
Contents
What is parasomnia
Parasomnia refers to all the abnormal things or unusual behaviors that can happen to people while they sleep, apart from sleep apnea 1. Parasomnias encompass a broad spectrum of events including abnormal motor, behavioral, and sensory experiences. Excessive motor activity and abnormal motor behaviors, when present, adversely affect the patient or the bed partner resulting in sleep fragmentation, psychosocial effects, and even injuries. Parasomnia examples are sleep-related eating disorder, sleepwalking, sleeptalking nightmares, sleep terrors, sleep paralysis, REM sleep behavior disorder, and sleep aggression 2. Sexsomnia, sometimes called “sleepsex,” is also a parasomnia. It refers to sexual acts that are carried out by a person who is sleeping. Parasomnias can have negative effects on people during the daytime, including sleepiness.
In general, most parasomnias are more common in children and become less prevalent as they get older. Approximately 4% of adult population have been reported to have parasomnias 3. Parasomnias are also more frequent in psychiatric disorders 4. Other risk factors include sleep disorders, medical comorbidities and substance abuse.
Parasomnias can occur as a person is falling asleep or at any point in the sleep cycle. If they occur while falling asleep, a person may experience disturbing hallucinations or sleep paralysis, which is when the body is unable to move for seconds or minutes. Sleep paralysis can be quite frightening, especially when it occurs with hallucinations.
Parasomnias that occur during sleep, such as REM sleep behavior disorder (RBD), often involve vigorous and harmful dream-enacting behaviors. REM sleep behavior disorder is a brain disorder that usually occurs in men over 50 years of age, but can affect people of any age who are taking certain medications, such as antidepressants, and people with neurologic disorders, such as Parkinson’s disease, narcolepsy or stroke. Other parasomnias that occur during sleep include nightmares and sleep-related groaning, which can be loud and prevent a person’s bed partner or roommate from sleeping.
In addition, there are parasomnias that occur when a person has abrupt, partial awakenings, such as confusional arousals, sleepwalking, sleep terrors, and sleep-related eating disorder.
Sleep-related hallucinations may also occur as a person is waking up.
Trying to awaken a “parasomniac in action” – especially by shaking or shouting – can sometimes trigger an irritable, aggressive or violent response. Therefore, gently redirect the person back to bed by guiding him or her by the elbow and speaking softly.
Parasomnias affect approximately 10% of Americans. They occur in people of all ages, but are more common in children. Children are particularly vulnerable because of brain immaturity. The good news is that parasomnias are usually not associated with negative health consequences and disappear as a child matures.
Many people who suffer with parasomnias see an improvement in their symptoms simply by improving their sleep habits. Good sleep habits include keeping a regular sleep schedule, managing stress, having a relaxing bedtime routine, and getting enough sleep. There are also drug therapies that are used to control symptoms.
A person should seek treatment whenever there is risk for injury to oneself or another person from the parasomnia. It is also important to seek treatment if the parasomnia disrupts a person’s own sleep or the sleep of the bed partner or roommate, of if there is distress about the symptoms (e.g., nightmares), or if the frequency is quite high or escalating. An overnight sleep lab study may be needed.
It is important to keep in mind that no matter how weird, bizarre, or violent the behavior, a parasomnia is rarely linked with a psychiatric disorder. However, people who suffer from parasomnias may endure ridicule, confusion, and/or shame about their symptoms. In addition, bed partners, family members, and roommates may suffer sleep loss as a result of the parasomnia. In many cases, seeking help from a therapist or support group can help people with parasomnias and the people close to them cope with these issues.
Parasomnias can be successfully managed by appropriate investigation, education and the strategic use of psychologic and pharmacologic therapies.
Despite the variety of pharmacological and non-pharmacological strategies, there are still no standard of practice guidelines.
How can a parasomnia sufferer be protected?
Door alarms can help by awakening a person during an episode. Also, a person who suffers from parasomnias should not sleep on a top bunk, or next to a window. It is important to remove sharp objects from the bedside area and to be sure roommates and household members are aware of the problem and what to do about it.
Sleep Stages
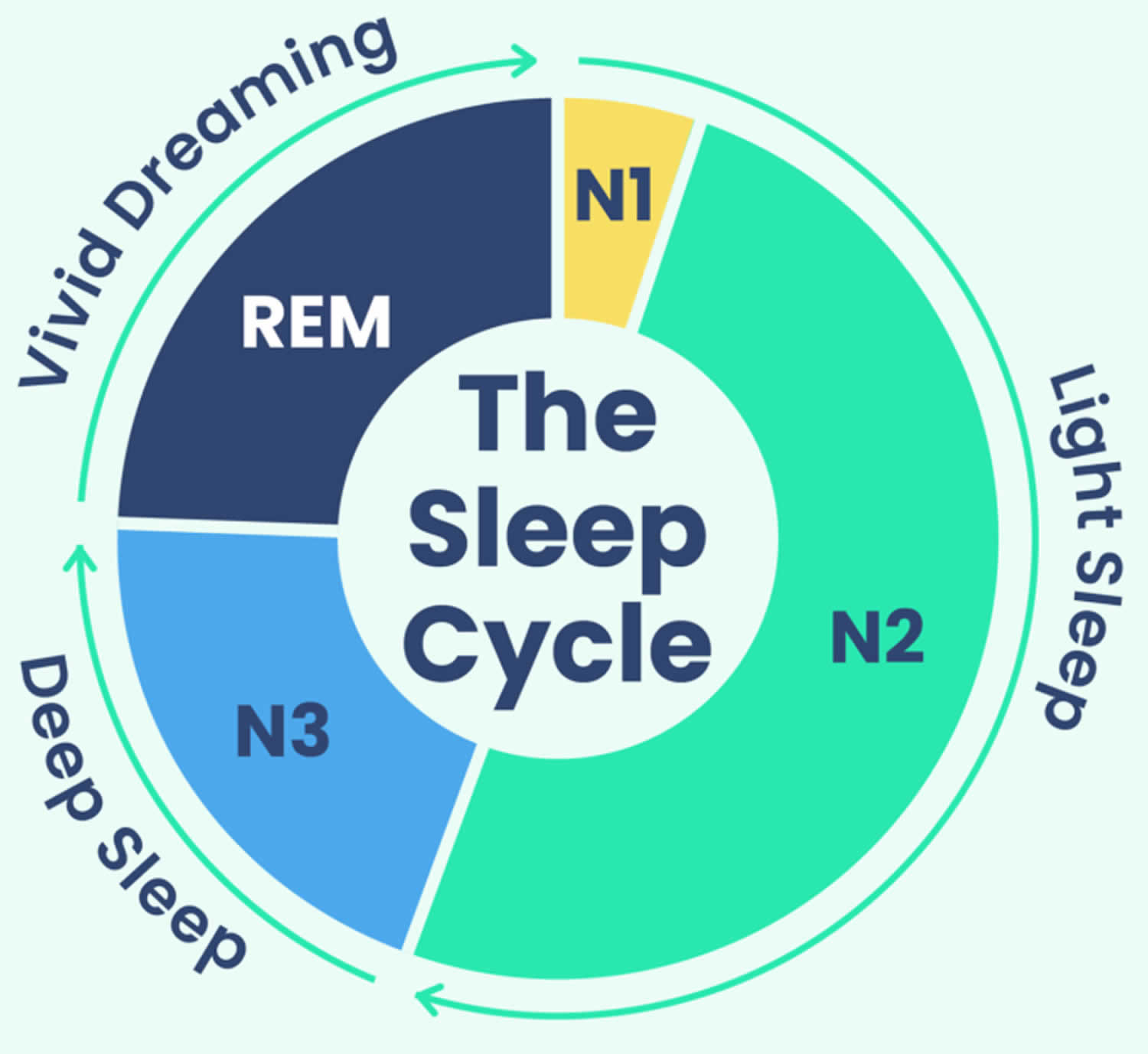
Sleep occurs in 2 main phases, Non-Rapid Eye Movement (NREM) sleep, which has three stages (N1, N2, and N3), and Rapid Eye Movement (REM) sleep 5. Each sleep phase and stage of sleep includes variations in muscle tone, brain wave patterns, and eye movements. Your body cycles through all stages approximately 4 to 6 times each night, averaging 90 minutes for each cycle 6. Each sleep stage serves different functions, from the light transition into sleep (N1), to the restorative deep sleep (N3) and the active dreaming of REM sleep.
- Stage 1 (N1 or light sleep) is the lightest stage of sleep and occurs as a person first falls asleep. This brief stage is when your drowsiness gives way to falling asleep. Your heartbeat and breathing start to slow down, but it’s still pretty easy to wake you up during this stage. Average length 1 to 7 minutes.
- Stage 2 (N2 or intermediate sleep) is where the body starts to relax more deeply. Your body temperature drops, your muscles relax, and your breathing and heart rate slow even more. Average length 10 to 25 minutes.
- Stage 3 (N3 or deep sleep) is the deepest and more restorative sleep, allowing your body to recover and grow. In stage 3 sleep, your breathing and pulse are slow and steady. Average length 20 to 40 minutes.
- Stage 4 (REM Sleep) is where most dreaming occurs, brain activity increases almost as if you were awake, and your muscles become temporarily paralyzed. Your heart rate and respiration speed up and become more erratic, and your eyes move quickly behind your eyelids. Dreams are most vivid during the REM stage. Average length 10 to 60 minutes.
Although the sleep stages are described numerically, you don’t always progress through them in this exact order. For example, in many sleep cycles, you transition from stage 3 sleep back to stage 2 sleep before beginning a period of REM sleep.
Sleep occurs in 5 stages: Wake, Non-Rapid Eye Movement (NREM) stage N1, then progress through N2 and N3, and after N3 you enter REM sleep 5. You then return to NREM stages, often starting again at N2. Throughout the night, the REM periods lengthen, and deep N3 sleep decreases, with most N3 sleep occurring in the first half of the night, with each stage leading to progressively deeper sleep. Approximately 75% of sleep is spent in the NREM (Non-Rapid Eye Movement) stages, with the majority spent in the N2 stage 9. A typical night’s sleep consists of 4 to 5 sleep cycles, with the progression of sleep stages in the following order: N1, N2, N3, N2, REM 10. A complete sleep cycle takes roughly 90 to 120 minutes. The first REM period is short, and as the night progresses, longer periods of REM and decreased time in deep sleep (NREM) occur 5. With each new cycle, you spend increasing amounts of time in REM sleep, so most of your REM sleep takes place in the second half of the night.
Sleep isn’t uniform. Sleep cycles can vary from person to person and from night to night based on a wide range of factors such as your age, recent sleep patterns, and alcohol consumption. Over the course of the night, you go through several rounds of the sleep cycle, which is composed of four stages. In a typical night, a person goes through four to six sleep cycles 5. Not all sleep cycles are the same length, but on average they last about 90 minutes each.
The first sleep cycle is often the shortest, ranging from 70 to 100 minutes, while later cycles tend to fall between 90 and 120 minutes. In addition, the composition of each cycle — how much time is spent in each phase of sleep — changes as the night goes along.
Figure 1. Sleep Stages
Footnotes: A sleep episode begins with a short period of NREM stage N1 progressing through stage N2, followed by stage N3 and finally to REM. However, individuals do not remain in REM sleep the remainder of the night but, rather, cycle between stages of NREM and REM throughout the night. NREM sleep constitutes about 75 to 80 percent of total time spent in sleep, and REM sleep constitutes the remaining 20 to 25 percent. The average length of the first NREM-REM sleep cycle is 70 to 100 minutes. The second, and later, cycles are longer lasting—approximately 90 to 120 minutes 11. In normal adults, REM sleep increases as the night progresses and is longest in the last one-third of the sleep episode. As the sleep episode progresses, stage 2 begins to account for the majority of NREM sleep, and stages 3 and 4 may sometimes altogether disappear.
[Source 7 ]Figure 2. Typical Sleep Pattern in Young Adults
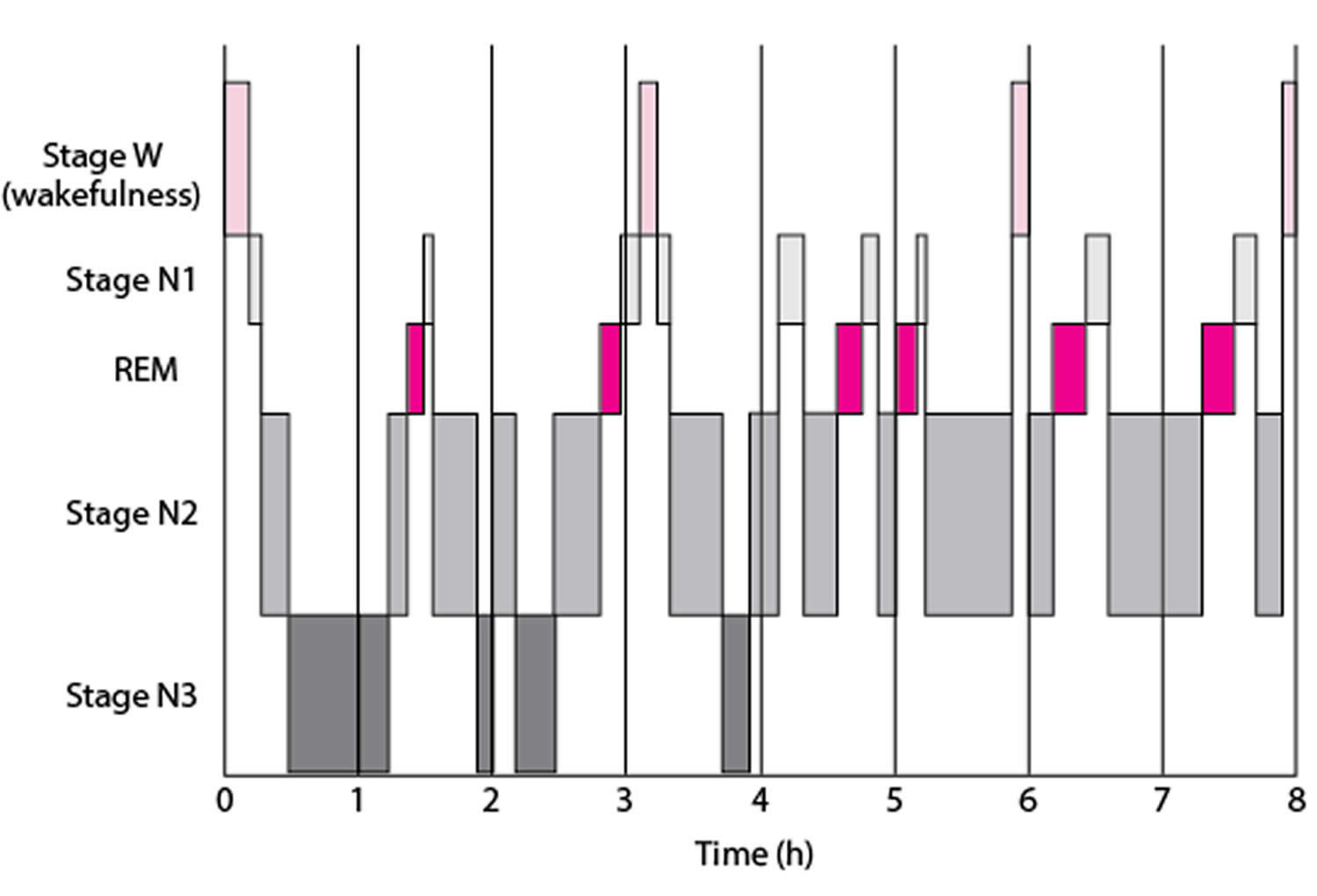
Footnotes: Average times and sequences of sleep cycles during the night. Over the course of a period of sleep, NREM and REM sleep alternate cyclically. The function of alternations between these two types of sleep is not yet understood, but irregular cycling and/or absent sleep stages are associated with sleep disorders 12. For example, instead of entering sleep through NREM, as is typical, individuals with narcolepsy enter sleep directly into REM sleep 13. Rapid eye movement (REM) sleep occurs cyclically throughout the night every 90 to 120 minute. Brief periods of wakefulness (stage W) occur periodically. Sleep time is spent as follows:
- Stage N1: 2–5%
- Stage N2: 45–55%
- Stage N3: 13–23%
- REM: 20–25%
Figure 3. EEG activity of the four stages of sleep
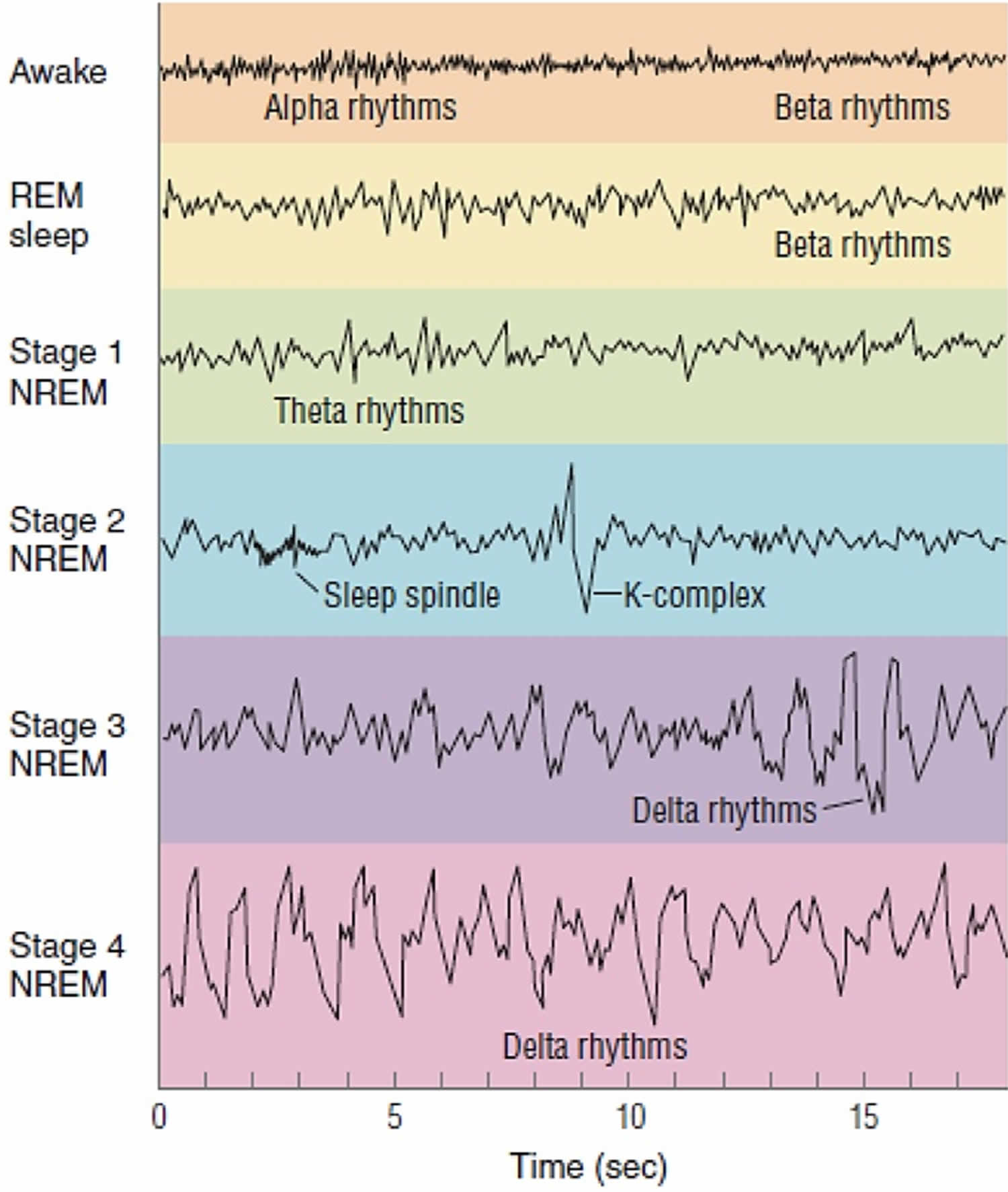
Footnotes: EEG activity during wakefulness with eyes open and closed and during the different stages of sleep. Brainwave activity changes drastically over the course of the different stages of sleep. REM sleep brain activity most closely resembles brain activity while awake.
- Alpha activity is a smooth electrical activity of 8-12 Hz recorded from the brain; generally associated with a state of relaxation during wakefulness.
- Beta activity is a irregular electrical activity of 13-30 Hz recorded from the brain; generally associated with a state of alertness during wakefulness.
- Theta activity is EEG activity of 3.5-7.5 Hz that occurs intermittently during lighter stages of NREM sleep.
- Delta activity is a regular, synchronous electrical activity of less than 4 Hz recorded from the brain; occurs during the deepest stages of slow-wave sleep.
- Sleep spindle is a short burst of 12 to 14 cycle per-second waves observed during NREM sleep, decrease brain’s sensitivity to sensory input and keeps person asleep.
- K complex are single delta waves, sudden sharp wave forms, 1 per minute but can be triggered by noise.
Your sleep-wake cycle is regulated by the circadian rhythm (your body’s natural internal 24-hour clock that manages your sleep-wake cycle and other vital functions, like hormone release and body temperature, by synchronizing with the day-night cycle), which is driven by the suprachiasmatic nucleus (SCN) of the hypothalamus that acts as a “master clock” or “circadian pacemaker”, receiving light cues from your eyes to control the circadian rhythm 16, 17, 18. The circadian rhythm also controls the nocturnal release of adrenocorticotropic hormone (ACTH), prolactin, melatonin, and norepinephrine (NE) 19. External factors like light exposure, meal timing, and activity can influence the circadian rhythm, and disruptions to the circadian rhythm, such as from shift work or jet lag, can negatively affect your health.
The suprachiasmatic nucleus (SCN) of the hypothalamus receives input from nerve cells in the retina that detect light to regulate the circadian rhythm and sleep via multiple pathways that cause the nocturnal release of adrenocorticotropic hormone (ACTH), prolactin, melatonin, and norepinephrine 20. One of the most commonly recognized pathways by which this occurs is via the stimulation of norepinephrine release by the suprachiasmatic nucleus (SCN), which in turn stimulates the pineal gland to release melatonin 21, 18. Wakefulness is maintained by subcortical structures and pathways activating the cortical system 21. This system is termed the “ascending arousal system” and utilizes several major neurochemicals, including:
- Norepinephrine (locus ceruleus)
- Serotonin (midline raphe nuclei)
- Histamine (tuberomammillary nucleus)
- Dopamine (ventral periaqueductal gray matter)
- Acetylcholine (pedunculopontine tegmentum and laterodorsal tegmentum of the pons)
- Orexin (perifornical area)
Transitions between sleep and wake states are influenced by multiple brain structures, including 5:
- Hypothalamus: controls onset of sleep
- Hippocampus: memory region active during dreaming
- Amygdala: emotion center active during dreaming
- Thalamus: prevents sensory signals from reaching the cortex
- Reticular formation: regulates the transition between sleep and wakefulness
- Pons: helps initiate REM sleep. The extraocular movements (eye movements) that occur during REM sleep are due to the activity of PPRF (paramedian pontine reticular formation/conjugate gaze center).
Although it is apparent that humans need sleep, the current understanding of why sleep is an essential part of life is still yet to be determined 5. The current hypotheses on the function of sleep include 22:
- Neural maturation
- Facilitation of learning or memory
- Targeted erasure of synapses to “forget” unimportant information that might clutter the synaptic network
- Cognition
- Clearance of metabolic waste products generated by neural activity in the awake brain
- Conservation of metabolic energy.
Wake or Alert Stage
The first stage is the wake stage or stage W, which further depends on whether your eyes are open or closed. During wakefulness, the EEG is characterized by waves of low amplitude and high frequency. This kind of EEG pattern is known as low-voltage fast activity or activated. During eye-open wakefulness, beta waves predominate. Alpha waves (8–13 Hz) become the predominant pattern as you become drowsy and close your eyes, particularly in occipital regions 23. The Electromyography (EMG, a test that measures the electrical activity of muscles) reveals tonic muscle activity with additional phasic activity related to voluntary movements.
EEG recording: beta waves – highest frequency, lowest amplitude (alpha waves are seen during quiet/relaxed wakefulness)
Non-Rapid Eye Movement (NREM) Sleep Stages
- Stage N1 (Light Sleep): This is the transition between wakefulness and sleep, characterized by slowing heart rate and breathing.
- Stage N2 (Intermediate Sleep): Your heart rate and body temperature decrease further, and your body relaxes.
- Stage N3 (Deep Sleep): This is the deepest stage of Non-Rapid Eye Movement (NREM) sleep, when your body performs restorative work, and it is crucial for feeling rested.
Stage 1 or N1 Sleep
NREM Stage 1 (N1) or Light Sleep serves a transitional role in sleep-stage cycling. This is the lightest stage of sleep and begins when more than 50% of the alpha waves are replaced with low-amplitude mixed-frequency (LAMF) activity. Muscle tone is present in the skeletal muscle, and breathing occurs regularly. This stage lasts around 1 to 7 minutes in the initial cycle, comprising 5% of total sleep time and is easily interrupted by a disruptive noise.
Brain activity on the EEG in stage 1 transitions from wakefulness (marked by rhythmic alpha waves) to low-voltage, mixed-frequency waves. Alpha waves are associated with a wakeful relaxation state and are characterized by a frequency of 8 to 13 cycles per second 13.
EEG recording: Theta waves – low voltage.
Stage 2 or N2 Sleep
NREM Stage 2 (N2) represents deeper sleep as the heart rate and body temperature drop 5. The presence of sleep spindles, K-complexes, or both characterizes it 5. Sleep spindles are brief, powerful bursts of neuronal firing in the superior temporal gyri, anterior cingulate, insular cortices, and thalamus, inducing calcium influx into cortical pyramidal cells. This mechanism is believed to be integral to synaptic plasticity. Numerous studies suggest that sleep spindles are essential in memory consolidation, specifically procedural and declarative memory 24. Individuals who learn a new task have a significantly higher density of sleep spindles than those in a control group 25.
K-complexes are long delta waves that last approximately one second and are known to be the longest and most distinct of all brain waves. K-complexes are shown to function in maintaining sleep and memory consolidation 26.
Stage 2 sleep lasts approximately 10 to 25 minutes in the initial cycle and lengthens with each successive cycle, eventually constituting between 45 to 55 percent of the total sleep episode. Stage 2 sleep is when bruxism (teeth grinding) occurs. An individual in stage 2 sleep requires more intense stimuli than in stage 1 to awaken. Brain activity on an EEG shows relatively low-voltage, mixed-frequency activity characterized by the presence of sleep spindles and K-complexes.
EEG recording: Sleep spindles and K complexes.
Stage 3 or N3 Sleep (Deepest Non-REM Sleep)
Sleep stage 3 or N3 sleep is also known as slow-wave sleep (SWS). This is considered the deepest stage of sleep and is characterized by signals with lower frequencies and higher amplitudes, known as delta waves 5. Sleep stage 3 or N3 sleep is the most difficult to awaken from; for some people, loud noises (> 100 decibels) will not lead to an awake state 5. As people age, they spend less time in this slow, delta-wave sleep and more time in stage N2 sleep 5. Although this stage has the greatest arousal threshold, if someone is awoken during this stage, they will have a transient phase of mental fogginess, known as sleep inertia 5. Cognitive testing shows that individuals awakened during this stage tend to have moderately impaired mental performance for 30 minutes to 1 hour 27. Sleep stage 3 or N3 sleep stage is when the body repairs and regrows tissues, builds bone and muscle, and strengthens the immune system. Sleep stage 3 or N3 sleep is also the stage when sleepwalking, night terrors, and bedwetting occur 28.
Sleep stage 3 or N3 sleep lasts only a few minutes and constitutes about 3 to 8 percent of sleep. The EEG shows increased high-voltage, slow-wave activity.
EEG recording: Delta waves – lowest frequency, highest amplitude.
Rapid Eye Movement (REM) Sleep Stage
Rapid eye movement sleep or REM sleep is the fourth and final stage of sleep and is when you have your most vivid and intense dreams. During REM sleep your brain activity increases to near-waking levels, your eyes dart quickly under your eyelids with fluctuating in your breathing and heart rate and most vivid dreams occur in this phase of sleep. Your muscles become limp (atonia) to prevent you from acting out your dreams. EEG recording shows beta waves – similar to brain waves during wakefulness. You experience your first period of REM sleep about 60 to 90 minutes after falling asleep 20.
REM sleep is defined by the presence of desynchronized (low-voltage, mixed-frequency) brain wave activity, muscle atonia, and bursts of rapid eye movements 13. “Sawtooth” wave forms, theta activity (3 to 7 counts per second), and slow alpha activity also characterize REM sleep 11. During the initial cycle, the REM period may last only 1 to 5 minutes; however, it becomes progressively prolonged as the sleep episode progresses 11.
Most adults need about 2 hours of REM sleep each night, which contributes to brain development, brain function, memory consolidation, and emotional health 29, 30.
Infants and children need more REM sleep, because their brains are still rapidly developing. For example, newborn babies spend around eight hours in REM sleep each day.
How much time you actually spend in REM sleep can vary from night to night. On a night when you’re short of sleep, your total REM time can get cut short. This can trigger your brain to initiate more REM sleep the following night, which is known as a REM rebound 31. Some research also suggests that REM sleep may increase after learning new information 32.
Because REM sleep enables better brain function, memory, and emotional regulation, a lack of REM sleep can cause a range of issues. On top of that, a lack of REM sleep circumvents healthy sleep overall, contributing to sleep deprivation. In the short term, signs of sleep deprivation can include 33:
- Difficulty concentrating
- Excessive daytime sleepiness
- Forgetfulness or poor memory
- Irritability or frustration
- Greater risk of accidents
Over the long term, insufficient sleep can weaken your immune system and raise your risk of conditions like heart disease, diabetes, depression, and anxiety.
How Much Deep Sleep Do I Need?
Different people need different amounts of sleep. Most adults need 7 to 8 hours of sleep a night for good health and mental functioning. Some adults need up to 9 hours a night 34. During a healthy night’s sleep for most adults, deep sleep (stage 3 or N3 sleep) makes up between 10% and 20% of total sleeping time 35. People who sleep less than approximately 7 hours a night are at a greater risk for heart disease, stroke, asthma, arthritis, depression, and diabetes. Nearly 20% of all car crashes, both fatal and nonfatal, are attributed to drowsy driving. Without enough sleep, your brain may struggle to perform basic functions. You may find it hard to concentrate or remember things. You may become moody and lash out at co-workers or people you love.
If you’re not sure about how much sleep you really need, you can use an online Sleep Calculator (https://www.sleepfoundation.org/sleep-calculator). However, your doctor is in the best position to make a detailed sleep recommendation for you based on your age, your overall health and your unique situation.
Table 1. Recommended Sleep Duration
| Age Range | Recommended Daily Sleep | |
|---|---|---|
| Infant | 4–12 months | 12-16 hours (including naps) |
| Toddler | 1–2 years | 11-14 hours (including naps) |
| Preschool | 3–5 years | 10-13 hours (including naps) |
| School-age | 6-12 years | 9-12 hours |
| Teens | 13-18 years | 8-10 hours |
| Adults | 18 years and older | 7 or more hours |
Just as your brain needs sleep to restore itself, so does your body. When you do not have enough sleep, your risk goes up for several illnesses.
- Diabetes. Your body does not do as well controlling blood sugar when you do not get enough sleep.
- Heart disease. Lack of sleep can lead to high blood pressure and inflammation, two things that can damage your heart.
- Obesity. When you do not get enough rest from sleep, you are more prone to overeat. It is also harder to resist foods high in sugar and fat.
- Infection. Your immune system needs you to sleep so it can fight colds and keep you healthy.
- Mental health. Depression and anxiety often make it hard to sleep. They also can become worse after a string of sleepless nights.
The cancer research branch of the World Health Organization has determined that disruption of regular sleep is “probably carcinogenic to humans”, putting it in the same risk category as the infectious agents malaria and human papillomavirus (HPV), as well as the biochemical weapon mustard gas. Sexual health is affected by sleep deprivation as well, as men with the worst sleeping habits have significantly lower sperm counts, decreased circulating testosterone, and even testicular shrinkage.
Adults generally need about 1.5 to 2 hours of deep sleep per night, which equates to roughly 13-23% of their total recommended sleep time. This stage of sleep is crucial for physical recovery, immune function, and cognitive health, so ensure you are getting sufficient overall sleep and practicing healthy sleep habits to obtain enough deep sleep
Why Deep Sleep is Important?
While all stages of sleep are necessary for good health, deep sleep is important because it is when your body undergoes essential physical restoration, immune system strengthening, and hormone production, while your brain processes and stores memories, consolidates learning, and clears waste products 8. During deep sleep, your body works to build and repair tissue, muscles, and bones, including by producing high levels of growth hormone 37. Achieving sufficient deep sleep helps you wake feeling refreshed, promotes long-term physical and mental health, and supports healthy weight and cardiovascular function 8. Deep sleep also promotes immune system functioning. Research suggests that it helps you build stronger immune responses and reduce unwanted chronic inflammation 38.
Slow-wave sleep also helps regulate blood sugar levels. As a result, the risk of developing type 2 diabetes may be higher if you don’t get enough deep sleep 39. And a shortage of deep sleep has also been linked to high blood pressure 40.
Deep sleep is important for cognitive function and memory. Although brain activity slows during deep sleep, this may actually facilitate learning by keeping the brain from becoming oversaturated with information. Evidence suggests that deep sleep also helps eliminate waste material from the brain, which may help protect against dementia 41.
Because deep sleep is an essential component of your nightly rest, a shortage of deep sleep contributes to broader impacts of sleep deprivation. In addition to causing tiredness, a shortage of deep sleep can cause general symptoms of sleep deprivation, including 42:
- Reduced alertness and attention
- Trouble learning and remembering things
- Irritability
- Symptoms of depression or anxiety
- Increased likelihood of accidents and injuries
On top of these immediate effects, a chronic lack of quality sleep can increase the likelihood of multiple health problems, such as:
- Infections and reduced immune system function
- Obesity
- Type 2 diabetes
- Cardiovascular problems, including high blood pressure, stroke, and heart disease
- Kidney disease
If you want to get more deep sleep, focus on enhancing your overall sleep. If your sleep quality and quantity are good, it usually means you’re getting plenty of restorative deep sleep. You get the most deep sleep during the early part of the night.
One of the most reliable ways to improve your sleep is by practicing good sleep hygiene. Good habits include 43:
- Establishing a consistent bedtime and wake-up time
- Ensuring you have a quiet, cool, and dark sleep environment
- Creating a relaxing bedtime routine to wind down in the evening
- Reducing caffeine intake in the afternoon and evening
- Limiting use of mobile devices, tablets, laptops, and other screens for 30 minutes or more before bedtime
There are some additional steps you can try to encourage more deep sleep:
- Take a warm bath: Some research suggests that heating your body with a warm bath before bedtime may induce more slow-wave sleep 44. A warm bath raises body temperature, which promotes blood circulation, and the subsequent cooling may help ease the transition to sleep.
- Change your diet: What you eat and drink before bedtime impacts your sleep. One small study found that people eating a diet high in saturated fats obtained less slow-wave sleep 45. People who ate more fiber were more likely to have increased amounts of deep sleep.
- Listen to binaural beats: Binaural beats are created by listening to two slightly different tones, one in each ear. The difference between the frequencies of those tones creates a perceived third tone, or binaural beat. Limited research suggests that listening to certain binaural beats may contribute to more stage 3 sleep 46.
Parasomnia types
Parasomnias are typically classified by the sleep state from which they arise: non-rapid eye movement sleep (NREM) and rapid eye movement sleep (REM) 47.
Non-REM Parasomnias
The common feature of these parasomnias is recurrent episodes of incomplete awakening from non-REM sleep along with amnesia for the event. Clinical phenotypes of this incomplete arousal from non-REM sleep include sleepwalking, sleep terrors, confusional arousals, and sleep-related eating disorder. They usually arise out of slow wave sleep but can also arise from N2 sleep and are more frequent in the first half of the night. These parasomnias are more frequently seen in children. Factors that impair sleep consolidation and increase sleep fragmentation (e.g, pain, restless legs syndrome, sleep apnea) can result in these parasomnias. Similarly, sleep deprivation and sedating medications can also increase the emergence of these abnormal behaviors by enhancing sleep inertia and by hindering normal sleep-wake transition. Consequently, these disorders manifest as arousals associated with disorientation, amnesia, and confusion.
Immaturity of sleep-wake boundary regulation may be the reason why these occur more commonly in pediatric population. Studies have shown a higher prevalence of HLA DQB1*05:01 and HLA DQB1*04 alleles in various non-REM parasomnias6. Sleepwalking also shows an autosomal dominant trait involving chromosome 20 48.
Sleepwalking
Ambulatory behavior is the primary manifestation of this disorder of arousal. In a systematic review analyzing 51 different studies, Stallman et al. 49 reported a lifetime prevalence of sleepwalking of 6.9% which did not change significantly between childhood and adulthood. This number increased to 47.4% for children with one parent with history of sleepwalking and up to 61.5% for children with both parents with history of sleepwalking 50.
The behaviors can range from aimless wandering to complex, prolonged, and inappropriate episodes that involve driving an automobile, urinating, walking naked, etc. Sleepwalkers typically do not respond to redirection during the episode. In adults, sleepwalking is frequently associated with other disorders like sleep apnea, restless leg syndrome and usage of hypnotic medications. Multiple different medications like benzodiazepine receptor agonists, antidepressants (amitriptyline, paroxetine, mirtazapine, bupropion), antipsychotics (Olanzapine, quetiapine), antihypertensives (Propranolol, metoprolol), fluoroquinolones, montelukast, topiramate have been implicated as triggers for sleepwalking 51.
Sleep Terrors
Sleep terrors consist of episodes of intense fear accompanied by very loud ‘piercing’ screams and loud crying during which the patient appears terrified. The associated autonomic activation results in increase in heartrate, breathing, pupillary dilatation, and sweating. The typical duration of sleep terrors is 3–5 minutes. The prevalence of sleep terrors varies widely in children from 14.7% to 56% 50 and they almost always resolve by late childhood. Sleep terrors in adults are rare, and are more likely to be associated with medications or psychopathology.
Confusional Arousals
These are partial arousals from non-REM sleep that results in a state of disorientation and occasionally, automatic behavior like vocalizations and motor activity. Ambulation and significant sympathetic over-activity is typically absent. Confusional arousals are more common in pediatric population with a prevalence of up to 17% 52. They are brief, lasting for a few minutes, but may sometimes be prolonged, particularly with sedative hypnotic usage. The individuals with confusional arousals show diminished responsiveness to external stimuli during the episode, and have a partial or complete amnesia of the episode afterward.
Sleep-Related Eating Disorder
This parasomnia is more common in women and is characterized by recurrent episodes of binge eating after a partial arousal from non-REM sleep 53. During these episodes patients show a predilection for high carbohydrate food and other peculiar inedible items including raw meat, pet foods etc. This parasomnia is closely related to and is thought to be a variant of sleepwalking. Patients are completely amnestic of their eating behavior, and can have adverse consequences due to their nocturnal eating including weight gain, worsening of diabetes, etc. This parasomnia is different from nocturnal eating disorder/night eating syndrome where patients are aware of their eating behavior, and is associated with anxiety in most cases. Ambien is the most common medication that induces sleep-related eating disorder though several other psychotropic medications are known to precipitate it. Certain other factors like smoking cessation, alcohol consumption, and acute stress are also associated with sleep-related eating disorder. Treatment should begin with elimination of precipitating factors like hypnotic medications and treating the comorbid sleep disorders. Medications that can be used to treat sleep-related eating disorder include dopamine agonists and topiramate.
Sexsomnia
Sexsomnia refers to sleep-related abnormal sexual behaviors. It is classified as a subtype of non-REM parasomnia disorders of arousal in ICSD-3 with abnormal sexual behaviors emerging from partial arousals during slow-wave sleep. It is more common in young males. A wide range of behaviors have been reported including sexual intercourse, attempted intercourse, masturbation, assaultive sexual behavior, sexual vocalizations, etc. Like other parasomnias, other causes of sleep fragmentation should be investigated before initiating pharmacotherapy. Nocturnal seizures, medications like selective serotonin reuptake inhibitors (SSRIs) and pramipexole have been reported to be some of the other causes for sexsomnia. Treatment data is limited but Clonazepam might be helpful in bothersome cases 54.
REM Parasomnias
REM Sleep Behavior Disorder
REM sleep is characterized by rapid eye movements and skeletal muscle atonia. Respiration is diaphragm–based during REM sleep. Dreaming during REM sleep tends to be vivid and detailed, compared to the vague dream content of non-REM sleep. Muscle atonia mediated by brainstem centers, pedunculopontine nucleus and locus coeruleus, serves as a protective mechanism preventing dream enactment during REM sleep. (Figure 2) However, conditions resulting in disruption of this protective mechanism can lead to physical enactment of dream content during REM sleep. This phenomenon is called REM sleep behavior disorder (RBD) 1.
Parkinson disease is strongly associated with REM sleep behavior disorder 1. In fact, REM sleep behavior disorder can predate the initial motor symptoms by years, and is one of the best-known biomarkers for Parkinson’s disease 1. REM sleep behavior disorder is present in 25–50% of Parkinson’s disease patients and is even more frequent in other neurodegenerative disorders such as Multiple System Atrophy and Lewy body dementia. Forty percent of the patients with idiopathic REM sleep behavior disorder develop parkinsonian syndrome within a decade and two-thirds within two decades.
Secondary REM sleep behavior disorder can also be seen in the setting of pontine tegmental lesions, withdrawal from alcohol, medication usage (SSRIs, SNRIs, TCAs, MAO inhibitors), Type 1 narcolepsy, and other neurodegenerative disorders like fronto-temporal dementia, Alzheimer’s dementia. Patients experiencing REM sleep behavior disorder may have mild, low amplitude limb movements that are often overlooked. Some patients have vocalizations. These movements can be significant and violent with apparent goal directed behaviors that can cause injury with lacerations. Curiously, the motor activity in REM sleep behavior disorder in patients with Parkinson’s disease appears smoother, faster, and stronger than the patient’s daytime motor performance. Patients experiencing REM sleep behavior disorder may report falling from their beds during the night. Their bed partners may sometimes be able to understand the dream content based on the patient’s behavior. Some episodes result in arousal from sleep. Usually, REM sleep behavior disorder episodes do not cause significant sleep disruption. Nocturnal REM sleep without atonia is found to be strongly associated with pediatric narcolepsy 55.
Nightmare Disorder
Nightmare disorder is characterized by recurrent dysphoric dreams of disturbing mental experiences. These nightmares mostly occur during REM sleep and result in awakening. The theme of the nightmare is usually distressing to the individual and result in a variety of emotions including anxiety, fear, rage, embarrassment, and disgust. Nightmares are very common in children and the child that wakes up from a nightmare usually can give a good description of the dream. They are also common in patients with increased anxiety levels and in those with posttraumatic stress. Childhood nightmares usually resolve spontaneously. Diagnosis of nightmare disorder should only be given in patients that are experiencing persistent distress and impairments 1.
Recurrent Isolated Sleep Paralysis
The core feature of sleep paralysis is complete inability to move during wakefulness. Unlike REM sleep behavior disorder (RBD) where muscle tone persists during REM sleep, sleep paralysis is characterized by the extension of REM sleep-related muscle atonia into wakefulness. Most cases of sleep paralysis are isolated and sporadic with about 7% of the general population reporting at least one episode of sleep paralysis 56. Sometimes, sleep paralysis can be associated with a sensation of difficult breathing and hallucinatory experiences. Isolated sleep paralysis is a benign condition but can contribute to significant distress when experienced for the first time. Sleep paralysis can happen either during falling asleep (hypnogogic sleep paralysis) or while when waking up (hypnopompic sleep paralysis). In some cases, triggers for sleep paralysis include sleep deprivation and comorbid sleep apnea. Though sleep paralysis is a benign problem, it can happen frequently causing a significant fear of initiating sleep at which time the more appropriate term for it would be recurrent isolated sleep paralysis.
Other Parasomnias
Sleep Enuresis
Sleep enuresis is characterized by recurrent, involuntary voiding during sleep for at least three months. sleep enuresis occurs in 15 to 20% of five-year olds, and is three times more common in boys. In primary sleep enuresis, recurrent episodes of involuntary voiding happen at least twice a week during sleep after five years of age in a patient who was never consistently dry during sleep for six consecutive months. It is considered secondary sleep enuresis if the patient was consistently dry for at least six months before and began wetting later. This condition is associated with difficulty waking up from sleep in response to an urge to urinate in the setting of a full urinary bladder. Though psychological problems are a rare cause of primary sleep enuresis, secondary sleep enuresis is more commonly seen in children who have recently experienced a significant psychosocial stress. Secondary sleep enuresis is also commonly associated with chronic constipation and fecal soiling. There is often a high prevalence of enuresis among the parents, siblings and other relatives of children with primary enuresis.
Three important factors contribute to the risk of developing sleep enuresis: large nocturnal urine volume production, nocturnal bladder over-activity and difficulty arousing from sleep. Multiple studies suggest that difficulty arousing from sleep is more important in primary enuresis while bladder overactivity is more important in secondary enuresis. Sleep fragmentation by disorders like sleep apnea is also highly correlated with sleep enuresis and successful treatment of sleep apnea results in reduction or elimination of sleep enuresis. Typically, the spontaneous cure rate of primary sleep enuresis is about 15% per year.
Sleep-Related Hallucinations
Sleep-related hallucinations are unreal experiences that occur at the onset of sleep or upon awakening from sleep. They are predominantly visual hallucinations but can also be auditory or even tactile in nature. Hallucinations occurring at sleep onset are called ‘Hypnogogic hallucinations’ while those occurring on awakening are called ‘Hypnopompic hallucinations.’ Sometimes, they can be very complex and can follow a sudden awakening without recall of a preceding dream. These ‘complex nocturnal hallucinations’ can result in injuries when patients jump out of bed in terror. Sleep-related hallucinations can be associated with other parasomnias including sleep talking or sleepwalking. They are also very common in narcolepsy but can also be seen in a high proportion of general population. They are more common in younger persons, and occur slightly more frequently in women. Large populations studies suggest that alcohol use, mood disorders, insomnia, and drug use increase the likelihood of sleep-related hallucinations. Complex nocturnal visual hallucinations, on the other hand, are very rare and may be seen in patients with narcolepsy, Parkinson disease, Lewy body dementia, midbrain and diencephalic pathology, and in the setting of beta-blocker medication usage.
Exploding Head Syndrome
Exploding Head Syndrome is a condition where the affected individuals experience a sudden noise or a sense of explosion that results in abrupt arousal with a sense of fright and happens in the setting of either falling asleep or while waking up. This whole experience is not associated with significant complaints of pain. The term exploding head syndrome was first coined by J.M.S Pearce 57 and despite its memorable name, relatively little is known about this condition. It is not uncommon for patients suffering from exploding head syndrome to interpret their condition to be far more serious and seek medical attention. The sounds reported during exploding head syndrome are varied and include violent explosions, door slamming sounds, buzzing, nearby thunder, whip lash, etc 58. Some patients experience visual symptoms like light flashes, feelings of intense heat, epigastric sensations and an aura of electrical sensation that ascends from lower torso to the head 59. Exploding head syndrome should be differentiated from headache syndromes like cluster headache, thunderclap headaches, hypnic headache and from nocturnal seizures. Patient education and reassurance are the mainstay treatments, though medications like flunarizine, nifedipine, clomipramine, topiramate and carbamazepine have been tried with limited benefit. Stress and anxiety reduction has been found to be helpful.
Parasomnias Due to Medical Disorder
The primary feature of this diagnosis is the presence of a parasomnia that can be explained by an underlying medical or neurological disorder. Charles Bonnet syndrome is characterized by vivid visual imagery in the setting of partial or complete visual loss. Peduncular hallucinosis is a syndrome of hallucinations that can happen in the setting of brainstem and diencephalic pathology 60. Sleep-related hallucinations, seen in the setting of Charles Bonnet syndrome and peduncular hallucinosis, are good examples of parasomnias due to medical disorder. Though REM sleep behavior disorder is technically a parasomnia that occurs in the setting of an underlying neurological disorder (α-synucleopathy), it is considered as a separate parasomnia.
Parasomnia Due to Medication or Substance Abuse
The essential feature of this diagnosis is dependent upon the onset or worsening of a parasomnia in the setting of usage of a medication or bioactive substance. Multiple medications including selective serotonin reuptake inhibitors, venlafaxine, tricyclic antidepressants, monoamine oxidase (MAO) inhibitors have been associated with worsening of REM sleep behavior disorder (RBD). Beta-adrenergic blocking agents can be associated with sleep-related hallucinations. Zolpidem and Zopiclone are associated with a variety of parasomnias including sleep driving and sleep-related eating disorder.
Parasomnia in the Setting of IgLON5 Autoimmunity
Sabater, et al. 61 described a case series of patients showing a unique NREM and REM parasomnia in the setting of autoantibodies against IgLON5, a neuronal cell adhesion protein. This syndrome is characterized by breathing dysfunction, gait instability and brainstem symptoms. Despite being described as a unique parasomnia, this disease has some features of abnormal sleep-related motor activation (agrypnia excitata) and may not be a true parasomnia 62.
Sleep Talking
Sleep talking is highly prevalent with a lifetime prevalence up to 66% 63. Due to its high prevalence and the benign nature of this parasomnia, it is typically considered a normal variant. It is characterized by varying degrees of comprehensibility, and can happen both, during REM and non-REM sleep. It rarely causes problems but sometimes can be frequent and loud disrupting the sleep of bed partners or roommates.
Catathrenia is another sleep-related phenomenon consisting of loud groaning sounds during episodes of prolonged expiration. It was first reported in 1983 by De Roeck et al. Initially, it was classified among Parasomnias in the International Classification of Sleep Disorders– 2nd edition 47 but was later included among respiratory disorders in the International Classification of Sleep Disorders-3rd edition 64.
Parasomnia causes
Parasomnias often run in families and so there is probably a genetic factor in many cases. Brain disorders may be responsible for some parasomnias, such as many cases of REM sleep behavior disorder (RBD). Parasomnias may also be triggered by other sleep disorders such as obstructive sleep apnea, and by various medications.
The three states of human behavior are Wakefulness, Non-REM sleep and REM sleep, and are previously thought to be mutually exclusive. Non-REM sleep in turn is divided into three stages (N1, N2, and N3) Transitions from one behavioral state to another is not a quick switch but involves reorganization and transition of various neural centers before a specific state manifests unequivocally. Recent research has shown that combinations of one or more of these states can result in unstable states, and an arousal out of these unstable states can give rise to abnormal behaviors manifesting as parasomnias 65. It is also suggested that deafferentation of locomotor centers in the spinal and at supraspinal levels, from the generators of different sleep states may result in motor activity in the setting of arousals 66.
Most of the non-REM parasomnias arise out of N3 non-REM sleep. Any condition that promotes non-REM sleep fragmentation (such as pain conditions, restless legs syndrome, periodic limb movements, sleep-related breathing disorders, etc.) increase the risk of parasomnias. Also, conditions of increased sleep drive including sleep deprivation and sedative medications are risk factors for parasomnias. Certain HLA haplotypes like HLA DQ B1*05:01 and HLA DQ B1*04 are considered risk factors for the development of parasomnias. First-degree relatives of patients with parasomnias have a higher prevalence of similar parasomnias.
The major differential diagnoses for both non-REM and REM parasomnia include nocturnal seizures, intoxicated states, medication-induced complex behaviours, nocturnal panic attacks and dissociative disorders 67.
Figure 1. Pathogenesis of parasomnias

Parasomnia symptoms
All parasomnias occur from sleep, and non-REM parasomnias usually occur among individuals aged 5–25 years with a family history of similar parasomnias (e.g., sleepwalking or sleep terrors) and involve physical and verbal activity of varying complexity 2. Typically, the sleeper returns to sleep and is amnestic in the morning, with the behaviour being reported by others or discovered because items have been moved or used during the night or the events have resulted in injury 47.
External (e.g., noise, temperature change) or internal (e.g., apnea, periodic limb movement) events may cause an arousal or partial awakening, usually from stage III and IV sleep, which occurs in the first 90 minutes of the sleep period. Arousal or partial awakening can also occur during stage II sleep later in the night 67. Sleep deprivation or disruption from any cause (e.g., restless legs syndrome, obstructive sleep apnea) can precipitate these events in susceptible individuals.
In contrast, REM sleep behaviour disorder is characterized by verbalizations and actions consistent with dream enactment (e.g., fight or flight behaviours) that usually awaken the sleeper who, unlike those with NREM parasomnias, can often recall the event, including the dream and its associated actions 47.
The characteristics of non-REM and REM parasomnias are summarized in Table 1. Distinguishing between non-REM and REM parasomnias is important because the treatment and prognosis are different. Nonrapid eye movement parasomnias are more common in younger people and are usually “outgrown” by young adulthood, whereas REM parasomnias present in late adult life and are associated with degenerative brain diseases 67.
Table 1. Characteristics of parasomnias
| Nonrapid eye movement parasomnia | Rapid eye movement parasomnia | ||||||
|---|---|---|---|---|---|---|---|
| Confusional arousal | Sleepwalking | Sleep terrors | Sleep-related eating disorder | REM sleep behaviour disorder | Sleep paralysis | Nightmare disorder | |
| Emerges from | Stages II, III and IV* | Stages III and IV | Stages III and IV | Stages II, III and IV | REM sleep | REM sleep | REM sleep |
| Time of night | Anytime during sleep | First third of sleep | First third of sleep | Anytime during sleep | Anytime but most frequently last third of sleep | Anytime | Anytime but most frequently last third of sleep |
| Vocalizations | Yes | Yes | Marked (screaming or crying) | Yes | Marked | Slight (moaning or groaning) | Sometimes |
| Getting out of bed | Rare | Usual | Sometimes | Always (food seeking) | Yes | No | No |
| Responsiveness on awakening | Decreased | Decreased | Decreased | Decreased | Responsive | Responsive | Responsive |
| Autonomic activity | Normal | Normal | Increased | Normal | No | No | Yes |
| Post-event confusion | Yes | Yes | Yes | Yes | No | No | No |
| Prevalence | 4.2% | 1%–4% in adults, 80% of adults have sleep walked as children | 1%–2% in adults | Unknown; estimated to be 1%–5% in general population but higher among patients with eating disorders; 2–4 times more common among women | Unknown; estimated to be 0.38% in the general population and 0.5% among elderly people; about 33% of patients with newly diagnosed Parkinson Disease1; more common among men | Unknown. 15%–40% has been reported among students under 30 years for at least one episode1 and 1%–10% of the population for multiple episodes | 5%–8% of adults; more common among women |
| Amnesia of event | Yes | Yes | Yes | Variable | No | No | No |
| Injury risk | Low if undisturbed | Low if undisturbed; may strike out if disturbed or intoxicated | More common; may injure self trying to escape; may strike out if disturbed or intoxicated | Self-injury from food preparation (cuts, burns, poisoning) | May injure self or partner as part of dream enactment | None | None |
| Family history of parasomnias | Yes | Yes | Yes | Yes | Occasionally | Yes | Yes; twin studies suggest a genetic predisposition and co-occurrence with other parasomnias |
Footnote: *The scoring of sleep has changed recently with Stage II sleep being renamed N2, and stages III and IV being named N3. Because most clinicians are familiar with the old staging nomenclature.
[Source 2 ]Parasomnia diagnosis
The approach to a patient presenting with abnormal nocturnal behaviors should start with a good history and if possible, an account from a firsthand witness. A comprehensive video polysomnography with expanded electroencephalogram (EEG) and electromyography (EMG) channels should be considered if the parasomnia is presenting with an unusual phenotype or an atypical age and if it is happening frequently. The main purpose of polysomnographic evaluation is to identify triggers of parasomnias like sleep apnea, periodic limb movements and mimics of parasomnias like nocturnal seizures.
It should be noted that not all nocturnal abnormal behaviors are parasomnias. Nocturnal seizures can be sometimes confused with parasomnias. Both temporal lobe and frontal lobe seizures can present during sleep. Similarly, psychogenic/psychiatric conditions like post-traumatic stress disorder (PTSD) and nocturnal panic attacks also mimic parasomnias.
Parasomnia treatment
As parasomnias are more common in children, their presence tends to elicit anxiety and panic in the parents. Reassurance and education is very important as most kids grow out of these behaviors without any intervention.
In general, for non-REM parasomnias, the diagnostic evaluation should start with an attempt to find out potential triggers. One of the common risk factors for non-REM parasomnias is sleep disruption, and so the clinician should use a combination of history and diagnostic testing to determine if there are any sleep disorders like sleep-related breathing disorder, periodic limb movements, etc. Similarly, a careful history should be able to identify any environmental stimulants like loud noise that can be contributing to sleep disruption. Patients should be educated about maintaining a good sleep hygiene. Medications (Z drugs [zolpidem, zopiclone and zaleplon], antidepressants, antipsychotics) that are associated with a variety of parasomnias should be evaluated for the possibility of causality.
Patients with REM sleep behavior disorder should be carefully assessed for risk of injury and safety measures should be undertaken. The first step is to make the sleeping environment safe – e.g. putting soft pads around the bed to minimize the impact of falls, using pillows, keeping distance from the bed partner, removing sharp and potentially injurious objects. Bed partner should be aware of these behaviors and try to have an alternative sleeping arrangement rather than sleeping on the same bed as the patient. Similar safety measures should be employed in cases of non-REM parasomnias like sleepwalking. Bed or door alarms can help prevent patient wandering away in their sleep.
Safety precautions for patients with parasomnia
- Identify, then reduce or eliminate known precipitating factors
- Avoid sleep deprivation: maintain a regular sleep–wake schedule with a constant waking time
- Limit, preferably eliminate, the use of alcohol and recreational drugs
- Maximize safety of the sleeping environment
- Sleep on the lowest floor in the house
- Use a mattress on the floor
- Sleep solo or use two queen-sized mattresses pushed together for co-sleeping
- Minimize or pad bedside furniture
- Secure bedside light above bed but out of reach
- Use plastic cups or bottles, if bedside water is required
- Consider child-proof door knobs, door wedges or alarms
- Remove or lock any weapons or dangerous household items
Patients with confusional arousals (as well as those with other parasomnias) should be counselled to not co-sleep with children, because even a single event has the potential for very serious consequences. It is also useful for patients to let others know of the disorder if they are going on a group trip (e.g., business trip, camping) 2.
Pharmacological treatments for REM sleep behavior disorder include Clonazepam and Melatonin. Clonazepam is a benzodiazepine and acts at GABA receptors. Melatonin on the other hand is an over-the-counter dietary supplement in the United States and acts on melatonin receptors. Other medications that showed success in limited case series include pramipexole, levodopa, carbamazepine, and imipramine.
- Bollu PC, Goyal MK, Thakkar MM, Sahota P. Sleep Medicine: Parasomnias. Mo Med. 2018;115(2):169–175. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6139852[↩][↩][↩][↩][↩]
- Fleetham JA, Fleming JA. Parasomnias. CMAJ. 2014;186(8):E273–E280. doi:10.1503/cmaj.120808 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4016090[↩][↩][↩][↩][↩]
- Night terrors, sleepwalking, and confusional arousals in the general population: their frequency and relationship to other sleep and mental disorders. Ohayon MM, Guilleminault C, Priest RG. J Clin Psychiatry. 1999 Apr; 60(4):268-76; quiz 277.[↩]
- Psychiatric Illness and Parasomnias: a Systematic Review. Waters F, Moretto U, Dang-Vu TT. Curr Psychiatry Rep. 2017 Jul; 19(7):37.[↩]
- Patel AK, Reddy V, Shumway KR, et al. Physiology, Sleep Stages. [Updated 2024 Jan 26]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK526132[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Memar P, Faradji F. A Novel Multi-Class EEG-Based Sleep Stage Classification System. IEEE Trans Neural Syst Rehabil Eng. 2018 Jan;26(1):84-95. doi: 10.1109/TNSRE.2017.2776149[↩]
- Stages of Sleep: What Happens in a Normal Sleep Cycle? https://www.sleepfoundation.org/stages-of-sleep[↩][↩]
- How Much Deep Sleep Do You Need? https://www.sleepfoundation.org/stages-of-sleep/deep-sleep[↩][↩][↩]
- Malik J, Lo YL, Wu HT. Sleep-wake classification via quantifying heart rate variability by convolutional neural network. Physiol Meas. 2018 Aug 20;39(8):085004. doi: 10.1088/1361-6579/aad5a9[↩]
- Feinberg I, Floyd TC. Systematic trends across the night in human sleep cycles. Psychophysiology. 1979 May;16(3):283-91. doi: 10.1111/j.1469-8986.1979.tb02991.x[↩]
- Institute of Medicine (US) Committee on Sleep Medicine and Research; Colten HR, Altevogt BM, editors. Sleep Disorders and Sleep Deprivation: An Unmet Public Health Problem. Washington (DC): National Academies Press (US); 2006. 2, Sleep Physiology. Available from: https://www.ncbi.nlm.nih.gov/books/NBK19956[↩][↩][↩]
- Zepelin H, Siegel JM, Tobler I. Mammalian sleep. In: Kryger MH, Roth T, Dement WC, editors. Principles and Practice of Sleep Medicine. 4th ed. Philadelphia: Elsevier/Saunders; 2005. pp. 91–100.[↩]
- Carskadon M, Dement W. Normal human sleep: An overview. In: Kryger MH, Roth T, Dement WC, editors. Principles and Practice of Sleep Medicine. 4th ed. Philadelphia: Elsevier Saunders; 2005. pp. 13–23.[↩][↩][↩]
- Approach to the Patient With a Sleep or Wakefulness Disorder. https://www.msdmanuals.com/professional/neurologic-disorders/sleep-and-wakefulness-disorders/approach-to-the-patient-with-a-sleep-or-wakefulness-disorder[↩]
- Electroencephalogram (EEG) techniques measuring sleep activity and sleep stages. https://quizlet.com/au/336073417/electroencephalogram-eeg-techniques-measuring-sleep-activity-and-sleep-stages-diagram[↩]
- Reddy S, Reddy V, Sharma S. Physiology, Circadian Rhythm. [Updated 2023 May 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK519507[↩]
- Tononi G, Cirelli C. Sleep and the price of plasticity: from synaptic and cellular homeostasis to memory consolidation and integration. Neuron. 2014 Jan 8;81(1):12-34. doi: 10.1016/j.neuron.2013.12.025[↩]
- España RA, Scammell TE. Sleep neurobiology from a clinical perspective. Sleep. 2011 Jul 1;34(7):845-58. doi: 10.5665/SLEEP.1112[↩][↩]
- Zajac A, Skowronek-Bała B, Wesołowska E, Kaciński M. Napadowe zaburzenia snu u dzieci w wideo/polisomnografii [Sleep paroxysmal events in children in video/polysomnography]. Przegl Lek. 2010;67(9):762-9. Polish.[↩]
- Feriante J, Araujo JF. Physiology, REM Sleep. [Updated 2023 Feb 13]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK531454[↩][↩]
- Carley DW, Farabi SS. Physiology of Sleep. Diabetes Spectr. 2016 Feb;29(1):5-9. doi: 10.2337/diaspect.29.1.5[↩][↩]
- Frank, M.G., Heller, H.C. (2018). The Function(s) of Sleep. In: Landolt, HP., Dijk, DJ. (eds) Sleep-Wake Neurobiology and Pharmacology . Handbook of Experimental Pharmacology, vol 253. Springer, Cham. https://doi.org/10.1007/164_2018_140[↩]
- Varga B, Gergely A, Galambos Á, Kis A. Heart Rate and Heart Rate Variability during Sleep in Family Dogs (Canis familiaris). Moderate Effect of Pre-Sleep Emotions. Animals (Basel). 2018 Jul 2;8(7):107. doi: 10.3390/ani8070107[↩]
- Antony JW, Schönauer M, Staresina BP, Cairney SA. Sleep Spindles and Memory Reprocessing. Trends Neurosci. 2019 Jan;42(1):1-3. doi: 10.1016/j.tins.2018.09.012[↩]
- Gais S, Mölle M, Helms K, Born J. Learning-dependent increases in sleep spindle density. J Neurosci. 2002 Aug 1;22(15):6830-4. doi: 10.1523/JNEUROSCI.22-15-06830.2002[↩]
- Gandhi MH, Emmady PD. Physiology, K Complex. [Updated 2023 May 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK557469[↩]
- Hilditch CJ, McHill AW. Sleep inertia: current insights. Nat Sci Sleep. 2019 Aug 22;11:155-165. doi: 10.2147/NSS.S188911[↩]
- El Shakankiry HM. Sleep physiology and sleep disorders in childhood. Nat Sci Sleep. 2011 Sep 6;3:101-14. doi: 10.2147/NSS.S22839[↩]
- Blumberg MS, Lesku JA, Libourel PA, Schmidt MH, Rattenborg NC. What Is REM Sleep? Curr Biol. 2020 Jan 6;30(1):R38-R49. doi: 10.1016/j.cub.2019.11.045[↩]
- Peever J, Fuller PM. The Biology of REM Sleep. Curr Biol. 2017 Nov 20;27(22):R1237-R1248. doi: 10.1016/j.cub.2017.10.026[↩]
- Feriante J, Singh S. REM Rebound Effect. [Updated 2024 Sep 12]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK560713[↩]
- Rasch B, Born J. About sleep’s role in memory. Physiol Rev. 2013 Apr;93(2):681-766. doi: 10.1152/physrev.00032.2012[↩]
- Sleep and your health. https://medlineplus.gov/ency/patientinstructions/000871.htm[↩]
- Consensus Conference Panel; Watson NF, Badr MS, Belenky G, et al. Recommended Amount of Sleep for a Healthy Adult: A Joint Consensus Statement of the American Academy of Sleep Medicine and Sleep Research Society. J Clin Sleep Med. 2015 Jun 15;11(6):591-2. doi: 10.5664/jcsm.4758[↩]
- Normal Sleep, Sleep Physiology, and Sleep Deprivation. https://emedicine.medscape.com/article/1188226-overview#showall[↩]
- https://www.sleepfoundation.org/sleep-calculator[↩]
- Dijk DJ. Regulation and functional correlates of slow wave sleep. J Clin Sleep Med. 2009 Apr 15;5(2 Suppl):S6-15. https://pmc.ncbi.nlm.nih.gov/articles/PMC2824213[↩]
- Besedovsky L, Lange T, Born J. Sleep and immune function. Pflugers Arch. 2012 Jan;463(1):121-37. doi: 10.1007/s00424-011-1044-0[↩]
- Vlahoyiannis A, Aphamis G, Bogdanis GC, Sakkas GK, Andreou E, Giannaki CD. Deconstructing athletes’ sleep: A systematic review of the influence of age, sex, athletic expertise, sport type, and season on sleep characteristics. J Sport Health Sci. 2021 Jul;10(4):387-402. doi: 10.1016/j.jshs.2020.03.006[↩]
- Javaheri S, Zhao YY, Punjabi NM, Quan SF, Gottlieb DJ, Redline S. Slow-Wave Sleep Is Associated With Incident Hypertension: The Sleep Heart Health Study. Sleep. 2018 Jan 1;41(1):zsx179. doi: 10.1093/sleep/zsx179[↩]
- Zhang Y, Gruber R. Can Slow-Wave Sleep Enhancement Improve Memory? A Review of Current Approaches and Cognitive Outcomes. Yale J Biol Med. 2019 Mar 25;92(1):63-80. https://pmc.ncbi.nlm.nih.gov/articles/PMC6430170[↩]
- Healthy Sleep. https://medlineplus.gov/healthysleep.html[↩]
- Changing your sleep habits. https://medlineplus.gov/ency/patientinstructions/000757.htm[↩]
- Maeda T, Koga H, Nonaka T, Higuchi S. Effects of bathing-induced changes in body temperature on sleep. J Physiol Anthropol. 2023 Sep 8;42(1):20. doi: 10.1186/s40101-023-00337-0[↩]
- St-Onge MP, Roberts A, Shechter A, Choudhury AR. Fiber and Saturated Fat Are Associated with Sleep Arousals and Slow Wave Sleep. J Clin Sleep Med. 2016 Jan;12(1):19-24. doi: 10.5664/jcsm.5384[↩]
- Lee M, Song CB, Shin GH, Lee SW. Possible Effect of Binaural Beat Combined With Autonomous Sensory Meridian Response for Inducing Sleep. Front Hum Neurosci. 2019 Dec 2;13:425. doi: 10.3389/fnhum.2019.00425[↩]
- International classification of sleep disorders: diagnostic and coding manual. 2nd ed Westchester (IL): American Academy of Sleep Medicine; 2007[↩][↩][↩][↩]
- Novel genetic findings in an extended family pedigree with sleepwalking. Licis AK, Desruisseau DM, Yamada KA, Duntley SP, Gurnett CA. Neurology. 2011 Jan 4; 76(1):49-52.[↩]
- Stallman HM, Kohler M. Prevalence of sleepwalking: a systematic review and meta-analysis. PloS one. 2016;11(11):e0164769[↩]
- Childhood Sleepwalking and Sleep Terrors: A Longitudinal Study of Prevalence and Familial Aggregation. Petit D, Pennestri MH, Paquet J, Desautels A, Zadra A, Vitaro F, Tremblay RE, Boivin M, Montplaisir J. JAMA Pediatr. 2015 Jul; 169(7):653-8.[↩][↩]
- Medication induced sleepwalking: A systematic review. Stallman HM, Kohler M, White J. Sleep Med Rev. 2018 Feb; 37():105-113.[↩]
- Parasomnias: epidemiology and management. Wills L, Garcia J. CNS Drugs. 2002; 16(12):803-10.[↩]
- Sleep-related eating disorder and its associated conditions. Inoue Y. Psychiatry Clin Neurosci. 2015 Jun; 69(6):309-20.[↩]
- Sexsomnia: parasomnia associated with sexual behaviour during sleep. Ariño H, Iranzo A, Gaig C, Santamaria J. Neurologia. 2014 Apr; 29(3):146-52.[↩]
- Bin-Hasan S, Videnovic A, Maski K. Nocturnal REM Sleep Without Atonia Is a Diagnostic Biomarker of Pediatric Narcolepsy. Journal of Clinical Sleep Medicine. 2018;14(02):245–252[↩]
- Sharpless BA, Barber JP. Lifetime prevalence rates of sleep paralysis: a systematic review. Sleep medicine reviews. 2011;15(5):311–315.[↩]
- Pearce J. Exploding head syndrome. The Lancet. 1988;332(8605):270–271[↩]
- Sharpless BA. Exploding head syndrome. Sleep medicine reviews. 2014;18(6):489–493[↩]
- Kowey P, Marinchak R, Rials S. More things that go bang in the night. N Engl J Med. 1993;328:1570–1571[↩]
- Benke T. Peduncular hallucinosis. Journal of neurology. 2006;253(12):1561–1571[↩]
- Sabater L, Gaig C, Gelpi E, et al. A novel non-rapid-eye movement and rapid-eye-movement parasomnia with sleep breathing disorder associated with antibodies to IgLON5: a case series, characterisation of the antigen, and post-mortem study. The Lancet Neurology. 2014;13(6):575–586[↩]
- Della Marca G, Iorio R, Losurdo A, Mirabella M, Frisullo G. Sleep disorder associated with antibodies to IgLON5: parasomnia or agrypnia? The Lancet Neurology. 2014;13(9):864[↩]
- Bjorvatn B, Grønli J, Pallesen S. Prevalence of different parasomnias in the general population. Sleep Medicine. 2010;11(10):1031–1034[↩]
- American Academy of Sleep Medicine (2014) International classification of sleep disorders, 3rd edn. American Academy of Sleep Medicine, Darien[↩]
- Mahowald M. Overview of parasomnias. American Academy of Sleep Medicine; 1999.[↩]
- Neuroethological approach to frontolimbic epileptic seizures and parasomnias: The same central pattern generators for the same behaviours. Tassinari CA, Cantalupo G, Högl B, Cortelli P, Tassi L, Francione S, Nobili L, Meletti S, Rubboli G, Gardella E. Rev Neurol (Paris). 2009 Oct; 165(10):762-8.[↩]
- Diagnostic and statistical manual of mental disorders, 5th edition: DSM-5. Arlington (VA): American Psychiatric Association, 2013[↩][↩][↩]





{kind=link}