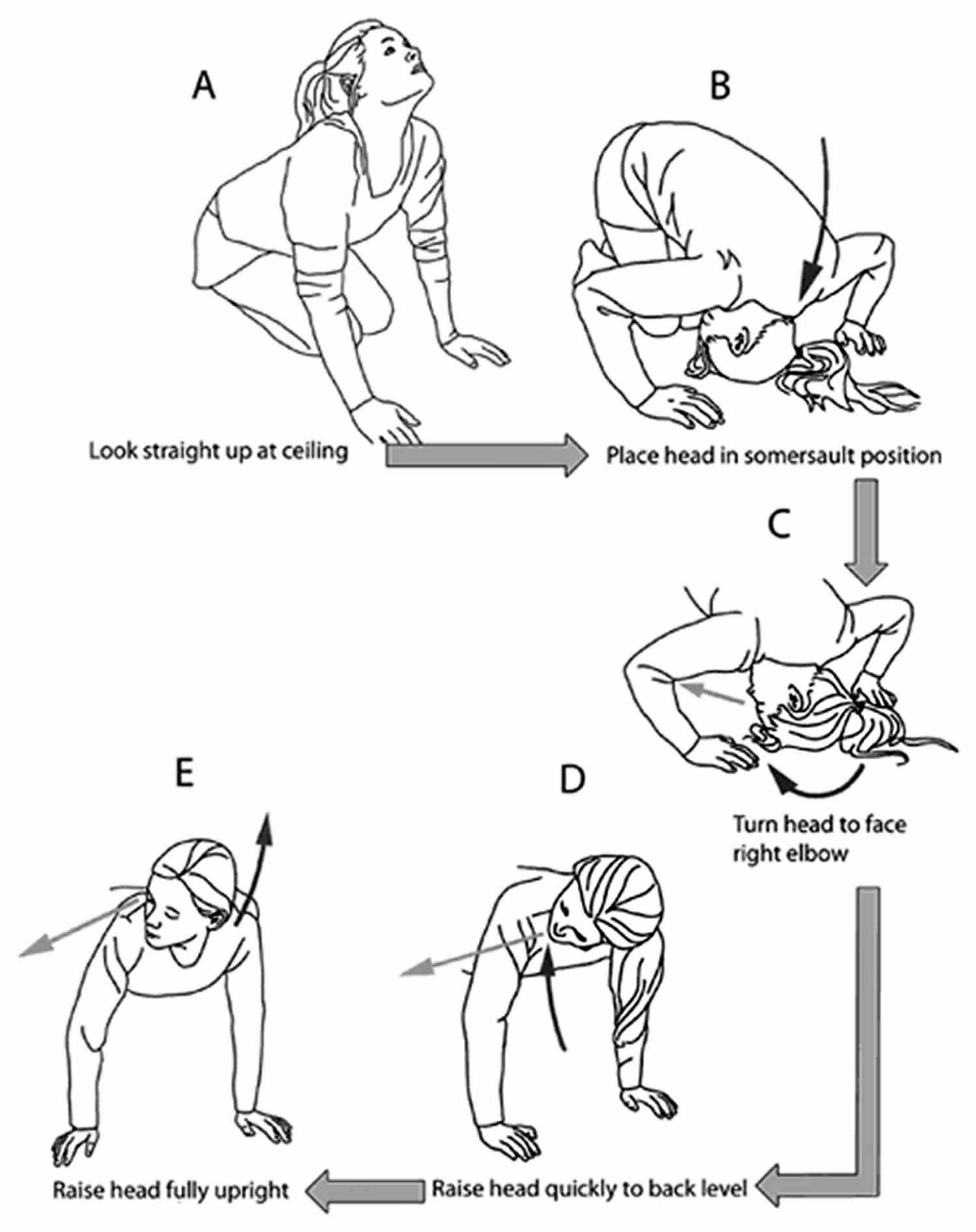
The Foster Half-Somersault is probably the most feasible to perform in situations where laying down is not possible (i.e., at work or in a public place).
Half somersault for right-sided BPPV. After each position change, any dizziness is allowed to subside before moving into the next position; if there is no dizziness, the position should be held for 15 s. (A) While kneeling, the head is quickly tipped upward and back. (B) The somersault position is assumed, with the chin tucked as far as possible toward the knee. (C) The head is turned about 45° toward the right shoulder, to face the right elbow. (D) Maintaining the head at 45°, the head is raised to back/shoulder level. (E) Maintaining the head at 45°, the head is raised to the fully upright position. Dark curved arrows show head movements. Lighter arrows near eyes show the direction one should be facing.
- While kneeling, the head is quickly tipped upward and back.
- The somersault position is assumed, with the chin tucked as far as possible toward the knee.
- The head is turned about 45° toward the right shoulder, to face the right elbow (if the right ear is affected).
- Maintaining the head at 45°, the head is raised to back/shoulder level.
- Maintaining the head at 45°, the head is raised to the fully upright position. Dark curved arrows show head movements. Lighter arrows near eyes show the direction one should be facing.
Figure 10. Foster Half-Somersault maneuver
Brandt-Daroff exercises
Home treatment with Brandt-Daroff exercises can also be successful (see video below). If there is no improvement with repeated repositioning Epley, Semont, or Foster maneuvers, or if atypical or ongoing nystagmus with nausea is present, another cause should be considered 3. Pharmacologic treatment has no role in the treatment of BPPV. Vestibular suppressant medications should be avoided because they interfere with central compensation and may increase the risk of falls 24.
Summary
The whole idea with the Epley, Semont, or Foster maneuver is to move the free-floating particles into the utricle of the inner ear where it will no longer cause vertigo.
- After the Epley, Semont, or Foster maneuver has been completed, it is important to follow post-treatment instructions to maximize the success of resolving the BPPV.
- Sleep semi-recumbent for the next two nights (head at a 45 degree angle). This is most easily done by using a recliner chair or by using pillows arranged on a couch. During the day, try to keep your head vertical and stilll.
- For at least one week, avoid provoking head positions that might bring BPPV on again. Use two pillows when you sleep. Avoid sleeping on the "bad" side. Don’t turn your head far up or far down. Be careful to avoid head-extended positions. This basically means to be cautious at the beauty parlor, dentist’s office, and while undergoing minor surgery where the head is often bent back. Try to stay as upright as possible.
- One week after treatment, no more restrictions are required and hopefully, the dizziness has completely resolved.
- Fife TD, Iverson DJ, Lempert T, et al.; Quality Standards Subcommittee, American Academy of Neurology. Practice parameter: therapies for benign paroxysmal positional vertigo (an evidence-based review): report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology. 2008;70(22):2067–2074.[↩]
- Hilton MP, Pinder DK. The Epley (canalith repositioning) manoeuvre for benign paroxysmal positional vertigo. Cochrane Database Syst Rev. 2014;(12):CD003162.[↩][↩]
- Hornibrook J. Benign paroxysmal positional vertigo (BPPV): history, pathophysiology, office treatment and future directions. Int J Otolaryngol. 2011;2011:835671.[↩][↩]
- Dohlman G. Investigators in the function of the semicurcular canals. Acta Otolaryngol Suppl (Stockh) 1944;51:211.[↩]
- Diagnosis and management of benign paroxysmal positional vertigo (BPPV). Lorne S. Parnes, Sumit K. Agrawal, Jason Atlas. CMAJ Sep 2003, 169 (7) 681-693; http://www.cmaj.ca/content/169/7/681.full[↩][↩][↩][↩][↩][↩][↩]
- Hall SF, Ruby RR, McClure JA. The mechanics of benign paroxysmal vertigo. J Otolaryngol 1979;8(2):151.[↩]
- Parnes LS, McClure JA. Free-floating endolymph particles: a new operative finding during posterior semicircular canal occlusion. Laryngoscope 1992; 102 (9):988-92.[↩]
- Schuknecht HF, Ruby RR. Cupulolithiasis. Adv Otorhinolaryngol 1973;20:434.[↩]
- Parnes LS, Agrawal SK, Atlas J. Diagnosis and management of benign paroxysmal positional vertigo (BPPV). CMAJ. 2003;169(7):681–693.[↩]
- Agrawal SK, Parnes LS. Human experience with canal plugging. Ann N Y Acad Sci 2001;942:300-5.[↩]
- Epley JM. Human experience with canalith repositioning maneuvers. Ann N Y Acad Sci 2001;942:179-91.[↩]
- Cohen B, Suzuki JI, Bender MB. Eye movements from semicircular canal nerve stimulation in the cat. Ann Otolaryngol 1964;73:153-69.[↩]
- Uno A, Moriwaki K, Kato T, Nagai M, Sakata Y. [Clinical features of benign paroxysmal positional vertigo]. Nippon Jibiinkoka Gakkai Kaiho 2001;104:9-16.[↩][↩]
- Kerber KA, Burke JF, Skolarus LE, et al. A prescription for the Epley maneuver: www.youtube.com?. Neurology. 2012;79(4):376-80. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3400093/[↩]
- Epley JM. The canalith repositioning procedure: for treatment of benign paroxysmal positional vertigo. Otolaryngol Head Neck Surg 1992;107:399-404.[↩]
- Parnes LS, Robichaud J. Further observations during the particle repositioning maneuver for benign paroxysmal positional vertigo. Otolaryngol Head Neck Surg 1997;116: 238-43.[↩]
- Parnes LS, Price-Jones RG. Particle repositioning maneuver for benign paroxysmal positional vertigo. Ann Otol Rhinol Laryngol 1993;102:325-31.[↩]
- Semont A, Freyss G, Vitte E. Curing the BPPV with a liberatory maneuver. Adv Otorhinolaryngol 1988;42:290-3.[↩]
- Nuti D, Nati C, Passali D. Treatment of benign paroxysmal positional vertigo: no need for postmaneuver restrictions. Otolaryngol Head Neck Surg 2000;122:440-4.[↩]
- Haynes DS, Resser JR, Labadie RF, Girasole CR, Kovach BT, Scheker LE, et al. Treatment of benign postional vertigo using the semont maneuver: efficacy in patients presenting without nystagmus. Laryngoscope 2002;112:796-801.[↩]
- Herdman SJ, Tusa RJ, Zee DS, Proctor LR, Mattox DE. Single treatment approaches to benign paroxysmal positional vertigo. Arch Otolaryngol Head Neck Surg 1993;119:450-4.[↩]
- Cohen HS, Jerabek J. Efficacy of treatments for posterior canal benign paroxysmal positional vertigo. Laryngoscope 1999;109:584-90.[↩]
- Foster C, A, Ponnapan A, Zaccaro K, Strong D: A Comparison of Two Home Exercises for Benign Positional Vertigo: Half Somersault versus Epley Maneuver. Audiol Neurotol Extra 2012;2:16-23. doi: 10.1159/000337947 https://www.karger.com/Article/Pdf/337947[↩]
- Wipperman J. Dizziness and vertigo. Prim Care. 2014;41(1):115–131.[↩]




{kind=link}