
Contents
What is microalbumin
Urine microalbumin or microalbuminuria is the presence of a small amount of albumin in the urine. Microalbuminuria is defined as urinary albumin excretion of 30-300 mg/day or 20-200 µg/min 1. However, “microalbuminuria” is slowly being replaced with the term “albuminuria,” which refers to any elevation of albumin in the urine. The presence of microalbuminuria (a small amount of albumin in the urine) is an early indicator of kidney disease. Microalbuminuria is also a marker of general vascular dysfunction and nowadays is considered a predictor of worse outcomes for both kidney and heart patients. Studies have shown that elevated levels of urinary albumin in people with diabetes or hypertension are associated with increased risk of developing cardiovascular disease. More recently, research has been focused on trying to determine if increased levels of albumin in the urine are also indicative of cardiovascular disease risk in those who do not have diabetes or high blood pressure. There is currently some evidence that albuminuria is associated with an increased risk of death in adults.
Albumin is a type of protein that is normally found in the blood, and under normal physiological conditions, only a very small amount of albumin is found in urine (virtually no albumin is present in the urine when the kidneys are functioning properly). Your body needs protein. Albumin is an important nutrient that helps build muscle, repair tissue, and fight infection. But it should be in your blood, not your urine. When you have albumin (protein) in your urine, it is called “albuminuria” or “proteinuria.” Having protein in your urine may mean that your kidneys are not filtering your blood well enough. This can be a sign of early kidney disease. If your urine test comes back “positive” for protein, the test should be repeated to confirm the results. Three positive results over three months or more is a sign of kidney disease.
Albumin may be detected in the urine even in the early stages of kidney disease. The urine albumin test (formerly called microalbumin) detects and measures the amount of albumin in the urine to screen for kidney disease. Tests for microalbuminuria can detect abnormal kidney leakage of protein 2. In diabetic nephropathy and hypertensive nephropathy, microalbumin level is used as an early biomarker of kidney damage 3.
One in three American adults is at risk for kidney disease 4. Anyone can get kidney disease at any time. If kidney disease is found and treated early, you can help slow or even stop it from getting worse. Most people with early kidney disease do not have symptoms. That is why it is important to be tested.
According to the American Diabetes Association and National Kidney Foundation, everyone with type 1 diabetes should get urine albumin test (microalbumin) starting 5 years after onset of the disease and then annually, and all those with type 2 diabetes should get tested starting at the time of diagnosis and then annually. If albumin in the urine (albuminuria) is detected, it should be confirmed by retesting twice within a 3-6 month period. People with hypertension may be tested at regular intervals, with the frequency determined by their healthcare practitioner.
What is albumin?
Albumin is a protein made by your liver. Albumin makes up about 60% of the total protein in the blood and plays many roles. Albumin keeps fluid from leaking out of blood vessels; nourishes tissues; and transports hormones, vitamins, drugs, and substances like calcium throughout the body. Levels of albumin may decrease, to a greater or lesser degree, when conditions interfere with its production by the liver, increase protein breakdown, increase protein loss via the kidneys, and/or expand plasma volume (diluting the blood).
Two important causes of low blood albumin include:
- Severe liver disease—since albumin is produced by the liver, its level can decrease with loss of liver function; however, this typically occurs only when the liver has been severely affected.
- Kidney disease—one of the many functions of the kidneys is to conserve plasma proteins such as albumin so that they are not released along with waste products when urine is produced. Albumin is present in high concentrations in the blood, and when the kidneys are functioning properly, virtually no albumin is lost in the urine. However, if a person’s kidneys become damaged or diseased, they begin to lose their ability to conserve albumin and other proteins. This is frequently seen in chronic diseases, such as diabetes and hypertension. In nephrotic syndrome, very high amounts of albumin are lost through the kidneys.
If I have urine microalbumin, does it mean I have kidney disease?
Albumin in the urine (albuminuria) may be an early sign of kidney disease, but your doctor will check you again to make sure albuminuria is not caused by something else, like not drinking enough water. If your doctor suspects that you have kidney disease, the test for albumin will be repeated. Three positive results over three months or more is a sign of kidney disease.
You will also be given a simple blood test to estimate glomerular filtration rate (GFR). Your GFR number helps determine how well your kidneys are working.
You may also be given:
- Imaging tests. (An ultrasound or CT scan). This produces a picture of your kidneys and urinary tract. It can show whether your kidneys have kidney stones or other problems.
- A kidney biopsy. This can help find out what caused your kidney disease and how much damage to the kidneys has happened.
How often do I need to have a test for urine microalbumin (proteinuria)?
People who are at increased risk for kidney disease should have this test as part of routine checkups by a healthcare provider. Those at increased risk include:
- People with diabetes
- People with high blood pressure
- People with a family history of kidney failure
- People who are 65 years or older
- Certain ethnic groups including African Americans, Hispanics, Asians, American Indians
Microalbumin creatinine ratio
A routine dipstick is not sensitive enough to detect small amounts of urine protein (albuminuria). Therefore, it is recommended that screening in adults with chronic kidney disease or at risk for chronic kidney disease be done by testing for albuminuria.
Albumin-to-creatinine ratio (ACR) is the first method of preference to detect elevated protein. The recommended method to evaluate albuminuria is to measure urinary albumin-to-creatinine ratio in a spot urine sample. Albumin-to-creatinine ratio is calculated by dividing albumin concentration in milligrams by creatinine concentration in grams.
Although the 24-hour collection has been the “gold standard,” alternative methods for detecting protein excretion such as urinary albumin-to-creatinine ratio (ACR) correct for variations in urinary concentration due to hydration as well as provide more convenience than timed urine collections. The spot specimen correlates well with 24-hour collections in adults.
Most of the time, tests for albumin and creatinine are done on a urine sample collected randomly (not timed) and an albumin-to-creatinine ratio (ACR) is calculated. This is done to provide a more accurate indication of the how much albumin is being released into the urine. Creatinine, a byproduct of muscle metabolism, is normally released into the urine at a constant rate and its level in the urine is an indication of the urine concentration. This property of creatinine allows its measurement to be used to correct for urine concentration when measuring albumin in a random urine sample.
Plasma, the liquid portion of blood, contains many different proteins, including albumin. One of the many functions of the kidneys is to conserve plasma proteins so that they are not released along with waste products when urine is produced. There are two mechanisms that normally prevent protein from passing into urine:
- Specialized structures in the kidney called glomeruli are composed of loops of specialized capillaries that filter the blood, allowing small substances to pass through towards the urine, but provide a barrier that keeps most large plasma proteins inside the blood vessels.
- The smaller proteins that do get through are almost entirely reabsorbed by tubes (tubules) that have a number of sections that collect the fluid and molecules that pass through the glomeruli.
Protein in the urine (proteinuria) most often occurs when either the glomeruli or tubules in the kidney are damaged. Inflammation and/or scarring of the glomeruli can allow increasing amounts of protein to leak into the urine. Damage to the tubules can prevent protein from being reabsorbed.
If a person’s kidneys become damaged or diseased, they begin to lose their ability to conserve albumin and other proteins. This is frequently seen in chronic diseases, such as diabetes and hypertension, with increasing amounts of protein in the urine reflecting increasing kidney dysfunction.
Albumin is one of the first proteins to be detected in the urine with kidney damage. People who have consistently detectable small amounts of albumin in their urine (albuminuria) have an increased risk of developing progressive kidney failure and cardiovascular disease in the future.
How is microalbumin creatinine ratio test used?
A urine albumin test and albumin to creatinine ratio (ACR) are used to screen for kidney disease in people with chronic conditions, such as diabetes and high blood pressure (hypertension). It can detect small amounts of albumin that escape from the blood through the kidneys into the urine several years before significant kidney damage becomes apparent. Studies have shown that identifying individuals in the very early stages of kidney disease helps people and healthcare providers adjust treatment. Controlling diabetes and hypertension by maintaining tight glycemic control and reducing blood pressure delay or prevent the progression of kidney disease.
If albumin is detected in a urine sample collected at random, over 4 hours, or overnight, the test may be repeated and/or confirmed with urine that is collected over a 24-hour period (24-hour urine).
For urine samples collected randomly (not timed), both albumin and creatinine usually are measured and an albumin to creatinine ratio (ACR) is calculated. This is done to provide a more accurate indication of the how much albumin is being released into the urine. The American Diabetes Association has stated a preference for the albumin to creatinine ratio for screening for albuminuria indicating early kidney disease. Since the amount of albumin in the urine can vary considerably, an elevated albumin to creatinine ratio should be repeated twice within 3 to 6 months to confirm the diagnosis.
Moderately increased albuminuria, historically known as microalbuminuria, (albumin to creatinine ratio 30-300 mg/g) refers to albumin excretion above the normal range but below the level of detection by tests for total protein. Severely increased albuminuria, historically known as macroalbuminuria, (albumin to creatinine ratio >300 mg/g) refers to a higher elevation of albumin associated with progressive decline in glomerular filtration rate (GFR). The following chart lists the albuminuria categories in chronic kidney disease (Figure 1).
Figure 1. Albumin to creatinine ratio chart (normal amount of albumin in your urine is less than 30 mg/g)
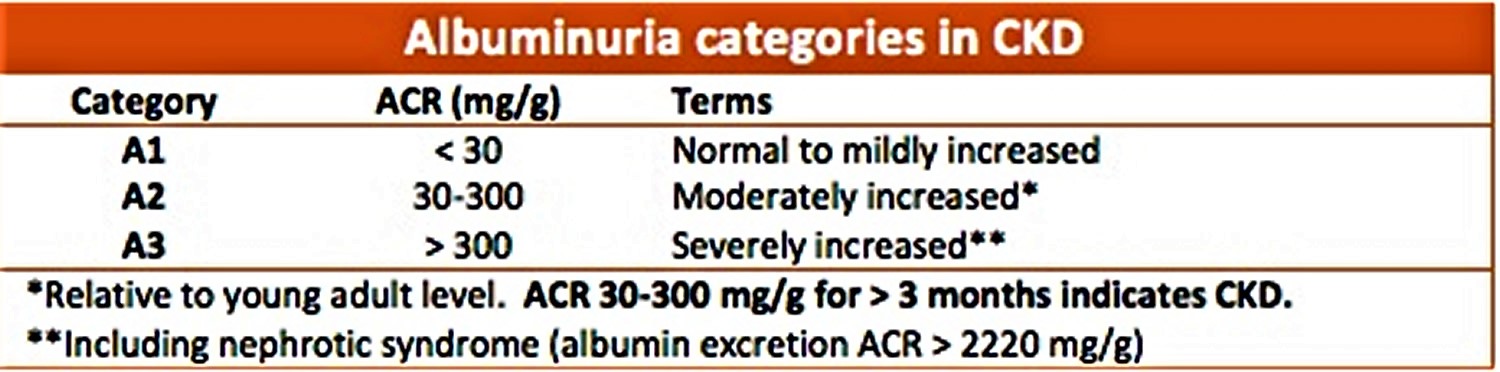
Footnote: CKD = chronic kidney disease
Microalbumin test
A urine microalbumin test is a test to detect very small levels of a blood protein (albumin) in your urine. A microalbumin test is used to detect early signs of kidney damage in people who are at risk of developing kidney disease.
Healthy kidneys filter waste from your blood and hang on to the healthy components, including proteins such as albumin. Kidney damage can cause proteins to leak through your kidneys and exit your body in your urine. Albumin is one of the first proteins to leak when kidneys become damaged.
Microalbumin tests are recommended for people with an increased risk of kidney disease, such as those with type 1 diabetes, type 2 diabetes or high blood pressure.
- If albumin in undetectable in the urine, it is an indication that kidney function is normal.
- Moderately increased albumin levels found in both initial and repeat urine tests indicate that a person is likely to have early kidney disease. Very high levels are an indication that kidney disease is present in a more severe form.
- The presence of blood in the urine, a urinary tract infection, vigorous exercise, and other acute illnesses may cause a positive test result that is not related to kidney disease. Testing should be repeated after these conditions have resolved.
Results of the microalbumin test are measured as milligrams (mg) of protein leakage over 24 hours. Generally:
- Less than 30 mg is normal
- Thirty to 300 mg may indicate early kidney disease (microalbuminuria)
- More than 300 mg indicates more advanced kidney disease (macroalbuminuria)
Discuss your test result with your doctor and what it means for your health. If your urinary microalbumin level is higher than normal, your doctor may recommend repeating the test.
Several factors can cause higher than expected urinary microalbumin results, such as:
- Blood in your urine (hematuria)
- Certain medications
- Fever
- Recent vigorous exercise
- Urinary tract infection
- Other kidney diseases
Why is urine microalbumin test done?
Your doctor may recommend a urine microalbumin test to detect early signs of kidney damage. Treatment may prevent or delay more advanced kidney disease.
How often you need microalbumin tests depends on any underlying conditions and your risk of kidney damage. For example:
- Type 1 diabetes. If you have type 1 diabetes, your doctor may recommend a microalbumin test once a year beginning five years after your diagnosis.
- Type 2 diabetes. If you have type 2 diabetes, your doctor may recommend a microalbumin test once a year beginning immediately after your diagnosis.
- High blood pressure. If you have high blood pressure, your doctor may recommend microalbumin tests more regularly. Discuss with your doctor how often to repeat this test.
If your urinary microalbumin level is elevated, your doctor may recommend treatment and more frequent testing.
How you prepare for a urine microalbumin test
The microalbumin test is a simple urine test. You can eat and drink normally before the test.The amount of urine your doctor may want to test may vary — you may only need to provide a random sample, or your doctor may ask you to collect 24 hours’ worth of urine.
What you can expect
During the microalbumin test, you simply need to provide a fresh urine sample. This may be done in several ways:
- 24-hour urine test. Your doctor may ask you to collect all of your urine in a special container over a 24-hour period and submit it for analysis.
- Timed urine test. Your doctor may ask you to provide a urine sample first thing in the morning or after a four-hour period of not urinating.
- Random urine test. A random urine test can be taken at any time. But to improve accuracy of the results, it’s often combined with a urine test for creatinine — a waste product usually filtered by the kidneys.
The urine sample is sent to a lab for analysis. After you provide the urine sample, you can return to your usual activities immediately.
Urine microalbumin normal range
A normal amount of albumin in your urine is less than 30 mg/g. Anything above 30 mg/g may mean you have kidney disease, even if your GFR number is above 60.
How to reduce urine microalbumin
If kidney disease is confirmed, your healthcare provider will create a treatment plan. You may also be asked to see a special kidney doctor called a nephrologist. Your treatment may include:
- Medications
- Changes in your diet
- Lifestyle changes such as losing extra weight, exercising, and stopping smoking.
If you have diabetes, follow your healthcare practitioner’s instructions for maintaining control over your blood glucose level. Keeping high blood pressure under control is also effective in preventing kidney damage that leads to albumin in urine (albuminuria). Some studies have shown that those who have albuminuria can prevent it from worsening or may reverse it with good glycemic control and blood pressure control, or by quitting smoking.
Albumin in the urine (albuminuria) is not specific for diabetes. It may also be associated with hypertension (high blood pressure), some lipid abnormalities, and several immune disorders. Elevated results may also be caused by vigorous exercise, blood in the urine, urinary tract infection, dehydration, and some drugs.
- Koroshi A. Microalbuminuria, is it so important?. Hippokratia. 2007;11(3):105-7. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2658722/[↩]
- Qiao P, Zeng HS, Huang F, He XW. (2015). Relationship between micoalbuminuria to estimated glomerular filtration rate ratio and incident of contrast induced nephropathy. Chin J Pract Med, 31: 1790–1793[↩]
- Abudiab M, Krause ML, Fidler ME, Nath KA, Norby SM. (2013). Differentiating scleroderma renal crisis from other causes of thrombotic microangiopathy in a postpartum patient. Clin Nephrol, 80: 293–297.[↩]
- Know Your Kidney Numbers: Two Simple Tests. https://www.kidney.org/atoz/content/know-your-kidney-numbers-two-simple-tests[↩]





{kind=link}