Contents
What is lattice degeneration
Lattice degeneration of the retina also called circumferential, equatorial or palisade retinal degeneration, is a developmental thinning of the retina that occurs in about 6-8 percent of the general population 1. Lattice degeneration is a risk factor for retinal tears and retinal detachment, but the vast majority of people with lattice degeneration never have a problem. Lattice degeneration of the retina is present in 30% of retinal detachments in implanted intraocular lens patients 2. Retinal tears are present in up to 2.4% cases of lattice degeneration. Retinal tears usually develop along the posterior and lateral edges of the lattice degeneration lesion. In many such tears, an incomplete posterior vitreous detachment is present with its edge attached to the posterior margin of the lattice degeneration lesion 3. Retinal detachment is seen in less than 1% of patients with lattice degeneration if the fellow eye did not have a retinal detachment 4. However, with a history of retinal detachment in one eye, the risk of retinal detachment in the fellow eye over seven years is between 2-5% 5. People with lattice degeneration should immediately report any floaters, flashing lights or loss of vision and should have a yearly dilated examination by an ophthalmologist.
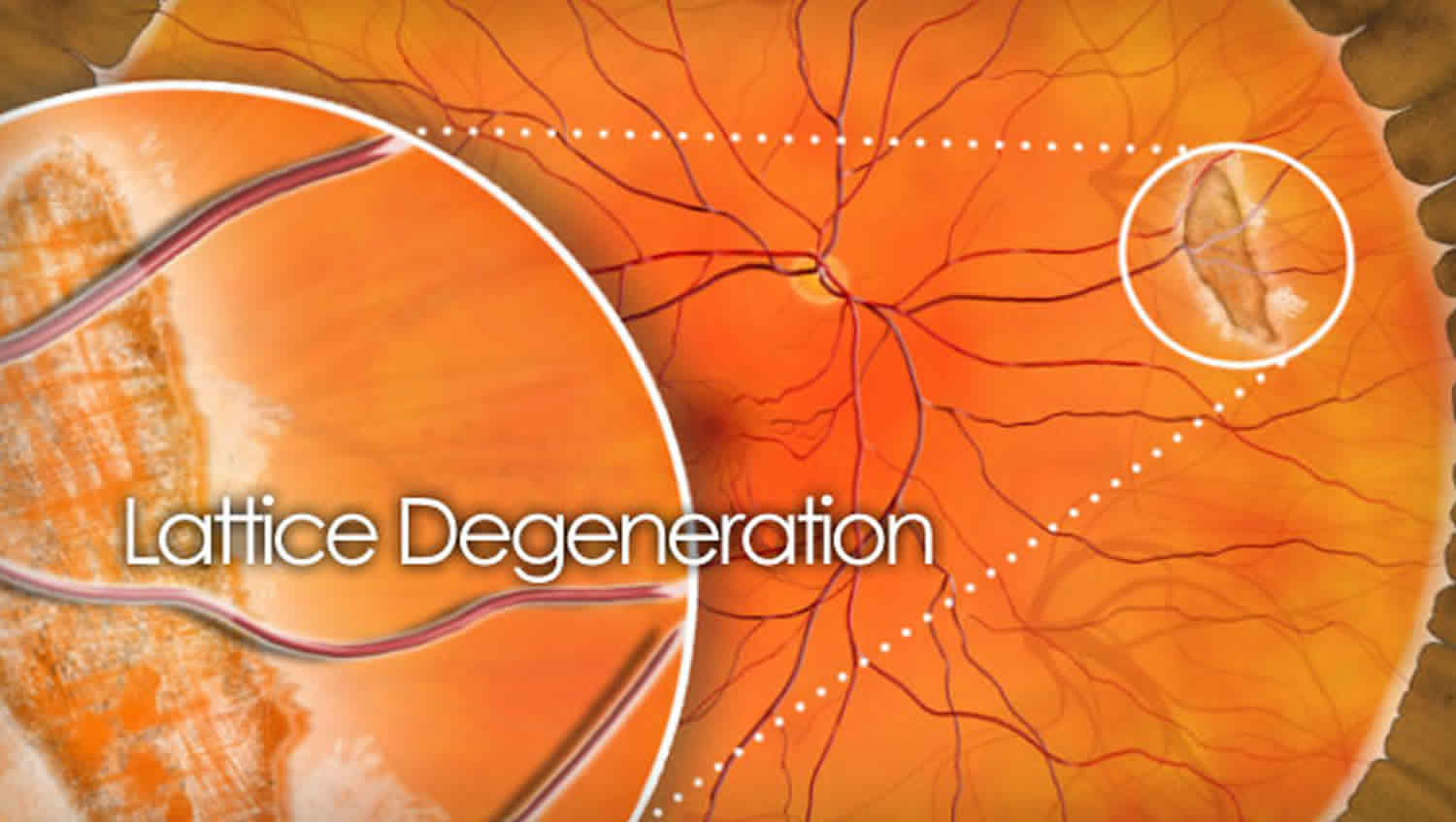
Lattice degeneration often takes the appearance of an elongated area of inner retinal thinning, its long axis tending to lie parallel to the ora serrata 6. Lattice degeneration may also be seen on either side of a major retinal vessel, following a perivascular pattern in Wagner or Stickler syndrome 6. Lesions that are located at or posterior to the equator tend to be larger. The base of the lesion has a moth-eaten uneven appearance and the overlying thin degenerating retina is often jagged 7. White lines in a criss-crossing or fish-bone pattern may or may not be seen within the lesion, which renders the name “lattice” degeneration to this lesion. These white lines are in fact glial or hyaline sheathed vessels which may be occluded. These white lines are seen in 11.9 to 42.9% of patients with lattice degeneration 7. Normal appearing retina exists between the lesion and the ora serrata as in this case. This may be confirmed in appropriate cases by scleral depression to differentiate lattice from a pigmented prominent vitreous base 8.
While there are no know risk factors for lattice degeneration, it is most commonly found as an incidental finding on routine ophthalmologic exams. Lattice degeneration may be found in symptomatic patients in association with retina tears or holes.
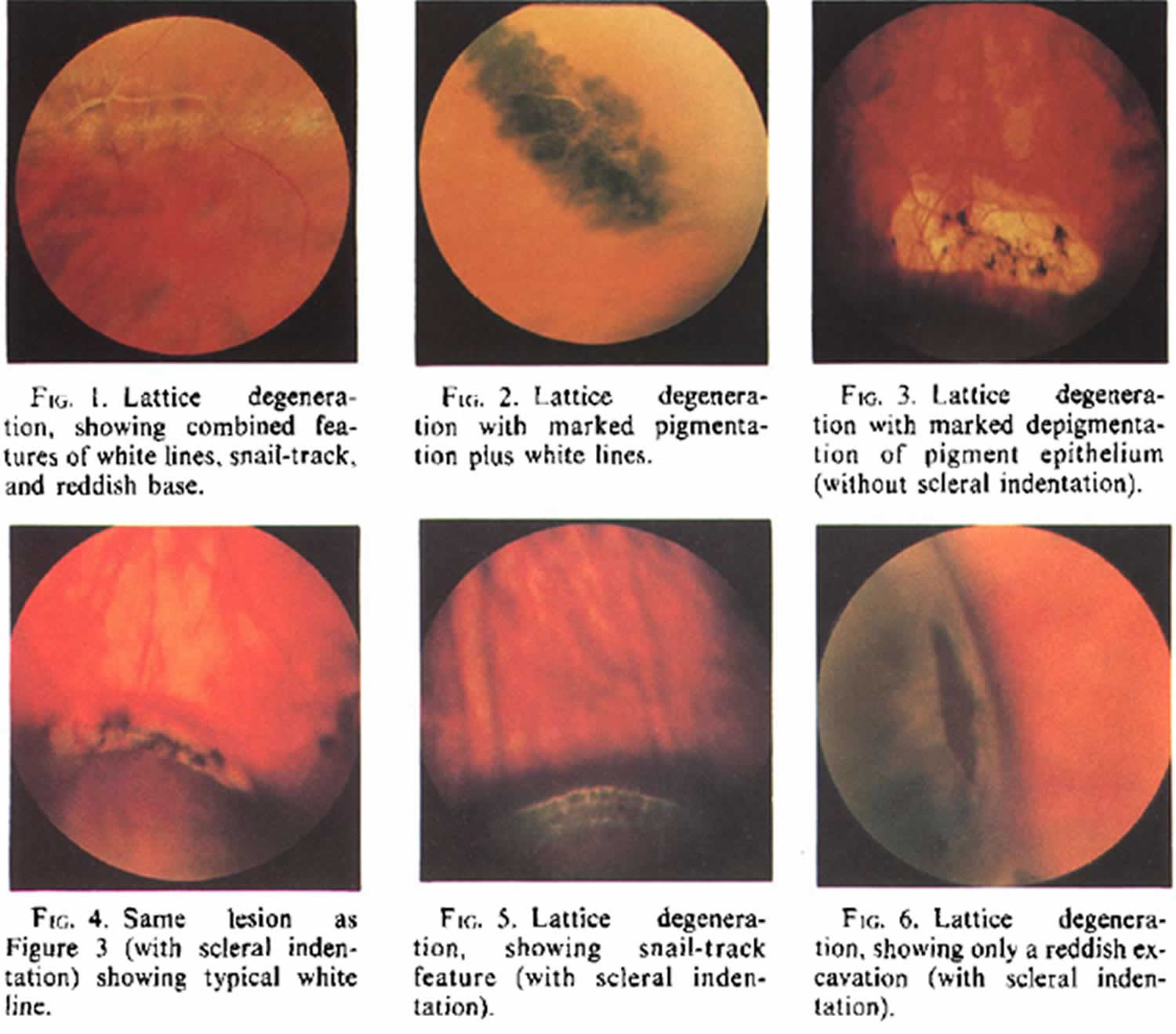
The observation of lesions in the peripheral retina suggestive of lattice degeneration must be carefully examined with scleral indentation and indirect ophthalmoscopy. The borders of lattice lesions will have an abrupt, discrete edge adjacent to otherwise normal retina. Examples of various lattice lesions are shown below 9.
Lattice degeneration though commonly encountered, can vary in its appearance. Though most cases can be observed without intervention, some present a real risk of retinal detachment. These cases require laser photocoagtulation or cryotherapy to seal off the affected areas.
Figure 1. Lattice degeneration
Is lattice degeneration serious?
No, however lattice degeneration is a risk factor for retinal tears and retinal detachment, but the vast majority of people with lattice degeneration never have a problem. The chances of a retinal detachment developing in an eye with lattice degeneration were less than 1% over an average of 11 years if retinal detachment had not occurred in the other eye 10. In people with lattice degeneration in both eyes and a history of detachment in the first eye, the incidence of retinal detachment in the second eye over seven years was between 2% to 5% 11. Asymptomatic retinal breaks frequently are observed within the lesions of lattice degeneration. These are usually small atrophic holes; retinal detachments due to these breaks are usually slowly progressive and are most frequent in myopic eyes of patients less than 60 years of age 12.
Asymptomatic retinal breaks are present in approximately 6% of eyes in both clinical and autopsy studies 13. The chances of retinal detachment due to an asymptomatic retinal break in people in which a retinal detachment has not occurred in either eye were approximately 0.5% over a follow-up period averaging 11 years 10. If a retinal detachment has occurred in one eye of a person with an asymptomatic retinal break in the second eye, the chances of retinal detachment in the latter eye appear to be higher, with incidence figures ranging from 0% to 15% 13. However, data regarding such cases are incomplete, and the relationship between the asymptomatic breaks, new retinal breaks, and retinal detachment remains unclear.
Treatment is indicated in symptomatic patients, positive family history of retinal detachment, retinal detachment in the fellow eye, trauma related retinal breaks, myopia and clinical progression of retinal detachment 2.
Lattice degeneration causes
Lattice degeneration is a common clinical entity which has many morphologies. Lattice degeneration is defined to have one or more of the following features organized in accordance to their presumed frequency of occurrence: localized round, oval or linear shaped retinal thinning; pigmentation; whitish-yellow surface flecks; round, oval or linear white patches; round, oval or linear red craters; small atrophic round holes; branching white lines; yellow atrophic spots (depigmentation of pigment epithelium); and rarely tractional tears at the ends or posterior margins of lesions 14. Usually one, but sometimes two or more of these features predominate in each individual lesion.
Post-mortem histology studies of lattice degeneration lesions have shown that there are three invariable findings in all types of lattice degeneration:
- Retinal thinning.
- Vitreous liquefaction overlying the thinned retina
- Vitreous condensation and exaggerated vitreo-retinal attachments at the borders of the lesion 15.
Electron microscopy of lesions shows thinning with fibrosis of blood vessels, loss of neurons, accumulation of glial material, pigment changes, and changes to the inner limiting lamina 15. It has also been shown that there is a lack of basement membrane over the surface of lattice degeneration lesions and replacement with astrocytes 16.
Lattice degeneration prevention
There are no preventative measures to the development of lattice degeneration.
Lattice degeneration symptoms
While lattice degeneration lesions alone are not symptomatic in themselves, they do lend to a higher risk of retinal holes, tears, and detachments that may become symptomatic. This is thought to occur at the junction of normal retina and lesions where there is observed vitreous traction leading to eventual retinal tear or retinal detachment.
Asymptomatic retinal breaks frequently are observed within the lesions of lattice degeneration. These are usually small atrophic holes; retinal detachments due to these breaks are usually slowly progressive and are most frequent in myopic eyes of patients less than 60 years of age 12.
Lattice degeneration signs
Lattice degeneration in itself is asymptomatic but may be associated with retinal tears, retinal detachments, or retinal traction that may present with photopsias, floaters, or visual disturbances.
Lattice degeneration diagnosis
This is a clinical diagnosis based on history and clinical exam, including slit lamp and dilated fundus examination with sclera depression.
Patients with lattice degeneration generally are asymptomatic. They may present for other ocular findings causing their symptoms such as a tear or detachment where there is found to be lattice degeneration. It is approximated that there is an overall incidence of lattice degeneration in 10% of the general population and the long term chance of retinal detachment in this population to be 0.5%1 On the other hand, one-third of patients with retinal detachments, without compounding factors such as surgery or other conditions, have been reported to have lattice degeneration 17. Therefore, it is recommended to be considerate of patients with lattice degeneration and other risk factor for detachment such as surgery or high myopia.
Physical examination
A full ophthalmic exam is necessary for the purposes of identifying lattice degeneration lesions and differentiating them from holes, tears, or other pathologic findings.
Clinical diagnosis
Lattice is diagnosed with a dilated direct and indirect ophthalmic exam with the use of sclera depression.
Diagnostic procedures
Lattice degeneration is most often found on routine ophthalmic exam and delineated from other peripheral lesions with scleral depression.
Laboratory test
No laboratory tests are indicated.
Lattice degeneration treatment
There is no mandatory treatment for lattice degeneration alone. While lattice degeneration is associated with retinal holes, tears and detachments, it is not advocated to treat lattice degeneration lesions on a solely prophylactic basis.
When lattice degeneration lesions are associated with retinal holes, tears or detachments, then the treatment of those conditions may dictate the course of action for lattice degeneration lesions 18. Laser photocoagtulation is the preferred treatment for lattice degeneration lesions at risk for retinal tears/detachment. Based on the risk for future retinal tears or detachments, eye doctors may decide to treat with other modalities such as cryotherapy or scleral buckling depending on their assessment of retinal detachment risk.
Lattice degeneration prognosis
The prognosis for lattice degeneration in itself is good. The vast majority of patients will have lattice degeneration lesions that are completely stable or slowly progressive. Patients who develop to retinal tears, detachments, and subsequent vitreo-retinal traction should be treated as those conditions arise. Eyes with lattice degeneration (with or without holes) are at very low risk for retinal detachment overall. Eyes which develop a posterior vitreous detachment and a horsehoe tear are at risk for retinal detachment and those eyes require laser photocoagulation or cyrotherapy to the horseshoe tear 19.
- Byer NE. Rethinking prophylactic therapy of retinal detachment. In: Stirpe M, editor. Advances in Vitreoretinal Surgery. Ophthalmic Communications Society; New York: 1992. pp. 399–411.[↩]
- Wilkinson CP. Interventions for asymptomatic retinal breaks and lattice degeneration for preventing retinal detachment. Cochrane Database Syst Rev. 2014;9:CD003170[↩][↩]
- Straatsma BR, Zeegen PD, Foos RY, Feman SS, Shabo AL. XXX Edward Jackson Memorial Lecture. Lattice degeneration of the retina. Trans Am Acad Ophthalmol Otolaryngol. 1974;78(2):OP87–113.[↩]
- Byer NE. Long-term natural history of lattice degeneration of the retina. Ophthalmology. 1989;96(9):1396-1401-02[↩]
- Folk JC, Arrindell EL, Klugman MR. The fellow eye of patients with phakic lattice retinal detachment. Ophthalmology. 1989;96(1):72–79.[↩]
- Mathew DJ, Sarma SK, Basaiawmoit JV. An Unusual Case of Extensive Lattice Degeneration and Retinal Detachment. J Clin Diagn Res. 2016;10(7):ND01–ND2. doi:10.7860/JCDR/2016/20312.8096 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5020263[↩][↩]
- Byer NE. Lattice degeneration of the retina. Surv Ophthalmol. 1979;23(4):213–48.[↩][↩]
- Jones W. In: Peripheral Ocular Fundus. 3rd ed. Missouri: Butterworth-Heinemann, Elsevier; 2007. Lattice degeneration; pp. 88–99[↩]
- Byer NE. Lattice degeneration of the retina. Surv Ophthalmol. Jan-Feb 1979;23(4):213-48.[↩]
- Long-term natural history of lattice degeneration of the retina. Byer NE. Ophthalmology. 1989 Sep; 96(9):1396-401; discussion 1401-2. https://www.ncbi.nlm.nih.gov/pubmed/2780007[↩][↩]
- The fellow eye of patients with phakic lattice retinal detachment. Folk JC, Arrindell EL, Klugman MR. Ophthalmology. 1989 Jan; 96(1):72-9. https://www.ncbi.nlm.nih.gov/pubmed/2919051[↩]
- Wilkinson CP. Interventions for asymptomatic retinal breaks and lattice degeneration for preventing retinal detachment. Cochrane Database Syst Rev. 2014;9(9):CD003170. Published 2014 Sep 5. doi:10.1002/14651858.CD003170.pub4 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4423540[↩][↩]
- Wilkinson CP, Rice TA. Michels Retinal Detachment. Mosby-Year Book; St Louis: 1997[↩][↩]
- Lattice degeneration. https://eyewiki.org/Lattice_Degeneration[↩]
- Straatsma BR, Zeegen PD, Foos RY, et al: Lattice degeneration of the retina. Trans Am Acad Ophthalmol Otolaryngol 78:87-113, 1974.[↩][↩]
- Streeten BW, Bert M: The retinal surface in lattice degeneration of the retina. Am J Ophthalmol 74:1201-1209, 1972.[↩]
- Burton TC: The influence of refractive erro and lattice degeneration on the incidence of retinal detachment. Trans Am Ophthalmol Soc. 87: 143-157, 1989.[↩]
- Wilkinson, CP: Evidence-based analysis of prophylactic treatment of asymptomatic retinal breaks and lattice degeneration. Ophthalmology: 107: 12-15, 2000.[↩]
- Byer NE. Rethinking prophylactic therapy of retinal detachment. In: Stirpe M, ed. Advances in Vitreoretinal Surgery. New York, NY: Ophthalmic Communications Society; 1992:399-411.[↩]





{kind=link}