Contents
What is intertrigo
Intertrigo describes an inflammatory skin rash in the body folds, such as behind the ears, in the folds of the neck, under the arms (armpits), under a protruding abdomen, under the breasts, in the groin, between the buttocks, in the finger webs or toe spaces. Intertrigo is caused by irritation of touching skin surfaces (skin-on-skin friction) in body fold regions (armpits, under the breasts, belly, buttocks, groin, and sometimes between fingers or toes). Intertrigo’s Latin translation, inter (between) and terere (to rub) helps explain the physiology of the condition 1. Intertrigo tends to occur in warm, moist areas of the body where two skin surfaces rub or press against each other. Such areas are called intertriginous areas. Intertrigo can be worsened by any conditions causing increased heat, wetness, and friction. Intertrigo may be complicated by superficial skin infection with fungus or bacteria.
Intertrigo can be acute (recent onset), relapsing (recurrent), or chronic (present for more than 6 weeks).
Although intertrigo may affect one skin fold, it is common for it to involve multiple sites. Intertrigo is most commonly found in the groin, armpits and under the breasts (inframammary folds). It also may affect antecubital fossae; umbilical, groin, or interdigital areas between fingers or toes; neck creases; and folds of the eyelids.
Intertrigo affects the top layers of skin. It is caused by moisture, bacteria, or fungus in the folds of the skin. The affected areas of skin are usually pink to brown. The exact appearance and behavior depends on the underlying cause or causes. The skin affected by intertrigo is inflamed, i.e., reddened and uncomfortable. It may become moist and macerated, leading to fissuring (cracks) and peeling. If the skin is very moist, it may begin to break down. In severe cases, there may be a bad odor.
Patients may present with itching, burning, and pain in the affected areas.
Intertrigo is most common in people who are overweight and obese. It may also occur in people who must stay in bed or who wear medical devices such as artificial limbs, splints, and braces. These devices may trap moisture against the skin.
Intertrigo is common in warm, moist climates.
Clinical findings
Morphology
- Intertrigo is characterized primarily by erythematous patches, which are often symmetrical
- The erythema may progress to more intense inflammation with erosions, fissures, exudation, crusting and maceration
- Candidal intertrigo may present as typical satellite macules, papules or pustules
- Toe web intertrigo may be mild, and asymptomatic, but it also can present with intense erythema and desquamation, which sometimes is erosive, malodorous, and macerated. Patients also may have profuse or purulent discharge and be unable to ambulate. Patients with advanced gram-negative infections may have green discoloration at the infection site. Individuals with severe toe web intertrigo who are overweight or who have diabetes are at a higher risk for cellulitis
Investigations
- If a secondary infection is suspected a swab should be taken for culture and sensitivity (C&S)
- If there is scale, skin scrapings should be sent for mycology to look for tinea
Treatment options for intertrigo include:
- Antibiotic or antifungal cream applied to the skin
- Drying medicine, such as Domeboro soaks
- Low-dose steroid cream or immune modulating cream may be used
- Creams that protect the skin
Self-care guidelines
- Gently cleanse the affected areas daily with mild soap substitutes.
- Keep the areas dry and exposed to the air. If this is not easy to do, using absorbent cotton or fabric, as well as absorbent powders, may help (as long as fabrics are changed if they become damp). Mild antiperspirants may help, but these can cause further irritation in some individuals.
- Barrier creams, such as zinc oxide paste, may be helpful for individuals wearing diapers or having incontinence problems.
If overweight, weight loss is recommended. - For persistent irritation, 0.5–1.0% hydrocortisone cream twice daily may help. Discontinue if you are no better after 2 weeks of use. Adding a topical antifungal to the hydrocortisone, such as clotrimazole cream, may help if yeast infection is suspected. Apply the barrier paste (if used) after application of these creams.
To properly treat intertrigo, it is imperative to recognize the underlying factor that is causing the condition (see intertrigo causes).
For mild cases, your doctor will tell you to keep the affected area of your skin dry and exposed to air. Your doctor may also want to prescribe a topical steroid cream. For more severe cases, your doctor may prescribe an antibiotic or antifungal cream. There are also antifungal powders that may help dry the skin. Talk to your doctor about which treatment is right for you.
Figure 1. Intertrigo rash

Figure 2. Intertrigo armpit

Figure 3. Intertrigo groin

Figure 4. Intertrigo buttocks

Figure 5. Intertrigo baby
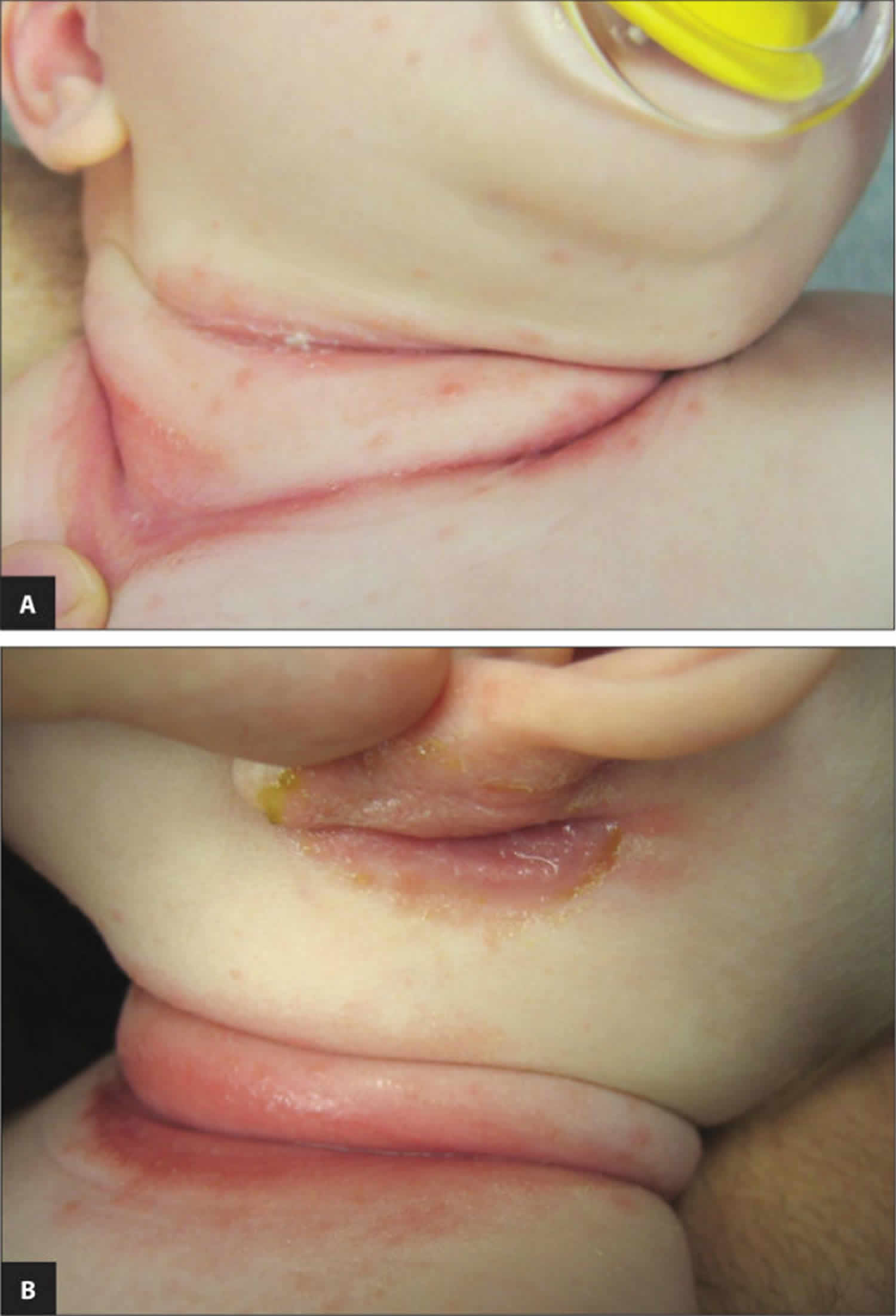
Figure 6. Intertrigo fingers

Is intertrigo contagious?
No. Intertrigo is primarily caused by skin-on-skin friction where it is facilitated by moisture trapped in deep skinfolds. Intertrigo affects the top layers of skin. The microorganisms that are normally resident on the folds of the skin, the microbiome, include corynebacteria, other bacteria and yeasts. These multiply in warm moist environments and may cause intertrigo.
Intertrigo is most common in people who are overweight and obese. It may also occur in people who must stay in bed or who wear medical devices such as artificial limbs, splints, and braces. These devices may trap moisture against the skin.
Intertrigo is common in warm, moist climates.
Who’s at risk of intertrigo?
Intertrigo can affect people of all ages. Intertrigo is most frequently seen in overweight people, diabetics, people spending a lot of time in bed, diaper users, or anyone with incontinence problems. It can also occur in individuals wearing or using anything that causes friction or holds moisture against the skin surface.
Intertrigo is most commonly seen in skin fold areas. In people who are obese, the skin my become inflamed in neck creases, on the skin behind the knee or in front of the elbows, in the thigh and groin folds, or, less commonly, under the breast or belly folds. Redness and breaks in the skin (erosions) of opposing skin surfaces may be noted. The area may ooze or be sore or itchy.
What causes intertrigo
Intertrigo is due to genetic and environmental factors.
- Genetic tendency to skin disease
- Hyperhidrosis (excessive sweating)
Intertrigo is primarily caused by skin-on-skin friction where it is facilitated by moisture trapped in deep skinfolds where air circulation is limited.
- Flexural skin has relatively high surface temperature
- Moisture from insensible water loss and sweating cannot evaporate due to occlusion.
- Friction from movement of adjacent skin results in chafing.
Individuals at particular risk of intertrigo include:
- Obese or overweight patients
- Infants, due to short necks, relative chubbiness, and flexed posture. Drooling also can facilitate intertrigo in infants
- Toe web intertrigo may be associated with closed-toe or tight-fitting shoes and commonly affects persons participating in athletic, occupational, or recreational activities
- Other predisposing factors include urinary and fecal incontinence, hyperhidrosis, diabetes, poor hygiene, and malnutrition
The moist damaged skin associated with intertrigo is a fertile breeding ground for various germs, and secondary skin infections are commonly observed in these areas:
- Bacterial infection – Staphylococcus aureus, group A beta-haemolytic streptococcus, and various gram-negative organisms may occur alone or simultaneously. Proliferation may be associated with keratinocytic necrosis
- Fungal infection – candida is the fungus most commonly associated with intertrigo. In the toe webs, gram-negative bacteria are often copathogens.
Experts classify intertrigo into infectious and inflammatory origin but there is often overlap:
- Infections tend to be unilateral and asymmetrical.
- Inflammatory disorders tend to be symmetrical affecting armpits, groins, under the breasts and the abdominal folds, except atopic dermatitis, which more often arises on the neck, and in elbow and knee creases.
Infections causing intertrigo
Candida albicans (thrush)
- Rapid development
- Itchy moist peeling red and white skin
- Small superficial papules and pustules
Erythrasma (Corynebacterium minutissimum)
- Persistent brown patches
- Minimal scale
- Asymptomatic
Tinea (Trichophyton rubrum + Trichophyton interdigitale)
- Tinea cruris (groin) and athletes foot (between toes)
- Slowly spreads over weeks to months
- Irregular annular plaques
- Peeling, scaling
Impetigo (Staphylococcus aureus and Streptococcus pyogenes)
- Rapid development
- Moist blisters and crusts on red base
- Contagious, so other family members may also be affected
Common inflammatory skin conditions causing intertrigo
Flexural psoriasis
- Well-defined smooth or shiny red patches
- Very persistent
- Common under the breasts and groin creases
- Symmetrical involvement
- May fissure (crack) in the crease
- Red patches on other sites are scaly
Seborrheic dermatitis
- Ill-defined salmon-pink thin patches
- Common in axilla and groin creases
- Fluctuates in severity
- May be asymmetrical
- Often unnoticed
- Red patches on face and scalp tend to be flaky
Atopic dermatitis
- First occurs in infancy
- Common in elbow and knee creases
- Characterized by flares
- Very itchy
- Acute eczema is red, blistered, swollen
- Chronic eczema is dry, thickened, lined (lichenified)
Contact irritant dermatitis
- Acute, relapsing or chronic
Irritants include:
- Body fluids: sweat, urine
- Friction due to movement and clothing
- Dryness due to antiperspirant
- Soap
- Excessive washing
Contact allergic dermatitis
- Acute or relapsing
Allergen may be:
- Fragrance, preservative or medicament in deodorant, wet-wipe or other product
- Component of underwear (rubber in elastic, nickel in bra wire).
Can intertrigo be prevented or avoided?
You can help prevent intertrigo by doing these things:
- Keep skin cool and dry.
- Do not wear tight shoes or clothing. Wear a bra that has good support.
- Wear clothes made with absorbent fabrics, such as cotton. Avoid nylon or other synthetic (manmade) fibers.
- If you are overweight, try to lose weight.
- After exercising, shower and dry off completely. Use a hair dryer with a cool setting to dry areas that can trap wetness, such as under your arms or breasts.
Intertrigo symptoms
Symptoms of intertrigo include a red or reddish-brown rash that can appear anywhere skin rubs together or traps wetness. This rash may burn or itch. The most common areas include:
- between toes
- in the armpits
- in the groin area
- on the underside of the belly or breasts
- in the crease of the neck.
Intertrigo can also affect the skin between the buttocks. The affected skin will often be very raw and may itch or ooze. In severe cases, intertrigo may cause a foul odor, and the skin may crack and bleed.
Intertrigo diagnosis
Your doctor can usually tell if you have the condition by looking at your skin.
Other tests may include:
- A skin scraping and a test called a KOH (potassium hydroxide) examination to rule out a fungal infection
- Looking at your skin with a special lamp called a Wood’s lamp, to rule out a bacterial infection called erythrasma
- A swab for microscopy and culture of bacteria (microbiology)
- A scraping for microscopy and culture of fungi (mycology)
- In rare cases, a skin biopsy may be performed for histopathology if the skin condition is unusual or fails to respond to treatment.
How to treat intertrigo
Treatment depends on the underlying cause, if identified, and on which micro-organisms are present in the rash. Combinations are common.
- Sweating may be reduced with a gentle antiperspirant.
- Physical exertion should be followed by a bath and completely drying the skin folds using a hair dryer on cool setting, soft towel and/or corn starch powder.
- Triple paste contains petrolatum, zinc oxide, and aluminium acetate solution to reduce friction, irritation and sweating.
- Bacteria may be treated with topical antibiotics such as fusidic acid cream, mupirocin ointment, or oral antibiotics such as flucloxacillin and erythromycin.
- Yeasts and fungi may be treated with topical antifungals such as clotrimazole and terbinafine cream or oral antifungal agents such as itraconazole or terbinafine.
- Inflammatory skin diseases are often treated with low potency topical steroid creams such as hydrocortisone. More potent steroids are usually avoided in the flexures because they may cause skin thinning resulting in stretch marks (striae) and even ulcers. Calcineurin inhibitors such as tacrolimus ointment or pimecrolimus cream may also prove effective.
Step 1: Prevention and general measures
- Optimal prevention includes minimizing skin-on-skin friction, reducing heat and moisture around skinfolds, and keeping high-risk areas clean and dry. Patients should be warned about heat, humidity, and outside activities. Physical exercise usually is desirable, but patients should shower after exercise and keep intertriginous areas thoroughly dry. Wearing open-toed shoes may help prevent toe web intertrigo.
- Obese patients should lose weight, if possible.
- Patients should wear light, non-constricting, and absorbent clothing and avoid nylon and other synthetic fibres. Bio-textiles (eg cotton or polyester gauze with built-in antiseptic molecules) may help patients with intertrigo.
- Avoid the use of absorptive powders, such as talc and cornstarch, which may irritate the skin.
Step 2: Medical treatment
- Daktacort cream twice daily, for many, is a sensible first-line option as it contains miconazole (which treats candida, as well as having some Gram‐positive bacteriostatic action) and 1% hydrocortisone cream (helps reduce inflammation)
- For more significant inflammation consider the short-term use of Trimovate ® cream
- If the skin is not settling then further treatment, such as topical or oral antibiotics, or oral antifungal therapy, may be required, the specific treatment should be guided by results of skin swabs.
- Toe web infection can be very difficult to treat:
- The skin must be allowed to breathe by the wearing of appropriate footwear and leaving the feet bare at home when possible
- Daktacort cream twice daily for 2-4 weeks can still be used first-line, however, if not responding consider:
- Swabs should be taken for culture and sensitivity (C&S) as the proper identification of organisms is critical so that effective therapy can be initiated
For potential co-existing gram-negative bacteria, soak the feet in 1:80000 potassium permanganate solution (one Permitab ® dissolved in four litres warm water), twice a day for 10-15 minutes. Warn patients to apply Vaseline to nails to avoid staining them brown. Keep the Pemitabs away from children - In those responding poorly to treatment consider a ten day trail of ciprofloxacin 500 mg oral twice daily
- Occasionally tissue removal may be needed to allow absorption of topical treatments
Step 3: Other treatments
- Surgery, to remove excess skin, may be required for patients with moderate-severe recalcitrant intertrigo
Intertrigo home treatment
To properly treat intertrigo, it is imperative to recognize the underlying factor that is causing the condition (see intertrigo causes).
If there is an infectious component to the rash, then the proper antimicrobial should be administered.
- In simple intertrigo, drying agents such as antiperspirants can be used to minimize the sweating.
- It may help to lose weight and often change your body position.
- Separate skin folds with dry towels.
- Wear loose clothing and moisture wicking fabrics.
- Blow a fan on moist areas.
- A bath with proper drying using a soft towel should follow excessive physical activity that causes excessive perspiration.
- Aluminum acetate solution, zinc oxide, and petrolatum, the ingredients that comprise triple paste, is an effective antiperspirant that also reduces frictional exposure and improves skin irritation 2.
- Staying cool by wearing loose clothing, and working in air-conditioned environments will help in the prevention of the rash.
- Absorbent powders compress with an aqueous solution of aluminium triacetate 1:40, and wet tea bags are other preventative measures that have been proven to be effective.
- Absorbent diapers are more effective at decreasing the moisture; however, if treatment is required, petrolatum ointment cream is effective and safe for diaper dermatitis.
If the lesion is infected with a bacteria, then use a topical treatment such as mupirocin. If oral medication is required, an effective option against gram-positive bacteria, notably Staphylococcus or Streptococcus, like flucloxacillin or erythromycin should be prescribed. Topical clotrimazole is an effective treatment for yeast or fungal infected intertrigo. Low-dose steroids may be initiated for anti-inflammatory properties, for example, hydrocortisone cream, yet it is not always needed. A lower strength steroid should be preferred if chosen to prevent atrophy in the already thinner epidermis of the flexural surfaces 3.
Living with intertrigo
Intertrigo may come and go many times over. If you know that you are predisposed to getting intertrigo, take precautions. Before physical activity, treat the area with deodorant or with petroleum jelly. Do what you can to keep skin folds dry.
Intertrigo prognosis
Intertrigo prognosis is positive for the majority of patients. The underlying risk factors should be addressed to diminish the intertrigo outbreaks. However, if the risks such as diabetes and obesity are not properly managed, the condition tends to relapse quite frequently.
Candidal intertrigo
Candidal intertrigo refers to superficial skin-fold infection caused by the yeast, candida.
Candidal intertrigo is triggered by a combination of the following factors:
- The hot and damp environment of skin folds, which is conducive to the growth of candida species, particularly Candida albicans 4
- Increased skin friction 5
- Immunocompromise 6
Who gets candidal intertrigo?
Factors that increase an individual’s risk of developing candidal intertrigo include:
- Occlusive clothing, gloves and footwear
- Obesity
- Excessive sweating (hyperhidrosis)
- Incontinence causing irritant contact dermatitis
- Diabetes mellitus
- Immune deficiency conditions, such as human immunodeficiency virus infection (HIV) or immune suppression by medications (chemotherapy, systemic corticosteroids) 7.
What are the clinical features of candidal intertrigo?
Candidal intertrigo classically presents as erythematous and macerated plaques with peripheral scaling. There are often associated superficial satellite papules or pustules 8.
Affected areas may include:
- Skin folds below the breasts or under the abdomen
- Armpits and groin
- Web spaces between the fingers or toes (erosio interdigitalis blastomycetica) 9.
Figure 7. Candidal intertrigo

How is candidal intertrigo diagnosed?
Diagnosis of candidal intertrigo requires recognition of consistent clinical features. In cases of uncertainty, confirmation can be sought by way of fungal microscopy and culture of skin swabs and scrapings 10. Skin biopsy is usually not necessary.
Candidal intertrigo treatment
- Predisposing factors should be addressed primarily, such as weight loss, blood glucose control and avoidance of tight clothing 11.
- Patients should be advised to maintain cool and moisture-free skin. This may be aided by regular use of a drying agent such as talcum powder, especially if infection is recurrent 12.
- Topical antifungal agents such as clotrimazole cream are recommended as first-line pharmacological treatments 13.
- Severe, generalised and/or refractory cases may require oral antifungal treatments such as fluconazole or itraconazole 14.
- Wolf R, Oumeish OY, Parish LC. Intertriginous eruption. Clin. Dermatol. 2011 Mar-Apr;29(2):173-9.[↩]
- Nobles T, Miller RA. Intertrigo. [Updated 2018 Oct 27]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2018 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK531489[↩]
- Wilmer EN, Hatch RL. Resistant “candidal intertrigo”: could inverse psoriasis be the true culprit? J Am Board Fam Med. 2013 Mar-Apr;26(2):211-4.[↩]
- Yaar M, Gilchrest BA. Aging of skin. In: Fitzpatrick’s Dermatology in General Medicine, Freedberg IM, Eisen AZ, Wolff K, et al (Eds), McGraw-Hill, New York 2003. p.1386[↩]
- Garcia Hidalgo L. Dermatologic complications of obesity. Am J Clin Dermatol. 2002;3(7):497.[↩]
- Jautova J, Baloghova J, Dorko E, et al. Cutaneous candiosis in immunosuppressed patients. Folia Microbiol. 2001;46(4):359.[↩]
- Ingordo V, Naldi L, Fracchiolla S. Prevalence and risk factors for superficial fungal infections among italian navy cadets. Dermatol.2004;209(3):190-6.[↩]
- Klenk AS, Martin AG, Heffernan MP. Yeast infections: candidiasis, pityriasis (tinea) versicolor. In: Dermatology in General Medicine, Freedberg IM, Eisen AZ, Wolff K, et al (Eds), McGraw-Hill, New York 2003. p.2006.[↩]
- Sobera JO, Elewski BE. Fungal Diseases. In: Dermatology, Bolognia JL, Jorizzo JL, Rapini RP (Eds), Mosby, London 2003. p.1171.[↩]
- Guitart J, Woodley DT. Intertrigo: a practical approach. Compr Ther. 1994;20(7):402.[↩]
- Gray M. Optimal management of incontinence-associated dermatitis in the elderly. Am J Clin Dermatol. 2010;11(3):201.[↩]
- Hay RJ. The management of superficial candidiasis. J Am Acad Dermatol. 1999;40(6 Pt 2):s35.[↩]
- Metin A, Dilek N, Demireseven DD. Fungal infections of the folds (intertriginous areas). Clin Dermatol. 2015;33(4):437-47.[↩]
- Karla MG, Higgins KE, Kinney BS. Intertrigo and secondary skin infections. Am Fam Physician. 2014.89(1):569-573.[↩]





{kind=link}