
Contents
What is microtia
Microtia is the medical name for an ear which has developed differently. Microtia is a congenital (present at birth) birth defect where the ear may be very small, folded over, missing or a different shape. In rare cases, the ear canal is very narrow or missing altogether. The medical term for this complete absence of the external ear is anotia. Microtia can occur in one or both ears. Microtia is mostly a cosmetic condition. The majority of children with microtia — even those with completely absent outer ears — experience only a partial hearing loss, because the inner ear (the part of the body responsible for hearing) usually remains unaffected.
There are four different types of microtia, ranging from type 1, the mildest form, to type 4, the most severe. Most commonly, various parts of the ear are malformed or underdeveloped (i.e. lobule type, conchal type, and small conchal type).
In almost all cases of microtia, the outer ear, the ear canal and the middle ear are all affected.
- The Outer Ear: The change may vary from being very mild to very severe. Occasionally the ear does not develop at all.
- The Ear Canal: This is often very narrow and may be missing.
- The Middle Ear: This is the part of the ear behind the ear drum. It is usually affected and the changes vary from mild to severe deformity of the ossicles (little bones of hearing).
Most patients with microtia have an earlobe, but they may lack any other recognizable ear elements. Some will have a conchal cavity and some may have an ear canal.
In most children, there is poorer hearing in the ear with microtia. If your child has no ear canal there is at least a moderate degree of hearing loss in that ear (i.e. at least a 60 decibel hearing loss). Sometimes, there may be hearing loss in the other ear as well. If there is hearing loss in both ears, your child will be referred to an audiologist (hearing specialist) to discuss amplification options.
Microtia occurs in approximately 1 in 6,000 to 7,000 births. It is more common in Hispanics, Asians, and Native Americans. It occurs twice as often in males than in females, and appears on the right side of the head twice as often as the left. Both ears will be affected in approximately 20 percent of microtia patients.
Microtia affects your baby’s appearance. You may feel shocked or disappointed that your baby looks different. This is a normal feeling. When children are older, they may sometimes become self-conscious about the appearance of their ears. They may ask for the ear to be fixed.
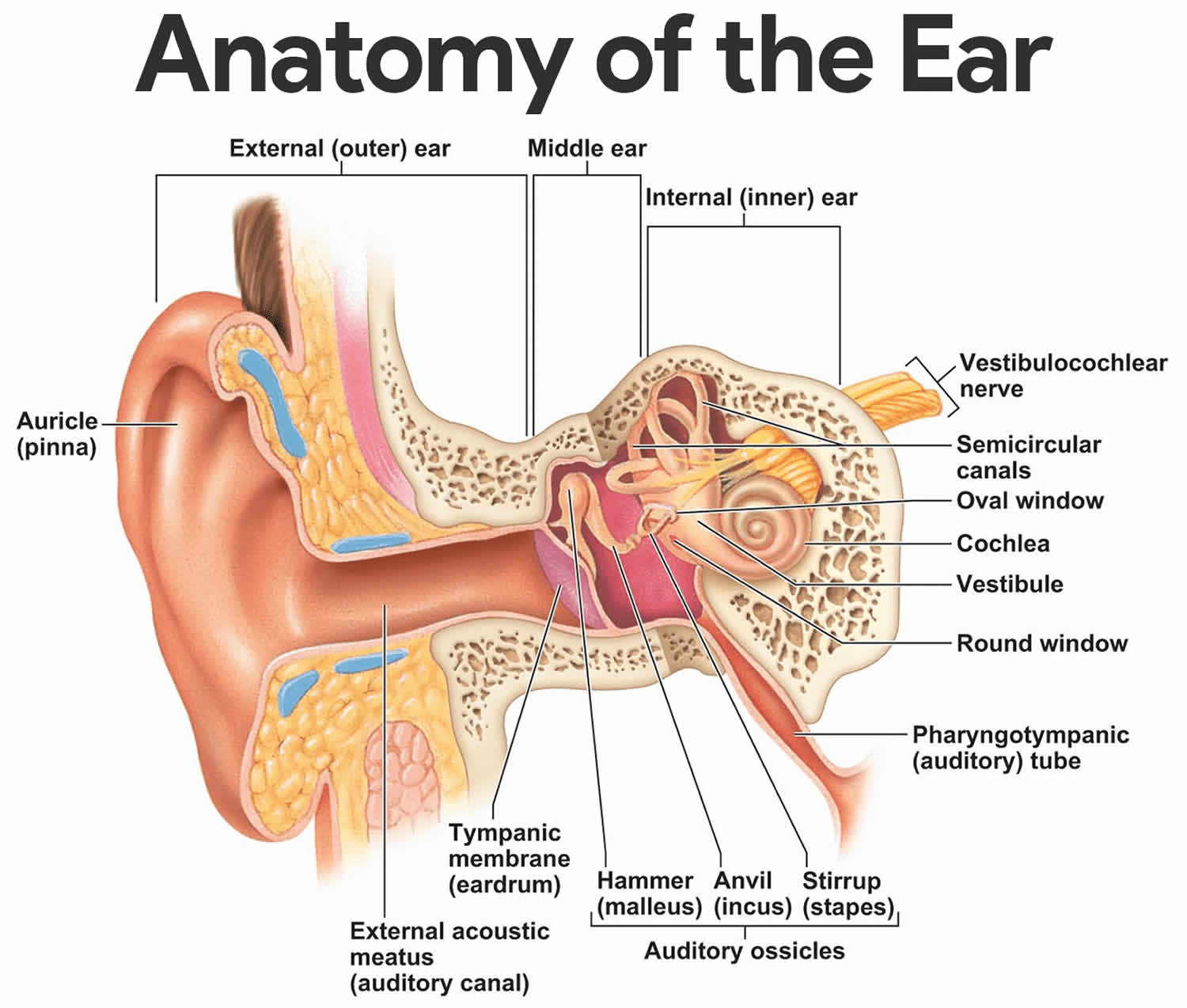
Figure 1. Normal ear anatomy
Is microtia hereditary?
In most children, microtia is not hereditary. In a few genetic syndromes, microtia may be inherited. Discussion with a genetic specialist is recommended if there are questions about inheritance.
Will my child have other problems?
In many children with microtia, the ear is the only part of your child that has developed differently. In a few children, the microtia may be part of a syndrome such as Goldenhaar syndrome where other problems are present. It is important for your child with microtia to be examined carefully after birth by a pediatrician so that any problems in other areas can be identified and managed.
If your child has a hearing problem related to microtia, she/he will be followed by an audiologist (hearing specialist) and an otolaryngologist (ear, nose and throat expert). Together, the team will:
- monitor the hearing loss with regularly scheduled hearing tests (audiograms)
- recommend hearing aids and other ways to maximize the use of the remaining hearing • suggest a hearing aid (either worn as a headband or implanted into the bone) in the event of serious hearing loss
- offer surgery to recreate a missing ear canal (called atresia repair) and improve hearing. Alternatively, a bone anchored hearing aid (BAHA) may be offered.
recommend additional language or developmental assessments for your child, as needed - direct you to community resources for educational or financial assistance.
There are two main types of hearing loss:
- Conductive hearing loss—problems transmitting sound from the outer ear (where sound is collected) to the inner ear. This is the predominant type of hearing loss that’s associated with microtia.
- Sensorineural hearing loss—problems with the nerves connecting the inner ear to the brain. In the inner ear, tiny hairs on the cochlea act as a neural pathway, transmitting through the inner ear. Usually, problems with these hairs on the cochlea are responsible for sensorineural hearing loss.
Sensorineural hearing loss is present in 10 to 15 percent of children with microtia.
Can microtia affect a child’s speech or learning?
This can happen if your child is not hearing well. Children with hearing loss in one ear often hear poorly if there is background noise and may miss things said to them in the classroom or at home. A child who misses a great deal of what is said may have trouble with schoolwork.
If a child with microtia has many ear infections in the better hearing ear, there may be long periods of poor hearing, and this may affect speech and language development. It is best to talk with an ENT (ear, nose, and throat) surgeon and /or a pediatrician if this happens.
Microtia causes
The causes of microtia is, for the most part, unknown. Some infants have microtia because of a change in genes or an abnormality in a single gene. Microtia may occur with syndromes such as hemifacial microsomia, where the entire half of the face is smaller, Treacher Collins syndrome and Goldenhar syndrome. Another known cause for microtia is a medicine called isotretinoin (Accutane®), which if taken during pregnancy can lead to birth defects, including microtia.
Microtia occurs more commonly in infants of diabetic mothers, and infants who were exposed to isotretinoin, thalidomide, alcohol or mycophenolate.
How is microtia diagnosed?
Because microtia is a congenital condition, your child’s malformed ear will be obvious at birth, and therefore diagnosed by the doctor immediately upon physical examination. Doctors also recommend an Auditory Brainstem Response Evaluation (ABR) soon after every child’s birth to evaluate babies’ inner ear function on both sides. An Auditory Brainstem Response Evaluation (ABR) is a type of test that evaluates how well sounds travel along the hearing nerve pathways from the ear to the brainstem. ABR evaluations, both sedated and unsedated, take two to three hours to complete.
An ABR test is a sleep EEG hearing test, which shows the softest sounds your child’s ears can detect at various pitches. The ABR compares changes in brain activity to the timing of repetitive sounds to determine whether the particular intensity of sound can be heard. There will be three or four small stickers on your child’s head, connected to leads going into a computer. Sounds will be presented through an earphone to each ear separately while a computer analyzes the changes in the brain wave pattern in response to sounds. Your child should be sleeping for the duration of the test. Young children under the age of 6 months are not usually sedated, and the test is performed while your baby is naturally sleeping, following a feeding. Children older than 6 months are usually sedated.
The ABR test is not painful or uncomfortable in any way, but it is necessary for your child to be asleep in order to obtain clear recordings during the test.
You will be in the room with your child during the test, and the results will be explained immediately afterward.
Children with microtia should also have a kidney ultrasound to rule out possible deformities, since the urinary system forms at the same time as the ear during prenatal development.
The care and treatment of a child with microtia depends on the severity of the case. Some children will need a series of operations, while others might not need any treatment at all.
When your child is older and getting closer to an age where surgical treatment may be an option, a CT scan may be used to evaluate middle and inner ear abnormalities. CT imaging is not recommended during infancy to limit exposure to any unnecessary radiation, and because children are not yet candidates for surgery.
Though the prospect of your child needing a surgical procedure is worrisome, it’s important to remember that these procedures have excellent success rates.
Microtia treatment
Specialists involved in the treatment of children with microtia may include a clinical geneticist, audiologist, otolaryngologist and plastic surgeon. Some children with microtia have other problems such as a cleft palate, jaw problems, eye problems, orthodontic problems etc. They may need to attend other clinics as well, such as the Craniofacial Clinic, Cleft Clinic or Dental Clinic.
In children who have diminished hearing, a bone anchored hearing aid (BAHA) may be recommended. This is a surgically implanted device that helps transmit sound by direct conduction through bone. Your child’s otolaryngologist will determine if a bone anchored hearing aid (BAHA) is the best treatment option for your child. It is important to coordinate any planned surgeries around the ear with a plastic surgeon to optimize the reconstruction possibilities.
Most children with microtia will eventually have surgery to rebuild the ear. Microtia reconstruction is a staged operation that first rebuilds the ear and later requires separation of the ear from the side of the head and placement of a skin graft. Additional stages may be needed to give additional definition to the final ear shape.
There are several different methods your child’s surgeon may use in ear reconstruction surgery. These techniques are mainly broken down by the material used to rebuild the ear: cartilage from the patient’s ribs, an implant, or an external prosthesis.
It is important to know that reconstructed ears are never as detailed and delicate as normal ears. The goal is to create an ear shape that is realistic enough that it does not attract attention to itself.
Though surgical reconstruction does not occur until your child is 6 to 10 years of age, early consultation can be reassuring and help you prepare for what to expect and as your child grows.
Hearing loss management
Children with a hearing loss should have a hearing test every year. If a child has microtia affecting both ears, he or she will probably need a hearing device. This may be a traditional behind the ear hearing aid or a bone conductor hearing aid. An implanted hearing aid may be suitable for older children. Hearing early intervention may be helpful for your child. Ask your audiologist, ENT (ear, nose, and throat) surgeon or pediatrician what services are available in your area.
Microtia surgery
Plastic surgery is available to improve the appearance of the ear lobe once your child is over 8-10 years of age and if your child wants to undergo this surgery. Not all parents or children with microtia want to have surgery for this condition. Others may want it very much.
Sometimes a narrow ear canal can be widened, but the surgery is difficult and is rarely undertaken if there is good hearing in the other ear. Surgery on the middle ear is rarely undertaken unless the problem is very mild and there is good access to the middle ear. Children with ear infections or persistent fluid in the middle ear (glue ear) may need antibiotics or surgery such as insertion of ventilation tubes (grommets).
The most common type of operation for microtia we perform is called autologous auricular construction. During this operation, specially trained pediatric plastic surgeons will take cartilage from your child’s ribcage and use it to “plant” a new ear on the affected side of the head. The process uses your child’s own tissue, so if the new ear is ever injured it can heal itself just as a natural ear would. Autologous construction is performed when a child is 6 years of age or older. He/she needs to be old enough to have sufficient rib cartilage to “spare”, and 6 years is about the age when the ear on the other side (if applicable) will reach its approximate adult size—so the surgeons can be sure to line up the new ear to match it.
Timeline of care
- Infancy: Possible headband hearing aid
- 6 years of age or older: First stage autologous reconstruction
- 6 months later: Second stage autologous reconstruction
- 6 months later: Third stage autologous reconstruction
- 6 months later: Possible bone anchored hearing aid (BAHA), possible atresia repair
Will my child need further operations as he/she ages?
Yes. Autologous construction usually requires three procedures in total, depending on the type and severity of your child’s microtia. Procedures are typically scheduled six months apart to allow your child time to heal.
- First procedure Surgeons remove some cartilage from the ribcage to build a new ear.
- Second procedure Surgeons refine and reposition the new earlobe.
- Third procedure Surgeons lift the new ear for better alignment and perform “touch-ups” as needed.
It is possible that your child also may need an operation on the middle or inner ear. In that case, surgeons will perform the procedure after the last operation is done.
How will my child look after microtia surgery?
While your child’s reconstructed ear will not look exactly like his other ear, it will greatly improve his/her appearance (and will allow practical things like wearing eyeglasses or sunglasses).
Are there alternatives to surgical treatment for microtia?
In general, ENT surgeons recommend autologous construction as the most effective treatment for microtia. It offers children a comfortable new ear that feels natural, facilitates the use of eyewear, boosts self-esteem and improves their quality of life. At the same time, doctors understand that every child and family is different. Your doctors will work with you to decide on the right option.
Alternatives to autologous construction include:
- No treatment. You may opt not to have any treatment at all. Talk to your child’s care team for guidance and advice.
- Ear implant. An artificial ear made from synthetic materials can be used instead of cartilage. Advantages include no chest scar and ear construction as early as age three. Disadvantages include a higher complication rate and potential long-term problems compared to autologous construction.
- Ear prosthesis. This type of artificial ear, made from a synthetic material, can be attached to the side of your child’s head with a minimally invasive procedure. Disadvantages include the need for daily care.
Microtia long term outlook
Most children born with microtia will develop and grow normally. If your child has an associated hearing problem, audiologic testing and follow up may be needed.
In addition to restoring normal appearance, ear reconstruction also provides functional advantages, such as being able to wear glasses or masks.
Facial differences may lead to teasing by peers — patient and family support groups can help you and your child connect with others with similar experiences.





{kind=link}