
Contents
What is achromatopsia
Achromatopsia is rare non-progressive inherited vision disorder characterized by a partial or total absence of color vision, decreased vision, light sensitivity, and nystagmus 1. Achromatopsia is a disorder of the retina, which is the light-sensitive tissue at the back of the eye. The retina contains two types of light receptor cells, called rods and cones. These cells transmit visual signals from the eye to the brain through a process called phototransduction. Rods provide vision in low light (night vision). Cones provide vision in bright light (daylight vision), including color vision. The cause of achromatopsia is absence of functioning cones (photoreceptors) in the retina 2. People with complete achromatopsia cannot perceive any colors; they see only black, white, and shades of gray. Achromatopsia also involves other problems with vision, including an increased sensitivity to light and glare (photophobia), involuntary back-and-forth eye movements (pendular nystagmus), significantly reduced sharpness of vision (low visual acuity), a small central scotoma, eccentric fixation, and reduced or complete loss of color discrimination 3. Affected individuals can also have farsightedness (hyperopia) or, less commonly, nearsightedness (myopia). These vision problems develop in the first few months of life.
All individuals with achromatopsia (achromats) have impaired color discrimination along all three axes of color vision corresponding to the three cone classes: the protan or long-wavelength-sensitive cone axis (red), the deutan or middle-wavelength-sensitive cone axis (green), and the tritan or short-wavelength-sensitive cone axis (blue). Most individuals have complete achromatopsia, with total lack of function of all three types of cones. Rarely, individuals have incomplete achromatopsia, which is is a milder form of the condition that allows some color discrimination where one or more cone types may be partially functioning. The manifestations are similar to those of individuals with complete achromatopsia, but generally less severe.
Achromatopsia is different from the more common forms of color vision deficiency also called color blindness, in which people can perceive color but have difficulty distinguishing between certain colors, such as red and green.
Hyperopia is common in achromatopsia. Nystagmus develops during the first few weeks after birth followed by increased sensitivity to bright light. Best visual acuity varies with severity of the disease; it is 20/200 or less in complete achromatopsia and may be as high as 20/80 in incomplete achromatopsia. Visual acuity is usually stable over time; both nystagmus and sensitivity to bright light may improve slightly. Although the fundus is usually normal, macular changes (which may show early signs of progression) and vessel narrowing may be present in some affected individuals. Defects in the macula are visible on optical coherence tomography.
Achromatopsia is rare hereditary vision disorder that affects an estimated 1 in 30,000 people worldwide 4. Complete achromatopsia is more common than incomplete achromatopsia.
Because there is a genetic link, achromatopsia is more common in regions where there is a high rate of consanguineous marriages (marriages between relatives) and in the eastern Pacific islands of Pingelap. Complete achromatopsia occurs frequently among Pingelapese islanders, who live on one of the Eastern Caroline Islands of Micronesia. Between 4 and 10 percent of people in this population have a total absence of color vision.
What are the types of achromatopsia?
Achromatopsia has two types; the complete type in which there is no functional cones in the retina at all and patients will have severe visual symptoms. The incomplete type in which there is some functional cones and patients will have less severe visual symptoms than the complete type.
What is cerebral achromatopsia?
Congenital, inherited achromatopsia should not be confused with cerebral achromatopsia, which is an acquired form of total colorblindness that can result from trauma, illness, or some other cause. Persons who develop cerebral achromatopsia report that they see a monochromatic world, all in shades of gray. They are able to see gray because they previously experienced color vision, making it possible for them to perceive the absence of color as gray. This is in sharp contrast to the visual perception of congenital, complete achromats (i.e., complete rod monochromats), who report that the concept of “gray” is as mystifying to them as is the concept of any of the other colors. Persons with cerebral achromatopsia are diagnosed by neurologists, rather than eye specialists. Their loss of color perception is not accompanied by severely impaired vision, extreme light sensitivity, or abnormality in the photoreceptors of the retina, as is the case with persons who have congenital, inherited achromatopsia.
What does a child with achromatopsia have?
Children with achromatopsia will have reduced vision (20/200 or less), no color vision (they perceive only black, white and gray shades), sensitivity to light (photophobia) and the presence of nystagmus (shaking of the eyes). Achromatopsia is sometimes called ‘Day Blindness’, as these children see better in subdued light. Children with incomplete Achromatopsia may have better vision (20/120 to 20/80) and usually have less visual symptoms. Moreover, children may show paradoxical constriction of the pupil in the dark, usually have high hyperopic refractive errors (need for plus power glasses). Nystagmus and photophobia, marked in infancy, may improve with age. Achromatopsia is a non progressive disorder.
How will achromatopsia affect my child’s schooling?
With adequate help from teachers for the visually impaired, children with achromatopsia are usually able to attend mainstream schools. Front seat placement, large print books, and magnifying devices can be very helpful. A low vision evaluation will be necessary before school begins. More severely affected individuals may benefit from services available in schools specifically designated for the visually impaired.
Are red-green color blindness and Achromatopsia the same condition?
No, red-green color blindness patients have difficulty distinguishing red and green colors. People with red-green color blindness have otherwise normal visual acuity and they do not have complete lack of color perception, instead they can perceive other colors.
Achromatopsia causes
Achromatopsia is a genetic disorder in which a child is born with nonfunctioning cones. The cones are special photoreceptor cells in the retina that absorb different color lights. There are three types of cones that are responsible for normal color vision. These are the red cones, the green cones, and the blue cones. A balanced distribution of these cells is necessary for normal color vision. A child born with non-functioning cones will have achromatopsia.
There are several known genes mutations to cause achromatopsia and these are CNGA3, CNGB3, GNAT2, PDE6C or PDE6H 1. A particular CNGB3 gene mutation underlies the condition in Pingelapese islanders 1.
Mutations in any of the genes listed above prevent cones from reacting appropriately to light, which interferes with phototransduction. In people with complete achromatopsia, cones are nonfunctional, and vision depends entirely on the activity of rods. The loss of cone function leads to a total lack of color vision and causes the other vision problems. People with incomplete achromatopsia retain some cone function. These individuals have limited color vision, and their other vision problems tend to be less severe.
Some people with achromatopsia do not have identified mutations in any of the known genes. In these individuals, the cause of the disorder is unknown. Other genetic factors that have not been identified likely contribute to this condition.
Achromatopsia inheritance pattern
Achromatopsia is inherited in an autosomal recessive pattern, which means both copies of the abnormal gene, one from each parent (one abnormal gene from mum and one abnormal gene from dad), is needed to cause the disorder or disease. The parents of an individual with achromatopsia each carry one copy of the mutated gene, but they typically do not show signs and symptoms of the condition.
If a person inherits one abnormal gene and one normal gene, then in most cases that person will be a healthy carrier because the normal gene compensates for the abnormal gene. Being a carrier means that you do not have the condition, but carry a changed copy of the gene on one of a pair of genes.
It is rare to see any history of autosomal recessive conditions within a family because if someone is a carrier for one of these conditions, they would have to have a child with someone who is also a carrier for the same condition. Autosomal recessive conditions are individually pretty rare, so the chance that you and your partner are carriers for the same recessive genetic condition are likely low. Even if both partners are a carrier for the same condition, there is only a 25% chance that they will both pass down the non-working copy of the gene to the baby, thus causing a genetic condition. This chance is the same with each pregnancy, no matter how many children they have with or without the condition.
Key points to remember
- A person must inherit two copies of a abnormal gene, one from each parent, in order to be affected by the condition (25% chance). If a person inherits only one abnormal gene then they will be a carrier (50% chance). These outcomes occur randomly. They remain the same in every pregnancy and are the same for boys and girls.
- A abnormal gene cannot be corrected – it is present for life.
- Carrier testing for at-risk relatives, prenatal testing for pregnancies at increased risk, and preimplantation genetic diagnosis are possible if the pathogenic variants have been identified in the family.
- A abnormal gene is not something that can be caught from other people. They can still be a blood donor, for example.
- People often feel guilty about a genetic condition which runs in the family. It is important to remember that it is no-one’s fault and no-one has done anything to cause it to happen.
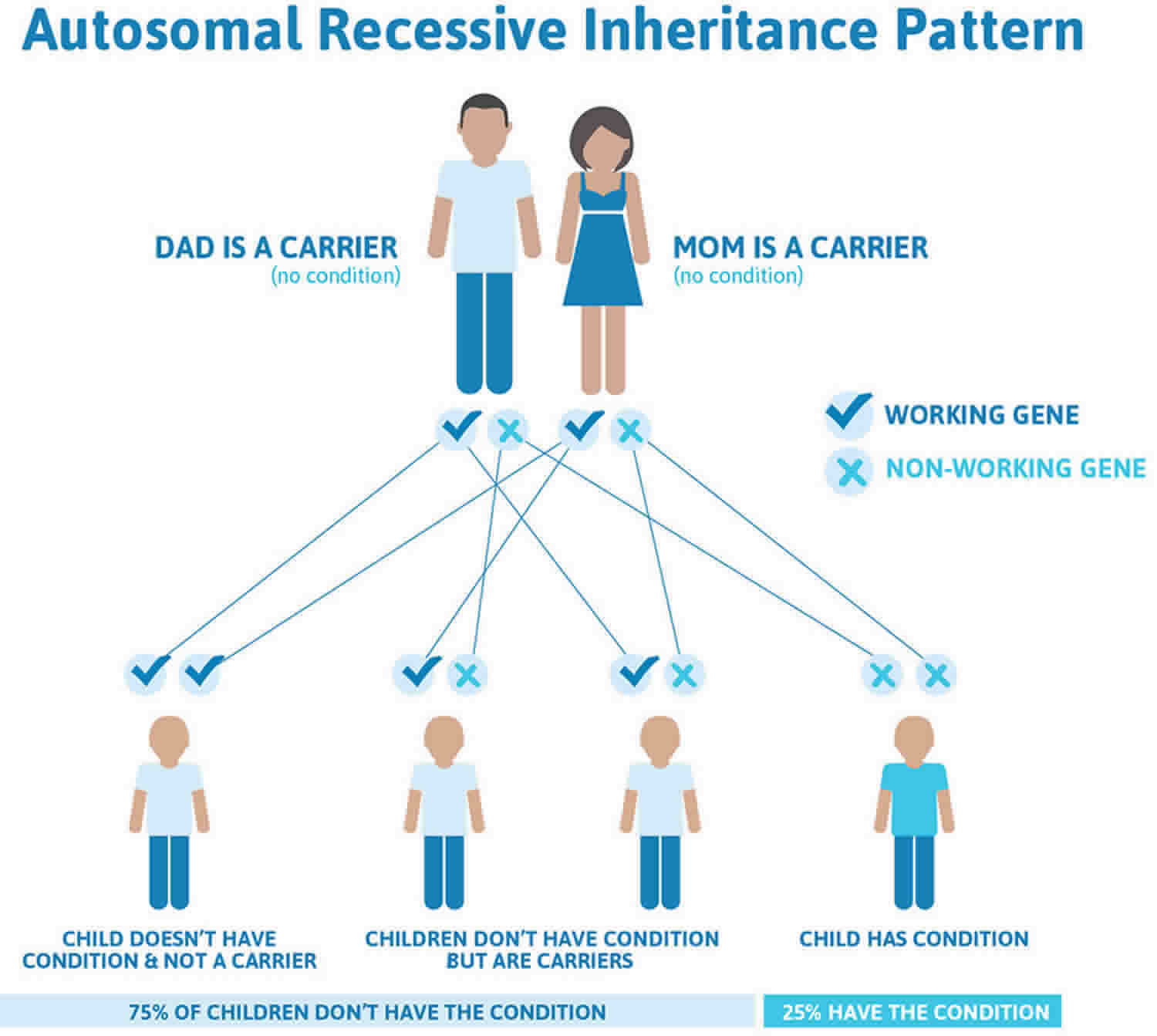
Figure 1 illustrates autosomal recessive inheritance. The example below shows what happens when both dad and mum is a carrier of the abnormal gene, there is only a 25% chance that they will both pass down the abnormal gene to the baby, thus causing a genetic condition.
Figure 1. Achromatopsia autosomal recessive inheritance pattern
Achromatopsia symptoms
Achromatopsia is characterized by partial or total absence of color vision, reduced visual acuity, pendular nystagmus, increased sensitivity to light (photophobia), a small central scotoma (which is often difficult to demonstrate), eccentric fixation, and reduced or complete lack of color discrimination. Hyperopia is common. Nystagmus develops during the first few weeks after birth and is followed by increased sensitivity to bright light.
Best visual acuity varies with severity of the disease; it is 20/200 or less in complete achromatopsia and may be as high as 20/80 in incomplete achromatopsia. Visual acuity is usually stable over time, but both nystagmus and sensitivity to bright light may improve slightly. The fundus is usually normal, but macular changes and vessel narrowing may be present in some individuals, and optical coherence tomography (OCT) reveals macular changes that can progress with time 5
Most individuals have complete achromatopsia, in which the symptoms can be explained by a total lack of function of all three types of cone (i.e., photopic) photoreceptors of the eye, with all visual functions being mediated by the rod (i.e., scotopic) photoreceptors.
Rarely, individuals have incomplete achromatopsia, in which one or more cone types may be partially functioning along with the rods. The symptoms are similar to those of individuals with complete achromatopsia but generally less severe 4. Color discrimination ranges from well preserved to severely impaired; photophobia is usually absent; visual acuity is better preserved than in complete achromatopsia.
Achromatopsia diagnosis
The diagnosis will be made by your ophthalmologist. Achromatopsia should be suspected in individuals with the following typical clinical findings, additional testing, and family history. Family history is consistent with autosomal recessive inheritance.
Clinical findings
- Pendular nystagmus
- Increased sensitivity to light (photophobia)
- Eccentric fixation
- Reduced visual acuity
- Reduced or complete lack of color discrimination
- Small central scotoma
- Fundus appearance: normal in many affected individuals, but can show subtle bilateral macular changes such as absence of the foveal reflex, pigment mottling, or narrowing of the retinal vessels. Frank atrophy of the retinal pigment epithelium (RPE) in the fovea can occur in older individuals.
The diagnosis of achromatopsia is established in a proband through clinical and family history, examination for nystagmus, visual acuity testing, color vision assessment, and fundoscopic examination. If achromatopsia is suspected, additional testing may include optical coherence tomography, fundus autofluorescence, visual fields, and electroretinogram. Identification of biallelic pathogenic variants in ATF6, CNGA3, CNGB3, GNAT2, PDE6C, or PDE6H confirms the clinical diagnosis.
Additional testing
Color vision tests. The color perception of individuals with achromatopsia (achromats) is unreliable; many achromats learn to associate certain colors with objects and to recognize some colors by discerning differences in brightness [Sharpe et al 1999]. In general, all achromats have anomalous (impaired) color discrimination along all three axes of color vision corresponding to the three cone classes: the protan or long-wavelength-sensitive cone axis (red), the deutan or middle-wavelength-sensitive cone axis (green), and the tritan or short-wavelength-sensitive cone axis (blue). The following results are found on standard testing for color vision:
- Generally, no specific axis of color confusion is found on the Farnsworth Munsell 100-hue test.
- An achromat axis (in which the constituent color chips are arranged according to their rod-perceived lightness) is characteristic for complete achromatopsia on both the saturated and desaturated versions of the Panel D-15 test.
- The most important and diagnostic test is red-green color discrimination with the Rayleigh anomaloscope equation. Although a complete achromat can always fully color-match the spectral yellow primary to any mixture of the spectral red and green primaries, a brightness match is only possible to red primary-dominated mixtures.
Visual field testing. Small central scotomas can be demonstrated in some individuals by careful testing. However, unsteady fixation can make demonstration of a central scotoma difficult.
Electroretinogram (ERG)
- Full-field ERG. The photopic response (including the 30-Hz flicker response) is absent or markedly diminished; the scotopic response is normal or mildly abnormal.
- 15-Hz flicker ERG. A typical finding is absence of the cone-driven fast pathway response elicited by high flash intensities 6.
Optical coherence tomography (OCT). A variable degree of foveal hypoplasia as well as disruption and/or loss of inner-/outer-segment junction of the photoreceptors and an attenuation of the RPE layer within the macular region can be observed at an early age 7.
Fundus autofluorescence imaging shows missing or variable formation of foveal hypofluorescence or a larger lesion with a surrounding hyperautofluorescent ring and a central region of absent autofluorescence corresponding to the lesion area seen on OCT 8.
Adaptive optics imaging shows remnant cone structure; however, the number and spatial distribution of the foveal cones are highly variable – the foveal cone mosaic ranges from a contiguously packed mosaic to a sparsely arranged collection of cones 9.
Achromatopsia treatment
Currently there is no cure for achromatopsia. Research on gene therapy is ongoing and may lead to clinical treatments in the future. Animal models of achromatopsia in dogs and mice have shown promising results in restoring some cone function in the retina. Children should be checked for refractive errors (need for glasses). Prescribing glasses to correct refractive conditions such as far-sightedness (hyperopia), near-sightedness (myopia) and astigmatism can improve the vision somewhat but will not restore normal levels of vision. Red colored lenses help reduce the sensitivity to light and thus enhance visual functioning. NoIR (injection-molded) plastic wrap-around glasses have a top ‘shield’ that covers the top of a prescription frame as well as broad side shields which is important since stray light can be disabling. Examples are Corning Lenses: CPF 550 lenses (5% transmission, darkened) and CPF 550XD lenses (4% transmission, darkened). These lenses are available through Winchester Optical. A newer device known as an eyeborg can help people with no color vision to perceive color through sound waves.
- Achromatopsia. https://ghr.nlm.nih.gov/condition/achromatopsia[↩][↩][↩]
- Achromatopsia. https://aapos.org/glossary/achromatopsia[↩]
- Kohl S, Jägle H, Wissinger B, et al. Achromatopsia. 2004 Jun 24 [Updated 2018 Sep 20]. In: Adam MP, Ardinger HH, Pagon RA, et al., editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2019. Available from: https://www.ncbi.nlm.nih.gov/books/NBK1418[↩]
- Sharpe LT, Stockman A, Jagle H, Nathans J. Opsin genes, cone photopigments, color vision, and color blindness. In: Gegenfurtner K, Sharpe LT, eds. Color Vision: from Genes to Perception. Cambridge, UK: Cambridge University Press; 1999:3-52[↩][↩]
- Thomas MG, McLean RJ, Kohl S, Sheth V, Gottlob I. Early signs of longitudinal progressive cone photoreceptor degeneration in achromatopsia. Br J Ophthalmol. 2012;96:1232–6.[↩]
- Bijveld MM, Riemslag FC, Kappers AM, Hoeben FP, van Genderen MM. An extended 15 Hz ERG protocol (2): data of normal subjects and patients with achromatopsia, CSNB1, and CSNB2. Doc Ophthalmol. 2011;123:161–72.[↩]
- Zobor D, Werner A, Stanzial F, Benedicenti F, Rudolph G, Kellner U, Hamel C, Andréasson S, Zobor G, Strasser T, Wissinger B, Kohl S, Zrenner E. RD-CURE Consortium (2017) The clinical phenotype of CNGA3-related achromatopsia: pretreatment characterization in preparation of a gene replacement therapy trial. Invest Ophthalmol Vis Sci. 2017;58:821–32.[↩]
- Kohl S, Zobor D, Chiang WC, Weisschuh N, Staller J, Menendez IG, Chang S, Beck SC, Garrido MG, Sothilingam V, Seeliger MW, Stanzial F, Benedicenti F, Inzana F, Héon E, Vincent A, Beis J, Strom TM, Rudolph G, Roosing S, Hollander AI, Cremers FP, Lopez I, Ren H, Moore AT, Webster AR, Michaelides M, Koenekoop RK, Zrenner E, Kaufman RJ, Tsang SH, Wissinger B, Lin JH. Mutations in the unfolded protein response regulator ATF6 cause the cone dysfunction disorder achromatopsia. Nat Genet. 2015;47:757–65[↩]
- Langlo CS, Patterson EJ, Higgins BP, Summerfelt P, Razeen MM, Erker LR, Parker M, Collison FT, Fishman GA, Kay CN, Zhang J, Weleber RG, Yang P, Wilson DJ, Pennesi ME, Lam BL, Chiang J, Chulay JD, Dubra A, Hauswirth WW, Carroll J., ACHM-001 Study Group. Residual foveal cone structure in CNGB3-associated achromatopsia. Invest Ophthalmol Vis Sci. 2016;57:3984–95[↩]





{kind=link}