
Contents
What is lichenification
Lichenification simply means thickening of the skin with accentuation of normal skin markings that is caused by repetitive scratching and rubbing. Lichenification is often associated with chronic dermatitis or chronic eczema, which is characterized by thickened dry patches, often lichenified from repetitive scratching and rubbing (increased skin markings). The terms eczema and dermatitis are generally regarded as synonymous. Eczema (dermatitis) is a common inflammatory skin condition characterized histologically by spongiosis with varying degrees of acanthosis, and a superficial perivascular lymphohistiocytic infiltrate.
The clinical features of eczema (dermatitis) may include itching, redness, scaling and clustered papulovesicles. The condition may be induced by a wide range of external and internal factors acting singly or in combination.
Figure 1. Lichenification (thickening of all layers of skin)
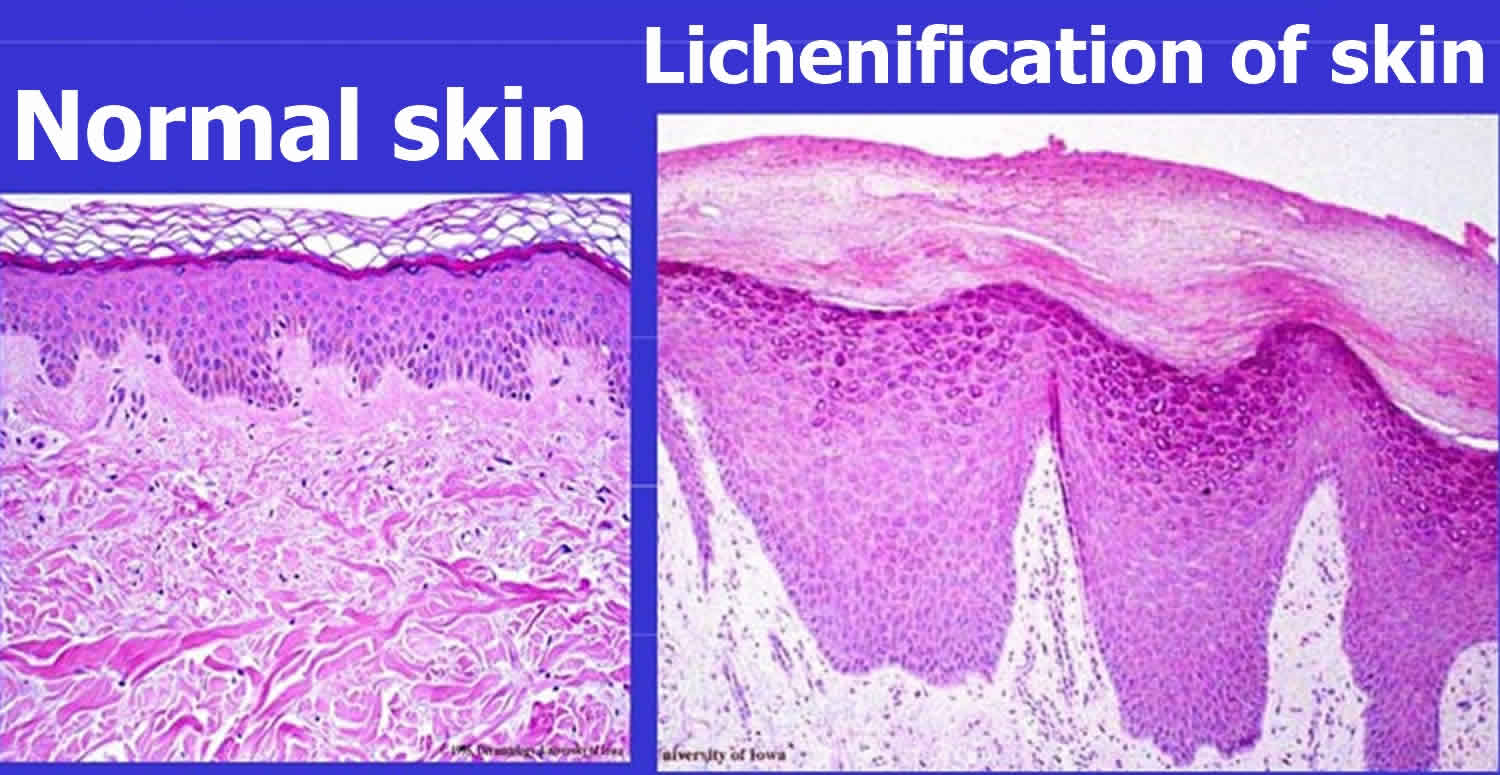
Figure 2. Skin epidermis
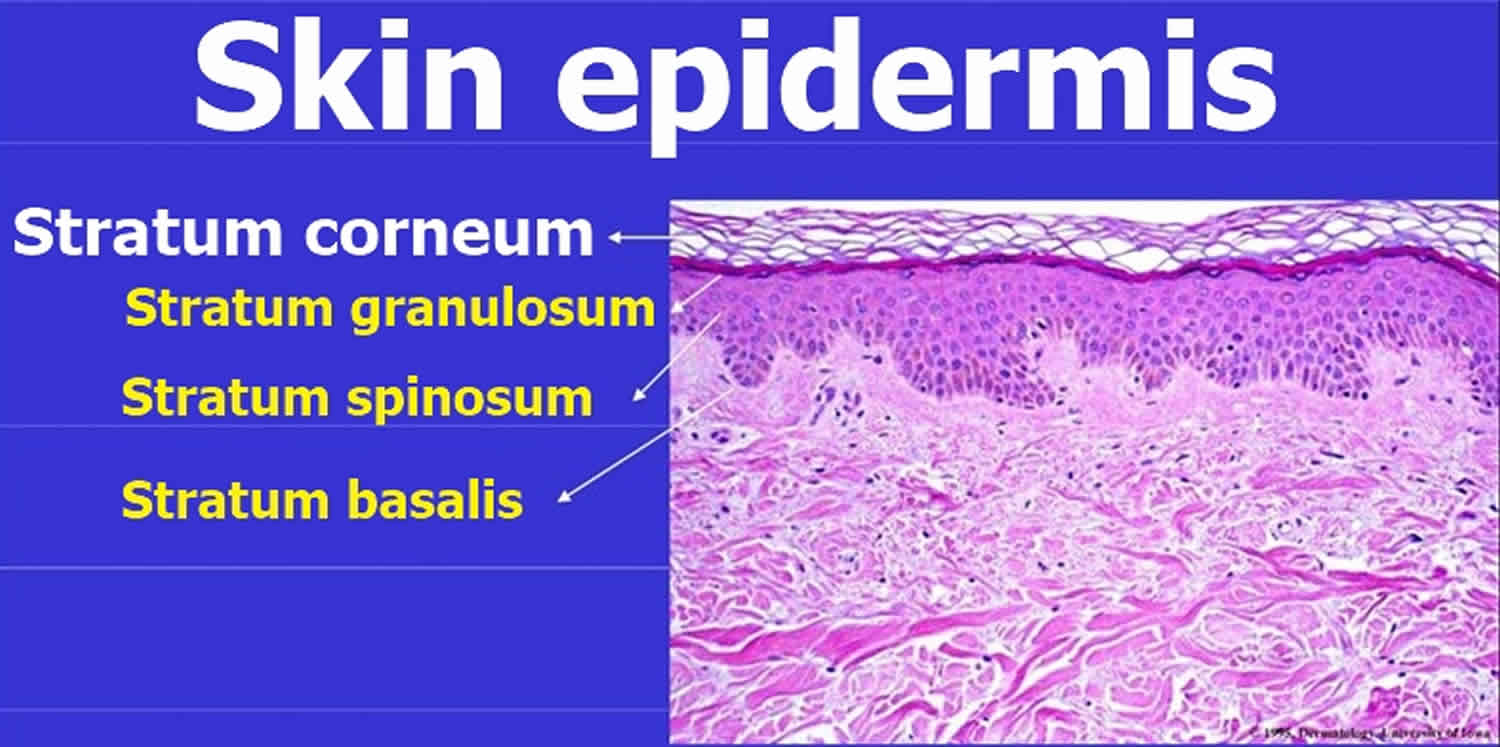
Figure 3. Lichenification skin

Lichenification and lichen simplex chronicus
Lichen simplex chronicus also known as neurodermatitis circumscripta, describes localized thickened skin patches of lichenification because of repeated rubbing and scratching; the patches become increasingly itchy so it is difficult to stop scratching. It may be a complication of atopic dermatitis. Well-defined papules and bumpy thickened plaques are found most often in adults on the nape of the neck, occipital scalp, lower legs, forearms, vulva or scrotum. Widespread lichen simplex is often called neurodermatitis.
Lichen simplex chronicus is not a primary disease but rather the skin’s response to chronic physical injury (trauma). The gradual thickening of skin, , is called lichenification.
Lichen simplex chronicus begins as itchy skin. The itching leads to scratching and rubbing, which causes lichenification or thickening of skin. The thickened skin is itchy, which causes more scratching and, thus, more skin thickening. This scratch-itch cycle continues if not treated.
Lichen simplex chronicus can occur in people of any age, of any race, and of either sex. However, it is more common in females than in males and appears more frequently in middle-aged and older adults.
Conditions that can lead to lichen simplex chronicus include:
- Insect bites
- Scars
- Eczema (atopic dermatitis)
- Dry skin (xerosis)
- Poor circulation in legs (venous insufficiency)
- Anxiety and stress
Lichen simplex chronicus signs and symptoms
Lichen simplex chronicus is often solitary and unilateral, usually affecting the patient’s dominant side. Multiple plaques can also arise, with bilateral and symmetrical or asymmetrical distribution. The location of lichen simplex chronicus is not random, as some body sites are particularly commonly affected.
Although it can occur anywhere on the body, lichen simplex chronicus is most commonly seen in the following areas:
- Inner wrists, forearms, and elbows
- Sides and back of neck
- Upper thighs, knees, shins, ankles, and tops of feet
- Vulva, scrotum, anus (anogenital areas)
- Scalp
Each patch of lichen simplex chronicus appears as leathery, thickened skin in which the normal skin lines are exaggerated. The thickened skin is darker than surrounding skin (hyperpigmented). This darkening is even more apparent in dark-skinned people.
Individuals with lichen simplex chronicus report periodic itching that is most intense at night or any time they are still.
How is lichen simplex chronicus diagnosed?
Clinical appearance is generally typical. At times, it may be helpful to do some investigations. These would include:
- Skin scrapings for possible tinea infection
- Skin biopsy.
In the absence of known underlying skin problem or infection, consider neuropathy. Is there a history of spinal injury, disease or symptoms? In severe cases, the following tests may be performed (although they are often unhelpful):
- Spinal imaging: X-rays, CT scans, MRI scans
- Electrophysiological nerve conduction studies.
Lichenification treatment
It is important to understand that the itchy patch of skin is, at least in part, due to scratching and rubbing. Treatment needs to address the symptoms and any underlying cause.
- The primary treatment is to stop scratching. However, this can be very difficult once a scratch-itch cycle has started. Areas of lichen simplex chronicus may need to be covered at night, as many people scratch in their sleep.
- Use moisturizers to help relieve itchy skin. When choosing a moisturizer, look for oil-based creams and ointments, which work better than water-based lotions. Apply moisturizers just after bathing, while the skin is still moist.
- Apply over-the-counter hydrocortisone cream to decrease the itch. However, if the itching is limited to the groin area, you may have a fungal infection (jock itch [tinea cruris]) rather than lichen simplex chronicus. Do not apply hydrocortisone to the groin area unless recommended to do so by a doctor.
- If there are breaks or cracks in the skin, apply an antibiotic ointment to prevent infection.
See your doctor if the itching does not improve with self-care measures, if you are developing more lesions, or if you develop symptoms of infection such as pain, redness, drainage of pus, or fever.
Treatments your doctor may prescribe
Management of dermatitis (eczema) involves:
- Emollients to relieve itch and dryness
- Antipruritic cooling lotions containing 0.5% menthol / camphor
- Topical steroids for short courses or intermittently for flare-ups
- Coal tar, ichthammol or zinc paste
- Topical calcineurin preparations
- Oral antibiotics for secondary infection
- Behavioral changes to reduce rubbing and scratching
- Occlusive bandages
- Oral sedative antihistamines to help sleep.
- Sometimes, oral corticosteroids or immunosuppressive agents such as cyclosporine or azathioprine
If your doctor is not sure if you have lichen simplex chronicus, he/she may wish to perform a skin biopsy to confirm the diagnosis. The procedure involves:
- Numbing the skin with an injectable anesthetic.
- Sampling a small piece of skin by using a flexible razor blade, a scalpel, or a tiny cookie cutter (called a “punch biopsy”). If a punch biopsy is taken, a suture or two may be placed and will need to be removed 6–14 days later.
- Having the skin sample examined under the microscope by a specially trained physician (dermatopathologist).
Once you are sure you have lichen simplex chronicus, it is important to break the scratch-itch cycle. In addition to the above self-care measures, your doctor may recommend one or more of the following treatments to reduce itching and scratching:
- Aggressive moisturizing techniques. Moisturizers to relieve dryness and reduce desire to scratch
- Potent topical steroids until the plaque is resolved (4–6 weeks) — occlusion for a few hours after application may enhance efficacy
- Reduce potency or frequency of topical steroids once lichenification has resolved
- Creams containing salicylic acid or urea, to improve penetration of the topical corticosteroid
- Oral anti-histamines or tricyclic antidepressant (eg, amitriptyline or nortriptyline), especially for use at bedtime to help sleep.
- Steroid injections every 4–6 weeks. Injection of corticosteroid solution directly into the lichen simplex chronicus lesions
- Coal tar preparations
- Cooling creams containing menthol
- Ultraviolet light therapy
- Sedatives or anti-depressants for people with lichen simplex chronicus strongly related to psychological stress. Tricyclic antidepressants (amitriptyline, nortriptyline, doxepin), other antidepressants (e.g., duloxetine) or antiepileptic medications (valproate, lamotrigine, gabapentin) for radiculopathy.
- Doxepin or capsaicin cream
- Topical or oral antibiotics if infection is present
- Antifungal agents for dermatophyte infection
- Phototherapy and immunomodulatory medications for inflammatory dermatoses (oral corticosteroids, methotrexate, azathioprine or ciclosporin)





{kind=link}