Contents
- Subarachnoid hemorrhage
- Subarachnoid hemorrhage causes
- Types of subarachnoid hemorrhage
- Subarachnoid hemorrhage pathophysiology
- Subarachnoid hemorrhage prevention
- Subarachnoid hemorrhage symptoms
- Subarachnoid hemorrhage complications
- Subarachnoid hemorrhage diagnosis
- Subarachnoid hemorrhage grades
- Subarachnoid hemorrhage treatment
- Subarachnoid hemorrhage prognosis
Subarachnoid hemorrhage
Subarachnoid hemorrhage (SAH) also called subarachnoid bleeding or subdural hemorrhage is a life-threatening condition defined as bleeding in the space between your brain and the surrounding membrane (between the arachnoid and pia mater called the arachnoid layer) that cover your brain called subarachnoid space 1, 2, 3, 4, 5. Subarachnoid hemorrhage (SAH) is an emergency and prompt medical attention is needed. The main symptom of subarachnoid hemorrhage (SAH) is a severe headache that starts suddenly often called thunderclap headache. Some people describe the headache as the worst headache they have ever felt, the “worst headache ever” and unlike any other type of headache pain. The headache may start after a popping or snapping feeling in the head. Along with having a headache, some people with subarachnoid hemorrhage (SAH) may experience:
- Nausea
- Vomiting
- Stiff neck
- Problems with vision
- Brief loss of consciousness
- Decreased consciousness and alertness
- Eye discomfort in bright light (photophobia)
- Mood and personality changes, including confusion and irritability
- Muscle aches (especially neck pain and shoulder pain)
- Numbness in part of the body
- Seizure
- Vision problems, including double vision, blind spots, or temporary vision loss in one eye
Other symptoms that may occur with subarachnoid hemorrhage (SAH) include:
- Eyelid drooping
- Pupil size difference
- Sudden stiffening of back and neck, with arching of the back (opisthotonos; not very common)
In subarachnoid hemorrhage (SAH) the bleeding usually happens when an irregular bulge in a blood vessel (aneurysm) bursts in the brain also known as ruptured brain aneurysm or aneurysmal subarachnoid hemorrhage (aSAH) 6, 7. Sometimes, subarachnoid hemorrhage (SAH) is caused by trauma (traumatic brain injury), a tangle of blood vessels in the brain (arteriovenous malformation), or other blood vessel or health problems.
The incidence of subarachnoid hemorrhage in the United States is between 10 to 15 out of 100,000 individuals per year 8, 9, 10.
Noncontrast head computed tomography (CT) scan is the mainstay of diagnosis of subarachnoid hemorrhage (SAH) 11. Cerebral angiography is then pursued to identify the cause of SAH. Both CT angiography (CTA) and magnetic resonance angiography (MRA) can identify aneurysms 3‐5 mm or larger with a high degree of sensitivity, but digital subtraction cerebral angiography remains the gold standard test to identify the cause of SAH 12. Lumbar puncture can be considered if there is a strong suspicion of SAH despite a normal head CT.
Untreated, a subarachnoid hemorrhage can lead to permanent brain damage or death. Go to the emergency room or call your local emergency number if you or someone you know has symptoms of a subarachnoid hemorrhage.
The goals of subarachnoid hemorrhage treatment are to:
- Save your life
- Repair the cause of bleeding
- Relieve symptoms
- Prevent complications such as permanent brain damage (stroke)
A patient presenting with aneurysmal subarachnoid hemorrhage (aSAH) is admitted to an intensive care unit (ICU) for hemodynamic and neurological monitoring, and commonly ventriculostomy placement for drainage of CSF and recording of intracranial pressure. This is followed by definitive treatment of the ruptured aneurysm or pathology causing the SAH 11.
Treatment options for subarachnoid hemorrhage include surgery (including an endovascular procedure like an angiogram) to stop the bleeding from a ruptured aneurysm or arteriovenous malformation and medications to control pain and prevent vasospasm (clamping down of the brain blood vessels). Unfortunately, only up to a third of patients survive without neurological deficits.
Figure 1. Subarachnoid space anatomy
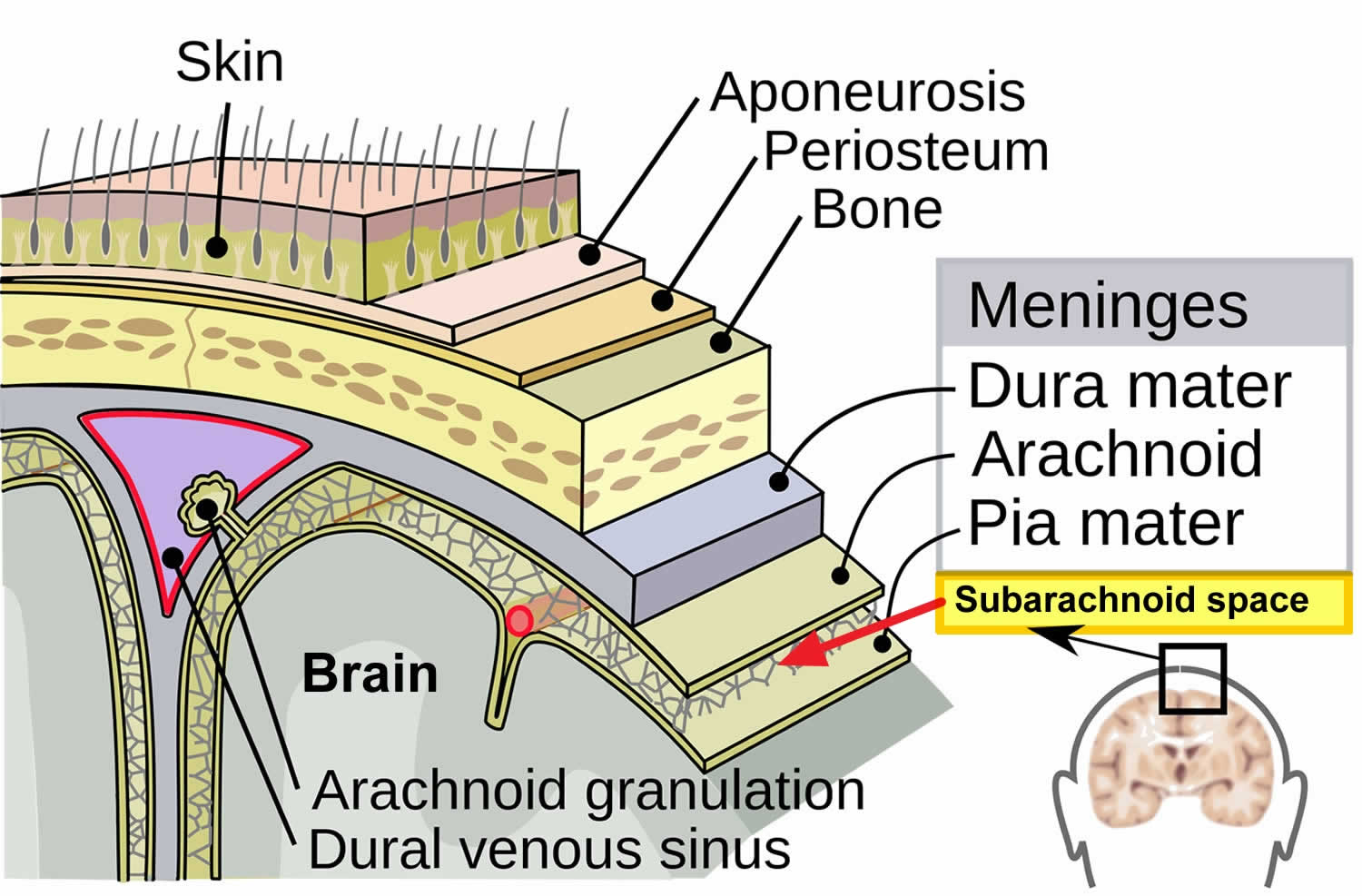 Figure 2. Subarachnoid hemorrhage
Figure 2. Subarachnoid hemorrhage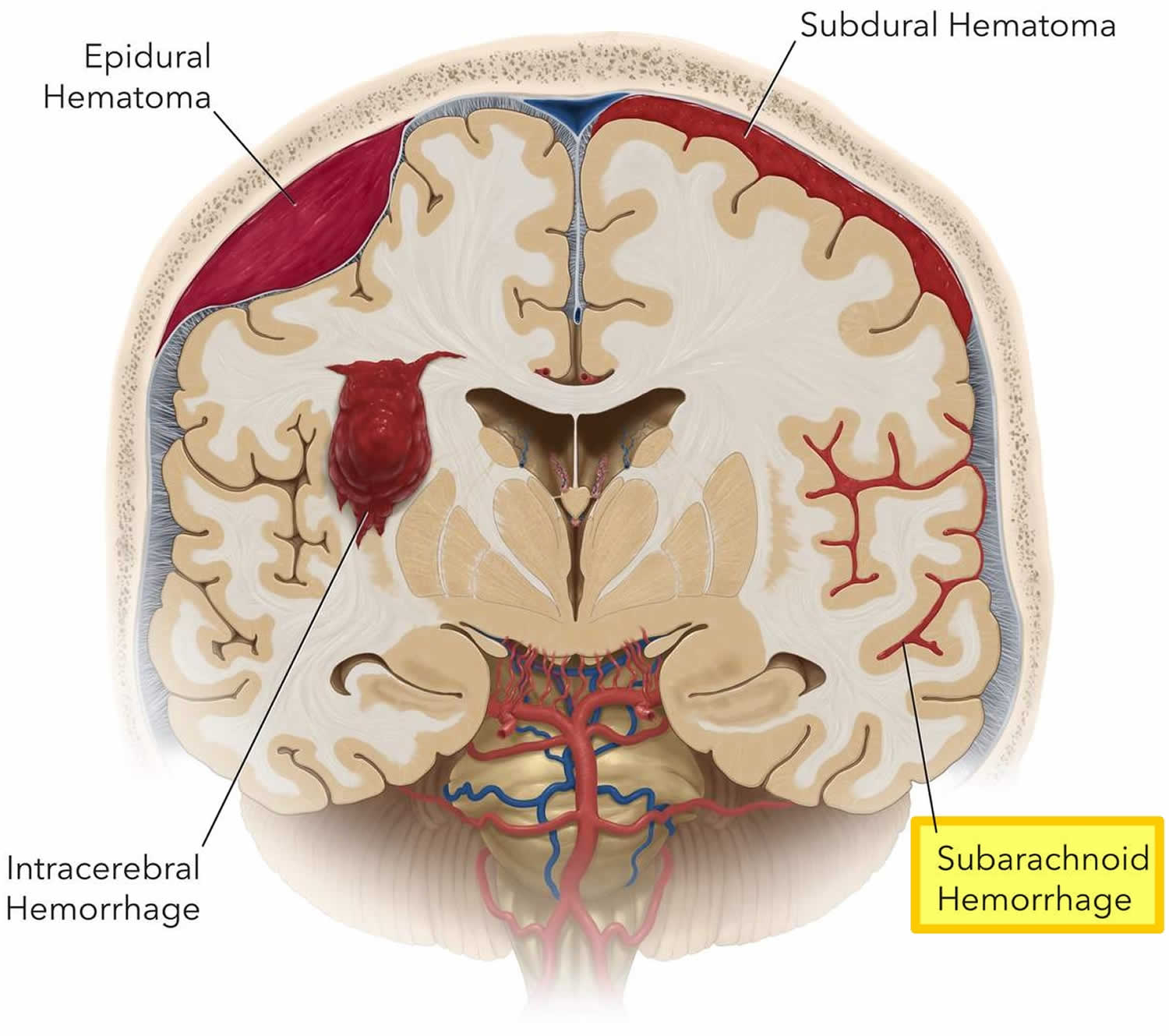
Figure 3. Subarachnoid hemorrhage CT
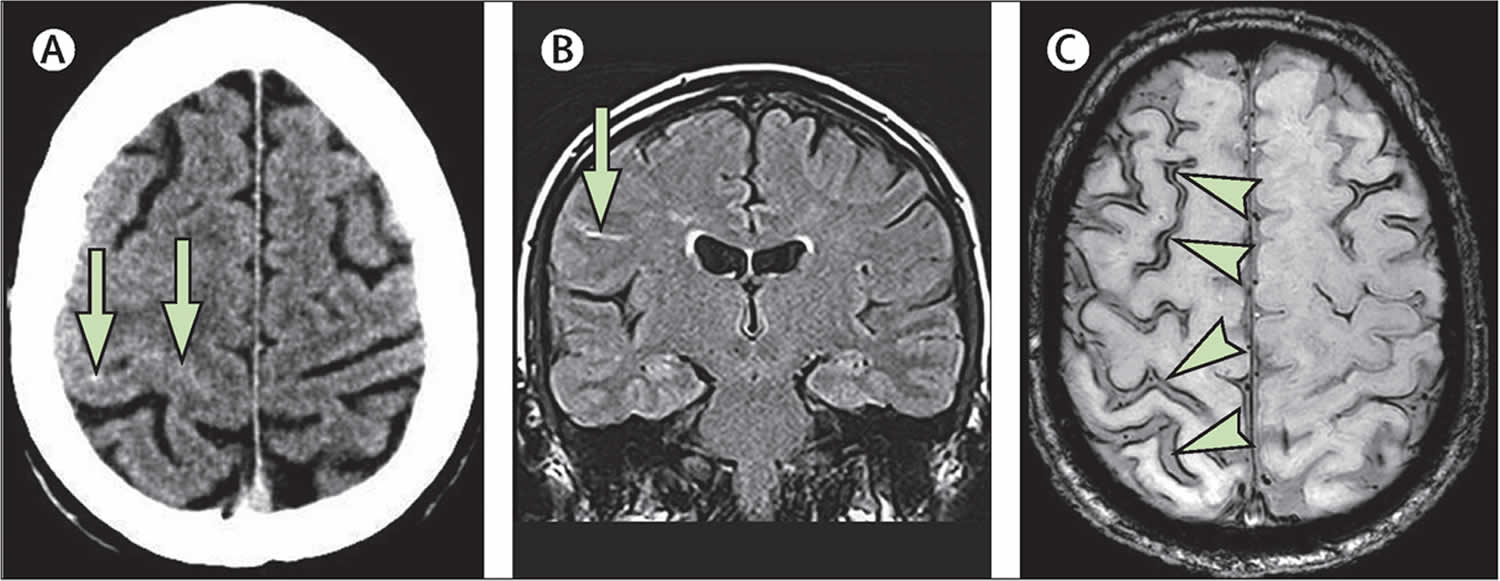
Footnotes: (A) Acute axial CT scan showing subtle high density due to acute bleeding in the right central sulcus (arrows). (B) Coronal FLAIR MRI showing high signal also consistent with acute blood in the sulcus (arrow). (C) Axial susceptibility-weighted MRI at follow-up showing multifocal cortical superficial siderosis (due to haemosiderin deposition from previous convexity subarachnoid haemorrhage appearing as serpiginous black lines adjacent to multiple sulci; arrowheads)
[Source 13 ]Subarachnoid hemorrhage causes
Subarachnoid hemorrhage (SAH) can be caused by:
- Bleeding from a cerebral aneurysm (weak area in the wall of a blood vessel that causes the blood vessel to bulge or balloon out) in 85% 14. Subarachnoid hemorrhageaccounts is most commonly caused by a ruptured aneurysm 15
- Perimesencephalic subarachnoid hemorrhage (PMSAH) is a distinct pattern of non-aneurysmal subarachnoid hemorrhage (SAH) centered on the basal cisterns around the midbrain with an excellent prognosis 16. 95% of cases of perimesencephalic subarachnoid hemorrhage (PMSAH) have a normal cerebral angiogram and the source of bleeding is not identified; the cause is thought to be a venous bleed 17.
- Bleeding from a tangle of blood vessels called an arteriovenous malformation (AVM). Brain arteriovenous malformations (BAVMs) also called cerebral arteriovenous malformations (CAVMs) are a type of intracranial high-flow vascular malformation composed of enlarged feeding arteries, a nidus of vessels closely associated with the brain parenchyma through which arteriovenous shunting occurs, and draining veins 18.
- Cerebral amyloid angiopathy
- Ruptured mycotic aneurysm
- Reversible cerebral vasoconstriction syndrome
- Dural arteriovenous fistula
- Spinal arteriovenous malformation
- Venous infarction 14
- Intradural arterial dissection
- Pituitary apoplexy
- Sympathomimetic drugs (e.g. cocaine)
- Cerebral vasculitis 19
- Bleeding disorder
- Head injury (traumatic brain injury)
- Unknown cause (idiopathic)
- Use of blood thinners (anticoagulation therapy)
Subarachnoid hemorrhage caused by head injury (traumatic brain injury) in older people is often due to falls. Among the young, the most common injury leading to subarachnoid hemorrhage is motor vehicle crashes. When caused by trauma, subarachnoid hemorrhage commonly occurs with other types of bleeding in the head.
Risk factors for developing subarachnoid hemorrhage
Risks for developing subarachnoid hemorrhage include 20:
- Unruptured aneurysm in the brain and other blood vessels
- Fibromuscular dysplasia and other connective tissue and autoimmune disorders
- Ehlers-Danlos disease type 4
- Marfan syndrome
- Neurofibromatosis type 1
- High blood pressure (hypertension)
- History of polycystic kidney disease (autosomal dominant polycystic kidney disease)
- Smoking. Smoking by itself (without the presence of other risk factors) almost doubles a person’s risk for ischemic stroke. Smoking promotes atherosclerosis and aneurysm formation and stimulates blood clotting factors. The risk for stroke decreases significantly two years after a person quits smoking; by five years, the risk decreases even further to the level of nonsmokers. Smoking also increases the risk of rupture and subarachnoid hemorrhage in people with cerebral aneurysms.
- Heavy alcohol consumption
- Use of illicit drugs such as cocaine and methamphetamine
- Use of blood thinners such as warfarin
- A strong family history of aneurysms may also increase your risk
- Female gender: ~1.5x baseline risk 21
- African descent: ~2x baseline risk
- Japanese or Finnish descent 22.
Types of subarachnoid hemorrhage
Aneurysmal subarachnoid hemorrhage (aSAH)
An aneurysmal cause of subarachnoid hemorrhage (SAH) has similar risk factors associated with aneurysm formation. High blood pressure (hypertension), cigarette smoking, and family history are the most consistently observed risk factors. Other factors include alcohol, sympathomimetic drugs, and estrogen deficiency. Older age (>60 years), posterior circulation location, atherosclerosis, hypertension, and large intra-arterial aneurysm size (greater than 5 mm) are contributing factors for an intra-arterial aneurysm to rupture. A family history of intra-arterial aneurysm or subarachnoid hemorrhage (SAH), previous history of SAH, or the presence of autosomal dominant polycystic kidney disease increases the risk of intra-arterial aneurysm rupture 23.
Aneurysms are divided according to their morphology into:
- Saccular aneurysms that are pouch-like protrusions of the vessel wall, usually arising in cerebral artery bifurcations (A);
- Fusiform aneurysms that are dilatations of the vessel wall that do not lead to the formation of a separate saccular pouch (B); and
- Dolichoectasias are elongated, tortuous, and sometimes dilated vessel segments (C).
Furthermore, a rare fourth type of cerebral artery aneurysm is the dissecting aneurysm that usually has a fusiform shape (B), but originates from acute dissection or tearing of the arterial wall layers.
Nonaneurysmal subarachnoid hemorrhage (NASAH)
- Perimesencephalic nonaneurysmal subarachnoid hemorrhage (PMSAH) is characterized by a specific pattern of localized blood on CT, normal cerebral angiography, and a benign course of illness 24. Perimesencephalic nonaneurysmal subarachnoid hemorrhage (PMSAH) subtype makes up the majority, up to two-thirds, of patients with nonaneurysmal subarachnoid hemorrhage (NASAH) 25. The CT findings typically include blood isolated to the perimesencephalic cisterns anterior to the brainstem 26.
- Occult aneurysm: A small percentage of cases are not diagnosed in initial angiographic studies but may be identified on repeat angiography and are classified under this group 27. The reasons are technical or reading errors, small aneurysm size, and obscuration of aneurysm because of vasospasm, hematoma, or thrombosis within the aneurysm 28.
- Vascular malformations: These can be intracranial or spinal in location. Most brain vascular malformations that cause SAH are either arteriovenous malformations (AVM) or dural arteriovenous fistulae 29, 30. They are usually visualized on cerebral angiography. Dural arteriovenous fistulae are the most common type of spinal vascular malformation 31. Vascular malformation associated with bleeding is usually managed surgically and or with endovascular interventions.
- Intracranial arterial dissection: Dissection of an intracranial artery can produce SAH. When the dissection of the intracranial artery extends through the adventitia, SAH occurs 32. In these situations, the bleeding is massive and often devastating. Dissection of an intracranial artery is diagnosed by conventional angiography and treated surgically or with endovascular interventions 32, 33.
- Other causes: Cocaine abuse is associated with aneurysmal and nonaneurysmal SAH 29, 34. Cerebral amyloid angiopathy can cause SAH in older adults 35. Cerebral venous thrombosis, sickle cell disorders, moyamoya disease, cerebral vasculitis, and bleeding disorders are some of the conditions that cause SAH 36, 37, 38.
Subarachnoid hemorrhage pathophysiology
Saccular aneurysms account for most cases of subarachnoid hemorrhage (SAH) 39. These intracranial aneurysms are thin-walled protrusions from an intracranial artery with a thin (or absent) tunica media and an absent internal elastic lamina 39. Persistent hemodynamic stress is the initiating factor for intracranial aneurysm formation and resulting in excessive wear on the wall of these arteries causing turbulent blood flow within the vessel, leading to structural fatigue and aneurysm development 40, 41, 39. Hypertension, cigarette smoking, and various connective tissue diseases can also contribute to arterial wall breakdown 42. The typical locations include the bifurcation of the basilar artery at the junction of the ipsilateral posterior inferior cerebellar artery (PICA), vertebral artery, and the anterior communicating artery 43. Large unruptured aneurysms compress the adjacent cerebral tissue causing neurological signs. However, the rupture of these lesions creates a state of reduced blood flow and vasospasm leading to cerebral ischemia. The pathophysiological mechanisms by which these lesions are formed and eventually rupture are not fully understood. The hemodynamic stress to the vessel wall caused by increased blood pressure and other risk factors promotes the formation and rupture of intracranial aneurysm 41. Multiple studies point to inflammation as a dominant factor in the pathogenesis of intracranial aneurysm 44. A hemodynamic insult initiates the inflammatory process. It leads to matrix metalloproteinases (MMPs)–mediated degradation of the extracellular matrix and apoptosis of smooth muscle cells, which are the predominant matrix-synthesizing cells of the vascular wall. These processes significantly weaken the arterial wall, resulting in dilatation, aneurysm formation, and ultimately rupture. The two main constituents of the inflammatory response and the associated degenerative response are macrophages and smooth muscle cells 44.
Fusiform aneurysms are caused by dilation of the entire circumference of the vessel, often formed as a result of atherosclerosis 39. Mycotic (infected) aneurysms often result from emboli due to infective endocarditis 39. However, these aneurysms are less likely to rupture than a saccular aneurysm.
Traumatic subarachnoid hemorrhage commonly occurs near the site of a skull fracture and intracerebral contusion. Radiologic clues of a traumatic origin include localized bleeding in a superficial sulcus, an adjacent skull fracture, and a cerebral contusion with external evidence of traumatic injury 45.
Subarachnoid hemorrhage prevention
The following measures may help prevent subarachnoid hemorrhage:
- Stopping smoking
- Treating high blood pressure
- Identifying and successfully treating an aneurysm
- Not using illicit drugs
Subarachnoid hemorrhage symptoms
The main symptom of subarachnoid hemorrhage (SAH) is a severe headache that starts suddenly often called thunderclap headache. Some people describe the headache as the worst headache they have ever felt, the “worst headache ever” and unlike any other type of headache pain. The headache may start after a popping or snapping feeling in the head. Along with having a headache, some people with subarachnoid hemorrhage (SAH) may experience 46:
- Nausea
- Vomiting
- Stiff neck
- Problems with vision
- Brief loss of consciousness
- Decreased consciousness and alertness
- Eye discomfort in bright light (photophobia)
- Mood and personality changes, including confusion and irritability
- Muscle aches (especially neck pain and shoulder pain)
- Numbness in part of the body
- Seizure
- Vision problems, including double vision, blind spots, or temporary vision loss in one eye
Other symptoms that may occur with subarachnoid hemorrhage (SAH) include:
- Eyelid drooping
- Pupil size difference
- Sudden stiffening of back and neck, with arching of the back (opisthotonos; not very common)
Subarachnoid hemorrhage signs include:
- A physical exam may show a stiff neck.
- A brain and nervous system exam may show signs of decreased nerve and brain function (focal neurologic deficit).
- An eye exam may show decreased eye movements which may indicate damage to the cranial nerves (in milder cases, an eye exam may show no problems).
Subarachnoid hemorrhage complications
Repeated bleeding is the most serious complication of subarachnoid hemorrhage. If a cerebral aneurysm bleeds for a second time, the outlook is much worse.
Changes in consciousness and alertness due to a subarachnoid hemorrhage may become worse and lead to coma or death.
Other complications include:
- Seizures
- Stroke
- Vasospasm
- Rebleed
- Hydrocephalus
- Increased intracranial pressure
- Brain herniation
- Cerebral infarction
- Medical complications
- Medicine side effects
- Neurogenic pulmonary edema 47
- Complications of surgery
- Death
Delayed cerebral ischemia (DCI) is a frequent complication of subarachnoid hemorrhage (SAH). Delayed cerebral ischemia (DCI) contributes substantially to the morbidity and mortality following subarachnoid hemorrhage (SAH). Delayed cerebral ischemia (DCI) is defined as symptomatic vasospasm related to subarachnoid hemorrhage or cerebral infarction demonstrated on imaging felt to be attributable to vasospasm 48. Delayed cerebral ischemia (DCI) presents clinically as new focal neurological deficits or altered consciousness felt to be attributable to ischemia in the setting of vasospasm 48, 49.
Early brain injury is increasingly considered a critical factor in the development of delayed cerebral ischemia (DCI) and prediction of unfavorable outcomes 50, 51. Early brain injury include acute cerebral ischemia, energy dysfunction following cortical spreading depolarizations, mitochondrial dysfunction 51, 52. In recent decades, vasospasm has been considered the primary culprit of delayed cerebral ischemia 53. However, delayed cerebral ischemia is now attributed to cerebral vasospasm, micro thombosis, and cortical spreading depolarization 54. Moreover, delayed cerebral ischemia was the result of these independent courses acting in concert 55. Delayed cerebral ischemia can occur in 30% of SAH patients. The current standard prophylactic intervention for delayed cerebral ischemia is limited to oral nimodipine and maintaining normal blood volume and normal circulating volume 56.
Subarachnoid hemorrhage diagnosis
If your doctor thinks you have a subarachnoid hemorrhage, a head CT scan (without contrast dye) will be done right away. In some cases, the scan is normal, especially if there has only been a small bleed. If the CT scan is normal, a lumbar puncture (spinal tap) may be done. Additional CT scans may be needed for further confirmation.
To diagnose a subarachnoid hemorrhage, your doctor is likely to recommend:
- CT scan. This imaging test can detect bleeding in the brain. While a CT scan is a highly effective test when performed properly, the scan may not find the bleed if you have a low red blood cell count (anemia) and only a small amount of blood is lost during the bleed. Your doctor may inject a contrast dye to view your blood vessels in greater detail (CT angiogram).
- Magnetic resonance imaging (MRI). This imaging test also can detect bleeding in the brain. Your doctor might inject a dye into a blood vessel to view the arteries and veins in greater detail (MR angiogram) and to highlight blood flow. This may show signs of a subarachnoid hemorrhage in rare cases when the signs don’t show on a CT scan.
- Cerebral angiography. You doctor inserts a long, thin tube (catheter) into an artery and threads it to your brain. Dye is injected into the blood vessels of your brain to make them visible under X-ray imaging. Your doctor might recommend cerebral angiography to get more-detailed images. They may also recommend the test if a subarachnoid hemorrhage is suspected, but the cause isn’t clear or doesn’t appear on other imaging. You might need a second cerebral angiogram if the first one did not show an aneurysm, but your doctor thinks an aneurysm is likely.
- Transcranial Doppler ultrasound, to look at blood flow in the arteries of the brain
In some cases of aneurysmal subarachnoid hemorrhages, the bleeding may not appear on initial imaging. If your first CT scan doesn’t show bleeding, your doctor might recommend lumbar puncture. A needle is inserted into the lower back to withdraw a small amount of the fluid that surrounds the brain and spinal cord (cerebrospinal fluid). The fluid is studied to look for blood, which may mean that you have a subarachnoid hemorrhage.
Subarachnoid hemorrhage grades
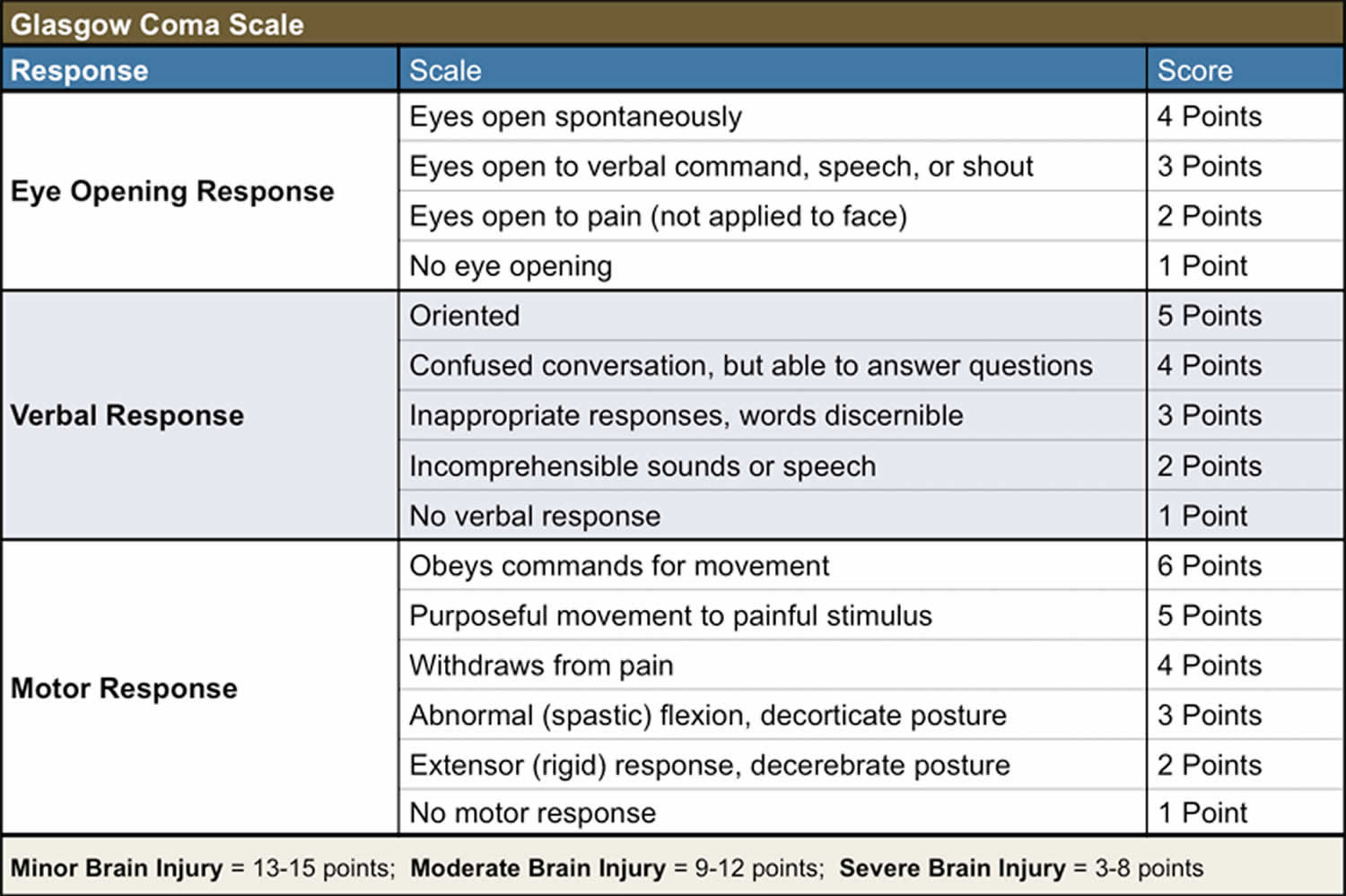
Several grading scales are used in clinical practice to standardize the classification of patients with aneurysmal subarachnoid hemorrhage (aSAH) and to monitor progression and change in condition. These scales are based on the initial clinical neurological examination and the appearance of blood on the initial head CT. These scales include the Glasgow Coma Scale (GCS), the Hunt and Hess grading scale, the World Federation of Neurosurgical Societies (WFNS) scale, the Fisher grading scale, and the modified Fisher grading scale.
Figure 4. Subarachnoid hemorrhage grades
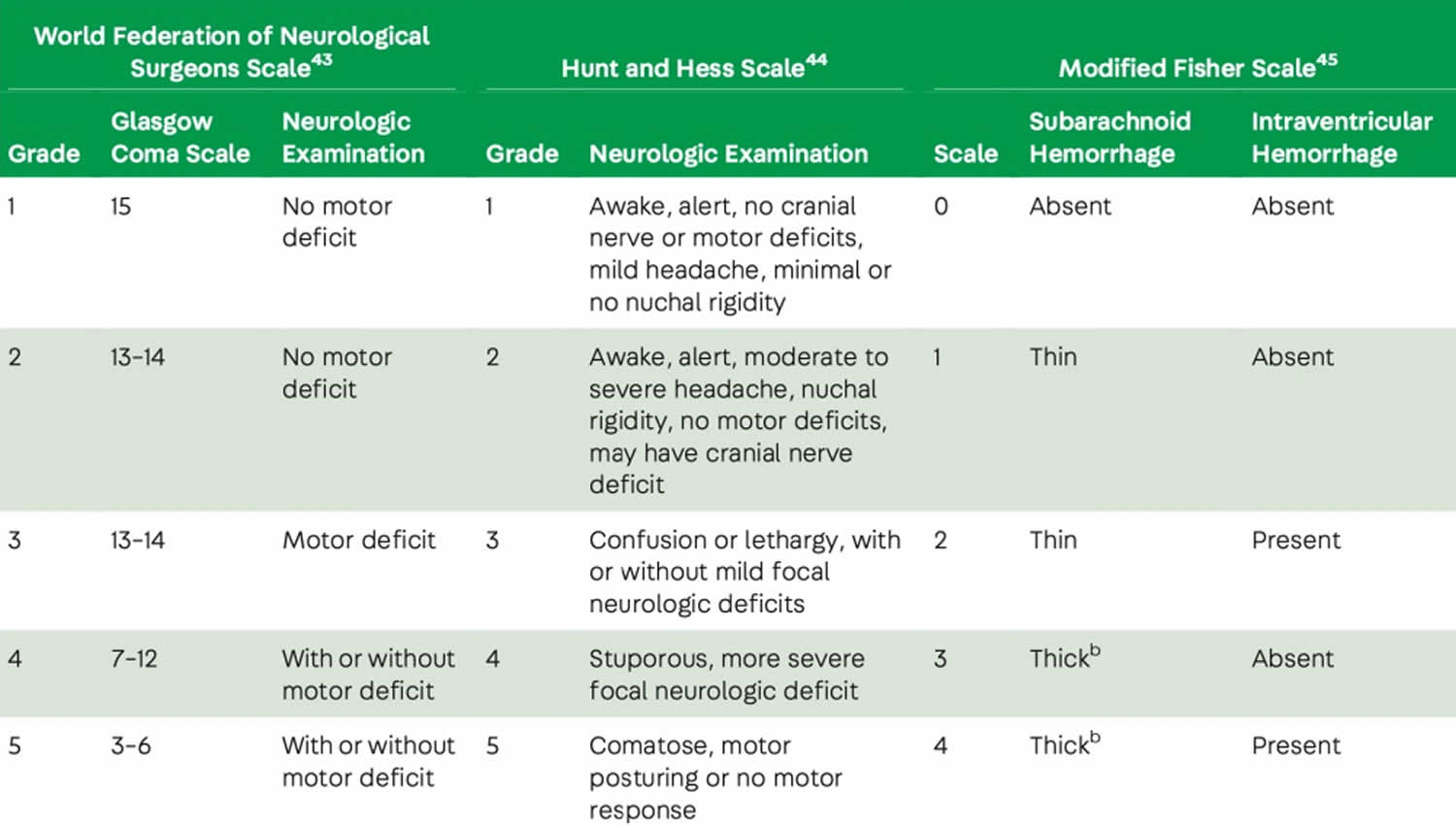
The Glasgow Coma Scale (GCS), introduced in 1974, is designed as a reliable and objective scale of neurological function in three subscales of level of consciousness, eye-opening, and motor function 57 The scale ranges from 3 to 15, and points are denoted based on the level of response. A higher score correlates to a better patient’s neurological condition. The GCS is commonly used for the initial and ongoing assessment of a patient with possible or confirmed brain injury. It is used to determine neurological deficits and their changes over time.
Figure 5. Glasgow Coma Scale (GCS)
The World Federation of Neurosurgical Societies (WFNS) developed the WFNS grading scale, which describes the clinical presentation of SAH patients. The scale includes consciousness and motor deficits in its scoring system. The World Federation of Neurosurgical Societies (WFNS) grading system uses a combination of consciousness and motor deficits from the GCS and the presence of focal neurological deficits to grade the severity of SAH 58. The WFNS scale helps predict recovery and response to treatment. For example, elderly patients with a WFNS grade of 1 to 3 have the best clinical recovery and seem to benefit from aggressive treatment compared to patients younger than 70 years with a WFNS score of 4 or 5.
Figure 6. World Federation of Neurosurgical Societies (WFNS) and Hunt and Hess grading scale

The Hunt and Hess grading scale, introduced in 1968, helps to classify the severity of aneurysmal subarachnoid hemorrhage (aSAH) based on the patient’s clinical condition. It is used as a predictor of a patient’s prognosis and outcome. A higher score (grade) correlates to a lower survival rate 59.
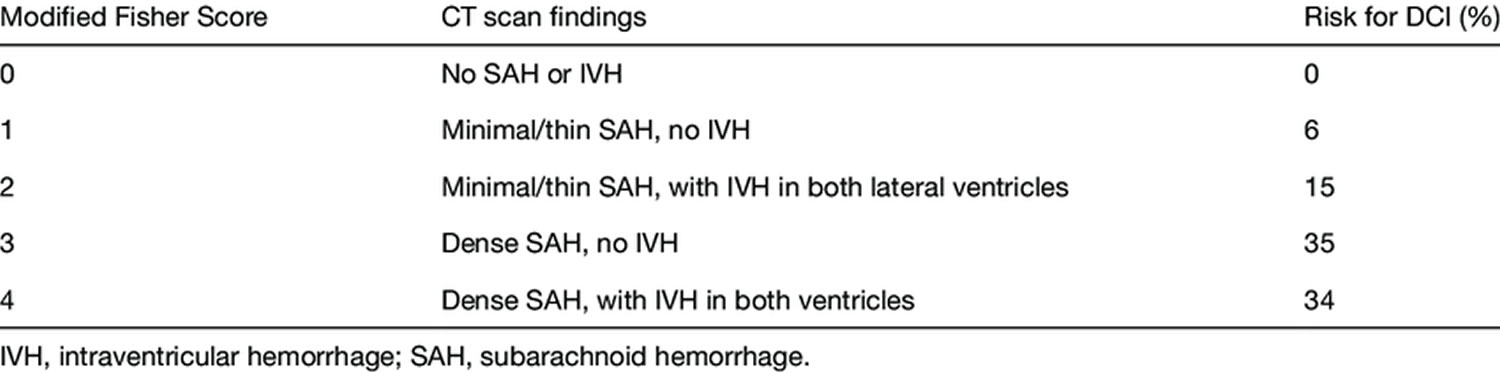
The Fisher grading scale is a numerical scale from 0 to 4 that provides insight into the amount of subarachnoid blood on a CT scan. These grading scales correlate to the hemorrhage’s severity, the intra-arterial aneurysm’s clinical grade, and the vasospasm’s incidence after the SAH. In comparison, the modified Fisher grading scale provides more specific descriptions of the amount and location of blood seen on a CT scan 60.
Figure 7. Fisher grading scale
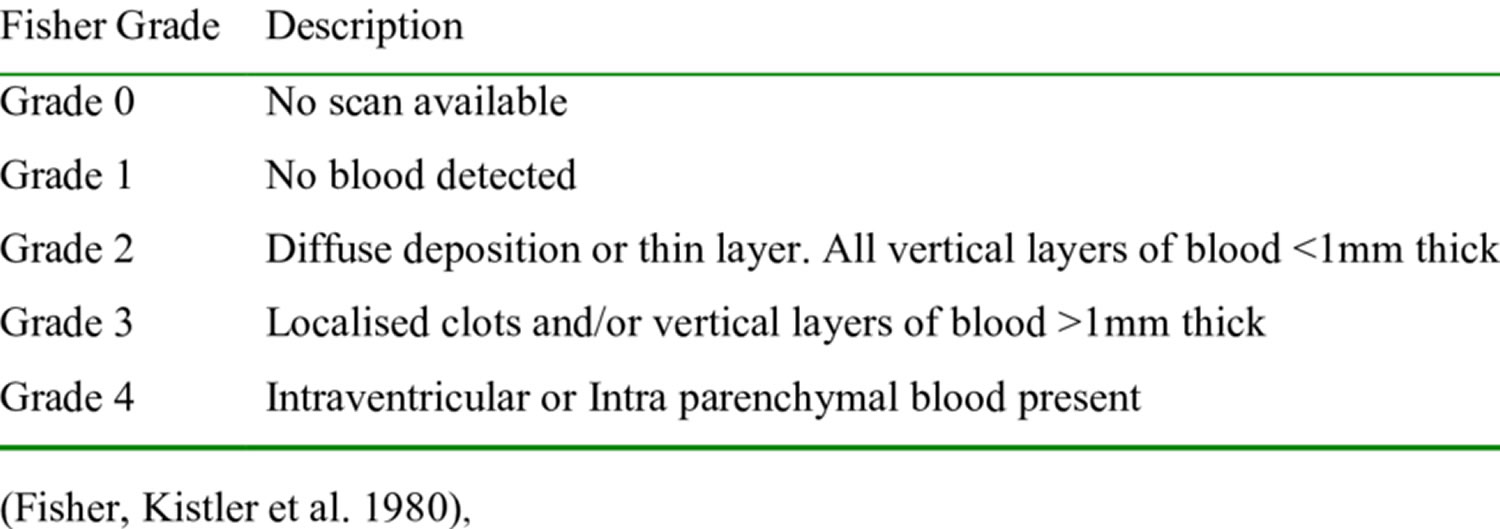
Figure 8. Modified Fisher grading scale
Subarachnoid hemorrhage treatment
Treatment focuses on stabilizing your condition, treating an aneurysm if you have one, and preventing complications.
Your doctor checks your breathing, blood pressure, and blood flow.
If your bleeding is caused by a ruptured brain aneurysm, your doctor might recommend:
Surgery.
- If your subarachnoid hemorrhage is due to an aneurysm rupture, your surgeon makes an incision in the scalp and locates the brain aneurysm. A metal clip is placed on the aneurysm to stop the blood flow to it.
- If your subarachnoid hemorrhage is due to head injury, surgery may be done to remove large collections of blood or relieve pressure on your brain
- If the person is critically ill, surgery may have to wait until the person is more stable.
Surgery may involve:
- Craniotomy (cutting a hole in the skull) and aneurysm clipping, to close the aneurysm
- Endovascular coiling: The surgeon inserts a catheter into an artery and threads it to your brain. Detachable platinum coils are guided through the catheter and placed in the aneurysm. The coils fill the aneurysm, reducing blood flow into the aneurysm sac and causing the blood to clot reducing the risk of further bleeding. Different types of coils have been developed to treat various aneurysms.
- Other endovascular treatments. Certain aneurysms can be treated with endovascular embolization that uses newer technology such as stent-assisted or balloon-assisted coiling or devices that divert blood flow.
If no aneurysm is found, the person should be closely watched by a health care team and may need more imaging tests.
Treatment for coma or decreased alertness includes:
- Draining tube placed in the brain to relieve pressure
- Life support
- Methods to protect the airway
- Special positioning
- Special medicines to decrease swelling in the skull
A person who is conscious may need to be on strict bed rest. The person will be told to avoid activities that can increase pressure inside the head, including:
- Bending over
- Straining
- Suddenly changing position
Treatment may also include:
- Medicines given through an IV line to control blood pressure
- Medicine to prevent artery spasms
- Painkillers and anti-anxiety medicines to relieve headache
- Medicines to prevent or treat seizures
- Stool softeners or laxatives to prevent straining during bowel movements
- Medicines to prevent seizures
Preventing complications is important because you can bleed again, have poor blood flow to the brain, have low salts such as sodium in your blood, develop too much fluid on the brain, or have high or low blood sugar. One medication, nimodipine (Nymalize) has been shown to decrease circulation problems to the brain after a subarachnoid hemorrhage.
A common complication after an aneurysmal subarachnoid hemorrhage is delayed spasm of the blood vessels in the brain. This can cause stroke if it reduces the blood flow below a certain level. When this complication occurs, strokes may be avoided by raising the blood pressure with intravenous medications or increasing the width of the blood vessels in the brain with medications.
Another common complication is hydrocephalus which is an accumulation of fluid in brain spaces. This problem can be treated with drains inserted in the head (ventriculostomy catheter) or in the lower back (lumbar drains).
Sometimes, procedures need to be repeated. You’ll have regular follow-up appointments with your doctor to watch for any changes. You may also need physical, occupational and speech therapy.
Surgical management
Once an aneurysmal subarachnoid hemorrhage (aSAH) or a ruptured aneurysm is identified, repair with surgical clipping or endovascular coiling is the only effective treatment and should be performed as early as feasible, preferably within 24 hours; some expert centers report a median time to aneurysm repair of 7 hours from admission 11. Patients in whom aneurysm treatment is not possible or must be delayed may be candidates for antifibrinolytic therapy, but these agents should not be used for more than 72 hours 61.
Monitoring
- Transcranial Doppler – Transcranial Doppler (TCD) sonography is used for detecting and monitoring vasospasm in SAH. A Transcranial Doppler (TCD) is able to detect changes in velocity prior to the clinical sequelae of vasospasm. However, it is an operator-dependent technology that has imperfect sensitivity and specificity 62, 11, 63, 64. In general, digital subtraction angiography is required to diagnose vasospasm and institute treatment.
- Imaging studies – In the acute phase of SAH, imaging studies like CT angiography (CTA) and CT perfusion (CTP) can detect arterial narrowing or perfusion asymmetry. These methods are sensitive and help in predicting delayed cerebral ischemia 65, 66. The use of this technique as a monitoring tool may be limited by risks of recurrent dye loads and radiation exposure 11. A finding of perfusion-diffusion mismatch on magnetic resonance imaging may be another method of detecting brain areas at risk of infarction in this setting 67. The clinical utility of either of these methods remains to be established.
- Electroencephalography (EEG) – Continuous EEG can be useful to detect subclinical seizures or nonconvulsive status epilepticus, particularly for patients with poor-grade SAH who develop unexplained neurologic deterioration or fail to improve 63.
- Frequency of neuro checks – Patients with acute SAH should be carefully examined every one to two hours, especially during the high-risk period for delayed cerebral ischemia 61. Symptomatic vasospasm and delayed cerebral ischemia are manifested clinically by neurologic decline, including the onset of focal neurologic abnormalities.
A development of neurologic deficits should be evaluated with an urgent head CT scan (to identify rebleeding, cerebral infarction, hydrocephalus), angiography (to identify symptomatic vasospasm), and/or EEG (to detect subclinical seizures). Medical complications can also contribute to a change in neurologic status.
Even in the absence of clinical change, it is important to identify cerebral vasospasm and decreased cerebral perfusion. Therefore, some centers monitor all patients with aneurysmal SAH with Transcranial Doppler (TCD) sonography daily and head CT, CTA, and CT perfusion on admission and between days 3 to 5 and days 7 to 10 to screen for evidence of decreased cerebral perfusion or vasospasm 61. Digital subtraction angiography can be used in place of CT angiography (CTA) or CT perfusion (CTP) in situations of high suspicion. Additional monitoring may be employed for high-risk patients with poor neurologic status, including EEG, and invasive monitoring of brain tissue oxygenation and cerebral blood flow 68.
- Intracranial pressure monitoring – It is recommended to perform a ventriculostomy in patients with enlarged ventricles on CT or with World Federation of Neurosurgical Societies (WFNS) scale score ≥3; this allows direct measurement of ICP and also allows treatment by drainage of cerebrospinal fluid (CSF) when appropriate 69.
Medical management
The significant concerns after an aneurysmal subarachnoid hemorrhage (aSAH) are rebleeding, hydrocephalus, and vasospasm. The most immediate problem is rebleeding. The most significant risk of rebleeding and mortality is within the first 6 hours of the initial hemorrhage 70. Commonly, patients risk rebleeding with elevated systolic blood pressure, poor Hunt-Hess grades, intracerebral or intraventricular hematomas, aneurysms > 10 mm in size, and aneurysms in the posterior circulation 70. About 9% to 17% of patients risk rebleeding in the first 72 hours. Rebleeding carries a mortality rate of up to 50%. Nearly 15% of patients rebleed in the first few hours after the initial hemorrhage; however, once the IA is secured, the risk of rebleeding is about 1% 71. Blood pressure control is a significant component in the prevention of rebleeding 71.
Blood Pressure Control
Blood pressure control is critical to reducing the risk of rebleeding until the intracranial aneurysm is secured and during the first 24 to 48 hours postoperative period 71. The sudden surge in central sympathetic stimulation associated with aneurysmal subarachnoid hemorrhage (aSAH) results in hypertension, and the generally accepted goal is to maintain the systolic blood pressure to less than 160 mm Hg 72. The risk of rebleeding is highest in the first 24 hours of the initial hemorrhage and carries a mortality rate up to 78%. Opioid pain medications may help to decrease the blood pressure and promote patient comfort; however, administering rapid-acting intravenous (IV) antihypertensive medications given as needed or via continuous infusion work to maintain the blood pressure within ordered parameters 71. Nitrates and nitroprusside have fallen out of favor as first-line agents for blood pressure control due to the potential for increased ICP and toxic side effects, particularly with prolonged nitroprusside infusions 73.
Labetalol and hydralazine are often the favored intermittent dosing medications, whereas nicardipine (Cardene) and clevidipine (Cleviprex) are continuous infusions used for blood pressure control 71. Labetalol is a beta-blocker that may be administered over 2 minutes in doses ranging from 5 to 20 mg IV every 15 minutes 74. Hydralazine is given in incremental IV doses of 20 to 40 mg every 30 to 60 minutes. The action of hydralazine is also vasodilation, but with a direct effect on arterioles to decrease systemic resistance and reduce blood pressure 74. The duration of action is more prolonged than labetalol and lasts 1 to 4 hours with a half-life of 2 to 8 hours. Contraindications include coronary artery disease (CAD). The precaution for stroke patients is to avoid a sudden drop in blood pressure related to antihypertensive medications, particularly in ischemic stroke, that may result in a hypoperfusion injury to the brain.
Nicardipine (Cardene) is given via continuous IV infusion in titrated doses from 5 to 15 mg/hr to maintain the systolic blood pressure of 150 to 160 mm Hg to prevent rebleeding. Some clinicians prefer to maintain a blood pressure of less than 140 mm Hg to prevent rebleeding 75.
Clevidipine (Cleviprex) is also a calcium channel blocker with a similar mechanism of action as nicardipine 76. The onset of action is about 2 to 4 minutes, with a half-life of about 15 minutes. Dosing and titration begin at 1 to 2 mg/hr and repeated every 90 seconds. Clevidipine is in a lipid base without preservatives.
Vasospasm Prevention and Treatment
The drug categories that prevent and treat vasospasm include calcium channel blockers, magnesium, endothelin antagonists, and statins. These categories are revieNimodipine following sections to describe their current use, if any, in vasospNimodipinement.
Calcium channel blockers
Calcium channel blockers reduce cardiac and smooth muscle contraction without an effect on skeletal muscle. The effectiveness of this classification of drugs in the management of aneurysmal subarachnoid hemorrhage (aSAH) has been a source of many studies over the years. Still, it is considered that calcium channel blockers mitigate the abnormal vasoconstriction of cerebral vascular smooth muscle. Oral administration of the dihydropyridine-type calcium channel blocker nimodipine is the only treatment with consistent, high-quality evidence for decreasing delayed cerebral ischemia (DCI) and is now standard of care in patients with aneurysmal subarachnoid hemorrhage (aSAH). However, these results are advocated by one large trial 77, 78. These early studies showed the role of oral Nimodipine in reducing delayed cerebral ischemia (DCI) and improving outcomes without affecting vasospasm 79. This suggests nimodipine may have an important vessel-independent effect not completely understood. A recent trial (NEWTON [Nimodipine microparticles to enhance recovery while reducing toxicity after subarachnoid hemorrhage] involving administration of intraventricular nimodipine showed no improvements over standard oral administration 80. Oral nimodipine is given in doses of 60 mg every 4 hours or 30 mg every 2 hours for 21 days. If hypotension is a recurring problem, the recommendation is to administer smaller, more frequent dosing 2.
Magnesium
The use of Magnesium sulfate has shown to have mixed results on neuroprotective and its vasodilatation properties—vasodilation results from an inhibition of Voltage-gated calcium channel-mediated smooth muscle contractions. Various spasmogenic agents such as endothelin-1, norepinephrine, angiotensin II, and serotonin are counteracted by magnesium. The Magnesium for Aneurysmal Subarachnoid Hemorrhage (MASH-2) trial was a phase 3, randomized, placebo-controlled trial 81. A total of 1,204 patients were enrolled. The study concluded with no improvement in outcomes in the intervention group 81. Additionally, an updated Cochrane meta-analysis of seven prior randomized trials from MASH-2 and those randomized trials that were eligible for inclusion since the MASH-2 trial involved 2,047 patients demonstrated that magnesium was not superior to a placebo in reducing poor outcomes after aneurysmal subarachnoid hemorrhage (aSAH). Therefore, magnesium cannot be recommended for routine administration in aneurysmal subarachnoid hemorrhage (aSAH) 82.
Endothelin Antagonists
Endothelin antagonists (ET-A) are another potential treatment under investigation. Endothelin antagonist (ET-A) receptors mediate vasoconstriction in arterial smooth muscle. Clazosentan is a selective ET-A receptor antagonist that demonstrated a decrease and a reversal in vasospasm after SAH. One study, CONSCIOUS-1 (Clazosentan to Overcome Neurological Ischemia and Infarct Occurring after Subarachnoid Hemorrhage), found a significant dose-dependent effect on vasospasm when evaluated with angiography 83. The 413 patients in this study were randomized and given placebo or clazosentan within 56 hours and continued on their assigned protocol for up to 14 days 83. Subsequent studies with clazosentan have reported no benefit with this drug.
Statins
Research with statin drugs have also demonstrated a lack of efficacy and have shown no benefit in the treatment of vasospasm and neither does it improve short term or long term outcomes in aneurysmal subarachnoid hemorrhage (aSAH) 84, 85; however, studies are ongoing. To date, the recommendations have been to continue the statin medication if the patient had been taking it prior to the onset of the SAH 86.
Anticoagulants
As per the 2015 guidelines from the Neurocritical Care Society and Society of Critical Care Medicine, it is recommended to discontinue all antithrombotic agents and reverse all anticoagulation until the aneurysm is definitively repaired by surgery or coiling 87. Patients presenting with aneurysmal subarachnoid hemorrhage (aSAH) on anticoagulant therapy have a worse prognosis and outcomes. Anticoagulants tend to increase the amount of bleeding at the time of rupture, thereby increasing the overall amount of blood in the subarachnoid space, basal cisterns, and the parenchyma 88. On the other hand, thrombotic complications related to venous thromboembolism (VTE) may be equally as lethal in patients with stroke. An accepted clinical practice is to initiate pharmacological prophylaxis therapy 24 to 48 hours after surgery with unfractionated or a low-molecular-weight heparin. Nurse-driven protocols often support venous thromboembolism prevention measures intermittent pneumatic compression devices on admission to the critical care unit. Additional measures may consist of early mobilization and prevention of dehydration. Stroke units that promote early mobilization have demonstrated lower rates of deep vein thrombosis (DVT) 89.
Pain Control
Pain management is an essential aspect of patient care. With complaints of the “worst headache of my life”, the interprofessional health care team needs to provide interventions to make the patient as comfortable as possible. Nonopioid medications such as acetaminophen (650 mg oral or 1,000 mg IV) are first line medications and be administered every 4 to 6 hours; however, consideration must be given to contraindications, that is, liver disease 90. Non-steroidal anti-inflammatory drugs (NSAIDs) like aspirin should be avoided until the aneurysm is secured 63. Opioid medications such as fentanyl (12.5 to 25 mg IV every hour as needed), Dilaudid (0.2 to 4 mg IV every 3 to 4 hours as needed), and morphine sulfate (2 to 4 mg IV every 1 to 2 hours as required) may provide pain relief as well as a degree of sedation and serve to decrease anxiety 2. Patients response to pain medications must be monitored closely to avoid oversedation and an inability to accurately assess the patients’ neurological status. Pain management is essential but with caution so that worsening in neurological status is not masked.
Rehabilitation
Rehabilitation is vital to subarachnoid hemorrhage or stroke recovery.
- Physical therapy is the main form of rehabilitation for most people with stroke. The aim of physical therapy is to help people relearn simple motor activities such as walking, sitting, standing, lying down, and the process of switching from one type of movement to another. To achieve this, physical therapists use training and exercises to restore movement, balance, and coordination. In one stroke rehabilitation study, researchers compared at home physical therapy to a locomotor training program using treadmill walking with body weight support followed by walking practice. The Locomotor Experience Applied Post-Stroke (LEAPS) trial found that people who had a stroke and had physical therapy at home improved their ability to walk just as well as those who were treated with the locomotor training program. Study investigators also found that patients continued to improve up to one year after stroke, defying conventional wisdom that recovery occurs early and largely ends at six months.
- Occupational therapy helps people relearn the skills needed to perform everyday activities such as eating, drinking and swallowing, dressing, bathing, cooking, reading and writing, and toileting. This type also involves exercise and training. Occupational therapists can recommend home or workplace modifications to better help the person resume living an independent or semi-independent lifestyle.
- Speech therapy helps people with stroke relearn language and speaking skills or learn other forms of communication. Speech therapy is appropriate for people who have no problems with cognition or thinking but have problems understanding speech or written words, or problems forming speech. Speech therapy also helps people develop coping skills to deal with the frustration of not being able to communicate fully. With time and patience, speech therapy can help a stroke survivor regain some, and sometimes all, language and speaking abilities.
- Vocational therapy helps people return to the workforce. Approximately one-fourth of all strokes occur in people between the ages of 45 and 65. For most people in this age group, returning to work is a major concern. It may involve relearning the more complex skills that were performed on the job or learning new skills for a different job. Vocational therapists can help people with lasting disabilities identify job skills and strengths and look for new work opportunities if necessary.
- Psychological or psychiatric therapy can assist many people as they recuperate from stroke. Depression, anxiety, frustration, and anger are common disabilities in people with stroke. Therapy, along with medication, can help ease some of the mental and emotional problems that result from stroke. Sometimes it is useful for family members to seek psychological help for themselves, as well.
- The U.S. Food and Drug Administration (FDA) approved the Neurolutions Upper Extremity Rehabilitation System for individuals age 18 and older with upper arm disability who are undergoing stroke rehabilitation to increase range of motion and grasping. The brain-computer interface uses non-invasive electroencephalography electrodes to record brain activity, which is then wirelessly conveyed to a tablet for the analysis of the intended muscle movement, and a signal is sent to a wireless electronic hand brace, which in turn moves the person’s hand.
- The FDA approved the MicroTransponder Vivistim Paired VNS (vagus nerve stimulation) System, which is to be used along with stroke rehabilitation to help individuals who have moderate to severe impaired upper limb and extremity motor defects caused by a chronic ischemic stroke. The system electrically stimulates the vagus nerve, which runs from the brain down to the abdomen, to improve upper limb and extremity motor function and to improve an individual’s ability to move the arms and hands..
Subarachnoid hemorrhage prognosis
How well a person with subarachnoid hemorrhage does depends on a number of different factors, including:
- Cause of subarachnoid hemorrhage
- Location and amount of bleeding (grade of subarachnoid hemorrhage)
- Presence of other injuries/pathologies/co-morbidities
- Complications
In general subarachnoid hemorrhage (SAH) is associated with a high early mortality rate 91. Older age and more severe symptoms can lead to a poorer outcome.
A small amount of traumatic subarachnoid hemorrhage or small perimesencephalic blood has an excellent prognosis with little if any significant long-term consequences. A grade 5 aneurysmal subarachnoid hemorrhage, on the other hand, has a dismal prognosis, despite aggressive treatment.
People can recover completely after treatment. Survivors of subarachnoid hemorrhage (SAH) often endure numerous ongoing complications, including disabilities, cognitive disorders, and psychological problems 92. But some people die, even with treatment 93. At least 10%‐15% of patients with aneurysmal subarachnoid hemorrhage (aSAH) die before reaching the hospital 6.
A population-based study published in 2017 found that approximately 18 percent of patients with SAH died suddenly before being evaluated in a hospital 94. Among patients who reach the hospital alive, much of the subsequent early mortality is caused by the common complications of aneurysmal SAH related to initial bleeding, rebleeding, vasospasm and delayed cerebral ischemia, hydrocephalus, increased intracranial pressure, seizures, and cardiac complications 94.
Long-term complications of SAH include neurocognitive dysfunction, epilepsy, and other focal neurologic deficits. In one registry, more than 10 percent of patients with SAH remained moderately or severely disabled 95.
- Subarachnoid hemorrhage. https://n.neurology.org/content/neurology/80/5/e56.full.pdf[↩]
- Ziu E, Khan Suheb MZ, Mesfin FB. Subarachnoid Hemorrhage. [Updated 2023 Jun 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK441958[↩][↩][↩]
- Kairys N, M Das J, Garg M. Acute Subarachnoid Hemorrhage. [Updated 2022 Oct 10]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK518975[↩]
- Smith M., Citerio G. What’s new in subarachnoid hemorrhage. Intensive Care Med. 2015;41(1):123–126. doi: 10.1007/s00134-014-3548-5[↩]
- Subarachnoid hemorrhage. https://medlineplus.gov/ency/article/000701.htm[↩]
- Daou BJ, Koduri S, Thompson BG, Chaudhary N, Pandey AS. Clinical and experimental aspects of aneurysmal subarachnoid hemorrhage. CNS Neurosci Ther. 2019 Oct;25(10):1096-1112. doi: 10.1111/cns.13222[↩][↩]
- Vlak MH, Algra A, Brandenburg R, Rinkel GJ. Prevalence of unruptured intracranial aneurysms, with emphasis on sex, age, comorbidity, country, and time period: a systematic review and meta-analysis. Lancet Neurol. 2011 Jul;10(7):626-36. doi: 10.1016/S1474-4422(11)70109-0[↩]
- de Rooij NK, Linn FH, van der Plas JA, Algra A, Rinkel GJ. Incidence of subarachnoid haemorrhage: a systematic review with emphasis on region, age, gender and time trends. J Neurol Neurosurg Psychiatry. 2007 Dec;78(12):1365-72. doi: 10.1136/jnnp.2007.117655[↩]
- Shea AM, Reed SD, Curtis LH, Alexander MJ, Villani JJ, Schulman KA. Characteristics of nontraumatic subarachnoid hemorrhage in the United States in 2003. Neurosurgery. 2007 Dec;61(6):1131-7; discussion 1137-8. doi: 10.1227/01.neu.0000306090.30517.ae[↩]
- Labovitz DL, Halim AX, Brent B, Boden-Albala B, Hauser WA, Sacco RL. Subarachnoid hemorrhage incidence among Whites, Blacks and Caribbean Hispanics: the Northern Manhattan Study. Neuroepidemiology. 2006;26(3):147-50. doi: 10.1159/000091655[↩]
- Connolly ES Jr, Rabinstein AA, Carhuapoma JR, Derdeyn CP, Dion J, Higashida RT, Hoh BL, Kirkness CJ, Naidech AM, Ogilvy CS, Patel AB, Thompson BG, Vespa P; American Heart Association Stroke Council; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular Nursing; Council on Cardiovascular Surgery and Anesthesia; Council on Clinical Cardiology. Guidelines for the management of aneurysmal subarachnoid hemorrhage: a guideline for healthcare professionals from the American Heart Association/american Stroke Association. Stroke. 2012 Jun;43(6):1711-37. doi: 10.1161/STR.0b013e3182587839[↩][↩][↩][↩][↩]
- White PM, Teasdale EM, Wardlaw JM, Easton V. Intracranial aneurysms: CT angiography and MR angiography for detection prospective blinded comparison in a large patient cohort. Radiology. 2001 Jun;219(3):739-49. doi: 10.1148/radiology.219.3.r01ma16739[↩]
- Werring DJ, Banerjee G. Convexity subarachnoid haemorrhage. Lancet. 2023 Jan 21;401(10372):193-194. https://doi.org/10.1016/S0140-6736(23)00004-1[↩]
- Oppenheim C, Domigo V, Gauvrit JY, Lamy C, Mackowiak-Cordoliani MA, Pruvo JP, Méder JF. Subarachnoid hemorrhage as the initial presentation of dural sinus thrombosis. AJNR Am J Neuroradiol. 2005 Mar;26(3):614-7. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7976499[↩][↩]
- Benjamin E.J., Virani S.S., Callaway C.W., et al. American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics-2018 update: A report from the american heart association. Circulation. 2018;137(12):e67–e492. doi: 10.1161/CIR.0000000000000558[↩]
- Marder CP, Narla V, Fink JR, Tozer Fink KR. Subarachnoid hemorrhage: beyond aneurysms. AJR Am J Roentgenol. 2014 Jan;202(1):25-37. doi: 10.2214/AJR.12.9749[↩]
- Perimesencephalic subarachnoid hemorrhage. https://radiopaedia.org/articles/perimesencephalic-subarachnoid-haemorrhage?lang=us[↩]
- Brain arteriovenous malformation. https://radiopaedia.org/articles/brain-arteriovenous-malformation?lang=us[↩]
- Berlit P. Diagnosis and treatment of cerebral vasculitis. Ther Adv Neurol Disord. 2010 Jan;3(1):29-42. doi: 10.1177/1756285609347123[↩]
- van Gijn J, Rinkel GJ. Subarachnoid haemorrhage: diagnosis, causes and management. Brain. 2001 Feb;124(Pt 2):249-78. doi: 10.1093/brain/124.2.249[↩]
- Eden SV, Meurer WJ, Sánchez BN, Lisabeth LD, Smith MA, Brown DL, Morgenstern LB. Gender and ethnic differences in subarachnoid hemorrhage. Neurology. 2008 Sep 2;71(10):731-5. doi: 10.1212/01.wnl.0000319690.82357.44[↩]
- Correction. Circulation. 2015 Jun 16;131(24):e535. doi: 10.1161/CIR.0000000000000219. Erratum for: Circulation. 2015 Jan 27;131(4):e29-322[↩]
- Vlak MH, Rinkel GJ, Greebe P, van der Bom JG, Algra A. Trigger factors for rupture of intracranial aneurysms in relation to patient and aneurysm characteristics. J Neurol. 2012 Jul;259(7):1298-302. doi: 10.1007/s00415-011-6341-1[↩]
- Rinkel GJ, Wijdicks EF, Vermeulen M, Ramos LM, Tanghe HL, Hasan D, Meiners LC, van Gijn J. Nonaneurysmal perimesencephalic subarachnoid hemorrhage: CT and MR patterns that differ from aneurysmal rupture. AJNR Am J Neuroradiol. 1991 Sep-Oct;12(5):829-34. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8333493/pdf/1950905.pdf[↩]
- Schwartz TH, Solomon RA. Perimesencephalic nonaneurysmal subarachnoid hemorrhage: review of the literature. Neurosurgery. 1996 Sep;39(3):433-40; discussion 440. doi: 10.1097/00006123-199609000-00001[↩]
- Canhão P, Ferro JM, Pinto AN, Melo TP, Campos JG. Perimesencephalic and nonperimesencephalic subarachnoid haemorrhages with negative angiograms. Acta Neurochir (Wien). 1995;132(1-3):14-9. doi: 10.1007/BF01404842[↩]
- Tatter SB, Crowell RM, Ogilvy CS. Aneurysmal and microaneurysmal “angiogram-negative” subarachnoid hemorrhage. Neurosurgery. 1995 Jul;37(1):48-55. doi: 10.1227/00006123-199507000-00007[↩]
- Jung JY, Kim YB, Lee JW, Huh SK, Lee KC. Spontaneous subarachnoid haemorrhage with negative initial angiography: a review of 143 cases. J Clin Neurosci. 2006 Dec;13(10):1011-7. doi: 10.1016/j.jocn.2005.09.007[↩]
- Rinkel GJ, van Gijn J, Wijdicks EF. Subarachnoid hemorrhage without detectable aneurysm. A review of the causes. Stroke. 1993 Sep;24(9):1403-9. doi: 10.1161/01.str.24.9.1403[↩][↩]
- Cordonnier C, Al-Shahi Salman R, Bhattacharya JJ, Counsell CE, Papanastassiou V, Ritchie V, Roberts RC, Sellar RJ, Warlow C; SIVMS Collaborators. Differences between intracranial vascular malformation types in the characteristics of their presenting haemorrhages: prospective, population-based study. J Neurol Neurosurg Psychiatry. 2008 Jan;79(1):47-51. doi: 10.1136/jnnp.2006.113753[↩]
- Koch C. Spinal dural arteriovenous fistula. Curr Opin Neurol. 2006 Feb;19(1):69-75. doi: 10.1097/01.wco.0000200547.22292.11[↩]
- Caplan LR. Dissections of brain-supplying arteries. Nat Clin Pract Neurol. 2008 Jan;4(1):34-42. doi: 10.1038/ncpneuro0683[↩][↩]
- Santos-Franco JA, Zenteno M, Lee A. Dissecting aneurysms of the vertebrobasilar system. A comprehensive review on natural history and treatment options. Neurosurg Rev. 2008 Apr;31(2):131-40; discussion 140. doi: 10.1007/s10143-008-0124-x[↩]
- Nolte KB, Brass LM, Fletterick CF. Intracranial hemorrhage associated with cocaine abuse: a prospective autopsy study. Neurology. 1996 May;46(5):1291-6. doi: 10.1212/wnl.46.5.1291[↩]
- Karabatsou K, Lecky BR, Rainov NG, Broome JC, White RP. Cerebral amyloid angiopathy with symptomatic or occult subarachnoid haemorrhage. Eur Neurol. 2007;57(2):103-5. doi: 10.1159/000098060[↩]
- Beitzke M, Gattringer T, Enzinger C, Wagner G, Niederkorn K, Fazekas F. Clinical presentation, etiology, and long-term prognosis in patients with nontraumatic convexal subarachnoid hemorrhage. Stroke. 2011 Nov;42(11):3055-60. doi: 10.1161/STROKEAHA.111.621847[↩]
- Marcolini E, Hine J. Approach to the Diagnosis and Management of Subarachnoid Hemorrhage. West J Emerg Med. 2019 Mar;20(2):203-211. doi: 10.5811/westjem.2019.1.37352[↩]
- Kuroda H, Mochizuki T, Shimizu S, Kumabe T. Rupture of Thrombosed Cerebral Aneurysm During Antithrombotic Therapy for Ischemic Stroke: Case Report and Literature Review. World Neurosurg. 2019 Jun;126:468-471. doi: 10.1016/j.wneu.2019.02.238[↩]
- Shipman KE, Ramalingam SK, Dawson CH, Yasear ZA. Subarachnoid haemorrhage. Clin Med (Lond). 2019 Jan;19(1):88-89. doi: 10.7861/clinmedicine.19-1-88a[↩][↩][↩][↩][↩]
- Chalouhi N, Ali MS, Jabbour PM, Tjoumakaris SI, Gonzalez LF, Rosenwasser RH, Koch WJ, Dumont AS. Biology of intracranial aneurysms: role of inflammation. J Cereb Blood Flow Metab. 2012 Sep;32(9):1659-76. doi: 10.1038/jcbfm.2012.84[↩]
- Penn DL, Komotar RJ, Sander Connolly E. Hemodynamic mechanisms underlying cerebral aneurysm pathogenesis. J Clin Neurosci. 2011 Nov;18(11):1435-8. doi: 10.1016/j.jocn.2011.05.001[↩][↩]
- Feigin V, Parag V, Lawes CM, Rodgers A, Suh I, Woodward M, Jamrozik K, Ueshima H; Asia Pacific Cohort Studies Collaboration. Smoking and elevated blood pressure are the most important risk factors for subarachnoid hemorrhage in the Asia-Pacific region: an overview of 26 cohorts involving 306,620 participants. Stroke. 2005 Jul;36(7):1360-5. doi: 10.1161/01.STR.0000170710.95689.41[↩]
- Brisman JL, Song JK, Newell DW. Cerebral aneurysms. N Engl J Med. 2006 Aug 31;355(9):928-39. doi: 10.1056/NEJMra052760[↩]
- Chalouhi N, Hoh BL, Hasan D. Review of cerebral aneurysm formation, growth, and rupture. Stroke. 2013 Dec;44(12):3613-22. doi: 10.1161/STROKEAHA.113.002390[↩][↩]
- Hostettler IC, Werring DJ. Acute Convexity Subarachnoid Hemorrhage: What the Neurosurgeon Needs to Know. World Neurosurg. 2019 Mar;123:184-187. doi: 10.1016/j.wneu.2018.12.062[↩]
- Bassi P, Bandera R, Loiero M, Tognoni G, Mangoni A. Warning signs in subarachnoid hemorrhage: a cooperative study. Acta Neurol Scand. 1991 Oct;84(4):277-81. doi: 10.1111/j.1600-0404.1991.tb04954.x[↩]
- Al-Dhahir MA, M Das J, Sharma S. Neurogenic Pulmonary Edema. [Updated 2023 Jul 17]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK532984[↩]
- Frontera JA, Fernandez A, Schmidt JM, Claassen J, Wartenberg KE, Badjatia N, Connolly ES, Mayer SA. Defining vasospasm after subarachnoid hemorrhage: what is the most clinically relevant definition? Stroke. 2009 Jun;40(6):1963-8. doi: 10.1161/STROKEAHA.108.544700[↩][↩]
- Veldeman M, Höllig A, Clusmann H, Stevanovic A, Rossaint R, Coburn M. Delayed cerebral ischaemia prevention and treatment after aneurysmal subarachnoid haemorrhage: a systematic review. Br J Anaesth. 2016 Jul;117(1):17-40. doi: 10.1093/bja/aew095[↩]
- Kusaka G., Ishikawa M., Nanda A., Granger D.N., Zhang J.H. Signaling pathways for early brain injury after subarachnoid hemorrhage. J. Cereb. Blood Flow Metab. 2004;24(8):916–925. doi: 10.1097/01.WCB.0000125886.48838.7E[↩]
- Rass V., Helbok R. Early brain injury after poor-grade subarachnoid hemorrhage. Curr. Neurol. Neurosci. Rep. 2019;19(10):78. doi: 10.1007/s11910-019-0990-3[↩][↩]
- Sehba F.A., Hou J., Pluta R.M., Zhang J.H. The importance of early brain injury after subarachnoid hemorrhage. Prog. Neurobiol. 2012;97(1):14–37. doi: 10.1016/j.pneurobio.2012.02.003[↩]
- Dhar R., Diringer M.N. Relationship between angiographic vasospasm, cerebral blood flow, and cerebral infarction after subarachnoid hemorrhage. Acta Neurochir. Suppl. (Wien) 2015;120:161–165. doi: 10.1007/978-3-319-04981-6_27[↩]
- Macdonald R.L. Delayed neurological deterioration after subarachnoid haemorrhage. Nat. Rev. Neurol. 2014;10(1):44–58. doi: 10.1038/nrneurol.2013.246[↩]
- Hansen-Schwartz J., Vajkoczy P., Macdonald R.L., Pluta R.M., Zhang J.H. Cerebral vasospasm: looking beyond vasoconstriction. Trends Pharmacol. Sci. 2007;28(6):252–256. doi: 10.1016/j.tips.2007.04.002[↩]
- Connolly E.S., Jr, Rabinstein A.A., Carhuapoma J.R., et al. American Heart Association Stroke Council; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular Nursing; Council on Cardiovascular Surgery and Anesthesia; Council on Clinical Cardiology. Guidelines for the management of aneurysmal subarachnoid hemorrhage: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2012;43(6):1711–1737. doi: 10.1161/STR.0b013e3182587839[↩]
- Teasdale G, Murray G, Parker L, Jennett B. Adding up the Glasgow Coma Score. Acta Neurochir Suppl (Wien). 1979;28(1):13-6. doi: 10.1007/978-3-7091-4088-8_2[↩]
- Teasdale GM, Drake CG, Hunt W, Kassell N, Sano K, Pertuiset B, De Villiers JC. A universal subarachnoid hemorrhage scale: report of a committee of the World Federation of Neurosurgical Societies. J Neurol Neurosurg Psychiatry. 1988 Nov;51(11):1457. doi: 10.1136/jnnp.51.11.1457[↩]
- Hunt WE, Hess RM. Surgical risk as related to time of intervention in the repair of intracranial aneurysms. J Neurosurg. 1968 Jan;28(1):14-20. doi: 10.3171/jns.1968.28.1.0014[↩]
- Claassen J, Bernardini GL, Kreiter K, Bates J, Du YE, Copeland D, Connolly ES, Mayer SA. Effect of cisternal and ventricular blood on risk of delayed cerebral ischemia after subarachnoid hemorrhage: the Fisher scale revisited. Stroke. 2001 Sep;32(9):2012-20. doi: 10.1161/hs0901.095677[↩]
- Suarez JI. Diagnosis and Management of Subarachnoid Hemorrhage. Continuum (Minneap Minn). 2015 Oct;21(5 Neurocritical Care):1263-87. doi: 10.1212/CON.0000000000000217[↩][↩][↩]
- Djelilovic-Vranic J, Basic-Kes V, Tiric-Campara M, Djozic E, Kulenovic J. Follow-up of Vasospasm by Transcranial Doppler Sonography (TCD) in Subarachnoid Hemorrhage (SAH). Acta Inform Med. 2017 Mar;25(1):14-18. doi: 10.5455/aim.2017.25.14-18[↩]
- Diringer MN, Bleck TP, Claude Hemphill J 3rd, Menon D, Shutter L, Vespa P, Bruder N, Connolly ES Jr, Citerio G, Gress D, Hänggi D, Hoh BL, Lanzino G, Le Roux P, Rabinstein A, Schmutzhard E, Stocchetti N, Suarez JI, Treggiari M, Tseng MY, Vergouwen MD, Wolf S, Zipfel G; Neurocritical Care Society. Critical care management of patients following aneurysmal subarachnoid hemorrhage: recommendations from the Neurocritical Care Society’s Multidisciplinary Consensus Conference. Neurocrit Care. 2011 Sep;15(2):211-40. doi: 10.1007/s12028-011-9605-9[↩][↩][↩]
- Krejza J, Kochanowicz J, Mariak Z, Lewko J, Melhem ER. Middle cerebral artery spasm after subarachnoid hemorrhage: detection with transcranial color-coded duplex US. Radiology. 2005 Aug;236(2):621-9. doi: 10.1148/radiol.2362031662[↩]
- van der Schaaf I, Wermer MJ, van der Graaf Y, Velthuis BK, van de Kraats CI, Rinkel GJ. Prognostic value of cerebral perfusion-computed tomography in the acute stage after subarachnoid hemorrhage for the development of delayed cerebral ischemia. Stroke. 2006 Feb;37(2):409-13. doi: 10.1161/01.STR.0000198831.69035.43[↩]
- van der Schaaf I, Wermer MJ, van der Graaf Y, Hoff RG, Rinkel GJ, Velthuis BK. CT after subarachnoid hemorrhage: relation of cerebral perfusion to delayed cerebral ischemia. Neurology. 2006 May 23;66(10):1533-8. doi: 10.1212/01.wnl.0000216272.67895.d3[↩]
- Vatter H, Güresir E, Berkefeld J, Beck J, Raabe A, du Mesnil de Rochemont R, Seifert V, Weidauer S. Perfusion-diffusion mismatch in MRI to indicate endovascular treatment of cerebral vasospasm after subarachnoid haemorrhage. J Neurol Neurosurg Psychiatry. 2011 Aug;82(8):876-83. doi: 10.1136/jnnp.2010.219592[↩]
- Francoeur CL, Mayer SA. Management of delayed cerebral ischemia after subarachnoid hemorrhage. Crit Care. 2016 Oct 14;20(1):277. doi: 10.1186/s13054-016-1447-6[↩]
- Hellingman CA, van den Bergh WM, Beijer IS, van Dijk GW, Algra A, van Gijn J, Rinkel GJ. Risk of rebleeding after treatment of acute hydrocephalus in patients with aneurysmal subarachnoid hemorrhage. Stroke. 2007 Jan;38(1):96-9. doi: 10.1161/01.STR.0000251841.51332.1d[↩]
- Tang C, Zhang TS, Zhou LF. Risk factors for rebleeding of aneurysmal subarachnoid hemorrhage: a meta-analysis. PLoS One. 2014 Jun 9;9(6):e99536. doi: 10.1371/journal.pone.0099536[↩][↩]
- D’Souza S. Aneurysmal Subarachnoid Hemorrhage. J Neurosurg Anesthesiol. 2015 Jul;27(3):222-40. doi: 10.1097/ANA.0000000000000130[↩][↩][↩][↩][↩]
- Bath PM, Song L, Silva GS, Mistry E, Petersen N, Tsivgoulis G, Mazighi M, Bang OY, Sandset EC. Blood Pressure Management for Ischemic Stroke in the First 24 Hours. Stroke. 2022 Apr;53(4):1074-1084. doi: 10.1161/STROKEAHA.121.036143[↩]
- Osgood ML. Aneurysmal Subarachnoid Hemorrhage: Review of the Pathophysiology and Management Strategies. Curr Neurol Neurosci Rep. 2021 Jul 26;21(9):50. doi: 10.1007/s11910-021-01136-9[↩]
- MacCarthy EP, Bloomfield SS. Labetalol: a review of its pharmacology, pharmacokinetics, clinical uses and adverse effects. Pharmacotherapy. 1983 Jul-Aug;3(4):193-219. doi: 10.1002/j.1875-9114.1983.tb03252.x[↩][↩]
- Huang RQ, Jiang FG, Feng ZM, Wang TY. Nicardipine in the treatment of aneurysmal subarachnoid haemorrhage: a meta-analysis of published data. Acta Neurol Belg. 2013 Mar;113(1):3-6. doi: 10.1007/s13760-012-0142-x[↩]
- Varelas PN, Abdelhak T, Corry JJ, James E, Rehman MF, Schultz L, Mays-Wilson K, Mitsias P. Clevidipine for acute hypertension in patients with subarachnoid hemorrhage: a pilot study. Int J Neurosci. 2014 Mar;124(3):192-8. doi: 10.3109/00207454.2013.836703[↩]
- Dorhout Mees SM, Rinkel GJ, Feigin VL, Algra A, van den Bergh WM, Vermeulen M, van Gijn J. Calcium antagonists for aneurysmal subarachnoid haemorrhage. Cochrane Database Syst Rev. 2007 Jul 18;2007(3):CD000277. doi: 10.1002/14651858.CD000277.pub3[↩]
- Pickard JD, Murray GD, Illingworth R, Shaw MD, Teasdale GM, Foy PM, Humphrey PR, Lang DA, Nelson R, Richards P, et al. Effect of oral nimodipine on cerebral infarction and outcome after subarachnoid haemorrhage: British aneurysm nimodipine trial. BMJ. 1989 Mar 11;298(6674):636-42. doi: 10.1136/bmj.298.6674.636[↩]
- Petruk KC, West M, Mohr G, Weir BK, Benoit BG, Gentili F, Disney LB, Khan MI, Grace M, Holness RO, et al. Nimodipine treatment in poor-grade aneurysm patients. Results of a multicenter double-blind placebo-controlled trial. J Neurosurg. 1988 Apr;68(4):505-17. doi: 10.3171/jns.1988.68.4.0505[↩]
- Carlson AP, Hänggi D, Wong GK, Etminan N, Mayer SA, Aldrich F, Diringer MN, Schmutzhard E, Faleck HJ, Ng D, Saville BR, Bleck T, Grubb R Jr, Miller M, Suarez JI, Proskin HM, Macdonald RL; NEWTON Investigators. Single-Dose Intraventricular Nimodipine Microparticles Versus Oral Nimodipine for Aneurysmal Subarachnoid Hemorrhage. Stroke. 2020 Apr;51(4):1142-1149. doi: 10.1161/STROKEAHA.119.027396[↩]
- Dorhout Mees SM, Algra A, Vandertop WP, van Kooten F, Kuijsten HA, Boiten J, van Oostenbrugge RJ, Al-Shahi Salman R, Lavados PM, Rinkel GJ, van den Bergh WM; MASH-2 Study Group. Magnesium for aneurysmal subarachnoid haemorrhage (MASH-2): a randomised placebo-controlled trial. Lancet. 2012 Jul 7;380(9836):44-9. doi: 10.1016/S0140-6736(12)60724-7. Epub 2012 May 25. Erratum in: Lancet. 2012 Dec 8;380(9858)1994. MASH-2 Study Group [added]; Boiten, J [added]; Kerklaan, J [added]; Dennesen, P J W [added]. Erratum in: Lancet. 2012 Jul 7;380(9836):28.[↩][↩]
- Dorhout Mees SM, Algra A, Wong GK, et al. Early Magnesium Treatment After Aneurysmal Subarachnoid Hemorrhage: Individual Patient Data Meta-Analysis. Stroke. 2015 Nov;46(11):3190-3. doi: 10.1161/STROKEAHA.115.010575[↩]
- Rhoney DH, McAllen K, Liu-DeRyke X. Current and future treatment considerations in the management of aneurysmal subarachnoid hemorrhage. J Pharm Pract. 2010 Oct;23(5):408-24. doi: 10.1177/0897190010372334[↩][↩]
- Kirkpatrick PJ, Turner CL, Smith C, Hutchinson PJ, Murray GD; STASH Collaborators. Simvastatin in aneurysmal subarachnoid haemorrhage (STASH): a multicentre randomised phase 3 trial. Lancet Neurol. 2014 Jul;13(7):666-75. doi: 10.1016/S1474-4422(14)70084-5[↩]
- Wong GK, Chan DY, Siu DY, Zee BC, Poon WS, Chan MT, Gin T, Leung M; HDS-SAH Investigators. High-dose simvastatin for aneurysmal subarachnoid hemorrhage: multicenter randomized controlled double-blinded clinical trial. Stroke. 2015 Feb;46(2):382-8. doi: 10.1161/STROKEAHA.114.007006[↩]
- Liu J, Chen Q. Effect of statins treatment for patients with aneurysmal subarachnoid hemorrhage: a systematic review and meta-analysis of observational studies and randomized controlled trials. Int J Clin Exp Med. 2015 May 15;8(5):7198-208. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4509204[↩]
- Frontera JA, Lewin JJ 3rd, Rabinstein AA, Aisiku IP, Alexandrov AW, Cook AM, del Zoppo GJ, Kumar MA, Peerschke EI, Stiefel MF, Teitelbaum JS, Wartenberg KE, Zerfoss CL. Guideline for Reversal of Antithrombotics in Intracranial Hemorrhage: A Statement for Healthcare Professionals from the Neurocritical Care Society and Society of Critical Care Medicine. Neurocrit Care. 2016 Feb;24(1):6-46. doi: 10.1007/s12028-015-0222-x[↩]
- Rinkel GJ, Prins NE, Algra A. Outcome of aneurysmal subarachnoid hemorrhage in patients on anticoagulant treatment. Stroke. 1997 Jan;28(1):6-9. doi: 10.1161/01.str.28.1.6[↩]
- Xu T, Yu X, Ou S, Liu X, Yuan J, Chen Y. Efficacy and Safety of Very Early Mobilization in Patients with Acute Stroke: A Systematic Review and Meta-analysis. Sci Rep. 2017 Jul 26;7(1):6550. doi: 10.1038/s41598-017-06871-z[↩]
- Muehlschlegel S. Subarachnoid Hemorrhage. Continuum (Minneap Minn). 2018 Dec;24(6):1623-1657. doi: 10.1212/CON.0000000000000679[↩]
- van Gijn J, Kerr RS, Rinkel GJ. Subarachnoid haemorrhage. Lancet. 2007 Jan 27;369(9558):306-18. https://doi.org/10.1016/S0140-6736(07)60153-6[↩]
- Muehlschlegel S. Subarachnoid hemorrhage. Continuum (Minneap. Minn.) 2018;24(6):1623–1657. doi: 10.1212/CON.0000000000000679[↩]
- Rincon F, Rossenwasser RH, Dumont A. The epidemiology of admissions of nontraumatic subarachnoid hemorrhage in the United States. Neurosurg. 2013;73:217–223. doi: 10.1227/01.neu.0000430290.93304.33[↩]
- Lindbohm JV, Kaprio J, Jousilahti P, Salomaa V, Korja M. Risk Factors of Sudden Death From Subarachnoid Hemorrhage. Stroke. 2017 Sep;48(9):2399-2404. doi: 10.1161/STROKEAHA.117.018118[↩][↩]
- Schatlo B, Fung C, Stienen MN, et al. Incidence and Outcome of Aneurysmal Subarachnoid Hemorrhage: The Swiss Study on Subarachnoid Hemorrhage (Swiss SOS). Stroke. 2021 Jan;52(1):344-347. doi: 10.1161/STROKEAHA.120.029538[↩]





{kind=link}