Contents
What is radical prostatectomy
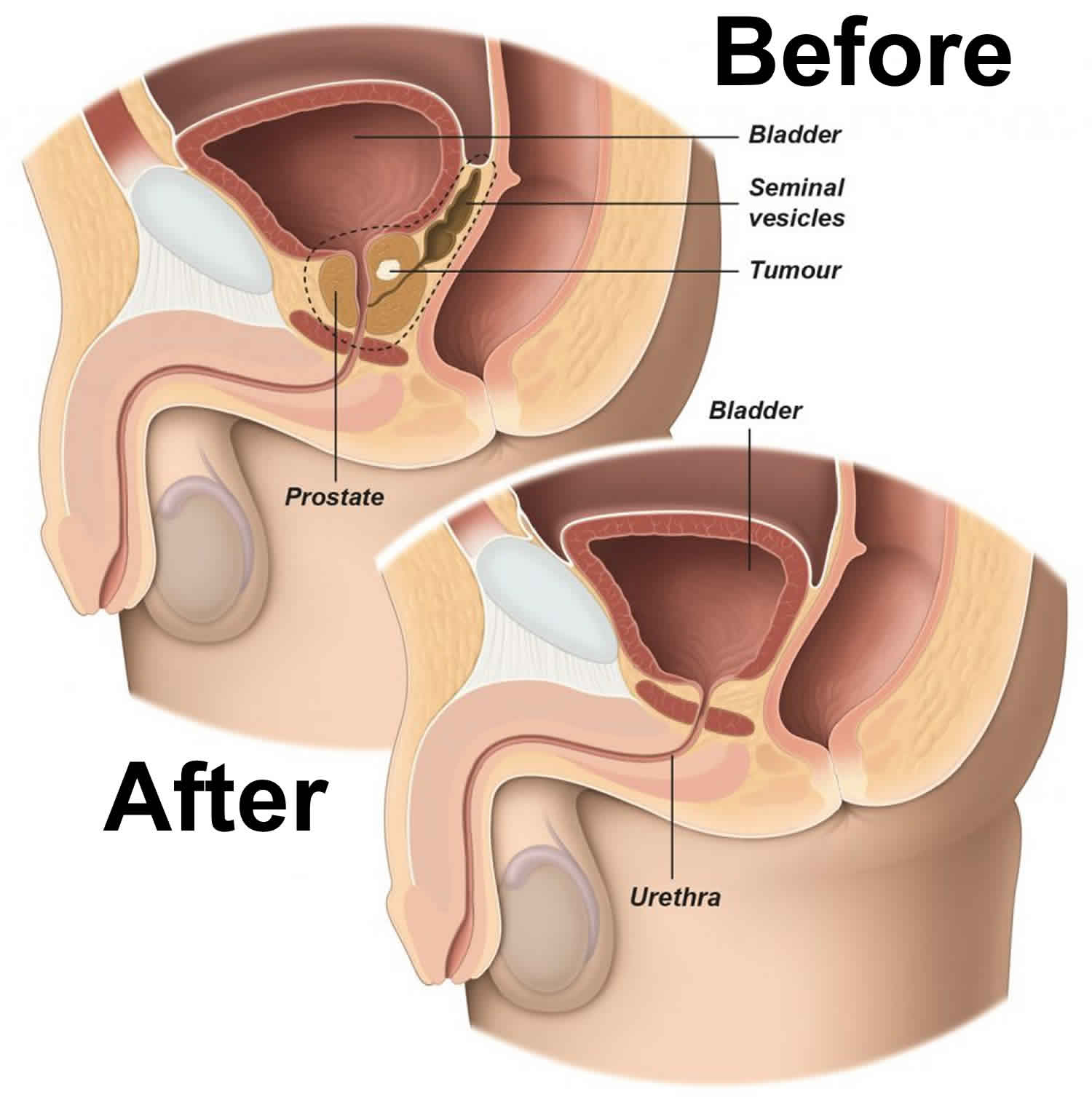
Radical prostatectomy is a surgery to remove the entire prostate gland, the seminal vesicles and surrounding lymph nodes as treatment for men with localized prostate cancer (when the cancer has not spread beyond the prostate gland). There are four main types of radical prostatectomy.
Your doctor may recommend one treatment for you because of what is known about your type of cancer and your risk factors. Or, your doctor may talk with you about other treatments that could be good for your cancer. These treatments may be used instead of surgery or after surgery has been performed.
Factors to consider when choosing a type of surgery include your age and other medical problems. This surgery is often done on healthy men who are expected to live for 10 or more years after the procedure.
For the removal of a localised tumour or a locally-advanced tumour with radical prostatectomy, open and laparoscopic surgery appear to be equally effective.
Keep in mind that the main goal of radical prostatectomy is to remove the tumour and cure you.
A surgeon can perform a radical prostatectomy using different techniques, including:
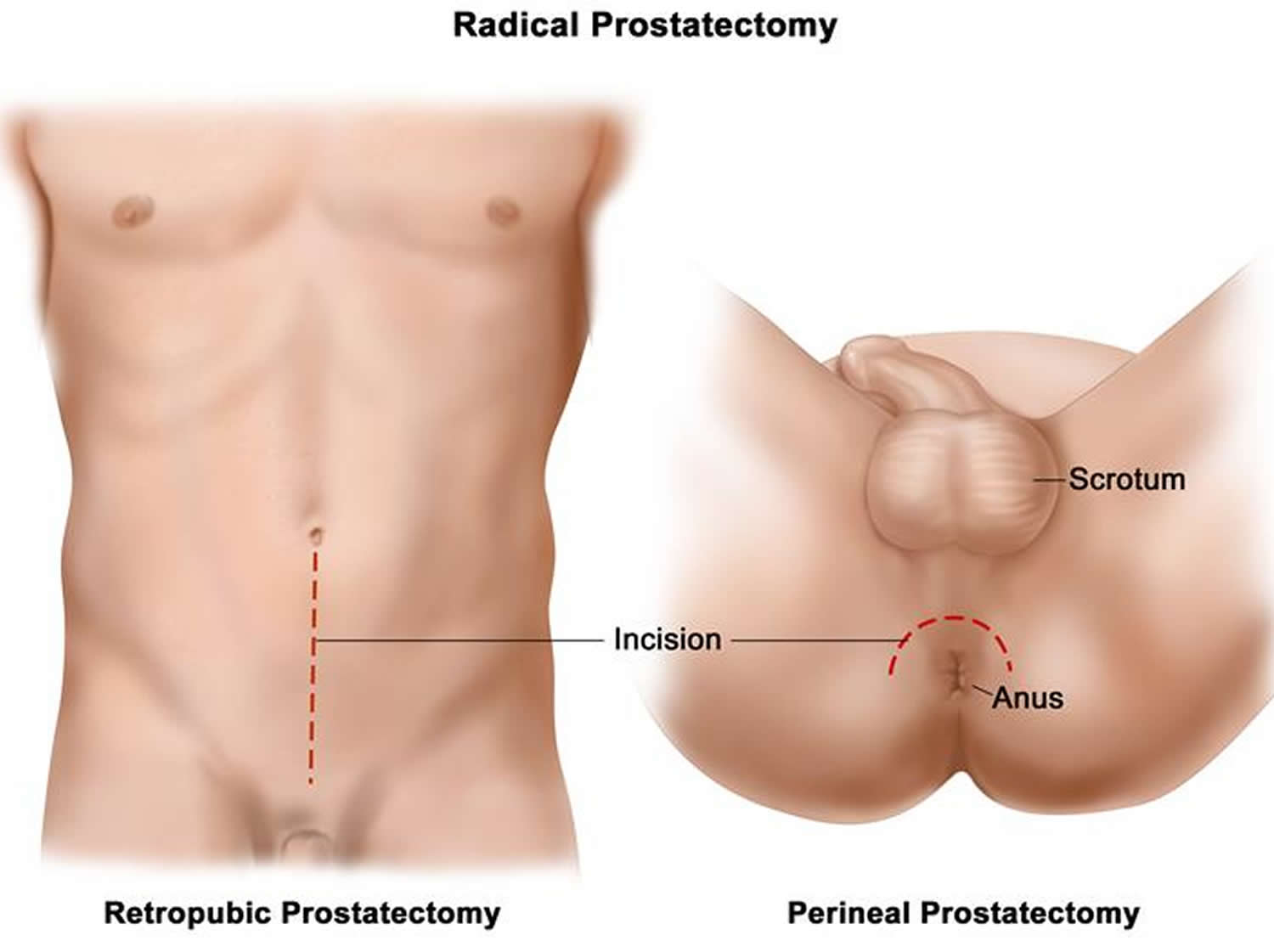
- In a retropubic prostatectomy also called open radical prostatectomy, the prostate is removed through an incision (cut) in the wall of the lower abdomen. This surgery takes 90 minutes to 4 hours.
- In a perineal prostatectomy, the prostate is removed through an incision (cut) in the perineum (the area between the anus and the scrotum). The cut is smaller than with the retropubic technique. This type of surgery often takes less time and causes less loss of blood. However, it is harder for the surgeon to spare the nerves around the prostate or to remove nearby lymph nodes with this technique.
- Robot-assisted radical prostatectomy. The surgeon makes several small incisions in your lower abdomen to remove the prostate. He or she sits at a console, using instruments attached to a computer-assisted mechanical device (robot). The robotic device allows a more precise response to movement of the surgeon’s hands.
- Laparoscopic radical prostatectomy. In a laparoscopic radical prostatectomy, several small incisions (cuts) are made in the wall of the abdomen. A laparoscope (a thin, tube-like instrument with a light and lens for viewing) is inserted through one opening to guide the surgery. Surgical instruments are inserted through the other openings to do the surgery.
For these procedures, you may have general anesthesia so that you are asleep and pain free. Or, you will get medicine to numb the lower half of your body (spinal or epidural anesthesia).
- The surgeon removes the prostate gland from the surrounding tissue. The seminal vesicles, two small fluid-filled sacs next to your prostate, are also removed.
- The surgeon will take care to cause as little damage as possible to the nerves and blood vessels.
- The surgeon reattaches the urethra to a part of the bladder called the bladder neck. The urethra is the tube that carries urine from the bladder out through the penis.
- Your surgeon may also remove lymph nodes in the pelvis to check them for cancer.
- A drain, called a Jackson-Pratt drain, may be left in your belly to drain extra fluid after surgery.
- A tube (catheter) is left in your bladder to drain urine. This will stay in place for a few days to a few weeks. Usually, the catheter is removed after 7 days.
Figure 1. Radical prostatectomy
Before the radical prostatectomy rocedure
You may have several visits with your health care provider. You will have a complete physical exam and may have other tests. Your provider will make sure medical problems such as diabetes, high blood pressure, and heart or lung problems are being controlled.
If you smoke, you should stop several weeks before the surgery. Your provider can help.
Always tell your provider what drugs, vitamins, and other supplements you are taking, even ones you bought without a prescription.
During the weeks before your surgery:
- You may be asked to stop taking aspirin, ibuprofen (Advil, Motrin), naproxen (Aleve, Naprosyn), vitamin E, clopidogrel (Plavix), warfarin (Coumadin), and any other blood thinners or drugs that make it hard for your blood to clot.
- Ask which drugs you should still take on the day of your surgery.
- On the day before your surgery, drink only clear fluids.
- Sometimes, you may be asked by your provider to take a special laxative on the day before your surgery. This will clean the contents out of your colon.
On the day of your surgery:
- Do not eat or drink anything after midnight the night before your surgery.
- Take the drugs you have been told to take with a small sip of water.
- You will be told when to arrive at the hospital. Be sure to arrive on time.
Prepare your home for when you come home after the surgery.
Radical prostatectomy recovery time
Most people stay in the hospital for 1 to 4 days. After laparoscopic or robotic surgery, you may go home the day after the procedure.
You may need to stay in bed until the morning after surgery. You will be encouraged to move around as much as possible after that.
Your nurse will help you change positions in bed and show you exercises to keep blood flowing. You will also learn coughing or deep breathing to prevent pneumonia. You should do these steps every 1 to 2 hours. You may need to use a breathing device to keep your lungs clear.
After your surgery you may:
- Wear special stockings on your legs to prevent blood clots.
- Receive pain medicine in your veins or take pain pills.
- Feel spasms in your bladder.
- Have a Foley catheter in your bladder when you return home.
What to expect at home
You may be tired and need more rest for 3 to 4 weeks after you go home. You may have pain or discomfort in your belly or the area between your scrotum and anus for 2 to 3 weeks.
You will go home with a catheter (tube) to drain urine from your bladder. This will be removed after 1 to 3 weeks.
Wound Care
Change the dressing over your surgical wound once a day, or sooner if it becomes soiled. Your health care provider will tell you when you do not need to keep your wound covered. Keep the wound area clean by washing it with mild soap and water.
- You may remove the wound dressings and take showers if sutures, staples, or glue were used to close your skin. Cover the incision with plastic wrap before showering for the first week if you have tape (Steri-Strips) over it.
- DO NOT soak in a bathtub or hot tub, or go swimming, as long as you have a catheter. You can do these activities after the catheter is removed and your doctor has told you it is OK to do so.
Your scrotum may be swollen for 2 to 3 weeks if you had open surgery. You may need to wear either a support (like a jock strap) or brief underwear until the swelling goes away. While you are in bed, you may use a towel under your scrotum for support.
You may have a drain (called a Jackson-Pratt, or JP drain) below your belly button that helps extra fluid drain from your body and prevent it from building up in your body. Your provider will take it out after 1 to 3 days.
Urinary Catheters
While you have a urinary catheter:
- You may feel spasms in your bladder. Your provider can give you medicine for this.
- You will need to make sure your indwelling catheter is working properly. You will also need to know how to clean the tube and the area where it attaches to
- your body so that you do not get an infection or skin irritation.
- The urine in your drainage bag may be a darker red color. This is normal.
After your catheter is removed:
- You may have burning when you pee, blood in the urine, frequent urination, and an urgent need to urinate.
- You may have some urine leakage (incontinence). This should improve over time. You should have almost normal bladder control within 3 to 6 months.
- You will learn exercises (called Kegel exercises) that strengthen the muscles in your pelvis. You can do these exercises any time you are sitting or lying down.
Other Self-care
DO NOT drive the first 3 weeks after you come home. Avoid long car trips if you can. If you need to take a long car trip, stop at least every 2 hours.
DO NOT lift anything heavier than a 1-gallon (4 liters) milk jug for the first 6 weeks. You can slowly work back up to your normal exercise routine after that. You can do everyday activities around the house if you feel up to it. But expect to get tired more easily.
Drink at least 8 glasses of water a day, eat a lot of fruits and vegetables, and take stool softeners to prevent constipation. DO NOT strain during bowel movements.
DO NOT take aspirin, ibuprofen (Advil, Motrin), naproxen (Aleve, Naprosyn), or other similar medicines for 2 weeks after your surgery. They may cause problems with blood clots.
Sexual Problems After Surgery
Sexual problems you may notice are:
- Your erection may not be as rigid. Some men are not able to have an erection.
- Your orgasm may not be as intense or pleasurable as before.
- You may notice no semen at all when you have an orgasm.
These problems may get better or even go away, but it may take many months or more than a year. The lack of an ejaculate (semen coming out with orgasm) will be permanent. Ask your doctor about medicines that will help.
Call your doctor if:
- You have pain in your belly that does not go away when you take your pain medicines
- It is hard to breathe
- You have a cough that does not go away
- You cannot drink or eat
- Your temperature is above 100.5°F (38°C)
- Your surgical cuts are bleeding, red, warm to the touch, or have a thick, yellow, green, or milky drainage
- You have signs of infection (burning sensation when you urinate, fever, or chills)
- Your urine stream is not as strong or you cannot pee at all
- You have pain, redness, or swelling in your legs
While you have a urinary catheter, call your doctor if:
- You have pain near the catheter
- You are leaking urine
- You notice more blood in your urine
- Your catheter seems blocked
- You notice grit or stones in your urine
- Your urine smells bad, or it is cloudy or a different color
- Your catheter has fallen out
Radical prostatectomy side effects
Usually, you can leave the hospital between 3 and 7 days after surgery. The length of hospital stay can vary in different countries. You may experience minor pain in the lower abdomen for some weeks after open radical prostatectomy. After the surgery, you may suffer from urinary incontinence or erectile dysfunction. You may need treatment for these conditions. You need to go to your doctor or go back to the hospital right away if you:
- Develop a fever
- Have heavy blood loss
- Experience severe pain
- Have problems urinating
The removal of pelvic lymph nodes may cause lymphorrhea. This is a leakage of lymph fluid on the skin. The fluid leads to skin damage, and may cause an infection. Discuss the treatment of lymphorrhea with your medical team.
Erectile dysfunction after radical prostatectomy
Radical prostatectomy is a surgical treatment option to remove the entire prostate and surrounding tissue. If the tumor is limited to the prostate gland, the surgeon will try to keep the nerves that lead to the penis intact during surgery. This is called nerve-sparing surgery. Even if nerve-sparing surgery is successful, temporary erectile dysfunction is common after radical prostatectomy.
This is because your nerves are so delicate that they are affected by the slightest injuries. If any injury happens during surgery, the nerves stop transporting signals to the blood vessels in the penis. It can take up to 2 years for the nerves to recover.
The blood vessel running to and from the penis can also be affected by the surgery. As a result, less blood will flow to the spongy tissue of the penis, and damage it. Because of the damage it can be more difficult to recover from erectile dysfunction.
In some cases, nerve-sparing surgery is not possible because the tumor has spread outside of the prostate, or for other reasons. Recovery of erectile function after non-nerve sparing surgery is unlikely but not impossible. Discuss your concerns and possible treatment options with your doctor.
Radical prostatectomy complications
Radical prostatectomy complications are:
- Problems controlling bowel movements (bowel incontinence)
- Problems controlling urine (stress urinary incontinence)
- Erection problems (impotence)
- Injury to the rectum
- Urethral stricture (tightening of the urinary opening due to scar tissue)
Radical prostatectomy may cause stress urinary incontinence. This is because the prostate surrounds the urethra, helping it to resist the pressure of a full bladder. If your prostate is removed this may have an effect on how much pressure the urethra can resist. There are several treatment options to improve or cure stress urinary incontinence.
Another common risk of the surgery is erectile dysfunction. Because the surgeon may need to remove tissue outside of the prostate, there is a risk that vessels and nerves are damaged or removed during surgery. This is a common cause of erectile dysfunction. During surgery, the surgeon tries to keep the nerves to the penis undamaged. The success of this depends on the aggressiveness of the cancer and where the tumor is located. If necessary, your doctor can recommend treatment for erectile dysfunction.
Radical prostatectomy prognosis
Radical prostatectomy should remove all of the cancer cells. However, you will be monitored carefully to make sure the cancer does not come back. After radical prostatectomy for prostate cancer, your doctor will plan regular follow-up visits with you. Routine follow-up lasts at least 5 years. During each visit, the doctor will test the level of prostate-specific antigen (PSA) in your blood. In some cases, you may need a digital rectal examination (DRE). Follow-up is important to monitor how you recover from surgery, to check your general state of health, and to detect possible recurrence of the cancer.
Depending on the pathology results and PSA test results after prostate removal, your provider may discuss radiation therapy or hormone therapy with you.
If during follow-up the PSA level shows that the prostate cancer has not been completely removed you may need additional treatment to remove all tumor cells. Discuss with your doctor which option is best for you.





{kind=link}