Contents
What is Babinski reflex
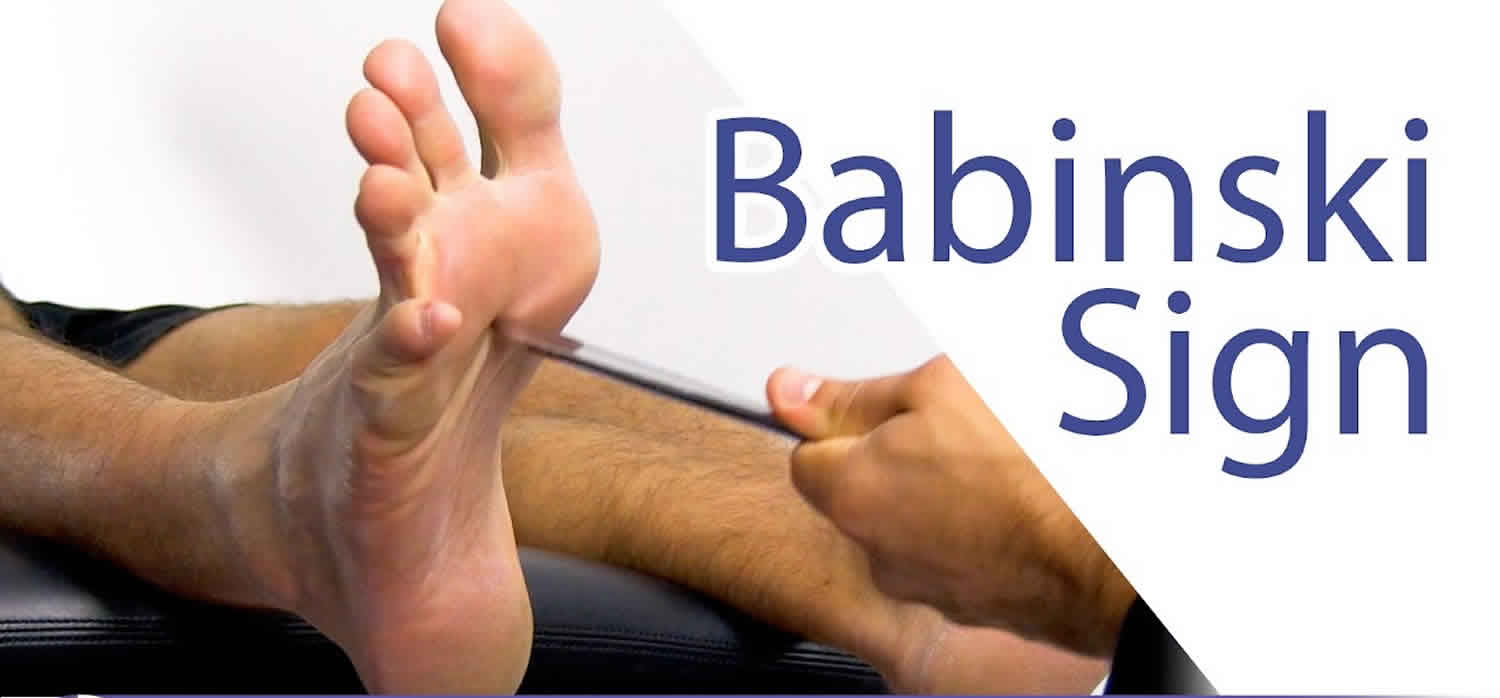
The Babinski reflex (plantar reflex) was described by the neurologist Joseph Babinski in 1899 1. According to Dr. Joseph Babinski, plantar stimulation by stroking the lateral sole of the foot to the base of 5th toe and arcing toward the base of the big toe produce a downward deflection (or plantar flexion) of the great toe in those with normal upper motor neuron function and upward deflexion (or dorsiflexion) of the great toe and fanning of the other toes in those with an upper motor neuron lesion (UMNL) 2. This response is now referred eponymously as the “Babinski sign” or descriptively as the extensor plantar response 3. Since that time, Babinski reflex has been incorporated into the standard neurological examination.
Little is known about the reliability and validity of Babinski’s sign 2. Plantar responses can be inconsistent with differences in tools, strength, methods, and assessors. Isaza Jaramillo et al. 4 has reported that Babinski sign has low sensitivity (50.8%), but high specificity (99%) in identifying pyramidal tract dysfunction with a positive likelihood ratio of 51.8 and calculated interobserver variability of 0.73. Deng et al. 5 observed that dorsiflexion of the big toe without recruitment of the other toes is more common in patients with cortical pyramidal tract lesions, while in those with lesions lower than cortex (corona radiata to the spinal cord) movement of other toes in addition to the big toe is more common. De Jong 6 has noted that an extensor plantar response may occasionally occur in patients with no evidence of corticospinal tract lesion. Loo et al. 2 conducted a study on the variability of plantar response in normal population which demonstrated positive Babinski’s sign in 5%–11% of the normal population, including those with withdrawal response, consistent with previous studies. Withdrawal responses induced by nociception and ticklish sensation are seen in about 5% of the normal population. These responses are mostly characterized by flexion of the big toe and other toes, knee, and hip flexion with dorsiflexion of the ankle 7.
The Babinski reflex tests the integrity of the cortical spinal tract 1. The cortical spinal tract is a descending fiber tract that originates from the cerebral cortex through the brainstem and spinal cord. Fibers from the cortical spinal tract synapse with the alpha motor neuron in the spinal cord and help direct motor function. The cortical spinal tract is considered the upper motor neuron (UMN) and the alpha motor neuron is considered the lower motor neuron (LMN). Sixty percent of the cortical spinal tract fibers originate from the primary motor cortex, premotor areas, and supplementary motor areas. The remainder originates from primary sensory areas, the parietal cortex, and the operculum. Damage anywhere along the cortical spinal tract can result in the presence of a Babinski sign.
Stimulation of the lateral plantar aspect of the foot (S1 dermatome) normally leads to plantar flexion of the toes (due to stimulation of the S1 myotome). The response results from nociceptive fibers in the S1 dermatome detecting the stimulation. Nociceptive input travels up the tibial and sciatic nerve to the S1 region of the spine and synapse with anterior horn cells. The motor response which leads to the plantar flexion is mediated through the S1 root and tibial nerve. The toes curl down and inward. Sometimes there is no response to stimulation. This is called a neutral response. This response does not rule out pathology.
The descending fibers of the cortical spinal tract normally keep the ascending sensory stimulation from spreading to other nerve roots. When there is damage to the cortical spinal tract, nociceptive input spreads beyond S1 anterior horn cells. This leads to the L5/L4 anterior horn cells firing, which results in the contraction of toe extensors (extensor hallucis longus, extensor digitorum longus) via the deep peroneal nerve.
Positive Babinski sign occurs when stimulation of lateral plantar aspect of the foot leads to extension (dorsiflexion or upward movement) of the big toe (hallux). Also, there may be fanning of the other toes. This suggests that there is been spread of the sensory input beyond the S1 myotome to L4 and L5. An intact cortical spinal tract prevents such spread.
In infants with at cortical spinal tract which is not fully myelinated the presence of a Babinski sign in the absence of other neurological deficits is considered normal up to 24 months of age. Babinski’s may be present when a patient is asleep.
The Babinski reflex is easy to elicit without sophisticated equipment. Also, Babinski reflex requires little active patient participation, so it can be performed in patients who are otherwise unable to cooperate with the neurological exam 8.
Figure 1. Spinal cord
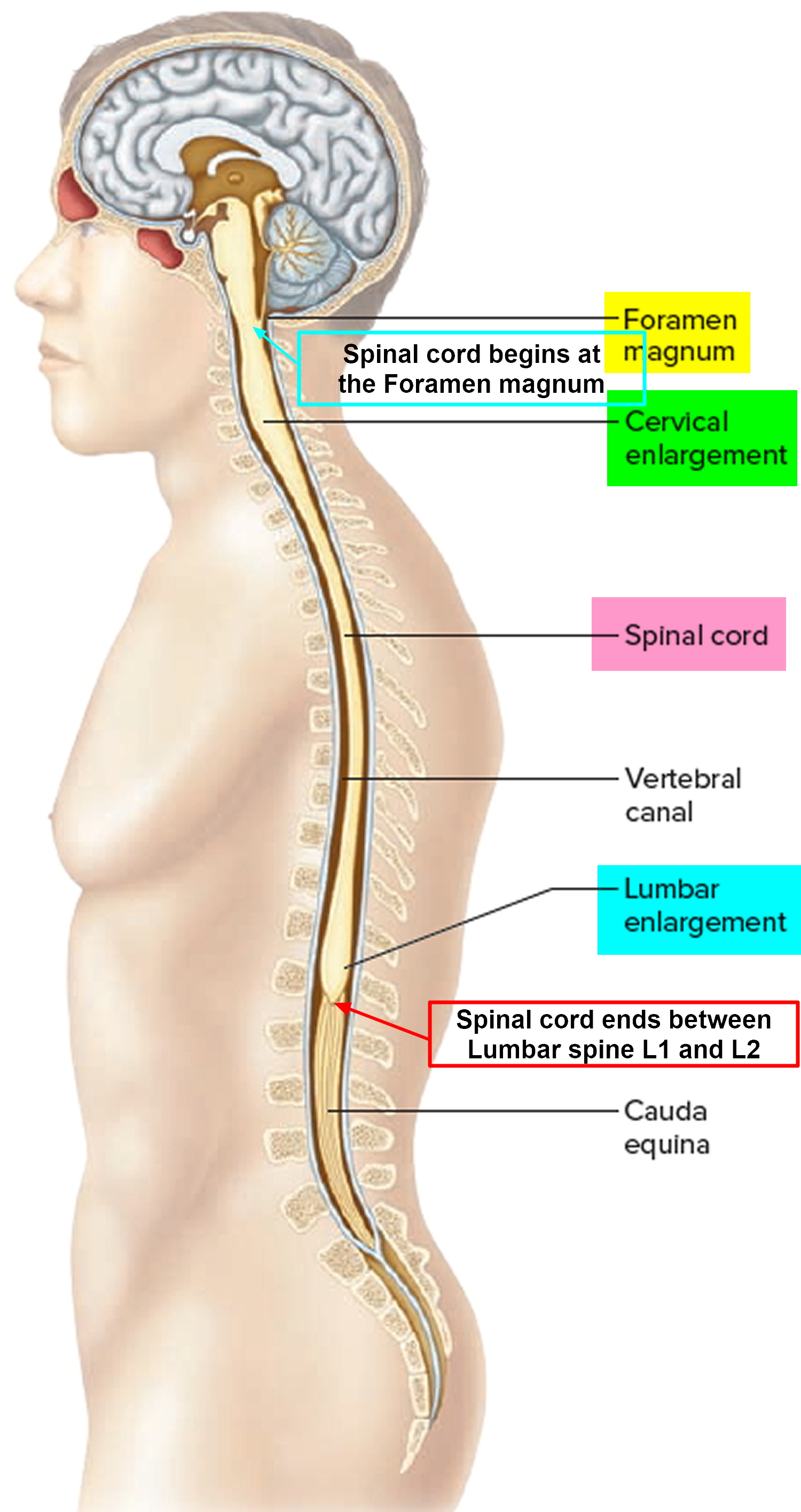
Figure 2. Spinal cord segments
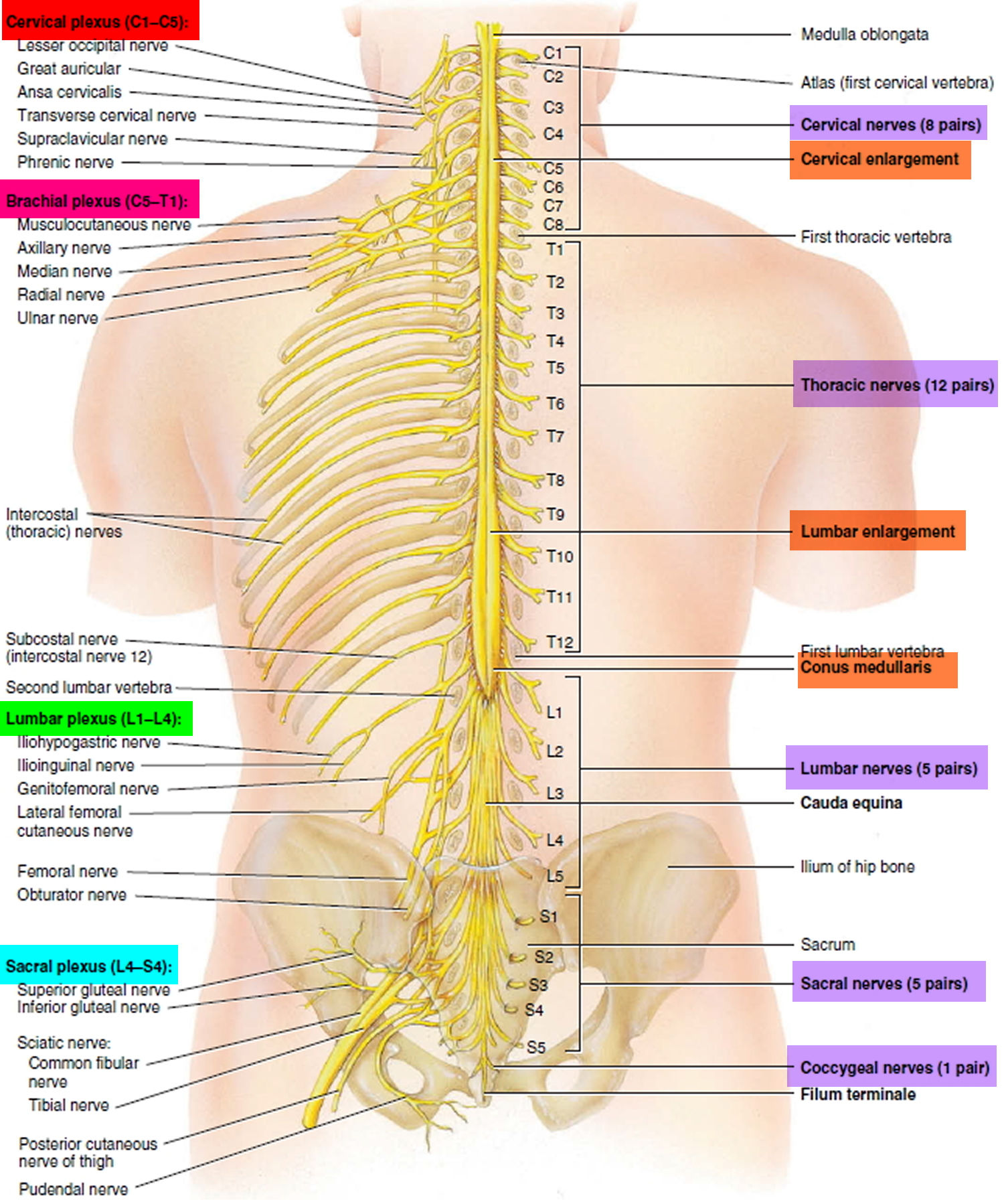
Figure 3. Spinal cord cross section
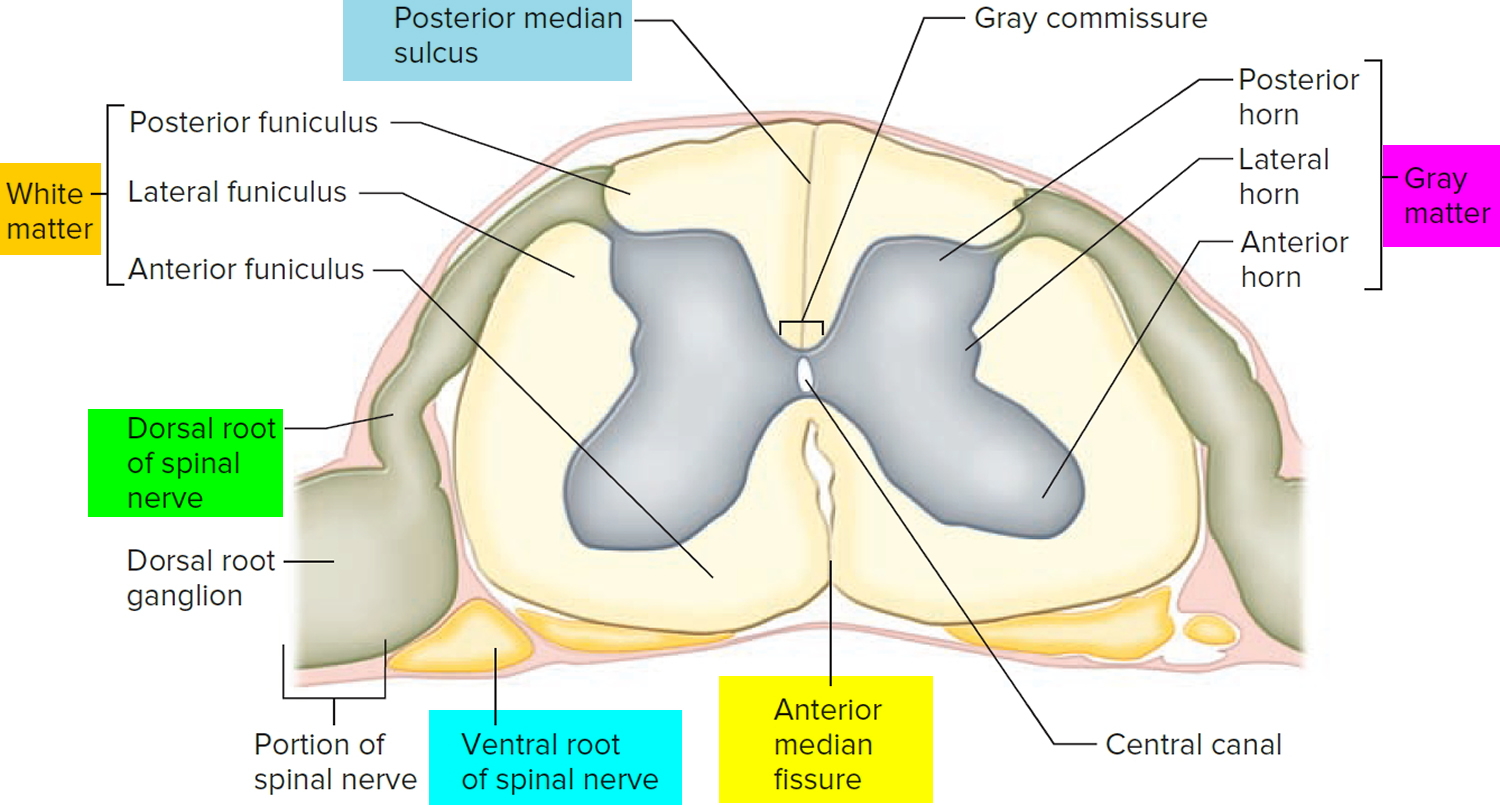
Figure 4. Spinal cord tracts
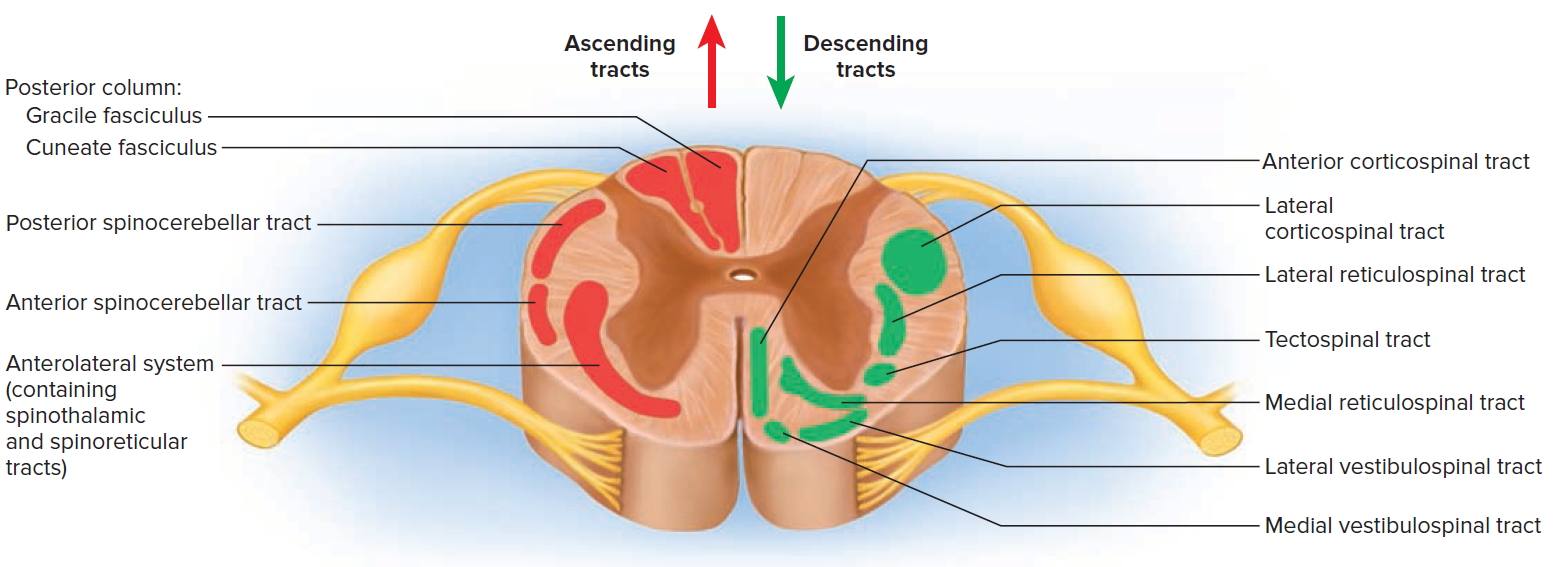
Figure 5. Processing of sensory input and motor output by the spinal cord
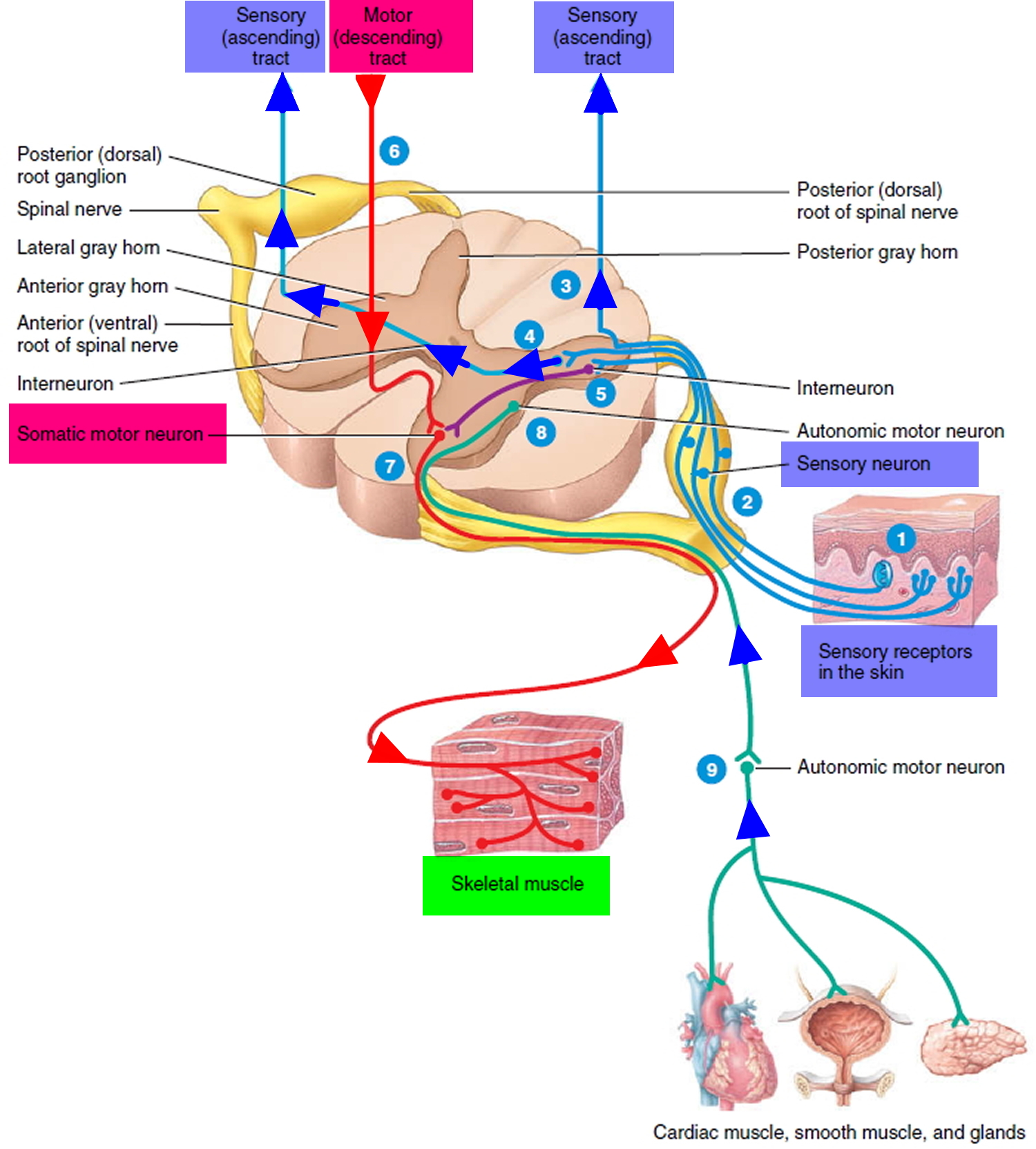
Figure 6. Dermatome (spinal nerves sensory innvervation)
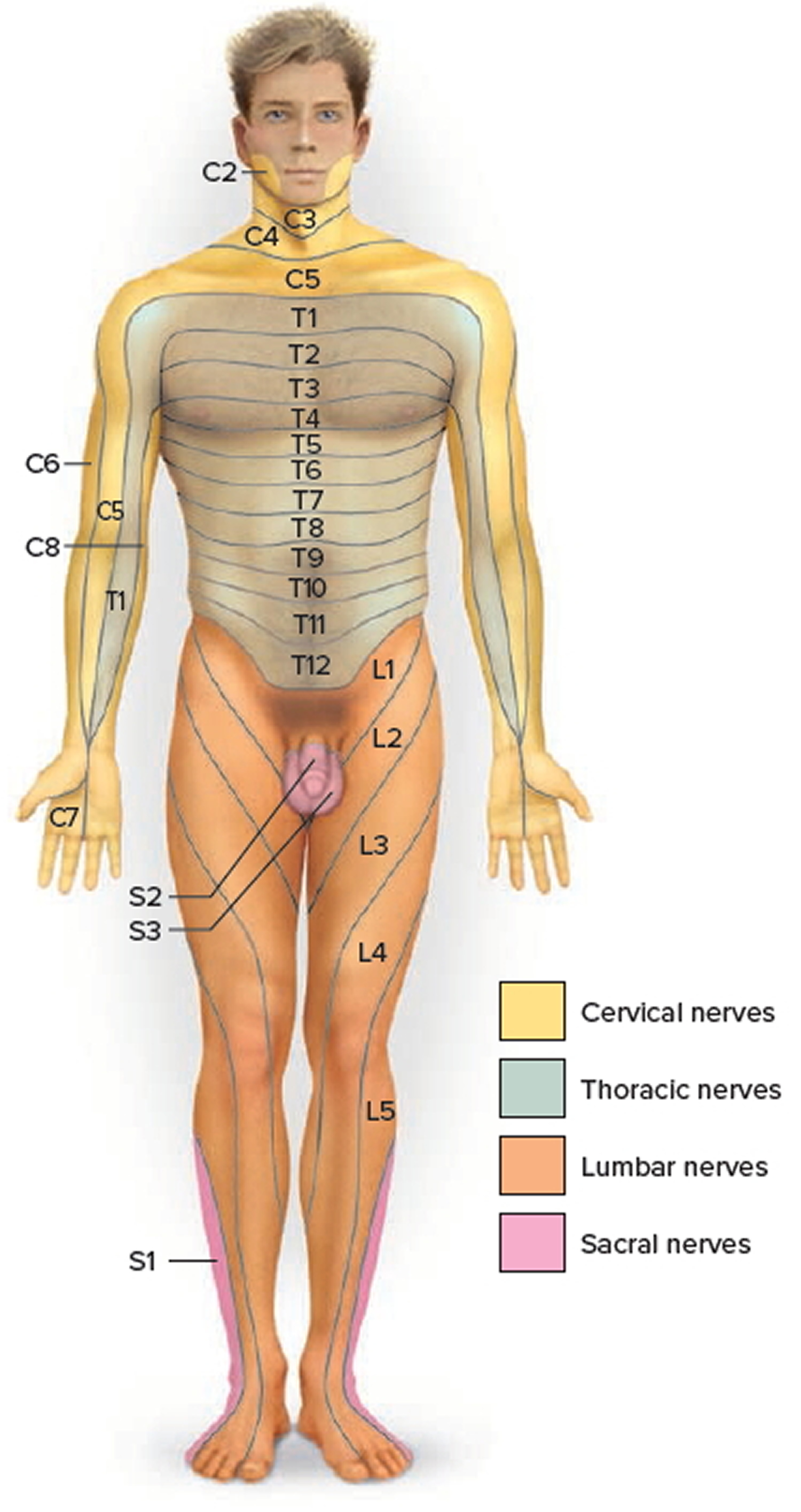
Footnote: Each zone of the skin is innervated by sensory branches of the spinal nerves indicated by the labels. Nerve C1 does not innervate the skin.
Babinski reflex in babies
Babinski reflex is one of the normal reflexes in infants. Reflexes are responses that occur when the body receives a certain stimulus.
The Babinski reflex occurs after the sole of the foot has been firmly stroked. The big toe then moves upward or toward the top surface of the foot. The other toes fan out.
Babinski reflex is normal in children up to 2 years old. Babinski reflex disappears as the child gets older. It may disappear as early as 12 months.
When does babinski reflex disappears?
Babinski reflex is normal in children up to 2 years old. Babinski reflex disappears as the child gets older. It may disappear as early as 12 months.
Babinski reflex test
The Babinski reflex test is done as part of the routine neurological exam and is utilized to determine the integrity of the cortical spinal tract. The presence of a Babinski sign suggests damage to the cortical spinal tract. Because the cortical spinal tract fiber tracts run from the brain, through the brainstem and into the spinal cord, lesions of the central nervous system (CNS) often affect the integrity of the cortical spinal tract. Thus, the presence or absence of the Babinski reflex can provide very useful information on the presence or absence of pathology affecting the central nervous system. Babinski reflex is especially important in the setting where there is suspicion of spinal cord injury or stroke, as it may be an early indicator of the presence of these emergency conditions 9.
Babinski reflex equipment
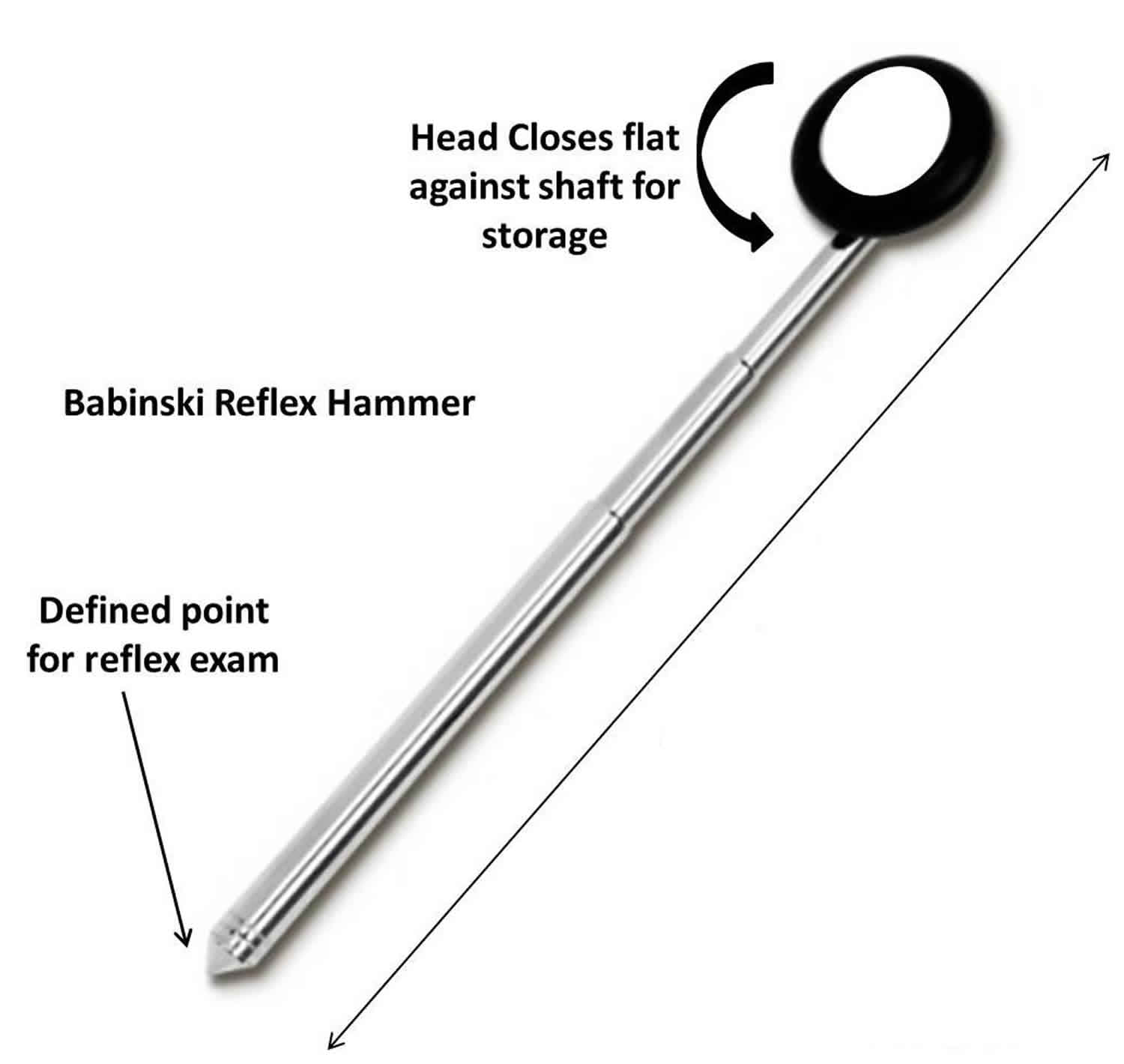
The Babinski reflex should be elicited by a dull, blunt instrument that does not cause pain or injury. Sharp objects should be avoided. The dull point of a Babinski reflex hammer, a tongue depressor, or the edge of a key are often utilized.
Figure 7. Babinski reflex hammer
Preparation
The patient should be relaxed and comfortable. It is best to advise the patient that the sensation may be slightly uncomfortable. Patients may experience both a mildly unpleasant sensation as well as a tickling sensation. The examiner should ensure that the plantar surface of the foot is free of any lesions before proceeding.
Technique
To test for Babinski’s sign, the instrument is run up the lateral plantar side of the foot from the heel to the toes, and across the metatarsal pads to the base of the big toe.
Many variations of the Babinski’s sign have been described. Each of them designed to elicit dorsiflexion (upward movement) of the big toe and fanning of the other toes. The more common include Chaddock (stimulating under lateral malleolus), Gordon (squeezing calf), Oppenheim (applying pressure to the medial side of the tibia), and Throckmorton (hitting the metatarsophalangeal joint of the big toe). The mechanism by which these alternatives elicit this response is likely similar to the Babinski response. These variations are useful in patients who have a significant withdrawal response to the conventional testing for the Babinski reflex.
Babinski reflex in adults
The examiner watches for dorsiflexion (upward movement) of the big toe and fanning of the other toes. When this occurs, then the Babinski reflex is present. If the toes deviated downward, then the reflex is absent. If there is no movement, then this is considered a neutral response and has no clinical significance 10.
The presence of the Babinski reflex is indicative of dysfunction of the cortical spinal tract. Oftentimes, the presence of the Babinski reflex is the first indication of spinal cord injury after acute trauma. Care must be exercised in interpreting the results because many patients have significant withdrawal response to plantar stimulation. When this occurs, one of the variations on eliciting a Babinski sign can be utilized.
In comatose patients, one may witness a triple flexion response. In this case, one observes dorsiflexion of the big toe, fanning of the other toes, dorsiflexion of the foot, as well as knee flexion 1. The triple flexion response represents profound dysfunction of the cortical spinal tract, with a spread of the reflex to the L3 and L2 myotomes. Care must be made to distinguish this from a withdrawal response. The triple flexion response is very stereotyped whereas the withdrawal response can vary with each stimulation.
Causes of positive babinski reflex in adults
When the Babinski reflex is present in a child older than 2 years or in an adult, it is often a sign of a central nervous system disorder. The central nervous system (CNS) includes the brain and spinal cord.
Central nervous system disorders may include:
- Amyotrophic lateral sclerosis (Lou Gehrig disease)
- Brain tumor or injury
- Meningitis (infection of the membranes covering the brain and spinal cord)
- Multiple sclerosis
- Spinal cord injury, defect, or tumor
- Stroke
- Acharya AB, Dewey JJ. Babinski Reflex. [Updated 2018 Dec 16]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2018 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK519009[↩][↩][↩]
- Loo SF, Justin NK, Lee RA, Hew YC, Lim KS, Tan CT. Differentiating Extensor Plantar Response in Pathological and Normal Population. Ann Indian Acad Neurol. 2018;21(2):144-149. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6073965/[↩][↩][↩]
- Morrow MJ, Mary MR. ‘The babinski sign’. Br J Hosp Med. 2011;72:157–8.[↩]
- Isaza Jaramillo SP, Uribe Uribe CS, García Jimenez FA, Cornejo-Ochoa W, Alvarez Restrepo JF, Román GC, et al. Accuracy of the babinski sign in the identification of pyramidal tract dysfunction. J Neurol Sci. 2014;343:66–8.[↩]
- Deng T, Jia JP, Zhang T, Guo D, Yang L. Cortical versus non-cortical lesions affect expression of babinski sign. Neurol Sci. 2013;34:855–9.[↩]
- Campbell WW. Dejong’s the Neurologic Examination. 6th ed. United States of America: Lippincott Williams & Wilkings; 2005[↩]
- Lee RA, Tay LL, Lim KS, Tan CT. Variability of plantar response in normal population. Neurol Asia. 2011;16:143–7.[↩]
- Loo SF, Justin NK, Lee RA, Hew YC, Lim KS, Tan CT. Differentiating Extensor Plantar Response in Pathological and Normal Population. Ann Indian Acad Neurol. 2018 Apr-Jun;21(2):144-149.[↩]
- Drouin E, Drouin G, Péréon Y. The Babinski sign. Lancet Neurol. 2017 Mar;16(3):180.[↩]
- Sumner AJ. The Babinski sign. J. Neurol. Sci. 2014 Aug 15;343(1-2):2.[↩]





{kind=link}