
Contents
What is a meniscus tear
A meniscus tear is a common knee injury. The meniscus is a rubbery, C-shaped disk that acts as a “shock absorber” between the thighbone and shinbone. The meniscus helps cushion and stabilize your knee joint. Each knee has two menisci—one on the outside of the knee (lateral meniscus) and one on the inside (medial meniscus).
Meniscus tears are among the most common knee injuries. Athletes, particularly those who play contact sports, are at risk for meniscus tears. However, anyone at any age can tear a meniscus. When people talk about torn cartilage in the knee, they are usually referring to a torn meniscus.
A meniscus tear is often caused by a single acute injury—such as a sudden twist or quick turn during sports activity. Because the menisci weaken and wear thin over time, older people are more likely to experience a degenerative meniscus tear.
Menisci tear in different ways. Tears are noted by how they look, as well as where the tear occurs in the meniscus. Common tears include bucket handle, flap, and radial.
Sports-related meniscus tears often occur along with other knee injuries, such as anterior cruciate ligament (ACL) tears.
Once the meniscus is torn, symptoms like locking, clicking, and catching may occur. In addition, patients will frequently notice swelling in the knee. The pain will be localized along the joint line on the inside or the outside of the knee depending on the tear. The diagnosis is made based upon a history and physical exam and frequently special tests. X-rays are usually normal. If there is some question regarding the diagnosis, an MRI can be obtained to confirm a tear. Most tears remain symptomatic and will ultimately require treatment if they interfere with activities of daily living or sports and recreation activities.
In 90% of the time, a surgical procedure called “arthroscopy” is used to repair or remove a torn meniscus. Often the meniscus cannot be repaired due to the lack of blood supply, which prevents healing factors from getting to the area of injury even when repaired by stitches. Arthroscopic meniscal debridement is one of the most common procedures performed in orthopedics. It is typically very successful in decreasing symptoms and allowing patients to return to their normal activities. The fact that the patient has torn the meniscus increases their risk of arthritis over the next 15 to 20 years. Removing the torn fragments does not increase this risk, but merely decreases the symptoms from the tear.
Over the last 5 years, there have been many scientific studies 1 showing that the pain from a degenerative meniscus tear has the same chance of going away with surgery or physical therapy. Other papers 2 show that your risk of needing a knee replacement increase if you have surgery to remove the torn pieces. Some of patients are under the misconception that having surgery now will prevent knee arthritis. That is simply not true. A more recent study in the New England Journal of Medicine 2013 3 on meniscus tears showed that surgery had the same result as sham surgery. That means that some people were put under anesthesia, had two little cuts made in their skin, but the meniscus was not treated. Those people had the same chance of feeling better as those who had the actual surgery.
However, some tears will not heal. Some tears will continue to hurt. Surgery may become a reasonable option for some people. But meniscus surgery should not be near as common as it is today. Some tears, particularly those in athletes or meniscus tears that occurred due to trauma will require surgery. Most acute meniscus tears should be sutured or repaired. Healing after a meniscus repair is becoming more successful with better techniques. Many tears were deemed non-repairable decades ago. Many of those tears can now be repaired with a reasonable chance of success.
Whether or not a meniscus tear can be fixed, and whether or not a meniscus tear might heal depends on the type of tear and the cause of the tear.
Bottom Line: The meniscus serves a very important function within our knee. When a meniscus tears, it will not serve to protect your knee from developing osteoarthritis. Many tears are now repairable with modern techniques. If these repairs are successful at restoring the integrity of the meniscus, then you may not go on to suffer the consequences of an arthritic knee.
Repairs are generally reserved for acute, traumatic tears in children and young adults. Surgery for degenerative meniscus tears in adult knees with osteoarthritis is rarely required. Although your degenerative tear will not heal spontaneously, physical therapy and other non-surgical measures are usually effective at minimizing pain and maximizing function as effectively as surgery.
This video provides information about the causes and symptoms of meniscus tears, surgical and nonsurgical treatment options, and what to expect during recovery.
Can meniscus tears heal without surgery?
In a very small group of people that can happen. Meniscus tears that heal themselves tend to be traumatic tears which occur at the same time you tear your anterior cruciate ligament or ACL. Otherwise, most tears do not heal unless they are sutured back together.
Meniscus tear repair
Since the meniscus helps protect the knee from wear and tear, surgeons try to repair the meniscus whenever possible. However, most meniscus tears are not considered repairable. The meniscus has a limited blood supply, and tears in areas of little or no blood flow have a high risk of not healing. The pattern of the tear is also important. It is not always possible to predict whether a meniscus tear is repairable prior to surgery.
If a meniscus tear is considered appropriate for an attempt at repair, a number of techniques can be used. The surgery is primarily arthroscopic (minimally invasive) although additional small incisions, or cuts, may be necessary to perform the repair. A variety of devices or sutures can be used to perform a repair. If a patient has an anterior cruciate ligament (ACL) reconstruction at the same time as the repair of the meniscus, there is more blood present in the knee joint. As a result, the success rates of meniscus repair are higher when an anterior cruciate ligament (ACL) reconstruction is performed at the same time. Other methods can be used to improve the blood supply to a meniscus repair, for example using a portion of the patient’s own blood with a technique called platelet rich plasma (PRP).
Knee joint anatomy
Three bones meet to form your knee joint: your thighbone (femur), shinbone (tibia), and kneecap (patella).
The ends of the thighbone and shinbone, as well as the back of the patella, are covered with articular cartilage, a slippery substance that helps your knee bones glide smoothly across each other when bending or straightening the leg.
The menisci are two wedge-shaped pieces of cartilage that act as “shock absorbers” between your thighbone and shinbone. These are called meniscus. Unlike the articular cartilage, menisci are strong, rubbery and elastic. The menisci help cushion your knee joint and keep it stable. There are two menisci in each knee, one on each side of the joint.
Another important part of the knee joint is the synovium. The knee joint is surrounded by a thin lining that surrounds the knee joint called the synovium. The synovium releases a fluid that lubricates the cartilage and reduces friction during movement.
Ligaments connect bones to other bones and the four main ligaments in your knee act like strong ropes to hold the bones together and keep your knee stable. Two collateral ligaments are on either side of the knee. Two cruciate ligaments are inside the knee joint and cross each other to form an “X” – anterior cruciate ligament (ACL) and posterior cruciate ligament (PCL)
Figure 1. Knee joint anatomy (Normal anatomy of the knee. The menisci are two rubbery disks that helps cushion the knee joint.)
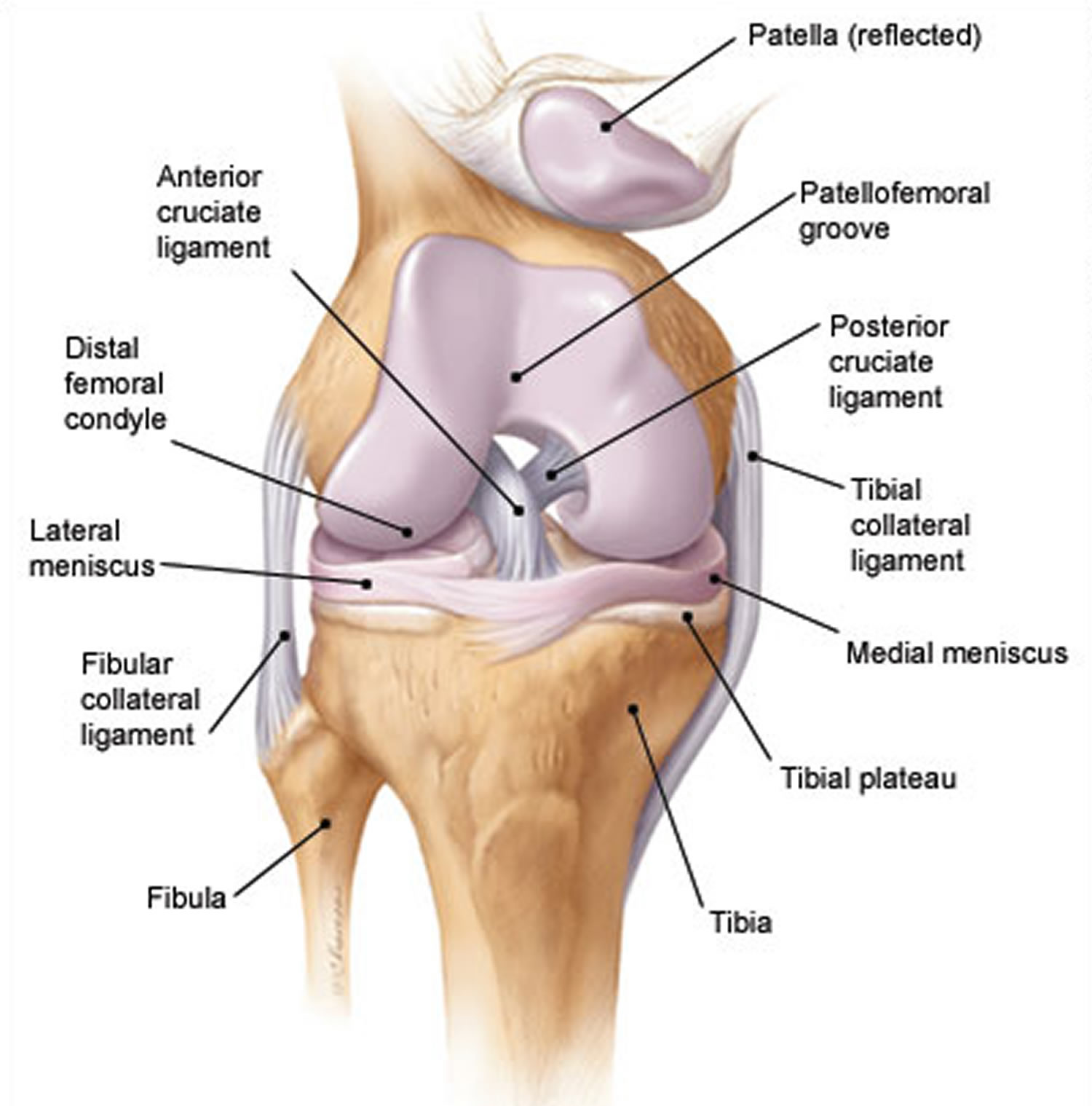
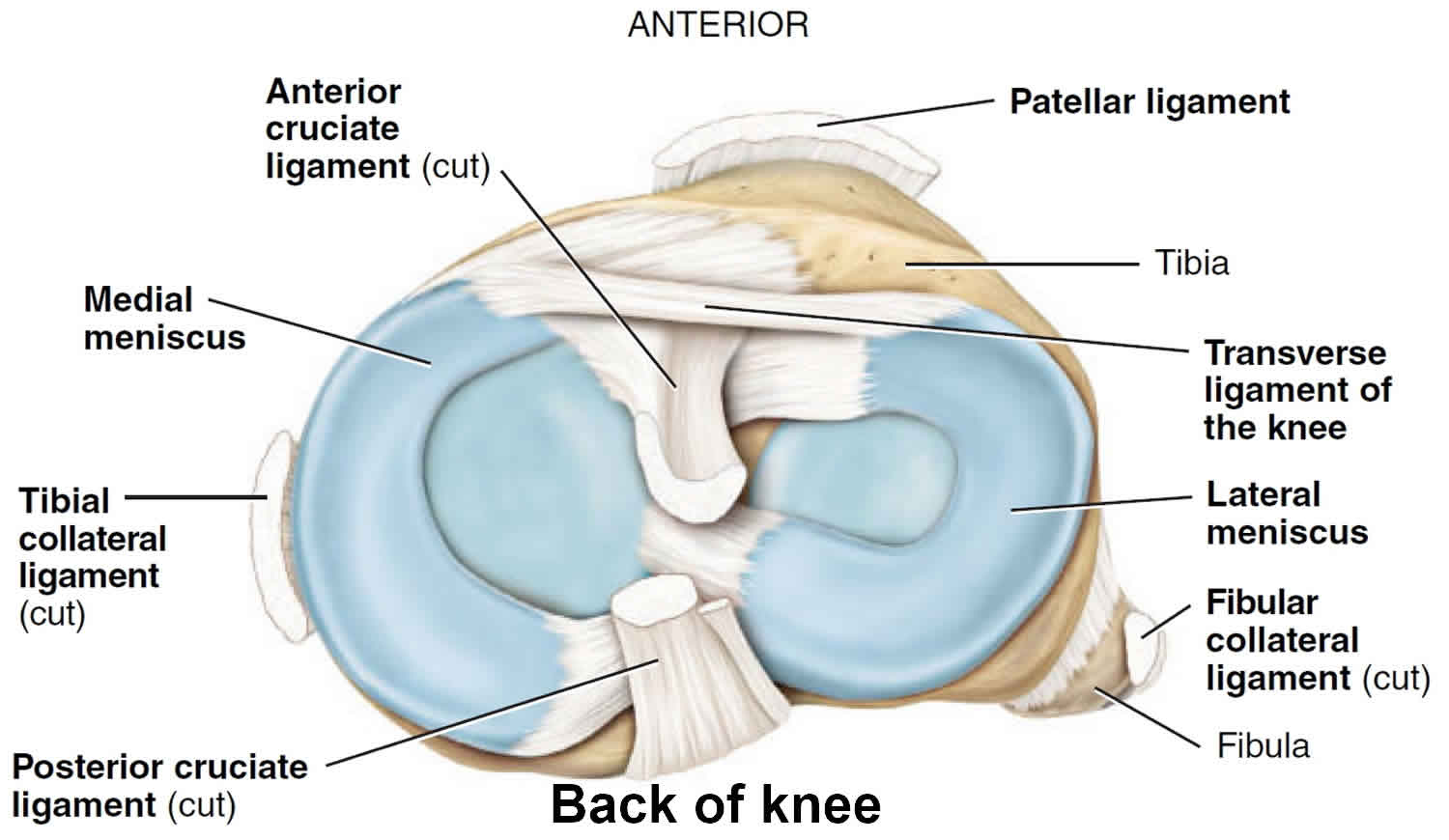
Figure 2. Knee meniscus anatomy
What does a meniscus do?
The meniscus serves and important function of transmitting force across the knee joint with all weightbearing activities ( walking, running, jumping, etc..) They are crescent-shaped, allowing the rounded lower part of the thigh bone (femur) to better fit the flat top of the shin bone (tibia). Its triangular shape allows the two bones to “fit” better and distribute force over a larger area. It also helps maintain joint stability, improves the lubrication of the knee joint and absorbs some of the forces during walking.
Why is the meniscus important?
The meniscus, because of its weight-distributing function, prevents excessively high stresses from being applied to one small area of the joint surface. If the forces of walking and running are consistently concentrated in one small area of the joint the articular cartilage will, over time, become overloaded. Long-term high forces in one area overloads the ability of the articular cartilage to handle the “wear and tear” the knee must tolerate, and early arthritis may develop.
How does the meniscus get injured/torn?
The meniscus provides stability to the joint and act as “shock absorbers” for the knee joint. When the knee is twisted during sports or other activities, the meniscus can become caught between the femur and the tibia. The meniscus can then be torn away from its attachments on the outside edges.
Are meniscal tears associated with other injuries?
Meniscal tears are frequently associated with injuries to the anterior cruciate ligament (ACL), up to 80%. In addition, injury to other ligaments around the knee can be damaged at the time of meniscal tear. The medial (inside) and lateral (outside) meniscus are equally involved.
Meniscus tears types
Not all meniscus tears are the same. They do not look the same. They were not all caused by the same trauma. And most important of all, not all meniscus tears should be treated the same. Having an understanding of the different types of meniscus tears will help you understand what treatment if any is necessary to improve your knee pain.
Meniscus tears come in many different shapes and sizes. The various types of meniscus tears you could have will dictate whether or not you may need surgery. The various types of meniscus tears will also determine whether or not the torn piece can be stitched or repaired, or whether the torn piece will simply need to be removed. The type of meniscus tear you have will also determine whether or not you will likely have persistent pain on an ongoing basis or whether or not you can expect to feel better after a period of rest.
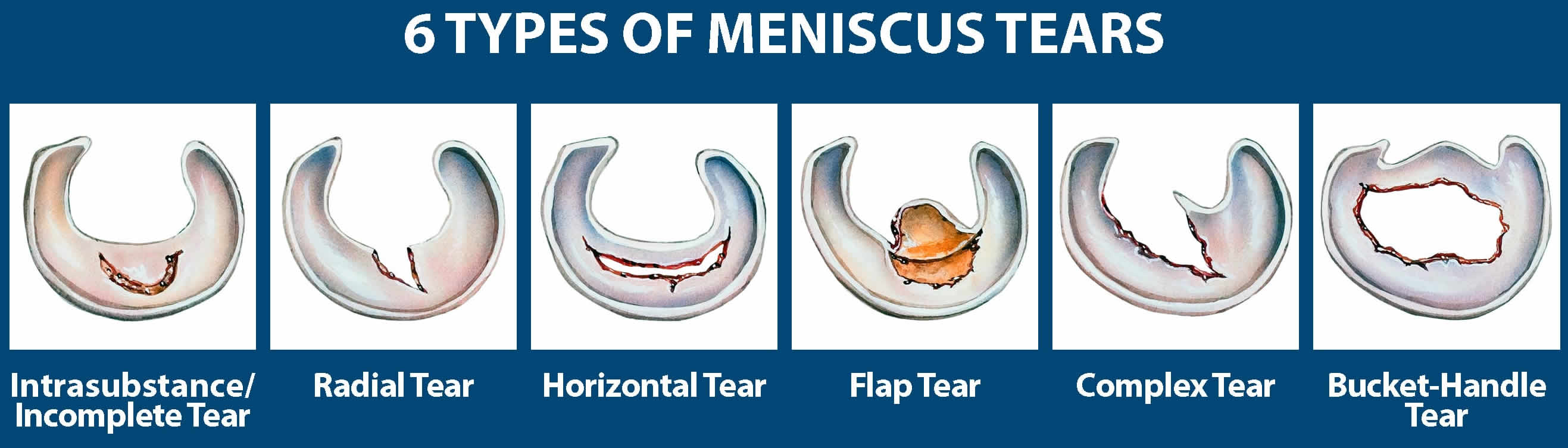
There are several ways that the meniscus is torn. Tears are classified by how they look, as well as where the tear occurs in the meniscus. Common tears include:
- Bucket Handle
- Degenerative
- Flap
- Radial
First there are acute or traumatic meniscus tears that occur as a result of an injury. A bucket handle meniscus tear or flap tear is a common type of traumatic meniscus tear. Next, there are degenerative meniscus tears which occur as a result of wear and tear or attrition, and usually are not preceded by trauma . Traumatic meniscus tears come in all sorts of shapes and sizes. There are radial tears, which are short tears that extend from the inner margin of the meniscus and head towards the periphery or outer part of the meniscus. There is a picture above of a radial tear. There are also horizontal cleavage tears. These are very common and literally cleave a big portion of the meniscus in half, so there are nearly two “c” shaped discs sitting on top of one another. The largest of all meniscus tears is a bucket handle tear. Think of a bucket handle. You can flip it from one side of the bucket to the other. The same thing occurs inside the knee. The entire meniscus tears, and the entire c shaped disc flips over and sits in front of the knee. Figure 4 below shows a bucket handle tear where the entire meniscus is sitting in front of the femur.
Meniscus tears occur along with other knee injuries, such as anterior cruciate ligament tears, especially in sports. If players squat and twist the knee or have direct contact (like a tackle), it can cause a meniscus tear.
Degenerative meniscus tears occur more often in older people. Cartilage wears thin and weakens over time and is more prone to tears. When the menisci have weakened with age something as simple as an awkward twist when getting up from a chair can be enough to cause a tear.
Figure 3. Meniscus tears types
Unstable versus stable meniscus tear
Similar to how the type of meniscus tear can determine whether or not your meniscus tear is repairable — The various types of meniscus tears you have will determine how much the meniscus tear will bother you. In general, large unstable tears (radial tears, flap tears and bucket handle tears) tend to remain bothersome, whereas degenerative tears typically do not produce significant ongoing discomfort. When you look at a degenerative tear, the edges are simply frayed. The tissue has been worn out from years and years of use. Nothing you did wrong. The tissue simply wore out.
Then there are those who have one of the other acute tears. The size, shape and type of meniscus tear will determine whether or not the meniscus tear is “stable” or “unstable” — and thus help your surgeon determine whether or not your pain will improve or persist. If a loose flap of tissue is created and that flap is moving around within your knee—that’s when you’re going to have giving way and you’re going to have pain with many activities. You’re not going to tolerate meniscus flap tears well and those patients with meniscus flap tears (or unstable meniscus tears) will usually (not always) go on to require an arthroscopy or a scope to try to either repair or remove that torn piece.
Most people with degenerative meniscus tears may have one or two exacerbations or periods during the year where their knee hurts — but, by and large they get around just fine and lead very active lifestyles with these degenerative tears and do not require surgery (arthroscopy) for treatment of those tears.
Bucket Handle Meniscus Tear
A bucket handle meniscus tear is a unique type of meniscus tear. Bucket handle meniscus tears are more common in younger athletes. Bucket handle meniscus tears can occur in older adult athletes too, but most bucket handle meniscus tears occur in people under 35 years of age. Bucket handle meniscus tears are unique because they are very large tears. In addition to being large, the torn part tends to flip over on itself and become stuck in the middle of the knee joint. If the meniscus flips over it can make it very painful to walk, and it can make it impossible to fully straighten your knee.
The injury is usually non-contact and involves twisting or pivoting. You may have felt a pop when the meniscus tore. Most patients with a large meniscus tear such as a bucket handle or flap tear will develop significant swelling or bleeding in the knee joint. A bucket handle meniscus tear is a unique type of tear. It represents a complete tear of the meniscus support or the ligament that holds the meniscus in place. Without the support that holds the meniscus in place, the meniscus can flop over like the handle on a bucket. When the meniscus flips over it becomes stuck in the middle of the knee joint. That results in a loss of motion, because the meniscus is physically blocking you from fully straightening your knee. If you lose the ability to fully straighten the knee then you have a “locked knee”. Many people with a locked knee are found to have a large piece of meniscus which has flipped into the middle of the knee joint.
Figure 4. Bucket handle meniscus tear

Bucket Handle Meniscus Tear Symptoms
Bucket handle tears of the meniscus tend to cause significant swelling and pain when they initially tear. After the initial swelling goes down you will usually find that you can not straighten the knee. This is what we refer to as a locked knee. That’s because the torn bucket handle meniscus tear is stuck in the center of the knee and is physically blocking the knee from straightening. Because of the loose piece of meniscus you will notice a lot of popping, and you will have the sensation that something is stuck deep inside the knee. The knee simply feels very abnormal.
Many patients with a bucket handle meniscus tear will also complain that the knee feels loose or unstable. They will notice a lot of clunking or catching too.
How Is A Bucket Handle Meniscus Tear Treated?
Most patients with a bucket handle meniscus tear will need to be treated surgically via an arthroscopy. During an arthroscopy, we put a small camera in the knee to see the meniscus tear. Again, these tears are usually flipped over and stuck in the middle of the knee. The first thing we do is to put the tear back into its normal position. Then we look at the tear and see if it is repairable. Most bucket handle tears are able to be repaired by placing sutures or stitches in it. A repair is preferred over a removal of the torn piece. We want to try and repair these, because if we do not repair it and we trim a bucket handle tear out, then you will lose a lot of your meniscus and you will be at high risk for developing osteoarthritis. While many bucket handle tears can be repaired, others can not be repaired. The decision whether or not it can be repaired is made at the time of surgery when we are looking at the meniscus. If the meniscus has a good chance of healing then we will proceed to repair it. If we do not believe that the meniscus will heal then we need to remove the torn piece.
Recovery After A Bucket Handle Meniscus Tear
After surgery, you might be on crutches for a short while to protect the stitches and allow the meniscus to heal. After therapy and waiting enough time for the meniscus to heal, many athletes can enjoy a full return to activities after repair of a bucket handle tear. Return to sports after the repair of a bucket handle meniscus tear can take 4-6 months or more.
Meniscus tear causes
Sudden meniscus tears often happen during sports. Players may squat and twist the knee, causing a tear. Direct contact, like a tackle, is sometimes involved.
Older people are more likely to have degenerative meniscus tears. Cartilage weakens and wears thin over time. Aged, worn tissue is more prone to tears. Just an awkward twist when getting up from a chair may be enough to cause a tear, if the menisci have weakened with age.
Meniscus tears usually happen because of an injury — often after twisting or turning the knee while it is bent and the foot is firmly planted. This might happen when:
- lifting heavy objects
- making sudden changes in direction or slowing or stopping quickly, as can happen in sports like soccer, baseball, basketball, tennis, and racquetball
- taking a direct hit to the knee while playing a contact sport, such as football, hockey, or rugby, where the knee may be forced to twist or turn awkwardly
- falling in a way that puts a lot of strain on the knee during a fall, as can happen in sports like skiing or snowboarding
Meniscus tears often happen along with other knee injuries such as ligament tears.
Can I prevent a meniscus tear?
Because they generally happen without any warning, meniscus tears can be hard to prevent. You can reduce your risk, though, by taking these precautions:
- Get regular exercise, including strength training for your leg muscles. Strong leg muscles help stabilize and protect the knee.
- Always warm up and stretch properly before playing sports or engaging in any strenuous activity involving your legs.
- Give your muscles plenty of time to rest and recover between activities.
- Get the right footwear for your sport, and keep shoes, boots, or skates laced up tight while you play.
- Learn and use the proper techniques for your sport.
- If you’ve previously had another knee injury, a brace or wrap can give your knee added support.
Meniscus tear signs and symptoms
You might feel a “pop” when you tear a meniscus. Most people can still walk on their injured knee. Many athletes keep playing with a tear. Over 2 to 3 days, your knee will gradually become more stiff and swollen. Someone who gets a minor tear may only have slight pain and swelling that goes away after 2 or 3 weeks.
The most common symptoms of meniscus tear are:
- Pain
- Stiffness and swelling
- Catching or locking of your knee
- The sensation of your knee “giving way”
- You are not able to move your knee through its full range of motion
Without treatment, a piece of meniscus may come loose and drift into the joint. This can cause your knee to slip, pop, or lock.
Meniscus tear test
After discussing your symptoms and medical history, your doctor will examine your knee. He or she will check for tenderness along the joint line where the meniscus sits. Tenderness along the joint line often signals a tear.
One of the main tests for meniscus tears is the McMurray test. Your doctor will bend your knee, then straighten and rotate it. This puts tension on a torn meniscus. If you have a meniscus tear, this movement will cause a clicking sound. Your knee will click each time your doctor does the test.
Imaging Tests
Because other knee problems cause similar symptoms, your doctor may order imaging tests to help confirm the diagnosis.
X-rays. Although x-rays do not show meniscus tears, they may show other causes of knee pain, such as osteoarthritis.
Magnetic resonance imaging (MRI). This study can create better images of the soft tissues of your knee joint, like a meniscus. The popularity of the MRI is due to its being noninvasive, and the >90% accuracy in detecting meniscal tears.
Meniscus tear treatment
How your orthopaedic surgeon treats your tear will depend on the type of tear you have, its size, and location.
The outside one-third of the meniscus has a rich blood supply. A tear in this “red” zone may heal on its own, or can often be repaired with surgery. A longitudinal tear is an example of this kind of tear.
In contrast, the inner two-thirds of the meniscus lacks a blood supply. Without nutrients from blood, tears in this “white” zone cannot heal. These complex tears are often in thin, worn cartilage. Because the pieces cannot grow back together, tears in this zone are usually surgically trimmed away.
Along with the type of tear you have, your age, activity level, and any related injuries will factor into your treatment plan.
Nonsurgical Treatment
If your tear is small and on the outer edge of the meniscus, it may not require surgical repair. As long as your symptoms do not persist and your knee is stable, nonsurgical treatment may be all you need.
RICE. The RICE protocol is effective for most sports-related injuries. RICE stands for Rest, Ice, Compression, and Elevation.
- Rest. Take a break from the activity that caused the injury. Your doctor may recommend that you use crutches to avoid putting weight on your leg.
- Ice. Use cold packs for 20 minutes at a time, several times a day. Do not apply ice directly to the skin.
- Compression. To prevent additional swelling and blood loss, wear an elastic compression bandage.
- Elevation. To reduce swelling, recline when you rest, and put your leg up higher than your heart.
Take non-steroidal anti-inflammatory medicines. Drugs like aspirin and ibuprofen reduce pain and swelling.
If your doctor prescribes it, do physical therapy. Physical therapy can help you strengthen your leg muscles, stabilize your knee, and get your knee back to its full range of motion and flexibility.
For severe tears or tears that don’t respond to other forms of treatment, a doctor may have to perform surgery. Usually, this will be in the form of arthroscopic surgery, where a small camera is inserted into the knee to help surgeons see what they’re doing without having to open the knee up.
Meniscus tear surgery
If your symptoms persist with nonsurgical treatment, your doctor may suggest arthroscopic surgery.
Knee arthroscopy is one of the most commonly performed surgical procedures. In it, a miniature camera is inserted through a small incision (portal). This provides a clear view of the inside of the knee. Your orthopaedic surgeon inserts miniature surgical instruments through other portals to trim or repair the tear.
- Partial meniscectomy. In this procedure, the damaged meniscus tissue is trimmed away.
- Meniscus repair. Some meniscus tears can be repaired by suturing (stitching) the torn pieces together. Whether a tear can be successfully treated with repair depends upon the type of tear, as well as the overall condition of the injured meniscus. Because the meniscus must heal back together, recovery time for a repair is much longer than from a meniscectomy.
Once the initial healing is complete, your doctor will prescribe rehabilitation exercises. Regular exercise to restore your knee mobility and strength is necessary. You will start with exercises to improve your range of motion. Strengthening exercises will gradually be added to your rehabilitation plan.
For the most part, rehabilitation can be carried out at home, although your doctor may recommend physical therapy. Rehabilitation time for a meniscus repair is about 3 months. A meniscectomy requires less time for healing — approximately 3 to 4 weeks.
Meniscus tear recovery time
Recovery from an arthroscopy to remove the torn meniscus is relatively short. It is a minimally invasive outpatient surgery with typically 2 to 3 small puncture wounds to perform the surgery. The patient will typically be weight bearing as tolerated, but he/she may need to use crutches for a few days following the surgery. Swelling typically improves during the first week. Patients with sedentary jobs can return within one to two days. More physical laborers may take longer to recover. Patients typically return to sports or exercise by 4 to 6 weeks following a short period of physical therapy.
The physical therapy following meniscal repair varies depending on a number of factors. Most patients can put weight on the knee soon after surgery, although a brace may be used. Running is usually delayed until 3-4 months after surgery while a full return to sports and squatting typically occurs after 4-6 months.
When the repair of the meniscus is not possible, the torn area is removed through the scope during surgery. Because the meniscus does not have to heal immediate weightbearing is allowed. Running and jogging is typically allowed after 2-4 weeks and sports shortly after.
Key factors that will influence meniscal tear recovery after surgery
There are many factors that will determine how quickly, or completely you recover from your meniscal tear surgery. Key elements include your age, weight, and activity demands. The older you are, and the heavier you are, the longer your recovery will be.
The type of surgery you had will also impact upon your recovery. In some cases we only remove the torn piece, that procedure is called a partial menisectomy. In general you should progress faster following a partial menisectomy than someone who had sutures placed to repair the meniscus tear. That’s because a repair might take longer to heal.
If you have osteoarthritis and a meniscus tear you should anticipate a more rocky recovery. Arthritis found at the time of your meniscus surgery will also significantly influence your recovery following an arthroscopy. If you have arthritis then you are missing some or all of the cartilage on the ends of the bones. Knees with arthritis are prone to being more “cranky” during the recovery process. In those cases, an ice compression device can provide temporary relief of pain/swelling. Many patients note they also feel better wearing a compression sleeve during recovery. People with arthritis sometimes report improvement in their symptoms with supplements like glucosamine, curcumin, or hyaluronic acid which they believe (not proven) will smooth out the surface of the joint.
Some of the variables affecting your recovery from meniscus surgery are under your surgeon’s control. Your surgeon can improve your immediate response after surgery with the use of various medications they inject within your knee before the surgery. Your surgeon can also block a nerve on the side of your leg which will improve your pain for 18-24 hours after surgery. A knee brace can be protective after surgery and make the knee feel more stable. Perhaps the best predictor of who will do well after surgery is proper patient selection. Meniscus surgery in patients who are obese, have arthritis, and poorly controlled diabetes tend to do very poorly after surgery.
In general, young, healthy active people with no evidence of osteoarthritis will experience a much more rapid recovery. In many cases the knee will feel better within a few days. Most people are off crutches in a day, and stop taking pain medicine within a day or two. In contrast, if you are a older, heavier and have arthritis as well as a meniscus tear, then you may take much longer to recover. In addition, is you have had a partial menisectomy and also have osteoarthritis you may not experience a “full” recovery.
Discussing the realistic goals of surgery with your surgeon is critical here. You may think that you will be able to return to running 8 miles a day. That might not be your surgeon’s goals for you. Be sure to dive into this before having surgery.
Improve your health before surgery
To ensure a good response to surgery, your surgeon also need to look at your health before surgery. Smoking leads to an increased infection rate and poorer healing. Diabetics with poor sugar control are at higher risk for infection and delays in healing as well. Obesity is a potential problem with anesthesia, the recovery from surgery and it may lead to more rapid progression of arthritis after surgery. The better shape you are in prior to surgery will have an influence on your recovery.
Movement of the knee is encouraged during recovery from your meniscal surgery.
After surgery you may be hesitant to get up and move about. No matter how hesitant, you should actually be encouraged to move around as much as tolerated. This is important because it minimizes muscle atrophy, minimizes the risk of blood clots, and helps your lungs recover from the anesthesia. However, there are also some limitations to be expected. For example, if you had a meniscus repair surgery your surgeon may ask you to use crutches and avoid deep squats or pivoting and twisting on that leg for a few weeks. But if you simply had the piece cleared out of the knee, then you can resume fairly normal activities as tolerated. Consider a cryo cuff and compression sleeve to minimize swelling which will improve your motion. Once cleared by your surgeon, certain exercises are helpful for recovery. Be sure to check with your surgeon first — then you will find these videos on quadriceps knee exercises and these hamstring exercises useful.
What are the long term success rates for the surgeries?
Overall, the long-term success rates for meniscal repairs vary from 84% to 94%. The success rate decreases when the knee is unstable, such as when there is an ACL tear. This is why if there is an ACL tear. This is why if there is an ACL tear with meniscal tear, both structures should be surgically repaired or reconstructed.
Can the meniscal get torn a second time?
Yes and the same issues dictate whether the meniscus can be repaired or removed.
- Yim, J.-H., Seon, J.-K., Song, E.-K., Choi, J.-I., Kim, M.-C., Lee, K.-B., & Seo, H.-Y. (2013). A Comparative Study of Meniscectomy and Nonoperative Treatment for Degenerative Horizontal Tears of the Medial Meniscus. The American Journal of Sports Medicine, 41(7), 1565–1570. https://doi.org/10.1177/0363546513488518[↩]
- Increased risk for knee replacement surgery after arthroscopic surgery for degenerative meniscal tears: a multi-center longitudinal observational study using data from the osteoarthritis initiative. Rongen, J.J. et al. Osteoarthritis and Cartilage , Volume 25 , Issue 1 , 23 – 29 https://www.oarsijournal.com/article/S1063-4584(16)30292-8/pdf[↩]
- Arthroscopic Partial Meniscectomy versus Sham Surgery for a Degenerative Meniscal Tear. New England Journal of Medicine December 26, 2013 369(26):2515 https://www.nejm.org/doi/full/10.1056/NEJMoa1305189[↩]





{kind=link}