Contents
- Guillain Barre syndrome
- Types of Guillain-Barre syndrome
- Guillain-Barre syndrome signs and symptoms
- Guillain-Barre syndrome complications
- Guillain-Barre syndrome causes
- Guillain-Barre syndrome pathophysiology
- Guillain-Barre syndrome diagnosis
- Guillain-Barre syndrome differential diagnosis
- Guillain-Barre syndrome treatment
- Guillain-Barre syndrome prognosis
Guillain Barre syndrome
Guillain-Barre syndrome also called acute inflammatory demyelinating polyneuropathy (AIDP) or Landry’s ascending paralysis, is an umbrella term describing a heterogeneous group of rare autoimmune neurological disorders including Miller Fisher syndrome (MFS) and Guillain–Barré syndrome (GBS) subtypes, where your immune system attacks your nerves with resultant weakness and diminished reflexes 1, 2, 3. Guillain–Barré Syndrome (GBS) is defined as an inflammatory ascending polyradiculoneuropathy 4. This damage is called demyelination. It causes nerve signals to move more slowly. Damage to other parts of the nerve can cause the nerve to stop working. About five per cent of Miller Fisher syndrome patients develop weakness during disease course, indicating that Miller Fisher syndrome (MFS) and Guillain–Barré syndrome (GBS) form a continuum 5. Guillain-Barré syndrome initially causes weakness and tingling (pins and needles) in your hands and feet. These symptoms can quickly progress up your body and become more severe, paralyzing your whole body. There may be weakness of the face muscles, of the muscles that enable a person to swallow, or of the muscles in charge of moving the eyes. Breathing muscles may be involved, and 10-30% of patients with Guillain-Barré syndrome will need a ventilator to breathe. Blood pressure or heart rate can vary from high to low, often unexpectedly, and the patient may not be able to empty their bladder or may be constipated. Pain associated with Guillain-Barre syndrome is most severe in the shoulder girdle, back, buttocks, and thighs and may occur with even the slightest movements. The pain is often described as aching or throbbing in nature. In its most severe form of Guillain-Barre syndrome is a medical emergency.
Guillain-Barre syndrome progression can be rapid, and most patients with GBS reach their maximum disability within 2 weeks 6. About 20% of patients with Guillain-Barre syndrome develop respiratory failure and require mechanical ventilation. Cardiac arrhythmias and blood pressure instability can occur owing to involvement of the autonomic nervous system 7. This involvement of the autonomic nervous system contributes to mortality, which is estimated at 3–10% for patients with GBS even with the best medical care available 8, 9. After the initial progressive phase, patients with GBS reach a plateau phase that can last from days to weeks or months, after which they start to recover, and 60–80% of patients with GBS are able to walk independently 6 months after disease onset, with or without treatment 10, 11. Guillain-Barre syndrome is a monophasic illness, although some patients can deteriorate after first stabilizing or improving on therapy, a phenomenon that is referred to as a treatment-related fluctuation 6. Relapses of GBS can occur in 2–5% of patients 12, 10. In ~5% of patients with GBS, repeated clinical relapses suggest a more chronic disease process, and the diagnosis is changed to acute-onset chronic inflammatory demyelinating polyneuropathy (CIDP) 13. Acute-onset chronic inflammatory demyelinating polyneuropathy (CIDP) typically presents with three or more treatment-related fluctuations and/or clinical deterioration ≥8 weeks after disease onset 13.
The cause of Guillain-Barre syndrome is currently unknown. But two-thirds of patients report symptoms of an infection (viral or bacterial) in the six weeks preceding. These include the flu, respiratory or a gastrointestinal infection (food poisoning) or Zika virus. Guillain-Barre syndrome is also a rare reaction in those who receive the Johnson & Johnson or AstraZeneca COVID-19 vaccine 14, 4, 15, 16, 17, 18, 19, 20. In the past Guillain-Barre syndrome had been previously observed in individuals who received the meningococcal, tetanus-toxoid, human papillomavirus (HPV), and most prominently, the influenza vaccines 21, 22, 23, 24. Some theories suggest an autoimmune trigger, in which the patient’s defense system of antibodies and white blood cells are called into action against the body, damaging myelin (nerve covering or insulation), leading to numbness and weakness.
To confirm a Guillain-Barre syndrome diagnosis, two tests may be performed:
- A lumbar puncture looking for elevated fluid protein
- Electrical test of nerve and muscle function
Most people with Guillain-Barre syndrome must be hospitalized to receive treatment. Frequent evaluations of pulmonary function parameters should be performed at bedside to monitor respiratory status and the need for ventilatory assistance. Approximately one third of patients require admission to an intensive care unit (ICU), primarily because of respiratory failure, to be on a ventilator in to help you breathe.
At the present time there is no known cure for Guillain-Barre syndrome, but several treatments can ease symptoms and reduce the duration of the illness. Although most people recover completely from Guillain-Barre syndrome, some severe cases can be deadly. While recovery may take up to several years, most people are able to walk again six months after symptoms first started. Some people may have lasting effects from it, such as weakness, numbness or fatigue.
Recurrent episodes of GBS are rare, affecting 2–5% of patients, but this percentage is still higher than the lifetime risk of GBS in the general population (0.1%) 12, 25.
Figure 1. Diagnosis and management of Guillain–Barré syndrome
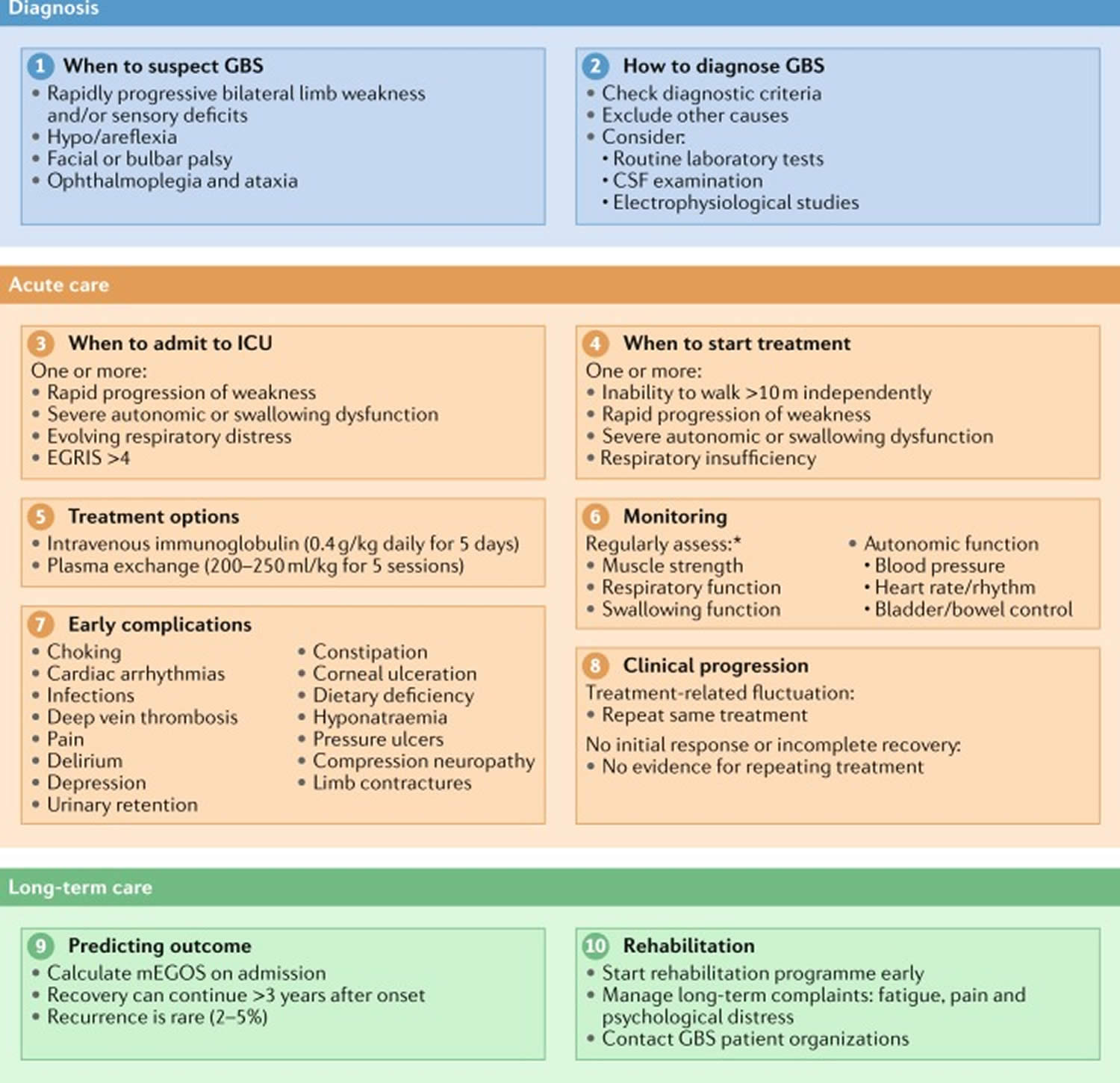
Footnote: This summary for the diagnosis and management of Guillain–Barré syndrome provides an overview of each of the ten steps described in the guideline. *Frequency of monitoring is dependent on the clinical picture and should be assessed in individual patients.
Abbreviations: CSF = cerebrospinal fluid; EGRIS = Erasmus GBS Respiratory Insufficiency Score; GBS = Guillain-Barré syndrome; ICU = intensive care unit; mEGOS = modified Erasmus GBS Outcome Score.
[Source 6 ]See your doctor if you have mild tingling in your toes or fingers that doesn’t seem to be spreading or getting worse. Seek emergency medical help if you have any of these severe signs or symptoms:
- Tingling that started in your feet or toes and is now moving up your body
- Tingling or weakness that’s spreading rapidly
- Difficulty catching your breath or shortness of breath when lying flat
- Choking on saliva
Guillain-Barre syndrome is a serious condition that requires immediate hospitalization because it can worsen rapidly. The sooner appropriate treatment is started, the better the chance of a good outcome.
How long will I have Guillain-Barre syndrome?
Most patients make a full recovery from Guillain-Barre syndrome. Even if you were paralyzed or needed a ventilator, you are likely to recover within the first year after symptoms started. Some people have symptoms for life. About 30 percent of those with Guillain-Barré have residual weakness after three years. About three percent may suffer a relapse of muscle weakness and tingling sensations many years after the initial attack. About 15 to 20 percent of individuals are left with long-term problems such as long-term weakness being unable to walk without assistance; some may require ongoing use of a walker, wheelchair, or ankle support. Muscle strength may not return uniformly. Ongoing fatigue, pain, numbness, balance and co-ordination problems and other tingling or burning sensation can sometimes be troublesome. You may face physical difficulties and emotionally painful periods. Therapies such as physiotherapy, occupational therapy and speech and language therapy (a speech and language therapist can help with both communication and swallowing difficulties) may help you recover and cope with any lasting difficulties.
In a minority of cases, Guillain-Barré syndrome can cause life-threatening problems such as severe breathing difficulties or blood clots. Overall, around 1 in 20 will die from Guillain-Barré syndrome.
Some people with GBS need psychological counseling to help them adapt. Support groups can often ease emotional strain and provide valuable information. The GBS/CIDP Foundation International (https://www.gbs-cidp.org/) — the international patient association for GBS — and other national organizations can help establish these networks.
Who is more likely to get Guillain-Barre syndrome?
Both adults and children (although it is more frequent in adults and older people) can develop Guillain-Barre syndrome, with people older than 50 are at greatest risk. Guillain-Barre syndrome can strike at any age and both sexes are equally prone to the disorder. GBS is estimated to affect about one person in 100,000 each year. It is not contagious or inherited. About two-thirds of people with GBS were sick with diarrhea or respiratory illness days or weeks before developing symptoms. Infection with the bacteria Campylobacter jejuni, which causes gastroenteritis (including symptoms of nausea, vomiting and diarrhea), is one of the most common risk factors for GBS. People also can develop GBS after having the flu or other infections such as cytomegalovirus and Epstein-Barr virus. On very rare occasions, people develop GBS in the days or weeks after getting a vaccination.
What is myelin?
Myelin is a lipid-rich (fatty) substance and the myelin membranes originate from and are a part of the Schwann cells in the peripheral nervous system and the glial cells called oligodendrocytes in the central nervous system (CNS). Myelin is an electrical insulator that insulates nerve cell axons to increase the speed at which information (encoded as an electrical signal) travels from one nerve cell body to another (as in the central nervous system) or from a nerve cell body to a muscle (as in the peripheral nervous system). The myelinated axon can be likened to an electrical wire (the axon) with insulating material (myelin) around it. However, unlike the plastic covering on an electrical wire, myelin does not form a single long sheath over the entire length of the axon. Rather, each myelin sheath insulates the axon over a single section and in general, each axon comprises multiple long myelinated sections separated from each other by short gaps called the nodes of Ranvier. Nodes of Ranvier are the short (~1 micron) unmyelinated regions of the axon between adjacent long (~0.2 mm – >1 mm) myelinated internodes 26. Each myelin sheath is formed by the concentric wrapping of an oligodendrocyte or Schwann cell process around the axon. Each myelin-generating cell (oligodendrocyte in the CNS or Schwann cell in the peripheral nervous system) furnishes myelin for only one segment of any given axon. The periodic interruptions where short portions of the axon are left uncovered by myelin, the nodes of Ranvier, are critical to the functioning of myelin.
In myelinated axons, the excitable axonal membrane is exposed to the extracellular space only at the nodes of Ranvier; this is the location of sodium channels 27. When the membrane at the node of Ranvier is excited, the local circuit generated cannot flow through the high-resistance sheath and, therefore, flows out through and depolarizes the membrane at the next node, which might be 1 mm or farther away. The low capacitance of the myelin sheath means that little energy is required to depolarize the remaining membrane between the nodes of Ranvier, which results in local circuit spreading at an increased speed. Active excitation of the axonal membrane jumps from node to node; this form of impulse propagation is called saltatory conduction (Latin saltare, “to jump”). This saltatory conduction whereby the action potential “jumps” from one node of Ranvier, over a long myelinated stretch of the axon called the internode, before ‘recharging’ at the next node of Ranvier, and so on, until it reaches the axon terminal. Once it reaches the axon terminal, this electrical signal provokes the release of a chemical message or neurotransmitter that binds to receptors on the adjacent post-synaptic cell (e.g. nerve cell in the CNS or muscle cell in the peripheral nervous system) at specialized regions called synapses.
Furthermore, such movement of the wave of depolarization is much more rapid in myelinated nerve fibers than in unmyelinated fibers, because only the nodes of Ranvier are excited during conduction in myelinated fibers, Na+ (sodium) flux into the nerve is much less than in unmyelinated fibers, where the entire membrane is involved. An example of the advantage of myelination is obtained by comparison of two different nerve fibers, both of which conduct at 25 m/sec at 20°C. The 500-mm diameter unmyelinated giant axon of the squid requires 5,000 times as much energy and occupies about 1,500 times as much space as the 12-mm diameter myelinated nerve in the frog.
In another word, myelin speeds the transmission of electrical impulses called action potentials along myelinated axons by insulating the axon and reducing axonal membrane capacitance. Conduction velocity in myelinated fibers is proportional to the diameter, while in unmyelinated fibers it is proportional to the square root of the diameter 28. Thus, differences in energy and space requirements between the two types of fiber are exaggerated at higher conduction velocities. If nerves were not myelinated and equivalent conduction velocities were maintained, the human spinal cord would need to be as large as a good-sized tree trunk. Myelin, then, facilitates conduction while conserving space and energy 29.
This “insulating” role for myelin is essential for normal motor function (i.e. movement such as walking), sensory function (e.g. hearing, seeing or feeling the sensation of pain) and cognition (e.g. acquiring and recalling knowledge), as demonstrated by the consequences of disorders that affect it, such as the genetically determined leukodystrophies 30, the acquired inflammatory demyelinating disorder, multiple sclerosis 31 and the inflammatory demyelinating peripheral neuropathies 32. Due to its high prevalence, multiple sclerosis, which specifically affects the central nervous system (brain, spinal cord and optic nerve), is the best known disorder of myelin.
Figure 2. Neuron with myelin sheath
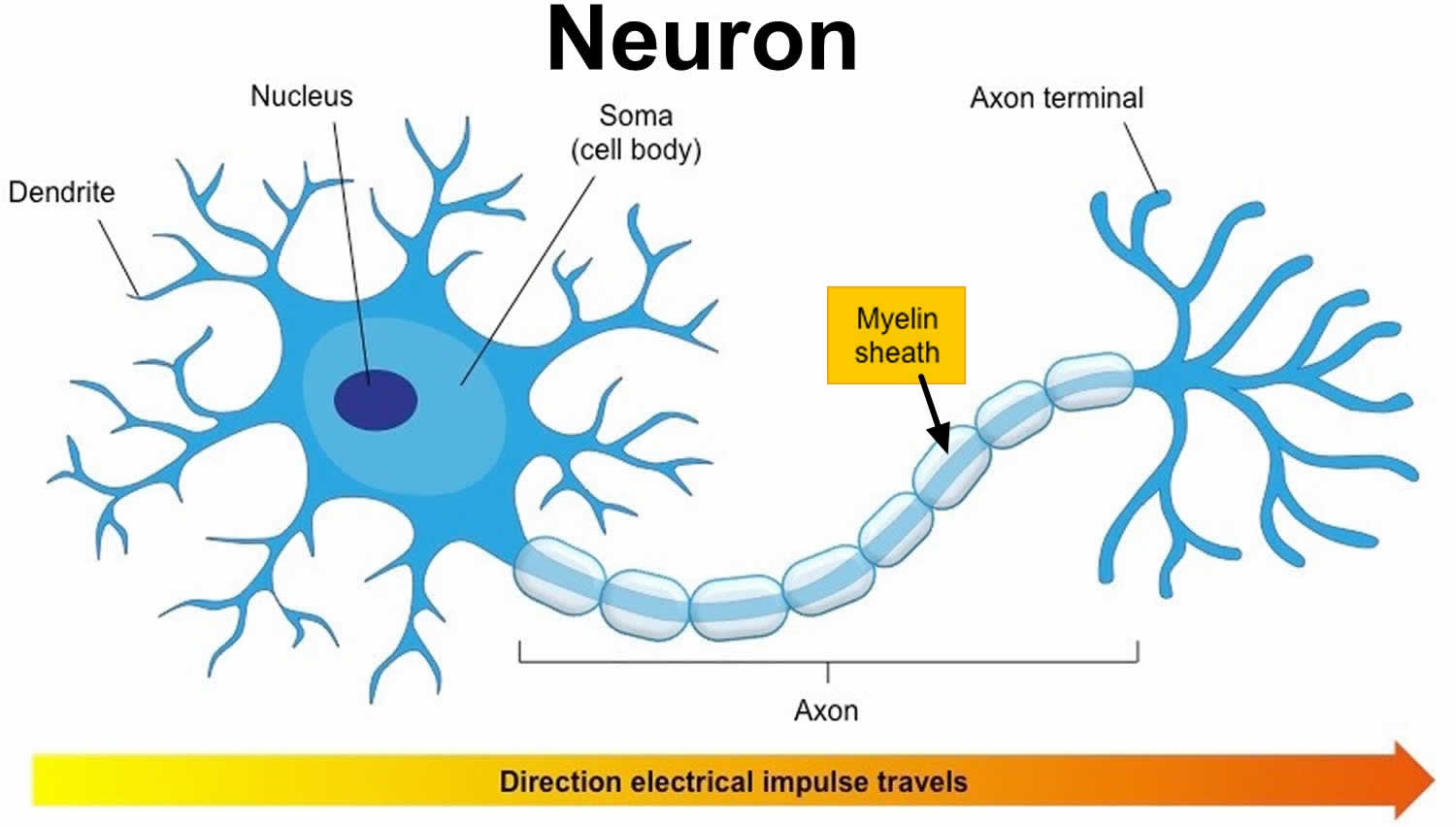
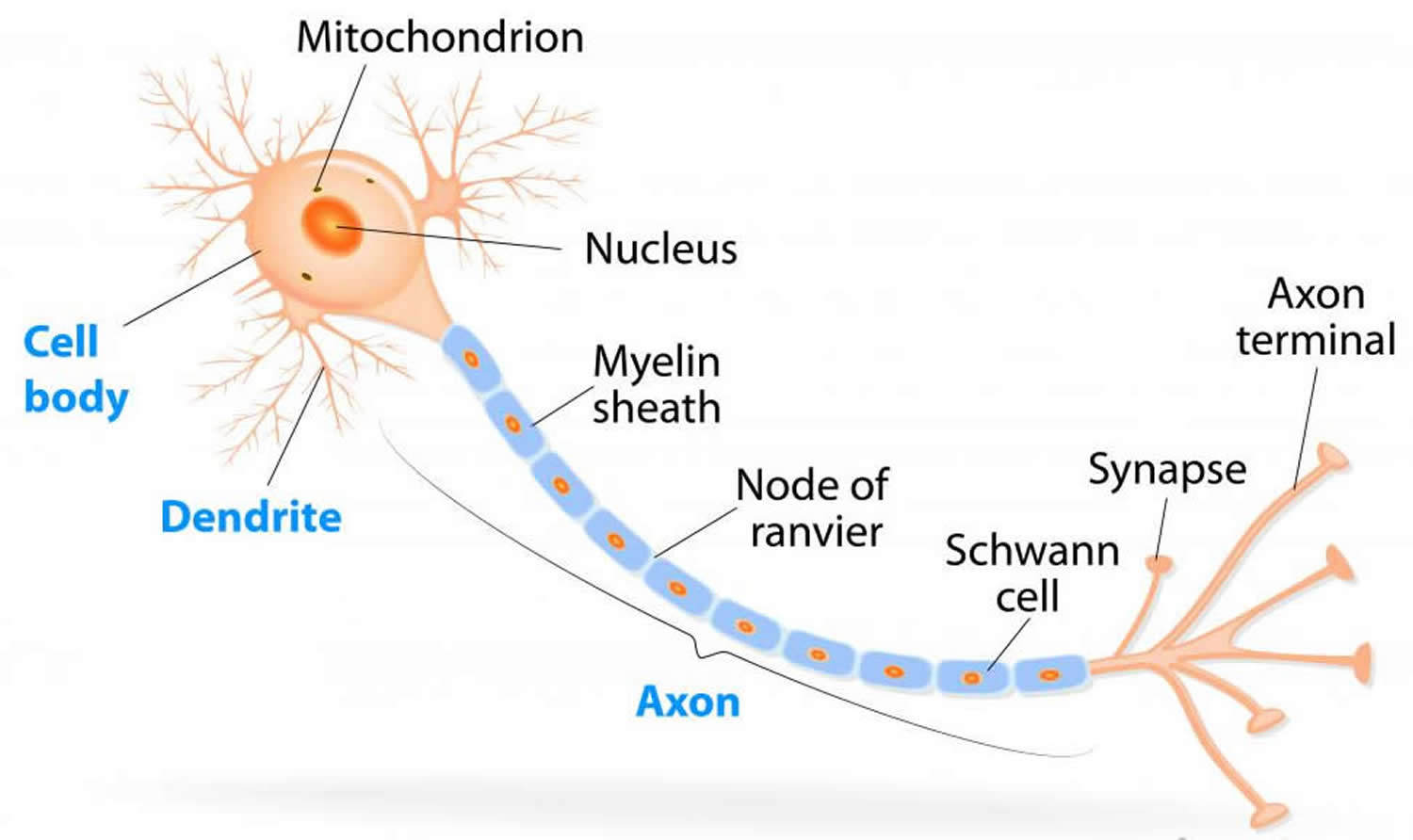
Figure 3. How electrical impulses travel down a neuron (myelinated and unmyelinated)
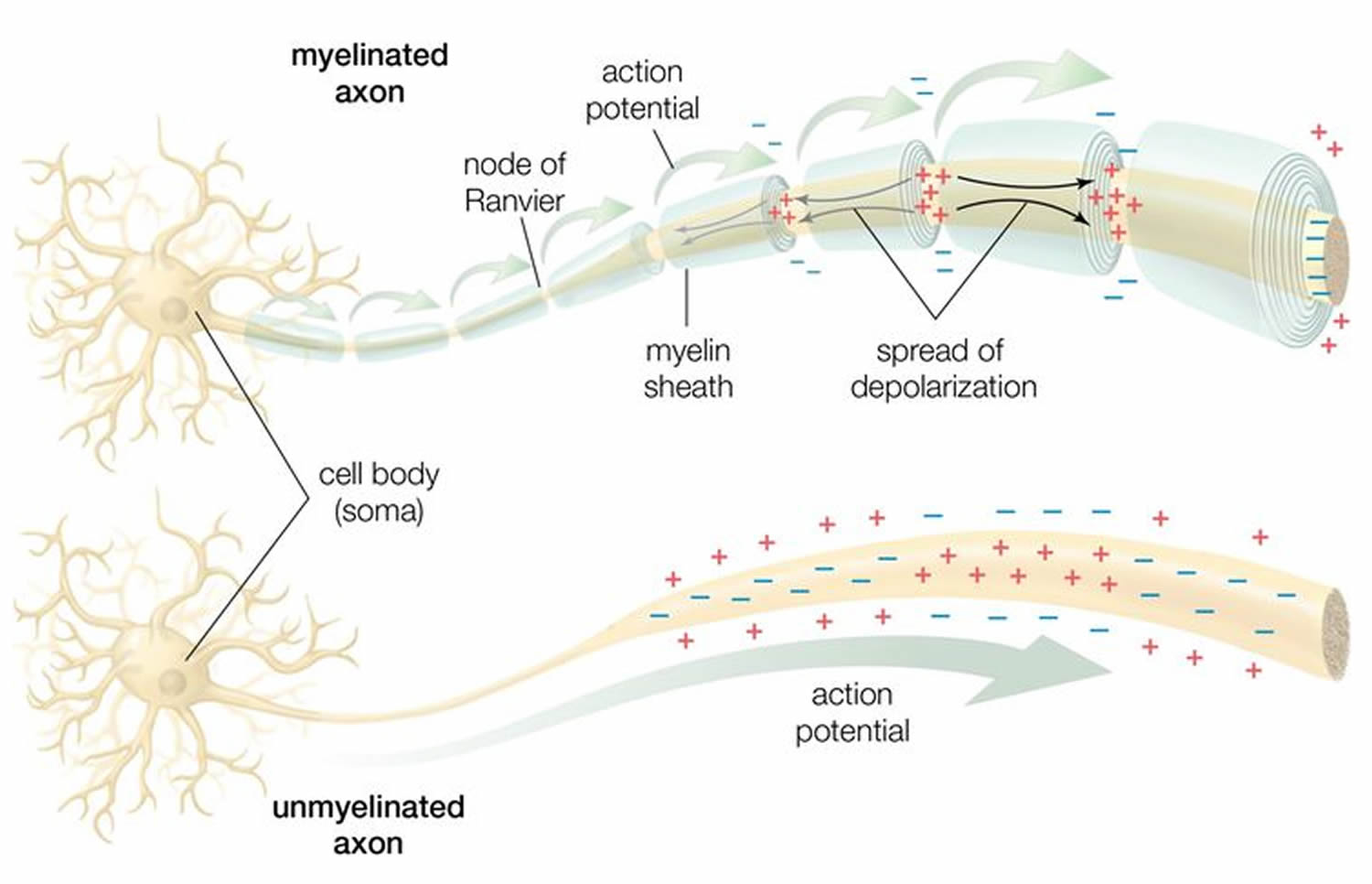
Figure 4. Formation of myelin sheath in the peripheral nervous system (PNS) – note that Schwann cell cytoplasm forms a ring both inside and outside of the myelin sheath.
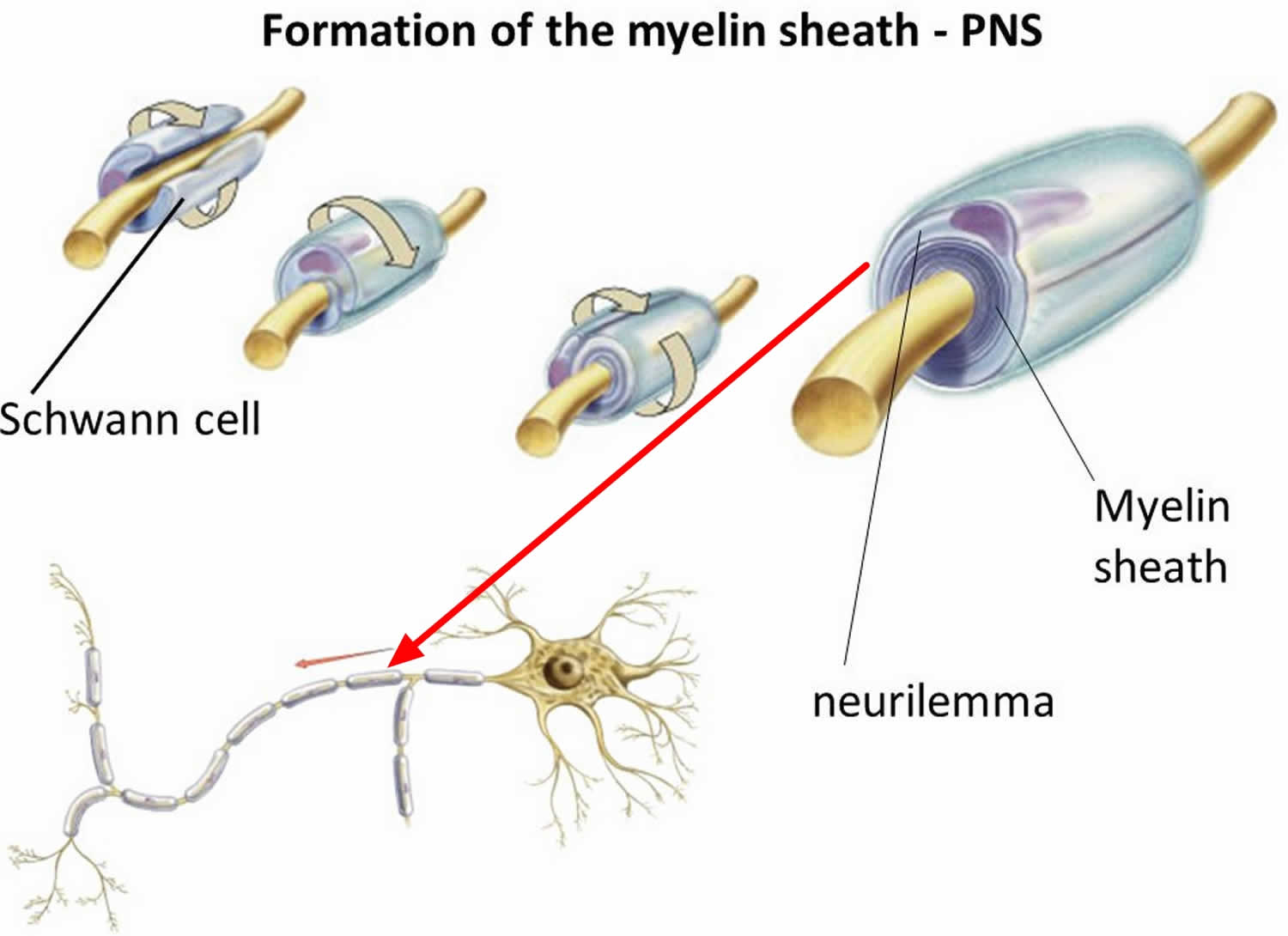
Figure 5. Myelin sheath (the Schwann cell has surrounded the nerve axon)
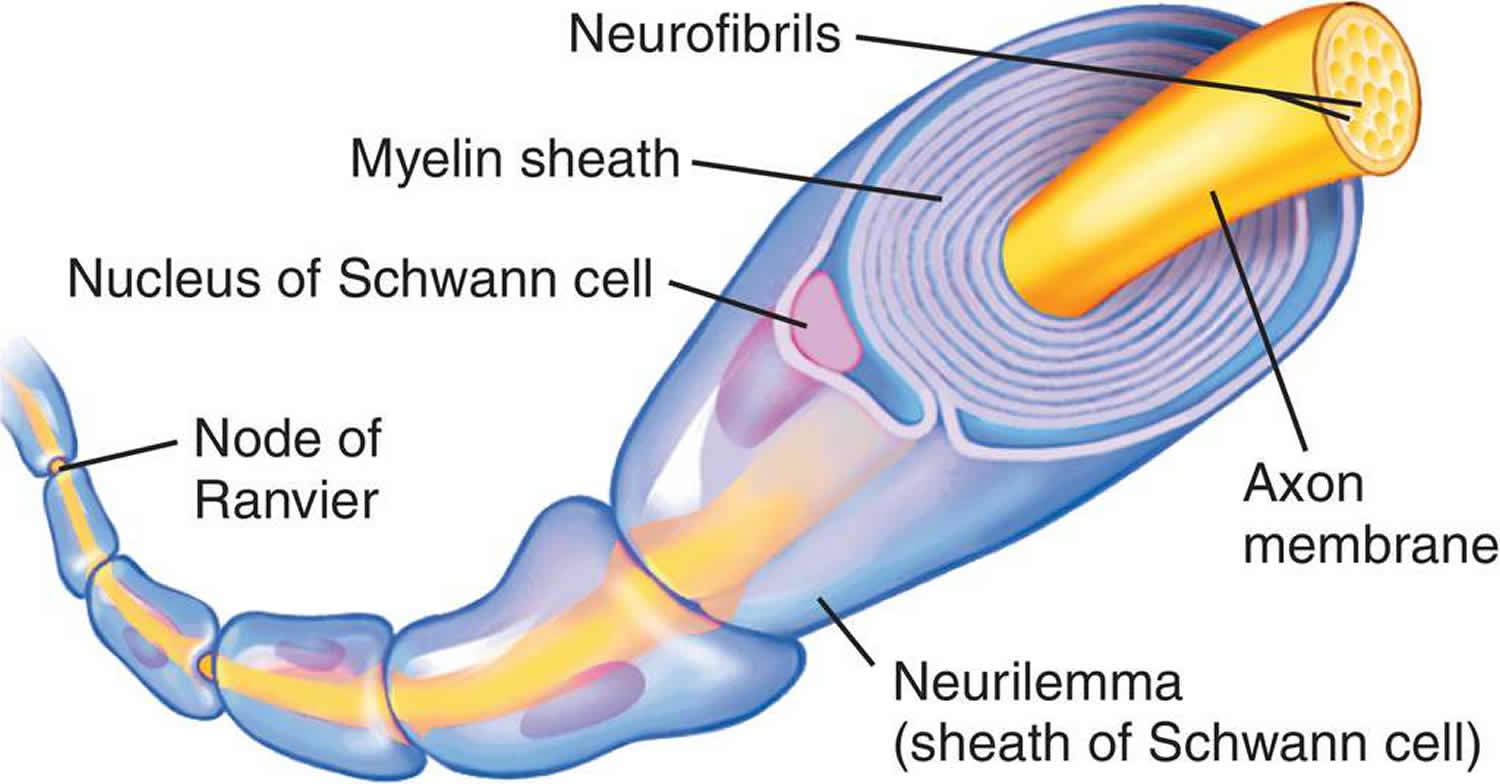
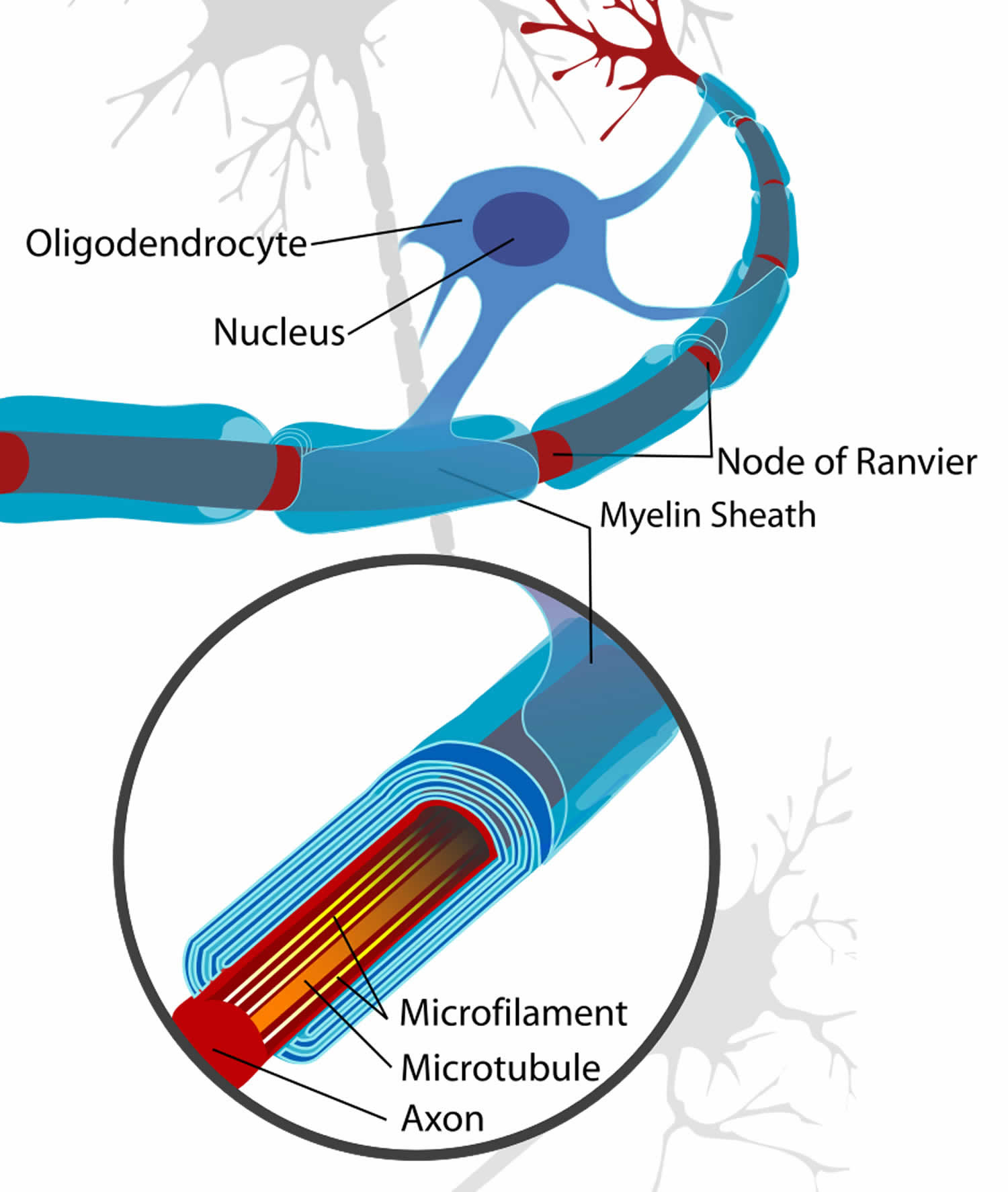
Figure 6. Formation of myelin sheath in the central nervous system (CNS)
Types of Guillain-Barre syndrome
Guillain-Barre syndrome has several forms. The main types are: Guillain–Barré syndrome and Miller Fisher syndrome, which have been subclassified into several subtypes, which together form a continuous spectrum of discrete and overlapping syndromes, affecting the cranial nerves and the limbs. Although neurophysiologically, Guillain–Barré syndrome-related disorders can be divided into axonal and demyelinating types; a classification based on clinical criteria is more useful 33.
Guillain–Barré syndrome subtypes 34:
- Acute inflammatory demyelinating polyradiculoneuropathy (AIDP), the most common Guillain-Barre syndrome type in North America and Europe. The most common sign of acute inflammatory demyelinating polyradiculoneuropathy (AIDP) is muscle weakness that starts in the lower part of your body and spreads upward.
- Miller Fisher syndrome (MFS), in which paralysis starts in the eyes (ophthalmoplegia) causing duble vision. Miller Fisher syndrome (MFS) is also associated with unsteady gait (ataxia) and absence of deep tendon reflexes (areflexia) 35, 36. Miller Fisher syndrome is less common in the U.S. but more common in Asia 37, 7.
- Acute Motor Axonal Neuropathy (AMAN) and Acute Motor-Sensory Axonal Neuropathy (AMSAN) are less common in the U.S. But acute motor axonal neuropathy (AMAN) and acute motor-sensory axonal neuropathy (AMSAN) are more frequent in China, Japan and Mexico. Acute Motor Axonal Neuropathy (AMAN) is similar to acute inflammatory demyelinating polyradiculoneuropathy (AIDP), but without sensory symptoms.
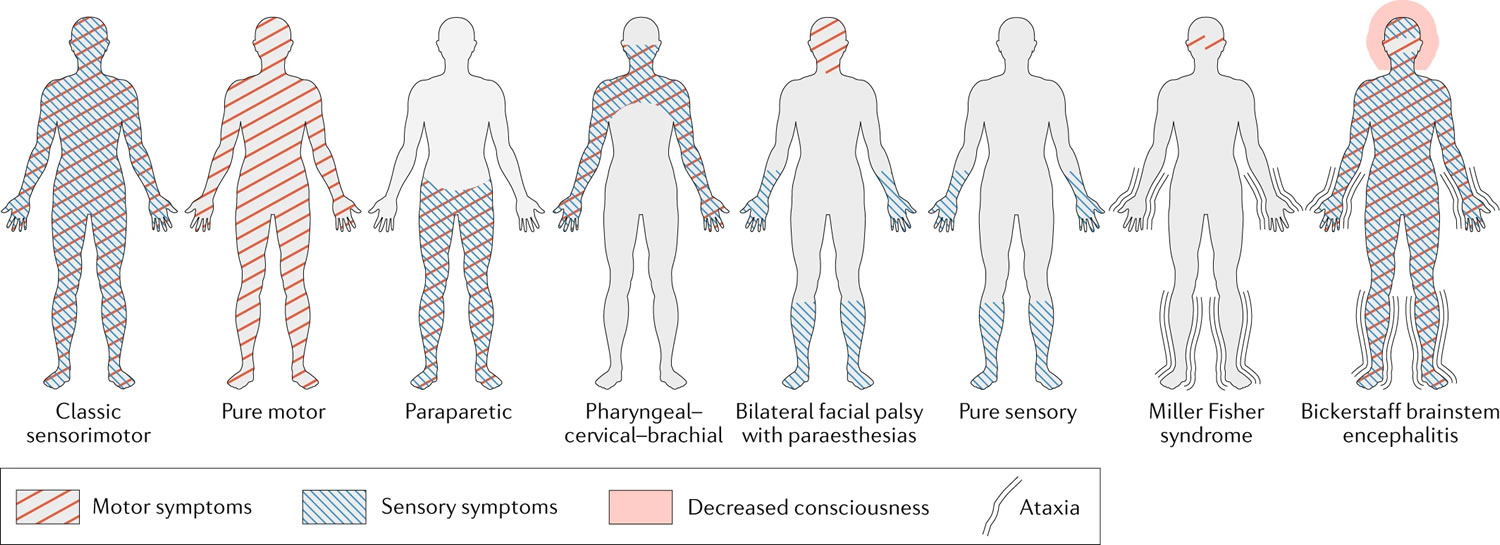
Some patients have a distinct and persistent clinical variant of GBS that does not progress to the classic pattern of sensory loss and weakness. These variants include: weakness without sensory signs (pure motor variant); weakness limited to the cranial nerves (bilateral facial palsy with paraesthesias), upper limbs (pharyngeal–cervical–brachial weakness) or lower limbs (paraparetic variant); and the Miller Fisher syndrome (MFS), which in its full manifestation consists of ophthalmoplegia, areflexia and ataxia (Figure 7 and Table 1) 1. In general, Guillain-Barre syndrome (GBS) variants are rarely ‘pure’ and often overlap in part with the classic syndrome or show features that are typical of other variant forms 38.
Besides the variants listed above, pure sensory ataxia, Bickerstaff brainstem encephalitis and a pure sensory variant are often included in the Guillain-Barre syndrome spectrum because they share clinical or pathophysiological features with GBS. However, the inclusion of these clinical variants is subject to debate as they do not fulfil the diagnostic criteria for Guillain-Barre syndrome 1. The pure sensory variant shares clinical features with the classic sensorimotor form of Guillain-Barre syndrome, with the exception of the presence of motor symptoms and signs 39, 1; pure sensory ataxia and Miller Fisher syndrome (MFS) have overlapping clinical profiles, and patients with Bickerstaff brainstem encephalitis usually present with symptoms resembling Miller Fisher syndrome (MFS) and subsequently develop signs of brainstem dysfunction, including impaired consciousness and pyramidal tract signs 40, 38. Similar to patients with Miller Fisher syndrome (MFS), individuals with sensory ataxia or Bickerstaff brainstem encephalitis can exhibit IgG antibodies to GQ1b or other gangliosides in their serum 41, 42. However, whether pure sensory GBS, pure sensory ataxia and Bickerstaff brainstem encephalitis are variants of GBS and/or an incomplete form of Miller Fisher syndrome (MFS) is subject to debate, and careful diagnostic work-up is required when these variants are suspected 1, 42, 39.
Table 1. Variants of Guillain–Barré syndrome
| Variant | Frequency (% of GBS cases) a | Clinical features | References |
|---|---|---|---|
| Classic sensorimotor Guillain–Barré syndrome b | 30–85 | Rapidly progressive symmetrical weakness and sensory signs with absent or reduced tendon reflexes, usually reaching nadir within 2 weeks | 43, 11, 44 |
| Pure motor c | 5–70 | Motor weakness without sensory signs | 11, 34 |
| Paraparetic | 5–10 | Paresis restricted to the legs | 10, 44 |
| Pharyngeal–cervical–brachial | <5 | Weakness of pharyngeal, cervical and brachial muscles without lower limb weakness | 43, 44, 10 |
| Bilateral facial palsy with paraesthesias d | <5 | Bilateral facial weakness, paraesthesias and reduced reflexes | 45, 43, 44 |
| Pure sensory | <1 | Acute or subacute sensory neuropathy without other deficits | 46, 47 |
| Miller Fisher syndrome | 5–25 | Ophthalmoplegia, ataxia and areflexia. Incomplete forms with isolated ataxia (acute ataxic neuropathy) or ophthalmoplegia (acute ophthalmoplegia) can occur 48. Overlaps with classical sensorimotor Guillain–Barré syndrome in an estimated 15% of patients | 11, 43, 44, 49 |
| Bickerstaff brainstem encephalitis d | <5 | Ophthalmoplegia, ataxia, areflexia, pyramidal tract signs and impaired consciousness, often overlapping with sensorimotor Guillain–Barré syndrome | 43, 44 |
Footnotes:
aEstimated frequencies, with percentages displayed to the nearest 5%, based on nine (primarily adult) cohort studies in various geographical regions. Frequencies differ by region and study, contributing to the variability. Most studies are biased owing to exclusion of some of the variants.
bThe sensorimotor form is seen in an estimated 70% of patients with GBS in Europe and the Americas, and in 30–40% of cases in Asia 11.
cThe pure motor variant is reported in 5–15% of patients with GBS in most studies, but in 70% cases in Bangladesh 11, 50.
dDoes not fulfil commonly used diagnostic criteria for GBS, which require the presence of bilateral limb weakness or fulfilment of the criteria for Miller Fisher syndrome 51, 52
[Source 6 ]Figure 7. Types of Guillain-Barre syndrome
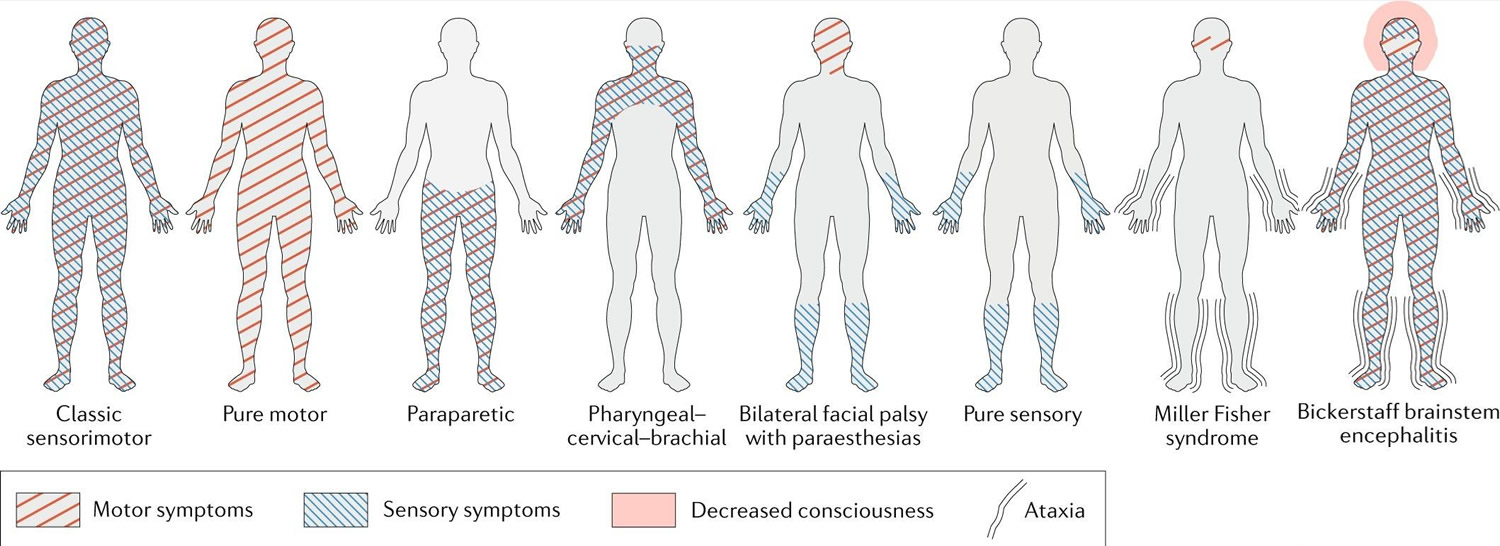
Footnotes: Pattern of symptoms typically observed in the different clinical variants of Guillain–Barré syndrome (GBS) and Miller Fisher syndrome and their subtypes. Guillain-Barré syndrome and Miller Fisher syndrome and their subtypes form a continuum of discrete and overlapping syndromes. Symptoms can be purely motor, purely sensory (rare) or a combination of motor and sensory. Ataxia can be present in patients with Miller Fisher syndrome and both decreased consciousness and ataxia can be present in patients with Bickerstaff brainstem encephalitis. Symptoms can be localized to specific regions of the body, and the pattern of symptoms differs between variants of GBS. Although bilateral facial palsy with paraesthesias, the pure sensory variant and Miller Fisher syndrome are included in the GBS spectrum, they do not fulfil the diagnostic criteria for Guillain–Barré syndrome (GBS).
- Classic Guillain-Barré syndrome: tetraparesis with or without motor cranial nerve involvement;
- Paraparetic Guillain-Barré syndrome: lower limbs;
- Pharyngeal–cervical–brachial weakness: bulbar, neck and upper limbs;
- Bifacial weakness with paraesthesias: facial and motor cranial nerve involvement are more frequent in demyelinating-type classic Guillain-Barré syndrome (acute inflammatory demyelinating polyradiculoneuropathy) than in axonal-type (acute motor axonal neuropathy).
- Miller Fisher syndrome: external ophthalmoplegia, ataxia (unsteady gait) and areflexia (absence of deep tendon reflexes)
- Bickerstaff’s brainstem encephalitis: Bickerstaff’s brainstem encephalitis, there is additional hypersomnolence and decreased consciousness.
Guillain-Barre syndrome signs and symptoms
Guillain-Barre syndrome can start in many different ways. Guillain-Barre syndrome often begins with tingling (pins and needles) and weakness starting in your feet and legs and spreading to your upper body and arms. Some people notice the first symptoms in the arms or face. As Guillain-Barre syndrome progresses, muscle weakness can turn into almost total paralysis.
Signs and symptoms of Guillain-Barre syndrome may include 53:
- A pins and needles sensation in your fingers, toes, ankles or wrists
- Weakness in your legs that spreads to your upper body
- Unsteady walking or inability to walk or climb stairs
- Difficulty with facial movements, including speaking, chewing or swallowing
- Double vision, blurred vision or difficulty moving your eyes
- Severe pain that may feel achy, shooting or cramplike and may be worse at night
- Difficulty difficulty controlling your bladder or bowels
- Rapid heart rate
- Low or high blood pressure
- Difficulty breathing
People with Guillain-Barre syndrome usually experience their most significant weakness within two weeks after symptoms begin.
Guillain-Barre syndrome complications
Guillain-Barre syndrome affects your nerves. Because nerves control your movements and body functions, people with Guillain-Barre may experience 6, 54:
- Breathing difficulties. The weakness or paralysis can spread to the muscles that control your breathing, a potentially fatal complication. Up to 22% of people with Guillain-Barre syndrome need temporary help from a machine to breathe within the first week when they’re hospitalized for treatment.
- Choking
- Residual numbness or other sensations. Most people with Guillain-Barre syndrome recover completely or have only minor, residual weakness, numbness or tingling.
- Heart and blood pressure problems. Blood pressure fluctuations and irregular heart rhythms (cardiac arrhythmias) are common side effects of Guillain-Barre syndrome.
- Pain. One-third of people with Guillain-Barre syndrome experience severe nerve pain, which may be eased with medication.
- Bowel and bladder function problems. Sluggish bowel function or constipation and urine retention may result from Guillain-Barre syndrome.
- Blood clots. People who are immobile due to Guillain-Barre syndrome are at risk of developing blood clots. Until you’re able to walk independently, taking blood thinners and wearing support stockings may be recommended.
- Pressure sores. Being immobile also puts you at risk of developing bedsores (pressure sores). Frequent repositioning may help avoid this problem.
- Compression neuropathy
- Corneal ulceration
- Hospital-acquired infections (e.g., pneumonia, sepsis or urinary tract infection)
- Pain and tactile allodynia
- Delirium
- Depression
- Dietary deficiency
- Limb contractures and ossifications
- Relapse. A small percentage of people with Guillain-Barre syndrome have a relapse, experiencing muscle weakness even years after the symptoms ended.
Severe, early symptoms of Guillain-Barre syndrome significantly increase the risk of serious long-term complications. With prolonged recovery possible, GBS patients with continued neurologic deficits may benefit from ongoing physical therapy and conditioning programs. Rarely, death may occur from complications such as respiratory distress syndrome and heart attacks.
Guillain-Barre syndrome causes
The exact cause of Guillain-Barre syndrome isn’t known. Some theories suggest an autoimmune trigger, where your immune system (antibodies and white blood cells) — which usually attacks only invading organisms begins attacking your nerves, damaging myelin (nerve covering or insulation), leading to numbness and weakness 7. In a subgroup of patients with GBS, serum antibodies are found against gangliosides, which reside at high densities in the axolemma and other components of the peripheral nerves 55, 56. Complement activation, infiltration of macrophages and oedema are typical characteristics of affected peripheral nerves and nerve roots in patients with Guillain-Barre syndrome 56. In acute inflammatory demyelinating polyradiculoneuropathy (AIDP), the nerves’ protective covering (myelin sheath) is damaged. The damage prevents nerves from transmitting signals to your brain, causing weakness, numbness or paralysis.
Guillain-Barre syndrome usually appears days or 6 weeks after a respiratory or digestive tract infection 11. Six pathogens have been temporally associated with Guillain-Barre syndrome in case–control studies: Campylobacter jejuni, cytomegalovirus, hepatitis E virus, Mycoplasma pneumoniae, Epstein–Barr virus and Zika virus 57, 58, 59. It has been suggested that other pathogens such as influenza, human immunodeficiency virus (HIV) infection, varicella-zoster virus (VZV) infection, dengue virus infection, Chikungunya virus infection and human T-cell lymphotropic virus type 3 (HTLV-III) infection have been linked to GBS on the basis of evidence from case series or epidemiological studies, but their role in the pathogenesis of GBS is uncertain 60, 61, 62, 63, 64, 65. Guillain-Barre syndrome may occur after infection with the COVID-19 virus. Rarely, recent surgery and cancer can trigger Guillain-Barre syndrome, but these relationships lack a clear biological rationale and the epidemiological evidence is limited 66, 67. In general, the absence of an antecedent illness does not exclude a diagnosis of GBS, as putative infections or other immunological stimuli can be subclinical 6.
A relationship between administration of immunobiologicals (for example, tumour necrosis factor antagonists, immune checkpoint inhibitors or type 1 interferons) and Guillain-Barre syndrome has been reported on the basis of case series information and biological plausibility 68.
In the past Guillain-Barre syndrome had been previously observed in individuals who received the meningococcal, tetanus-toxoid, human papillomavirus (HPV), and most prominently, the influenza vaccines 21, 22, 23, 24. Influenza vaccines were first linked to Guillain-Barre syndrome in 1976 when a 7.3-fold increase in the risk of GBS was observed among nonmilitary individuals in the United States who had received the ‘swine’ influenza vaccine 69. The epidemiological link between other vaccines and GBS has been examined many times since, but only two further studies showed a relationship between GBS and influenza vaccines 70, 71. These studies suggested an increase of approximately one additional Guillain-Barre syndrome case per one million influenza vaccinations, which is several orders of magnitude lower than that observed for the 1976 influenza vaccine 72, 73.
More recently, Guillain-Barre syndrome is also a rare reaction to those who receive the Johnson & Johnson or AstraZeneca COVID-19 vaccine 14, 4, 15, 16.
Risk factors for developing Guillain-Barre syndrome
Guillain-Barre syndrome can affect all age groups, but your risk increases as you age. Guillain-Barre syndrome is also slightly more common in males than females.
Guillain-Barre syndrome may be triggered by 74, 21, 22, 23, 24, 14, 4, 15, 16:
- Most commonly, infection with Campylobacter, a type of bacteria often found in undercooked poultry
- Influenza virus
- Cytomegalovirus
- Epstein-Barr virus
- Zika virus
- Hepatitis A, B, C and E virus
- HIV, the virus that causes AIDS
- Mycoplasma pneumonia
- Surgery
- Trauma
- Hodgkin’s lymphoma
- Rarely, influenza vaccinations or childhood vaccinations
- COVID-19 virus
- COVID-19 Johnson & Johnson and AstraZeneca vaccine
Guillain-Barre syndrome pathophysiology
The pathophysiology of Guillain-Barre syndrome is theorized to be an autoimmune response against peripheral nerve components namely the myelin sheath causing Acute Inflammatory Demyelinating Polyneuropathy (AIDP) or the axonal membranes causing Acute Motor Axonal Neuropathy (AMAN) or Acute Motor Sensory Axonal Neuropathy (AMSAN). Normally the immune system attacks any germs that get into the body. But in people with Guillain-Barré syndrome, something goes wrong and the immune system mistakenly attacks and damages the nerves. In most cases of GBS, the immune system damages the myelin sheath that surrounds the axons of many peripheral nerves; however, it also may also damage the axons themselves. As a result, the nerves cannot transmit signals efficiently and the muscles begin to lose their ability to respond to the brain’s commands. This causes weakness. It’s not clear exactly why this happens, but the condition often happens after an infection; especially an infection of the airways, such as flu, or an infection of the digestive system, such as food poisoning or a stomach bug (gastroenteritis) 57. In rare cases vaccinations may increase the risk of GBS (there have been reports of a few people who received a COVID-19 vaccine developing GBS, but the chance of this occurring is very low). Some countries worldwide reported an increased incidence of GBS following infection with the Zika virus. See more causes above.
GBS may occur with infections from viruses or bacteria, such as:
- Influenza
- Some gastrointestinal illnesses such as campylobacter jejuni (C. jejuni)
- Mycoplasma pneumonia
- HIV, the virus that causes HIV/AIDS (very rare)
- Herpes simplex virus (HSV)
- Cytomegalovirus (CMV)
- Epstein–Barr virus (EBV) causing infectious mononucleosis
- Hepatitis A, B, C and E virus
- Zika virus
- COVID-19
GBS may also occur with other medical conditions, such as:
- Systemic lupus erythematosus
- Hodgkin disease
- After surgery
- Cancer
The Guillain-Barre syndrome (GBS) and its variants are considered post-infectious, immune-mediated neuropathies. Evidence from animal models suggests a key role of molecular mimicry. The lipooligosaccharide of Campylobacter jejuni is similar to the gangliosides of peripheral nerve membranes 75. Passive immunization of rabbits with these ganglioside-like lipooligosaccharides have led to similar clinical syndromes of flaccid tetraplegia, similar to the acute motor axonal neuropathy variant of GBS 76, 77. Ganglioside antibodies have been shown to have different peripheral nerve targets. Anti-GD1a antibodies bind to paranadol myelin, nodes of Ranvier, and neuromuscular junction 78, 79. GM1 and GQ1B antibodies bind to a peripheral nerve or neuromuscular junction 80, 81. These different peripheral nerve targets may play a role in the heterogeneity of the clinical presentation of GBS. Additionally, complement cascade is activated and plays a key role in the Guillain-Barre syndrome pathogenesis 82.
Certain gangliosides are more likely to be associated with specific presentations. For example, Miller-Fisher syndrome is associated with the anti-GQ1B antibody 83. The axonal motor neuropathy form may be associated with anti-GM1 antibodies 84. The pharyngeal-cervical-brachial variant of GBS may be associated with anti-GT1A antibodies 85. However, besides Miller-Fisher syndrome’s association with anti-GQ1B antibodies, sensitivity and specificity of all antibodies for specific subtypes are low-to-moderate yield for clinical utility.
Given that not all patients test positive for anti-ganglioside antibodies, further research is needed to elucidate the roles of anti-ganglioside antibodies in GBS, as causal or epiphenomenon. Less is known about the pathophysiology behind the acute inflammatory demyelinating polyneuropathy variant (AIDP) of GBS, despite the fact that it is considered the most common variant in the United States 86.
Guillain-Barre syndrome diagnosis
Guillain-Barre syndrome can be difficult to diagnose in its earliest stages, because Guillain-Barré syndrome signs and symptoms are similar to those of other neurological disorders and may vary from person to person. Your doctor is likely to start with a medical history and thorough physical examination. You may need to see a neurologist and have spinal tap (lumbar puncture), electromyography, nerve conduction studies and antibody tests in order to exclude other diagnoses and confirm the diagnosis of Guillain-Barré syndrome.
Physical examination of patients with Guillain-Barre syndrome show weakness that is equal on both sides of the body and loss of reflexes, particularly at the ankles and knees.
Guillain-Barre syndrome test
The ordering of specific tests should be guided by the patient’s history and presentation.
- Spinal tap or lumbar puncture.A spinal tap or lumbar puncture is a procedure where a needle is inserted in the lower back to sample the spinal fluid that surrounds the brain, spinal cord, and the nerves that come out of the spinal cord. In Guillain-Barré syndrome, the spinal fluid protein concentration is high, but there is no evidence of inflammation. Most, but not all (the level may remain normal in 10% of patients), patients with Guillain-Barré syndrome have an elevated cerebrospinal fluid (CSF) protein level (>400 mg/L), with normal CSF cell counts. The increase in CSF protein is thought to reflect the widespread inflammation of the nerve roots. Elevated or rising protein levels on serial lumbar punctures and 10 or fewer mononuclear cells/mm³ strongly support the diagnosis 87. The test is most likely to be abnormal a week or more after symptoms start.
- Electromyography (EMG). Thin-needle electrodes are inserted into the muscles your doctor wants to study. The electrodes measure nerve activity in the muscles. Needle EMG may be normal in acute nerve lesions, and it may take 3-4 weeks for fibrillation to develop. In the acute phase, the only needle EMG abnormality may be abnormal motor recruitment, with decreased recruitment and rapid firing motor units in weak muscles. Unfortunately, electrodiagnostic studies can be completely normal in acute Guillain-Barre syndrome and a normal study does not rule out GBS 88, 89.
- Nerve conduction studies. Electrodes are taped to the skin above your nerves. A small shock is passed through the nerve to measure the speed of nerve signals. Nerve conduction studies can tell whether the insulation of the nerves or the nerves themselves are damaged. This test is more likely to be abnormal two weeks after symptoms start. Nerve conduction studies can also help determine prognosis, particularly if they are repeated during the first few weeks after symptoms start.
- Serum autoantibodies. There are antibody tests on blood that can help confirm that a patient has the Miller Fisher variant of Guillain-Barré syndrome, but routine antibody tests for the more common form of Guillain-Barre syndrome are not available. Antibodies to glycolipids are observed in the sera of 60-70% of patients with GBS during the acute phase, with gangliosides being the major target antigens 90. Specific antibodies found in association with Guillain-Barré syndrome include the following:
- Antibodies to GM1: Frequently found in the sera of patients with the acute motor axonal neuropathy (AMAN) or acute demyelinating polyradiculoneuropathy (AIDP) variants of Guillain-Barré syndrome.
- Anti-GM1 antibodies: Elevated titers are closely associated antecedent Campylobacter jejuni infections
- Anti-GQ1b antibodies: Found in patients with GBS with ophthalmoplegia, including patients with the Miller-Fisher variant
- Other antibodies to different major and minor gangliosides also have been found in GBS patients.
- Peripheral neuropathy workup. A basic peripheral neuropathy workup is recommended in cases in which the diagnosis is uncertain. These studies may include the following:
- Thyroid panel
- Rheumatology profiles
- Vitamin B-12
- Folic acid
- Hemoglobin A1C
- Erythrocyte sedimentation rate (ESR)
- Rapid protein reagent
- Immunoelectrophoresis of serum protein
- Tests for heavy metals
- The following should be considered:
- Liver function test (LFT) results are elevated in as many as one third of patients
- Creatine phosphokinase (CPK) and erythrocyte sedimentation rate (ESR) may be elevated with myopathies or systemic inflammatory conditions
- A stool culture for C jejuni and a pregnancy test are also indicated
- The syndrome of inappropriate antidiuretic hormone (SIADH) may occur
Basic laboratory studies, such as complete blood counts (CBCs) and metabolic panels, are normal and of limited value in the workup. They are often ordered, however, to exclude other diagnoses and to better assess functional status and prognosis.
Imaging studies, such as magnetic resonance imaging (MRI) and computed tomography (CT) scanning of the spine, may be more helpful in excluding other diagnoses, such as mechanical causes of myelopathy, than in assisting in the diagnosis of GBS.
Diagnostic criteria for Guillain-Barre syndrome
This diagnostic criteria for Guillain–Barré syndrome (GBS) was developed by the National Institute of Neurological Disorders and Stroke 52 and subsequently modified in a review paper 7. Some scientists have added some features that cast doubt on the diagnosis, which were not mentioned in the original criteria 91, 52, 7 and have made some adaptations to improve readability. These criteria are not applicable to some of the specific variants of Guillain–Barré syndrome, as described in Table 1 above.
Notes:
aStatements in the National Institute of Neurological Disorders and Stroke criteria that were adapted by authors to improve readability.
bAdditional features which were not included in the National Institute of Neurological Disorders and Stroke
Features required for Guillain–Barré syndrome (GBS) diagnosis
- Progressive bilateral weakness of arms and legs (initially only legs may be involved) a
- Absent or decreased tendon reflexes in affected limbs (at some point in clinical course) a
Features that strongly support Guillain–Barré syndrome (GBS) diagnosis
- Progressive phase lasts from days to 4 weeks (usually <2 weeks)
- Relative symmetry of symptoms and signs
- Relatively mild sensory symptoms and signs (absent in pure motor variant) a
- Cranial nerve involvement, especially bilateral facial palsy a
- Autonomic dysfunction
- Muscular or radicular back or limb pain b
- Increased protein level in cerebrospinal fluid (CSF); normal protein levels do not rule out the diagnosis b
- Electrodiagnostic features of motor or sensorimotor neuropathy (normal electrophysiology in the early stages does not rule out the diagnosis) b
Features that cast doubt on Guillain–Barré syndrome (GBS) diagnosis
- Increased numbers of mononuclear or polymorphonuclear cells in CSF (>50 × 106/l)
- Marked, persistent asymmetry of weakness
- Bladder or bowel dysfunction at onset or persistent during disease course b
- Severe respiratory dysfunction with limited limb weakness at onset b
- Sensory signs with limited weakness at onset a
- Fever at onset
- Nadir <24 hour b
- Sharp sensory level indicating spinal cord injury a
- Hyper-reflexia or clonus b
- Extensor plantar responses b
- Abdominal pain b
- Slow progression with limited weakness without respiratory involvement
- Continued progression for >4 weeks after start of symptoms b
- Alteration of consciousness (except in Bickerstaff brainstem encephalitis) b
Guillain-Barre syndrome differential diagnosis
The differential diagnosis of Guillain–Barré syndrome is broad and highly dependent on the clinical features of the individual patient. Here, we present an overview of the most important differential diagnoses categorized by location in the nervous system.
Central nervous system (brain and spinal cord)
- Inflammation or infection of the brainstem (for example, sarcoidosis, Sjögren syndrome, neuromyelitis optica or myelin oligodendrocyte glycoprotein antibody-associated disorder)
- Inflammation or infection of the spinal cord (for example, sarcoidosis, Sjögren syndrome or acute transverse myelitis)
- Malignancy (for example, leptomeningeal metastases or neurolymphomatosis)
- Compression of brainstem or spinal cord
- Brainstem stroke
- Vitamin deficiency (for example, Wernicke encephalopathya, caused by deficiency of vitamin B1, or subacute combined degeneration of the spinal cord, caused by deficiency of vitamin B12)
Anterior horn cells
- Acute flaccid myelitis (for example, as a result of polio, enterovirus D68 or A71, West Nile virus, Japanese encephalitis virus or rabies virus)
Nerve roots
- Infection (for example, Lyme disease, cytomegalovirus, HIV, Epstein–Barr virus or varicella zoster virus)
- Compression
- Leptomeningeal malignancy
Peripheral nerves
- Chronic inflammatory demyelinating polyradiculoneuropathy (CIDP)
- Metabolic or electrolyte disorders (for example, hypoglycaemia, hypothyroidism, porphyria or copper deficiency)
- Vitamin deficiency (for example, deficiency of vitamins B1 (also known as beriberi), B12 or E)
- Toxins (for example, drugs, alcohol, vitamin B6, lead, thallium, arsenic, organophosphate, ethylene glycol, diethylene glycol, methanol or N-hexane)
- Critical illness polyneuropathy
- Neuralgic amyotrophy
- Vasculitis
- Infection (for example, diphtheria or HIV)
Neuromuscular junction
- Myasthenia gravis
- Lambert–Eaton myasthenic syndrome
- Neurotoxins (for example, botulism, tetanus, tick paralysis or snakebite envenomation)
- Organophosphate intoxication
Muscles
- Metabolic or electrolyte disorders (for example, hypokalaemia, thyrotoxic hypokalaemic periodic paralysis, hypomagnesaemia or hypophosphataemia)
- Inflammatory myositis
- Acute rhabdomyolysis
- Drug-induced toxic myopathy (for example, induced by colchicine, chloroquine, emetine or statins)
- Mitochondrial disease
Other
- Conversion or functional disorder
Guillain-Barre syndrome treatment
There’s no cure for Guillain-Barre syndrome. In the early stages, you usually need to be in hospital so doctors can monitor your breathing. Approximately one third of patients require admission to an intensive care unit (ICU), primarily because of respiratory failure, to be on a ventilator in to help you breathe. Up to two-thirds of the deaths of patients with GBS occur during the recovery phase and are mostly caused by cardiovascular and respiratory dysfunction 7, 11. Therefore regular monitoring for disease progression and the occurrence of complications such as arrhythmias, blood pressure shifts, or respiratory distress caused by mucus plugs is especially important in patients who have recently left the ICU and in those with cardiovascular risk factors.
2 types of treatments can speed recovery and reduce the severity of the Guillain-Barre syndrome 6, 92, 93:
- Plasma exchange (plasmapheresis). The liquid portion of part of your blood (plasma) is removed and separated from your blood cells. The blood cells are then put back into your body, which manufactures more plasma to make up for what was removed. Plasmapheresis (200–250 ml plasma/kg body weight in five sessions) may work by getting rid of certain antibodies from your plasma that contribute to the immune system’s attack on the peripheral nerves.
- Intravenous immunoglobulin therapy (IVIG). Immunoglobulin containing healthy antibodies from blood donors is given through a vein (intravenously) (0.4 g/kg body weight daily for 5 days). High doses of immunoglobulin can block the damaging antibodies that may contribute to Guillain-Barre syndrome.
In well-controlled clinical trials, the efficacy of intravenous immunoglobulin therapy (IVIG) in GBS patients has been shown to equal that of plasma exchange (plasmapheresis) 34, 94, 95, 96. Mixing them or administering one after the other is no more effective than using either method alone 97. However, some clinicians prefer to try plasma exchange first, and if this does not provide patient improvement then they go to IVIG. Theoretically, if IVIG is given first, then the plasma exchange will be removing the IVIG, which was just given days earlier. There are no randomized controlled trials that allow one to decide on the best plan.
Other possible treatments modulating the immune system include complement inhibitors such as eculizumab. This has been shown to be effective in animal models of Miller-Fisher syndrome 98, 99 and to be safe in humans 100, 101. The Japanese Eculizumab Trial for GBS 101, a prospective, multicenter, placebo-controlled, double-blind, randomized phase 2 study, reported eculizumab to be safe in severe cases of GBS. The investigators also found that at 24 weeks, 91.6% of patients on eculizumab could walk independently and 74% could run, compared with 71.9% and 18%, respectively, for those on placebo. Nonetheless, the report noted that “the primary outcome measure did not reach the predefined response rate.” Moreover, the study, which was designed to evaluate safety, was considered underpowered with regard to showing efficacy 101.
Immunoglobulin for children with GBS has not been rigorously studied with randomized, well-controlled studies, but it is a standard aspect of treatment in this age group 102, 97. Immunoglobulin for pregnant women has not been studied, and safety for use during pregnancy has not been established.
Corticosteroids are ineffective as monotherapy 103, 104. According to moderate-quality evidence, corticosteroids given alone do not significantly hasten recovery from GBS or affect the long-term outcome 103. According to low-quality evidence, oral corticosteroids delay recovery 105, 103. Diabetes requiring insulin was significantly more common and hypertension less common with corticosteroids.
Substantial evidence shows that intravenous methylprednisolone alone produces neither significant benefit nor harm 105. In combination with IVIG, intravenous methylprednisolone may hasten recovery but does not significantly affect long-term outcome 103, 106.
You are also likely to be given medication to:
- Relieve pain, which can be severe. A tiered pharmacologic approach that starts with nonsteroidal anti-inflammatory drugs (NSAIDs) or acetaminophen, with narcotic agents added as needed, is usually recommended. Adjunct medications for pain, such as tricyclic antidepressants and certain anticonvulsants, may be beneficial for dysesthetic-type pains 107. Single small, randomized, controlled trials support the use of gabapentin or carbamazepine in the ICU for management during the acute phase of Guillain-Barre syndrome. Modalities such as transcutaneous electrical nerve stimulation (TENS) and heat may prove beneficial in the management of myalgia. Education and psychological counseling can decrease the amount of suffering associated with this pain and disability.
- Prevent blood clots, which can develop while you’re immobile. Prophylaxis with gradient compression hose and subcutaneous low-molecular-weight heparin (LMWH) may dramatically reduce the incidence of venous thromboembolism 108.
People with Guillain-Barre syndrome need physical help and therapy before and during recovery. Your care may include:
- Movement of your arms and legs by caregivers before recovery, to help keep your muscles flexible and strong
- Physical therapy during recovery to help you cope with fatigue and regain strength and proper movement
- Training with adaptive devices, such as a wheelchair or braces, to give you mobility and self-care skills
Guillain-Barre syndrome prognosis
Guillain-Barre syndrome recovery can take months and even years for some people. However, most people with Guillain-Barre syndrome experience this general timeline:
- After the first signs and symptoms, the condition tends to progressively worsen for about two weeks
- Symptoms reach a plateau within four weeks
- Recovery begins, usually lasting 6 to 12 months, though for some people it could take as long as three years
Among adults recovering from Guillain-Barre syndrome:
- About 80% can walk independently six months after diagnosis
- About 60% fully recover motor strength one year after diagnosis
- About 5% to 10% have very delayed and incomplete recovery
Children, who rarely develop Guillain-Barre syndrome, generally recover more completely than adults.
In a study by Gupta et al 109 in 35 patients (27 with classic Guillain-Barre syndrome and 8 with acute motor axonal neuropathy [AMAN]), Guillain-Barre syndrome-related deficits included neuropathic pain requiring medication therapy (28 patients), foot drop necessitating ankle-foot orthosis (AFO) use (21 patients), and locomotion difficulties requiring assistive devices (30 patients). At 1-year follow-up, the authors found continued foot drop in 12 of the AFO patients. However, significant overall functional recovery had occurred within the general cohort 109.
Studies have suggested that a large percentage of patients (60–80% of patients with GBS) continue to have fatigue-related problems, subsequently limiting their function at home and at work, as well as during leisure activities 110, 111, 112, 113. Treatment suggestions range from gentle exercise to improvement in sleep patterns to relief of pain or depression, if present 114.
Severe pain is reported in at least one-third of patients with GBS 1 year after disease onset and can persist for >10 years 115, 25. Chronic pain in GBS is characterized by muscle pain in the lower back and limbs, painful paraesthesias, arthralgia, and radicular pain. Although the pathogenesis of this pain is not fully understood, muscle pain and joint pain might be attributable to immobility, and neuropathic pain might be caused by regeneration of, or persistent damage to, small nerve fibers 115. Management strategies include encouraging mobilization and administering drugs for neuropathic or nociceptive pain 116.
Early recognition and management of psychological distress which may cause anxiety and/or depression is important in patients with GBS, especially as mental status can influence physical recovery and vice versa; referral to a psychologist or psychiatrist might be beneficial for some patients 117. Providing accurate information to patients on the relatively good chance of recovery and low recurrence risk (2–5%) can help reduce their fear 11. Connecting patients with others who have had GBS can also help guide them through the rehabilitation process. The GBS/CIDP Foundation International (https://www.gbs-cidp.org/) — the international patient association for GBS — and other national organizations can help establish these networks.
- Wakerley BR, Yuki N. Mimics and chameleons in Guillain–Barré and Miller Fisher syndromes. Practical Neurology 2015;15:90-99. http://dx.doi.org/10.1136/practneurol-2014-000937[↩][↩][↩][↩][↩][↩]
- Wakerley BR, Uncini A, Yuki N; GBS Classification Group; GBS Classification Group. Guillain-Barré and Miller Fisher syndromes–new diagnostic classification. Nat Rev Neurol. 2014 Sep;10(9):537-44. doi: 10.1038/nrneurol.2014.138. Erratum in: Nat Rev Neurol. 2014 Nov;10(11):612.[↩]
- Guillain-Barré Syndrome (GBS). https://www.gbs-cidp.org/gbs[↩]
- Mohseni Afshar Z, Sharma A, Babazadeh A, Alizadeh-Khatir A, Sio TT, Taghizadeh Moghadam MA, Tavakolli Pirzaman A, Mojadad A, Hosseinzadeh R, Barary M, Ebrahimpour S. A review of the potential neurological adverse events of COVID-19 vaccines. Acta Neurol Belg. 2022 Nov 16:1–36. doi: 10.1007/s13760-022-02137-2[↩][↩][↩][↩]
- Mori M, Kuwabara S, Fukutake T, Yuki N, Hattori T. Clinical features and prognosis of Miller Fisher syndrome. Neurology. 2001 Apr 24;56(8):1104-6. doi: 10.1212/wnl.56.8.1104[↩]
- Leonhard SE, Mandarakas MR, Gondim FAA, Bateman K, Ferreira MLB, Cornblath DR, van Doorn PA, Dourado ME, Hughes RAC, Islam B, Kusunoki S, Pardo CA, Reisin R, Sejvar JJ, Shahrizaila N, Soares C, Umapathi T, Wang Y, Yiu EM, Willison HJ, Jacobs BC. Diagnosis and management of Guillain-Barré syndrome in ten steps. Nat Rev Neurol. 2019 Nov;15(11):671-683. doi: 10.1038/s41582-019-0250-9[↩][↩][↩][↩][↩][↩][↩]
- Willison HJ, Jacobs BC, van Doorn PA. Guillain-Barré syndrome. Lancet. 2016 Aug 13;388(10045):717-27. doi: 10.1016/S0140-6736(16)00339-1[↩][↩][↩][↩][↩][↩]
- van den Berg B, Bunschoten C, van Doorn PA, Jacobs BC. Mortality in Guillain-Barre syndrome. Neurology. 2013 Apr 30;80(18):1650-4. doi: 10.1212/WNL.0b013e3182904fcc[↩]
- Domínguez-Moreno R, Tolosa-Tort P, Patiño-Tamez A, Quintero-Bauman A, Collado-Frías DK, Miranda-Rodríguez MG, Canela-Calderón OJ, Hurtado-Valadez P, de Gante-Castro R, Ortiz-Guillén KM, Estañol-Vidal B, Sentíes-Madrid H, García-Ramos G, Cantú-Brito C, Ruiz-Sandoval JL, Chiquete E. Mortalidad asociada al diagnóstico de síndrome de Guillain-Barré en adultos ingresados en instituciones del sistema sanitario Mexicano [Mortality associated with a diagnosis of Guillain-Barré syndrome in adults of Mexican health institutions]. Rev Neurol. 2014 Jan 1;58(1):4-10. Spanish.[↩]
- Christiaan Fokke, Bianca van den Berg, Judith Drenthen, Christa Walgaard, Pieter Antoon van Doorn, Bart Casper Jacobs, Diagnosis of Guillain-Barré syndrome and validation of Brighton criteria, Brain, Volume 137, Issue 1, January 2014, Pages 33–43, https://doi.org/10.1093/brain/awt285[↩][↩][↩][↩]
- Alex Y Doets, Christine Verboon, Bianca van den Berg, et al. IGOS Consortium, Regional variation of Guillain-Barré syndrome, Brain, Volume 141, Issue 10, October 2018, Pages 2866–2877, https://doi.org/10.1093/brain/awy232[↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Principi N, Esposito S. Vaccine-preventable diseases, vaccines and Guillain-Barre’ syndrome. Vaccine. 2019 Sep 3;37(37):5544-5550. doi: 10.1016/j.vaccine.2018.05.119[↩][↩]
- Ruts L, Drenthen J, Jacobs BC, van Doorn PA; Dutch GBS Study Group. Distinguishing acute-onset CIDP from fluctuating Guillain-Barre syndrome: a prospective study. Neurology. 2010 May 25;74(21):1680-6. doi: 10.1212/WNL.0b013e3181e07d14[↩][↩]
- Taga A, Lauria G. COVID-19 and the peripheral nervous system. A 2-year review from the pandemic to the vaccine era. J Peripher Nerv Syst. 2022 Mar;27(1):4-30. doi: 10.1111/jns.12482[↩][↩][↩]
- Chen, Y, Xu, Z, Wang, P, Li, X-M, Shuai, Z-W, Ye, D-Q, et al. New-onset autoimmune phenomena post-COVID-19 vaccination. Immunology. 2022; 165: 386– 401. https://doi.org/10.1111/imm.13443[↩][↩][↩]
- Kaulen LD, Doubrovinskaia S, Mooshage C, Jordan B, Purrucker J, Haubner C, Seliger C, Lorenz HM, Nagel S, Wildemann B, Bendszus M, Wick W, Schönenberger S. Neurological autoimmune diseases following vaccinations against SARS-CoV-2: a case series. Eur J Neurol. 2022 Feb;29(2):555-563. doi: 10.1111/ene.15147[↩][↩][↩]
- Goss AL, Samudralwar RD, Das RR, Nath A. ANA investigates: neurological complications of COVID-19 vaccines. Ann Neurol. 2021;89(5):856–857. doi: 10.1002/ana.26065[↩]
- Waheed S, Bayas A, Hindi F, Rizvi Z, Espinosa PS. Neurological complications of COVID-19: Guillain-Barre syndrome following Pfizer COVID-19 vaccine. Cureus. 2021 doi: 10.7759/cureus.13426[↩]
- James J, Jose J, Gafoor VA, Smita B, Balaram N. Guillain-Barre syndrome following ChAdOx1 nCoV-19 COVID-19 vaccination: a case series. Neurol Clin Neurosci. 2021;9(5):402–405. doi: 10.1111/ncn3.12537[↩]
- Patel SU, Khurram R, Lakhani A, Quirk B. Guillain-Barre syndrome following the first dose of the chimpanzee adenovirus-vectored COVID-19 vaccine, ChAdOx1. BMJ Case Rep. 2021;14(4):e242956. doi: 10.1136/bcr-2021-242956[↩]
- Babazadeh A, Mohseni Afshar Z, Javanian M, Mohammadnia-Afrouzi M, Karkhah A, Masrour-Roudsari J, Sabbagh P, Koppolu V, Vasigala VK, Ebrahimpour S. Influenza Vaccination and Guillain-Barré Syndrome: Reality or Fear. J Transl Int Med. 2019 Dec 31;7(4):137-142. doi: 10.2478/jtim-2019-0028[↩][↩][↩]
- Juurlink DN, Stukel TA, Kwong J, Kopp A, McGeer A, Upshur RE, et al. Guillain-Barre syndrome after influenza vaccination in adults: a population-based study. Arch Intern Med. 2006;166(20):2217–2221. doi: 10.1001/archinte.166.20.2217[↩][↩][↩]
- Souayah N, Michas-Martin PA, Nasar A, Krivitskaya N, Yacoub HA, Khan H, et al. Guillain-Barre syndrome after Gardasil vaccination: data from vaccine adverse event reporting system 2006–2009. Vaccine. 2011;29(5):886–889. doi: 10.1016/j.vaccine.2010.09.020[↩][↩][↩]
- Tuttle J, Chen RT, Rantala H, Cherry JD, Rhodes PH, Hadler S. The risk of Guillain-Barre syndrome after tetanus-toxoid-containing vaccines in adults and children in the United States. Am J Public Health. 1997;87(12):2045–2048. doi: 10.2105/AJPH.87.12.2045[↩][↩][↩]
- Kuitwaard, K., Bos-Eyssen, M.E., Blomkwist-Markens, P.H. and Van Doorn, P.A. (2009), Recurrences, vaccinations and long-term symptoms in GBS and CIDP. Journal of the Peripheral Nervous System, 14: 310-315. https://doi.org/10.1111/j.1529-8027.2009.00243.x[↩][↩]
- Stassart RM, Möbius W, Nave K-A, Edgar JM. The Axon-Myelin Unit in Development and Degenerative Disease. Frontiers in Neuroscience. 2018;12:467. doi:10.3389/fnins.2018.00467. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6050401/[↩]
- Waxman S G , Ritchie J M . Molecular dissection of the myelinated axon. Ann. Neurol. 1993;33:121–136.[↩]
- Morell P, Quarles RH. The Myelin Sheath. In: Siegel GJ, Agranoff BW, Albers RW, et al., editors. Basic Neurochemistry: Molecular, Cellular and Medical Aspects. 6th edition. Philadelphia: Lippincott-Raven; 1999. Available from: https://www.ncbi.nlm.nih.gov/books/NBK27954[↩]
- Ritchie, J. M. Physiological basis of conduction in myelinated nerve fibers. In P. Morell (ed.), Myelin, 2nd ed. New York: Plenum, 1984, pp. 117–141.[↩]
- Van der Knaap MS, Bugiani M. Leukodystrophies: a proposed classification system based on pathological changes and pathogenetic mechanisms. Acta Neuropathologica. 2017;134(3):351-382. doi:10.1007/s00401-017-1739-1. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5563342/[↩]
- Multiple sclerosis. Lancet. 2008 Oct 25;372(9648):1502-17. doi: 10.1016/S0140-6736(08)61620-7. https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(08)61620-7/fulltext[↩]
- Chronic inflammatory demyelinating polyneuropathy. Curr Opin Neurol. 2017 Oct;30(5):508-512. doi: 10.1097/WCO.0000000000000481. https://www.ncbi.nlm.nih.gov/pubmed/28763304[↩]
- Wakerley BR, Uncini A, Yuki N; GBS Classification Group; GBS Classification Group. Guillain-Barré and Miller Fisher syndromes–new diagnostic classification. Nat Rev Neurol. 2014 Sep;10(9):537-44. doi: 10.1038/nrneurol.2014.138 Erratum in: Nat Rev Neurol. 2014 Nov;10(11):612.[↩]
- Hadden, R.D.M., Cornblath, D.R., Hughes, R.A.C., Zielasek, J., Hartung, H.-.-P., Toyka, K.V., Swan, A.V. and (1998), Electrophysiological classification of guillain-barré syndrome: Clinical associations and outcome. Ann Neurol., 44: 780-788. https://doi.org/10.1002/ana.410440512[↩][↩][↩]
- Arányi, Z., Kovács, T., Sipos, I. and Bereczki, D. (2012), Miller Fisher syndrome: brief overview and update with a focus on electrophysiological findings. European Journal of Neurology, 19: 15-e3. https://doi.org/10.1111/j.1468-1331.2011.03445.x[↩]
- Lo, Y.L. (2007), Clinical and immunological spectrum of the Miller Fisher syndrome. Muscle Nerve, 36: 615-627. https://doi.org/10.1002/mus.20835[↩]
- Ito M, Kuwabara S, Odaka M, Misawa S, Koga M, Hirata K, Yuki N. Bickerstaff’s brainstem encephalitis and Fisher syndrome form a continuous spectrum: clinical analysis of 581 cases. J Neurol. 2008 May;255(5):674-82. doi: 10.1007/s00415-008-0775-0[↩]
- Sekiguchi, Y., Mori, M., Misawa, S., Sawai, S., Yuki, N., Beppu, M. and Kuwabara, S. (2016), How often and when Fisher syndrome is overlapped by Guillain-Barré syndrome or Bickerstaff brainstem encephalitis?. Eur J Neurol, 23: 1058-1063. https://doi.org/10.1111/ene.12983[↩][↩]
- Uncini, A. and Yuki, N. (2012), Sensory Guillain–Barré syndrome and related disorders: An attempt at systematization. Muscle Nerve, 45: 464-470. https://doi.org/10.1002/mus.22298[↩][↩]
- Graus F, Titulaer MJ, Balu R, Benseler S, Bien CG, Cellucci T, Cortese I, Dale RC, Gelfand JM, Geschwind M, Glaser CA, Honnorat J, Höftberger R, Iizuka T, Irani SR, Lancaster E, Leypoldt F, Prüss H, Rae-Grant A, Reindl M, Rosenfeld MR, Rostásy K, Saiz A, Venkatesan A, Vincent A, Wandinger KP, Waters P, Dalmau J. A clinical approach to diagnosis of autoimmune encephalitis. Lancet Neurol. 2016 Apr;15(4):391-404. doi: 10.1016/S1474-4422(15)00401-9[↩]
- Masaaki Odaka, Nobuhiro Yuki, Mitsunori Yamada, Michiaki Koga, Toshihiko Takemi, Koichi Hirata, Satoshi Kuwabara, Bickerstaff’s brainstem encephalitis: clinical features of 62 cases and a subgroup associated with Guillain–Barré syndrome, Brain, Volume 126, Issue 10, October 2003, Pages 2279–2290, https://doi.org/10.1093/brain/awg233[↩]
- Ito M, Matsuno K, Sakumoto Y, Hirata K, Yuki N. Ataxic Guillain-Barré syndrome and acute sensory ataxic neuropathy form a continuous spectrum. J Neurol Neurosurg Psychiatry. 2011 Mar;82(3):294-9. doi: 10.1136/jnnp.2010.222836[↩][↩]
- Wakerley BR, Kokubun N, Funakoshi K, Nagashima T, Hirata K, Yuki N. Clinical classification of 103 Japanese patients with Guillain-Barré syndrome. J Neurol Sci. 2016 Oct 15;369:43-47. doi: 10.1016/j.jns.2016.08.002[↩][↩][↩][↩][↩]
- Hiew FL, Ramlan R, Viswanathan S, Puvanarajah S. Guillain-Barré Syndrome, variants & forms fruste: Reclassification with new criteria. Clin Neurol Neurosurg. 2017 Jul;158:114-118. doi: 10.1016/j.clineuro.2017.05.006[↩][↩][↩][↩][↩][↩]
- Blum, S., Reddel, S., Spies, J. and McCombe, P. (2013), Clinical features of patients with Guillain-Barré syndrome at seven hospitals on the East Coast of Australia. J Peripher Nerv Syst, 18: 316-320. https://doi.org/10.1111/jns5.12045[↩]
- Zhang G, Li Q, Zhang R, Wei X, Wang J, Qin X. Subtypes and Prognosis of Guillain-Barré Syndrome in Southwest China. PLoS One. 2015 Jul 22;10(7):e0133520. doi: 10.1371/journal.pone.0133520[↩]
- Peric, S., Milosevic, V., Berisavac, I., Stojiljkovic, O., Beslac-Bumbasirevic, L., Marjanovic, I., Djuric, V., Djordjevic, G., Rajic, S., Cvijanovic, M., Babic, M., Dominovic, A., Vujovic, B., Cukic, M., Petrovic, M., Toncev, G., Komatina, N., Martic, V. and Lavrnic, D. (2014), Clinical and epidemiological features of Guillain-Barré syndrome in the Western Balkans. J Peripher Nerv Syst, 19: 317-321. https://doi.org/10.1111/jns.12096[↩]
- Wakerley BR, Uncini A, Yuki N; GBS Classification Group; GBS Classification Group. Guillain-Barré and Miller Fisher syndromes–new diagnostic classification. Nat Rev Neurol. 2014 Sep;10(9):537-44. doi: 10.1038/nrneurol.2014.138. Epub 2014 Jul 29. Erratum in: Nat Rev Neurol. 2014 Nov;10(11):612.[↩]
- Mitsui Y, Kusunoki S, Arimura K, Kaji R, Kanda T, Kuwabara S, Sonoo M, Takada K; Japanese GBS Study Group. A multicentre prospective study of Guillain-Barré syndrome in Japan: a focus on the incidence of subtypes. J Neurol Neurosurg Psychiatry. 2015 Jan;86(1):110-4. doi: 10.1136/jnnp-2013-306509[↩]
- Ishaque, T., Islam, M.B., Ara, G., Endtz, H.P., Mohammad, Q.D., Jacobs, B.C. and Islam, Z. (2017), High mortality from Guillain-Barré syndrome in Bangladesh. J Peripher Nerv Syst, 22: 121-126. https://doi.org/10.1111/jns.12215[↩]
- Sejvar JJ, Kohl KS, Gidudu J, Amato A, Bakshi N, Baxter R, Burwen DR, Cornblath DR, Cleerbout J, Edwards KM, Heininger U, Hughes R, Khuri-Bulos N, Korinthenberg R, Law BJ, Munro U, Maltezou HC, Nell P, Oleske J, Sparks R, Velentgas P, Vermeer P, Wiznitzer M; Brighton Collaboration GBS Working Group. Guillain-Barré syndrome and Fisher syndrome: case definitions and guidelines for collection, analysis, and presentation of immunization safety data. Vaccine. 2011 Jan 10;29(3):599-612. doi: 10.1016/j.vaccine.2010.06.003[↩]
- Asbury, A.K. and Cornblath, D.R. (1990), Assessment of current diagnostic criteria for Guillain-Barré syndrome. Ann Neurol., 27: S21-S24. https://doi.org/10.1002/ana.410270707[↩][↩][↩]
- Guillain-Barre syndrome. https://www.mayoclinic.org/diseases-conditions/guillain-barre-syndrome/symptoms-causes/syc-20362793[↩]
- Vereninging Spierziekten Nederland, Nederlandse Vereniging voor Neurologie & Nederlandse Vereniging van Revalidatieartsen [Dutch Association of Muscular Diseases & Dutch Society of Rehabilitation Specialists]. in Multidisciplinaire richtlijn Guillain-Barré syndroom [Multidisciplinary guideline Guillain-Barré syndrome] https://www.spierziekten.nl/fileadmin/user_upload/VSN/documenten/Hulpverleners_overig/R030-RichtlijnGBSherdruk2011metbijlagen.pdf[↩]
- Yoshikawa K, Kuwahara M, Morikawa M, Fukumoto Y, Yamana M, Yamagishi Y, Kusunoki S. Varied antibody reactivities and clinical relevance in anti-GQ1b antibody-related diseases. Neurol Neuroimmunol Neuroinflamm. 2018 Sep 11;5(6):e501. doi: 10.1212/NXI.0000000000000501[↩]
- Yuki N. Infectious origins of, and molecular mimicry in, Guillain-Barré and Fisher syndromes. Lancet Infect Dis. 2001 Aug;1(1):29-37. doi: 10.1016/S1473-3099(01)00019-6[↩][↩]
- Jacobs BC, Rothbarth PH, van der Meché FG, Herbrink P, Schmitz PI, de Klerk MA, van Doorn PA. The spectrum of antecedent infections in Guillain-Barré syndrome: a case-control study. Neurology. 1998 Oct;51(4):1110-5. doi: 10.1212/wnl.51.4.1110[↩][↩]
- Cao-Lormeau VM, Blake A, Mons S, Lastère S, Roche C, Vanhomwegen J, Dub T, Baudouin L, Teissier A, Larre P, Vial AL, Decam C, Choumet V, Halstead SK, Willison HJ, Musset L, Manuguerra JC, Despres P, Fournier E, Mallet HP, Musso D, Fontanet A, Neil J, Ghawché F. Guillain-Barré Syndrome outbreak associated with Zika virus infection in French Polynesia: a case-control study. Lancet. 2016 Apr 9;387(10027):1531-1539. doi: 10.1016/S0140-6736(16)00562-6[↩]
- van den Berg B, van der Eijk AA, Pas SD, Hunter JG, Madden RG, Tio-Gillen AP, Dalton HR, Jacobs BC. Guillain-Barré syndrome associated with preceding hepatitis E virus infection. Neurology. 2014 Feb 11;82(6):491-7. doi: 10.1212/WNL.0000000000000111[↩]
- Claudia Vellozzi, Shahed Iqbal, Karen Broder, Guillain-Barré Syndrome, Influenza, and Influenza Vaccination: The Epidemiologic Evidence, Clinical Infectious Diseases, Volume 58, Issue 8, 15 April 2014, Pages 1149–1155, https://doi.org/10.1093/cid/ciu005[↩]
- Thornton CA, Latif AS, Emmanuel JC. Guillain-Barré syndrome associated with human immunodeficiency virus infection in Zimbabwe. Neurology. 1991 Jun;41(6):812-5. doi: 10.1212/wnl.41.6.812[↩]
- Islam B, Islam Z, GeurtsvanKessel CH, Jahan I, Endtz HP, Mohammad QD, Jacobs BC. Guillain-Barré syndrome following varicella-zoster virus infection. Eur J Clin Microbiol Infect Dis. 2018 Mar;37(3):511-518. doi: 10.1007/s10096-018-3199-5[↩]
- Carod-Artal FJ, Wichmann O, Farrar J, Gascón J. Neurological complications of dengue virus infection. Lancet Neurol. 2013 Sep;12(9):906-919. doi: 10.1016/S1474-4422(13)70150-9[↩]
- Wielanek AC, Monredon JD, Amrani ME, Roger JC, Serveaux JP. Guillain-Barré syndrome complicating a Chikungunya virus infection. Neurology. 2007 Nov 27;69(22):2105-7. doi: 10.1212/01.wnl.0000277267.07220.88[↩]
- Cornblath, D.R., McArthur, J.C., Kennedy, P.G.E., Witte, A.S. and Griffin, J.W. (1987), Inflammatory demyelinating peripheral neuropathies associated with human T-cell lymphotropic virus type III infection. Ann Neurol., 21: 32-40. https://doi.org/10.1002/ana.410210107[↩]
- Hiew FL, Rajabally YA. Malignancy in Guillain-Barré syndrome: A twelve-year single-center study. J Neurol Sci. 2017 Apr 15;375:275-278. doi: 10.1016/j.jns.2017.02.024[↩]
- Rudant J, Dupont A, Mikaeloff Y, Bolgert F, Coste J, Weill A. Surgery and risk of Guillain-Barré syndrome: A French nationwide epidemiologic study. Neurology. 2018 Sep 25;91(13):e1220-e1227. doi: 10.1212/WNL.0000000000006246[↩]
- Kao JC, Brickshawana A, Liewluck T. Neuromuscular Complications of Programmed Cell Death-1 (PD-1) Inhibitors. Curr Neurol Neurosci Rep. 2018 Aug 4;18(10):63. doi: 10.1007/s11910-018-0878-7[↩]
- LAWRENCE B. SCHONBERGER, DENNIS J. BREGMAN, JOHN Z SULLIVAN-BOLYAI, RICHARD A. KEENLYSIDE, DONALD W. ZIEGLER, HENRY F. RETAILLIAU, DONALD L EDDINS, JOHN A. BRYAN, GUILLAIN-BARRE SYNDROME FOLLOWING VACCINATION IN THE NATIONAL INFLUENZA IMMUNIZATION PROGRAM, UNITED STATES, 1976–1977, American Journal of Epidemiology, Volume 110, Issue 2, August 1979, Pages 105–123, https://doi.org/10.1093/oxfordjournals.aje.a112795[↩]
- Burwen DR, Ball R, Bryan WW, Izurieta HS, La Voie L, Gibbs NA, Kliman R, Braun MM. Evaluation of Guillain-Barré Syndrome among recipients of influenza vaccine in 2000 and 2001. Am J Prev Med. 2010 Oct;39(4):296-304. doi: 10.1016/j.amepre.2010.05.022[↩]
- Kaplan JE, Katona P, Hurwitz ES, Schonberger LB. Guillain-Barré Syndrome in the United States, 1979-1980 and 1980-1981: Lack of an Association With Influenza Vaccination. JAMA. 1982;248(6):698–700. doi:10.1001/jama.1982.03330060038030[↩]
- Lasky T, Terracciano GJ, Magder L, Koski CL, Ballesteros M, Nash D, Clark S, Haber P, Stolley PD, Schonberger LB, Chen RT. The Guillain-Barré syndrome and the 1992-1993 and 1993-1994 influenza vaccines. N Engl J Med. 1998 Dec 17;339(25):1797-802. doi: 10.1056/NEJM199812173392501[↩]
- Juurlink DN, Stukel TA, Kwong J, et al. Guillain-Barré Syndrome After Influenza Vaccination in Adults: A Population-Based Study. Arch Intern Med. 2006;166(20):2217–2221. doi:10.1001/archinte.166.20.2217[↩]
- Haber P, Sejvar J, Mikaeloff Y, DeStefano F. Vaccines and Guillain-Barre syndrome. Drug Saf. 2009;32(4):309–323. doi: 10.2165/00002018-200932040-00005[↩]
- Yuki N, Taki T, Inagaki F, Kasama T, Takahashi M, Saito K, Handa S, Miyatake T. A bacterium lipopolysaccharide that elicits Guillain-Barré syndrome has a GM1 ganglioside-like structure. J Exp Med. 1993 Nov 1;178(5):1771-5. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2191246/pdf/je17851771.pdf[↩]
- Susuki, K., Nishimoto, Y., Yamada, M., Baba, M., Ueda, S., Hirata, K. and Yuki, N. (2003), Acute motor axonal neuropathy rabbit model: Immune attack on nerve root axons. Ann Neurol., 54: 383-388. https://doi.org/10.1002/ana.33333[↩]
- Yuki, N., Yamada, M., Koga, M., Odaka, M., Susuki, K., Tagawa, Y., Ueda, S., Kasama, T., Ohnishi, A., Hayashi, S., Takahashi, H., Kamijo, M. and Hirata, K. (2001), Animal model of axonal Guillain-Barré syndrome induced by sensitization with GM1 ganglioside. Ann Neurol., 49: 712-720. https://doi.org/10.1002/ana.1012[↩]
- Chiba A, Kusunoki S, Obata H, Machinami R, Kanazawa I. Serum anti-GQ1b IgG antibody is associated with ophthalmoplegia in Miller Fisher syndrome and Guillain-Barré syndrome: clinical and immunohistochemical studies. Neurology. 1993 Oct;43(10):1911-7. doi: 10.1212/wnl.43.10.1911[↩]
- Goodfellow JA, Bowes T, Sheikh K, Odaka M, Halstead SK, Humphreys PD, Wagner ER, Yuki N, Furukawa K, Furukawa K, Plomp JJ, Willison HJ. Overexpression of GD1a ganglioside sensitizes motor nerve terminals to anti-GD1a antibody-mediated injury in a model of acute motor axonal neuropathy. J Neurosci. 2005 Feb 16;25(7):1620-8. doi: 10.1523/JNEUROSCI.4279-04.2005[↩]
- Greenshields KN, Halstead SK, Zitman FM, Rinaldi S, Brennan KM, O’Leary C, Chamberlain LH, Easton A, Roxburgh J, Pediani J, Furukawa K, Furukawa K, Goodyear CS, Plomp JJ, Willison HJ. The neuropathic potential of anti-GM1 autoantibodies is regulated by the local glycolipid environment in mice. J Clin Invest. 2009 Mar;119(3):595-610. doi: 10.1172/JCI37338[↩]
- Hugh J. Willison, Graham O’Hanlon, Gary Paterson, Colin P. O’Leary, Jean Veitch, George Wilson, Mark Roberts, Teresa Tang, Angela Vincent, Mechanisms of Action of Anti-GM1 and Anti-GQ1b Ganglioside Antibodies in Guillain-Barré Syndrome, The Journal of Infectious Diseases, Volume 176, Issue Supplement_2, December 1997, Pages S144–S149, https://doi.org/10.1086/513799[↩]
- Susuki K, Rasband MN, Tohyama K, Koibuchi K, Okamoto S, Funakoshi K, Hirata K, Baba H, Yuki N. Anti-GM1 antibodies cause complement-mediated disruption of sodium channel clusters in peripheral motor nerve fibers. J Neurosci. 2007 Apr 11;27(15):3956-67. doi: 10.1523/JNEUROSCI.4401-06.2007[↩]
- Chiba, A., Kusunoki, S., Shimizu, T. and Kanazawa, I. (1992), Serum IgG antibody to ganglioside GQ1b is a possible marker of Miller Fisher syndrome. Ann Neurol., 31: 677-679. https://doi.org/10.1002/ana.410310619[↩]
- Gregson NA, Jones D, Thomas PK, Willison HJ. Acute motor neuropathy with antibodies to GM1 ganglioside. J Neurol. 1991 Dec;238(8):447-51. doi: 10.1007/BF00314652[↩]
- O’Leary CP, Veitch J, Durward WF, Thomas AM, Rees JH, Willison HJ. Acute oropharyngeal palsy is associated with antibodies to GQ1b and GT1a gangliosides. J Neurol Neurosurg Psychiatry. 1996 Dec;61(6):649-51. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC486666/pdf/jnnpsyc00012-0091.pdf[↩]
- Nguyen TP, Taylor RS. Guillain Barre Syndrome. [Updated 2022 Jul 4]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK532254[↩]
- Guillain-Barre Syndrome Workup. https://emedicine.medscape.com/article/315632-workup[↩]
- Albers, J.W. and Kelly, J.J., Jr (1989), Acquired inflammatory demyelinating polyneuropathies: Clinical and electrodiagnostic features. Muscle Nerve, 12: 435-451. https://doi.org/10.1002/mus.880120602[↩]
- Van Den Bergh, P.Y.K. and Piéret, F. (2004), Electrodiagnostic criteria for acute and chronic inflammatory demyelinating polyradiculoneuropathy. Muscle Nerve, 29: 565-574. https://doi.org/10.1002/mus.20022[↩]
- Kusunoki S. Antiglycolipid antibodies in Guillain-Barré syndrome and autoimmune neuropathies. Am J Med Sci. 2000 Apr;319(4):234-9. doi: 10.1097/00000441-200004000-00006[↩]
- Asbury AK, Arnason BGW, Karp HR, McFarlin DE. Criteria for diagnosis of Guillain-Barré syndrome. Ann. Neurol. 1978;3:565–566.[↩]
- Hughes RA, Swan AV, van Doorn PA. Intravenous immunoglobulin for Guillain-Barré syndrome. Cochrane Database Syst Rev. 2014 Sep 19;2014(9):CD002063. doi: 10.1002/14651858.CD002063.pub6[↩]
- Verboon C, van Doorn PA, Jacobs BC. Treatment dilemmas in Guillain-Barré syndrome. J Neurol Neurosurg Psychiatry. 2017 Apr;88(4):346-352. doi: 10.1136/jnnp-2016-314862[↩]
- Randomised trial of plasma exchange, intravenous immunoglobulin, and combined treatments in Guillain-Barré syndrome. Plasma Exchange/Sandoglobulin Guillain-Barré Syndrome Trial Group. Lancet. 1997 Jan 25;349(9047):225-30. https://doi.org/10.1016/S0140-6736(96)09095-2[↩]
- Koski CL, Patterson JV. Intravenous immunoglobulin use for neurologic diseases. J Infus Nurs. 2006 May-Jun;29(3 Suppl):S21-8. doi: 10.1097/00129804-200605001-00003[↩]
- Hughes RA, Swan AV, van Doorn PA. Intravenous immunoglobulin for Guillain-Barré syndrome. Cochrane Database Syst Rev. 2010 Jun 16;(6):CD002063. doi: 10.1002/14651858.CD002063.pub4. Update in: Cochrane Database Syst Rev. 2012;7:CD002063.[↩]
- Hughes RA, Wijdicks EF, Barohn R, Benson E, Cornblath DR, Hahn AF, Meythaler JM, Miller RG, Sladky JT, Stevens JC; Quality Standards Subcommittee of the American Academy of Neurology. Practice parameter: immunotherapy for Guillain-Barré syndrome: report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology. 2003 Sep 23;61(6):736-40. doi: 10.1212/wnl.61.6.736[↩][↩]
- Susan K. Halstead, Femke M. P. Zitman, Peter D. Humphreys, Kay Greenshields, Jan J. Verschuuren, Bart C. Jacobs, Russell P. Rother, Jaap J. Plomp, Hugh J. Willison, Eculizumab prevents anti-ganglioside antibody-mediated neuropathy in a murine model, Brain, Volume 131, Issue 5, May 2008, Pages 1197–1208, https://doi.org/10.1093/brain/awm316[↩]
- Halstead, S.K., Humphreys, P.D., Zitman, F.M.P., Hamer, J., Plomp, J.J. and Willison, H.J. (2008), C5 inhibitor rEV576 protects against neural injury in an in vitro mouse model of Miller Fisher syndrome. Journal of the Peripheral Nervous System, 13: 228-235. https://doi.org/10.1111/j.1529-8027.2008.00181.x[↩]
- Eculizumab Safe for Treatment of Guillain-Barré – Medscape – Oct 04, 2017. https://www.medscape.com/viewarticle/886564[↩]
- Misawa S, Kuwabara S, Sato Y, Yamaguchi N, et al. Japanese Eculizumab Trial for GBS (JET-GBS) Study Group. Safety and efficacy of eculizumab in Guillain-Barré syndrome: a multicentre, double-blind, randomised phase 2 trial. Lancet Neurol. 2018 Jun;17(6):519-529. doi: 10.1016/S1474-4422(18)30114-5[↩][↩][↩]
- 2003, High-dose immunoglobulin therapy for Guillain−Barré syndrome in Japanese children. Pediatrics International, 45: 543-549. https://doi.org/10.1046/j.1442-200X.2003.01768.x[↩]
- Hughes RA, Swan AV, van Doorn PA. Corticosteroids for Guillain-Barré syndrome. Cochrane Database Syst Rev. 2010 Feb 17;(2):CD001446. doi: 10.1002/14651858.CD001446.pub3. Update in: Cochrane Database Syst Rev. 2012;8:CD001446.[↩][↩][↩][↩]
- Winer JB. Guillain Barré syndrome. Mol Pathol. 2001 Dec;54(6):381-5. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1187127[↩]
- Hughes RA, Swan AV, van Koningsveld R, van Doorn PA. Corticosteroids for Guillain-Barré syndrome. Cochrane Database Syst Rev. 2006 Apr 19;(2):CD001446. doi: 10.1002/14651858.CD001446.pub2. Update in: Cochrane Database Syst Rev. 2010;(2):CD001446.[↩][↩]
- Odaka M, Tatsumoto M, Hoshiyama E, Hirata K, Yuki N. Side effects of combined therapy of methylprednisolone and intravenous immunoglobulin in Guillain-Barré syndrome. Eur Neurol. 2005;53(4):194-6. doi: 10.1159/000086477[↩]
- Pandey CK, Raza M, Tripathi M, Navkar DV, Kumar A, Singh UK. The comparative evaluation of gabapentin and carbamazepine for pain management in Guillain-Barré syndrome patients in the intensive care unit. Anesth Analg. 2005 Jul;101(1):220-5, table of contents. doi: 10.1213/01.ANE.0000152186.89020.36[↩]
- Richard A. C. Hughes, Jeremy H. Rees, Clinical and Epidemiologic Features of Guillain-Barré Syndrome, The Journal of Infectious Diseases, Volume 176, Issue Supplement_2, December 1997, Pages S92–S98, https://doi.org/10.1086/513793[↩]
- Gupta A, Taly AB, Srivastava A, Murali T. Guillain-Barre Syndrome – rehabilitation outcome, residual deficits and requirement of lower limb orthosis for locomotion at 1 year follow-up. Disabil Rehabil. 2010;32(23):1897-902. doi: 10.3109/09638281003734474[↩][↩]
- Hughes RA, Wijdicks EF, Benson E, Cornblath DR, Hahn AF, Meythaler JM, Sladky JT, Barohn RJ, Stevens JC; Multidisciplinary Consensus Group. Supportive care for patients with Guillain-Barré syndrome. Arch Neurol. 2005 Aug;62(8):1194-8. doi: 10.1001/archneur.62.8.1194[↩]
- Garssen, M.P.J., Blok, J.H., van Doorn, P.A. and Visser, G.H. (2006), Conduction velocity distribution in neurologically well-recovered but fatigued Guillain–Barré syndrome patients. Muscle Nerve, 33: 177-182. https://doi.org/10.1002/mus.20451[↩]
- de Vries JM, Hagemans ML, Bussmann JB, van der Ploeg AT, van Doorn PA. Fatigue in neuromuscular disorders: focus on Guillain-Barré syndrome and Pompe disease. Cell Mol Life Sci. 2010 Mar;67(5):701-13. doi: 10.1007/s00018-009-0184-2[↩]
- Merkies IS, Schmitz PI, Samijn JP, van der Meché FG, van Doorn PA. Fatigue in immune-mediated polyneuropathies. European Inflammatory Neuropathy Cause and Treatment (INCAT) Group. Neurology. 1999 Nov 10;53(8):1648-54. doi: 10.1212/wnl.53.8.1648[↩]
- Garssen MP, Bussmann JB, Schmitz PI, Zandbergen A, Welter TG, Merkies IS, Stam HJ, van Doorn PA. Physical training and fatigue, fitness, and quality of life in Guillain-Barré syndrome and CIDP. Neurology. 2004 Dec 28;63(12):2393-5. doi: 10.1212/01.wnl.0000148589.87107.9c[↩]
- Ruts L, Drenthen J, Jongen JL, Hop WC, Visser GH, Jacobs BC, van Doorn PA; Dutch GBS Study Group. Pain in Guillain-Barre syndrome: a long-term follow-up study. Neurology. 2010 Oct 19;75(16):1439-47. doi: 10.1212/WNL.0b013e3181f88345[↩][↩]
- Hughes RAC, Wijdicks EFM, Benson E, et al. Supportive Care for Patients With Guillain-Barré Syndrome. Arch Neurol. 2005;62(8):1194–1198. doi:10.1001/archneur.62.8.1194[↩]
- Bernsen, R.A.J.A.M., de Jager, A.E.J., Kuijer, W., van der MechÉ, F.G.A. and Suurmeijer, T.P.B.M. (2010), Psychosocial dysfunction in the first year after Guillain–Barré syndrome. Muscle Nerve, 41: 533-539. https://doi.org/10.1002/mus.21536[↩]





{kind=link}