Contents
- Intracranial hypertension
- Idiopathic intracranial hypertension
- Idiopathic intracranial hypertension causes
- Idiopathic intracranial hypertension pathophysiology
- Idiopathic intracranial hypertension symptoms
- Idiopathic intracranial hypertension complications
- Idiopathic intracranial hypertension diagnosis
- Idiopathic intracranial hypertension treatment
- Idiopathic intracranial hypertension prognosis
Intracranial hypertension
Intracranial hypertension is a build-up of pressure inside your skull (intracranial pressure [ICP]) or the cerebrospinal fluid (CSF) pressure within you skull is elevated 1. Normal cerebrospinal fluid (CSF) pressure varies by age. In general, CSF pressure above 25 mm water in adults and above 28 mm water in children signifies increased intracranial pressure (ICP) 2, 3, 1. Intracranial hypertension can happen as the result of a severe head injury, stroke or ruptured brain aneurysm. Intracranial hypertension can also be caused by a condition that affects your brain, such as a brain abscess, brain tumor, meningitis or encephalitis. Intracranial hypertension can also develop as a complication of another condition such as high blood pressure. Sometimes though there is no obvious reason why the pressure inside your skull (ICP) builds up around the brain. Build-up of pressure with no known cause is known as idiopathic intracranial hypertension (IIH).
An increase in intracranial pressure (ICP) is a serious and life-threatening medical problem. The pressure can damage the brain or spinal cord by pressing on important structures and by restricting blood flow into the brain.
Intracranial hypertension treatment depends on the cause.
What is cerebrospinal fluid?
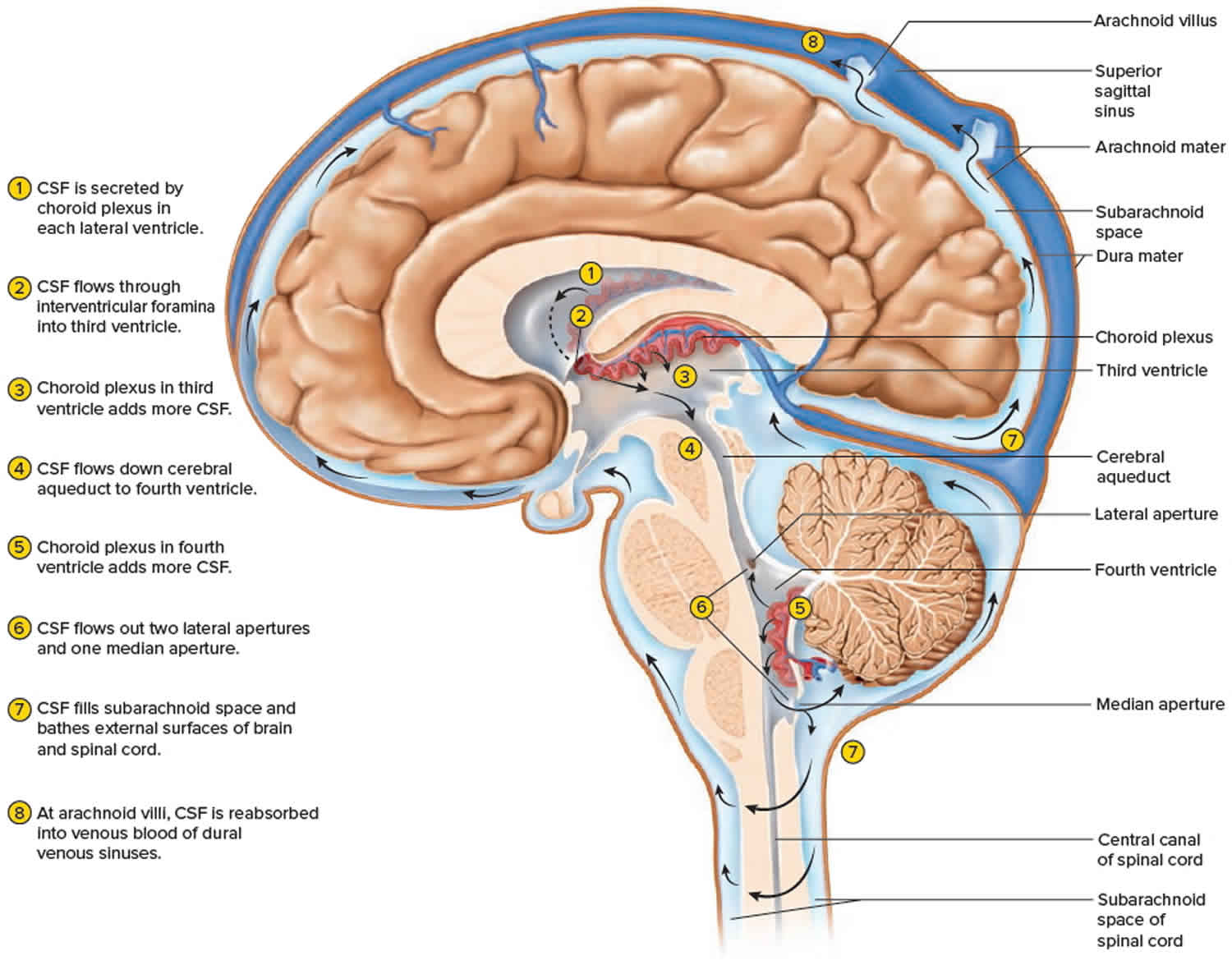
Cerebrospinal fluid (CSF) is a clear, colorless liquid that can be found around and within the ventricles and canals of the central nervous system (brain and spinal cord) and bathes its external surface. Your brain and spinal cord are surrounded by cerebrospinal fluid (CSF), which cushions these vital tissues from injury. The cerebrospinal fluid (CSF) flows in and around the hollow spaces of your brain and spinal cord, and between two of the meninges (the thin layers of tissue that cover and protect the brain and spinal cord). The brain produces about 500 mL of cerebrospinal fluid per day, but the cerebrospinal fluid is constantly reabsorbed at the same rate and only 100 to 160 mL is normally present at one time 4. It should be noted that cerebrospinal fluid is continuously generated and reabsorbed. Depending on the rate of production and absorption (which varies person to person), the supply of cerebrospinal fluid can be replaced about every 7.5 hours. Most this cerebrospinal fluid is produced in the ventricles of the brain by the choroid plexus. However, a smaller portion is produced by the ependymal cells which line the ventricles. After production, the cerebrospinal fluid travels through the ventricles and then around the brain and spinal cord. Cerebrospinal fluid (CSF) is then reabsorbed directly into the blood through structures in the arachnoid mater called arachnoid villi (arachnoid granulations). Importantly, cerebrospinal fluid can be examined clinically through a lumbar puncture. With a lumbar puncture, physicians can look for abnormalities in the cerebrospinal fluid, which can be helpful when creating a differential diagnosis 5.
Figure 1. Cerebrospinal fluid
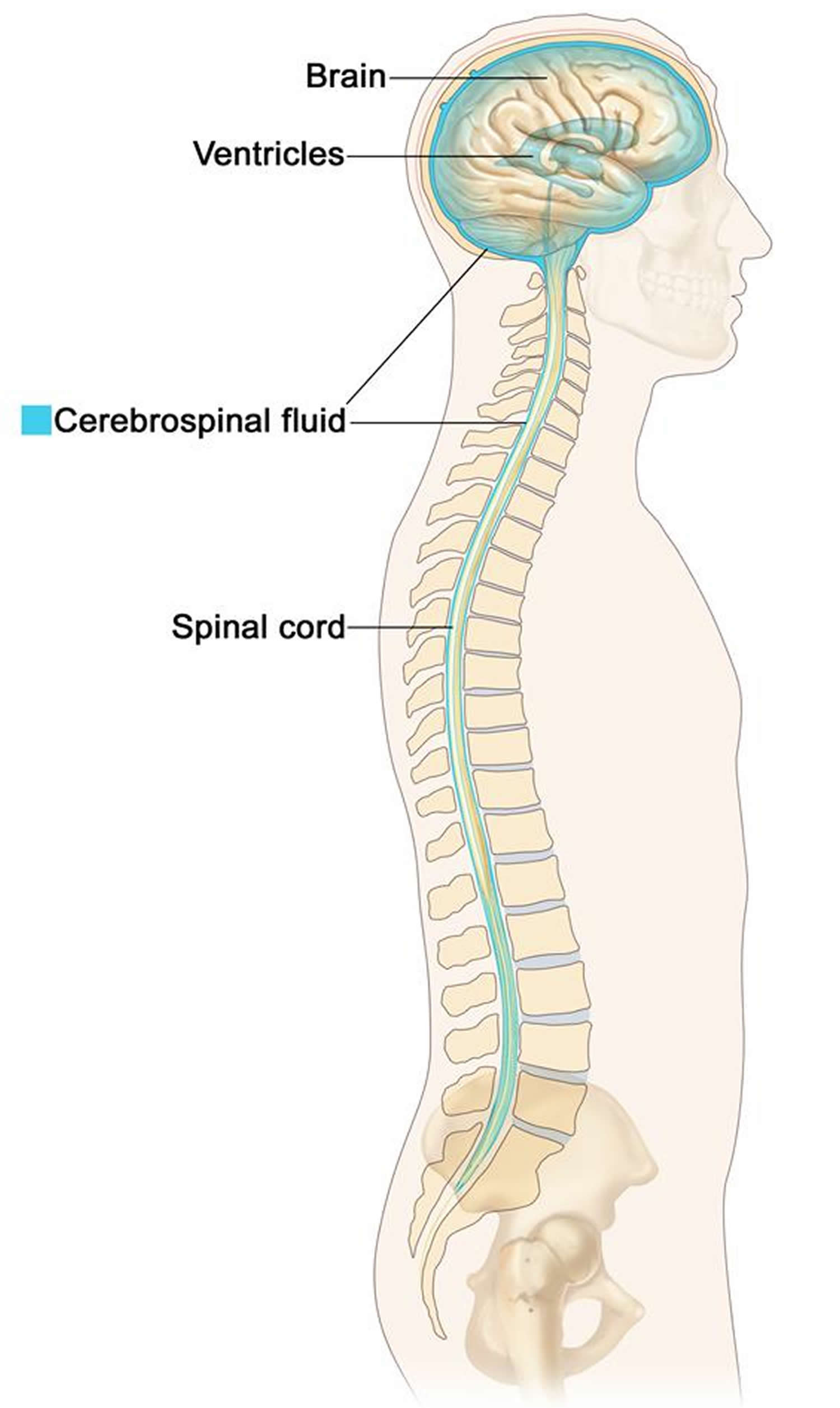
Figure 2. Cerebrospinal fluid formation, absorption and circulation around and within the brain
Intracranial hypertension causes
Intracranial hypertension or increased intracranial pressure can be due to a rise in the pressure of the cerebrospinal fluid (CSF). The cerebrospinal fluid is made by tissue called the choroid plexus in the ventricles (hollow spaces) in your brain and eventually is absorbed into your bloodstream at a rate that usually allows the pressure in your brain to remain constant. The cerebrospinal fluid (CSF) surrounds your brain and spinal cord. An increase in intracranial pressure can also be due to a rise in pressure within the brain itself. This can be caused by a mass such as a tumor, bleeding into the brain or fluid around the brain (hydrocephalus), or swelling of the brain.
Many conditions can increase intracranial pressure.
The cause of intracranial hypertension can be divided into two categories:
- Primary or Intracranial Causes
- Trauma (epidural hematoma, subdural hematoma, intracerebral hemorrhage or contusions)
- Brain tumors
- Stroke
- Nontraumatic intracerebral hemorrhage (aneurysm rupture)
- Idiopathic or benign intracranial hypertension
- Hydrocephalus
- Meningitis
- Secondary or Extracranial Causes
- Hypoventilation (hypoxia or hypercarbia)
- Hypertension
- Airway obstruction
- Metabolic (drug-induced)
- Seizures
- Hyperpyrexia
- High altitude cerebral edema
Intracranial hypertension common causes of include 1, 6, 7, 8, 9:
- Aneurysm rupture and subarachnoid hemorrhage (SAH)
- Brain tumor
- Encephalitis (irritation and swelling, or inflammation of the brain)
- Head injury
- Hydrocephalus (increased fluid within the brain)
- Hypertensive brain hemorrhage (bleeding in the brain from high blood pressure)
- Intraventricular hemorrhage (bleeding into the fluid-filled areas, or ventricles, inside the brain)
- Meningitis (infection of the membranes covering the brain and spinal cord)
- Subdural hematoma (bleeding between the covering of the brain and the surface of the brain)
- Epidural hematoma (bleeding between the inside of the skull and the outer covering of the brain)
- Seizure
- Stroke
- Brain injury following a cardiac arrest
- Clots in the veins of the brain (sinus thrombosis).
If doctors can’t find a reason for the high intracranial pressure (ICP), it’s called idiopathic intracranial hypertension (IIH).
The cause of intracranial hypertension can also be categorized into:
- Acute intracranial hypertension happens suddenly, usually because of an accident or stroke
- Chronic intracranial hypertension develops over time, usually because of a health problem like a blood clot or brain tumor, or from taking certain medicines
Intracranial hypertension prevention
Traumatic brain injury risk can be reduced by wearing appropriate protective headgear for contact sports, while riding a bicycle, and during similar activities. Otherwise, this condition usually cannot be prevented. If you have a persistent headache, blurred vision, changes in your level of alertness, nervous system problems, or seizures, seek medical help right away.
Intracranial hypertension symptoms
Intracranial hypertension symptoms can include:
- a constant throbbing headache which may be worse in the morning, or when coughing or straining; it may improve when standing up
- temporary loss of vision – your vision may become dark or “greyed out” for a few seconds at a time; this can be triggered by coughing, sneezing or bending down
- feeling and being sick
- feeling sleepy
- feeling irritable
- finding it difficult or painful to look at bright lights (photophobia)
- hearing a pulsing rhythmic noise in your ears (pulsatile tinnitus)
- problems with co-ordination and balance
- mental confusion
- loss of feeling or weakness
Intracranial hypertension diagnosis
Your doctor may suspect you have intracranial hypertension if you have symptoms of increased pressure on your brain, such as vision problems and headaches.
If a doctor thinks you have intracranial hypertension he/she will refer you to a neurologist (a doctor specializing in the brain).
You may have several different tests to diagnose intracranial hypertension, such as:
- an examination to check functions such as your muscle strength, reflexes and balance. Any problems could be a sign of an issue with your brain or nerves
- an assessment of your eyes and vision
- a magnetic resonance imaging (MRI) or computed tomography (CT) scan of your brain
- a lumbar puncture, where a needle is inserted into your spine to check for high pressure in the fluid that surrounds your brain and spinal cord
Idiopathic intracranial hypertension (IIH) may be diagnosed if you have increased pressure on your brain and no other cause can be found.
Intracranial hypertension treatment
Intracranial hypertension treatment depends on the cause. Sudden increased intracranial pressure is an emergency. The person will be treated in the intensive care unit of the hospital. The health care team will measure and monitor the person’s neurological and vital signs, including temperature, pulse, breathing rate, and blood pressure.
Intracranial hypertension treatment may include:
- Breathing support
- Draining of cerebrospinal fluid to lower pressure in the brain
- Medicines to decrease swelling
- Removal of part of the skull, especially in the first 2 days of a stroke that involves brain swelling
If a tumor, hemorrhage, or other problem has caused the increase in intracranial pressure, these problems will be treated.
Intracranial hypertension prognosis
Intracranial hypertension prognosis (outlook) depends on the underlying cause. Sudden increased intracranial pressure is a serious and often life-threatening condition. Prompt treatment results in a better outlook.
If the increased pressure pushes on important brain structures and blood vessels, it can lead to serious, permanent problems or even death.
Long-lasting increased intracranial pressure (such as with idiopathic intracranial hypertension) can result in permanent vision loss
Idiopathic intracranial hypertension
Idiopathic intracranial hypertension (IIH) also known as benign intracranial hypertension or pseudotumor cerebri is a disorder that causes the pressure inside your skull (intracranial pressure [ICP]) to increase for no obvious reason and occurring most commonly in obese women of childbearing age 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 8. The combination of raised intracranial pressure (ICP) without hydrocephalus or mass lesion, normal cerebrospinal fluid (CSF) composition and where no underlying cause is found are accepted criteria for the diagnosis of idiopathic intracranial hypertension (IIH) 19. Idiopathic intracranial hypertension (IIH) occurs more often in women than men, especially in young obese women 20 to 40 years old. Idiopathic intracranial hypertension (IIH) is rare in infants, but can occur in children 20. Before puberty, it occurs equally in boys and girls 20. The overall age-adjusted and gender-adjusted annual incidence is increasing and was reported to be 2.4 per 100,000 within the last decade (2002–2014) 21.
The majority of patients presenting with idiopathic intracranial hypertension (IIH) have symptoms that include a headache that is progressively more severe and frequent, as defined by International Classification of Headache Disorders, 3rd edition 22. The headache type is highly variable and may mimic other primary headache disorders. Other symptoms may include transient visual obscurations (unilateral or bilateral darkening of the vision typically seconds), reduced visual acuity and constriction of visual fields, pulsatile tinnitus, back pain, dizziness, neck pain, visual blurring, cognitive disturbances, radicular pain and typically horizontal diplopia 10, 23, 18; none of which are pathognomonic for idiopathic intracranial hypertension (IIH) 24. Papilledema is the hallmark finding on fundoscopic examination, which is typically bilateral but uncommonly may be unilateral or even absent, making the clinical diagnosis difficult 25. Neurological examination is usually normal, except visual field deficit or sixth cranial nerve palsy are sometimes encountered.
The cause of elevated intracranial pressure (ICP) in idiopathic intracranial hypertension (IIH) is not completely understood and a thorough investigation is required to rule out secondary known causes 26, 27.
Lumbar puncture is central in idiopathic intracranial hypertension (IIH) diagnosis 28. The CSF composition is normal but the opening pressure is elevated (with 20-25 cm H2O considered equivocal and >25 cm H2O considered definitely abnormal) 28. It is controversial whether positioning during lumbar puncture is clinically important, with some insisting that lateral decubitus is the most accurate but others believing the default position for fluoroscopy-guided lumbar puncture, prone, is close enough 29. It should also be noted that opening pressure can vary during the day. One study continuously measuring CSF pressures demonstrated many patients had intermittent pressure waves with amplitudes of 50–80 mmHg (68–109 cm H2O) that lasted 5 to 20 minutes 30.
Management of idiopathic intracranial hypertension depends on your symptoms and signs and requires an interdisciplinary team approach.
For most people, idiopathic intracranial hypertension symptoms get better with treatment. Treatments include:
- Weight loss. For people who are overweight or obese and have idiopathic intracranial hypertension, weight loss is usually the first treatment 31. Losing about 5 to 10 percent of your body weight can help lessen your symptoms — for example, if you weigh 200 pounds, that means losing about 10 to 20 pounds. Talk with your doctor about safe, sustainable ways to lose weight.
- Medicine. Your doctor may recommend a medicine called acetazolamide (Diamox) in addition to weight loss 28, 32. Acetazolamide (Diamox) helps your body make less CSF.
- Surgery. If other treatments don’t work, your doctor might suggest surgery to help relieve the pressure. In shunt surgery, doctors make a small hole and add a thin tube, called a shunt, to help extra fluid drain from around your brain into the rest of your body. There is also an eye surgery where doctors make a small hole in the covering around the optic nerve.
Figure 3. Idiopathic intracranial hypertension diagnostic criteria
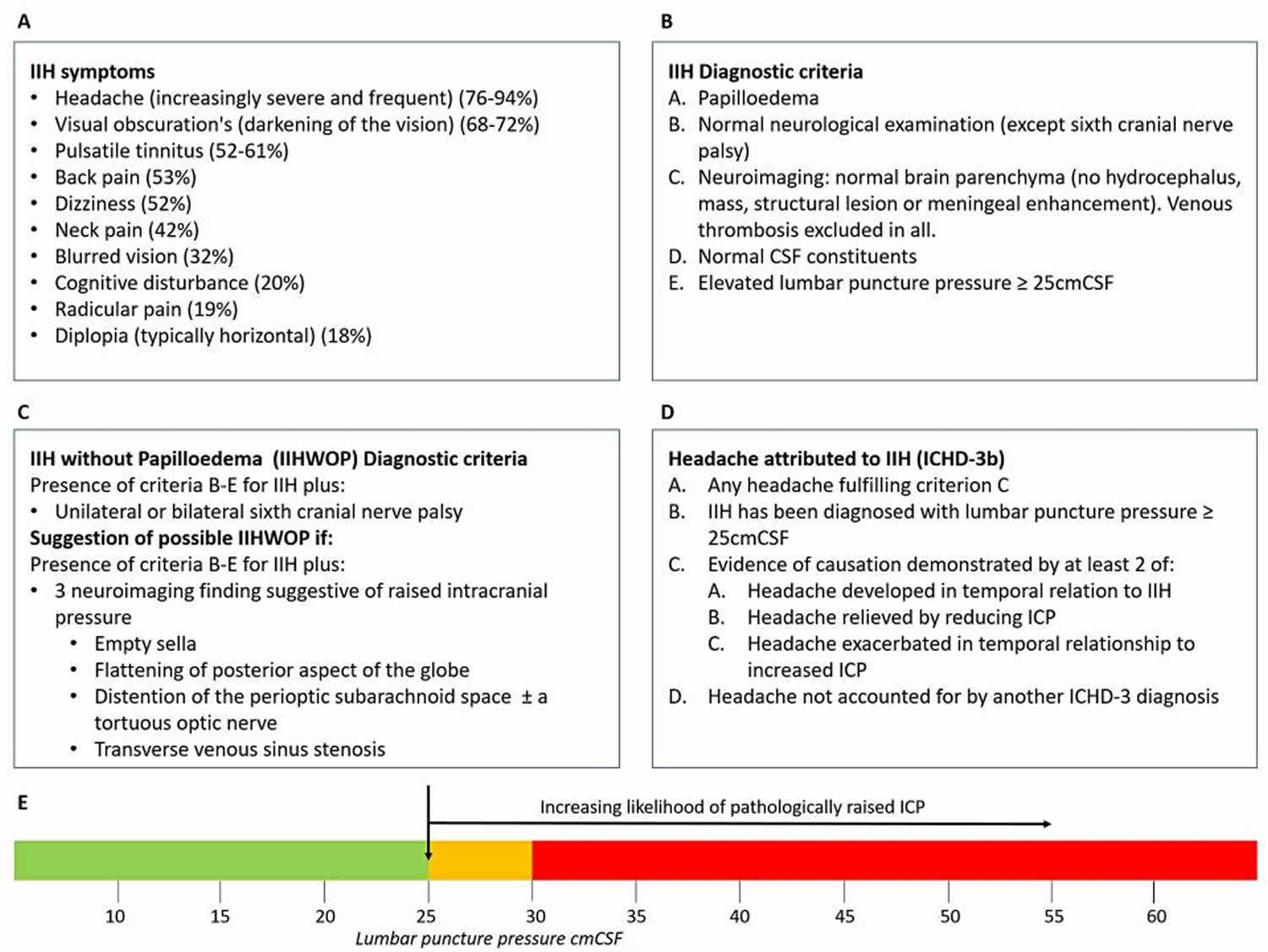
Footnotes: (A) Frequency of IIH symptoms reported, adapted from Markey et al. 3 (B) IIH diagnostic criteria, adapted from Friedman et al.4 (C) IIHWOP diagnostic criteria, adapted from Friedman et al.4 (D) Headache attributed to IIH, as described by the International Classification of Headache Disorders, 3rd edition (beta version) (ICHD-3 beta).6 (E) Line figure detailing the consensus of the interpretation of lumboperitoneal opening pressure. Uncertainty: it needs to be recognized that this is a single lumboperitoneal OP measurement; and after raised ICP what is then a normal ICP for this population on repeat lumboperitoneal readings is unknown.
Abbreviations: CSF = cerebrospinal fluid; IIH = idiopathic intracranial hypertension; LP = lumboperitoneal.
[Source 33 ]Figure 4. Idiopathic intracranial hypertension diagnosis

Footnote: Diagnostic approach for idiopathic intracranial hypertension.
Abbreviations: CP =, cranial pressure; CSF =, cerebrospinal fluid; CVST = cerebral venous sinus thrombosis; ICP = intracranial pressure.
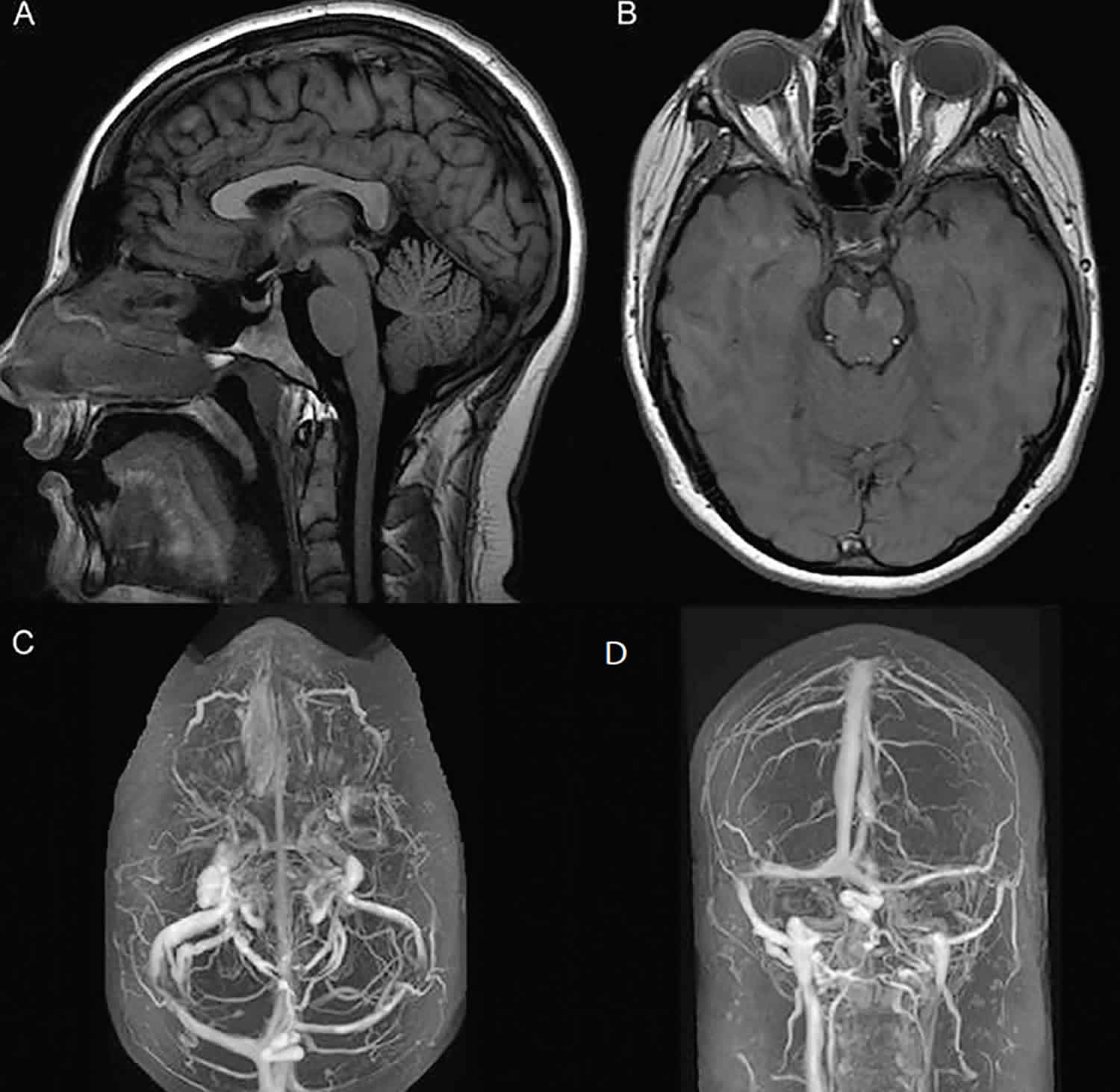
[Source 13 ]Figure 5. Idiopathic intracranial hypertension radiology

Footnotes: Idiopathic intracranial hypertension radiology showing prominent subarachnoid space around the optic nerves (yellow); mild vertical tortuosity of the optic nerves (red arrows); flattening of the posterior sclera (blue dotted lines); partially empty sella turcica (red circle); stenosis of the lateral segments of the transverse sinuses (green arrows)
[Source 34 ]Figure 6. Idiopathic intracranial hypertension treatment
Who gets idiopathic intracranial hypertension?
idiopathic intracranial hypertension can happen to anyone. Idiopathic intracranial hypertension is a condition found more commonly in women (90%), but some men are also affected by it. It is common in teenagers and young women, but can also affect children and adults of any age.
What is body mass index (BMI)?
Body mass index (BMI) is a person’s weight in kilograms divided by the square of height in meters. BMI is an inexpensive and easy screening method that estimates if a person has a healthy weight, underweight, overweight, or obesity. Having overweight or obesity can increase your risk for many health problems including idiopathic intracranial hypertension. Adults can use a BMI calculator to estimate their BMI (https://www.cdc.gov/healthyweight/assessing/bmi/adult_BMI/english_bmi_calculator/bmi_calculator.html).
Idiopathic intracranial hypertension causes
The cause of idiopathic intracranial hypertension is not known. Your brain and spinal cord are surrounded by cerebrospinal fluid (CSF), which cushions these vital tissues from injury. This fluid is produced in your brain and eventually is absorbed into your bloodstream at a rate that usually allows the pressure in your brain to remain constant. The increased intracranial pressure (ICP) of idiopathic intracranial hypertension might result from a problem in this absorption process which causes the pressure to increase. If a cause is determined, the condition is called secondary intracranial hypertension, rather than idiopathic intracranial hypertension (IIH).
Risk factors for idiopathic intracranial hypertension
While the cause of idiopathic intracranial hypertension (IIH) is unknown, a number of risk factors have been linked to idiopathic intracranial hypertension (IIH).
- Idiopathic intracranial hypertension is a rare condition that mainly affects women in their 20s and 30s.
- Obesity: Idiopathic intracranial hypertension most often happens in women of childbearing age who have gained weight. The reason for this is unclear.
Other factors that have been linked with idiopathic intracranial hypertension (IIH) include 35, 36:
- Conditions and diseases that have been linked to secondary intracranial hypertension include:
- Addison’s disease
- Adrenal insufficiency
- Behcet disease
- Cushing’s syndrome
- Hypothyroidism (underactive thyroid)
- Hyperthyroidism (overactive thyroid)
- Anemia (iron deficiency anemia)
- Blood-clotting disorders
- Chronic kidney disease/renal failure
- Systemic lupus erythematosis (an autoimmune disorder that can cause inflammation throughout your body, including in your joints, skin, blood vessels and organs, such as the kidneys)
- Polycystic ovary syndrome
- Sleep apnea or obstructive sleep apnea syndrome
- Underactive parathyroid glands (hypoparathyroidism)
- Chronic obstructive pulmonary disease (COPD)
- Pregnancy
- Sarcoidosis (inflammation of the lymph nodes, lungs, liver, eyes, skin, or other tissues)
- Infectious diseases such as HIV/AIDS, Lyme disease, following chickenpox in children
- Psittacosis
- Down syndrome
- Craniosynostosis
- Turner syndrome
- Obstruction to venous drainage
- Cerebral venous sinus thrombosis
- Jugular vein thrombosis
- Superior vena cava syndrome
- Jugular vein ligation following bilateral radical neck dissection
- Increased right heart pressure
- Arteriovenous fistulas
- Previous infection or subarachnoid hemorrhage causing decreased CSF absorption
- Medications. Substances linked to secondary intracranial hypertension include:
- Growth hormone
- Tetracycline antibiotic
- Fluoroquinolones
- Corticosteroid withdrawal
- Danazol
- Vitamin A derivatives (including isotretinoin and all-transretinoic acid)
- Levothyroxine
- Nalidixic acid
- Tamoxifen
- Ciclosporin
- Levonorgestrel impant
- Lithium
- Indomethacin
- Cimetidine
- Lithium (for mental health problems)
- Medicines for thyroid problems
- Too much vitamin A.
Idiopathic intracranial hypertension pathophysiology
The pathological processes underlying elevated intracranial pressure (ICP) in idiopathic intracranial hypertension patients are unknown. Current research is focused on understanding the respective roles of obesity, increased cerebrospinal fluid (CSF) production, outflow obstruction, and hormonal dysregulation. Additional theoretical mechanisms, such as venous hypertension or increased venous sinus pressures and reduced CSF absorption, may also play a role in the pathophysiology of idiopathic intracranial hypertension 37, 12, 38. There is however an emerging theme that idiopathic intracranial hypertension is a neurometabolic disease 38. Adderley et al. 39 found a twofold increase in cardiovascular disease risk in women with idiopathic intracranial hypertension compared to age-, sex- and, most importantly, body mass index (BMI)-matched controls. This suggests that multiple factors may be driving the disease.
Obesity
There is a well-established link between idiopathic intracranial hypertension and obesity; obesity dramatically increases young women’s risk of idiopathic intracranial hypertension 40, 41. The prevalence of idiopathic intracranial hypertension in populations with a higher body mass index (BMI) is greater than in the general population 42. The dramatic rise in obesity rates globally is mirrored in the rising incidence of idiopathic intracranial hypertension 43, 44, 42, 45. Even in women who aren’t obese, a moderate amount of weight gain can increase the risk. Losing extra pounds and maintaining a healthy weight might help reduce your chances of developing this potentially sight-stealing disorder.
Daniels et al. 46 found that, compared to controls, patients with idiopathic intracranial hypertension reported higher weight gain in the 1-year period prior to the onset of the disease. Higher BMI and weight gain percentage were also associated with higher (dose-dependent) risk of idiopathic intracranial hypertension. Interestingly, weight gain of just 5–15% can lead to an increased risk of idiopathic intracranial hypertension 46. Ko et al. 41 found that patients who experienced a recurrence of idiopathic intracranial hypertension following symptom resolution showed weight gain of just 6% of total body weight. Records were analysed over a 16-year period at two hospitals, and the authors found that 26 out of the 50 patients analysed had idiopathic intracranial hypertension recurrence (increase in an average BMI of 1.3 per year), and the 24 who had no recurrence did not gain weight (average decrease in BMI of 0.96 per year) 41. This shows the exquisite sensitivity between even modest weight gain and recurrence of idiopathic intracranial hypertension. Adderley et al. reported that the incidence of idiopathic intracranial hypertension increased rapidly above a BMI of 30 kg/m² 39. This evidence reinforces the close link between obesity and idiopathic intracranial hypertension.
Lifestyle interventions such as diet and exercise have long been known to be an effective treatment for idiopathic intracranial hypertension; the first study to demonstrate the effectiveness of a lifestyle intervention for improvement of idiopathic intracranial hypertension symptoms was carried out in 1974 47. In the mid-1990s, the first cases of weight-loss surgery for idiopathic intracranial hypertension were reported 48. Previous literature shows that between 3 and 15% loss in body weight is required to put the disease into remission. An objective evaluation of weight loss in idiopathic intracranial hypertension was performed as a prospective crossover cohort trial using a very low-calorie meal replacement to induce significant weight loss, defined as a loss of 15% or greater of total body weight. Such weight loss resulted in significantly lowered intracranial pressure (ICP) and improved papilloedema, visual function (perimetry and acuity) and headache outcomes (50% improvement in headache frequency, severity and frequency of analgesic use) 49. In the Idiopathic Intracranial Hypertension Treatment Trial (IIHTT), a randomised controlled trial (RCT) investigating the use of acetazolamide in idiopathic intracranial hypertension patients with mild visual loss, the treatment group used acetazolamide, and both groups (placebo and treatment) were provided a low-sodium diet with behavioral weight management support. The treatment group experienced an average 6% weight loss compared to 3% weight loss in the controls 32. The Idiopathic Intracranial Hypertension Treatment Trial (IIHTT) used a psychological statistical method to report that weight loss did not mediate the treatment effect of acetazolamide.
Distribution of body fat in idiopathic intracranial hypertension has been investigated, and it was demonstrated that truncal fat mass was the only parameter that correlated with lumbar puncture pressure, as compared with limb fat mass, BMI, waist circumference and total fat mass 50. A relationship has been established between truncal weight loss in patients with idiopathic intracranial hypertension and a reduction in disease activity 49.
The relationship between obesity and idiopathic intracranial hypertension in men is less clear, although men appear to be at risk of greater vision loss and obstructive sleep apnea if they have idiopathic intracranial hypertension 51.
CSF dysregulation
CSF is secreted by the choroid plexus, which consists of epithelial cells lining the ventricles in the brain. CSF secretion is driven by the net movement of sodium ions (Na+) from the blood to the cerebral ventricles, creating an osmotic gradient down which water moves. Although several channels are involved in this process, the principle channel and rate-limiting step is the Na+- and K+-dependent adenosine triphosphatase (Na+/K+/ATPase) that actively transports Na+ into the cerebral ventricle 52, 53. CSF flows through the ventricles and into the subarachnoid space, before being returned to the bloodstream via arachnoid granulations.
Specific inhibition of Na+/K+/ATPase with ouabain has been shown to reduce CSF secretion by 70–80% 54.
Aquaporins (AQPs), membrane-bound water transport channels, are thought to be involved in the osmotic homeostasis of the brain. Research has not demonstrated a pathogenic role for AQP4 in the genesis of idiopathic intracranial hypertension 55. AQP1, another channel, appears to be important in drug-induced elevation of ICP, and animal studies show a link between obesity, AQP1 expression and raised ICP 56. However, no investigations of the role of AQP1 in idiopathic intracranial hypertension in humans have yet been reported.
Impaired drainage of CSF into the subarachnoid space is another potential source of idiopathic intracranial hypertension. The turnover of CSF was found to be reduced in patients with papilloedema 57. Patients with idiopathic intracranial hypertension have been shown to have abnormalities in blood clotting 58, and it has been suggested that microthrombi could cause impaired CSF drainage in idiopathic intracranial hypertension 59. However, no direct evidence of microthrombi causing raised ICP has been shown to date 27.
Glucagon-Like Peptide 1
Glucagon-like peptide-1 (GLP-1) is an incretin with weight-modifying properties, and has been shown to have a natriuretic effect in the kidney through inhibition of the Na+/H+ exchanger in proximal tubule cells. CSF secretion, as discussed above, is controlled by Na+/K+/ATPase channels and pumps fluid into the ventricles akin to an inverted renal proximal tubule. Exploratory work showed that the choroid plexus expresses GLP-1 receptor 60. Botfield et al. thus hypothesised that GLP-1 could modulate CSF secretion at the choroid plexus, thereby mediating intracranial pressure (ICP) 60. Following from this, it was demonstrated that exendin-4, a GLP-1 receptor agonist, significantly reduced the activity of Na+/K+/ATPase. In a rodent study, Botfield et al. showed that exendin-4 led to a 65% reduction in intracranial pressure (ICP) within 30 min of administration, and that its effect on ICP was cumulative. This finding is now being translated into the idiopathic intracranial hypertension Pressure Clinical Study (idiopathic intracranial hypertensionPCS; ISRCTN12678718). The idiopathic intracranial hypertension pressure study is a double-blinded, placebo-controlled physiology study assessing the effects of exenatide on intracranial pressure (ICP) in patients with active idiopathic intracranial hypertension, and is expected to report soon.
Glucocorticoid Metabolism
Glucocorticoid metabolism has previously been characterised in idiopathic intracranial hypertension subjects before and after therapeutic weight reduction. 11beta-hydroxysteroid dehydrogenase type 1 (11β-HSD1) is an intracellular enzyme that converts inactive cortisone into the active cortisol. This amplifies local glucocorticoid activity independent of systemic cortisol 61. Global 11β-HSD1 activity was found to decrease with weight loss, and a significant correlation was found between the reduction in intracranial pressure (ICP) and the decrease in global 11β-HSD1 activity 62. It is now known that 11β-HSD1 is expressed and has activity in the choroid plexus epithelial cells, along with other key elements of the glucocorticoid signalling pathway. Inhibitors of 11β-HSD1, such as oral AZD4017, have been developed for type 2 diabetes mellitus, obesity and metabolic syndrome. The IIH Drug Trial hypothesised that specific inhibition of 11β-HSD1 using such drugs may decrease intracranial pressure (ICP) in individuals with idiopathic intracranial hypertension, which could open an entirely novel therapeutic avenue for targeting the disease 63.
Hormonal Dysregulation
Hormonal dysregulation has been shown to play an important role in the pathogenesis of idiopathic intracranial hypertension 37, 12, 38. Androgens have been identified as potential key players in idiopathic intracranial hypertension pathophysiology. Serum testosterone, and the enzyme 5α-reductase involved in its metabolism, has been shown to be higher in those with idiopathic intracranial hypertension compared to age- and BMI-matched controls 64. In a recent study that comprehensively compared the systemic and CSF androgen metabolome in women with idiopathic intracranial hypertension to sex-, BMI- and age-matched control groups with either simple obesity or polycystic ovary syndrome (PCOS), idiopathic intracranial hypertension women showed a pattern of androgen excess with increased serum testosterone and increased CSF testosterone and androstenedione 6. This was found to be distinct from that observed in PCOS and simple obesity. The authors went on to show that human choroid plexus expressed the androgen receptor, alongside the androgen-activating enzyme aldo-keto reductase type 1C3, and in a rodent model testosterone significantly enhanced the activity of Na+/K+ ATPase, a surrogate of CSF secretion. In summary, androgens can modulate CSF secretion via the choroid plexus, and these findings implicate androgen excess as a potential causal driver for idiopathic intracranial hypertension and therefore a potential therapeutic target 6.
The hormone leptin plays an important role in the regulation of fat storage. Leptin is secreted by adipocytes, and its concentration in the body correlates with total body fat 65. Higher serum leptin has been demonstrated in idiopathic intracranial hypertension patients, controlling for age and BMI, indicating that leptin dysregulation may be important in idiopathic intracranial hypertension 66. Another study showed that leptin was elevated in the CSF of idiopathic intracranial hypertension patients, though there was no correlation with leptin CSF levels and BMI 67. However, leptin is secreted disproportionately from subcutaneous fat compared to visceral fat 68, and since neither of these studies accounted for fat distribution, elevation of leptin in idiopathic intracranial hypertension patients may be a secondary effect of non-central body adiposity. These studies indicate that the role of leptin in idiopathic intracranial hypertension warrants further investigation.
Venous Hypertension
Increased dural venous sinus pressure has been proposed as a potential mechanism underlying idiopathic intracranial hypertension 69. Neuroimaging studies have established that venous sinus stenosis is a common finding among patients with idiopathic intracranial hypertension 70, 71, yet the extent of stenosis and the clinical course of idiopathic intracranial hypertension are still to be fully correlated 70. Reducing the intracranial pressure (ICP) by removal or diversion of CSF has been shown to reduce dural venous stenosis 72 and these findings may indicate that the stenosis may be a consequence, rather than a cause, of idiopathic intracranial hypertension 73. Despite good evidence of the effect of stenting on the venous sinus pressure gradient, the effect on CSF pressure is less clearly understood. There are many uncontrolled institutional case-based series reporting resolution of papilloedema and improvement in headache following venous sinus stenting, which is discussed below in management of idiopathic intracranial hypertension.
Idiopathic intracranial hypertension symptoms
Idiopathic intracranial hypertension (pseudotumor cerebri) signs and symptoms may include:
- Headaches that might originate behind your eyes
- A whooshing sound in your head that pulses with your heartbeat
- Tinnitus (ringing in the ears)
- Nausea, vomiting or dizziness
- Peripheral (side) vision loss
- Temporary blindness, lasting a few seconds and affecting one or both eyes
- Difficulty seeing to the side
- Double vision
- Seeing light flashes
- Blind spots
- Neck, shoulder or back pain
If you notice any changes to your vision or other symptoms, see your eye doctor.
Sometimes, symptoms that have resolved can recur months or years later.
Headache is present in over 90% of people diagnosed with idiopathic intracranial hypertension. The type of increased intracranial pressure (ICP) headache is no longer thought of as an early morning headache 74 and migraine is now reported to be the predominant headache type 75. The International Headache Society criteria have been modified to reflect that improvement in headache with intracranial pressure (ICP) reduction is no longer a requirement as a diagnostic criterion of headache attributable to idiopathic intracranial hypertension 76. Pulsatile tinnitus, either unilateral or bilateral, is commonly reported in idiopathic intracranial hypertension. Transient visual obscurations are common in idiopathic intracranial hypertension and are described by patients as ‘greying’ or ‘blacking out’ of vision in one or both eyes and lasting seconds. Transient visual obscurations are usually associated with changes in posture. Unilateral or bilateral sixth-nerve palsy may occur secondary to raised ICP and cause horizontal diplopia 12. Cognitive function has been reported to be affected in idiopathic intracranial hypertension 77.
Idiopathic intracranial hypertension complications
Idiopathic intracranial hypertension (pseudotumor cerebri) is not usually life threatening, but it can be a lifelong problem. Idiopathic intracranial hypertension (IIH) can affect your vision, and there’s a risk that you could lose your vision. This is because the increased pressure around your brain can cause swelling of the optic nerve (papilloedema). Treatment can help with problems with your vision and can reduce the risk of loss of vision.
It’s important to tell your doctor straight away if you notice any changes in your vision.
Other complications are mainly related to side effects from treatment of idiopathic intracranial hypertension (pseudotumor cerebri).
- Acetazolamide: hypokalemia, paresthesias of the extremities, and dysgeusia.
- Steroids: weight gain, refractory ICP increase when tapered, and fluid retention.
- Diuretics (furosemide, chlorthalidone): hypokalemia, hypomagnesemia (Furosemide), and ototoxicity.
- Lumbar puncture: infection, damage to surrounding structures, and post-lumbar puncture headache.
- Surgery: infection, diplopia (transient or permanent), and transient or permanent visual loss secondary to central retinal artery occlusion or ischemic optic neuropathy.
Idiopathic intracranial hypertension diagnosis
Your doctor may suspect you have intracranial hypertension if you have symptoms of increased pressure on your brain, such as vision problems and headaches.
If a doctor thinks you have intracranial hypertension he/she will refer you to a neurologist (a doctor specializing in the brain). To diagnose your condition, your doctor will review your symptoms and medical history, conduct a physical examination, and order tests.
Two useful mnemonics to remember the features of idiopathic intracranial hypertension are 78:
- VOMER
- V: ventricles of normal or reduced size
- O: optic disc protrusion
- M: Meckel’s cave enlargement
- E: empty sella
- R: reduced caliber (stenosis) venous sinuses
- MOVES
- M: Meckel’s cave enlargement
- O: optic disc protrusion
- V: venous sinus stenosis
- E: empty sella
- S: slit like ventricles
Idiopathic intracranial hypertension diagnosis involves utilization of the Modified Dandy Criteria 79:
- Signs and symptoms of increased intracranial pressure (ICP)
- The absence of localizing findings on neurologic examination
- The absence of deformity, displacement, or obstruction of the ventricular system with otherwise normal neurodiagnostic studies, except for evidence of increased cerebrospinal fluid pressure (greater than 200 mm water). Abnormal neuroimaging apart from empty sella turcica, optic nerve sheath with filled out CSF spaces, and smooth-walled non-flow-related venous sinus stenosis or collapse should lead to another diagnosis.
- Awake and alert
- No other causes of increased intracranial pressure present with CSF opening pressure of 20 cm to 25 cm water, required at least one of the following:
- Pulse-synchronous tinnitus (pulsatile tinnitus)
- Cranial nerve 6 palsy
- Frisen Grade 2 papilledema
- Echography for drusen negative and no other disc anomalies mimicking disc edema present
- MRV (Magnetic Resonance Venography) with lateral sinus collapse/stenosis preferably using ATECO technique
- Partially empty sella on coronal or sagittal views and optic nerve sheaths with filled out CSF spaces next to the globe on T2 weighted axial scans
Eye exams
If idiopathic intracranial hypertension (IIH) is suspected, a doctor trained in eye conditions (ophthalmologist) will look for a distinctive type of swelling affecting the optic nerve in the back of your eye. Your eye doctor will do several tests to check for signs of idiopathic intracranial hypertension (IIH), including a dilated eye exam to look at the back of your eye and a visual field test to check your peripheral vision.
To confirm a diagnosis of idiopathic intracranial hypertension (IIH), papilloedema needs to be present, and care must be taken in the examination of the optic nerve, as papilloedema can be misdiagnosed. This has led to unnecessary investigations, procedures and therapy, with the leading reason being the incorrect interpretation of the optic nerve appearance during clinical examination 80. Examination of the eye can be challenging, and where diagnostic uncertainty exists, the guidelines recommend that papilloedema be confirmed by an experienced specialist 33, 11.
You’ll also undergo a visual field test to see if there are any blind spots in your vision besides your so-called normal blind spot in each eye where the optic nerve enters the retina. And you’ll likely have photos taken of your eyes and an imaging test to measure the thickness of the layers of your retina (optical coherence tomography [OCT]) 33, 11.
The use of macular ganglion cell analysis may be more helpful in idiopathic intracranial hypertension 81.When imaging papilloedema, the scans can be prone to proprietary software segmentation error; therefore a qualitative assessment of the traces within the OCT should be made and adjustments in the segmentation made to ensure the reliability of the OCT parameters for longitudinal follow-up 82.
Brain imaging
Your doctor is likely to order an magnetic resonance imaging (MRI) or computed tomography (CT) scan. These tests can rule out other problems that can cause similar symptoms, such as brain tumors and blood clots.
- Magnetic resonance imaging (MRI) with venography (MRV) is the preferred imaging modality and is used to rule out other secondary causes of intracranial hypertension. Imaging reveals normal parenchyma and ventricles 83. Other findings on MRI that can suggest idiopathic intracranial hypertension but are nondiagnostic include transverse sinus stenosis 84, flattening of the posterior sclera, distension of the perioptic subarachnoid space, empty sella, and vertical tortuosity of the orbital optic nerve 85.
- Computed tomography (CT) can be performed if there are contraindications to MRI but is less sensitive and specific 86.
Spinal tap (lumbar puncture)
Lumbar puncture (spinal tap) is mandatory and forms part of the diagnostic criteria for idiopathic intracranial hypertension in addition to normal CSF composition analysis 87. Your doctor will order a lumbar puncture to measure the pressure inside your skull and analyze your spinal fluid. In this test, a specialist inserts a needle between two vertebrae in your lower back and removes a small amount of cerebrospinal fluid for testing in the laboratory. CSF analysis should include cell count and differential, glucose, protein, gram stain, and culture.
Diagnostic criteria require that opening pressure be measured in the lateral decubitus position with stretched legs, and without sedative medications. There is increasing consensus that there is no single absolute cut-off which is abnormal, but there is indication of a ’grey zone’ at which the lumbar puncture (spinal tap) opening pressure may suggestive for intracranial pressure (ICP) (between 25 cm H2O in adults and greater than 28cm H2O in children aged 1 to 18 years) 2, 3, 33, 11.
Blood tests
Blood tests may be performed to investigate for secondary causes of raised intracranial pressure (ICP) 88. Other medical conditions such as anemia, endocrine causes and vitamin A excess may present with symptoms similar to idiopathic intracranial hypertension 89, 90. In those patients who do not fit the typical phenotype for idiopathic intracranial hypertension (i.e. female, of childbearing age and who have a BMI greater than 30 kg/m²), a thorough drug history and exclusion of endocrine causes is required to exclude an underlying cause 33, 11.
Idiopathic intracranial hypertension treatment
The goal of idiopathic intracranial hypertension (IIH) treatment is to improve your symptoms and keep your eyesight from getting worse.
Idiopathic intracranial hypertension treatment can include:
- Losing weight if you’re overweight. If you’re obese, your doctor might recommend a low-sodium weight-loss diet to help improve your symptoms. You might work with a dietitian to help with your weight-loss goals. Some people benefit from weight-loss programs or weight-loss surgery. This can often help to reduce your symptoms and may sometimes relieve them altogether.
- Stopping any medicine that may be causing your symptoms
- Medicine to remove excess fluid from your body such as diuretics or water pills
- Medicine to reduce the production of cerebrospinal fluid in your brain
- A short course of steroid medicine to relieve headaches and reduce the risk of vision loss
- Regular lumbar punctures to remove excess fluid from your spine and help reduce the pressure on your brain.
Weight Loss
Obesity is associated with idiopathic intracranial hypertension and individuals with idiopathic intracranial hypertension who have a body mass index (BMI) greater than 40 kg/m² are at higher risk for vision loss, making weight loss critical in the treatment of idiopathic intracranial hypertension. Weight loss has been shown to be an effective method for improving headache symptoms, papilloedema and reducing intracranial pressure (ICP) 49. Sustaining weight loss is difficult, with patients on average regaining one-third to one-half of the weight that was lost at 1 year and returning to their original weight within 5 years 91. For idiopathic intracranial hypertension, a weight gain of 6% has led to documented recurrences 41.
Weight loss surgery (bariatric surgery) is the most effective method for sustained weight loss, resulting in 15–30% weight loss over 15–20 years depending on the surgical procedure 92. Gastric bypass (Roux-en-Y) surgery has been shown to be an effective method for reducing weight for idiopathic intracranial hypertension and can result in reduction or resolution of papilloedema, headache and tinnitus, with a concomitant reduction in intracranial pressure (ICP) 48. In addition, there is a decrease in circulating leptin, glucose, insulin and IGF-1, and an increase in adrenocorticotropic hormone (ACTH), following gastric bypass surgery 93. Gastric sleeve surgery has also been reported to be useful in idiopathic intracranial hypertension 94, leading to sufficient weight loss and resolution of papilloedema. Bariatric surgery is currently being investigated in the Idiopathic Intracranial Hypertension Weight Trial, a randomized controlled trial assessing bariatric surgery against a community weight-loss programme95.
Idiopathic intracranial hypertension diet
To lose weight, most people need to reduce the number of calories they get from food and beverages (Energy IN) and increase their physical activity (Energy OUT).
For a weight loss of 1 to 1.5 pounds per week, daily intake should be reduced by 500 to 750 calories. In general:
- Eating plans that contain 1,200–1,500 calories each day will help most women lose weight safely.
- Eating plans that contain 1,500–1,800 calories each day are suitable for men and for women who weigh more or who exercise regularly.
Very low calorie diets of fewer than 800 calories per day should not be used unless you are being monitored by your doctor.
After a low calorie diet, women with idiopathic intracranial hypertension had significantly reduced intracranial pressure, headaches, and papilloedema 49.
Healthy eating emphasizes fruits, vegetables, whole grains, dairy, and protein. Dairy recommendations include low-fat or fat-free milk, lactose-free milk, and fortified soy beverages. Other plant-based beverages do not have the same nutritional properties as animal’s milk and soy beverages. Protein recommendations include seafood, lean meats and poultry, eggs, legumes (beans, peas, and lentils), soy products, nuts, and seeds.
According to the Dietary Guidelines for Americans 2020–2025 (https://www.dietaryguidelines.gov), a healthy diet:
- Emphasizes fruits, vegetables, whole grains, and fat-free or low-fat milk and milk products
- Includes a variety of protein foods such as seafood, lean meats and poultry, eggs, legumes (beans and peas), soy products, nuts, and seeds.
- Is low in added sugars, sodium, saturated fats, trans fats, and cholesterol.
- Is rich in fiber. Fiber helps maintain digestive health and helps us feel fuller longer. Fiber also helps control blood sugar and lowers cholesterol levels. Fresh fruits and vegetables, whole grains, legumes, nuts, and seeds are good sources of fiber.
- Stays within your daily calorie needs
USDA’s MyPlate Plan (https://www.myplate.gov/myplate-plan) can help you identify what and how much to eat from the different food groups while staying within your recommended calorie allowance.
Fruit
Fresh, frozen, or canned fruits are great choices. Try fruits beyond apples and bananas such as mango, pineapple or kiwi fruit. When fresh fruit is not in season, try a frozen, canned, or dried variety. Be aware that dried and canned fruit may contain added sugars or syrups. Choose canned varieties of fruit packed in water or in its own juice.
Vegetables
Add variety to grilled or steamed vegetables with an herb such as rosemary. You can also sauté (panfry) vegetables in a non-stick pan with a small amount of cooking spray. Or try frozen or canned vegetables for a quick side dish—just microwave and serve. Look for canned vegetables without added salt, butter, or cream sauces. For variety, try a new vegetable each week.
Calcium and vitamin D rich foods
Calcium and vitamin D work together to promote optimal bone health. Our bodies can make vitamin D from sunshine, but some individuals may have difficulty producing enough vitamin D, and too much sun exposure can increase the risk of skin cancer. While very few foods naturally contain vitamin D, several foods and beverages are fortified with this essential nutrient.
To increase calcium and vitamin D intake, try this:
- Drink a fortified dairy beverage with your meals.
- When you pack your lunch, include a packet of salmon or can of sardines once a week. Salmon and sardines with bones has more calcium than salmon and sardines without bones.
Include spinach, collard greens, bok choy, mushrooms, and taro root in your vegetable dishes. - Look for foods that are fortified with calcium and vitamin D. Soy beverages, soy yogurt, orange juice, and some whole-grain cereals may have these added nutrients. Just be sure they do not include added sugars.
Meats
If your favorite recipe calls for frying fish or breaded chicken, try healthier variations by baking or grilling. Maybe even try dry beans in place of meats. Ask friends and search the internet and magazines for recipes with fewer calories ― you might be surprised to find you have a new favorite dish.
Limit added sugars
Too much added sugar in your diet can contribute to weight gain, obesity, type 2 diabetes, and heart disease. Some foods such as fruit and milk contain natural sugars. Added sugars are sugars and syrups that are added to foods and drinks when they are processed or prepared. Added sugars have many different names, such as cane juice, corn syrup, dextrose, and fructose. Table sugar, maple syrup, and honey are also considered added sugars. Sugary drinks are a common source of added sugars.
To limit added sugars, try this:
- Drink water instead of sugary drinks. Add berries or slices of lime, lemon, or cucumber for more flavor.
- Add fruit to your cereal or yogurt for sweetness.
- Don’t stock up on sugary drinks and snacks. Instead, drink water and keep fruit and vegetable slices handy for snacks.
- At coffee shops, skip the flavored syrups and whipped cream. Ask for low-fat or fat-free milk or an unsweetened, fortified soy beverage. Or get back to basics with black coffee.
- Read nutrition labels and choose foods with no or lower amounts of added sugars.
Replace saturated fats
Replacing saturated fat with healthier unsaturated fats can help protect your heart. Common sources of saturated fat are fatty meats such as beef ribs and sausage, whole milk, full-fat cheese, butter, and cream cheese.
To replace saturated fats with unsaturated fats, try this:
- Replace whole milk in a smoothie with low-fat yogurt and an avocado.
- Sprinkle nuts or seeds on salads instead of cheese.
- Use beans or seafood instead of meats as a source of protein.
- Cook with canola, corn, olive, peanut, safflower, soybean, or sunflower oil instead of butter or margarine.
- Replace full-fat milk and cheese with low-fat or fat-free versions.
Cut back on salt or sodium
Eating too much sodium can raise your risk of high blood pressure, heart attack, and stroke. More than 70% of the sodium Americans consume comes from packaged and prepared foods. While sodium has many forms, 90% of the sodium we consume is from salt.
To cut back on sodium, try this:
- Instead of using salt, add flavor to your meals with a squeeze of lemon juice, a dash of no-salt spice blends, or fresh herbs.
- Eat high-sodium processed and prepackaged food less frequently. Many common foods, including breads, pizza, and deli meats, have high amounts of sodium.
- At the grocery store, read the Nutrition Facts label to find low-sodium products.
- Buy unprocessed food, such as fresh or frozen vegetables, to prepare at home without salt.
Comfort foods
You can still enjoy your favorite foods, even if they are high in calories, fat or added sugars. The key is eating them only once in a while.
Some general tips for comfort foods:
- Eat them less often. If you normally eat these foods every day, cut back to once a week or once a month.
- Eat smaller amounts. If your favorite higher-calorie food is a chocolate bar, have a smaller size or only half a bar.
- Try a lower-calorie version. Use lower-calorie ingredients or prepare food differently. For example, if your macaroni and cheese recipe includes whole milk, butter, and full-fat cheese, try remaking it with non-fat milk, less butter, low-fat cheese, fresh spinach and tomatoes. Just remember to not increase your portion size.
Idiopathic intracranial hypertension medications
- Glaucoma drugs. One of the first drugs usually tried is acetazolamide (a carbonic anhydrase inhibitor), a glaucoma drug. Acetazolamide might reduce the production of cerebrospinal fluid and reduce symptoms. Acetazolamide can be started at 500 mg twice a day and increased by 250 mg weekly to a maximum dose of 4 g daily. If papilledema resolves, use a maintenance dose lower than 4 g daily. Because acetazolamide acts both at the choroid plexus and systemically, it is commonly associated with side effects. Possible side effects of acetazolamide include stomach upset, fatigue, tingling of fingers, toes and mouth, and kidney stones. In the clinical trial for acetazolamide, tingling of fingers (paresthesias) occurred in 47.7% of participants, 30.2% had nausea, and kidney stones occurred 32. Metabolic acidosis was apparent in laboratory studies for 10.5%, but this is usually well tolerated and does not require monitoring. Although acetazolamide provided statistically significant improvements in perimetry, papilledema grade, and quality-of-life scores, there was no significant difference in headache disability or visual acuity scores vs placebo. Overall, acetazolamide was well tolerated with less than 10% of participants discontinuing the study due to adverse effects 32. Acetazolamide has also been found to reduce the expression of aquaporin-1 96.
- Diuretics (furosemide, chlorthalidone). If acetazolamide alone isn’t effective, it’s sometimes combined with another diuretic (water pill), which reduces fluid retention by increasing urine output. Furosemide, a loop diuretic, also inhibits carbonic anhydrase. Data is limited on furosemide,which has primarily been studied in conjunction with acetazolamide. In a small pediatric case series, there was rapid improvement in intracranial pressure (ICP) when individuals with idiopathic intracranial hypertension were treated with acetazolamide and furosemide 31, 97. Although there is no evidence to support use of furosemide alone in the treatment of idiopathic intracranial hypertension, furosemide and other diuretics may be viable options for people who are unable to tolerate acetazolamide or for combination therapy 31.
- Migraine medications. These drugs can sometimes ease the severe headaches that often accompany idiopathic intracranial hypertension (IIH). Topiramate is an evidence-based medication for the preventive treatment of migraine that is a weak inhibitor of carbonic anhydrase and often used in the treatment of idiopathic intracranial hypertension. A small, randomized clinical trial showed that topiramate doses of up to 150 mg daily were comparable to acetazolamide doses up to 1500 mg daily for improvement in visual field loss. Papilledema grades, as well as headache severity, also improved over time with topiramate or acetazolamide and weight loss was comparable with either treatment.15 In the clinical trial of acetazolamide, 50% of participants had a history of migraine and 68% had headache that met criteria for definite or probable migraine during the trial.16 This suggests topiramate can be effective at reducing ICP and at treating comorbid migraine. Although weight loss associated with topiramate and its correlation with the symptoms of idiopathic intracranial hypertension has not been studied, it can be speculated that this may be another mechanism for lowering ICP and reducing headache. In practice, starting Topiramate at 25 mg once daily and titrating up to 100 mg twice daily is typically well tolerated and effective.
- Octreotide. Octreotide a somatostatin analogue, has been shown to reduce ICP and improve headache 31. In a small case series of individuals who had tried and failed multiple medical and surgical therapies, octreotide eliminated headache as a symptom of idiopathic intracranial hypertension. This case series did not include papilledema, vision loss, or ICP measurements as endpoints 98.
- Steroids. Steroids can rapidly lower ICP. Caution recommended as these can cause weight gain and rebound elevated ICP when tapered off. Steroid therapy should only be in cases with severe vision loss or in cases refractory to other medical treatments 83.
Idiopathic intracranial hypertension surgery
Surgery may be considered if other treatments do not help, particularly if your vision is getting worse or you’re at risk of loss of vision.
The main types of surgery for idiopathic intracranial hypertension are:
- Optic nerve sheath fenestration – In this procedure, a surgeon cuts a window into the membrane that surrounds the optic nerve (the nerve connecting the eye to the brain) to relieve pressure on it and allow excess cerebrospinal fluid to escape. Vision stabilizes or improves in most cases. Most people who have this procedure done on one eye notice a benefit for both eyes. However, this surgery isn’t always successful and can increase vision problems.
- Spinal fluid shunt – In this procedure, a surgeon inserts a thin, flexible tube (shunt) into the fluid-filled space in your brain or lower spine to divert excess fluid to another part of your body. The tubing is burrowed under your skin to your abdomen, where the shunt releases the excess fluid. A shunt is generally considered only if other treatments haven’t relieved your condition. Shunts can clog and often require other surgeries to keep them working. Complications can include low-pressure headaches and infections.
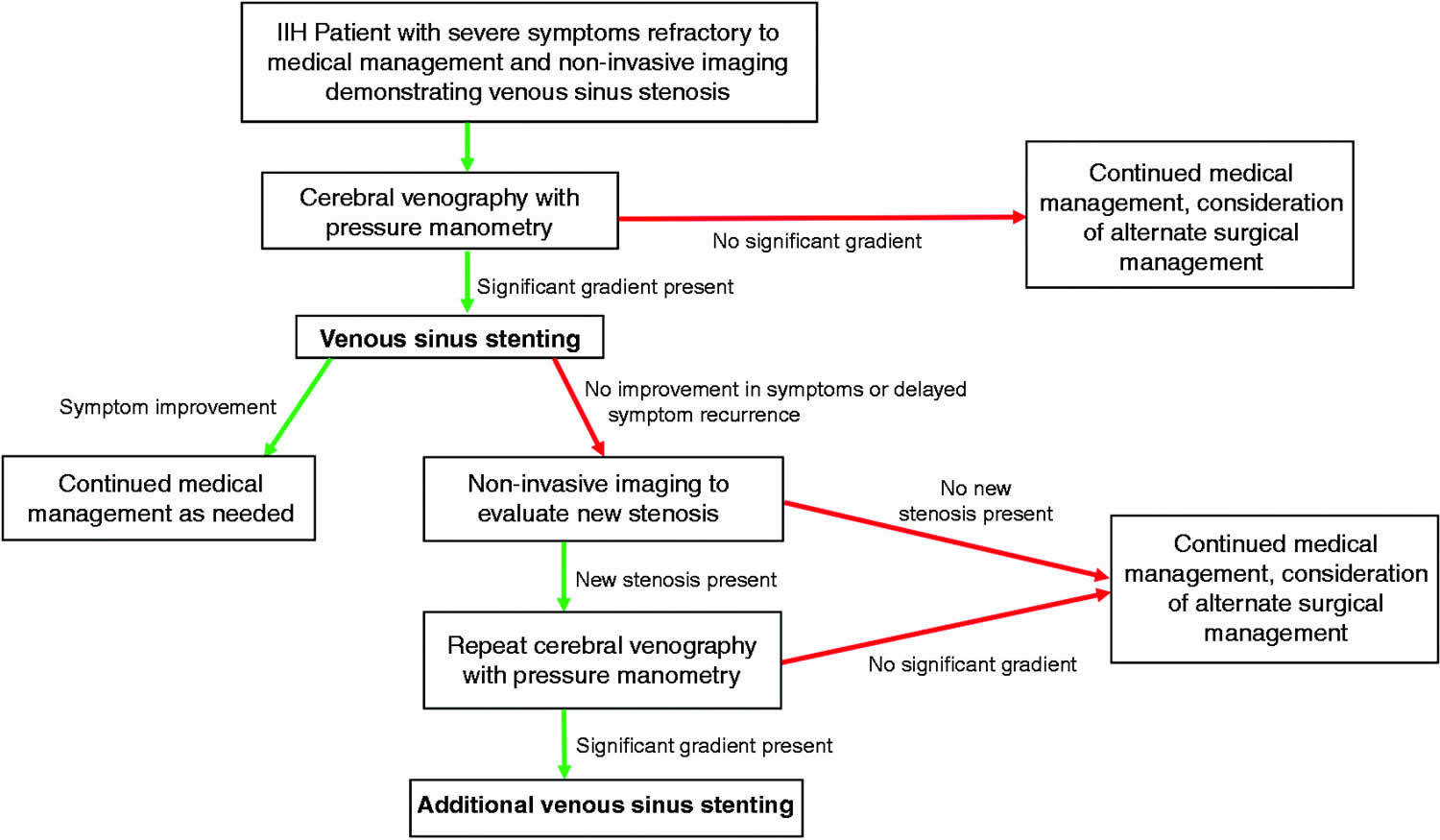
- Venous sinus stenting. This relatively new procedure is rarely used. It involves placing a stent in one of the larger veins in the head to increase the blood’s ability to flow. More study is needed to determine the benefits and risks of this procedure.
These procedures can provide relief from your symptoms, but they also carry a risk of potentially serious complications. Talk to your surgeon about what your operation involves and what the risks are.
Idiopathic intracranial hypertension prognosis
Idiopathic intracranial hypertension prognosis is variable. Idiopathic intracranial hypertension prognosis depends on several factors including:
- The rapidity of onset of symptoms: a more rapid onset requires more aggressive treatment
- Amount of vision loss at presentation: significant loss at the time of presentation suggests a higher risk of permanent vision loss 99
- The grade of papilledema at presentation: higher grades suggest a greater risk of permanent vision 100
Idiopathic intracranial hypertension (IIH) sometimes disappears on its own within 6 months. Symptoms can return in some people. It is not uncommon for this condition to cause symptoms for from months to years even with prompt treatment. Some patients will have continued papilledema, increased intracranial pressure (ICP), and even residual visual field deficits 101. A small number of people have symptoms that slowly get worse and lead to blindness 83.
Once you’ve had idiopathic intracranial hypertension (IIH), you’ll need to have your vision checked regularly to monitor changes and prevent blindness. Imaging the fundus (e.g. color fundus photography) is useful for longitudinal assessment. Optical coherence tomography (OCT) is increasingly being utilised to objectively monitor changes in the retinal nerve fibre layer and the optic nerve head disc volume to track papilloedema. Weight loss through lifestyle and behavioral modification may resolve papilloedema and/or loss of retinal nerve fibres.
- Sharma S, Hashmi MF, Kumar A. Intracranial Hypertension. [Updated 2023 May 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK507811[↩][↩][↩]
- Phillips PH, Sheldon CA. Pediatric Pseudotumor Cerebri Syndrome. J Neuroophthalmol. 2017 Sep;37 Suppl 1:S33-S40. doi: 10.1097/WNO.0000000000000548[↩][↩]
- Portelli M, Papageorgiou PN. An update on idiopathic intracranial hypertension. Acta Neurochir (Wien). 2017 Mar;159(3):491-499. doi: 10.1007/s00701-016-3050-7[↩][↩]
- Huff T, Tadi P, Varacallo M. Neuroanatomy, Cerebrospinal Fluid. [Updated 2019 May 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470578[↩]
- Javed K, Lui F. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): Feb 18, 2019. Neuroanatomy, Choroid Plexus.[↩]
- O’Reilly MW, Westgate CS, Hornby C, Botfield H, Taylor AE, Markey K, Mitchell JL, Scotton WJ, Mollan SP, Yiangou A, Jenkinson C, Gilligan LC, Sherlock M, Gibney J, Tomlinson JW, Lavery GG, Hodson DJ, Arlt W, Sinclair AJ. A unique androgen excess signature in idiopathic intracranial hypertension is linked to cerebrospinal fluid dynamics. JCI Insight. 2019 Mar 21;4(6):e125348. doi: 10.1172/jci.insight.125348[↩][↩][↩]
- Zanon E, Pasca S. Intracranial haemorrhage in children and adults with haemophilia A and B: a literature review of the last 20 years. Blood Transfus. 2019 Sep;17(5):378-384. doi: 10.2450/2019.0253-18[↩]
- Mondragon J, Klovenski V. Pseudotumor Cerebri. [Updated 2022 Sep 29]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK536924[↩][↩]
- Stevens SM, McClelland CM, Chen JJ, Lee MS. Idiopathic Intracranial Hypertension in a Mother and Pre-pubertal Twins. Neuroophthalmology. 2018 Jun 26;43(1):49-52. doi: 10.1080/01658107.2018.1480047[↩]
- Fargen KM, Coffman S, Torosian T, Brinjikji W, Nye BL, Hui F. “Idiopathic” intracranial hypertension: An update from neurointerventional research for clinicians. Cephalalgia. 2023;43(4). doi:10.1177/03331024231161323[↩][↩][↩]
- Hoffmann J, Mollan SP, Paemeleire K, Lampl C, Jensen RH, Sinclair AJ. European headache federation guideline on idiopathic intracranial hypertension. J Headache Pain. 2018 Oct 8;19(1):93. doi: 10.1186/s10194-018-0919-2[↩][↩][↩][↩][↩]
- Mollan SP, Ali F, Hassan-Smith G, Botfield H, Friedman DI, Sinclair AJ. Evolving evidence in adult idiopathic intracranial hypertension: pathophysiology and management. J Neurol Neurosurg Psychiatry. 2016 Sep;87(9):982-92. doi: 10.1136/jnnp-2015-311302[↩][↩][↩][↩]
- Idiopathic Intracranial Hypertension. https://practicalneurology.com/articles/2020-may/idiopathic-intracranial-hypertension[↩][↩]
- Dandy WE. Intracranial Pressure Without Brain Tumor: Diagnosis and Treatment. Ann Surg 1937;106(4):492–513. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1390605/pdf/annsurg00527-0013.pdf[↩]
- Friedman DI, Jacobson DM. Diagnostic criteria for idiopathic intracranial hypertension. Neurology. 2002 Nov 26;59(10):1492-5. doi: 10.1212/01.wnl.0000029570.69134.1b[↩]
- Smith JL. Whence pseudotumor cerebri? J Clin Neuroophthalmol. 1985 Mar;5(1):55-6.[↩]
- Mollan SP, Davies B, Silver NC, et al.. Idiopathic intracranial hypertension: consensus guidelines on management. J Neurol Neurosurg Psychiatry 2018;89:1088–100. 10.1136/jnnp-2017-317440[↩]
- Markey KA, Mollan SP, Jensen RH, et al.. Understanding idiopathic intracranial hypertension: mechanisms, management, and future directions. Lancet Neurol 2016;15:78–91. 10.1016/S1474-4422(15)00298-7[↩][↩]
- Friedman DI, Liu GT, Digre KB. Revised diagnostic criteria for the pseudotumor cerebri syndrome in adults and children. Neurology 2013;81:1159–65. 10.1212/WNL.0b013e3182a55f17[↩][↩]
- Idiopathic intracranial hypertension. https://medlineplus.gov/ency/article/000351.htm[↩][↩]
- Kilgore KP, Lee MS, Leavitt JA, et al.. Re-evaluating the incidence of idiopathic intracranial hypertension in an era of increasing obesity. Ophthalmology 2017;124:697–700. 10.1016/j.ophtha.2017.01.006[↩]
- Headache Classification Committee of the International Headache Society (IHS). The international classification of headache disorders, 3rd edition (beta version). Cephalalgia 2013;33:629–808. 10.1177/0333102413485658[↩]
- Degnan AJ, Levy LM. Pseudotumor cerebri: brief review of clinical syndrome and imaging findings. AJNR Am J Neuroradiol. 2011 Dec;32(11):1986-93. doi: 10.3174/ajnr.A2404[↩]
- Yri HM, Jensen RH. Idiopathic intracranial hypertension: clinical nosography and field-testing of the ICHD diagnostic criteria. A case-control study. Cephalalgia 2015;35:553–62. 10.1177/0333102414550109[↩]
- Suzuki H, Takanashi J, Kobayashi K, Nagasawa K, Tashima K, Kohno Y. MR imaging of idiopathic intracranial hypertension. AJNR Am J Neuroradiol. 2001 Jan;22(1):196-9. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7975547[↩]
- Lyons HS, Mollan SLP, Liu GT, Bowman R, Thaller M, Sinclair AJ, Mollan SP. Different Characteristics of Pre-Pubertal and Post-Pubertal Idiopathic Intracranial Hypertension: A Narrative Review. Neuroophthalmology. 2022 Dec 15;47(2):63-74. doi: 10.1080/01658107.2022.2153874[↩]
- Virdee J, Larcombe S, Vijay V, Sinclair AJ, Dayan M, Mollan SP. Reviewing the Recent Developments in Idiopathic Intracranial Hypertension. Ophthalmol Ther. 2020 Dec;9(4):767-781. doi: 10.1007/s40123-020-00296-0[↩][↩]
- Wall M, Kupersmith MJ, Kieburtz KD, Corbett JJ, Feldon SE, Friedman DI, Katz DM, Keltner JL, Schron EB, McDermott MP; NORDIC Idiopathic Intracranial Hypertension Study Group. The idiopathic intracranial hypertension treatment trial: clinical profile at baseline. JAMA Neurol. 2014 Jun;71(6):693-701. doi: 10.1001/jamaneurol.2014.133[↩][↩][↩]
- Lueck CJ, McClelland C. Is Positioning During Lumbar Puncture Clinically Significant? J Neuroophthalmol. 2019 Jun;39(2):268-272. doi: 10.1097/WNO.0000000000000696[↩]
- Johnston I, Paterson A. Benign intracranial hypertension. II. CSF pressure and circulation. Brain. 1974 Jun;97(2):301-12. doi: 10.1093/brain/97.1.301[↩]
- Friedman DI. Contemporary management of the pseudotumor cerebri syndrome. Expert Rev Neurother. 2019 Sep;19(9):881-893. doi: 10.1080/14737175.2019.1660163[↩][↩][↩][↩]
- NORDIC Idiopathic Intracranial Hypertension Study Group Writing Committee; Wall M, McDermott MP, Kieburtz KD, Corbett JJ, Feldon SE, Friedman DI, Katz DM, Keltner JL, Schron EB, Kupersmith MJ. Effect of acetazolamide on visual function in patients with idiopathic intracranial hypertension and mild visual loss: the idiopathic intracranial hypertension treatment trial. JAMA. 2014 Apr 23-30;311(16):1641-51. doi: 10.1001/jama.2014.3312[↩][↩][↩][↩]
- Mollan SP, Davies B, Silver NC, Shaw S, Mallucci CL, Wakerley BR, Krishnan A, Chavda SV, Ramalingam S, Edwards J, Hemmings K, Williamson M, Burdon MA, Hassan-Smith G, Digre K, Liu GT, Jensen RH, Sinclair AJ. Idiopathic intracranial hypertension: consensus guidelines on management. J Neurol Neurosurg Psychiatry. 2018 Oct;89(10):1088-1100. doi: 10.1136/jnnp-2017-317440[↩][↩][↩][↩][↩]
- Idiopathic intracranial hypertension. https://radiopaedia.org/cases/idiopathic-intracranial-hypertension-44[↩]
- Friedman DI. Novel.utah.edu Walsh and Hoyt Text, Chapter 5 : Miller N, Newman NJ, Walsh and Hoyt’s Clinical Neuro-Ophthalmology. 5 th edn Baltimore, MD: Williams & Wilkins Ed, 1998:237–91.[↩]
- Sodhi M, Sheldon CA, Carleton B, et al.. Oral fluoroquinolones and risk of secondary pseudotumor cerebri syndrome: nested case-control study. Neurology 2017;89:792–5. 10.1212/WNL.0000000000004247[↩]
- Markey KA, Mollan SP, Jensen RH, Sinclair AJ. Understanding idiopathic intracranial hypertension: mechanisms, management, and future directions. Lancet Neurol. 2016 Jan;15(1):78-91. doi: 10.1016/S1474-4422(15)00298-7[↩][↩]
- Hornby C, Mollan SP, Botfield H, OʼReilly MW, Sinclair AJ. Metabolic Concepts in Idiopathic Intracranial Hypertension and Their Potential for Therapeutic Intervention. J Neuroophthalmol. 2018 Dec;38(4):522-530. doi: 10.1097/WNO.0000000000000684[↩][↩][↩]
- Adderley NJ, Subramanian A, Nirantharakumar K, Yiangou A, Gokhale KM, Mollan SP, Sinclair AJ. Association Between Idiopathic Intracranial Hypertension and Risk of Cardiovascular Diseases in Women in the United Kingdom. JAMA Neurol. 2019 Sep 1;76(9):1088-1098. doi: 10.1001/jamaneurol.2019.1812[↩][↩]
- Andrews LE, Liu GT, Ko MW. Idiopathic intracranial hypertension and obesity. Horm Res Paediatr. 2014;81(4):217-25. doi: 10.1159/000357730[↩]
- Ko MW, Chang SC, Ridha MA, Ney JJ, Ali TF, Friedman DI, Mejico LJ, Volpe NJ, Galetta SL, Balcer LJ, Liu GT. Weight gain and recurrence in idiopathic intracranial hypertension: a case-control study. Neurology. 2011 May 3;76(18):1564-7. doi: 10.1212/WNL.0b013e3182190f51[↩][↩][↩][↩]
- McCluskey G, Doherty-Allan R, McCarron P, Loftus AM, McCarron LV, Mulholland D, McVerry F, McCarron MO. Meta-analysis and systematic review of population-based epidemiological studies in idiopathic intracranial hypertension. Eur J Neurol. 2018 Oct;25(10):1218-1227. doi: 10.1111/ene.13739[↩][↩]
- Obesity and overweight. https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight[↩]
- Mollan SP, Aguiar M, Evison F, Frew E, Sinclair AJ. The expanding burden of idiopathic intracranial hypertension. Eye (Lond). 2019 Mar;33(3):478-485. doi: 10.1038/s41433-018-0238-5[↩]
- Almarzouqi SJ, Morgan ML, Lee AG. Idiopathic intracranial hypertension in the Middle East: A growing concern. Saudi J Ophthalmol. 2015 Jan-Mar;29(1):26-31. doi: 10.1016/j.sjopt.2014.09.013[↩]
- Daniels AB, Liu GT, Volpe NJ, Galetta SL, Moster ML, Newman NJ, Biousse V, Lee AG, Wall M, Kardon R, Acierno MD, Corbett JJ, Maguire MG, Balcer LJ. Profiles of obesity, weight gain, and quality of life in idiopathic intracranial hypertension (pseudotumor cerebri). Am J Ophthalmol. 2007 Apr;143(4):635-41. doi: 10.1016/j.ajo.2006.12.040[↩][↩]
- Newborg B. Pseudotumor Cerebri Treated: by Rice-Reduction Diet. Arch Intern Med. 1974;133(5):802–807. doi:10.1001/archinte.1974.00320170084007[↩]
- Sugerman HJ, Felton WL 3rd, Salvant JB Jr, Sismanis A, Kellum JM. Effects of surgically induced weight loss on idiopathic intracranial hypertension in morbid obesity. Neurology. 1995 Sep;45(9):1655-9. doi: 10.1212/wnl.45.9.1655[↩][↩]
- Sinclair AJ, Burdon MA, Nightingale PG, Ball AK, Good P, Matthews TD, Jacks A, Lawden M, Clarke CE, Stewart PM, Walker EA, Tomlinson JW, Rauz S. Low energy diet and intracranial pressure in women with idiopathic intracranial hypertension: prospective cohort study. BMJ. 2010 Jul 7;341:c2701. doi: 10.1136/bmj.c2701[↩][↩][↩][↩]
- Hornby C, Botfield H, O’Reilly MW, Westgate C, Mitchell J, Mollan SP, Manolopoulos K, Tomlinson J, Sinclair A. Evaluating the Fat Distribution in Idiopathic Intracranial Hypertension Using Dual-Energy X-ray Absorptiometry Scanning. Neuroophthalmology. 2017 Jun 20;42(2):99-104. doi: 10.1080/01658107.2017.1334218[↩]
- Subramaniam S, Fletcher WA. Obesity and Weight Loss in Idiopathic Intracranial Hypertension: A Narrative Review. J Neuroophthalmol. 2017 Jun;37(2):197-205. doi: 10.1097/WNO.0000000000000448[↩]
- Speake T, Whitwell C, Kajita H, Majid A, Brown PD. Mechanisms of CSF secretion by the choroid plexus. Microsc Res Tech. 2001 Jan 1;52(1):49-59. doi: 10.1002/1097-0029(20010101)52:1<49::AID-JEMT7>3.0.CO;2-C[↩]
- Brown PD, Davies SL, Speake T, Millar ID. Molecular mechanisms of cerebrospinal fluid production. Neuroscience. 2004;129(4):957-70. doi: 10.1016/j.neuroscience.2004.07.003[↩]
- Pollay M, Hisey B, Reynolds E, Tomkins P, Stevens FA, Smith R. Choroid plexus Na+/K+-activated adenosine triphosphatase and cerebrospinal fluid formation. Neurosurgery. 1985 Nov;17(5):768-72. doi: 10.1227/00006123-198511000-00007[↩]
- Kerty E, Heuser K, Indahl UG, Berg PR, Nakken S, Lien S, Omholt SW, Ottersen OP, Nagelhus EA. Is the brain water channel aquaporin-4 a pathogenetic factor in idiopathic intracranial hypertension? Results from a combined clinical and genetic study in a Norwegian cohort. Acta Ophthalmol. 2013 Feb;91(1):88-91. doi: 10.1111/j.1755-3768.2011.02231.x[↩]
- Stiebel-Kalish H, Eyal S, Steiner I. The role of aquaporin-1 in idiopathic and drug-induced intracranial hypertension. Med Hypotheses. 2013 Dec;81(6):1059-62. doi: 10.1016/j.mehy.2013.10.002[↩]
- Uldall M, Bhatt DK, Kruuse C, Juhler M, Jansen-Olesen I, Jensen RH. Choroid plexus aquaporin 1 and intracranial pressure are increased in obese rats: towards an idiopathic intracranial hypertension model? Int J Obes (Lond). 2017 Jul;41(7):1141-1147. doi: 10.1038/ijo.2017.83[↩]
- Killer HE, Jaggi GP, Miller NR, Huber AR, Landolt H, Mironov A, Meyer P, Remonda L. Cerebrospinal fluid dynamics between the basal cisterns and the subarachnoid space of the optic nerve in patients with papilloedema. Br J Ophthalmol. 2011 Jun;95(6):822-7. doi: 10.1136/bjo.2010.189324[↩]
- Sussman J, Leach M, Greaves M, Malia R, Davies-Jones GA. Potentially prothrombotic abnormalities of coagulation in benign intracranial hypertension. J Neurol Neurosurg Psychiatry. 1997 Mar;62(3):229-33. doi: 10.1136/jnnp.62.3.229[↩]
- Botfield HF, Uldall MS, Westgate CSJ, Mitchell JL, Hagen SM, Gonzalez AM, Hodson DJ, Jensen RH, Sinclair AJ. A glucagon-like peptide-1 receptor agonist reduces intracranial pressure in a rat model of hydrocephalus. Sci Transl Med. 2017 Aug 23;9(404):eaan0972. doi: 10.1126/scitranslmed.aan0972[↩][↩]
- Sinclair AJ, Onyimba CU, Khosla P, Vijapurapu N, Tomlinson JW, Burdon MA, Stewart PM, Murray PI, Walker EA, Rauz S. Corticosteroids, 11beta-hydroxysteroid dehydrogenase isozymes and the rabbit choroid plexus. J Neuroendocrinol. 2007 Aug;19(8):614-20. doi: 10.1111/j.1365-2826.2007.01569.x[↩]
- Sinclair AJ, Walker EA, Burdon MA, van Beek AP, Kema IP, Hughes BA, Murray PI, Nightingale PG, Stewart PM, Rauz S, Tomlinson JW. Cerebrospinal fluid corticosteroid levels and cortisol metabolism in patients with idiopathic intracranial hypertension: a link between 11beta-HSD1 and intracranial pressure regulation? J Clin Endocrinol Metab. 2010 Dec;95(12):5348-56. doi: 10.1210/jc.2010-0729[↩]
- Markey KA, Ottridge R, Mitchell JL, Rick C, Woolley R, Ives N, Nightingale P, Sinclair AJ. Assessing the Efficacy and Safety of an 11β-Hydroxysteroid Dehydrogenase Type 1 Inhibitor (AZD4017) in the Idiopathic Intracranial Hypertension Drug Trial, IIH:DT: Clinical Methods and Design for a Phase II Randomized Controlled Trial. JMIR Res Protoc. 2017 Sep 18;6(9):e181. doi: 10.2196/resprot.7806[↩]
- Hornby C, Mollan SP, Mitchell J, Markey KA, Yangou A, Wright BLC, O’Reilly MW, Sinclair AJ. What Do Transgender Patients Teach Us About Idiopathic Intracranial Hypertension? Neuroophthalmology. 2017 May 10;41(6):326-329. doi: 10.1080/01658107.2017.1316744[↩]
- Zhang Y, Scarpace PJ. The role of leptin in leptin resistance and obesity. Physiol Behav. 2006 Jun 30;88(3):249-56. doi: 10.1016/j.physbeh.2006.05.038[↩]
- Lampl Y, Eshel Y, Kessler A, Fux A, Gilad R, Boaz M, Matas Z, Sadeh M. Serum leptin level in women with idiopathic intracranial hypertension. J Neurol Neurosurg Psychiatry. 2002 May;72(5):642-3. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1737898/pdf/v072p00642.pdf[↩]
- Ball AK, Sinclair AJ, Curnow SJ, Tomlinson JW, Burdon MA, Walker EA, Stewart PM, Nightingale PG, Clarke CE, Rauz S. Elevated cerebrospinal fluid (CSF) leptin in idiopathic intracranial hypertension (IIH): evidence for hypothalamic leptin resistance? Clin Endocrinol (Oxf). 2009 Jun;70(6):863-9. doi: 10.1111/j.1365-2265.2008.03401.x[↩]
- Van Harmelen V, Reynisdottir S, Eriksson P, Thörne A, Hoffstedt J, Lönnqvist F, Arner P. Leptin secretion from subcutaneous and visceral adipose tissue in women. Diabetes. 1998 Jun;47(6):913-7. doi: 10.2337/diabetes.47.6.913[↩]
- West JL, Greeneway GP, Garner RM, Aschenbrenner CA, Singh J, Wolfe SQ, Fargen KM. Correlation between angiographic stenosis and physiologic venous sinus outflow obstruction in idiopathic intracranial hypertension. J Neurointerv Surg. 2019 Jan;11(1):90-94. doi: 10.1136/neurintsurg-2018-014004[↩]
- Riggeal BD, Bruce BB, Saindane AM, Ridha MA, Kelly LP, Newman NJ, Biousse V. Clinical course of idiopathic intracranial hypertension with transverse sinus stenosis. Neurology. 2013 Jan 15;80(3):289-95. doi: 10.1212/WNL.0b013e31827debd6[↩][↩]
- Bidot S, Saindane AM, Peragallo JH, Bruce BB, Newman NJ, Biousse V. Brain Imaging in Idiopathic Intracranial Hypertension. J Neuroophthalmol. 2015 Dec;35(4):400-11. doi: 10.1097/WNO.0000000000000303[↩]
- King JO, Mitchell PJ, Thomson KR, Tress BM. Manometry combined with cervical puncture in idiopathic intracranial hypertension. Neurology. 2002 Jan 8;58(1):26-30. doi: 10.1212/wnl.58.1.26[↩]
- Saber H, Lewis W, Sadeghi M, Rajah G, Narayanan S. Stent Survival and Stent-Adjacent Stenosis Rates following Venous Sinus Stenting for Idiopathic Intracranial Hypertension: A Systematic Review and Meta-Analysis. Interv Neurol. 2018 Oct;7(6):490-500. doi: 10.1159/000490578[↩]
- Mollan SP, Spitzer D, Nicholl DJ. Raised intracranial pressure in those presenting with headache. BMJ. 2018 Oct 4;363:k3252. doi: 10.1136/bmj.k3252[↩]
- Mollan SP, Hoffmann J, Sinclair AJ. Advances in the understanding of headache in idiopathic intracranial hypertension. Curr Opin Neurol. 2019 Feb;32(1):92-98. doi: 10.1097/WCO.0000000000000651[↩]
- Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd edition. Cephalalgia. 2018 Jan;38(1):1-211. doi: 10.1177/0333102417738202[↩]
- Yri HM, Fagerlund B, Forchhammer HB, Jensen RH. Cognitive function in idiopathic intracranial hypertension: a prospective case-control study. BMJ Open. 2014 Apr 8;4(4):e004376. doi: 10.1136/bmjopen-2013-004376[↩]
- Idiopathic intracranial hypertension (mnemonic). https://radiopaedia.org/articles/idiopathic-intracranial-hypertension-mnemonic?lang=us[↩]
- Wall M, Corbett JJ. Revised diagnostic criteria for the pseudotumor cerebri syndrome in adults and children. Neurology. 2014 Jul 8;83(2):198-9. doi: 10.1212/01.wnl.0000452039.32455.3e[↩]
- Fisayo A, Bruce BB, Newman NJ, Biousse V. Overdiagnosis of idiopathic intracranial hypertension. Neurology. 2016 Jan 26;86(4):341-50. doi: 10.1212/WNL.0000000000002318[↩]
- Marzoli SB, Ciasca P, Curone M, Cammarata G, Melzi L, Criscuoli A, Bussone G, D’Amico D. Quantitative analysis of optic nerve damage in idiopathic intracranial hypertension (IIH) at diagnosis. Neurol Sci. 2013 May;34 Suppl 1:S143-5. doi: 10.1007/s10072-013-1373-1[↩]
- Aojula A, Mollan SP, Horsburgh J, Yiangou A, Markey KA, Mitchell JL, Scotton WJ, Keane PA, Sinclair AJ. Segmentation error in spectral domain optical coherence tomography measures of the retinal nerve fibre layer thickness in idiopathic intracranial hypertension. BMC Ophthalmol. 2018 Jan 4;17(1):257. doi: 10.1186/s12886-017-0652-7[↩]
- Friedman DI. The pseudotumor cerebri syndrome. Neurol Clin. 2014 May;32(2):363-96. doi: 10.1016/j.ncl.2014.01.001[↩][↩][↩]
- McGeeney BE, Friedman DI. Pseudotumor cerebri pathophysiology. Headache. 2014 Mar;54(3):445-58. doi: 10.1111/head.12291[↩]
- Hoffmann J, Huppertz HJ, Schmidt C, Kunte H, Harms L, Klingebiel R, Wiener E. Morphometric and volumetric MRI changes in idiopathic intracranial hypertension. Cephalalgia. 2013 Oct;33(13):1075-84. doi: 10.1177/0333102413484095[↩]
- Wall M. Idiopathic intracranial hypertension. Neurol Clin. 2010 Aug;28(3):593-617. doi: 10.1016/j.ncl.2010.03.003[↩]
- Friedman DI, Liu GT, Digre KB. Revised diagnostic criteria for the pseudotumor cerebri syndrome in adults and children. Neurology. 2013 Sep 24;81(13):1159-65. doi: 10.1212/WNL.0b013e3182a55f17[↩]
- Biousse V, Rucker JC, Vignal C, Crassard I, Katz BJ, Newman NJ. Anemia and papilledema. Am J Ophthalmol. 2003 Apr;135(4):437-46. doi: 10.1016/s0002-9394(02)02062-7[↩]
- Mollan SP, Ball AK, Sinclair AJ, Madill SA, Clarke CE, Jacks AS, Burdon MA, Matthews TD. Idiopathic intracranial hypertension associated with iron deficiency anaemia: a lesson for management. Eur Neurol. 2009;62(2):105-8. doi: 10.1159/000222781[↩]
- Benzimra JD, Simon S, Sinclair AJ, Mollan SP. Sight-threatening pseudotumour cerebri associated with excess vitamin A supplementation. Pract Neurol. 2015 Feb;15(1):72-3. doi: 10.1136/practneurol-2014-000934[↩]
- Middleton KM, Patidar SM, Perri MG. The impact of extended care on the long-term maintenance of weight loss: a systematic review and meta-analysis. Obes Rev. 2012 Jun;13(6):509-17. doi: 10.1111/j.1467-789X.2011.00972.x[↩]
- Sjöström L. Review of the key results from the Swedish Obese Subjects (SOS) trial – a prospective controlled intervention study of bariatric surgery. J Intern Med. 2013 Mar;273(3):219-34. doi: 10.1111/joim.12012[↩]
- Rubino F, Gagner M, Gentileschi P, Kini S, Fukuyama S, Feng J, Diamond E. The early effect of the Roux-en-Y gastric bypass on hormones involved in body weight regulation and glucose metabolism. Ann Surg. 2004 Aug;240(2):236-42. doi: 10.1097/01.sla.0000133117.12646.48[↩]
- Abdelbaki TN, Gomaa M. Outcome of idiopathic intracranial hypertension after laparoscopic sleeve gastrectomy. Surg Obes Relat Dis. 2020 Sep;16(9):1195-1201. doi: 10.1016/j.soard.2020.03.032[↩]
- Ottridge R, Mollan SP, Botfield H, Frew E, Ives NJ, Matthews T, Mitchell J, Rick C, Singhal R, Woolley R, Sinclair AJ. Randomised controlled trial of bariatric surgery versus a community weight loss programme for the sustained treatment of idiopathic intracranial hypertension: the Idiopathic Intracranial Hypertension Weight Trial (IIH:WT) protocol. BMJ Open. 2017 Sep 27;7(9):e017426. doi: 10.1136/bmjopen-2017-017426[↩]
- Libien J, Kupersmith MJ, Blaner W, McDermott MP, Gao S, Liu Y, Corbett J, Wall M; NORDIC Idiopathic Intracranial Hypertension Study Group. Role of vitamin A metabolism in IIH: Results from the idiopathic intracranial hypertension treatment trial. J Neurol Sci. 2017 Jan 15;372:78-84. doi: 10.1016/j.jns.2016.11.014[↩]
- Schoeman JF. Childhood pseudotumor cerebri: clinical and intracranial pressure response to acetazolamide and furosemide treatment in a case series. J Child Neurol. 1994 Apr;9(2):130-4. doi: 10.1177/088307389400900205[↩]
- House PM, Stodieck SR. Octreotide: The IIH therapy beyond weight loss, carbonic anhydrase inhibitors, lumbar punctures and surgical/interventional treatments. Clin Neurol Neurosurg. 2016 Nov;150:181-184. doi: 10.1016/j.clineuro.2016.09.016[↩]
- Acheson JF. Idiopathic intracranial hypertension and visual function. Br Med Bull. 2006;79-80:233-44. doi: 10.1093/bmb/ldl019[↩]
- Maturi RK, Folk JC. Human T-Cell Lymphotrophic Virus Antibody in Phakic Cystoid Macular Edema. Arch Ophthalmol. 1999;117(11):1571.[↩]
- Salman MS, Kirkham FJ, MacGregor DL. Idiopathic “benign” intracranial hypertension: case series and review. J Child Neurol. 2001 Jul;16(7):465-70. doi: 10.1177/088307380101600701[↩]


{kind=link}