Contents
- What is spinal stenosis
- Types of spinal stenosis
- Lumbar spinal stenosis
- Cervical spinal stenosis
- Spinal stenosis causes
- Spinal stenosis symptoms
- Spinal stenosis complications
- Spinal stenosis diagnosis
- Spinal stenosis treatment
- Spinal stenosis prognosis
What is spinal stenosis
Spinal stenosis is also called spinal canal stenosis, is a narrowing of the spinal canal in which the spinal cord sits, which can cause pain and weakness in your arms or legs. The narrowing can put pressure or compress on the spinal cord and the spinal nerve roots, leading to symptoms such as pain, numbness, and weakness. Spinal stenosis occurs most often in the lower back and the neck. Some people with spinal stenosis may not have symptoms. Others may experience pain, tingling, numbness and muscle weakness. Symptoms can worsen over time.
Spinal stenosis is often caused by arthritis or disc prolapse. As well, some people are born with a congenitally narrowed spinal canal. The spinal cord can be directly compressed by osteophytic bones and ligamentous hypertrophy. Compression of local vascular structures can lead to ischemia of the spinal cord from arterial insufficiency and venous stasis. A herniated disk can exert repeated local trauma to the spinal cord or nerve root during repetitive flexion and extension movements, especially in the unstable spine with multiple levels of subluxations.
Spinal stenosis most commonly is caused by degenerative osteoarthritis of the spine or spondylosis and occurs most frequently at the L4 to L5 level, followed by L5 through S1 and L3 to L4. Additional risk factors include obesity or a family history of this condition. Other factors such as disc protrusion or bulging (for example, caused by progressive disc degeneration with aging or trauma), loss of disc height, facet joint arthropathy, osteophyte formation, or ligamentum flavum hypertrophy can all lead to encroachment on and narrowing of the central canal and neural foramina.
Spondylolisthesis, the translation of one vertebral body anteriorly or posteriorly relative to an adjacent vertebral body, may also exacerbate spinal canal narrowing.
Additional acquired causes of spinal stenosis include space-occupying lesions such as synovial or neural cysts, neoplasms, or lipomas; traumatic or postoperative changes such as fibrosis; and skeletal diseases such as ankylosing spondylitis, rheumatoid arthritis, or Paget disease.
Congenital or developmental causes of spinal stenosis include dwarfism namely achondroplasia, Morquio’s syndrome, and spinal dysraphism such as spina bifida, spondylolisthesis, and myelomeningocele.
Spinal stenosis occurs mostly in people older than 50, caused by wear-and-tear changes in the spine related to osteoarthritis. Younger people with a spine injury or a narrow spinal canal are also at risk. Diseases such as arthritis and scoliosis can cause spinal stenosis, too. Spinal stenosis symptoms might appear gradually or not at all. They include:
- Pain in your neck or back
- Numbness, weakness, cramping, or pain in your arms or legs
- Pain going down the leg
- Foot problems
Doctors diagnose spinal stenosis with a physical exam and imaging tests. Treatments include medications, physical therapy, braces, and surgery.
The upper neck (cervical) and lower back (lumbar) areas most frequently are affected, although the thoracic spine also can be compressed most frequently by a disk herniation. Three different anatomic sites in the spine can be affected by spinal stenosis. First, the central canal, which houses the spinal cord, can be narrowed in an anterior-posterior dimension, leading to compression of neural elements and reduction of blood supply to the spinal cord in the cervical area and the cauda equina in the lumbar area 1. Secondly, the neural foramen, which are openings through which the nerve roots exit the spinal cord, can be compressed as a result of disk herniation, hypertrophy of the facet joints and ligaments, or unstable slippage of one vertebral body relative to the level below 1. Lastly, the lateral recess, which is seen in the lumbar spine only and is defined as the area long the pedicle that a nerve root enters just before its exit through the neural foramen, can be compressed from a facet joint hypertrophy 1. Depending on the level of the spine affected, each type of compression can lead to different symptoms that warrant a particular treatment modality.
See your doctor if you have symptoms of spinal stenosis.
More serious symptoms that need prompt attention include:
- Difficulty or poor balance when walking
- Worsening numbness and weakness of your limb
- Problems controlling urine or bowel movements
- Problems urinating or having a bowel movement
Figure 1. Spinal cord
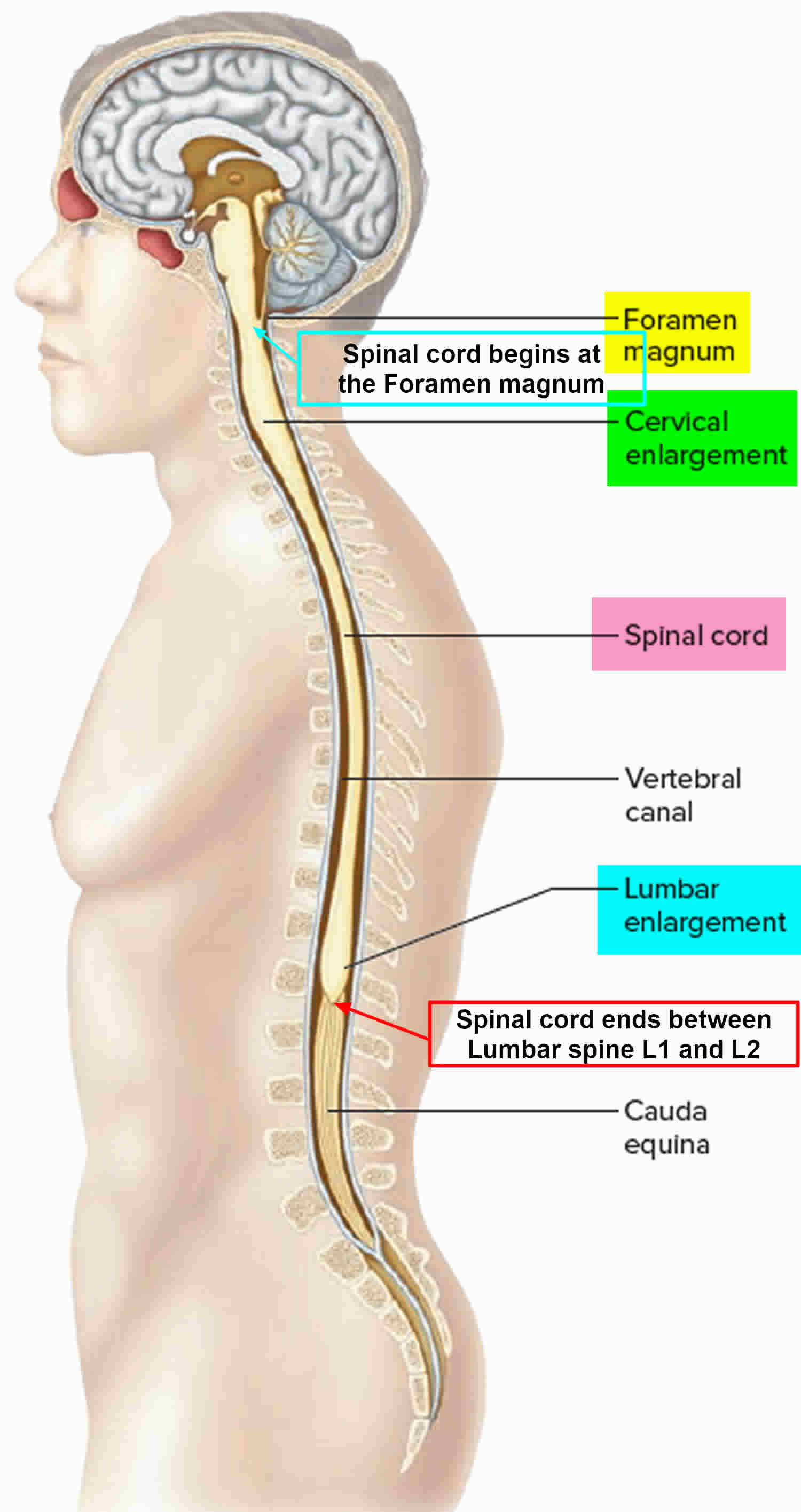
Figure 2. Spinal cord segments
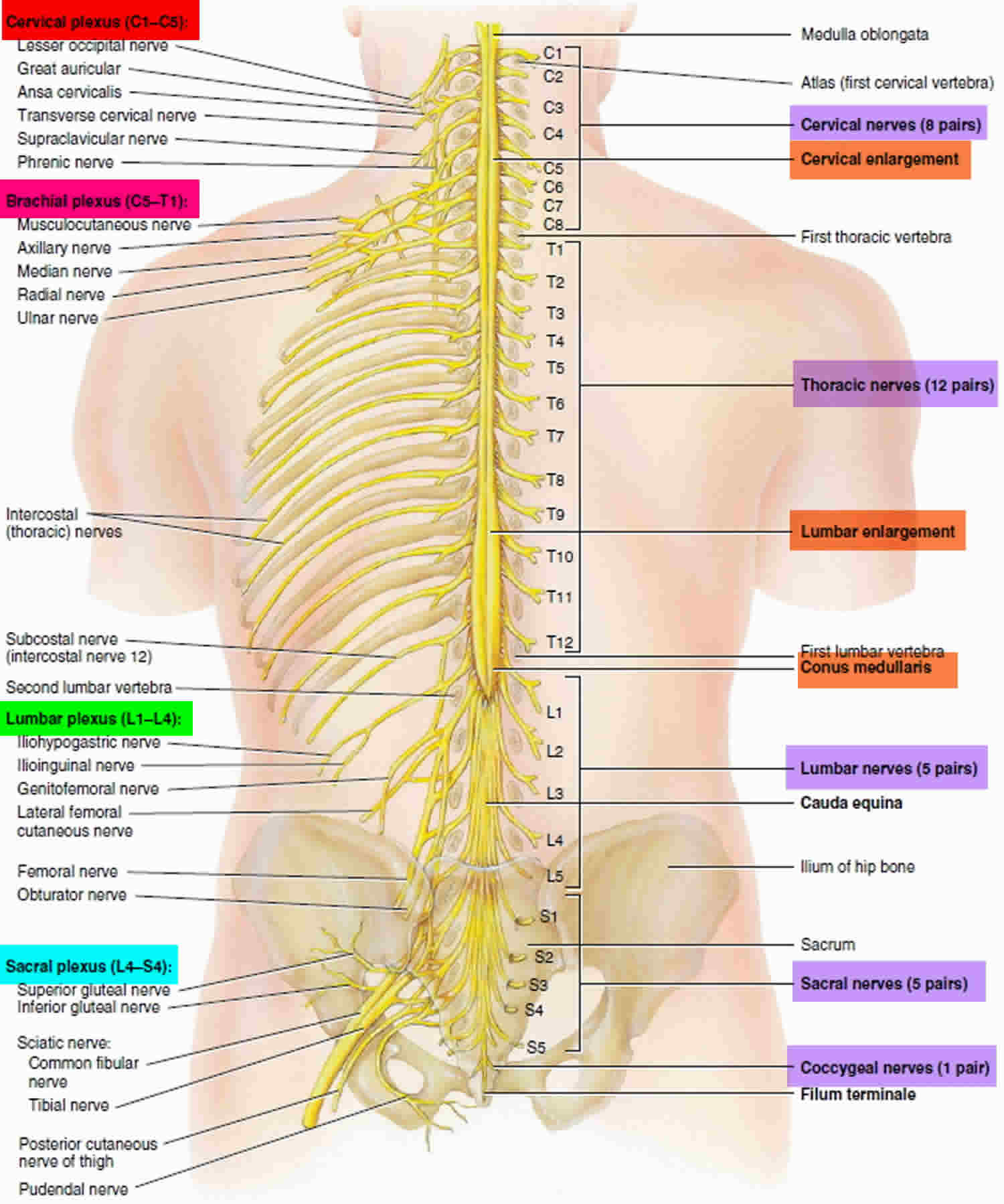
Figure 3. Spinal cord skin innervations
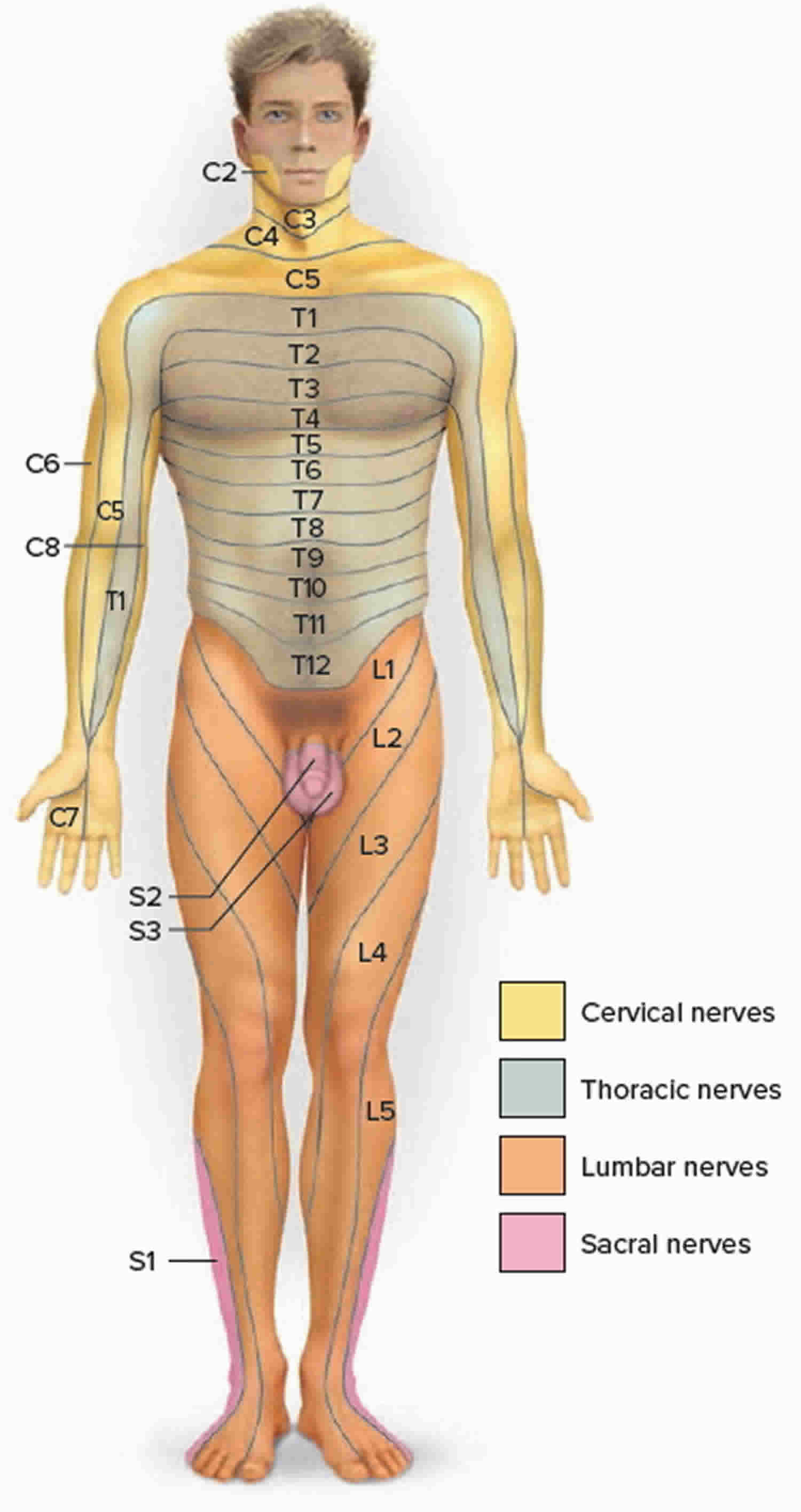 Figure 4. Spinal cord anatomy
Figure 4. Spinal cord anatomy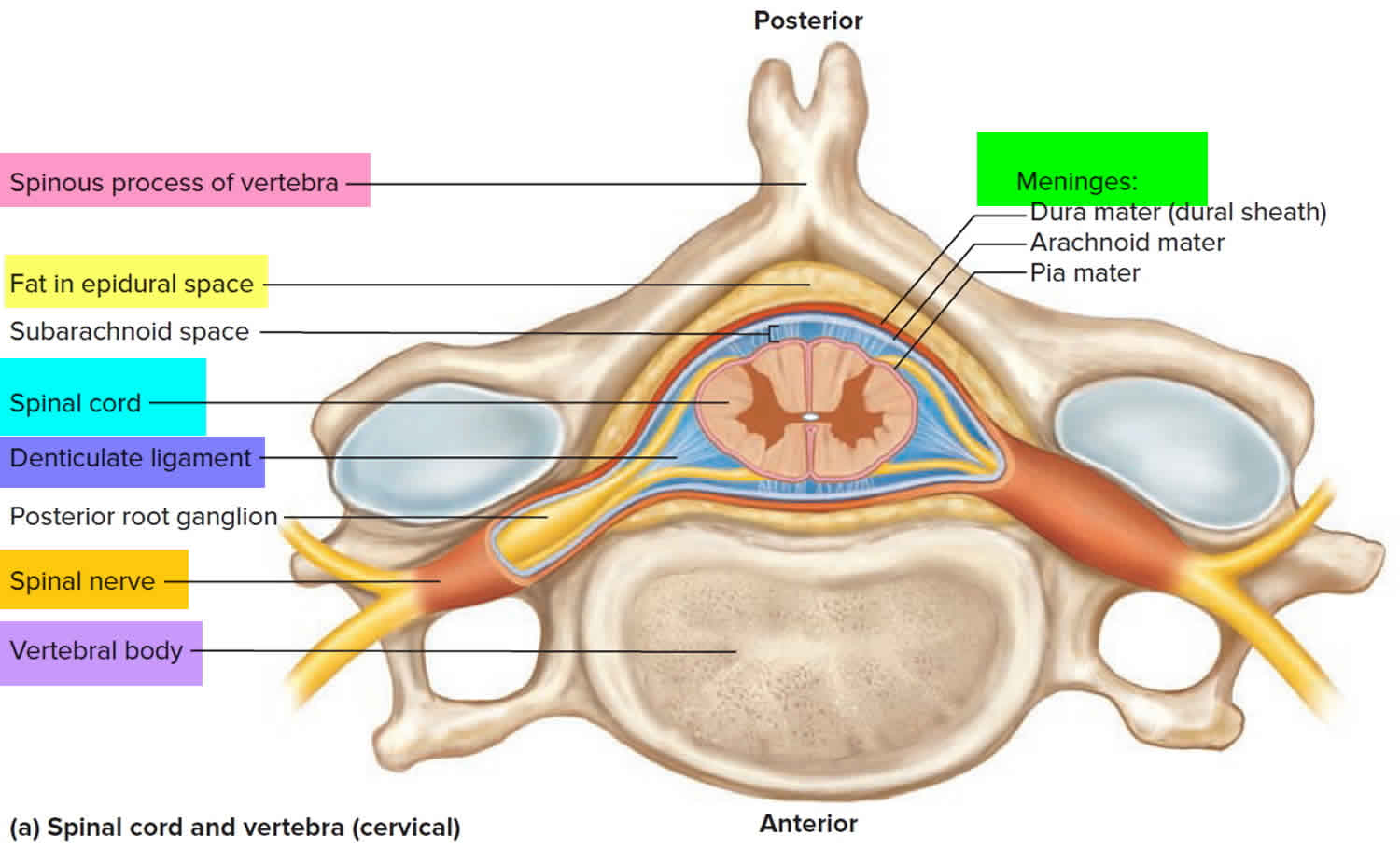
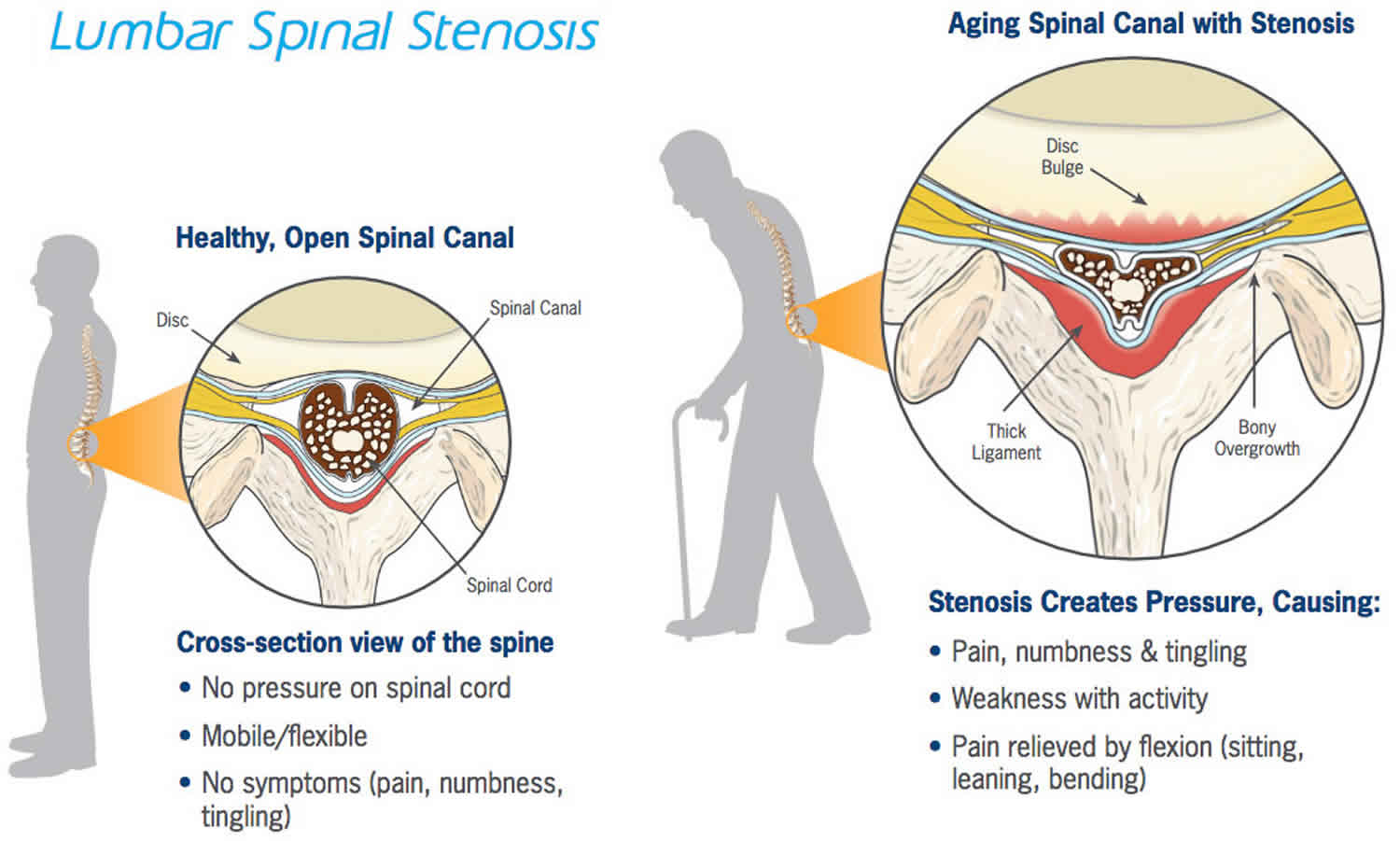
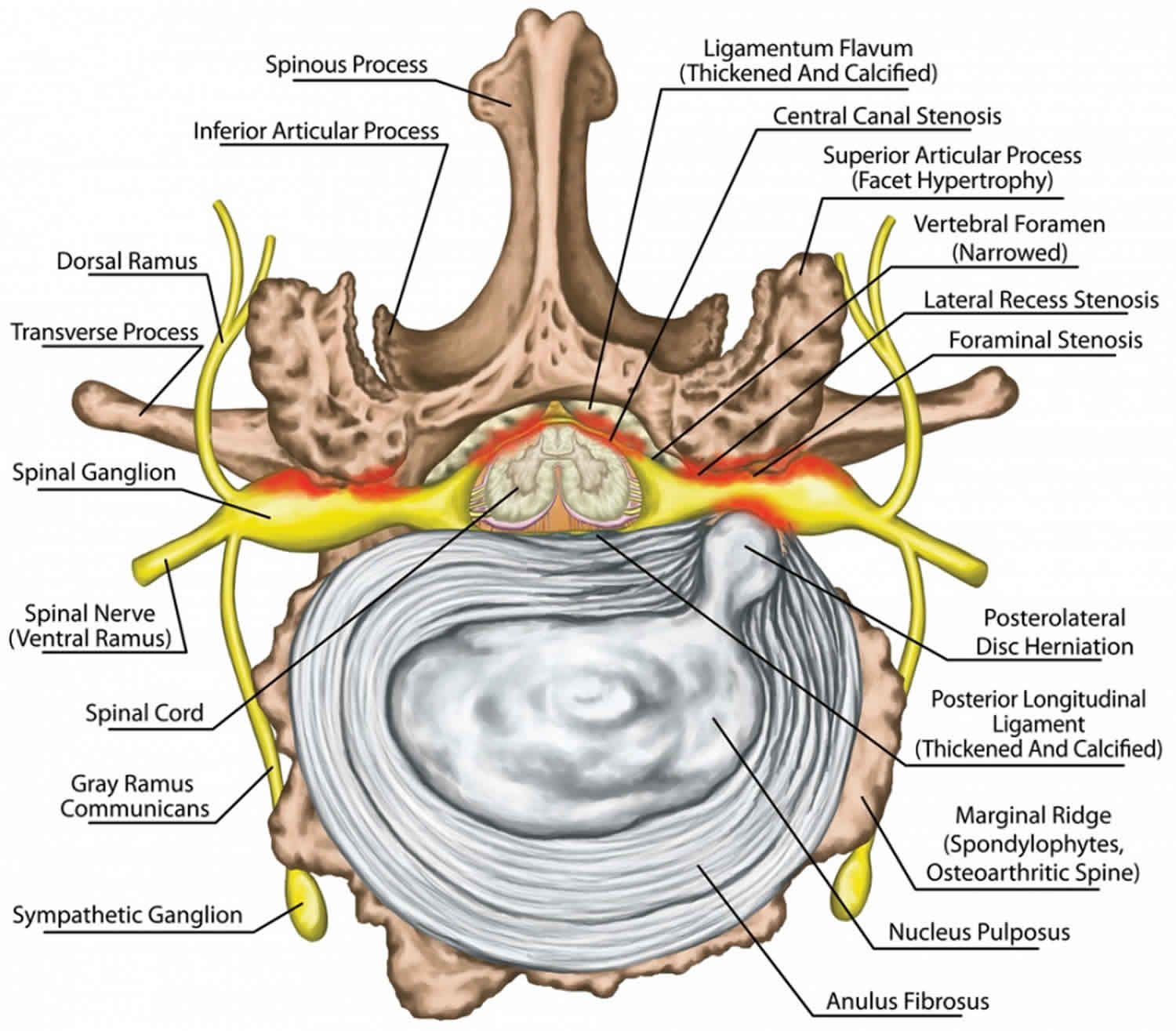
Figure 5. Spinal stenosis
Types of spinal stenosis
The types of spinal stenosis are classified according to where on the spine the condition occurs. It’s possible to have more than one type. The two main types of spinal stenosis are:
- Lumbar stenosis. Lumbar spinal stenosis is where the spinal canal narrows in the part of the spine in your lower back. This may cause pain or weakness in your legs. Lumbar spinal stenosis is the most common form of spinal stenosis. The prevalence of acquired lumbar spinal stenosis was 19.4%, for population aged between 60–69 years. In a Japanese population-based study where subjects underwent a symptoms questionnaire to predict lumbar stenosis, it was found that incidence increased with age, with 1.7–2.2% between ages 40-49, and 10.3%–11.2% between ages 70 to 79 2. It is also a significant contributor to spinal surgery in the US, 5.9 per 100 patients progressed to lumbar fusion within 1 year from the time of diagnosis of lumbar degeneration 3.
- Cervical stenosis. Cervical spinal stenosis is where the spinal canal narrows in the part of the spine in your neck, causing weakness or numbness in your arms and legs.
Lumbar spinal stenosis
Lumbar spinal stenosis is where the spinal canal narrows in your lower back. It refers to a narrowing in the vertebra, in the areas of the central canal, lateral recess or the neural foramen. A narrowed spinal canal means that there is not enough space for the nerves and blood vessels. You may have difficulty walking and leg pain.
Lumbar spinal stenosis is a common source of leg and back pain 4. Despite its prevalence, currently, there is no universally accepted definition of lumbar spinal stenosis, and there is also a lack of generally accepted radiologic diagnostic criteria 5. Lumbar spinal stenosis is a significant cause of disability in the elderly, and it is the most significant cause of spinal surgery in patients over 65 years of age 6.
The causes of neurologic symptoms of lumbar spinal stenosis have been thought to originate from the compression and ischemia of nerve roots. Nerve root compression can originate from direct mechanical compression or increased intrathecal pressure due to the narrowing of the canal. Inflammation of nerve roots is also a plausible but less likely mechanism of neurologic symptoms in lumbar spinal stenosis 7.
Lumbar spinal stenosis causes
Degenerative spondylosis is a significant cause of lumbar spinal stenosis. With aging, wear-and-tear changes and traumas, amongst other factors, the intervertebral discs can degenerate and protrude posteriorly, causing increased loading of the posterior elements of the vertebrae. This can lead to posterior vertebral osteophyte formation (uncinate spurs), facet hypertrophy, synovial facet cysts, and ligamentum flavum hypertrophy, which in turn will cause spinal stenosis.
Degenerative spondylolisthesis is another cause of lumbar spinal stenosis. When degenerative changes of the spine occur, the pars interarticularis can be fractured, and the resulting instability can lead to forward translation of the vertebra. Sufficient anterior slippage of one vertebra on top of the next vertebral segment (most commonly L4-on-L5) can narrow the spinal canal, leading to stenosis.
Other acquired conditions, although rarer than the aforementioned conditions, should also be considered by the clinician. These include space-occupying lesions, post-surgical fibrosis, and rheumatologic conditions as well as other skeletal diseases such as ankylosing spondylitis or diffuse idiopathic skeletal hyperostosis 8.
Even more rarely, lumbar spinal stenosis may be secondary to congenital causes such as achondroplasia, which can lead to short pedicles with medially placed facets.
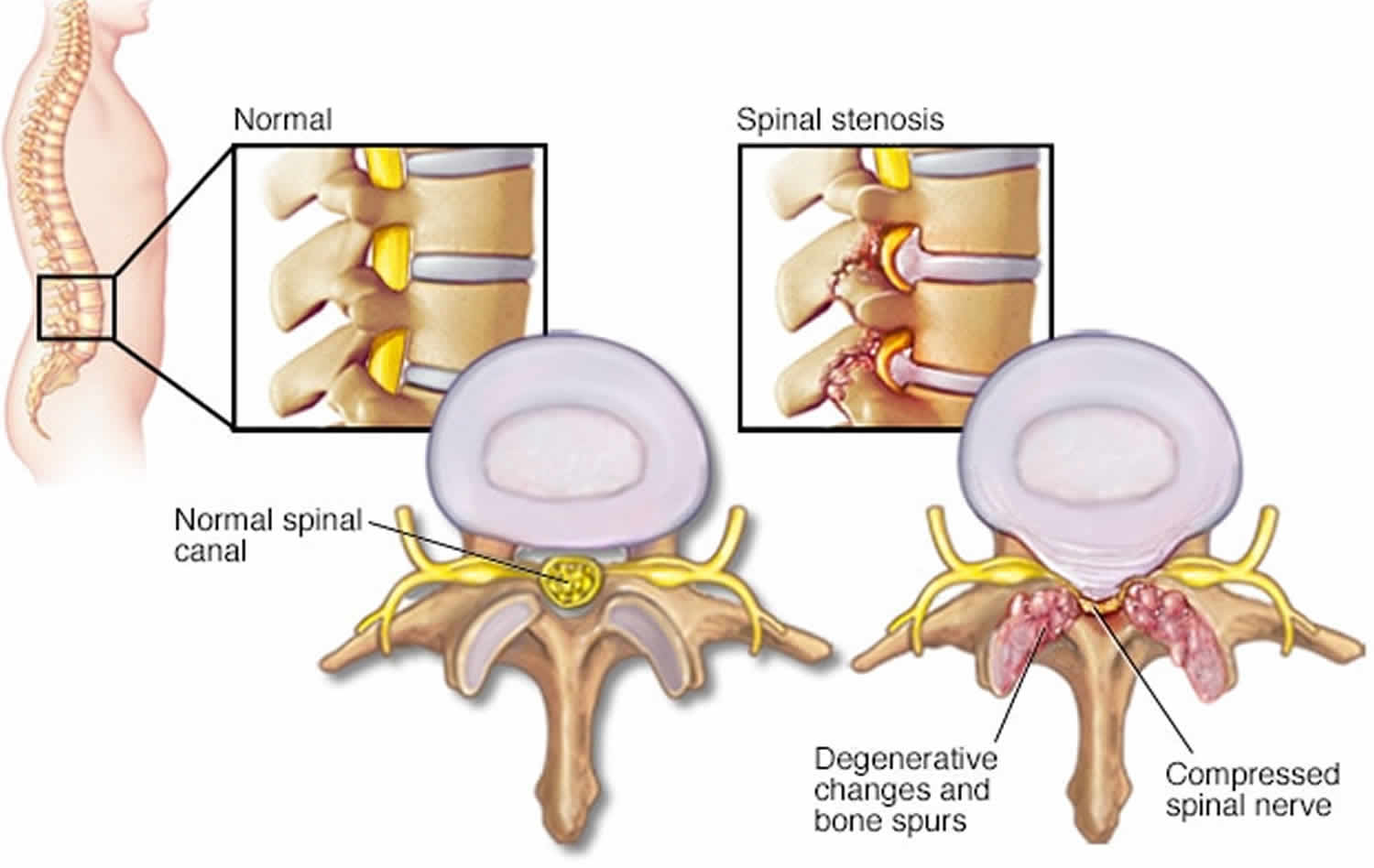
Figure 6. Lumbar spinal stenosis
Lumbar spinal stenosis symptoms
In the lower back (lumbar spine) spinal stenosis symptoms include:
- Numbness or tingling in a foot or leg
- Weakness in a foot or leg
- Pain or cramping in one or both legs when you stand for long periods of time or when you walk, which usually eases when you bend forward or sit
- Back pain
Classically, lumbar spinal stenosis presents as pain exacerbated by prolonged ambulation, standing, and with lumbar extension, and is relieved by forward flexion and rest. Neurogenic claudication is an important feature of lumbar spinal stenosis. Symptoms are typically bilateral, but usually asymmetric. Low back pain, numbness, and tingling are present in a majority of patients. Numbness and tingling in lumbar spinal stenosis involve usually the entire leg, and rarely involves only a single nerve root distribution 9. Approximately 43 percent of the patients experience weakness. Patients may also report walking upstairs being easier than walking downstairs, as the back is forward flexed with stairs climbing. If patients present with new-onset bowel or bladder dysfunction, saddle anesthesia, bilateral lower extremity weakness and/ or increased lower extremity, the patient may have developed cauda equina or conus medullaris syndromes.
A thorough physical examination should be performed on patients with suspected lumbar spinal stenosis. Pain with passive and active lumbar extension can be elicited. Although it is possible that patients can have superimposed lumbar radiculopathy, it should be noted that neurologic examinations on patients with lumbar spinal stenosis are typically normal, and only 10 percent of patients would present with a positive straight leg raise test 10. Pedal pulses should also be checked during physical exam as vascular claudication can present similarly.
Stenosis in the lumbar spine can lead to neurogenic claudication, myeloradiculopathic symptoms, sensory disturbances, motor weakness, and pathologic reflexes. Disk herniation is most common at the L4-5 and L5-S1 levels. A herniated disk at L5-S1 can lead to plantarflexion weakness, decrease sensation in the lateral foot, and cause pain in the posterior leg. A disk herniation at L4-5 can lead to a foot drop and numbness in the large toe web and dorsal aspect of the foot. Lastly, an L3-4 disk herniation can lead to knee extension weakness, numbness in the medial foot, and pain in the anterior thigh.
Lumbar spinal stenosis treatment
Management for lumbar spinal stenosis is aimed at reducing symptoms and improving functional status. Conservative treatment is the first-line treatment for this condition. Conservative treatment options include physical therapy, oral anti-inflammatory medications, and epidural steroid injections. Although there is no standardized physical therapy regimen, many therapists focus on stretching and strengthening of the core muscles, which can lead to correction of posture and improved symptom 11. Although there are short-term benefits, lumbar epidural steroid injections have not been shown to have long-term improvement of pain and disability in lumbar spinal stenosis patients, and there is no statistical difference between epidural injections with anesthetics alone versus a mixture of anesthetics with corticosteroids 12. Lumbar corsets may also be trialed for temporary relief of pain 13.
Barring emergencies such as cauda equina syndrome, surgical management for lumbar spinal stenosis is usually elective, as the goal of treatment is to improve function, rather than preventing neurologic impairment. The most frequently performed surgical procedure is laminectomy. A randomized trial has shown that there is a greater improvement of symptoms in patients undergoing laminectomy compared to the non-surgical group 14, however, the symptom improvement between the surgical and non-surgical groups diminish over time. Laminectomy with fusion is typically reserved for patients with concurrent spondylolisthesis to provide further stability. A less invasive approach is interspinous spacer implantation, this procedure is appropriate for patients with intermittent claudication symptoms without spondylolisthesis.
Lumbar spinal stenosis prognosis
Lumbar spinal stenosis is a significant cause of pain and disability, and approximately half the patients have involvement of other spinal segments over time; however, it typically follows a benign course. In one cohort study, 30% of patients electing to manage lumbar spinal stenosis with non-surgical procedures eventually requested for surgical management, and approximately 19% of patients who had an initial surgery eventually underwent a repeat surgery 15.
Cervical spinal stenosis
Cervical spinal stenosis is where the spinal canal narrows in your neck. A narrowed spinal canal in your neck can press on your spinal cord, preventing it from working properly. The condition can also trap the nerves. This may cause weakness or numbness in your arms and legs.
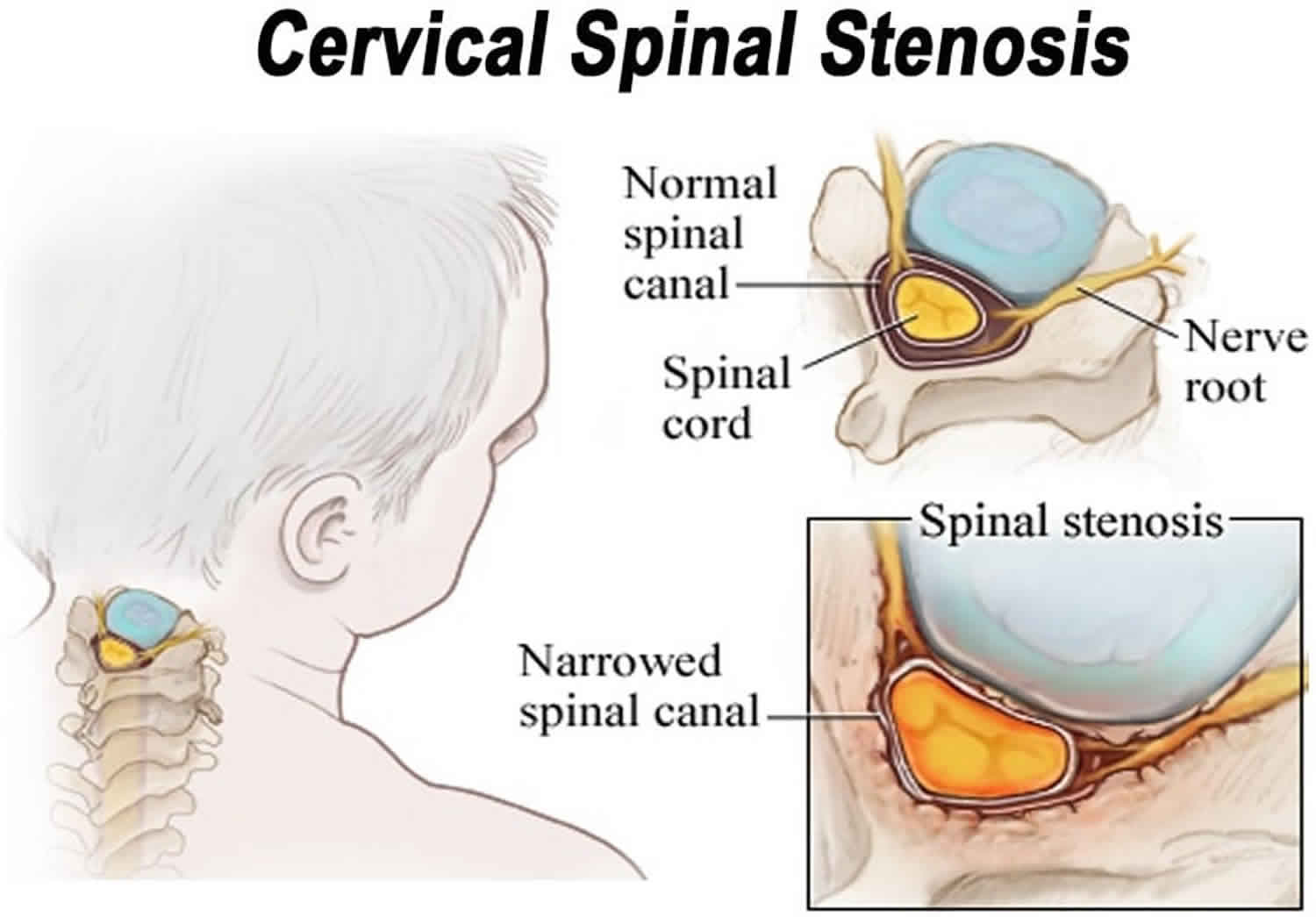
Figure 7. Cervical spinal stenosis
Cervical spinal stenosis symptoms
In the neck (cervical spine) spinal stenosis symptoms include:
- Numbness or tingling in a hand, arm, foot or leg
- Weakness in a hand, arm, foot or leg
- Problems with walking and balance
- Neck pain
- In severe cases, bowel or bladder dysfunction (urinary urgency and incontinence)
Stenosis in the cervical spinal can lead to radicular symptoms due to nerve root compression and myelopathy due to spinal cord compression. Radicular symptoms are dependent on the level affected, with the nerve root affected being the one that exists at that level. For example, a C5-6 disk herniation leads to a C6 radiculopathy. C6-7 disk herniation is the most common, leading to a wrist drop and paresthesia in the 2 and three fingers. C5-6 disk herniation is the next common, resulting in weakness in forearm flexion and paresthesia in the thumb and radial forearm. C7-T1 disk herniation can lead to weakness in the hand intrinsics muscles and numbness in the 4 and five digits. Lastly, a C4-5 disk herniation can lead to deltoid weakness and shoulder paresthesia. Patients also can experience pain and paresthesia in the head, neck, and shoulder. Cervical spondylotic myelopathy can be seen in patients with greater than 30% spinal narrowing, leading to gait disturbance, lower extremity weakness, and ataxia.
Spinal stenosis causes
Some people are born with a small spinal canal. But most spinal stenosis occurs when something happens to narrow the open space within the spine.
Spinal stenosis usually occurs as a person ages.
- The spinal disks become drier and start to bulge.
- The bones and ligaments of the spine thicken or grow larger. This is caused by arthritis or long-term swelling.
Overgrowth of bone (osteophytes)
Wear and tear damage from osteoarthritis on your spinal bones can prompt the formation of bone spurs, which can grow into the spinal canal. Paget’s disease, a bone disease that usually affects adults, also can cause bone overgrowth in the spine.
Herniated disks
The soft cushions that act as shock absorbers between your vertebrae tend to dry out with age. Cracks in a disk’s exterior may allow some of the soft inner material to escape and press on the spinal cord or nerves.
Thickened ligaments
The tough cords that help hold the bones of your spine together can become stiff and thickened over time. These thickened ligaments can bulge into the spinal canal.
Spinal stenosis may also be caused by:
- Arthritis of the spine, usually in middle-aged or older people
- Bone diseases, such as Paget disease
- Defect or growth in the spine that was present from birth
- Narrow spinal canal that the person was born with
- Herniated or slipped disk, which often happened in the past
- Injury that causes pressure on the nerve roots or the spinal cord
- Tumors in the spine
- Fracture or injury of a spinal bone
Tumors
Abnormal growths can form inside the spinal cord, within the membranes that cover the spinal cord or in the space between the spinal cord and vertebrae. These are uncommon and identifiable on spine imaging with an MRI or CT.
Spinal injuries
Car accidents and other trauma can cause dislocations or fractures of one or more vertebrae. Displaced bone from a spinal fracture may damage the contents of the spinal canal. Swelling of nearby tissue immediately after back surgery also can put pressure on the spinal cord or nerves.
In the cervical spine, stenosis can be caused by a combination of factors. Some individuals can have a congenitally narrowed spinal canal that is exacerbated by pathologic factors. Disk herniation together with the formation of osteophytic spurs, hypertrophy of the articular facets and ligamentum flavum, and ossification of posterior longitudinal ligaments can lead to central and foraminal stenosis. Structural factors such as subluxation from disk and facet joint degeneration and changes in the normal lordotic curvatures of the spine can lead to spinal compression. In the thoracic spine, disk herniation either from degenerative causes or trauma can lead to stenosis at specific levels. In the lumbar spine, hypertrophy of the facet joints and ligamentum flavum in the setting of disk herniation or spondylolisthesis can lead to worsening stenosis. Spondylolisthesis in the lumbar spine, defined as anterior subluxation of one vertebral body on top of another, is seen most commonly at L5 on S1 and L4 on L5. This can lead to compression of the nerve that exits below the pedicle of the anteriorly subluxed vertebra and results in neurogenic claudication.
Risk factors for spinal stenosis
Risk factors that lead to the development of spinal stenosis are multifactorial. There is a genetic influence as demonstrated in the study of twins. Cumulative trauma can lead to the progression of the disease. Osteoporosis can be a contributing factor. Cigarette smoking in several epidemiological studies has been shown to lead to back pain and degenerative spinal diseases. In the lumbar spine, obesity and loss of muscle tone can lead to stresses and dependence on the bony and ligamentous structures of the spine for structural support.
Most people with spinal stenosis are over the age of 50. Though degenerative changes can cause spinal stenosis in younger people, other causes need to be considered. These include trauma, congenital spinal deformity such as scoliosis, and a genetic disease affecting bone and muscle development throughout the body. Spinal imaging can differentiate these causes.
Spinal stenosis symptoms
Many people have evidence of spinal stenosis on an MRI or CT scan but may not have symptoms. When they do occur, they often start gradually and worsen over time.
Spinal stenosis symptoms often get worse slowly over time. Symptoms vary depending on the location of the spinal stenosis and which nerves are affected. Most often, symptoms will be on one side of the body, but may involve both legs.
Spinal stenosis symptoms include:
- Numbness, cramping, or pain in the back, buttocks, thighs, or calves, or in the neck, shoulders, or arms
- Weakness of part of a leg or arm
Symptoms are more likely to be present or get worse when you stand or walk. They often lessen or disappear when you sit down or lean forward. Most people with spinal stenosis cannot walk for a long period.
More serious spinal stenosis symptoms include:
- Difficulty or poor balance when walking
- Problems controlling urine or bowel movements
Spinal stenosis complications
Rarely, untreated severe spinal stenosis may progress and cause permanent:
- Numbness
- Weakness
- Balance problems
- Incontinence
- Paralysis
Spinal stenosis diagnosis
To diagnose spinal stenosis, your doctor may ask you about signs and symptoms, discuss your medical history, and conduct a physical examination, with a focus on sensation, motor strength, reflexes, and gait. He or she may order several imaging tests to help pinpoint the cause of your signs and symptoms.
During a physical exam, your health care provider will try to find the location of the pain and learn how it affects your movement. You will be asked to:
- Sit, stand, and walk. While you walk, your provider may ask you to try walking on your toes and then your heels.
- Bend forward, backward, and sideways. Your pain may worsen with these movements.
- Lift your legs straight up while lying down. If the pain is worse when you do this, you may have sciatica, especially if you also feel numbness or tingling in one of your legs.
Your doctor will also move your legs in different positions, including bending and straightening your knees. This is to check your strength and ability to move.
To test nerve function, your provider will use a rubber hammer to check your reflexes. To test how well your nerves sense feeling, your provider will touch your legs in many places with a pin, cotton swab, or feather. To check your balance, your provider will ask you to close your eyes while keeping your feet together.
A brain and nervous system (neurologic) examination helps confirm leg weakness and loss of sensation in the legs.
Diagnostic tests
You may have the following tests:
- X-ray of the spine. An X-ray of your back can reveal bony changes, such as bone spurs that may be narrowing the space within the spinal canal. Each X-ray involves a small exposure to radiation.
- Magnetic resonance imaging (MRI). An MRI uses a powerful magnet and radio waves to produce cross-sectional images of your spine. The test can detect damage to your disks and ligaments, as well as the presence of tumors. Most important, it can show where the nerves in the spinal cord are being pressured.
- CT or CT myelogram. If you can’t have an MRI, your doctor may recommend computerized tomography (CT), a test that combines X-ray images taken from many different angles to produce detailed, cross-sectional images of your body. In a CT myelogram, the CT scan is conducted after a contrast dye is injected. The dye outlines the spinal cord and nerves, and it can reveal herniated disks, bone spurs and tumors.
- Electromyography (EMG). Electromyography (EMG) is a test that checks the health of the muscles and the nerves that control the muscles. Your health care provider inserts a very thin needle electrode through the skin into the muscle. The electrode on the needle picks up the electrical activity given off by your muscles. This activity appears on a nearby monitor and may be heard through a speaker. After placement of the electrodes, you may be asked to contract the muscle. For example, by bending your arm. The electrical activity seen on the monitor provides information about your muscle’s ability to respond when the nerves to your muscles are stimulated. A nerve conduction velocity test is almost always performed during the same visit as an EMG. The velocity test is done to see how fast electrical signals move through a nerve.
Diagnosis can be made through imaging with extended release x-ray, CT, and MRI. With the availability of MRI, a plain radiograph is of limited value although dynamic views in flexion and extension modes can demonstrate dynamic instability or spondylolisthesis. CT can help differentiate calcified disks or bone osteophytes from “soft disks,” differentiate ossification of the posterior longitudinal ligament from a thickened posterior longitudinal ligament and detect bone fractures or lytic lesions. MRI is the gold standard; it is able to show intrinsic cord abnormalities, the degree of spinal stenosis, and differentiate other conditions such as tumors, hematoma, or infection. If a patient has a pacemaker and cannot obtain an MRI, a CT myelogram can be performed to identify the level and degree of stenosis.
Spinal stenosis treatment
Your doctor and other health professionals will help you manage your pain and keep you as active as possible.
- Your doctor may refer you for physical therapy. The physical therapist will teach you stretches and exercises that make your back muscles stronger.
- You may also see a chiropractor, a massage therapist, and someone who performs acupuncture. Sometimes, a few visits will help your back or neck pain.
- Cold packs and heat therapy may help your pain during flare-ups.
Treatments for back pain caused by spinal stenosis include:
- Medicines to help relieve back pain.
- A type of talk therapy called cognitive behavioral therapy to help you better understand your pain and teach you how to manage back pain.
- An epidural spinal injection, which involves injecting medicine directly into the space around your spinal nerves or spinal cord.
In patients who suffer from cervical stenosis without myelopathy, conservative management with bracing, rest, or anti-inflammatory medications initially can be employed 1. For those with myelopathy, surgical decompression can provide some relief from pain and sensory loss and can prevent the exacerbation of myelopathy. Depending on the levels involved and the pathology, an anterior or posterior decompression and fusion can be employed to relieve the compression and stabilize the spine.
In the lumbar spine, initial management of back pain can be done with NSAIDs (Nonsteroidal Anti-inflammatory Drugs) and physical therapy followed by interventional pain management strategies for persistent back pain. When conservative management is inadequate, or the patient develops progressive myelopathy, neurologic deficits, or spinal instability, surgical decompression and fusion are recommended. Depending on the nature of the pathology, a variety of approaches, including anterior, lateral, or posterior can be employed to restore lumbar lordosis, decompress the stenosis, and promote fusion.
Medications
Your doctor may prescribe:
- Pain relievers. Pain medications such as ibuprofen (Advil, Motrin IB, others), naproxen (Aleve, others) and acetaminophen (Tylenol, others) may be used temporarily to ease the discomfort of spinal stenosis. They are typically recommended for a short time only, as there’s little evidence of benefit from long-term use.
- Antidepressants. Nightly doses of tricyclic antidepressants, such as amitriptyline, can help ease chronic pain.
- Anti-seizure drugs. Some anti-seizure drugs, such as gabapentin (Neurontin) and pregabalin (Lyrica), are used to reduce pain caused by damaged nerves.
- Opioids. Drugs that contain codeine-related drugs such as oxycodone (Oxycontin, Roxicodone) and hydrocodone (Norco, Vicodin) may be useful for short-term pain relief. Opioids may also be considered cautiously for long-term treatment. But they carry the risk of serious side effects, including becoming habit forming.
Spinal stenosis physical therapy
It’s common for people who have spinal stenosis to become less active, in an effort to reduce pain. But that can lead to muscle weakness, which can result in more pain. A physical therapist can teach you exercises that may help:
- Build up your strength and endurance
- Maintain the flexibility and stability of your spine
- Improve your balance
Assigning patients to six weeks of physical therapy is as effective as initially sending them for decompression surgery, with fewer complications, even in patients who have a strong preference for surgery 16. A trial of six weeks of physical therapy makes sense for many patients with confirmed spinal stenosis before getting out the scalpel 17.
The investigators enrolled 169 patients (average age: 66 to 69 years) with image-confirmed lumbar stenosis who consented to surgery 17. This approach to enrollment eliminated many patients, presumably those with milder symptoms. The patients were randomly assigned (allocation concealed) to surgery or physical therapy. The decompression surgery was the typical procedure used in research and practice. Physical therapy, administered twice weekly for six weeks, consisted of lumbar flexion exercises and conditioning to identify the issues of strength and flexibility identified at enrollment. Analysis was by intention to treat, meaning that patients assigned to physical therapy were analyzed as being in that group even if they eventually received surgery, which 57% of them did over the two years of follow-up (most of them within the first 10 weeks of the study).
Approximately 20% in each group sought additional physical therapy. Two years after identification, general quality of life (as measured by the 36-Item Short Form Health Survey, a typical measure of quality of life) improved equally in both groups, to an average score of 48 to 50 from a baseline of 26 to 28 out of a possible 100. Analyzing by actual treatment rather than by intention to treat yielded similar results, although the study may not have had enough power to find a difference if one existed. Pain, disability, and neurogenic symptoms improved similarly in both groups. Complications were common in the back surgery group, including the need for reoperation. Many patients were not returned to “normal” but continued to visit a back surgeon or primary care physician for back pain two years after the intervention.
Spinal stenosis exercises
Home remedies
You’ll have regular follow-up appointments with your doctor to monitor your condition. He or she may suggest that you incorporate several home treatments into your life, including:
- Trying pain relievers. Over-the-counter medications such as aspirin, ibuprofen (Advil, Motrin IB, others), naproxen (Aleve, others) and acetaminophen (Tylenol, others) can help reduce pain and inflammation.
- Applying hot or cold packs. Some symptoms of cervical spinal stenosis may be relieved by applying heat or ice to your neck.
- Maintaining a healthy weight. Aim to keep a healthy weight. If you’re overweight or obese, your doctor may recommend that you lose weight. Losing excess weight can reduce pain by taking some stress off the back, particularly the lumbar portion of the spine.
- Exercising. Flexing, stretching and strengthening exercises may help open up the spine. Talk with a physical therapist or your doctor about what exercises are safe to do at home.
- Using a cane or walker. In addition to providing stability, these assistive devices can help relieve pain by allowing you to bend forward while walking.
Alternative medicine
Integrative medicine and alternative therapies may be used with conventional treatments to help you cope with spinal stenosis pain. Examples include:
- Massage therapy
- Chiropractic treatment
- Acupuncture
Talk with your doctor if you’re interested in these treatment options.
Steroid injections
Your nerve roots may become irritated and swollen at the spots where they are being pinched. While injecting a steroid medication (corticosteroid) into the space around impingement won’t fix the stenosis, it can help reduce the inflammation and relieve some of the pain.
Steroid injections don’t work for everyone. And repeated steroid injections can weaken nearby bones and connective tissue, so you can only get these injections a few times a year.
Spinal stenosis symptoms often become worse over time, but this may happen slowly. If the pain does not respond to these treatments, or you lose movement or feeling, you may need surgery.
- Surgery is done to relieve pressure on the nerves or spinal cord.
- You and your doctor can decide when you need to have surgery for these symptoms.
Surgery may include removing a bulging disk, removing part of the vertebra bone, or widening the canal and openings where your spinal nerves are located.
During some spinal surgeries, the surgeon will remove some bone to create more room for your spinal nerves or spinal column. The surgeon will then fuse some of the spine bones to make your spine more stable. But this will make your back more stiff.
Decompression procedure
With this procedure, needle-like instruments are used to remove a portion of a thickened ligament in the back of the spinal column to increase spinal canal space and remove nerve root impingement. Only patients with lumbar spinal stenosis and a thickened ligament are eligible for this type of decompression.
The procedure is called percutaneous image-guided lumbar decompression (PILD). It has also been called minimally invasive lumbar decompression (MILD), but to avoid confusion with minimally invasive surgical procedures, doctors have adopted the term percutaneous image-guided lumbar decompression.
Because percutaneous image-guided lumbar decompression is performed without general anesthesia, it may be an option for some people with high surgical risks from other medical problems.
Spinal stenosis surgery
Surgery may be considered if other treatments haven’t helped or if you’re disabled by your symptoms. The goals of surgery include relieving the pressure on your spinal cord or nerve roots by creating more space within the spinal canal. Surgery to decompress the area of stenosis is the most definitive way to try to resolve symptoms of spinal stenosis.
Surgery is performed when nerves branching out from the spine are being squashed, causing pain, weakness or numbness in the arms or in the buttocks or legs. Most people are advised to try other treatments first before resorting to surgery.
Research shows that spine surgeries result in fewer complications when done by highly experienced surgeons. Don’t hesitate to ask about your surgeon’s experience with spinal stenosis surgery. If you have any doubts, get a second opinion.
In most cases, these space-creating operations help reduce spinal stenosis symptoms. But some people’s symptoms stay the same or get worse after surgery. Other surgical risks include infection, a tear in the membrane that covers the spinal cord, a blood clot in a leg vein and neurological deterioration.
Examples of surgical procedures to treat spinal stenosis include:
Laminectomy
This procedure removes the back part (lamina) of the affected vertebra. A laminectomy is sometimes called decompression surgery because it eases the pressure on the nerves by creating more space around them.
In some cases, that vertebra may need to be linked to adjoining vertebrae with metal hardware and a bone graft (spinal fusion) to maintain the spine’s strength.
Laminotomy
This procedure removes only a portion of the lamina, typically carving a hole just big enough to relieve the pressure in a particular spot.
Laminoplasty. This procedure is performed only on the vertebrae in the neck (cervical spine). It opens up the space within the spinal canal by creating a hinge on the lamina. Metal hardware bridges the gap in the opened section of the spine.
Minimally invasive surgery
This approach to surgery removes bone or lamina in a way that reduces the damage to nearby healthy tissue. This results in less need to do fusions.
While fusions are a useful way to stabilize the spine and reduce pain, by avoiding them you can reduce potential risks, such as post-surgical pain and inflammation and disease in nearby sections of the spine. In addition to reducing the need for spinal fusion, a minimally invasive approach to surgery has been shown to result in a shorter recovery time.
Spinal stenosis surgery complications
General complications of surgery
- pain
- bleeding
- unsightly scarring
- infection of the surgical site (wound)
- difficulty passing urine
- blood clots
- chest infection
- heart attack or stroke
Specific complications of cervical spinal stenosis surgery
- neuropathic pain
- injury to your spinal cord and nerves
- infection in your spine
- damage to the nerve roots
- tear of the thin membrane that covers the nerves in your spine
- spinal instability
Specific complications of lumbar spinal stenosis surgery
- worse pain or numbness down your leg
- numbness between your legs, loss of normal bowel and bladder control and, for men, problems having an erection
- neuropathic pain
- tear of the thin membrane that covers the nerves in your spine
- infection in your spine
- spinal instability
Lumbar spinal stenosis surgery recovery
You should be able to go home after 2 to 3 days.
Do not lift anything heavy or twist your body. Make sure you keep a good posture when sitting and walking.
Regular exercise should help you to return to normal activities as soon as possible. Before you start exercising, ask the healthcare team or your doctor for advice.
Most people make a good recovery from surgery.
Spinal stenosis can sometimes come back.
Cervical spinal stenosis surgery recovery
You should be able to go home after 2 to 3 days.
Do not lift anything heavy or twist your body. Make sure you keep a good posture when sitting and walking.
Regular exercise should help you to return to normal activities as soon as possible. Before you start exercising, ask the healthcare team or your doctor for advice.
Most people make a good recovery from surgery.
Spinal stenosis prognosis
Many people with spinal stenosis are able to be active with the condition, although they may need to make some changes in their activities or work.
Spine surgery will often partly or fully relieve symptoms in your legs or arms. It is hard to predict if you will improve and how much relief surgery will provide.
- People who had long-term back pain before their surgery are likely to have some pain after surgery.
- If you needed more than one kind of back surgery, you may be more likely to have future problems.
- The area of the spinal column above and below a spinal fusion is more likely to be stressed and have problems and arthritis in the future. This may lead to more surgeries later.
In rare cases, injuries caused by pressure on the nerves are permanent, even if the pressure is relieved.
- Hoang S, Mesfin FB. Spinal Stenosis. [Updated 2018 Oct 27]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2018 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK441989[↩][↩][↩][↩]
- Yabuki S, Fukumori N, Takegami M, Onishi Y, Otani K, Sekiguchi M, Wakita T, Kikuchi S, Fukuhara S, Konno S. Prevalence of lumbar spinal stenosis, using the diagnostic support tool, and correlated factors in Japan: a population-based study. J Orthop Sci. 2013 Nov;18(6):893-900.[↩]
- Buser Z, Ortega B, D’Oro A, Pannell W, Cohen JR, Wang J, Golish R, Reed M, Wang JC. Spine Degenerative Conditions and Their Treatments: National Trends in the United States of America. Global Spine J. 2018 Feb;8(1):57-67[↩]
- Wu L, Cruz R. Lumbar Spinal Stenosis. [Updated 2018 Oct 27]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2018 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK531493[↩]
- Kalichman L, Cole R, Kim DH, Li L, Suri P, Guermazi A, Hunter DJ. Spinal stenosis prevalence and association with symptoms: the Framingham Study. Spine J. 2009 Jul;9(7):545-50.[↩]
- Zaina F, Tomkins-Lane C, Carragee E, Negrini S. Surgical Versus Nonsurgical Treatment for Lumbar Spinal Stenosis. Spine. 2016 Jul 15;41(14):E857-68.[↩]
- Jinkins JR. Gd-DTPA enhanced MR of the lumbar spinal canal in patients with claudication. J Comput Assist Tomogr. 1993 Jul-Aug;17(4):555-62.[↩]
- Binder DK, Schmidt MH, Weinstein PR. Lumbar spinal stenosis. Semin Neurol. 2002 Jun;22(2):157-66.[↩]
- Hall S, Bartleson JD, Onofrio BM, Baker HL, Okazaki H, O’Duffy JD. Lumbar spinal stenosis. Clinical features, diagnostic procedures, and results of surgical treatment in 68 patients. Ann. Intern. Med. 1985 Aug;103(2):271-5.[↩]
- Katz JN, Dalgas M, Stucki G, Katz NP, Bayley J, Fossel AH, Chang LC, Lipson SJ. Degenerative lumbar spinal stenosis. Diagnostic value of the history and physical examination. Arthritis Rheum. 1995 Sep;38(9):1236-41.[↩]
- Mazanec DJ, Podichetty VK, Hsia A. Lumbar canal stenosis: start with nonsurgical therapy. Cleve Clin J Med. 2002 Nov;69(11):909-17[↩]
- Fukusaki M, Kobayashi I, Hara T, Sumikawa K. Symptoms of spinal stenosis do not improve after epidural steroid injection. Clin J Pain. 1998 Jun;14(2):148-51[↩]
- Prateepavanich P, Thanapipatsiri S, Santisatisakul P, Somshevita P, Charoensak T. The effectiveness of lumbosacral corset in symptomatic degenerative lumbar spinal stenosis. J Med Assoc Thai. 2001 Apr;84(4):572-6.[↩]
- Malmivaara A, Slätis P, Heliövaara M, Sainio P, Kinnunen H, Kankare J, Dalin-Hirvonen N, Seitsalo S, Herno A, Kortekangas P, Niinimäki T, Rönty H, Tallroth K, Turunen V, Knekt P, Härkänen T, Hurri H., Finnish Lumbar Spinal Research Group. Surgical or nonoperative treatment for lumbar spinal stenosis? A randomized controlled trial. Spine. 2007 Jan 01;32(1):1-8.[↩]
- Chang Y, Singer DE, Wu YA, Keller RB, Atlas SJ. The effect of surgical and nonsurgical treatment on longitudinal outcomes of lumbar spinal stenosis over 10 years. J Am Geriatr Soc. 2005 May;53(5):785-92.[↩]
- Spinal Stenosis: Physical Therapy Before Surgery. Am Fam Physician. 2015 Sep 15;92(6):528. https://www.aafp.org/afp/2015/0915/p528.html[↩]
- Delitto A, Piva SR, Moore CG, et al. Surgery versus nonsurgical treatment of lumbar spinal stenosis: a randomized trial. Ann Intern Med. 2015; 162( 7): 465– 473.[↩][↩]




{kind=link}